Embed Size (px)
Citation preview

Diabetic foot care: assessing theimpact of care on the whole patient
Monica Sutton*, Clare McGrath, Lesley Brady, John Ward
ABSTRACTThere is little doubt that provision of special care for people with diabetic foot ulcers reduces morbidity andamputation. Global efforts have been made to improve care for those who have or are prone to develop diabetic footulcers. However, equal to successful treatment and prevention is the need to understand how people feel about having afoot ulcer and its impact on their lifestyle. This information is important in choosing the optimum treatmentapproachÐone that is effective as well as acceptable to the patients themselves and their carers.Recent major advances in wound care research have resulted in new treatments for people with diabetic foot ulcers. It isimportant to understand how these treatments differ from traditional ones in the way they affect patient well-being.Because of the fears, emotions and worries frequently underlying a consultation concerning diabetic foot problems itcan be useful for clinicians to have access to a method of assessing these psychological issues in a systematic andcomprehensive manner. The assessment of health-related quality of life (HRQoL) is one such method that maycontribute to the evaluation of future foot ulcer treatments and care practices. Copyright # 2000 John Wiley & Sons,Ltd.
Practical Diabetes Int 2000: 17(5); 147±151
KEY WORDSulcer; health-related quality of life; treatment
IntroductionIt is estimated that foot ulcers affect15% of all patients with diabetesduring their lifetimes.1 The annualincidence of diabetic foot ulcers hasbeen reported to be 2.4±3%, andprevalence estimates in the UnitedStates range from 9.5 to 10.5%.2 Acommunity-based study in the UnitedKingdom showed that 5.3% of people
with type 2 diabetes had a current orprevious foot ulcer.3 Although thehealing rate may be as high as80±90%, the recurrence rate forneuropathic ulcers over a 3 yearfollow-up period was shown to be41%, and 70% over a 5 year period.4
Failure to follow good wound carepractices in managing diabetic footulcers can lead to infection, gangrene,hospitalisation, and amputation. Inthe United States, foot ulcers accountfor 6% of hospital admissions forpatients with diabetes and for 50%of all non-traumatic amputations.2
Approximately 6% of those withdiabetes undergo lower extremityamputation as a result of foot ulcers,5
and those who have had an amputa-tion have an increased chance ofrequiring another amputation.2 Thus,it is important for clinicians, patients,and caregivers to be aware of thepotential for individuals with diabetesto develop foot ulcers and to follow
established guidelines for preventionand care.
Quality of care in footulcer managementThe US Department of Health has setthe goal of achieving a 40% reductionin amputation rates among peoplewith diabetes by the year 2000.6 Thechallenge facing those involved at alllevels of foot care is how to achievethe best outcome with the mostef®cient use of limited resources.Effective clinical management of footulcers should span the stages ofscreening and prevention as well astreatment and follow-up. Each stagerequires its own set of indicators,mediating factors, and outcome mea-sures to aid decision making on theappropriate course of action. Both theclinical course and the success oftreatment may be assessed in terms ofthe morphology of the lesion, thedevelopment of complications, and
Monica Sutton, SRN, RSCN, RNT, HV Cert,
MSc, Lesley Brady, SRN, John Ward, MD,
FRCP, Diabetes Centre, Royal Hallamshire
Hospital, Shef®eld, UK
Clare McGrath, BSc (Hons), Mapi Values
Limited, Maccles®eld, Cheshire, UK
*Correspondence to:
Monica R. Sutton
Diabetes Nurse Specialist, Royal
Hallamshire Hospital, Glossop Road,
Shef®eld S10 2JF, UK.
Submitted: 24 June 1999
Accepted: 14 December 1999
O R I G I N A L A R T I C L E
Pract Diab Int July/August 2000 Vol. 17 No. 5 Copyright # 2000 John Wiley & Sons, Ltd. 147

the impact on the well-being ofpatients, caregivers, and society as awhole.
Table 1 summarises the structureswithin which foot care is provided, thedifferent processes of care, and theoutcomes of care. Successful treatmentusually involves choosing the combi-nation of process elements that is bestsuited to each patient, taking intoconsideration both clinical and psy-chological factors.
As early as 1984 Maxwell proposeda framework for evaluating quality ina system of continuous improve-ment.7 This framework of per-formance goals encompassed thespeci®c outcomes of care at a popula-tion and individual patient level aswell as the ef®ciency with whichthese goals should be met. Thesegoals could be considered whenassessing the provision of care forpeople with diabetic foot ulceration:
$ accessibility to all patients withinprimary and secondary settings
$ relevance in response to individualneeds for screening, education, andtreatment relative to foot care
$ effectiveness in reducing ulcerationand amputation
$ equity in the provision and avail-ability of foot care to all individuals
$ social acceptability and concern forthe overall well-being of the patientusing an integrated, whole-patientapproach
$ ef®ciency through appropriate orga-nisation of foot care in primary andsecondary settings.
Although current treatment practiceaims to achieve these goals, relativelylittle attention has been given toevaluating the impact of treatment onthe overall well-being of the patient.Such information is particularlyimportant at the present time, as newtreatments become available forpatients with lower extremity diabeticulcers. For example, therapies such asthe topical preparation of recombi-nant human platelet-derived growthfactor-BB8 and living skin equivalents9
show promise for the improved man-agement of diabetic ulcers in terms ofef®cacy and safety. The clinicianhowever needs to consider not onlythe ef®cacy and cost of the therapybut also its effect on the patient bothin terms of functional status and well-being. Patients with similar clinical®ndings may not respond to the sametreatment in similar ways, and thesedifferences in response may stem fromdifferences in patient health-relatedquality of life (HRQoL). HRQoL isa multi-dimensional concept describ-ing those aspects of people's lives thatare affected by disease or treatment.Consideration of QoL factors isimportant in maintaining a balancein care that ensures that ef®cacy is notattained at the expense of patient well-being.
Preventive measures such as patienteducation may also improve the out-comes of care by lowering ulcerincidence and recurrence rates. How-ever, for maximum effectiveness andcompliance, patient education should
be designed from a patient-centred,individually relevant, QoL perspective.
Measurement of HRQoLUnderstanding the overall impact of acondition and its treatment is achallenge that relies on the ability tode®ne and quantify the subjectivewell-being and functional capacity ofthe patient. In the past 10 years, thescienti®c standards and methods formeasuring HRQoL have improvedgreatly, leading to the increasing useand development of instruments formonitoring the health and well-beingof populations with different illnessesand for evaluating new treatments inclinical trials. HRQoL can be thoughtof as the patient's subjective assess-ment of his or her health, and can bemeasured on two levels, generic andspeci®c. Generic HRQoL encom-passes those physical, psychological,social, and general health perceptionsthat are affected by most diseases.Speci®c HRQoL refers to the aspectsof life functioning and well-being thatare affected by a given disease ortreatment.
There are now many reliableand validated toolsÐin the formof self-administered or interviewer-administered questionnairesÐfor mea-suring HRQoL. Of these, the mostwidely used generic tool is theShort Form-36 (SF-36),10 a modi®edversion of the questionnaire usedin the Medical Outcomes Study(MOS).11 The SF-36 contains 36questions covering eight QoL
Table 1. Care and treatment process
Structure Process Outcomes of foot care
$ Multidisciplinary foot care team$ Fast track foot clinics$ Community care$ Database of at risk feet from
annual review
$ Patient education$ Non-weight-bearing appliances/
orthotic footwear$ Wound debridement$ Infection control$ Choice of dressing and healing agents$ Vascular surgery$ Glycaemic control$ Amputation
$ Healing rates$ Amputation rates$ Clinical severity of ulcer$ Patient's functional status$ Health-related quality of life$ Disability/bed days$ Work loss$ Health care resource utilisation$ Ulcer incidence/prevalence$ Recurrence rates
O R I G I N A L A R T I C L E
Care of diabetic foot ulcers
148 Pract Diab Int July/August 2000 Vol. 17 No. 5 Copyright # 2000 John Wiley & Sons, Ltd.

domains, asking patients to rate theirphysical health, psychological health,social and role functioning, bodilypain, vitality, and general health.Higher scores indicate better overallhealth. Because the questions apply toQoL indices associated with disease ingeneral, the SF-36 allows comparisonof self-reported health across disparateconditions, and it has been used inmany patient populations. Diabetes-speci®c instruments in use includethe Diabetes Quality-of-Life Measure,the Diabetes Health Pro®le, and theType 2 Diabetes Symptom Check-list.12±14
HRQoL in people withdiabetesHRQoL is compromised in peoplewith diabetes. In the MOS,11 theresponses of 844 patients with dia-betes were compared with those of2595 patients without chronic condi-tions, using the SF-20, a shortenedform of the SF-36. The SF-20 consistsof 20 questions representing six healthconcepts: (i) physical functioning, (ii)role functioning, (iii) social function-ing, (iv) mental health, (v) healthperceptions, and (vi) pain.15 Patientswith diabetes had signi®cantly lowerscores in all areas except for mentalhealth. Using the SF-20, Glasgow andcolleagues found lower QoL scores inall areas including mental health in apopulation of 2056 patients withdiabetes, compared with diabetes-speci®c norms from the MOS.16
Lower scores in that study werethought to be related to a largernumber of complications reported inthe group of patients with diabetesthan that in the group with diabetessurveyed in the MOS, giving furthersupport to the concept that quality oflife decreases in relation to thenumber of complications.
Treatment protocols have also beenevaluated in terms of their effects onQoL in patients with diabetes. Theeffect of controlling glucose concen-trations with intensive treatmentversus conventional treatment onQoL in patients with type 1 diabeteswas determined as part of the Diabetes
Control and Complications Trial(DCCT).12 This study used threedifferent instruments to evaluateQoLÐthe Diabetes Quality-of-LifeMeasure (disease speci®c), the Symp-tom Checklist-90R (a generic measureof psychiatric symptoms), and the SF-36 (generic)Ðbecause no singleinstrument is recognised as the stand-ard for measuring the effects oftreatment on QoL in patients withdiabetes. Although no comparisonswere made with a control population,no signi®cant differences in QoL werefound between treatment groups.These ®ndings that intensive treat-ment to control glycemia did notlower patient QoL signi®cantly fromthat seen with conventional treatmentprovide important information forclinicians to consider when planningpatient therapy.
Patients in the studies describedabove were not divided into subgroupsfor the evaluation of the effects ofspeci®c disease complications onHRQoL. In patients with diabeteswho have foot ulcers or a history offoot ulcers, other major complicationsof diabetes and other signi®cantcardiovascular or cerebrovascular dis-eases are often also present. Thus, theoverall health and QoL of thesepatients is likely to be lower than
that of patients with diabetes ingeneral, and this may complicate footulcer management. In a UK study,17
the self-reported health of people withdiabetes was measured using the SF-36. Patients evaluated were those withfoot ulcers, those who had a history offoot ulcers, and those with no historyof foot ulcers. Patients with foot ulcershad the lowest QoL scores, whilethose with healed foot ulcers had apro®le between that of the currentulcer patients and those with nohistory of a foot ulcer. The scoreswere signi®cantly different among thethree groups for the domains ofphysical health, role physical, andbodily pain (p<0.01) (Figure 1).
QoL issues speci®c topeople with diabetic footulcersRecent studies involving interviewswith patients with diabetic foot ulcersand their caregivers have alloweddescriptive information to be gatheredon the impact of foot ulcers and theirtreatment on QoL. It has been shownthat the non-weightbearing regimenscommonly used for treating footulcers have a deleterious effect onQoL.18 Such regimens require a lossof mobility to be effective, causingpatients to be restricted in their daily
Figure 1. Pro®les from the SF-36 for patients with no current ulcers, patients with currentulcers, and patients with healed ulcers, together with a normative diabetic population (datafrom McGrath et al.17)
O R I G I N A L A R T I C L E
Care of diabetic foot ulcers
Pract Diab Int July/August 2000 Vol. 17 No. 5 Copyright # 2000 John Wiley & Sons, Ltd. 149
lives. Because patients often rely onothers for help with foot care, restric-tions may also be placed on the dailyactivities, leisure pursuits, and socialinteractions of caregivers. Relation-ships may become strained, andpatients can feel isolated and aburden to others. Such frustratingsituations can lead to non-compliance,which may result in prolonged orrecurring ulcers and associated distressand concern about whether healingwill ever take place. These issues arevery speci®c to patients with footulcers and have not previously beenconsidered in questionnaires to evalu-ate treatments. Thus, it will beimportant to assess new treatments inthis context. This will require reliable,valid instruments to measure treat-ment impact on the patient's lifestyle,ability to function, and emotionalwell-being.
The Diabetic Foot Ulcer Scale(DFS) is a new questionnaire that hasbeen developed to measure the speci®cfactors affecting people's lives as aresult of having foot ulcers.17 TheDFS includes the following domains:leisure, physical health, daily activities,emotions, non-compliance, family,friends, treatment, satisfaction, posi-tive attitude, and ®nancial. The DFSwas used in the psychometric portionof the UK study by McGrath and
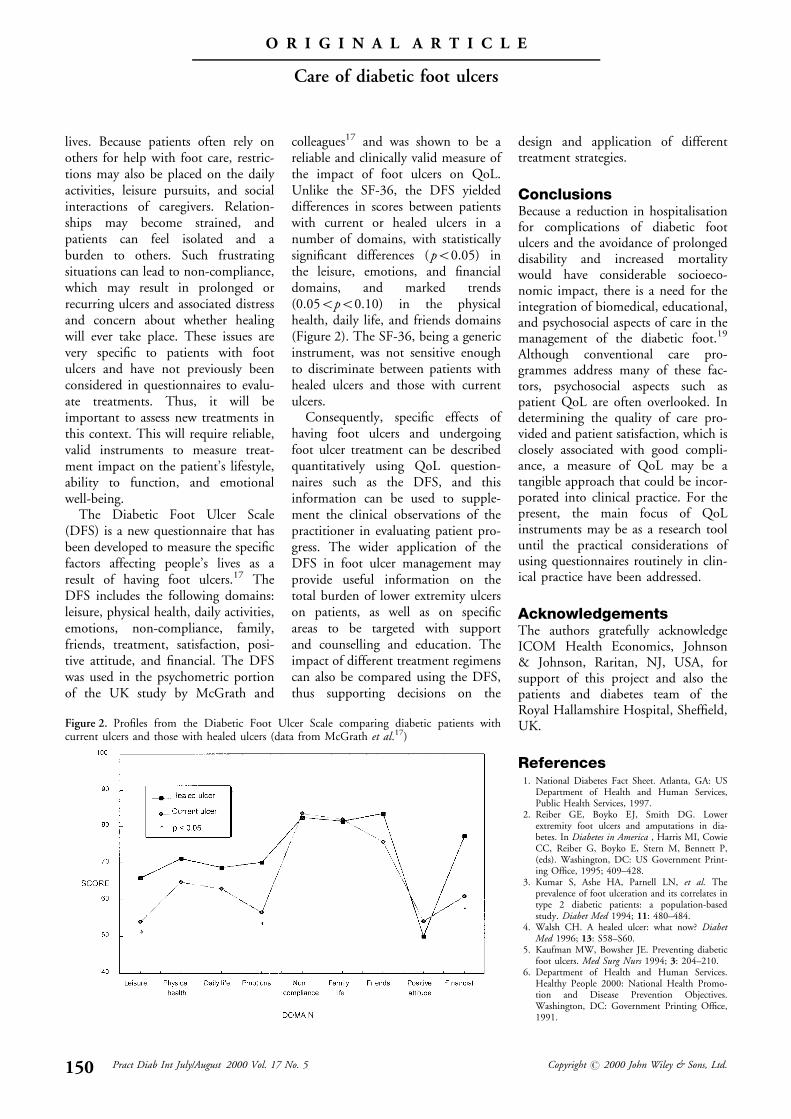
colleagues17 and was shown to be areliable and clinically valid measure ofthe impact of foot ulcers on QoL.Unlike the SF-36, the DFS yieldeddifferences in scores between patientswith current or healed ulcers in anumber of domains, with statisticallysigni®cant differences ( p<0.05) inthe leisure, emotions, and ®nancialdomains, and marked trends(0.05<p<0.10) in the physicalhealth, daily life, and friends domains(Figure 2). The SF-36, being a genericinstrument, was not sensitive enoughto discriminate between patients withhealed ulcers and those with currentulcers.
Consequently, speci®c effects ofhaving foot ulcers and undergoingfoot ulcer treatment can be describedquantitatively using QoL question-naires such as the DFS, and thisinformation can be used to supple-ment the clinical observations of thepractitioner in evaluating patient pro-gress. The wider application of theDFS in foot ulcer management mayprovide useful information on thetotal burden of lower extremity ulcerson patients, as well as on speci®careas to be targeted with supportand counselling and education. Theimpact of different treatment regimenscan also be compared using the DFS,thus supporting decisions on the
design and application of differenttreatment strategies.
ConclusionsBecause a reduction in hospitalisationfor complications of diabetic footulcers and the avoidance of prolongeddisability and increased mortalitywould have considerable socioeco-nomic impact, there is a need for theintegration of biomedical, educational,and psychosocial aspects of care in themanagement of the diabetic foot.19
Although conventional care pro-grammes address many of these fac-tors, psychosocial aspects such aspatient QoL are often overlooked. Indetermining the quality of care pro-vided and patient satisfaction, which isclosely associated with good compli-ance, a measure of QoL may be atangible approach that could be incor-porated into clinical practice. For thepresent, the main focus of QoLinstruments may be as a research tooluntil the practical considerations ofusing questionnaires routinely in clin-ical practice have been addressed.
AcknowledgementsThe authors gratefully acknowledgeICOM Health Economics, Johnson& Johnson, Raritan, NJ, USA, forsupport of this project and also thepatients and diabetes team of theRoyal Hallamshire Hospital, Shef®eld,UK.
References1. National Diabetes Fact Sheet. Atlanta, GA: US
Department of Health and Human Services,Public Health Services, 1997.
2. Reiber GE, Boyko EJ, Smith DG. Lowerextremity foot ulcers and amputations in dia-betes. In Diabetes in America , Harris MI, CowieCC, Reiber G, Boyko E, Stern M, Bennett P,(eds). Washington, DC: US Government Print-ing Of®ce, 1995; 409±428.
3. Kumar S, Ashe HA, Parnell LN, et al. Theprevalence of foot ulceration and its correlates intype 2 diabetic patients: a population-basedstudy. Diabet Med 1994; 11: 480±484.
4. Walsh CH. A healed ulcer: what now? DiabetMed 1996; 13: S58±S60.
5. Kaufman MW, Bowsher JE. Preventing diabeticfoot ulcers. Med Surg Nurs 1994; 3: 204±210.
6. Department of Health and Human Services.Healthy People 2000: National Health Promo-tion and Disease Prevention Objectives.Washington, DC: Government Printing Of®ce,1991.
Figure 2. Pro®les from the Diabetic Foot Ulcer Scale comparing diabetic patients withcurrent ulcers and those with healed ulcers (data from McGrath et al.17)
O R I G I N A L A R T I C L E
Care of diabetic foot ulcers
150 Pract Diab Int July/August 2000 Vol. 17 No. 5 Copyright # 2000 John Wiley & Sons, Ltd.
7. Maxwell RJ. Quality assessment in health. BMJ1984; 288: 1470±1472.
8. Wieman TJ, Smiell JM, Su Y. Ef®cacy and safetyof a topical gel formulation of recombinanthuman platelet-derived growth factor-BB (beca-plermin) in patients with chronic neuropathicdiabetic ulcers: a phase III., randomized., pla-cebo-controlled., double-blind study. DiabetesCare 1998; 21: 822±827.
9. Sorenson JC. Living skin equivalents and theirapplication in wound healing. Clin Podiatr MedSurg 1998; 15: 129±137.
10. McHorney CA, Ware JEJ, Raczek AE. TheMOS 36-Item Short-Form Health Survey (SF-36): II. Psychometric and clinical tests of validityin measuring physical and mental health con-structs. Med Care 1993; 31: 247±263.
11. Stewart AL, Green®eld S, Hays RD, et al.Functional status and well-being of patientswith chronic conditions. Results from theMedical Outcomes Study [published erratumappears in JAMA 1989; 262 (18): 2542]. JAMA1989; 262: 907±913.
12. Diabetes Control and Complications TrialResearch Group. In¯uence of intensive diabetestreatment on quality-of-life outcomes in theDiabetes Control and Complications Trial.Diabetes Care 1996; 19: 195±203.
13. van der Does FEE, de Neeling JND, Snoek FJ,et al. Symptoms and well-being in relation toglycemic control in type II diabetes. DiabetesCare 1996; 19: 204±210.
14. Vaughn NJA. Measuring the outcomes ofdiabetes care. Diabet Med 1994; 11: 418±423.
15. Stewart AL, Hays RD, Ware JEJ. The MOSshort-form general health survey. Reliability andvalidity in a patient population. Med Care 1988;26: 724±735.
16. Glasgow RE, Ruggiero L, Eakin EG, et al.Quality of life and associated characteristics in alarge national sample of adults with diabetes.Diabetes Care 1997; 20: 562±567.
17. Data on ®le. Mapi Values, Maccles®eld,Cheshire, UK.
18. Brod M. Quality of life issues in patients withdiabetes and lower extremity ulcers: patients andcaregivers. Qual Life Res 1998; 7: 365±372.
19. Edmonds ME, van Acker K, Foster AVM.Education and the diabetic foot. Diabet Med1996; 13 (suppl): S61±S64.
C O N F E R E N C E N O T I C E
FENDFederation of European Nurses in Diabetes
Fifth Annual Conference, ‘Education – 2000 and Beyond’14–15 September 2000, Jerusalem, Israel
Details: Stina Wallenkrans, PL 9747 Husebacken, S-44497 Svenshogen, Sweden. Tel/Fax: +46 303 774 111, or, MrsAnne-Marie Felton, 24 Holmesdale Avenue, London, SW14 7BQ. Fax: +44 (0)208 255 9169; E-mail: [email protected]
C O N F E R E N C E N O T I C E
‘‘NEW HORIZONS IN INSULIN PUMP THERAPY’’One day Symposium for Diabetologists and Diabetes Nurse Specialists on the current status of
Continuous Subcutaneous Insulin Infusion in diabetes careFriday, 8 December 2000, The Mayfair InterContinental Hotel, London W1
Supported by an educational grant by Disetronic Medical Systems LtdOrganising Chairman: Professor Ken Shaw MA MD FRCP
Programme$ Historical perspective on pumps * Pharmacokinetics * Insulin analogues and pumps *
$ Complications and safety profile * Psychological and quality of life aspects *$ Pumps and children * Patient selection * Organising and running a pump service *
$ Case studies * Resources and funding (patient and professional) *
Applications: There is no delegate fee for this Symposium and there are a limited number of places available. Delegate tickets willbe offered on a first come, first served basis. Please apply for further details and Application Form to:
Practical Diabetes Conferences, c/o Millbrook Medical Conferences Ltd, Suite Thirteen, Devonshire House,Bank Street, Lutterworth LE17 4AG.
Tel 01455 552559 Fax 01455 550098 E-mail: [email protected]
O R I G I N A L A R T I C L E
Care of diabetic foot ulcers
Pract Diab Int July/August 2000 Vol. 17 No. 5 Copyright # 2000 John Wiley & Sons, Ltd. 151