Embed Size (px)
Citation preview

SHK 1 ®
Diagnosis and Management
of Shock
SHK 1 ®

SHK 2 ®
Objectives
• Identify the major types of shock and principles
of management
• Review fluid resuscitation and use of
vasopressor and inotropic agents
• Understand concepts of O2 supply and demand
• Discuss the differential diagnosis of oliguria
SHK 2 ®

SHK 3 ®
Shock
• Always a symptom of primary cause
• Inadequate blood flow to meet tissue
oxygen demand
• May be associated with hypotension
• Associated with signs of hypoperfusion:
mental status change, oliguria, acidosis
SHK 3 ®

SHK 4 ®
Shock Categories
SHK 4
• Cardiogenic
• Hypovolemic
• Distributive
• Obstructive
®

SHK 5 ®
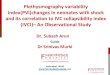
Cardiogenic Shock
• Decreased contractility
• Increased filling pressures,
decreased LV stroke work,
decreased cardiac output
• Increased systemic
vascular resistance –
compensatory

SHK 6 ®
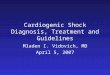
Hypovolemic Shock
• Decreased cardiac output
• Decreased filling pressures
• Compensatory increase in
systemic vascular resistance
SHK 6 ®

SHK 7 ®
Distributive Shock
• Normal or increased cardiac output
• Low systemic vascular resistance
• Low to normal filling pressures
• Sepsis, anaphylaxis, neurogenic,
and acute adrenal insufficiency
SHK 7 ®

SHK 8 ®
Obstructive Shock
• Decreased cardiac output
• Increased systemic vascular
resistance
• Variable filling pressures
dependent on etiology
• Cardiac tamponade, tension
pneumothorax, massive
pulmonary embolus

SHK 9 ®
Cardiogenic Shock Management
• Treat arrhythmias
• Diastolic dysfunction may
require increased filling
pressures
• Vasodilators if not hypotensive
• Inotrope administration

SHK 10 ®
Cardiogenic Shock Management
• Vasopressor agent needed if
hypotension present to raise
aortic diastolic pressure
• Consultation for mechanical
assist device
• Preload and afterload reduction
to improve hypoxemia if blood
pressure adequate

SHK 11 ®
Hypovolemic Shock
Management
• Volume resuscitation – crystalloid,
colloid
• Initial crystalloid choices
– Lactated Ringer’s solution
– Normal saline (high chloride may
produce hyperchloremic acidosis)
• Match fluid given to fluid lost
– Blood, crystalloid, colloid
SHK 11
®

SHK 12 ®
Distributive Shock Therapy
• Restore intravascular volume
• Hypotension despite volume therapy
– Inotropes and/or vasopressors
• Vasopressors for MAP < 60 mm Hg
• Adjunctive interventions dependent
on etiology
SHK 12 ®

SHK 13 ®
Obstructive Shock Treatment
• Relieve obstruction
– Pericardiocentesis
– Tube thoracostomy
– Treat pulmonary embolus
• Temporary benefit from fluid
or inotrope administration

SHK 14 ®
Fluid Therapy
• Crystalloids
– Lactated Ringer’s solution
– Normal saline
• Colloids
– Hetastarch
– Albumin
– Gelatins
• Packed red blood cells
• Infuse to physiologic endpoints
SHK 14
®

SHK 15 ®
Fluid Therapy
• Correct hypotension first
• Decrease heart rate
• Correct hypoperfusion abnormalities
• Monitor for deterioration of
oxygenation
SHK 15 ®

SHK 16 ®
Inotropic / Vasopressor Agents
• Dopamine
– Low dose (2-3 g/kg/min) – mild inotrope
plus renal effect (?)
– Intermediate dose (4-10 g/kg/min) –
inotropic effect
– High dose ( >10 g/kg/min) – vasoconstriction
– Chronotropic effect
SHK 16 ®

SHK 17 ®
Inotropic Agents
• Dobutamine
–5-20 g/kg/min
– Inotropic and variable chronotropic effects
–Decrease in systemic vascular resistance
SHK 17 ®

SHK 18 ®
Inotropic / Vasopressor
Agents
• Norepinephrine
–0.05 g/kg/min and titrate to effect
– Inotropic and vasopressor effects
–Potent vasopressor at high doses
SHK 18 ®

SHK 19 ®
Inotropic / Vasopressor Agents
• Epinephrine
–Both and actions for inotropic and
vasopressor effects
–0.1 g/kg/min and titrate
– Increases myocardial O2 consumption
SHK 19 ®

SHK 20 ®
Therapeutic Goals in Shock
• Increase O2 delivery
• Optimize O2 content of blood
• Improve cardiac output and
blood pressure
• Match systemic O2 needs with O2 delivery
• Reverse/prevent organ hypoperfusion

SHK 21 ®
Oliguria
• Marker of hypoperfusion
• Urine output in adults
<0.5 mL/kg/hr for >2 hrs
• Etiologies
–Prerenal
–Renal
–Postrenal
SHK 21 ®

SHK 22 ®
Evaluation of Oliguria
• History and physical examination
• Laboratory evaluation
–Urine sodium
–Urine osmolality or specific gravity
–BUN, creatinine
SHK 22 ®

SHK 23 ®
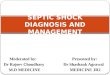
Evaluation of Oliguria
Laboratory Test Prerenal ATN
Blood Urea Nitrogen/ >20 10–20
Creatinine Ratio
Urine Specific Gravity >1.020 <1.010
Urine Osmolality (mOsm/L) >500 <350
Urinary Sodium (mEq/L) <20 >40
Fractional Excretion of Sodium (%) <1 >2

SHK 24 ®
Therapy in Acute Renal Insufficiency
• Correct underlying cause
• Monitor urine output
• Assure euvolemia
• Diuretics not therapeutic
• Low-dose dopamine may urine flow
• Adjust dosages of other drugs
• Monitor electrolytes, BUN, creatinine
• Consider dialysis or hemofiltration
SHK 24 ®

SHK 25 ®
Pediatric Considerations
• BP not good indication of hypoperfusion
• Capillary refill, extremity temperature better
signs of poor systemic perfusion
• Epinephrine preferable to norepinephrine due to
more chronotropic benefit
• Fluid boluses of 20 mL/kg titrated to BP or total
60 mL/kg, before inotropes or vasopressors
SHK 25 ®

SHK 26 ®
Pediatric Considerations
• Neonates – consider congenital
obstructive left heart syndrome (hypoplastic
left heart syndrome, AS, bicuspid aortic
valve, coartio aorta) as cause of obstructive
shock
• Oliguria
– <2 yrs old, urine volume <2 mL/kg/hr
– Older children, urine volume
<1 mL/kg/hr
SHK 26 ®

SHK 27 ®
Key Points