Embed Size (px)
Citation preview
Diagnosis of Urinary Tract Obstruction: Techniques and Limitations
Isabel Roca, MDHU VALL HEBRONBarcelona, Spain
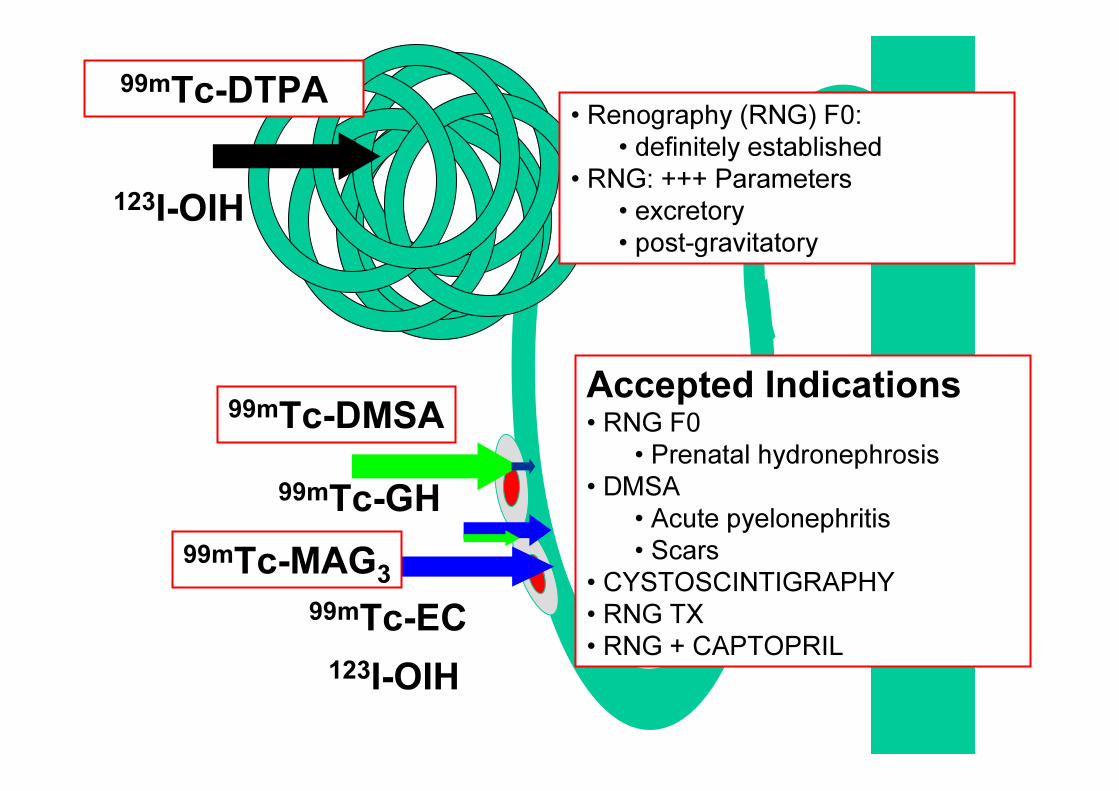
123I-OIH99mTc-EC
99mTc-MAG3
123I-OIH
99mTc-DMSA99mTc-GH
99mTc-DTPA • Renography (RNG) F0:• definitely established
• RNG: +++ Parameters • excretory • post-gravitatory
Accepted Indications• RNG F0
• Prenatal hydronephrosis• DMSA
• Acute pyelonephritis• Scars
• CYSTOSCINTIGRAPHY• RNG TX• RNG + CAPTOPRIL
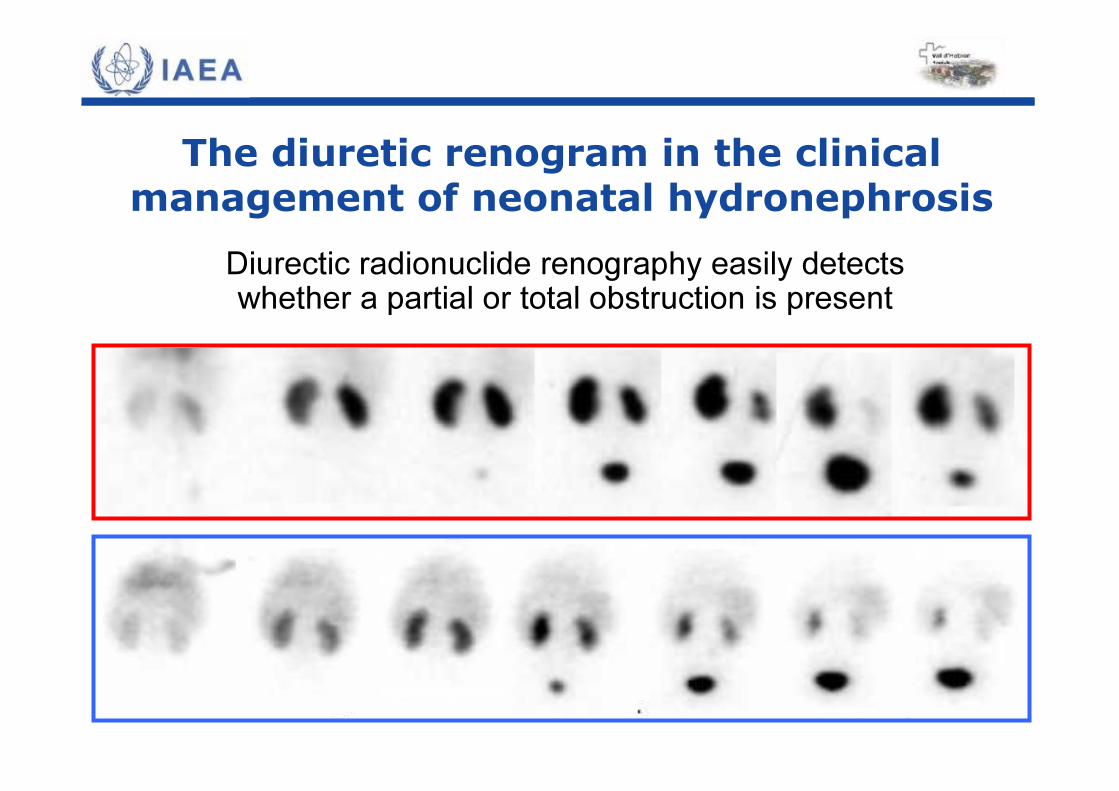
Diurectic radionuclide renography easily detects whether a partial or total obstruction is present
The diuretic renogram in the clinical management of neonatal hydronephrosis
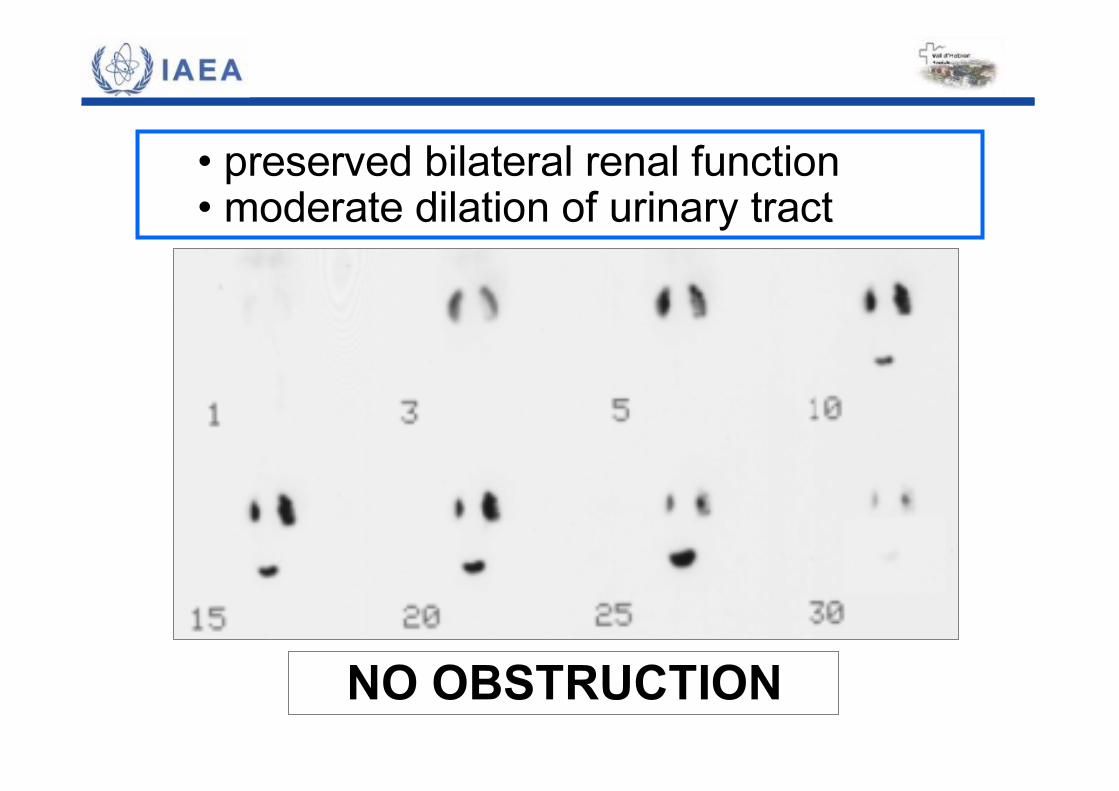
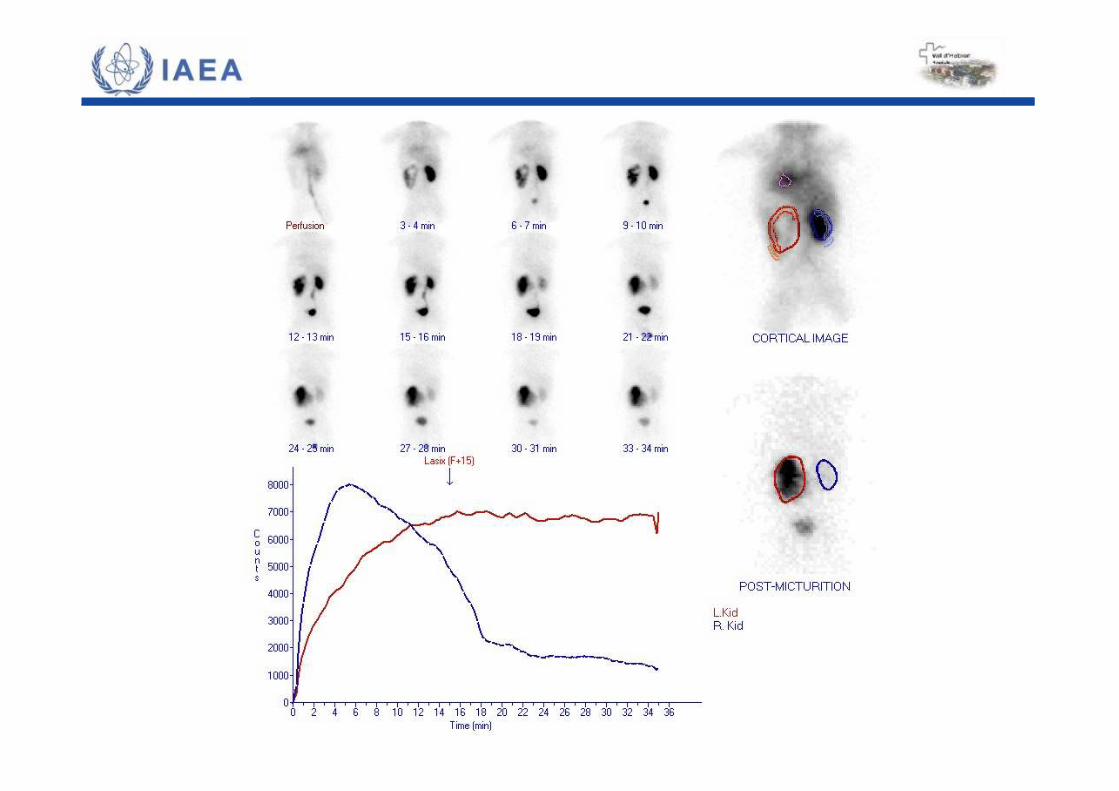
NO OBSTRUCTION
• preserved bilateral renal function• moderate dilation of urinary tract
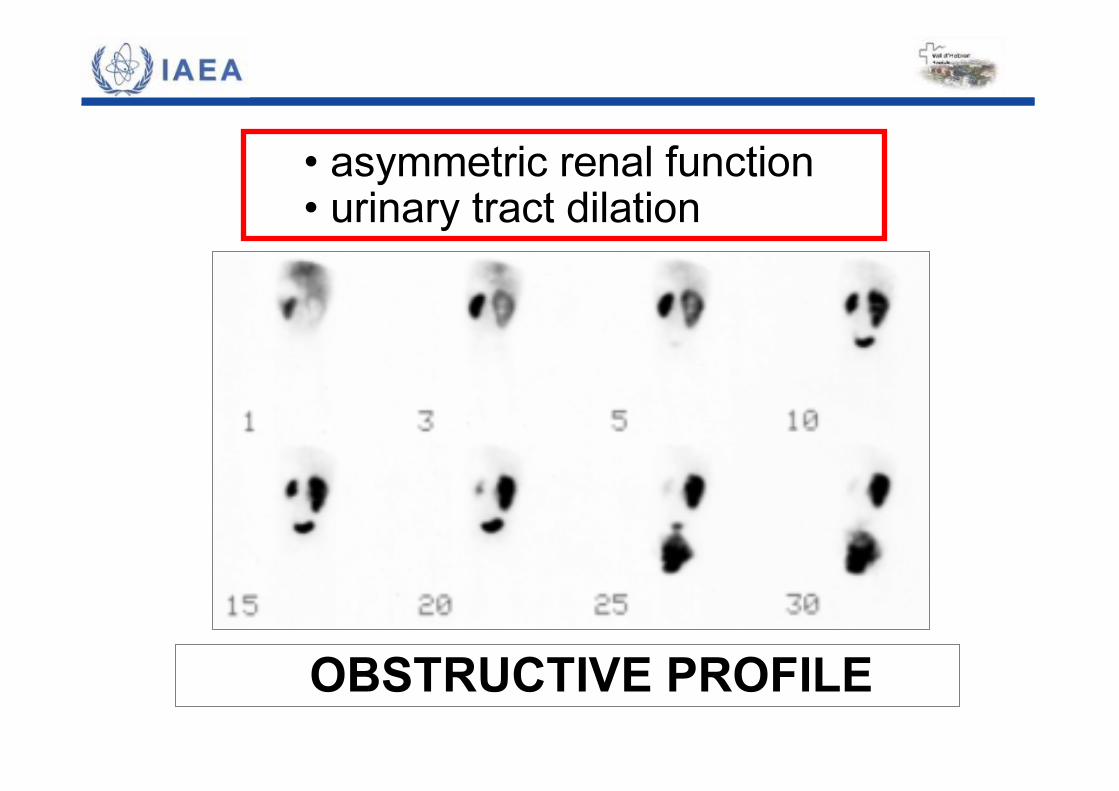
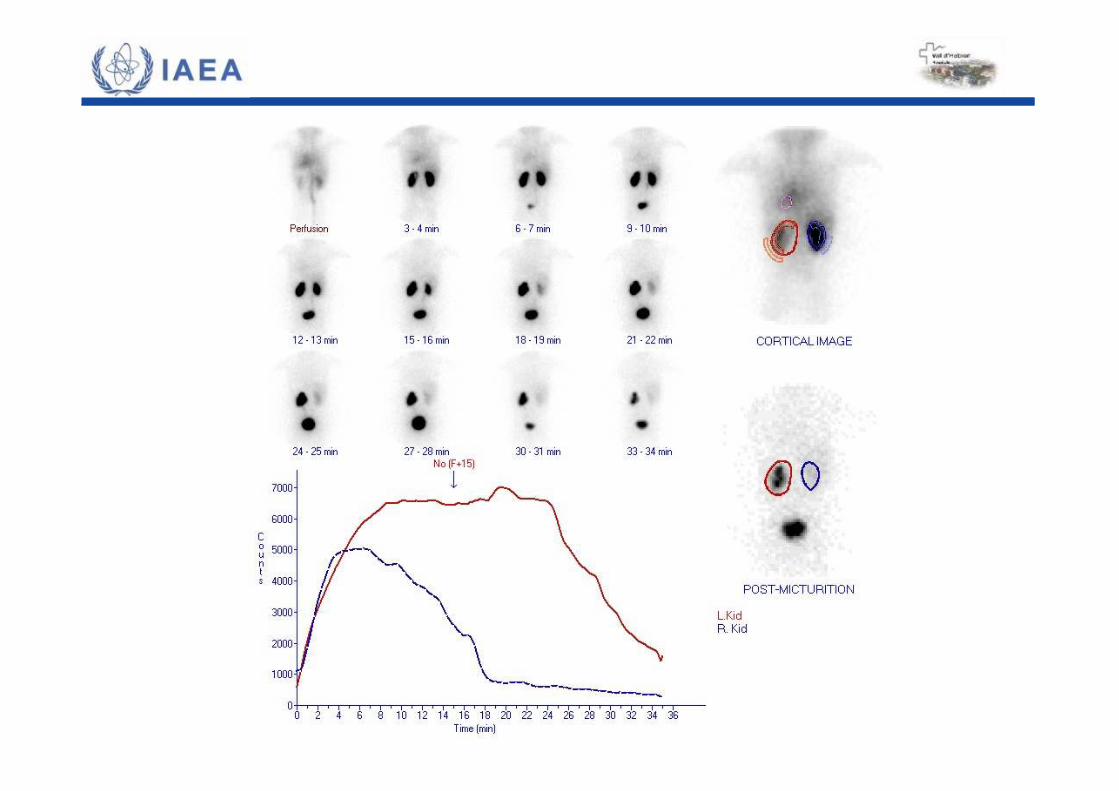
• asymmetric renal function• urinary tract dilation
OBSTRUCTIVE PROFILE
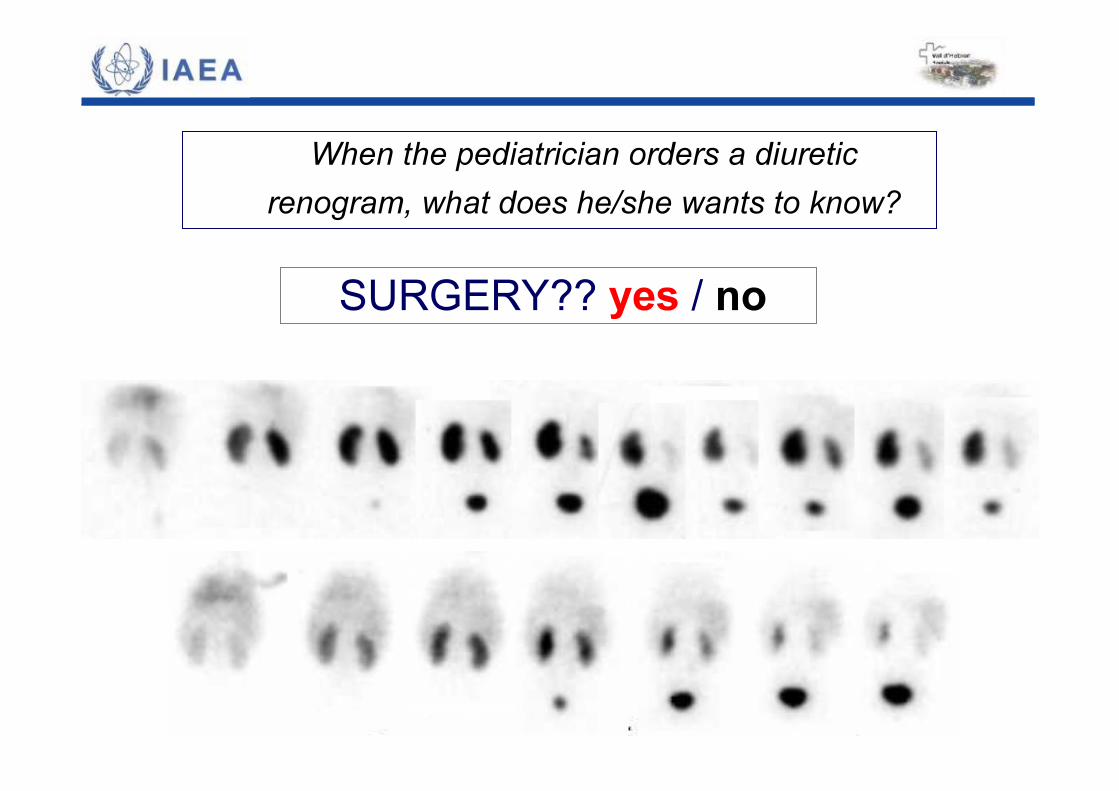
When the pediatrician orders a diuretic renogram, what does he/she wants to know?
SURGERY?? yes / no

Can we answer the question? NOCan we help decide? YES
HOW?
When the pediatrician orders a diuretic renogram, what does he/she wants to know?
SURGERY yes or no??
Providing information about:- renal function- excretory pattern
HOWCan we help the pediatrician evaluate
a patient with hydronephrosis?
OBSTRUCTIONObstacle to urine drainage which, left without treatment, may affect renal function
(Koff, Peters)
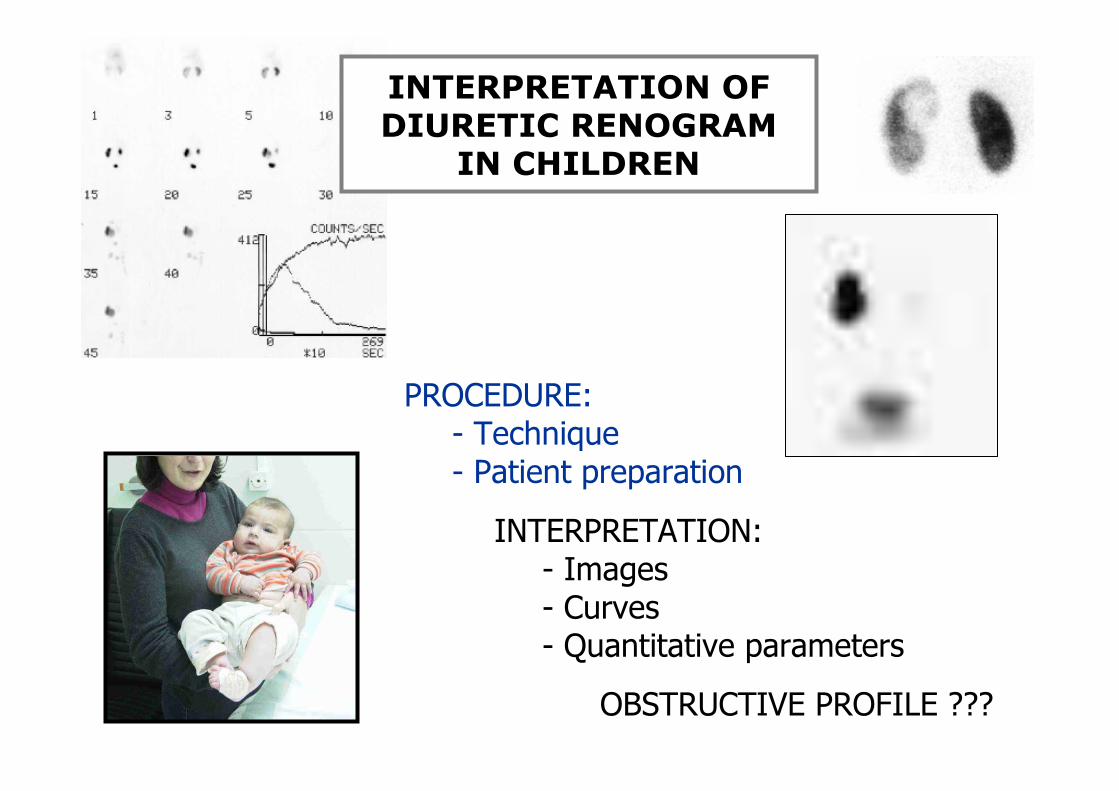
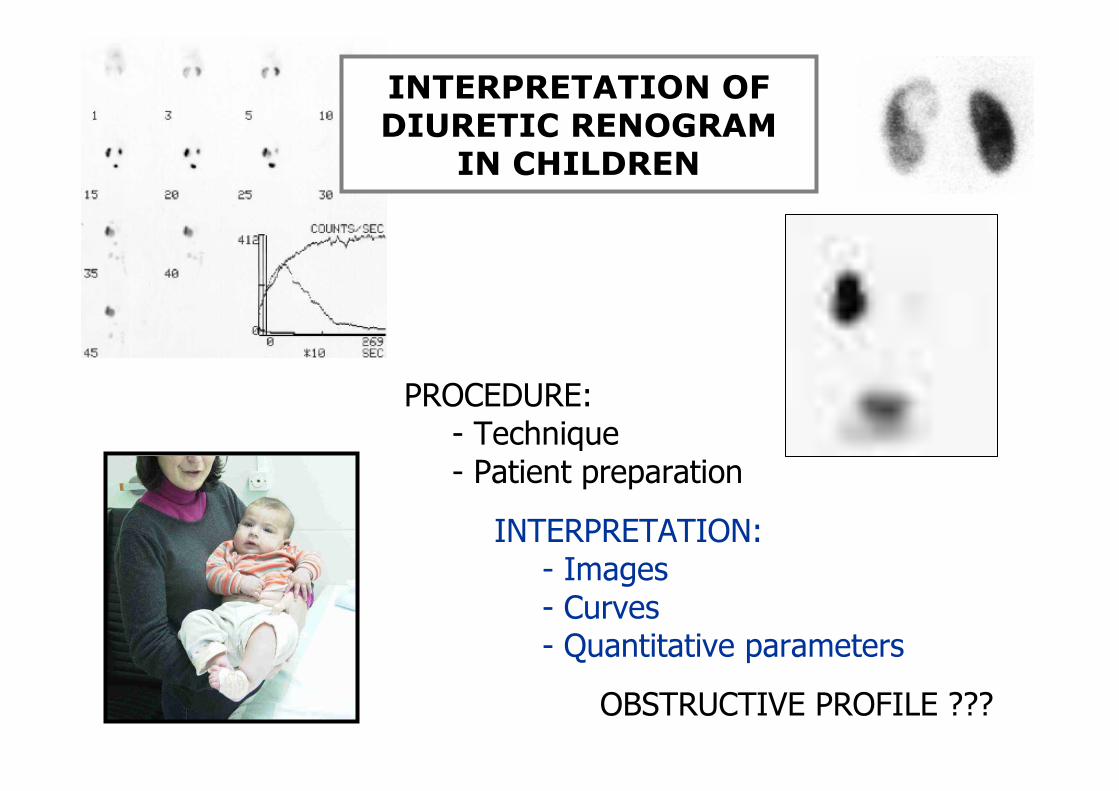
PROCEDURE:- Technique- Patient preparation
INTERPRETATION:- Images- Curves- Quantitative parameters
OBSTRUCTIVE PROFILE ???
INTERPRETATION OF DIURETIC RENOGRAM
IN CHILDREN
There are as many protocols as NM services !A comprehensive, complete software package is lacking
Oral hydrationFor a baby, best possible hydration is lactation
F-15 F0 F+15 F+20 ??Probably all options are valid and clinically useful
"Well tempered renography”
Diuretic renogram
Europe
USA
• difficulties: centers with different protocols, controversies in interpretation
Published GUIDELINES:Gordon I, Colarinha P, Fettich J et al.Guidelines for standard and diuretic renography in children.Eur J Nucl Med 2001; 28 : BP21–BP30O'Reilly P, Aurell M, Britton K, Kletter K, Rosenthal L, Testa T.Consensus on diuresis renography for investigating the dilated upper urinary tract. Radionuclides in Nephrourology Group. Consensus Committee on Diuresis Renography.J Nucl Med 1996; 37 : 1872–6BJU 2003; 91:239–243Conway JJ, Maizels M.The ‘well tempered’ diuretic renogram: a standard method to examine the asymptomatic neonate with hydronephrosis or hydroureteronephrosis. A report from combined meetings of The Society for Fetal Urology and members of The Pediatric Nuclear Medicine Council – The Society of Nuclear Medicine.J Nucl Med 1992; 33 : 2047–51
EANM
SNM
ISCORN
- recommends a physiologic procedure- evaluation of drainage takes into account renal function, and contemplates urinary excretion including gravity and micturation
- recommends a more invasive technique- evaluation of drainage does not account for influence of gravity, renal function, pelvis size.
Gordon I, Colarinha P, Fettich J et al.Guidelines for standard and diuretic renography in children.Eur J Nucl Med 2001; 28 : BP21–BP30
Conway JJ, Maizels M.The ‘well tempered’ diuretic renogram: a standard method to examine the asymptomatic neonate with hydronephrosis or hydroureteronephrosis. A report from combined meetings of The Society for Fetal Urology and members of The Pediatric Nuclear Medicine Council – The Society of Nuclear Medicine.J Nucl Med 1992; 33 : 2047–51
Guidelines for standard and diuretic renography in children
Paediatric Committee of European Association of Nuclear Medicine
Eur J Nucl Med 2001; 28:BP21-BP30
MAG-3 diuresis renography has been shown to be useful even in children
aged 1 month or less and this technique should be available to them
Guidelines for standard and diuretic renography in children
Age of the child
� Routine use of bladder catheter is not indicated.� Most children will void spontaneously, especially as a diuretic has been given.
� Recommend the acquisition of a post-micturition image obtained after gravity assisted drainage.
Guidelines for standard and diuretic renography in children
Bladder catheterization
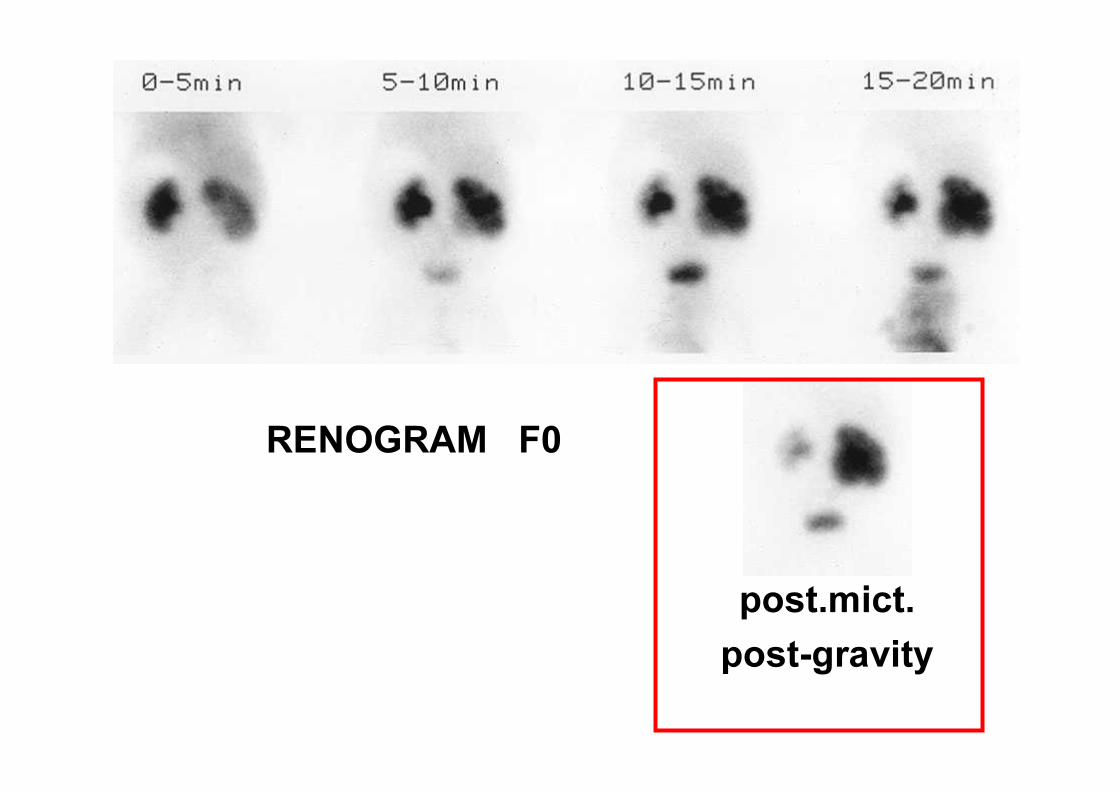
RENOGRAM F0
post.mict.post-gravity
Encourage oral fluid intake for adequate hydration rather than intravenous fluid administration
Guidelines for standard and diuretic renography in children
Hydration of the child
� F+20, F-15, F0: No evidence of any one of these timings being better than the others.
� If venous access is difficult, a single injection is recommended (F0).
Guidelines for standard and diuretic renography in childrenTime of diuretic administration
� Renal function
� Drainage assessment
Guidelines for standard and diuretic renography in children
Parameters used
Preparation
Offer water / orange juice.
No bladder catheterization, only if:
Previous hydrationNeonates: start acquisition just afterroutine lactation.
Pelvic ectopic kidney.Vesico-uretheral reflux present +++
Gravity effect
Previous micturation whenever possible.
Vertical position just before post-micturing image.
IV fluids only if necessary.
DiureticVariable timing.
IMMOBILIZATIONsand bags, Velcro strips
HYDRATION
POST-MICTURING IMAGEGRAVITYDIURETIC
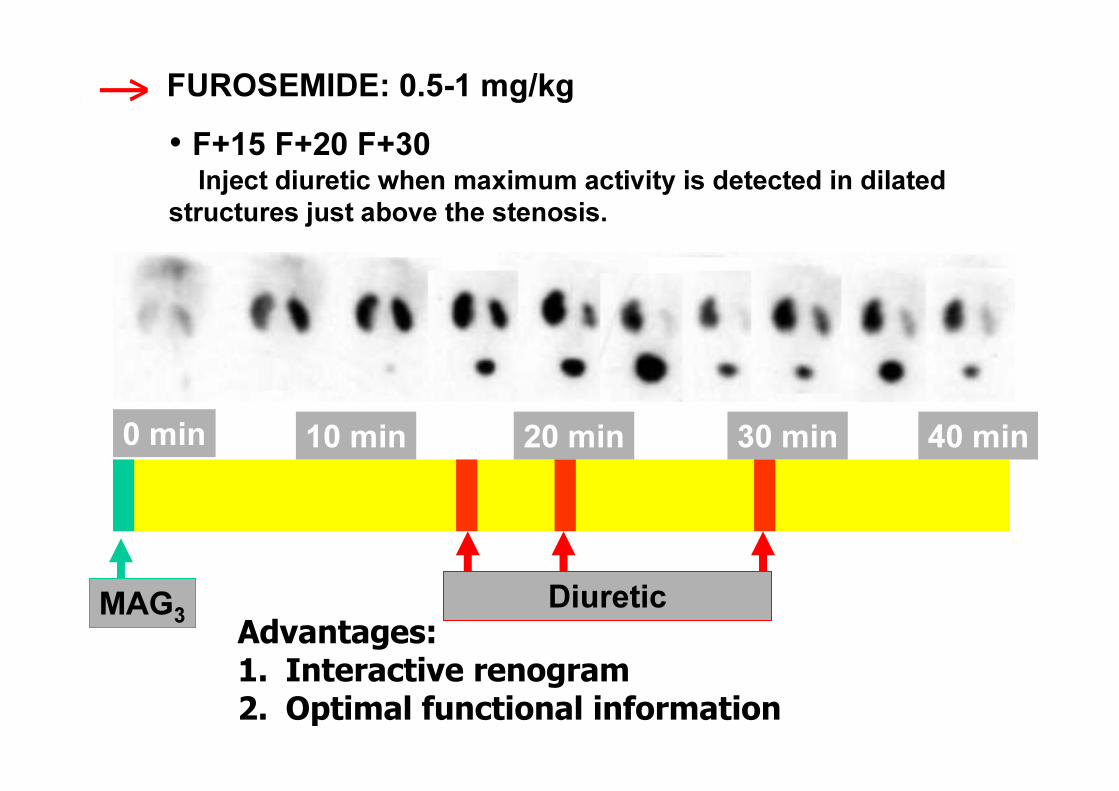
• F+15 F+20 F+30Inject diuretic when maximum activity is detected in dilated
structures just above the stenosis.
0 min 10 min 20 min 30 min 40 min
Advantages:1. Interactive renogram2. Optimal functional information
MAG3 Diuretic
FUROSEMIDE: 0.5-1 mg/kg
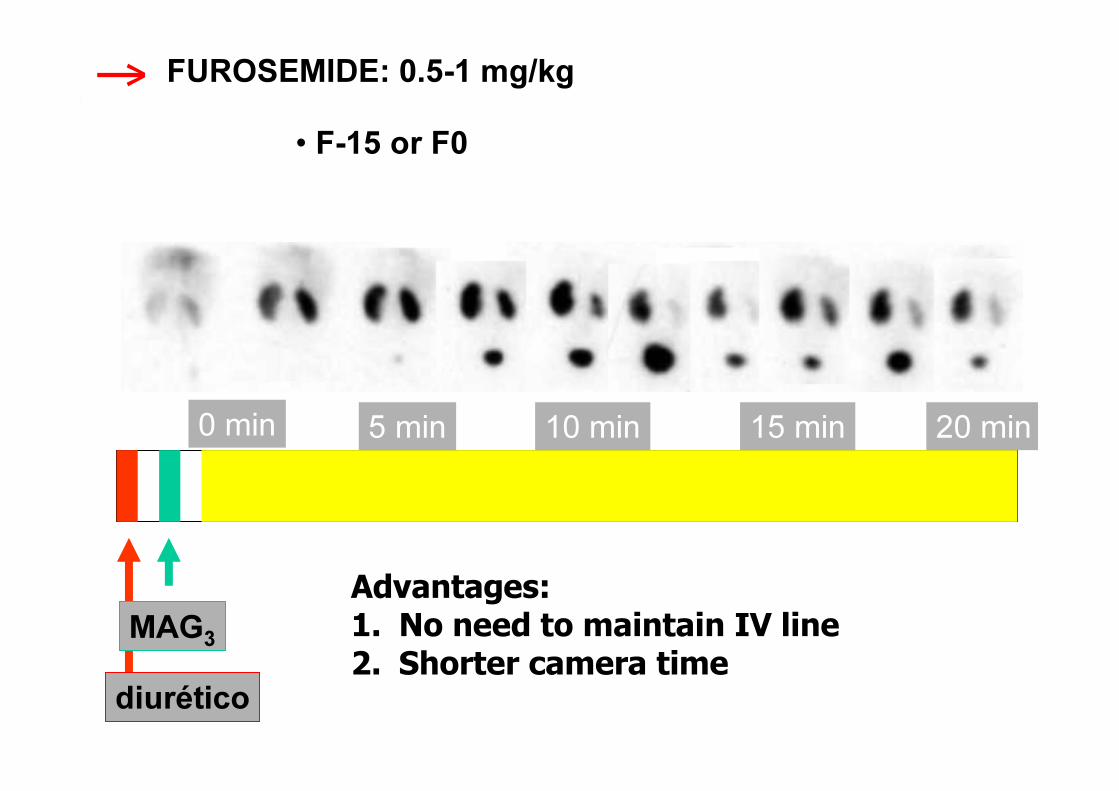
FUROSEMIDE: 0.5-1 mg/kg• F-15 or F0
0 min 5 min 10 min 15 min 20 min
MAG3
diurético
Advantages:1. No need to maintain IV line2. Shorter camera time
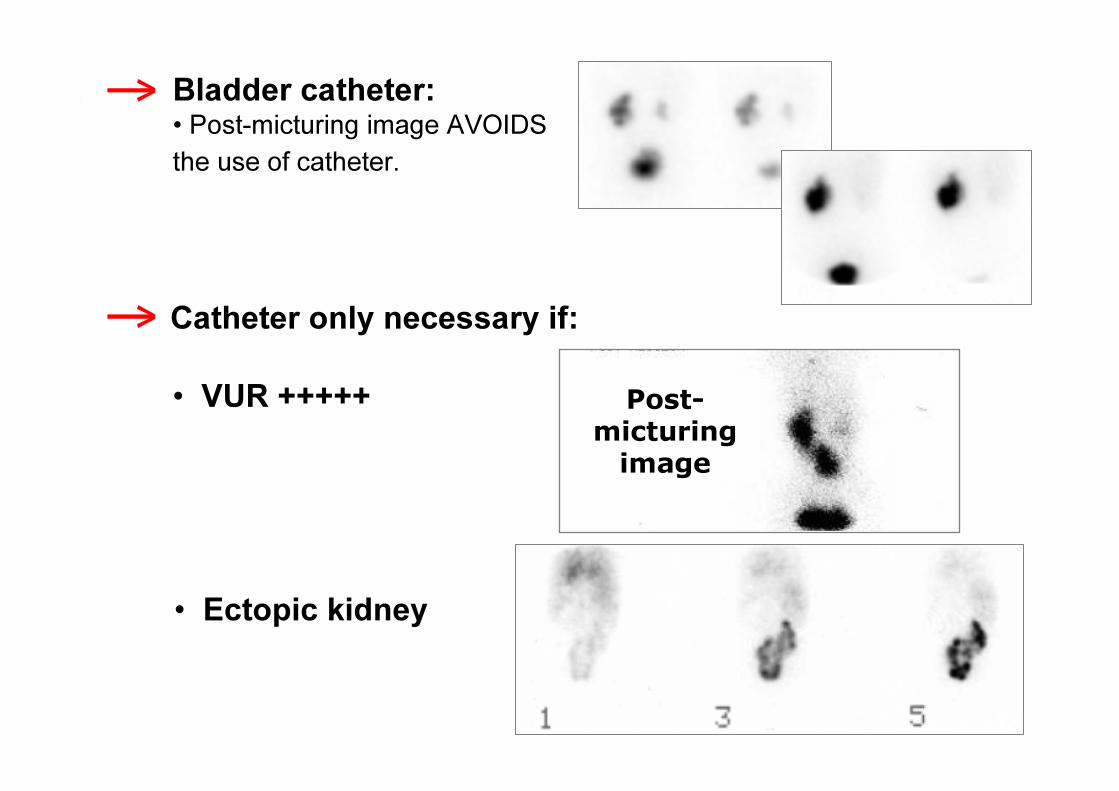
Catheter only necessary if:
• VUR +++++
• Ectopic kidney
Post-micturing image
Bladder catheter: • Post-micturing image AVOIDS the use of catheter.
INTERPRETATION OF DIURETIC RENOGRAM
IN CHILDREN
PROCEDURE:- Technique- Patient preparation
INTERPRETATION:- Images- Curves- Quantitative parameters
OBSTRUCTIVE PROFILE ???
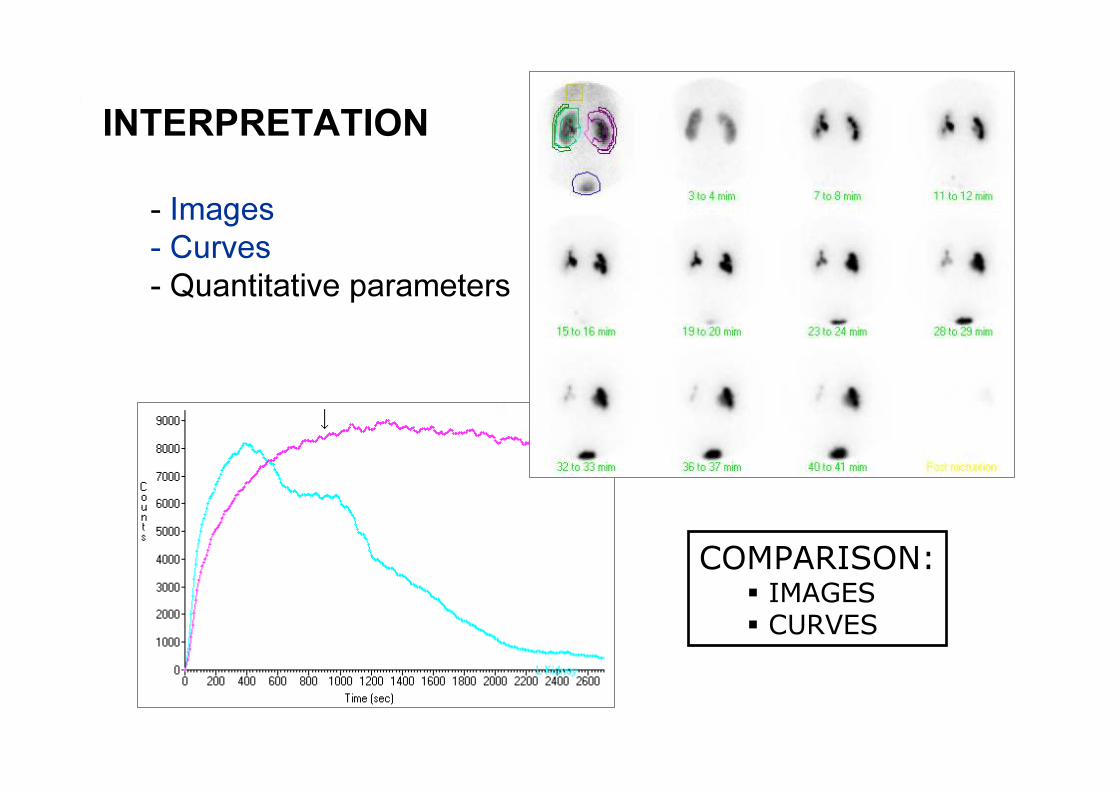
COMPARISON:� IMAGES� CURVES
INTERPRETATION- Images- Curves- Quantitative parameters
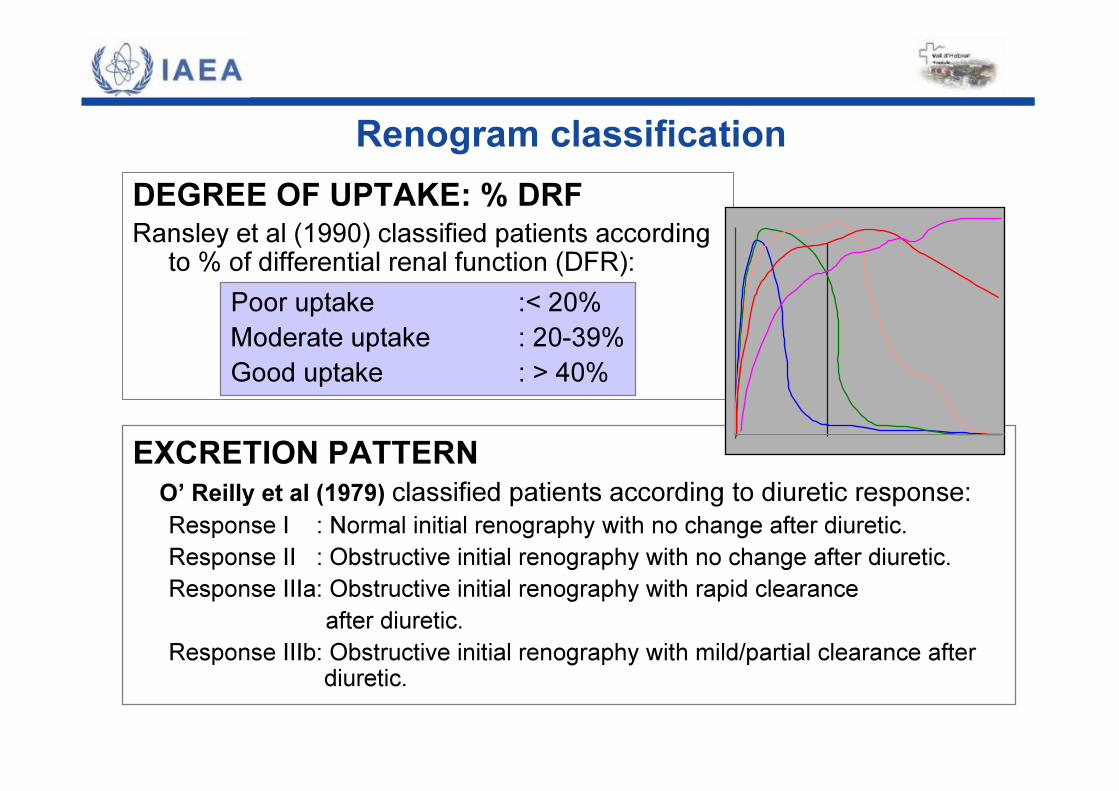
Renogram classificationDEGREE OF UPTAKE: % DRF Ransley et al (1990) classified patients according
to % of differential renal function (DFR):
EXCRETION PATTERNO’ Reilly et al (1979) classified patients according to diuretic response: Response I : Normal initial renography with no change after diuretic. Response II : Obstructive initial renography with no change after diuretic. Response IIIa: Obstructive initial renography with rapid clearance
after diuretic. Response IIIb: Obstructive initial renography with mild/partial clearance after
diuretic.
Poor uptake :< 20% Moderate uptake : 20-39%Good uptake : > 40%
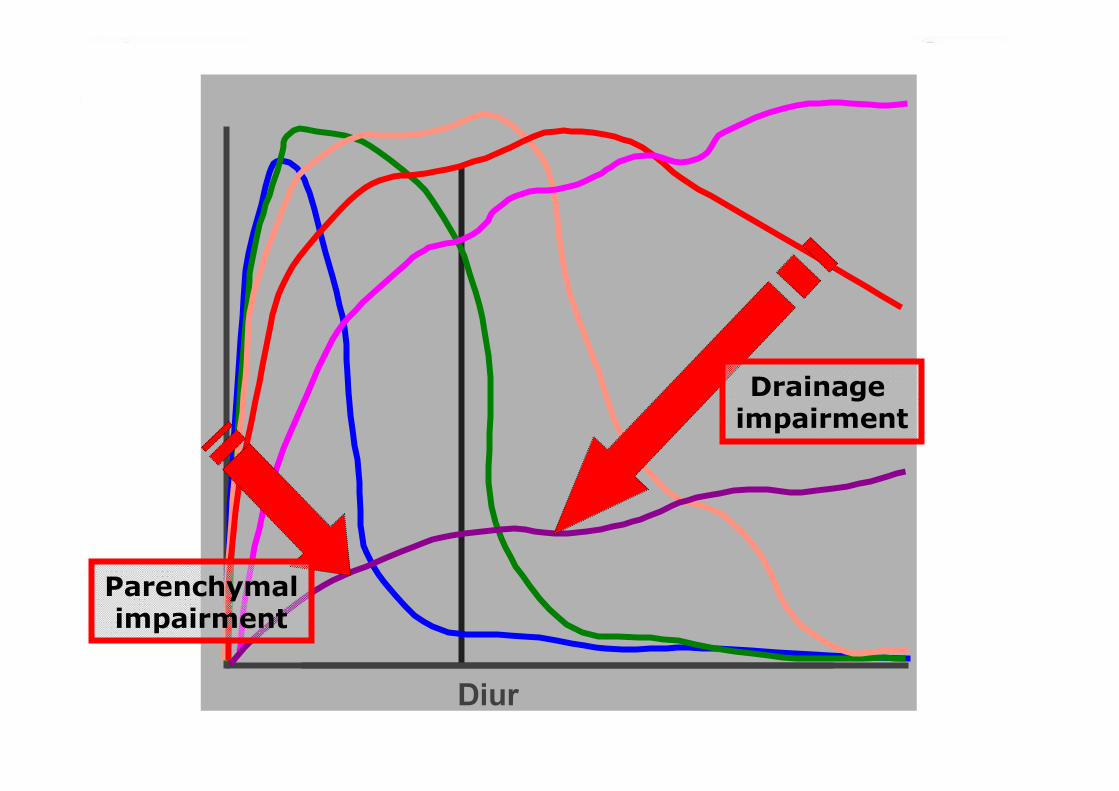
Diur
Parenchymalimpairment
Drainage impairment
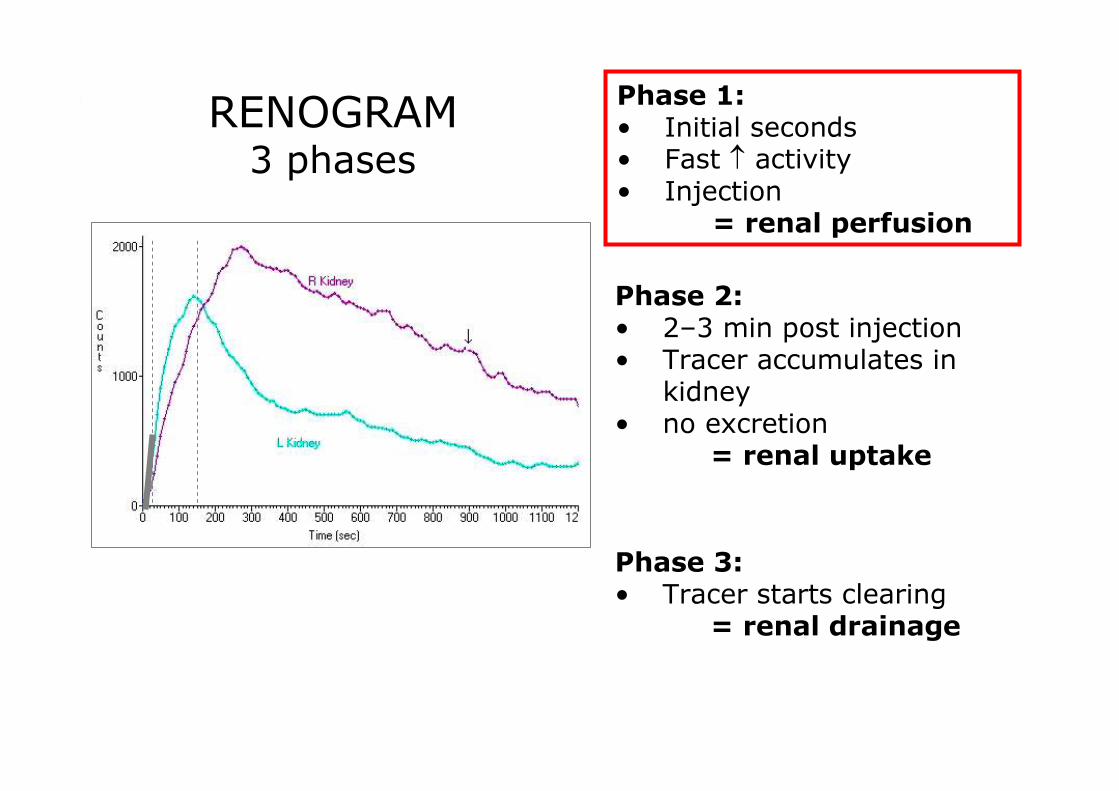
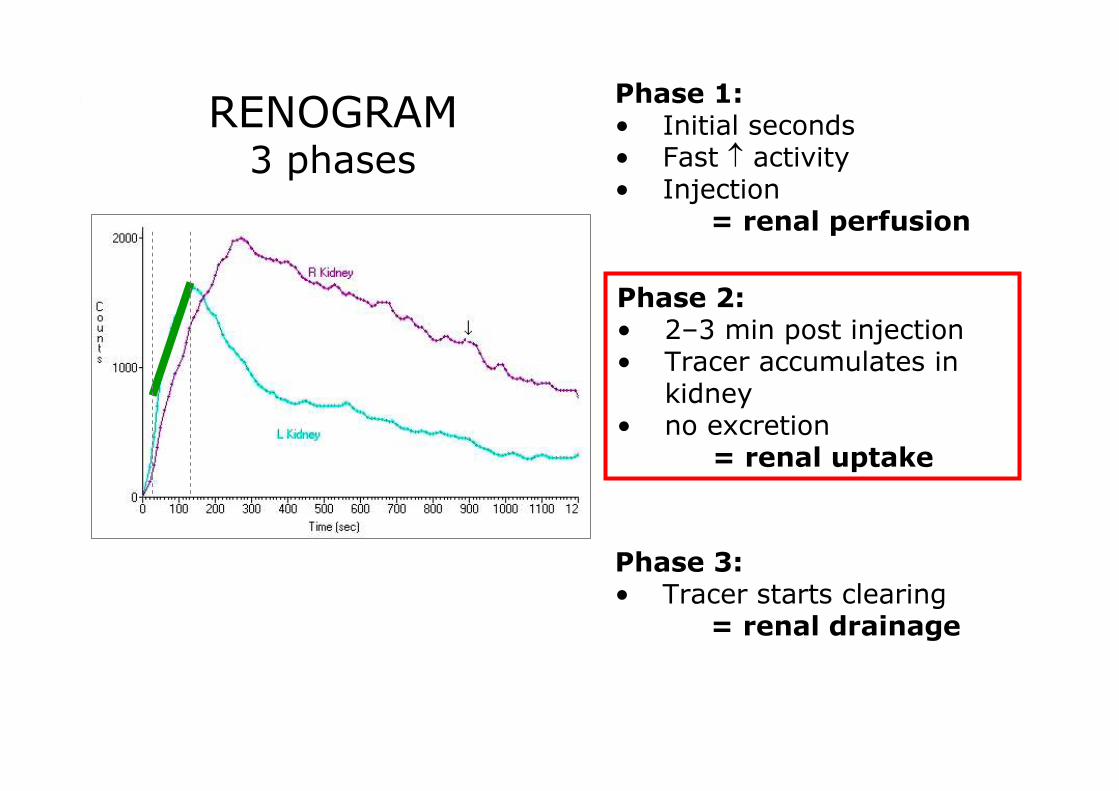
RENOGRAM3 phases
Phase 1:• Initial seconds• Fast ↑ activity• Injection
= renal perfusion
Phase 2:• 2–3 min post injection• Tracer accumulates in
kidney• no excretion
= renal uptake
Phase 3:• Tracer starts clearing
= renal drainage
Phase 1:• Initial seconds• Fast ↑ activity• Injection
= renal perfusion
Phase 2:• 2–3 min post injection• Tracer accumulates in
kidney• no excretion
= renal uptake
Phase 3:• Tracer starts clearing
= renal drainage
RENOGRAM3 phases
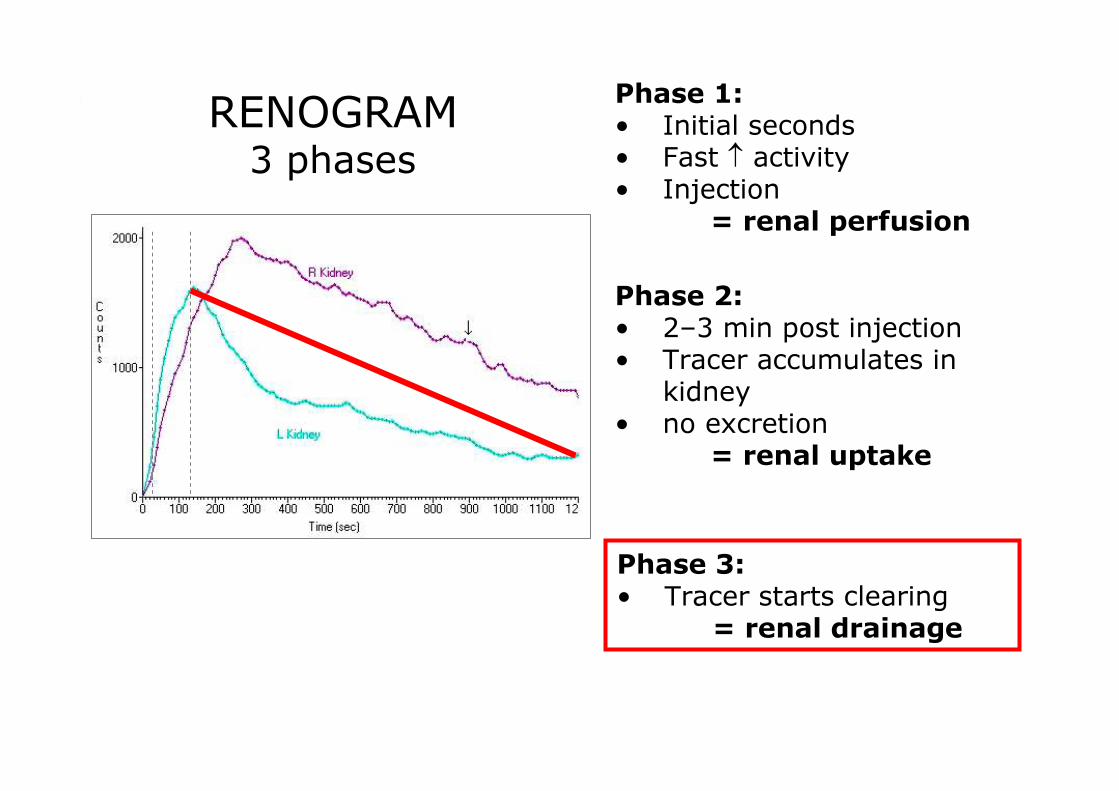
Phase 1:• Initial seconds• Fast ↑ activity• Injection
= renal perfusion
Phase 2:• 2–3 min post injection• Tracer accumulates in
kidney• no excretion
= renal uptake
Phase 3:• Tracer starts clearing
= renal drainage
RENOGRAM3 phases
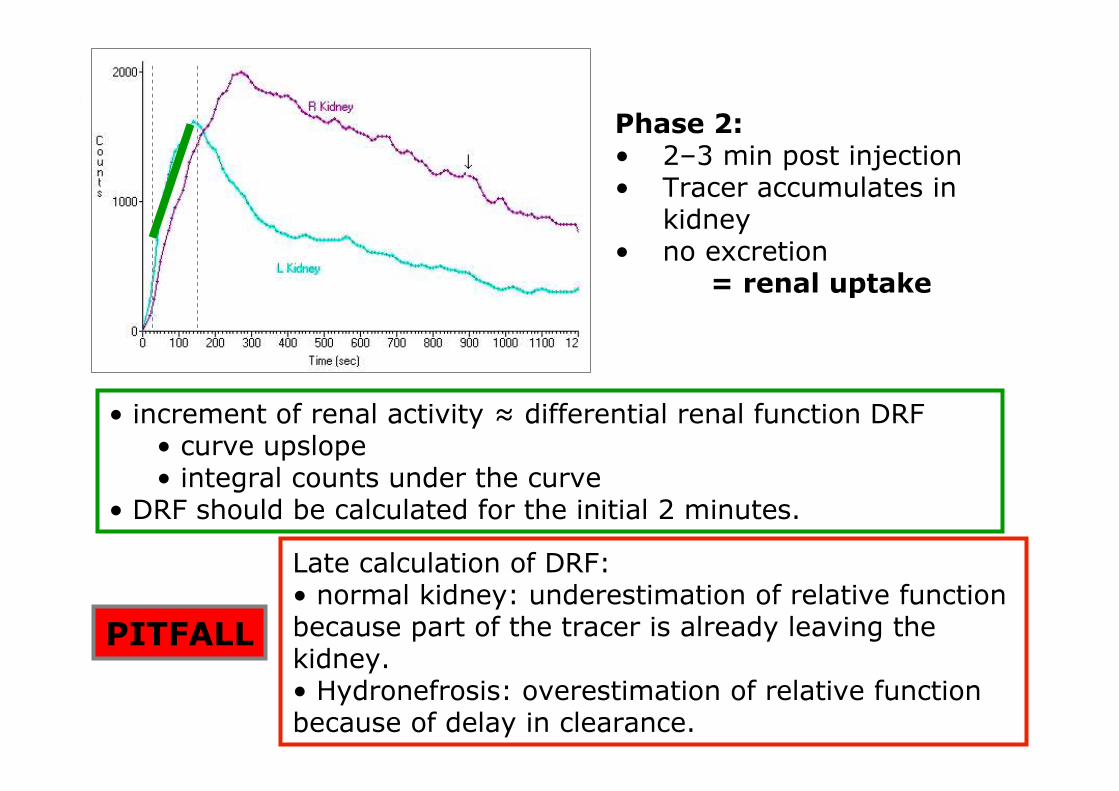
• increment of renal activity ≈ differential renal function DRF• curve upslope• integral counts under the curve
• DRF should be calculated for the initial 2 minutes.Late calculation of DRF:• normal kidney: underestimation of relative function because part of the tracer is already leaving the kidney.• Hydronefrosis: overestimation of relative function because of delay in clearance.
PITFALL
Phase 2:• 2–3 min post injection• Tracer accumulates in
kidney• no excretion
= renal uptake
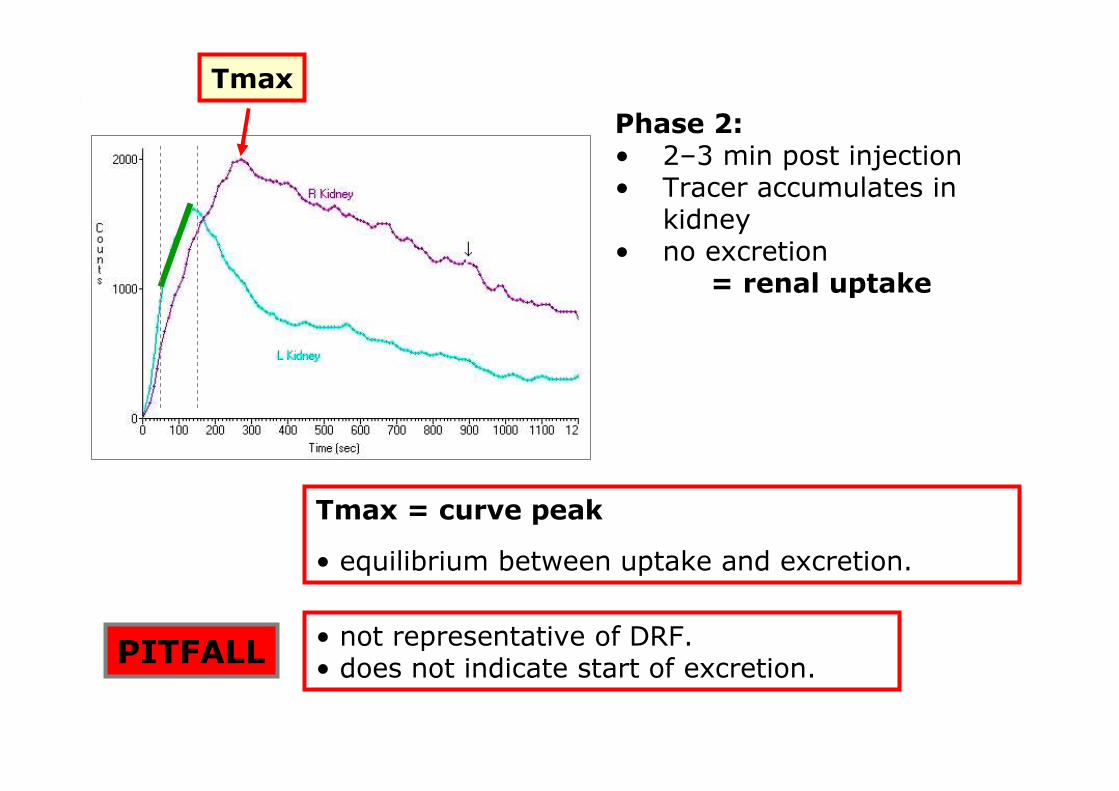
• not representative of DRF.• does not indicate start of excretion.
Tmax
PITFALL
Tmax = curve peak • equilibrium between uptake and excretion.
Phase 2:• 2–3 min post injection• Tracer accumulates in
kidney• no excretion
= renal uptake
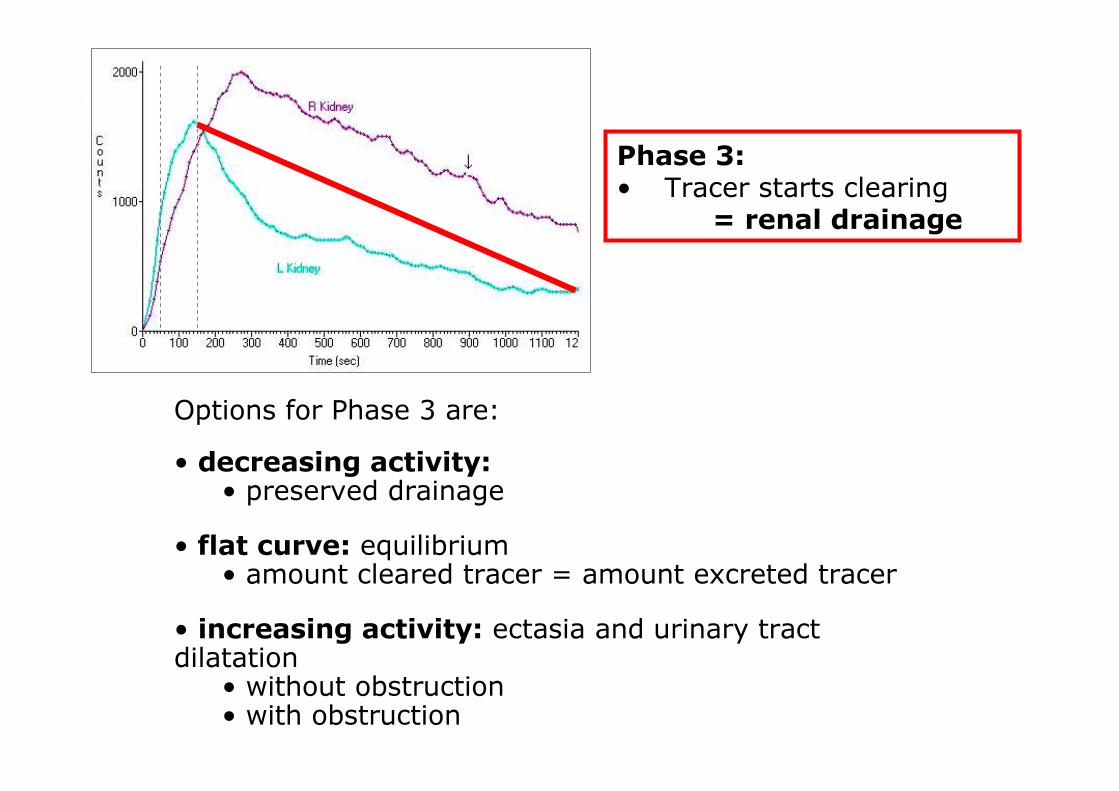
Options for Phase 3 are: • decreasing activity:
• preserved drainage• flat curve: equilibrium
• amount cleared tracer = amount excreted tracer• increasing activity: ectasia and urinary tract dilatation
• without obstruction• with obstruction
Phase 3:• Tracer starts clearing
= renal drainage
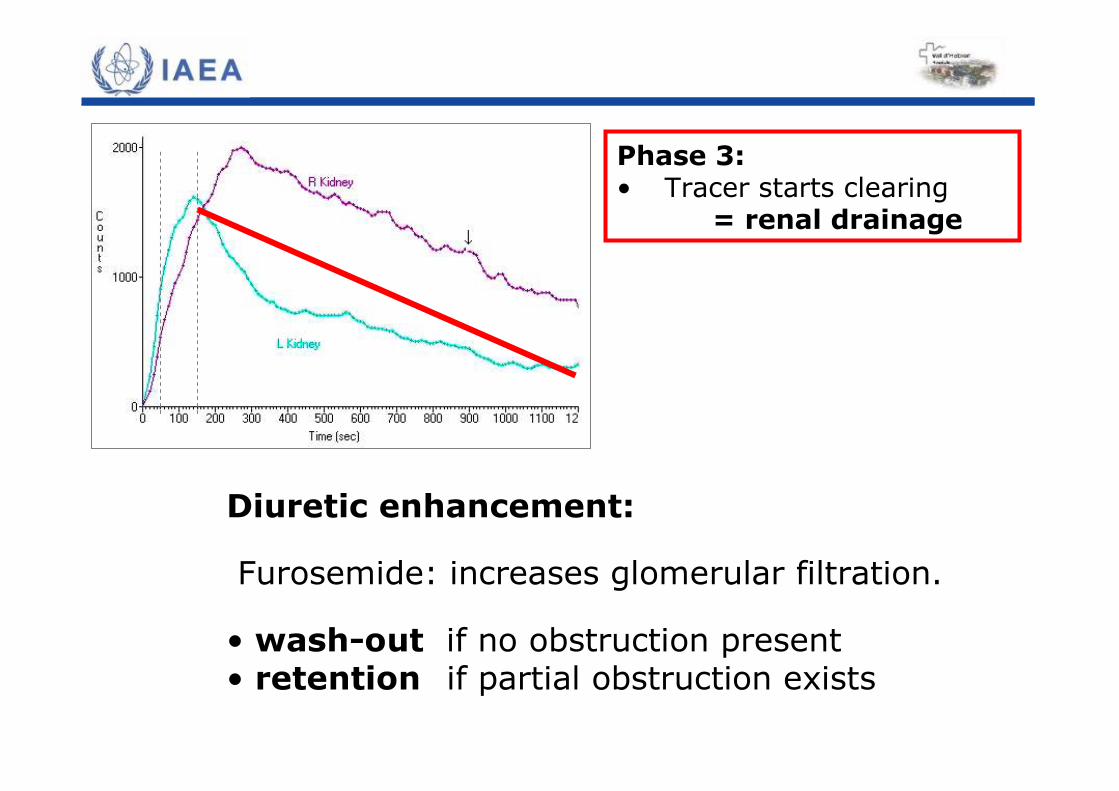
Diuretic enhancement:Furosemide: increases glomerular filtration.• wash-out if no obstruction present• retention if partial obstruction exists
Phase 3:• Tracer starts clearing
= renal drainage
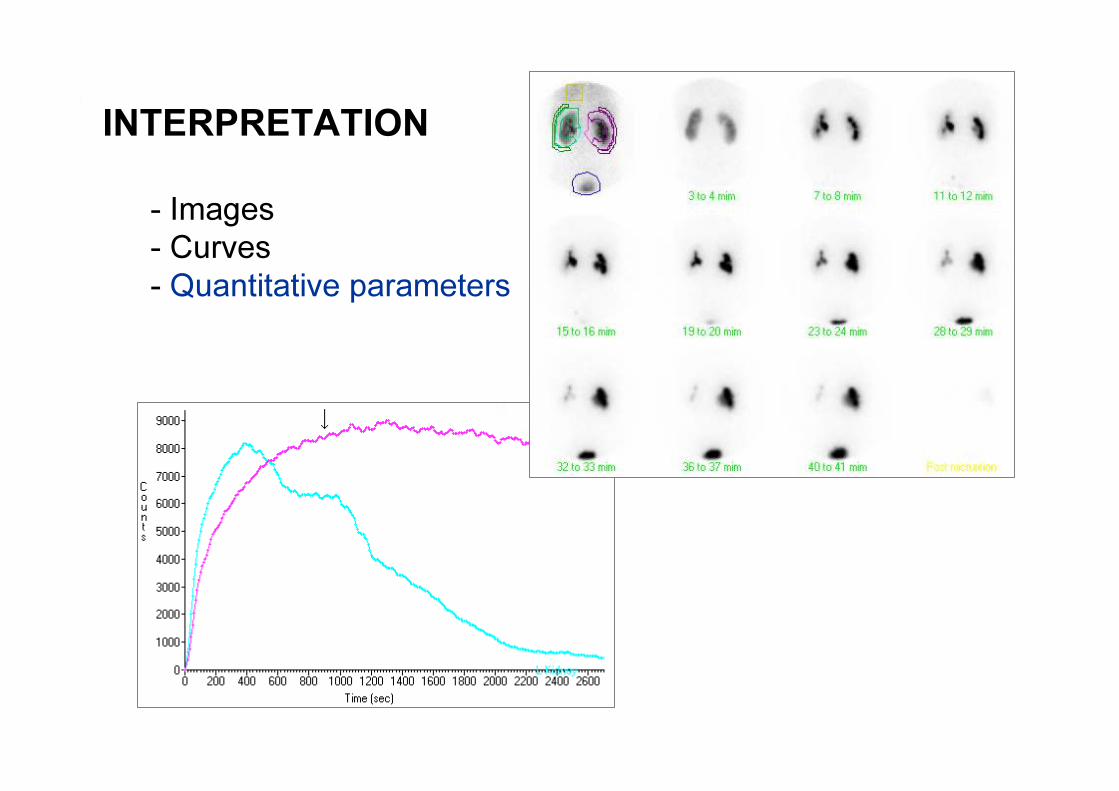
INTERPRETATION- Images- Curves- Quantitative parameters
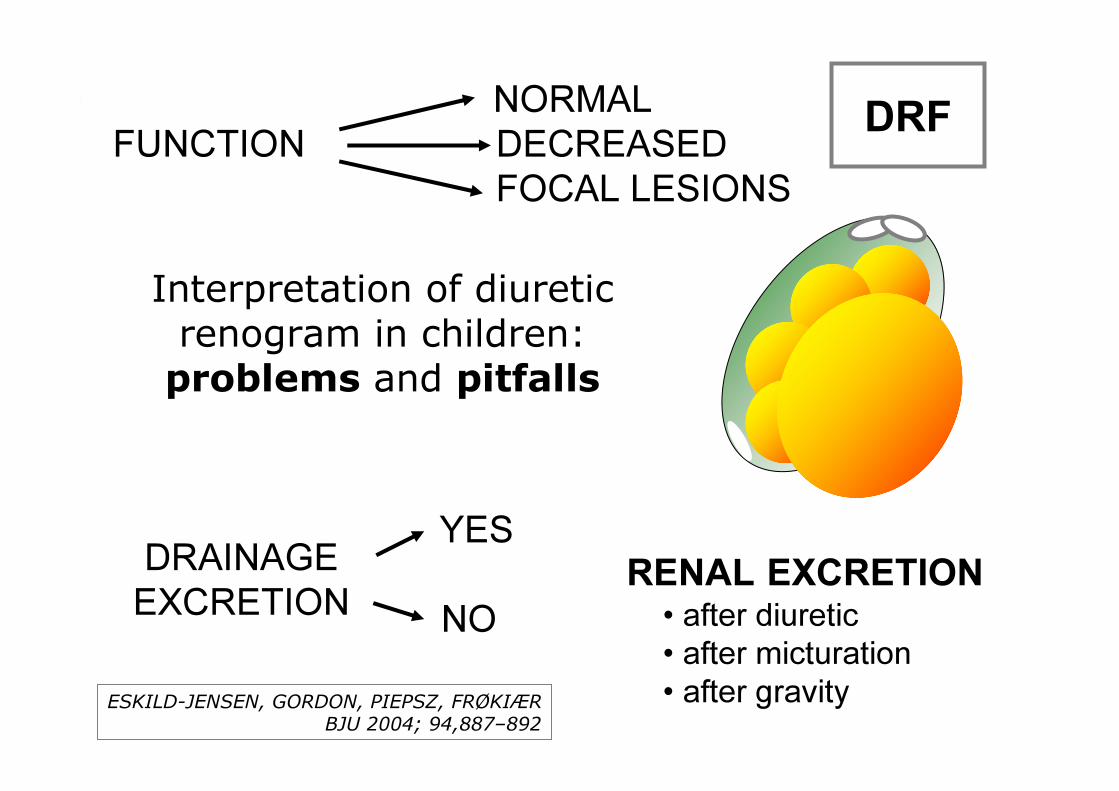
YES
NO
NORMALFUNCTION DECREASED
FOCAL LESIONSDRF
RENAL EXCRETION• after diuretic• after micturation• after gravity
DRAINAGEEXCRETION
Interpretation of diuretic renogram in children:problems and pitfalls
ESKILD-JENSEN, GORDON, PIEPSZ, FRØKIÆRBJU 2004; 94,887–892
DRF is independent of• degree of hydronephrosis• hydration status• bladder emptiness• gravity• diuretic administration
DRF – Differential Renal Function
1. LOW signal / background (BKG)• Renal insufficiency.• DTPA instead of MAG3 in young children.
2. Inappropriate BKG ROI• DFR influenced by extra-renal interstitial
activity included in BKG ROI.• Consensus regarding BKG subtraction ROI:
peri-renal area.• Problem: severe dilatation and very young
patients (renal contour similar to body contour). In this case, draw BKG ROI below kidney.
3. Technical errors• Injection problems.• Poor labelling (MAG3: liver, stomach).• Patient motion.• Wrong timing initiation of acquisition.
PITFALLSWRONG
ESTIMATIONOF RENAL FUNCTION
DFR
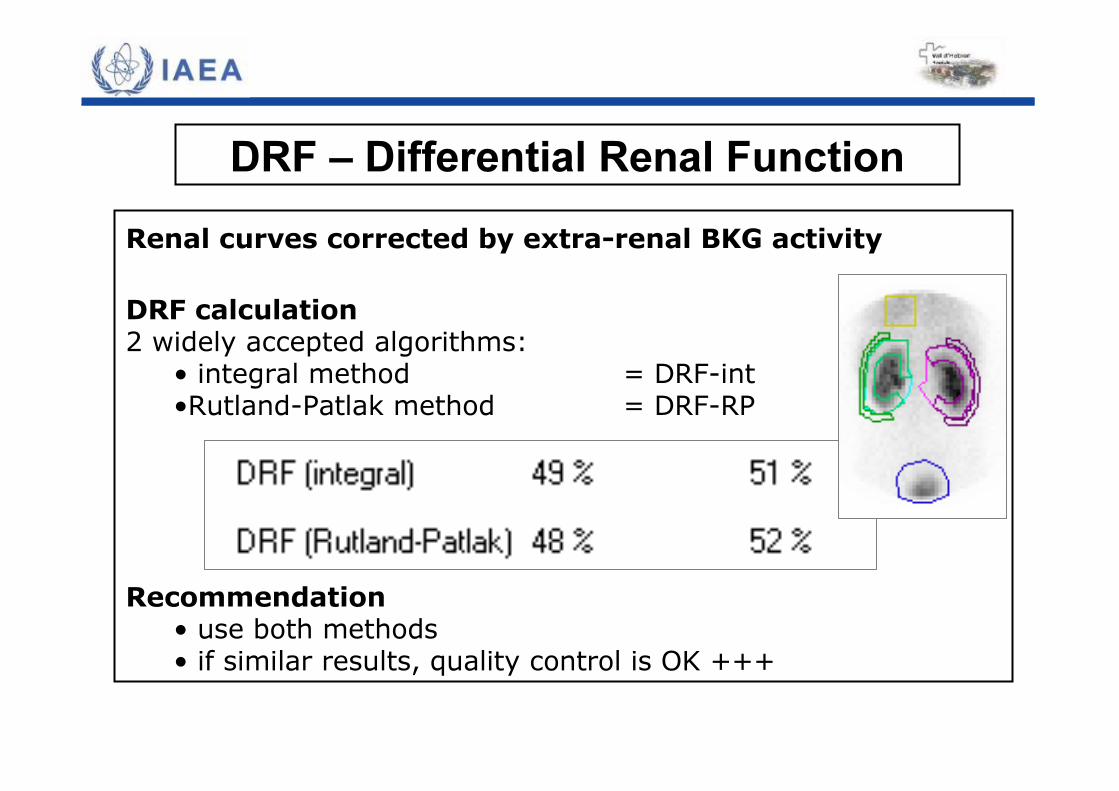
Renal curves corrected by extra-renal BKG activity
DRF calculation2 widely accepted algorithms:
• integral method = DRF-int•Rutland-Patlak method = DRF-RP
Recommendation• use both methods• if similar results, quality control is OK +++
DRF – Differential Renal Function
F-15 / F0DRF calculation – integral methodIf diuretic is given before (15 min) or simultaneously:
• there is increased renal transit time• risk of underestimation of DRF
SolutionCompare:
• Tmax (renogram peak) • with interval used to calculate DRF (usually 1-2’)
If Tmax <2 min, change to lower interval (30-90”)
DRF – Differential Renal Function
Normal range: 45–55%• It is a relative measure of renal function.• DRF may reflect changes due to contralateral kidney:
� contralateral kidney damage � compensatory function of contralateral kidney
Estimation of absolute renal function – GFR• Gamma-camera method:
� unaccurate� great variations, especially in young children� no consensus
• Plasma sampling method:� 99mTc-DTPA or 51Cr-EDTA � more accurate
DRF – Differential Renal Function
Supra-normal function > 55%• Technical error?• Hiperperfusion / hiperfiltration of “obstructed” kidney?• Relative to increased renal size?
(DRF-integral detects greater values in larger kidneys)• More frequent in younger children• 11 % with DRF-integral method• 8 % with DRF-RP method• only 5 % if FRD-integral and FRD-RP are coincident
• To obtain a robust measure of DRF in youngsters:� quality control (motion, injection, etc.)� correct BKG subtraction (ROI)
Robustness of estimation of differential renal function in infants and children with unilateral prenatal diagnosis of a hydronephrotic kidney on dynamic renography. How real is the supranormal kidney?
Gordon, I. EJNM, in pressContradictory Supranormal Function in Hydronephrotic
Kidneys: Fact or Artifact on Pediatric MAG-3 Renal Scans?Clin Nucl Med 2005; 30:91-96
PREDICTION OF RENAL FUNCTION DETERIORATION
Partial obstruction:• affects nephrogenesis• may cause hyperfiltration
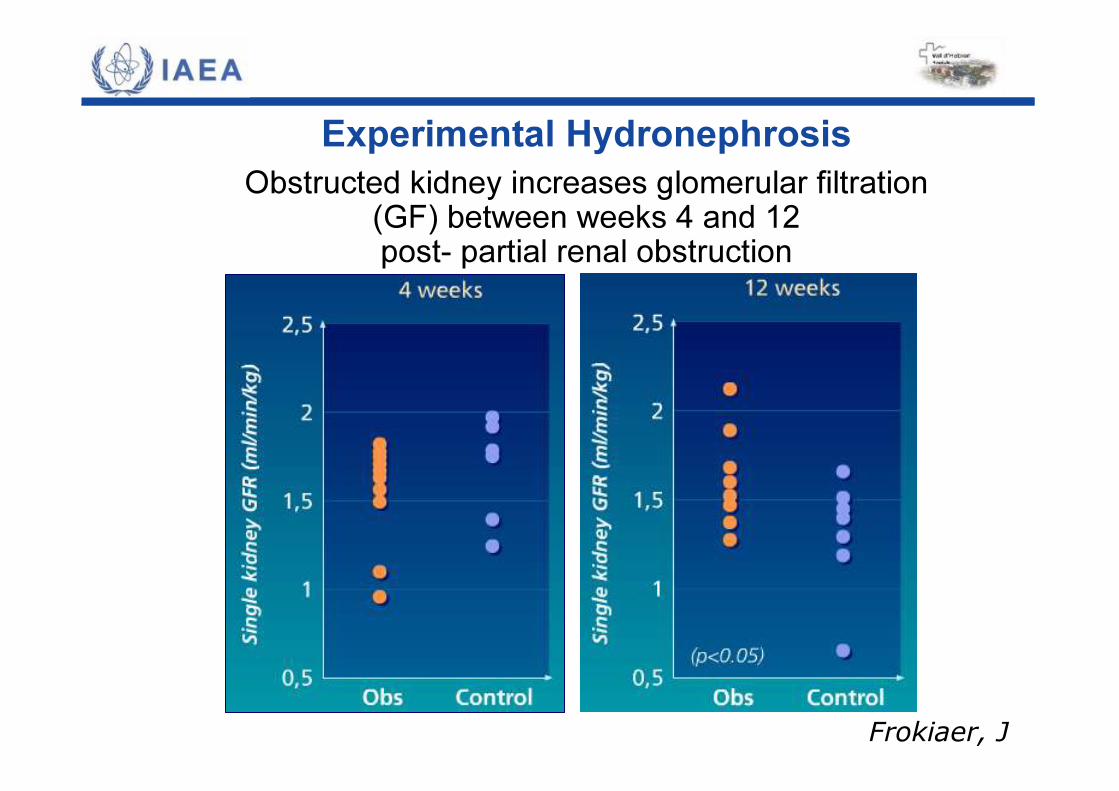
Experimental HydronephrosisObstructed kidney increases glomerular filtration
(GF) between weeks 4 and 12 post- partial renal obstruction
Frokiaer, J
If mentioned mistakes are avoided, DRF is: • A robust method to measure relative renal function.• Accurate: < 5 % inter-observer variability. • A decrease >5-10 % means deterioration.
PITFALLS• ROIs: similar renal and body contours.• Time interval for DRF calculation.
� 30-90 sec F0� 1– 3 min F+15
• MAG3 and dosis: adequate signal-BKG ratio.
DRF – Differential Renal Function
Based on residual activity• ROE = renal output efficiency• PEE = pelvic excretion efficiency • NORA20=normalized residual activity
METHODS FOR QUANTIFICATION OF
EXCRETION
• F-15• F0
� after diuretic� after micturition
Based on the curve response post-furosemide• % drainage 5-10 min• T1/2 post-diuretic • F15
• F20
Validation of renal output efficiency as an objective quantitative parameter in the evaluation of upper urinary tract obstruction.
Chaiwatanarat, Padhy, Bomanji, Nimmon, Sonmezoglu, Britton. J Nucl Med. 1993, 34: 845-8
NORA: A simple and reliable parameter for estimating renal output with or without furosemide challenge Piepsz, Tondeur, Ham. Nucl Med Commun 2000; 21: 317–23
Assessment of drainage in PUJ dilatation: Pelvic Excretion efficiency as an index of renal function Anderson, Rangarjan, Gordon. Nucl Med. Commun 1997, 18: 823-826
• after diuretic• after micturation• after gravity
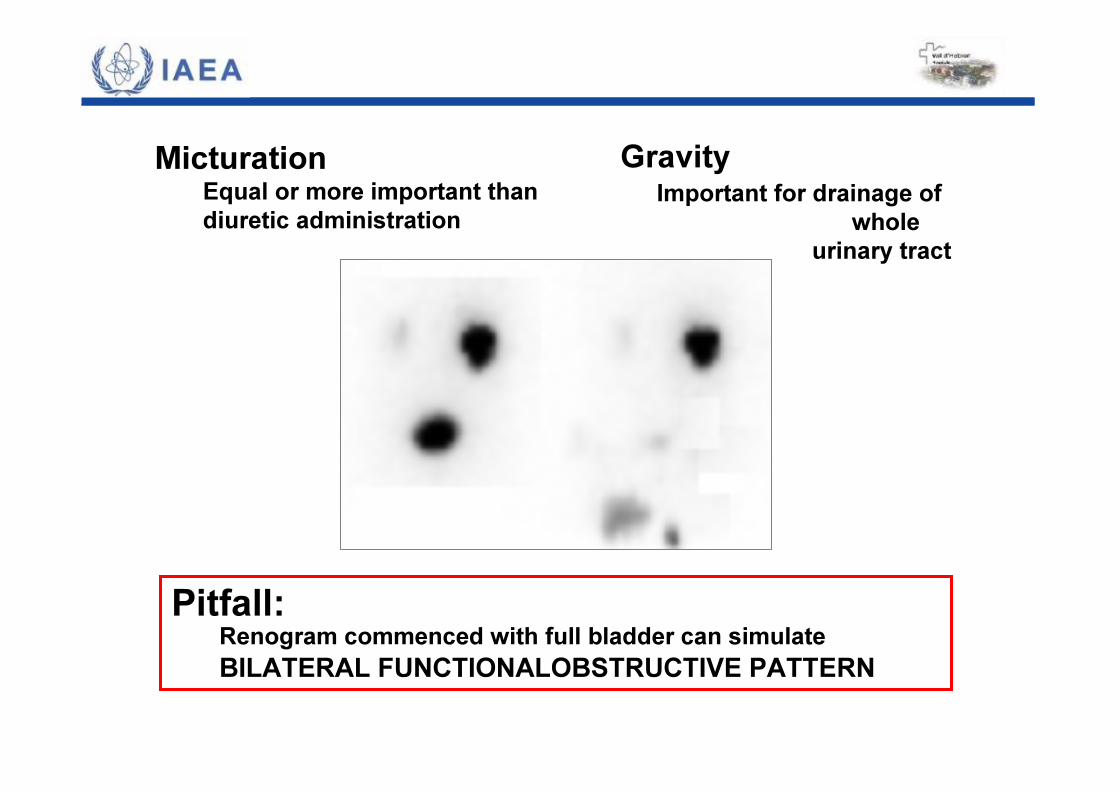
MicturationEqual or more important than diuretic administration
Pitfall:Renogram commenced with full bladder can simulate BILATERAL FUNCTIONALOBSTRUCTIVE PATTERN
Gravity Important for drainage of
whole urinary tract
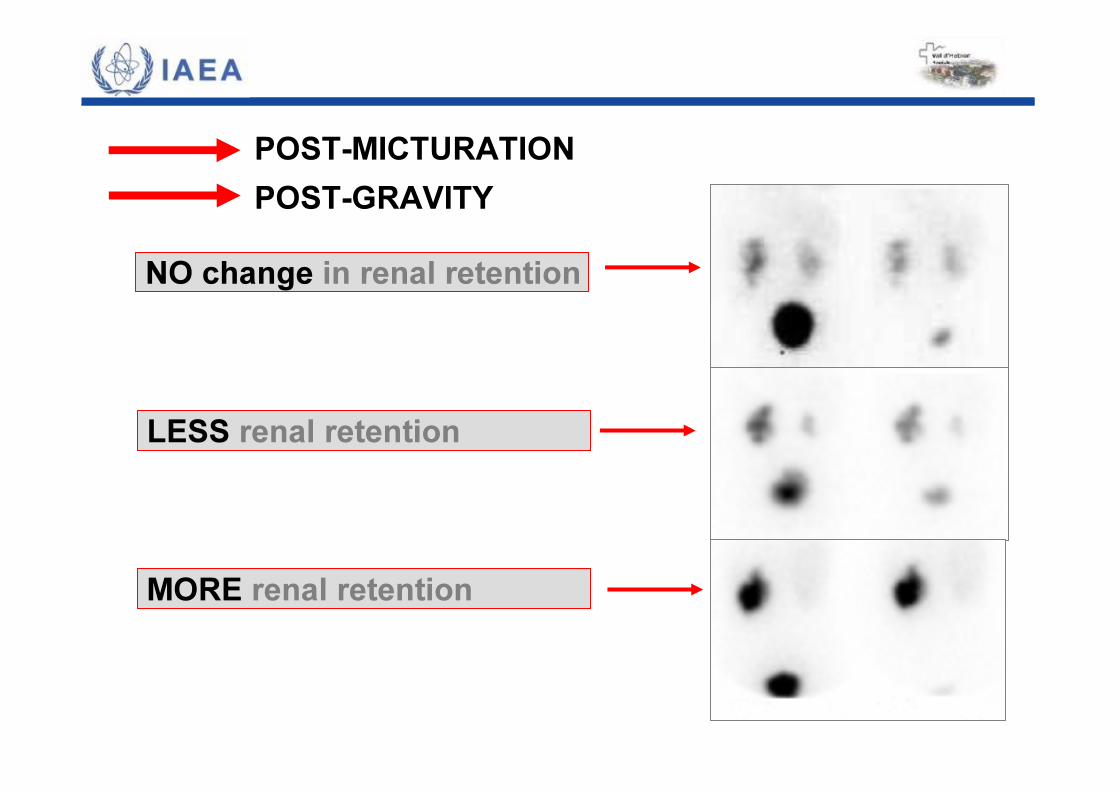
POST-MICTURATION
NO change in renal retentionPOST-GRAVITY
LESS renal retention
MORE renal retention
PITFALLS Causes affecting RENAL EXCRETION results:• Full bladder• Inappropriate hydration• No post-gravity imaging• Immature renal function (newborns) or renal insufficiency• Large volume of excretory structures (renal pelvis)• Increased compliance of excretory structures
LOW EXCRETION
RENAL PELVIS VOLUME DURING DIURESIS IN CHILDREN WITH HYDRONEPHROSIS: IMPLICATIONS FOR DIAGNOSING OBSTRUCTION WITH DIURETIC RENOGRAPHY
Koff. J Urol 2005 174, 303–307,
METHODS FOR QUANTIFICATION OF
EXCRETION
• after diuretic• after micturation• after gravity
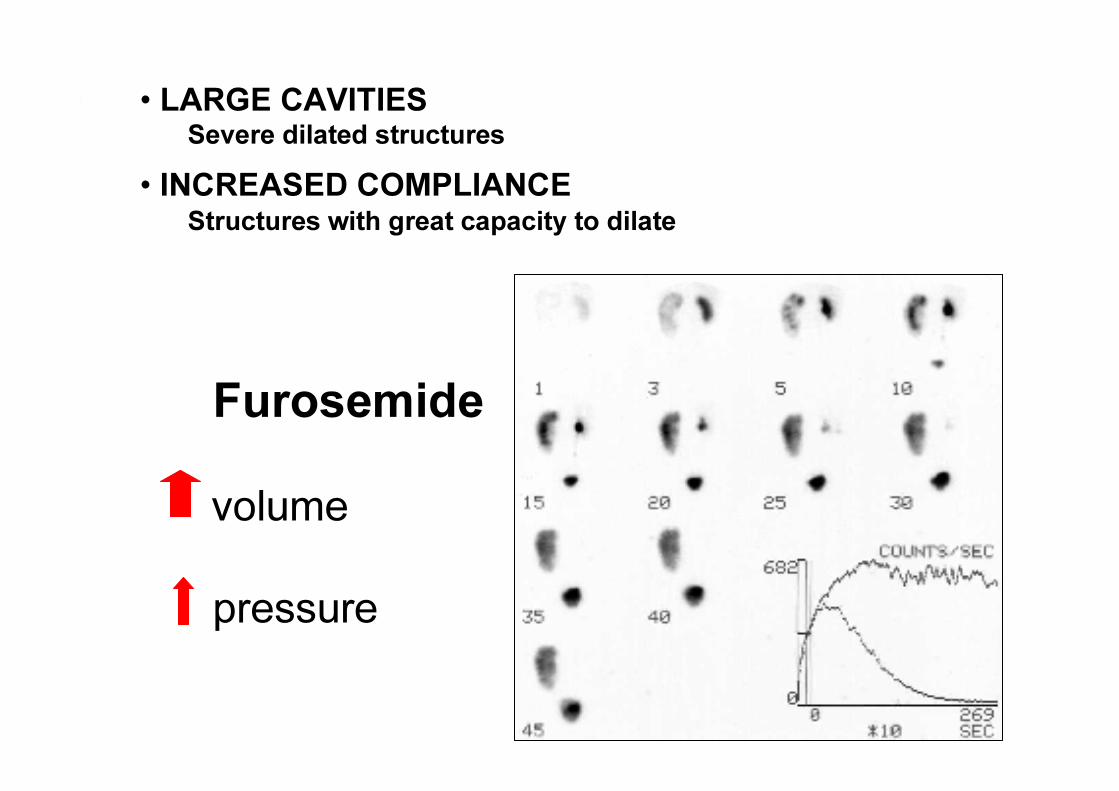
Furosemidevolume
pressure
• LARGE CAVITIESSevere dilated structures
• INCREASED COMPLIANCEStructures with great capacity to dilate
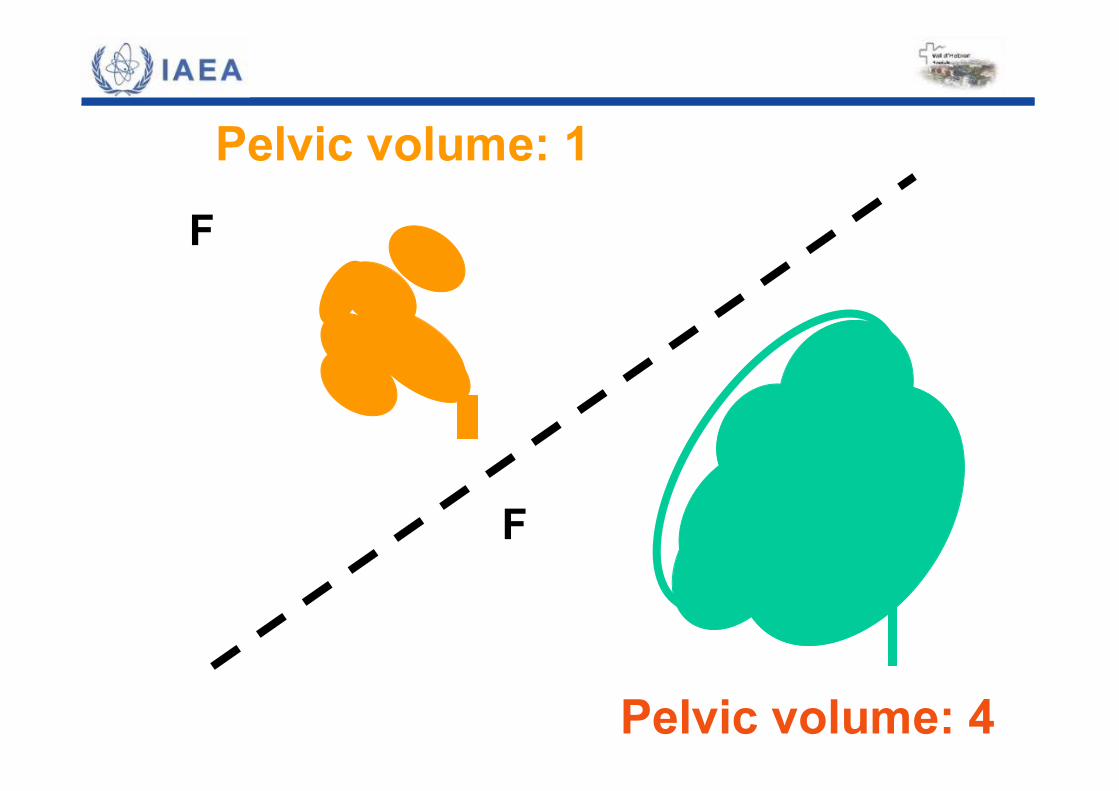
F
Pelvic volume: 1
Pelvic volume: 4
F
T 1/2 after diuretic:• not useful as obstructive parameter• renal pelvis dilates after diuretic • tracer dilutes in renal pelvis• Koff:
� found increased T1/2 post-diuretic in 40% of patients � but there was no obstruction� more frequent in <2 years old � more frequent in children with large volume of renal pelvis
Impaired drainage on diuretic renography using half-time or pelvic excretion efficiency is not a sign of obstruction in children with a prenatal diagnosis of unilateral renal pelvic dilatation
Amarante, Anderson, GordonJ Urol, 169, 1828–1831, 2003
Renal pelvis volume during diuresis in children with hydronephrosisimplications for diagnosing obstruction with diuretic renography
Koff, Binkovitz, Voley, JayanthiJ urol, 174, 303–307, july 2005
Drainage can be best quantified using tools to measure RESIDUAL ACTIVIDAD:• ROE : renal output efficiency• PEE : pelvic excretion efficiency• NORA : normalized residual activity
METHODS FOR QUANTIFICATION OF
EXCRETION
• after diuretic• after micturation• after gravity
Drainage can be best quantified using tools to measure RESIDUAL ACTIVIDAD:• ROE : renal output efficiency• PEE : pelvic excretion efficiency• NORA : normalized residual activity
Especially if diuretic administration time: • F-15• F0
These parameters take into account RENAL FUNCTION
METHODS FOR QUANTIFICATION OF
EXCRETION
• after diuretic• after micturation• after gravity
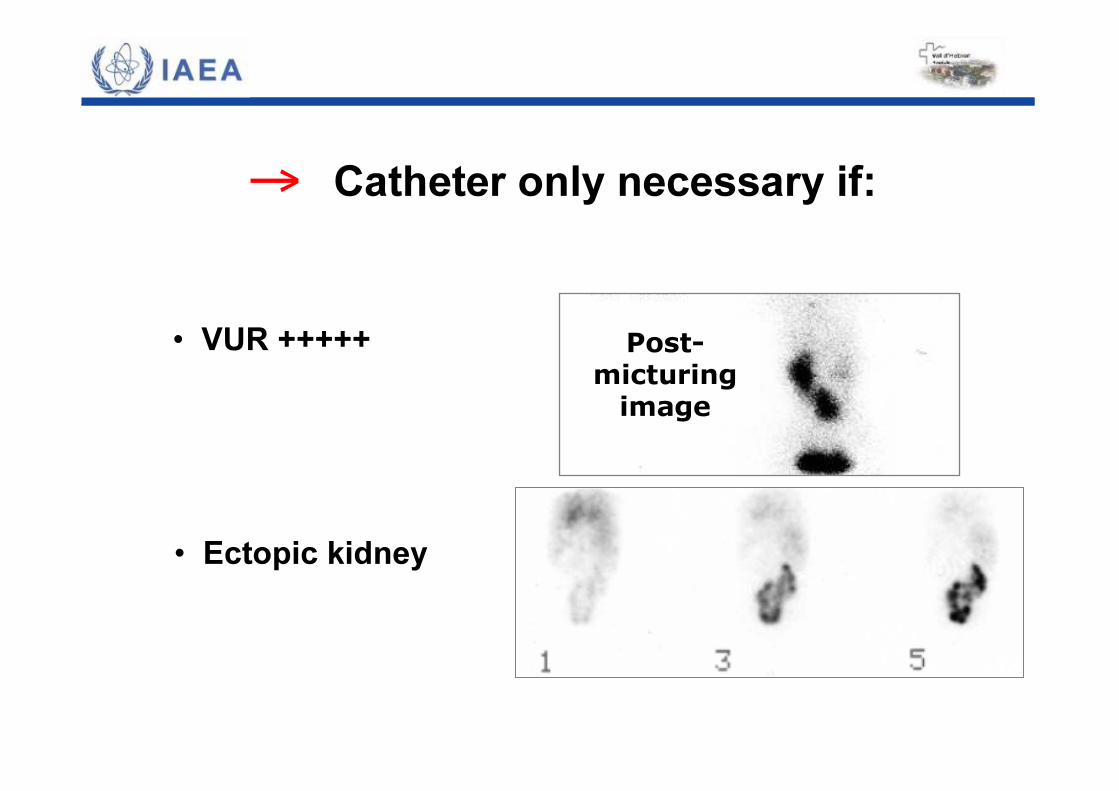
Catheter only necessary if:
• VUR +++++
• Ectopic kidney
Post-micturing image
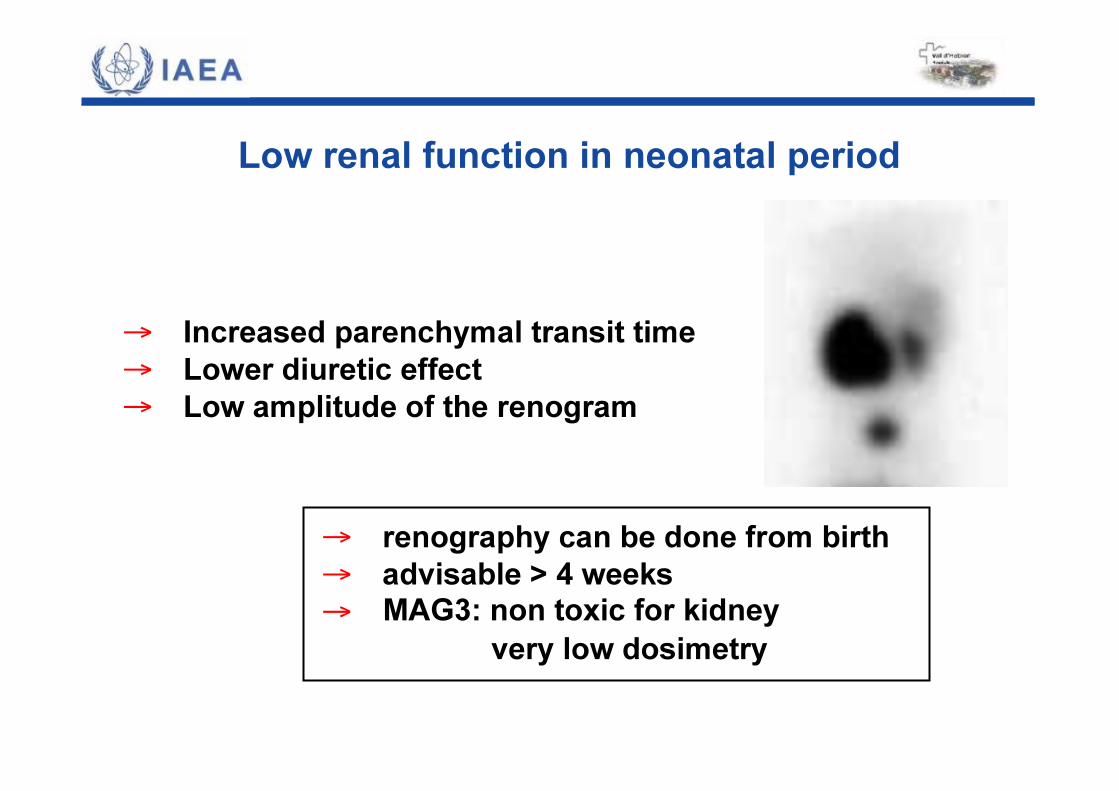
Low renal function in neonatal period
Increased parenchymal transit timeLower diuretic effectLow amplitude of the renogram
renography can be done from birthadvisable > 4 weeksMAG3: non toxic for kidney
very low dosimetry
PROCEDURE:- Technique- Patient preparation
INTERPRETATION:- Images- Curves- Quantitative parameters
OBSTRUCTIVE PROFILE ???
INTERPRETATION OF DIURETIC RENOGRAM
IN CHILDREN
• Drainage can vary with physiologic conditions• Drainage spontaneously improves with time• Surgery improves drainage• Good drainage = good prognosis• Impaired drainage = possible obstruction
Congenital unilateral hydronephrosis: a review of the impact of diuretic renography on clinical treatment
ESKILD-JENSEN, GORDON, PIEPSZ, FRØKIÆRJ Urol 173, 1471–1476, 2005
Indications for SURGERY• Progressive hydronephrosis• Absent or poor diuretic response• Deterioration of renal function• Infection
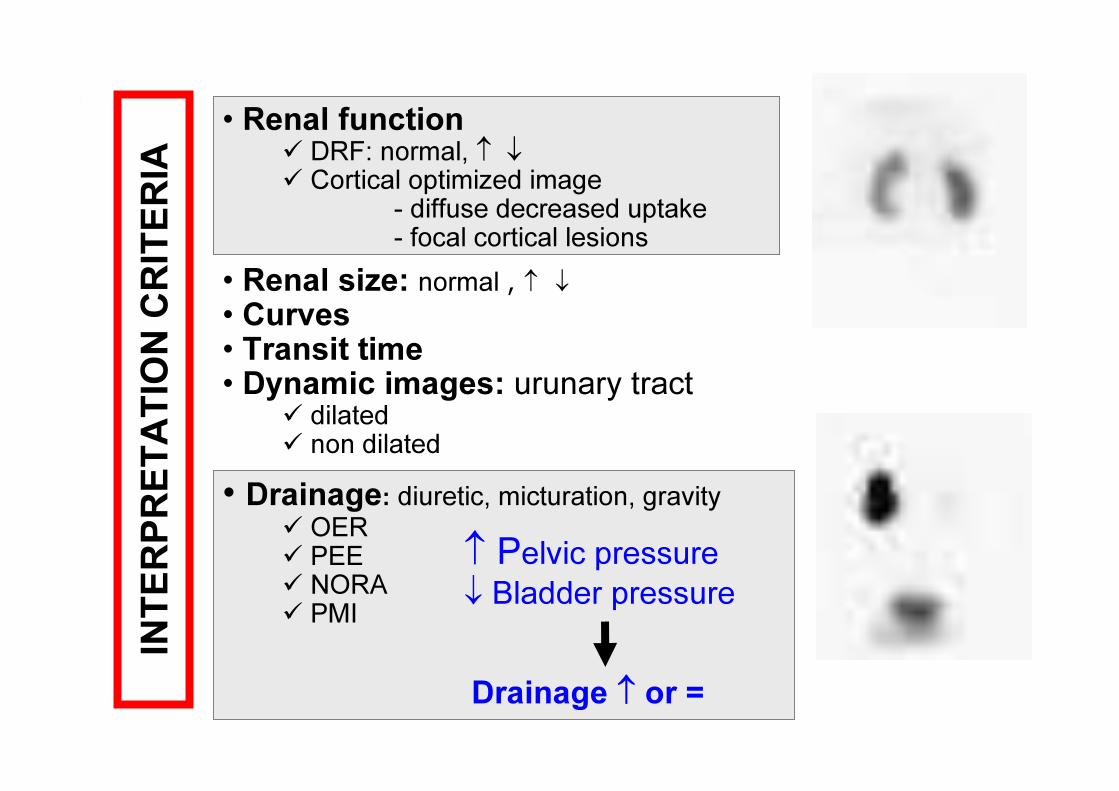
• Renal function� DRF: normal, ↑ ↓� Cortical optimized image
- diffuse decreased uptake- focal cortical lesions
• Renal size: normal , ↑ ↓• Curves• Transit time• Dynamic images: urunary tract
� dilated� non dilated
• Drainage: diuretic, micturation, gravity� OER� PEE� NORA� PMI
INTE
RPRE
TATI
ON
CRIT
ERIA
Drainage ↑ or =
↑ Pelvic pressure↓ Bladder pressure
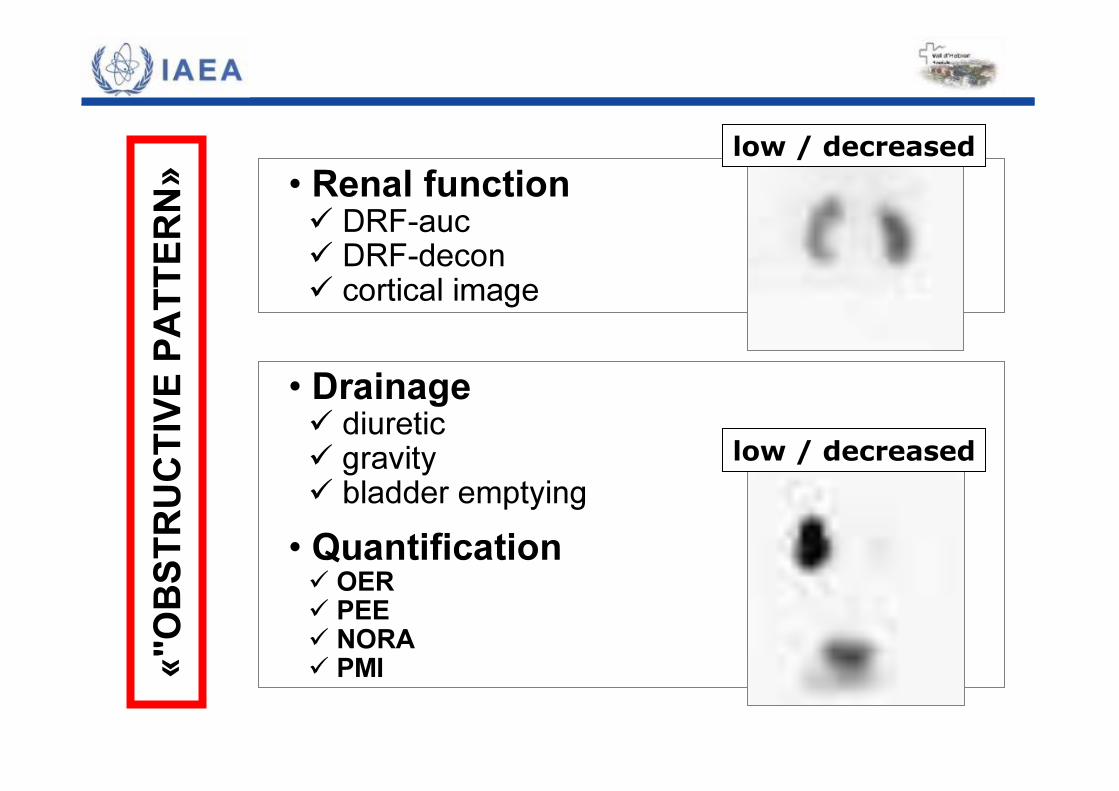
• Drainage� diuretic� gravity� bladder emptying
• Quantification� OER� PEE� NORA� PMI
• Renal function� DRF-auc� DRF-decon� cortical image
«"O
BSTR
UCTI
VE P
ATTE
RN»
low / decreased
low / decreased
Frequently, diuretic renography is performed without considering:
• previous hydration• renal function• renal pelvis size• gravity• bladder emptying
PITFALLS
Technical errors should also be considered:
• radiopharmaceutical labelling• injection technique• patient motion• diuretic injection• urine contamination• ROI delineation
Conclusion:IF DIURETIC RENOGRAPHY IS WELL STANDARDIZEDAND POTENTIAL PITFALLS CONSIDERED, IT IS A VALUABLE AND REPRODUCIBLE METHOD TO OBTAIN INFORMATION ON DRF AND RENAL DRAINAGE