Embed Size (px)
Citation preview
Diagnostic Immunohistochemistry
What Can Go Wrong and How to Prevent It
Allen M. Gown, MD
� Context.—There are a number of critical factors that canlead to incorrect results if the diagnostic pathologistperforming immunohistochemistry is unaware of, or notvigilant about, their influence.
Objective.—To highlight 3 arenas in which errors maybe introduced.
Data Sources.—For choosing the correct primaryantibody, selection of the most appropriate antibodies fora given clinical application can be aided by obtaininginformation from the vendor; however, this can yieldincomplete information. There are a number of onlinedatabases that have comparisons of antibodies fromdifferent vendors, particularly with respect to their useand properties. Reading the published literature can assistin this process, particularly with respect to determiningantibody sensitivity and specificity, but it is a daunting taskto keep up with all of the immunohistochemistry-related
papers published. Finally, Web sites of a number of qualityassurance organizations are accessible and can provide awealth of information comparing the ‘‘real world’’performance characteristics of different antibodies to thesame target protein. False-positive signals can result from anumber of factors, including the use of inappropriatelyhigh antibody concentration, and ‘‘pseudospecific’’ signalthat is in the wrong compartment of the cell. False-negative signal can result from factors such as use of anonoptimized epitope retrieval method. It is critical thatepitope retrieval methods be optimized for each antibodyemployed in the laboratory.
Conclusions.—By paying attention to these potentialproblems, the ‘‘black box’’ of diagnostic immunohisto-chemistry can be made more transparent.
(Arch Pathol Lab Med. 2016;140:893–898; doi: 10.5858/arpa.2016-0119-RA)
The great British science fiction writer, inventor, andfuturist Arthur C. Clarke noted that ‘‘any sufficiently
advanced technology is indistinguishable from magic.’’1
Immunohistochemistry (IHC), a technique invented in the1940s by Albert Coons and colleagues,2 is now performed,70 years later, in thousands of laboratories around theworld, many with closed autostainer systems that canresemble proverbial ‘‘black boxes.’’ As such, this advancedtechnology, may, in fact, appear to be inexplicable,especially to the neophyte. But it is important to have anunderstanding of the methodologies and to recognize theproblems that can make the result incorrect. It is importantto realize that IHC is not a ‘‘special stain,’’ akin to periodicacid–Schiff or trichrome stains, but is rather a slide-basedtest procedure that enables the detection of specific proteins,sugars, etc, in tissue sections, while simultaneously pre-serving tissue of histology. In the evaluation of theperformance of IHC in the diagnostic pathology laboratory,
and in analyzing possible problems, it is not always possibleto isolate the actual IHC procedure from the other‘‘preanalytic factors’’ to which the procedure is linked.Immunohistochemistry as a procedure is affected bypreanalytic variables, such as tissue fixation, embeddingthe tissue in paraffin, and performance of epitope retrieval,as parts of the actual IHC procedure. But perhaps the largestfactor determining the correct interpretation of the results isthe pathologist reading the slides; despite the besteducation, knowledge, and experience, misinterpretationscan occur. Different antibodies to the same target moleculecan produce very different results, and therefore this choiceis a critical one.In this review, I will focus on 3 common problems facing
the diagnostic pathologist in the use of IHC: antibodyselection, false-positive IHC signals, and false-negative IHCsignals.
ANTIBODY SELECTION
There are 4 major resources that can be employed to helpselect an addition to the laboratory’s IHC antibody library.These are the vendor, online databases, published literature,and independent quality assurance organizations.
The Vendor
There are a number of reliable vendors of immunohisto-chemical reagents, and it is generally a matter of experienceand word-of-mouth recommendations that can help thepathologist select the best antibody vendors. Virtually all
Accepted for publication May 19, 2016.From PhenoPath Laboratories, Seattle, Washington; and the
Department of Pathology, University of British Columbia, Vancouver,British Columbia, Canada.The author has no relevant financial interest in the products or
companies described in this article.Portions of this work were presented at the Canadian Anatomic
and Molecular Pathology Conference; January 29–30, 2016; Whis-tler, British Columbia, Canada.Reprints: Allen M. Gown, MD, PhenoPath Laboratories, 551 N
34th St, Seattle, WA 98103 (email: [email protected]).
Arch Pathol Lab Med—Vol 140, September 2016 Diagnostic Immunohistochemistry—Gown 893

vendors supply ‘‘product information sheets’’ describing theantibody, its protein (or other) target, and perhaps itsclinical applications. Nonetheless, even the best vendorsmay supply antibodies that are incompletely or evenincorrectly characterized (see below). And antibodies thatare ‘‘FDA cleared’’ (Food and Drug Administration cleared)are not necessarily better characterized (or even betterreagents) than those that have not been ‘‘FDA cleared.’’Nonetheless, in cases where an FDA-cleared and a non–FDA-cleared reagent to the same target are both available,the pathologist, in some situations, must select the FDA-cleared reagent.
Online Databases
There are a number of online databases that can assist thepathologist in selecting the most appropriate antibody totarget a specific molecule or marker. Some of the moreimportant Web sites are listed in the Table. Most of theseWeb sites contain lists of antibodies along with tables thatdetail critically important information, such as the type ofantibody (eg, monoclonal versus polyclonal, rabbit versusmouse) and the tested applications of the antibody (eg, IHC,Western blot, immunoprecipitation, etc). There are manyantibodies that will work well as reagents for Western blotsor immunoprecipitation but will not work in IHC. And thereare antibodies that will work on IHC studies performed onfrozen tissue sections, or cells grown in vitro, but will notwork on deparaffinized, formalin-fixed tissue. In addition,the antibodies may work for IHC on deparaffinized,formalin-fixed sections, but only under conditions notnecessarily determined by the vendor or listed in theInternet resources. Once received, it will be critical tooptimize every new antibody introduced into the laboratorywith its preferred epitope retrieval methodology, particularlywith respect to pH and buffer, as noted by Shi et al.3
Published Literature
There are a number of pathology publications, includingthis one, that reliably, every month, detail the results ofstudies of IHC applications to problems in diagnosticsurgical pathology. However, it is nearly impossible for thepracticing pathologist to keep up with the volume of paperspublished even in the most popular surgical pathologyjournals. To make matters worse, papers employing IHC asapplied, for example, to problems in oncology, areincreasingly published in the nonpathology literature,making them even more difficult to follow. The fallout inmissing new publications includes the potential failure toincorporate new markers with significantly increasedsensitivity compared with currently existing ones, as wellas the persistent use of antibodies with relatively poorspecificity. However, when one does read a paper describingthe IHC findings of a new antibody, my recommendation is
to first read the Materials and Methods section of the paperto determine the source of the antibody and learn how wellit has been characterized. Look at the photomicrographs: Isthe signal in the anticipated compartment of the cell (eg, ifan antibody to a nuclear transcription factor, is the signalexclusively in the nucleus, and not the cytoplasm?)? Asnoted below, the published IHC literature is still replete withantibodies with specificities that are not exactly what wasassumed by the authors.
Independent Organizations
Often, several different clones of monoclonal (rabbit ormouse) antibodies targeting different epitopes of the sameprotein are available, sometimes even from the samevendor. Independent IHC quality assurance organizations,such as Nordic Immunohistochemical Quality Control(NordicQC, Aalborg, Denmark; http://www.nordiqc.com)and the Canadian Immunohistochemistry Quality Control(cIQc, Vancouver, Canada; http://www.cpqa.ca), regularlypublish the results of surveys of the performance of manylaboratories employing different antibodies to the sametarget. It is possible to review the results of theseassessments and select not only antibodies but platformsand optimal procedures (heat-induced epitope retrieval,dilution, antibody incubation time).How can different antibodies to the same target molecule
behave differently in IHC assays? Even among antibodiesmade in the same species (eg, mouse or rabbit), there can bedramatic differences in antibody sensitivities, as well asantibody specificities (eg, cross-reactivity with nontargetproteins). Furthermore, there can be significant differencesin optimal protocols required by different antibodies (eg,epitope retrieval methods).One compelling example of striking differences in
antibody sensitivities is found in a recent study in whichthe sensitivities of several different antibodies to theintestinal transcription factor CDX-2 were compared.4 Therabbit monoclonal antibody to CDX-2, EPR2764Y, wasfound to be superior in sensitivity to the other anti–CDX-2clones tested, being the only antibody that identified thesubpopulation of CDX-2–positive cells in the normalpancreas. In a different study of the comparative sensitivitiesof two different TTF-1 antibodies, the SPT24 rabbitmonoclonal antibody was found to be significantly moresensitive for the detection of all lung carcinoma histologicsubtypes than the 8G7G3/1 mouse monoclonal antibody.5
Nonetheless, several studies have demonstrated decreasedspecificity of the SPT24 compared with 8G7G3/1.6
The importance of knowledge of differences in antibodyspecificities can be highlighted by recent experience withantibodies to the gynecological and genitourinary nucleartranscription factor PAX-8. Several studies published in2011 documented widespread expression of this transcrip-tion factor in normal tissues and in tumors of the kidney,ovary, and thyroid, where it is still employed today.However, these studies also ‘‘documented’’ PAX-8 expres-sion in lymphomas and thymomas.7–9 More recent studieshave shown that the rabbit polyclonal antibody employed inthese 2011 studies is not completely PAX-8 specific. Thispolyclonal antibody apparently cross-reacts with two othermembers of PAX family, PAX-5 and PAX-6, a fact that wasunknown when the vendor was first selling this antibody. Infact, using more specific monoclonal anti–PAX-8 antibodies,it has been demonstrated unequivocally that PAX-8 is notexpressed in thymic tumors or lymphomas.10–12 The lesson
Recommended Antibody Resource Web Sites
http://www.proteinatlas.org (last accessed May 16, 2016)http://www.antibodyresource.com (Cambridgeshire, UK; lastaccessed May 16, 2016)
http://www.antibodyregistry.org (last accessed May 16,2016)
http://www.biocompare.com/antibodies (South SanFrancisco, California; last accessed May 16, 2016)
http://www.antibodypedia.com (Solna, Sweden; lastaccessed May 16, 2016)
894 Arch Pathol Lab Med—Vol 140, September 2016 Diagnostic Immunohistochemistry—Gown

of this unfortunate ‘‘mischaracterization’’ of PAX-8 by usingantibodies of inferior specificity is that it is quite importantfor the pathologist performing immunohistochemistry tohave reasonable certainty about the specificity of the
antibodies being employed in the laboratory. In the caseof the cross-reacting PAX-8 antibodies, overreliance on theinformation provided by the vendor was partly responsible.And although it may be beyond the scope of the diagnostic
Figure 1. Effect of increasing antibody concentration on immunostaining signal, producing false-positive signal at excess antibody concentration. A,Hematoxylin-eosin–stained section of papillary lung adenocarcinoma. B through F, Anti–PAX-8 antibody BC-12 at working dilution, 1:250 (B); 1:10(C); 1:50 (D); 1:25 (E); and 1:10 (F). Note the appearance of false-positive nuclear (and cytoplasmic) signal at highest concentrations (originalmagnification3200).
Arch Pathol Lab Med—Vol 140, September 2016 Diagnostic Immunohistochemistry—Gown 895
pathology IHC laboratory, there are well-defined hierar-chies of proof of antibody specificity that can be tested.However, antibodies employed in the diagnostic IHClaboratory have rarely been subjected to high standards ofdetermination of their specificity. Perhaps the highest levelof proof of antibody specificity, and one that very few IHCreagents attain, is the abrogation of signal using tissueseither genetically deficient for the protein, or cells that havebeen treated with siRNAs which completely abrogatesexpression of the protein in question.13
FALSE-POSITIVE SIGNALS
The most common causes of false-positive signals in IHCpreparations include nonspecific background signal, endog-enous peroxidase, the use of inappropriately high antibodyconcentrations, pigment mistaken for true signal, endoge-nous biotin, drying artifact, and ‘‘pseudospecific’’ signal. Iwill focus on 3 of these factors.
High nonspecific background generally represents bind-ing of antibodies by mechanisms other than specific bindingof their epitope on the target antigen. This signal cangenerally be blocked with any protein that does not have anaffinity for the target or program components. Normalserum, bovine serum almond, gelatin, and dry milk aregenerally good blocking reagents.The effect of inappropriately high antibody concentrations
can be seen in Figure 1. Note that with increasing antibodyconcentration a tumor (papillary lung carcinoma) knownnot to express the transcription factor (PAX-8) in questioncan develop significant nuclear signal by just inappropriatelyincreasing the primary antibody concentration.A ‘‘pseudospecific’’ signal is one that is characterized by a
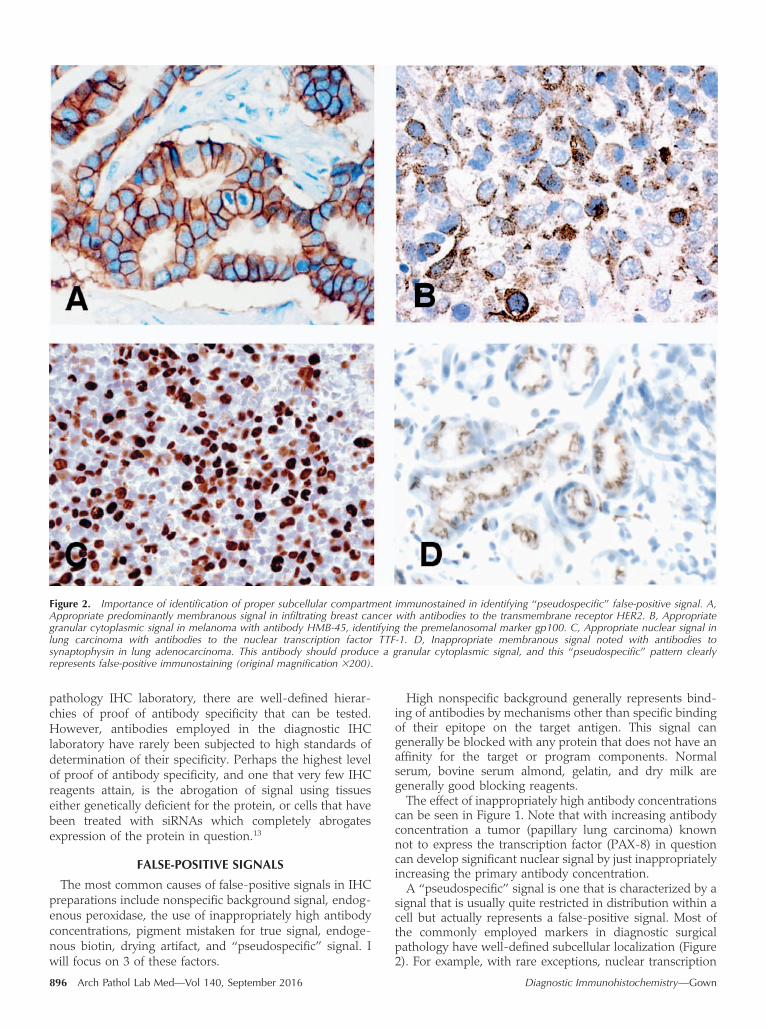
signal that is usually quite restricted in distribution within acell but actually represents a false-positive signal. Most ofthe commonly employed markers in diagnostic surgicalpathology have well-defined subcellular localization (Figure2). For example, with rare exceptions, nuclear transcription
Figure 2. Importance of identification of proper subcellular compartment immunostained in identifying ‘‘pseudospecific’’ false-positive signal. A,Appropriate predominantly membranous signal in infiltrating breast cancer with antibodies to the transmembrane receptor HER2. B, Appropriategranular cytoplasmic signal in melanoma with antibody HMB-45, identifying the premelanosomal marker gp100. C, Appropriate nuclear signal inlung carcinoma with antibodies to the nuclear transcription factor TTF-1. D, Inappropriate membranous signal noted with antibodies tosynaptophysin in lung adenocarcinoma. This antibody should produce a granular cytoplasmic signal, and this ‘‘pseudospecific’’ pattern clearlyrepresents false-positive immunostaining (original magnification3200).
896 Arch Pathol Lab Med—Vol 140, September 2016 Diagnostic Immunohistochemistry—Gown

factors, such as TTF-1, PAX-8, and CDX-2, are foundexclusively in the nucleus. Markers such as chromogranin Aand gp100 (the target of antibody HMB-45) localize togranular structures within the cell and tumor cytoplasm, indense core granules (chromogranin A) and premelano-somes (gp100), respectively. ‘‘Pseudospecific’’ signals cangenerally be identified by the inappropriate subcellularlocalization of the signal. For example, a nuclear signal withantibodies to synaptophysin should easily be recognized asa false-positive signal (Figure 2, B). However, there are rareexamples of ‘‘pseudospecific’’ false-positive signals occur-ring in the same cell compartment, as was shown severalyears ago using the SP2 anti–progesterone receptormonoclonal antibody, which also yielded a false-positivenuclear signal in progesterone receptor–negative cells.14
FALSE-NEGATIVE SIGNALS
The most common causes of false-negative immuno-staining are poor tissue fixation, antibodies too dilute or notproperly optimized, and epitope retrieval method notoptimized for individual antibodies. As shown in a recent
study from the cIQc, many laboratories have seriousproblems with false-negative immunostaining due toinappropriate calibration and optimization of pan-keratinand anti–low-molecular weight keratin antibodies.15
As was shown by Shi et al3 several decades ago, no singleepitope retrieval solution is optimal for all antigens orantibodies, and it behooves the individual laboratory to usea ‘‘test battery’’ of epitope retrieval buffers and pHs in orderto avoid suboptimal protocols for individual primaryantibodies.3 The importance of using optimal protocols isdemonstrated in Figure 3.
CONCLUSIONS
The diagnostic pathologist using IHC ignores thesepotential problems at his or her peril. Lack of awarenessof these and other pitfalls in diagnostic IHC may lead topotentially serious errors in diagnosis, affecting patientmanagement.
References
1. Clarke AC. Profiles of the Future. New York, NY: Henry Holt and Company;1984.
Figure 3. Effect of suboptimal epitope retrieval on producing dramatically reduced immunostaining. A and B, Mantle cell lymphomaimmunostained with antibodies to cyclin D1. A, Suboptimal epitope retrieval using 20 minutes of citrate buffer, pH 6. B, Optimal epitope retrievalusing 30 minutes of Tris buffer, pH 10. C and D, Small cell lung cancer immunostained with antibodies to TTF-1. C, Suboptimal epitope retrieval using30 minutes of Tris buffer, pH 10. D, Optimal epitope retrieval using 8 minutes of citrate buffer, pH 6. Note how different antibodies require differentoptimal epitope retrieval conditions (original magnifications3100 [A and B] and3200 [C and D]).
Arch Pathol Lab Med—Vol 140, September 2016 Diagnostic Immunohistochemistry—Gown 897

2. Coons AH, Creech HJ, Jones RN. Immunological properties of an antibodycontaining a fluorescent group. Proc Soc Exp Biol. 1941;47:200–202.
3. Shi SR, Cote RJ, Yang C, et al. Development of an optimal protocol forantigen retrieval: a ‘‘test battery’’ approach exemplified with reference to thestaining of retinoblastoma protein (pRB) in formalin-fixed paraffin sections. JPathol. 1996;179(3):347–352.
4. Borrisholt M, Nielsen S, Vyberg M. Demonstration of CDX2 is highlyantibody dependant. Appl Immunohistochem Mol Morphol. 2013;21(1):64–72.
5. Matoso A, Singh K, Jacob R, et al. Comparison of thyroid transcriptionfactor-1 expression by 2 monoclonal antibodies in pulmonary and nonpulmonaryprimary tumors. Appl Immunohistochem Mol Morphol. 2010;18(2):142–149.
6. Ordonez NG. Value of PAX 8 immunostaining in tumor diagnosis: a reviewand update. Adv Anat Pathol. 2012;19(3):140–151.
7. Ozcan A, Shen SS, Hamilton C, et al. PAX 8 expression in non-neoplastictissues, primary tumors, and metastatic tumors: a comprehensive immunohisto-chemical study. Mod Pathol. 2011;24(6):751–764.
8. Laury AR, Perets R, Piao H, et al. A comprehensive analysis of PAX8expression in human epithelial tumors. Am J Surg Pathol. 2011;35(6):816–826.
9. Tacha D, Zhou D, Cheng L. Expression of PAX8 in normal and neoplastictissues: a comprehensive immunohistochemical study. Appl ImmunohistochemMol Morphol. 2011;19(4):293–299.10. Toriyama A, Mori T, Sekine S, Yoshida A, Hino O, Tsuta K. Utility of PAX8
mouse monoclonal antibody in the diagnosis of thyroid, thymic, pleural and lung
tumours: a comparison with polyclonal PAX8 antibody. Histopathology. 2014;65(4):465–472.11. Tacha D, Qi W, Zhou D, Bremer R, Cheng L. PAX8 mouse monoclonal
antibody [BC12] recognizes a restricted epitope and is highly sensitive in renalcell and ovarian cancers but does not cross-react with b cells and tumors ofpancreatic origin. Appl Immunohistochem Mol Morphol. 2013;21(1):59–63.12. Moretti L, Medeiros LJ, Kunkalla K, Williams MD, Singh RR, Vega F. N-
terminal PAX8 polyclonal antibody shows cross-reactivity with N-terminal regionof PAX5 and is responsible for reports of PAX8 positivity in malignantlymphomas. Mod Pathol. 2012;25(2):231–236.13. Pradidarcheep W, Labruyere WT, Dabhoiwala NF, Lamers WH. Lack of
specificity of commercially available antisera: better specifications needed. JHistochem Cytochem. 2008;56(12):1099–1111.14. Ibrahim M, Dodson A, Barnett S, Fish D, Jasani B, Miller K. Potential for
false-positive staining with a rabbit monoclonal antibody to progesteronereceptor (SP2): findings of the UK National External Quality Assessment Schemefor Immunocytochemistry and FISH highlight the need for correct validation ofantibodies on introduction to the laboratory. Am J Clin Pathol. 2008;129(3):398–409.15. Copete M, Garratt J, Gilks B, et al. Inappropriate calibration and
optimisation of pan-keratin (pan-CK) and low molecular weight keratin (LMWCK)immunohistochemistry tests: Canadian Immunohistochemistry Quality Control(CIQC) experience. J Clin Pathol. 2011;64(3):220–225.
898 Arch Pathol Lab Med—Vol 140, September 2016 Diagnostic Immunohistochemistry—Gown
Copyright of Archives of Pathology & Laboratory Medicine is the property of College ofAmerican Pathologists and its content may not be copied or emailed to multiple sites orposted to a listserv without the copyright holder's express written permission. However, usersmay print, download, or email articles for individual use.