Embed Size (px)
Citation preview

Diagnosis of SternomastoidTumor of Infancy by Fine-NeedleAspiration CytologyBipin Kumar, M.D.* and Anju Pradhan, M.D.
Sternomastoid tumor of infancy, also known as fibromatosis collior muscular torticollis, is a benign fibroblastic lesion of thesternocleidomastoid muscle presenting as a firm, fusiform, non-tender neck mass of 1–3 cm in greatest dimension in theperinatal period. Various modalities are used for the diagnosisincluding radiographic studies, fine-needle aspiration cytology(FNAC), and open biopsy. We report eight cases of sternomas-toid tumor of infancy diagnosed by FNAC. The objective of thestudy is to present the role of FNAC in the diagnosis of sterno-mastoid tumor with its cytomorphological features. FNA wasdone by using 23-guage needle and 10 ml disposable plasticsyringe. The wet smears were fixed in 95% ethanol and proc-essed for Papanicolaou stain. The dried smears were stainedwith May–Grunwald–Giemsa stain. The smears were studied forcytomorphologic features. The age of the patients rangedbetween 2 and 10 weeks. Male: Female ratio was 1.6:1. Six ofeight had history of prolonged labor, two had history of breechpresentation, and three had history of forceps assisted vaginaldelivery. Cytologic findings included singly scattered andloose clusters of benign fibroblasts with moderate amount ofunipolar to bipolar cytoplasm and plumped, ovoid nuclei.Many multinucleated giant cells consistent with atrophic musclefibers were also seen. FNAC is a reliable, safe, and cost-effective method and can provide a rapid and reliable diagno-sis of sternomastoid tumor of infancy. Diagn. Cytopathol.2011;39:13–17. ' 2010 Wiley-Liss, Inc.
Key Words: sternomastoid tumor; fibromatosis colli; sternoclei-domastoid muscle; fine-needle aspiration cytology; benign fibro-blasts
Sternomastoid or sternocleidomastoid tumor of infancy
(SCMI) also known as fibromatosis colli is a benign fibro-
blastic lesion affecting the body of sternocleidomastoid
muscle (SCM).1–10 It is the most common cause of neck
mass in the perinatal period with an incidence of 0.4%
live births.1–3,5 The classic presentation is the presence of
firm to hard fusiform mass in the lower or middle portion
of the SCM.1–6 However, it can be anywhere along the
length of the muscle.1 The right side is more commonly
involved than left7 and male affected more than female.5,6
It is usually identified during the second to fourth week
of life.2–4 The swelling may increases in size for several
weeks, then stabilizes in size for few months and finally
diminishes spontaneously by 4–8 months.4,9,10 However
the lesion, that presents after 1 month of age may not
resolves but increases in size.1 Contraction of fibrous
tissue within the lesion can lead to tightening of the
muscle resulting into motion restriction and ipsilateral
head tilt or muscular torticollis also known as wry
neck.1,10 SCMI is the most common cause of congenital
muscular torticollis with incidence of 10–20% among the
cases.3,9 It has a characteristic appearance. The head is
rotated and tilted toward the side of mass and the chin is
turned away from the affected side.4,6,10 This is secondary
to fibrosis, shortening of the affected muscle and its
inability to keep pace with the growth of the normal mus-
cle.6,10 Persistent torticollis may develop into cranial or
facial asymmetry, if remain uncorrected.9,10 SCMI is
associated with increased incidence of musculoskeletal
disorder such as metatarsus adductus, hip dysplasia, and
talipes equinovarus.3,6 Hip dysplasia is an associated fea-
ture in approximately 2.4–10% cases and it ranges from
subluxation to dislocation.3 It involves more commonly in
the side of sternocleidomastoid fibrosis and severity of
it is correlated with the severity of the torticollis.3 In
addition, lytic clavicular lesions, ipsilateral mandibular
asymmetry, plagiocephaly, occipital condyle asymmetry,
elevation of the ipsilateral clavicle and shoulder, facial
deformities, postural cervico-thoracic scoliosis, and gas-
tro-esophageal reflux may be associated features seen in
the cases of SCMI.3,4,6,9,10
Department of Pathology, B. P. Koirala Institute of Health Sciences,Dharan, Nepal
*Correspondence to: Bipin Kumar, M.D., Department of Pathology, B.P. Koirala Institute of Health Sciences, Dharan, Nepal.E-mail: [email protected]
Received 22 September 2009; Accepted 1 December 2009DOI 10.1002/dc.21316Published online 20 January 2010 in Wiley Online Library
(wileyonlinelibrary.com).
' 2010 WILEY-LISS, INC. Diagnostic Cytopathology, Vol 39, No 1 13

In this study, five clinically diagnosed and three other
neck lesions are diagnosed as SCMI by fine-needle aspira-
tion cytology (FNAC). The pathogenic mechanism, differ-
ential diagnosis and its cytomorphological features are
discussed.
Methods
Cases
Eight infants (age: 2–10 weeks) were sent for FNAC
from the department of otorhinolaryngology between the
period of August 2006 to March 2009 and diagnosed as
SCMI. Five of them were suspected clinically as SCMI,
two as tuberculous lymphadenitis, and the remaining one
as branchial cyst.
Methods
FNA was done with a 23-gauge needle and 10 ml dispos-
able plastic syringe. The wet smears were fixed in 95%
ethanol and processed for Papanicolaou stain, and the
dried smears were stained with May–Grunwald–Giemsa
stain. The smears were studied for cytomorphological fea-
tures.
Results
The details of clinical and cytological findings are given
in Table I. The swelling was noticed at age 1–8 week
while age at diagnosis was 2–10 weeks. The male to
female ratio was 1.6:1 (5:3). Birth history was found in
all cases. Seven were delivered by primiparous. Six of
eight had relevant obstetrical history with associated pro-
longed labor. Two had history of breech presentation, one
delivered by normal vaginal root whereas other by cesar-
ean section; three had history of forceps extraction and
the remaining one had history of prolonged labor with
normal vaginal delivery. Two patients had normal obstet-
rical history. Each of these patients had neck mass of 2–3
cm in greatest dimension, five on right side and three on
the left. The mass was found in the middle part in four
cases, in lower third in three cases and one had mass
located in upper portion of SCM. Two cases had torticol-
lis in addition to neck mass and one had fever (viral?).
Cytological Findings
Smear showed scant to moderate cellularity comprising of
scattered singly or loosely cohesive clusters of spindle
and plump fibroblasts with associated strands of collagen.
These cells had oval to elongated nuclei, evenly dispersed
fine granular nuclear chromatin and unipolar or bipolar
tail of cytoplasm. Naked or stripped nuclei were also
present (Figs. 1–3). Atrophic skeletal muscle fibers in the Table
I.Clinical
andCytological
Details
SN
Clinicalfeatures
Cytolog
ical
features
Age/sex
Obstetrical
history
Location
(neck)
Size
(cm)
Associated
symptom
sClinical
diag
nosis
Cellularity
Giant
cells
Fibroblast
Bare
nuclei
Collagen
Backgroun
dDiagnosis
115d/M
Primi,breech,prolonged
labor,
delivered
byCS
Rt,middle
third
2.0
��SCMI
Moderate
++
++++
++
++
Hem
orrhagic
SCMI
228d/M
Primi,norm
alvaginal
delivery
Rt,lower
third
2.8
Fever
TBLN
Scant
+++
+++
++
+++
Myxoid,
hem
orrhagic
SCMI
310w/F
Primi,prolonged
labor,
norm
aldelivery
Lt,middle
third
2.5
��TBLN
Moderate
+++
+++
+++
++++
Myxoid
stroma
SCMI
435d/M
Para2,breech,prolonged
labor,
norm
aldelivery
Rt,lower
third
2.5
��SCMI
Moderate
++++
++++
+++
+++
Hem
orrhagic
SCMI
526d/F
Primi,prolonged
labor,
forcepsextraction
Lt,middle
third
3.0
Torticollis
SCMI
Scant
++
+++
++
+++
Hem
orrhagic
SCMI
627d/M
Priminorm
alvaginal
delivery
Rt,upper
third
2.5
��Branchial
cleftcyst
Scant
+++
++++
++
+++
Hem
orrhagic
SCMI
714d/M
Primi,prolonged
labor,
forcepsextraction
Rt,middle
third
2.0
��SCMI
Moderate
+++
++++
+++
+++
Myxoid
stroma
SCMI
817d/F
Primi,prolonged
labor,
forcepsextraction
Lt,lower
third
2.0
Torticollis
SCMI
Moderate
++
+++
++
+++
Hem
orrhagic
SCMI
SN,serial
number;d,day;w,week;M,male;
F,female;
CS,cesarean
section;Rt,right;Lt,left;SCMI,sternomastoid
tumorofinfancy;TBLN,tuberculouslymphadenitis.
KUMAR AND PRADHAN
14 Diagnostic Cytopathology, Vol 39, No 1
Diagnostic Cytopathology DOI 10.1002/dc

form of myofibers with cross striations and multinucleated
giant cells were also seen (Fig. 4).
Discussion
The pathogenic mechanism of SCMI is still not clear.
Mechanism includes fetal malposition, birth trauma, is-
chemic necrosis after vascular compression during birth,
infection, and the presence of endogenous factor.1–4,6–10
A birth trauma theory postulates about difficult labor and
delivery which cause tearing of the SCM with subsequent
bleeding, hematoma, fibrosis, and contracture.3,10 Infec-
tion theory postulates intrauterine infection of the muscle,
with subsequent myositis and fibrosis.3,4 A vascular com-
promise theory postulates arterial occlusion or venous sta-
sis during labor leading to vascular insult with subsequent
muscle infarction and fibrosis.2,3,6 None of these theory
confirm the features of SCMI as no evidence of acute
bleeding, hematoma formation, subacute or chronic blood
products, organisms or inflammatory cells are found.3,6
Proposed mechanism of injury consisting of localized
kinking or crushing followed by in utero ischemia, reper-
fusion, or neurologic damage of the SCM are also
found.1,3 Still another possible theory regarding the
growth as a peculiar hamartomatous process6 and role of
clonal chromosomal abnormalities are also proposed.8
Well-recognized association between the SCMI and pri-
miparous births, breech presentations, forceps deliveries,
and difficult labor are found.1,3,10 Most authors emphasize
the importance of obstetrical malposition, particularly
breech presentation as an associated factor.1,2,9,10 This
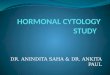
Fig. 4. Smear showing multinucleated giant cells (MGG; 340).[Color figure can be viewed in the online issue, which is available atwileyonlinelibrary.com.]
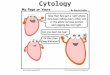
Fig. 1. Moderately cellular smear showing scattered singly or looselycohesive clusters of fibroblasts with associated strands of collagen andgiant cells (Papanicolaou; 320). [Color figure can be viewed in theonline issue, which is available at wileyonlinelibrary.com.]
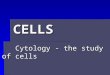
Fig. 2. smear showing scant cellularity revealing bundle of collagenfibers, fibroblasts, stripped or bare nuclei, and giant cells (Papanicolaou;320). [Color figure can be viewed in the online issue, which is availableat wileyonlinelibrary.com.]
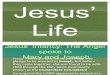
Fig. 3. Smear showing plumped oval to spindle shaped fibroblasts hav-ing bland nuclei and unipolar to bipolar tail of cytoplasm along with fewbare nuclei (Papanicolaou; 340). [Color figure can be viewed in theonline issue, which is available at wileyonlinelibrary.com.]
STERNOMASTOID TUMOR
Diagnostic Cytopathology, Vol 39, No 1 15
Diagnostic Cytopathology DOI 10.1002/dc

study also shows association of SCMI with primiparous
births (7/8), breech presentations (2/8), forceps deliveries
(3/8), and difficult labor (6/8).
The lesion represents benign but infiltrative process
with partial replacement of SCM by diffuse fibroblastic
proliferation.2,5,7 Muscle fibers divided by the proliferat-
ing fibroblasts undergo atrophy.2,7 The early diagnosis for
this lesion is important because it needs conservative ther-
apy.2,4 The diagnosis is often can be made by clinical his-
tory and physical examination.2 On examination, the mass
is mobile in horizontal plane and are free from overlying
skin, particularly when head tilt is found.2,9,10 If the head
tilt is minimal or absent and mass is poorly defined, fur-
ther evaluation is required.2
The differential diagnosis include various reactive and
benign process, and malignant lesions such as hemangi-
oma, lymphangioma, lipoma, lipoblastoma, teratoma, thy-
roglossal duct cyst, cervical lymphadnitis particularly
tuberculosis, congenital branchial cleft cyst, congenital
goiter, heteropic thyroid, accessory lobe of thyroid, lym-
phoma, neuroblastoma, embryonal rhabdomyosarcoma,
low-grade fibrosarcoma, nodular fascitis, and calcifying
aponeurotic fibroma.1–10 The malignant lesions require an
early diagnosis, so that immediate therapy can be insti-
tuted.4 The remaining benign conditions need delayed sur-
gical procedures unless the mass compresses the airway
or other vital structures.4 Diagnostic surgical procedures
are more invasive, expensive, inconvenient for the
patients and their parents, and may lead to complications
of cosmetic defects resulting from contracture bands and
hence, reserved for complicated cases.2 For early diagno-
sis and desirability, and to avoid surgery in this age
group, noninvasive diagnostic procedures have a great
value.4 Radiographic technique is useful in the diagnosis
of SCMI.4 Computed tomography (CT) and ultrasonogra-
phy (USG) can locate the tumor in the body of SCM, and
differentiate solid and cystic lesions.1–4,9,10 The typical
CT scan shows the mass to be part of the muscle.4,9 The
area of enlargement is usually in the inferior half of the
muscle.9 Calcification in the mass or rest of the muscle
remains absent, and the cervical spines remain normal.9
These investigative procedures eliminate congenital cystic
and lymphatic malformation from diagnostic considera-
tion.2 USG shows the well-defined noncystic ovoid or
fusiform homogenous mass as a part of the muscle.9 The
mass moves with the muscle and is usually isoechoic or
slightly hypoechoic to the rest of the muscle.9 USG can
help to rule out the thyroglossal duct cyst, lymphangioma,
and lymphadenopathy.9 It also gives idea about the nature
of the swelling whether it is due to inflammatory or
malignant process?9 The absence of calcification rules out
teratoma, neuroblastoma, hemangioma, and abscess.9 It
also distinguishes thyroid lesion from SCMI.9 Because it
can be difficult to differentiate SCMI from surrounding
tissue, using CT or MRI can be used to distinguish tumor
from muscle, fat, or even scar tissue.9 CT and MRI are
costly, require sedation and contrast administration, and
are more traumatic than USG.3,4 Hence, USG can be pref-
erable radiologic technique for evaluation of neck masses
in neonates.3,4 However, these procedures are costly and
not available in all hospitals.6
Fine-needle aspiration is minimally invasive, cost-effec-
tive, time saving, quick, safe way, and well-established
outdoor procedures for the evaluation and diagnosis of
head and neck masses.1–7 Clinical impression of SCMI is
readily and easily confirmed by FNAC at bed side and
thus avoid more invasive procedures.2 The cytomorphol-
ogy of it reveals spindle shaped fibroblasts having bland
ovoid nuclei or fusiform cells with unipolar or bipolar
wispy cytoplasm.1–7 Atrophic skeletal muscles, muscle
giant cells, and collagen fibers are seen in a clean or myx-
oid background.6 Neither inflammation nor necrosis is
seen.2,6 FNAC of neuroblastoma, rhabdomyosarcoma, and
lymphoma show small blue cells as compared with the
benign spindle cells of SCMI.1,2,6 These small round cell
tumor react with antibodies to neurone specific enolase,
myoglobin, and common leucocyte antigen, respectively.3
The cystic lesions can be ruled out on the basis of clinical
examination and USG findings.1 FNA can support and
confirm the diagnosis.1 FNA of branchial cleft cyst, thyro-
glossal duct cyst, and lymphangioma yield variable
amount of fluid.2 On microscopy, branchial cleft cyst
shows benign squamous cells and inflammatory cells in
the dirty background1; thyroglossal duct cyst shows squa-
mous or columnar cells and multiple cyst macrophages
with or without follicular epithelial cells1,2 and lymphan-
gioma shows modest number of lymphocytes, macro-
phages, and rare endothelial cells.1 Hemangioma yields
altered blood and shows blood elements, hemosiderin
laden macrophages, and endothelial cells. Teratoma
reveals mixture of different type of cells pertaining to dif-
ferent germ cell layers.1 Thyroid lesion shows follicular
epithelial cells and variable amount of colloid. Cervical
lymphadenitis shows lymphoid series cells and tuberculo-
sis shows granulomas with or without caseation. Mature
adipose tissue fragments are seen in lipoma and lipoblast
are seen in lipoblastoma.1,2 None of these lesions show
benign fibroblasts and atrophic muscle fibers or muscle
giant cells. The other fibroblastic lesion such as nodular
fascitis can be excluded by absence of inflammation and
edema in the background.2 Infantile fibromatosis and cal-
cifying aponeurotic fibroma show infiltration of skeletal
muscle with collection of immature fibroblasts. Infantile
fibromatosis is a more infiltrative process and not remains
confined to single muscle group as in SCMI.4 Calcifying
aponeurotic fibroma rarely involves cervical region in
older child and it shows calcification cytologically and ra-
diologically.3,4 Low-grade fibrosarcoma rarely affects the
KUMAR AND PRADHAN
16 Diagnostic Cytopathology, Vol 39, No 1
Diagnostic Cytopathology DOI 10.1002/dc

neck and usually present as larger lesion which show
hypercellularity and cellular atypia.4,5
After the diagnosis is confirmed, the parents of infants
are reassured and therapy can be immediately started.1
The treatment modalities are dependent on the size of the
mass and the presence of torticollis.1 Most of the cases of
sternomastoid tumor resolves spontaneously in few
months or respond to conservative treatment including
physical therapy with heat, massage, stretching exercises
for the affected muscle, strengthening exercises for con-
tralateral muscle, and occasionally the use of neck braces
during sleep.1,9,10 If the lesion is detected early, therapy
instituted during the first month of life and continued for
at least a year; 90% of patients will have a permanent
correction of the deformity.3,9 Surgical treatment is re-
served for those cases in whom contraction persists
beyond 1 year of age and for those who develop craniofa-
cial abnormalities.3,9,10 Surgical procedures include distal
tenotomy to avoid craniofacial asymmetry, scoliosis, and
plagiocephaly; muscle lengthening and excision of the
SCM and surrounding muscle.9 In our study, seven of
eight cases get free from the swelling after conservative
therapy and still one remaining is in follow up.
Conclusion
FNAC is safe, rapid, cost-effective, reliable outdoor pro-
cedure for the diagnosis of SCMI which can alley the
anxiety of parents quickly and guide for earlier conserva-
tive treatment so that permanent correction of the defor-
mity could be done and surgery can be avoided in these
cases, which can be reserved for the patients who develop
craniofacial abnormalities or have contraction that persists
beyond 1 year of age.
References
1. Kurtycz DF, Logrono R, Hoerl HD, Heatley DG. Diagnosis of fibro-matosis colli by fine needle aspiration. Diagn Cytopathol 2000;23:338–342.
2. Schwartz RA, Powers CN, Wakely PE, Jr, Kellman RM. Fibromato-sis colli. The utility of fine needle aspiration in diagnosis. Arch Oto-laryngol Head Neck Surg 1997;123:301–304.
3. Apple SK, Nieberg RK, Hirschowitz SL. Fine needle aspirationdiagnosis of fibromatosis colli. A report of three cases. Acta Cytol1997;41:1373–1376.
4. Gonzales J, Ljung BM, Guerry T, Schoenrock LD. Congenital torti-collis: Evaluation by fine-needle aspiration biopsy. Laryngoscope.1989;99:651–654.
5. Sauer T, Selmer L, Freng A. Cytologic features of fibromatosis colliof infancy. Acta Cytol 1997;41:633–635.
6. Sharma S, Mishra K, Khanna G. Fibromatosis colli in infants. Acytologic study of eight cases. Acta Cytol 2003;47:359–362.
7. Nayak SP, Munshi MM, Bobhate SK. Cytodiagnosis of fibromatosiscolli. Cytopathology 2007;18:266–268.
8. Ekinci S, Karnak I, Tanyel FC. Infantile fibromatosis of the sterno-cleidomastoid muscle mimicking muscular torticollis. J Pediatr Surg2004;39:1424–1425.
9. Jaber MR, Goldsmith AJ. Sternomastoid tumor of infancy: Twocases of interesting entity. Int J Pediatr Otorhinolaryngol 1999;47:269–274.
10. Tufano RP, Tom LWC, Austin MB. Bilateral sternomastoid tumorsof infancy. Int J Pediatr Otorhinolaryngol 1999;51:41–45.
STERNOMASTOID TUMOR
Diagnostic Cytopathology, Vol 39, No 1 17
Diagnostic Cytopathology DOI 10.1002/dc