Embed Size (px)
Citation preview

Diagnosis and new classificationProf. Dr. Adriaan Voors University Medical Center Groningen the Netherlands

Trea
tmen
t of D
iabe
tes
in H
F
University Medical Center Groningen
Disclosures• AAV received consultancy fees and/or research grants from: Alere,
AstraZeneca, Bayer, BMS, Boehringer, Cardio3Biosciences, Merck/MSD, Novartis, Servier, Singulex, Sphingotec, Stealth, Trevena, Vifor.
• AAV is supported by a grant from the European Commission: FP7-242209-BIOSTAT-CHF
• AAV is Clinical Established Investigator and supported by other grants of the Dutch Heart Foundation

www.escardio.org/guidelines
4
Now online available
http://www.escardio.org/Guidelines-&-Education/Clinical-Practice-Guidelines/Acute-and-Chronic-Heart-Failure

www.escardio.org/guidelines
Key Points
• Definition• New Classification HFrEF/HFpEF• Diagnosis of Heart Failure (general)
• (NT-pro)BNP cut-offs
• Diagnosis of HFpEF• Assessment of Diastolic Dysfunction
5

www.escardio.org/guidelines
Definition
• HF is a clinical syndrome characterized by typical symptoms (e.g. breathlessness, ankle swelling and fatigue) that may be accompanied by signs (e.g. elevated jugular venous pressure, pulmonary crackles and peripheral oedema) caused by a structural and/or functional cardiac abnormality, resulting in a reduced cardiac output and/or elevated intracardiac pressures at rest or during stress
6

www.escardio.org/guidelines
Key Points
• Definition• New Classification HFrEF/HFpEF• Diagnosis of Heart Failure (general)
• (NT-pro)BNP cut-offs
• Diagnosis of HFpEF• Assessment of Diastolic Dysfunction
7

www.escardio.org/guidelines
Hands-up Question 1
• Which LVEF cut-off to use for HFrEF?• A) ≤ 35%• B) ≤ 40%• C) ≤ 45%• D) ≤ 50%
8
www.escardio.org/guidelines
Hands-up Question 2
• Which LVEF cut-off to use for HFpEF?• A) ≥ 35%• B) ≥ 40%• C) ≥ 45%• C) ≥ 50%
9
www.escardio.org/guidelines
10
“The middle child of HF deserves attention: available data suggest that it constitutes a sizeable proportion (10–20%) of the HF population, has a unique clinical, echocardiographic, haemodynamic, and biomarker profile compared with HFrEF and HFpEF, and carries a poor prognosis. Large gaps in evidence regarding its treatment warrant further study.”

www.escardio.org/guidelines
• TOPCAT:n=3444; EF≥45%; • spironolactone vs. placebo• Primary outcome: neutral• HFmrEF greater treatment
effect than HFpEF
11
Solomon et a;. EHJ 2016

www.escardio.org/guidelines
Heart Failure with mid-range Ejection Fraction (HFmrEF)
Justification for the introduction of HFmrEF
• Grey area between 40-50 %; HFpEF or HFrEF?• EF 40-49% different phenotype compared with EF>50%• Potentially differential treatment effects• “ Identifying HFmrEF as a separate group will stimulate
research into the underlying characteristics, pathophysiology and treatment of this group of patients”
12

www.escardio.org/guidelines
New Classification of Heart Failure
13

www.escardio.org/guidelines
Key Points
• Definition• New Classification HFrEF/HFpEF• Diagnosis of Heart Failure (general)
• (NT-pro)BNP cut-offs
• Diagnosis of HFpEF• Assessment of Diastolic Dysfunction
14
www.escardio.org/guidelines
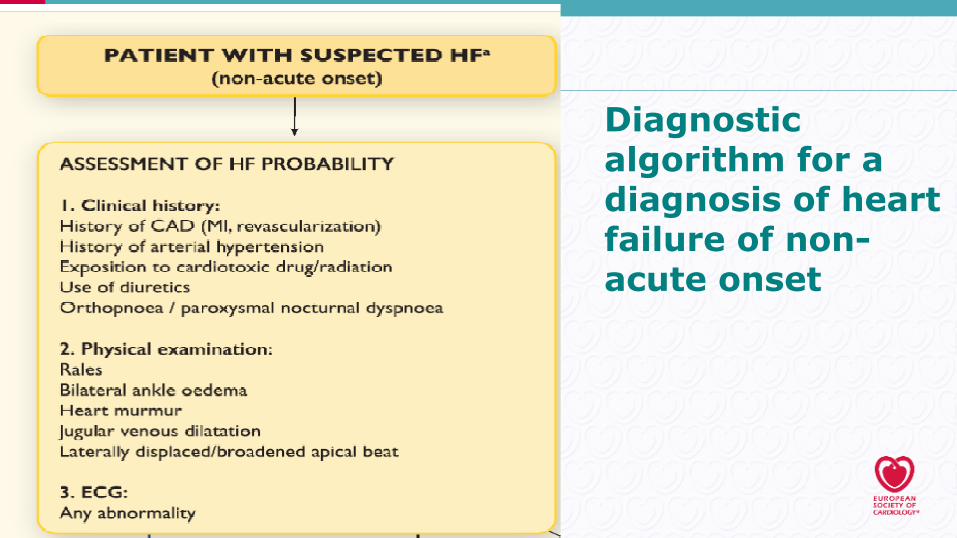
Diagnostic algorithm for a diagnosis of heart failure of non-acute onset

www.escardio.org/guidelines
Diagnostic algorithm for a diagnosis of heart failure of non-acute onset

www.escardio.org/guidelines
17
Natriuretic Peptides: cut-offs for EXCLUSION
Roberts E, et al.. BMJ 2015; Zaphiriou A, et al. Eur J Heart Fail 2005;Fuat A, et al. Br J Gen Pract 2006;Yamamoto K, et al. J Card Fail 2000;Cowie MR, et al. Lancet 1997; Krishnaswamy P, et al. Am J Med 2001;Kelder JC, et al. J Card Fail 2011.

www.escardio.org/guidelines
18
NT-proBNP cut-off in Non- Acute Setting
www.escardio.org/guidelines
Natriuretic Peptides: cut-offs for EXCLUSION
• “ At the mentioned exclusionary cut-points, the negative predictive values are very similar and high (0.94–0.98) in both the non-acute and acute setting, but the positive predictive values are lower both in the non-acute setting (0.44–0.57) and in the acute setting (0.66–0.67).54,56 – 61 Therefore, the use of NPs is recommended for ruling-out HF, but not to establish the diagnosis.”
19
www.escardio.org/guidelines
Key Points
• Definition• New Classification HFrEF/HFpEF• Diagnosis of Heart Failure (general)
• (NT-pro)BNP cut-offs
• Diagnosis of HFpEF• Assessment of Diastolic Dysfunction
20

www.escardio.org/guidelines
Definition
• HF is a clinical syndrome characterized by typical symptoms (e.g. breathlessness, ankle swelling and fatigue) that may be accompanied by signs (e.g. elevated jugular venous pressure, pulmonary crackles and peripheral oedema) caused by a structural and/or functional cardiac abnormality, resulting in a reduced cardiac output and/or elevated intracardiac pressures at rest or during stress.
21

www.escardio.org/guidelines
New Classification of Heart Failure
22

www.escardio.org/guidelines
Echocardiographic HFpEF/HFmrEF criteria for “structural and/or functional cardiac abnormality”
• How? Which parameters? Which cut-offs?
23
Paulus WJ, et al. Eur Heart J 2007; Dokainish H, et al. Eur J Echocardiogr 2011; Caballero L, et al. Eur Heart J Cardiovasc Imaging 2015. Lang RM, et al. Eur Heart J Cardiovasc Imaging 2015; Cohen GI, et al. J Am Coll Cardiol 1996; Gilman G, et al. J Am Soc Echocardiogr 2007; Nagueh SF, et al. Eur J Echocardiogr 2009; Nishimura RA, et al. J Am Coll Cardiol 1996; Ommen SR, et al. Circulation 2000;102:1788–1794.

www.escardio.org/guidelines
24
Diagnosis of HFpEF/HFmrEF
• Limited data (Unmet Need!)• Cut-offs arbitrary• More criteria; greater
certainty of diagnosis• Diastolic stress test?• Invasive hemodynamic
measurements?
HFpEF: EF≥50% HFmrEF: EF 40-49%
Signs (± symptoms) of HF
Structural abnormalities
Functional abnormalities
LAVI >34ml/m2
LVMI>115g/m2 (m) >95 g/m2 ( f )
E/e‘avg ≥ 13
e‘ average (lateral-septal) < 9 cm/s
+
+

www.escardio.org/guidelines
Conclusions: Diagnosis and new classification
• Definition: No symptoms, no heart failure• New Classification: Addition of HFmrEF• Diagnosis of Heart Failure: New diagnostic algorithm
• (NT-pro)BNP cut-offs for exclusion
• Diagnosis of HFpEF: structural (LAVI>34 mL/m2 or LVMI ≥115 g/m2 (m) ≥95 g/m2 (f) ) of functional (E/e′ ≥13 mean e’ < 9 cm/s) abnormalities
25









![[HF] FREEWEIGHT PRODUCTS - HOIST Fitness · [hf] flat bench hf-5163 [hf] 7-position folding f.i.d. bench hf-5167 new! warranty new! warranty [hf] 7-position f.i.d. olympic bench hf-5170](https://img.pdfslide.us/doc/110x75/5b5909d87f8b9ad0048c899a/hf-freeweight-products-hoist-fitness-hf-flat-bench-hf-5163-hf-7-position.jpg)







![EUCLID FINAL AHA LBCT 11-12-2016.pptx [Read-Only]clintrialresults.org/Slides/AHA2016/Patel_EUCLID.pdf · EUCLID Study Design Primary Endpoint: cardiovascular death, myocardial infarction,](https://img.pdfslide.us/doc/110x75/5fce124dcc1d01706c56c235/euclid-final-aha-lbct-11-12-2016pptx-read-only-euclid-study-design-primary-endpoint.jpg)












