Embed Size (px)
Citation preview

Doc: PHDDMWKB.15 Version: 1 Issued: Dec 2015 Page 1 of 25
Diabetes management workbook
Premium Health First Aid and Specialised Health Solutions
PO Box 7072, Brighton Vic 3185 Phone: 1300 72 12 92
Fax: 03 9596 1766 Email: [email protected]
www.premiumhealth.com.au
RTO No. 104032 ACN 060 000 017 | ABN 24 692 649 946
© Premium Health 2015
Publisher
This book is copyright. Apart from any fair dealings for purposes of private study, criticism or review, as permitted under the Copyright Act, no part may be reproduced by any process without written permission. Enquiries should be made to the publisher.

Diabetes management workbook
Doc: PHDDMWKB.15 Version: 1 Issued: Dec 2015 Page 2 of 25
Table of contents Training and assessment information ................................................................................................................... 3 Diabetes .............................................................................................................................................................. 4
Cause of diabetes .......................................................................................................................................................... 4 Classification of diabetes ............................................................................................................................................... 5 Treatment medication ................................................................................................................................................... 6 Blood glucose levels....................................................................................................................................................... 8 Glycosylated haemoglobin (HbA1c) test ....................................................................................................................... 9 Hypoglycaemia .............................................................................................................................................................. 9 Hyperglycaemia ........................................................................................................................................................... 10 Ketoacidosis ................................................................................................................................................................. 10 Hyperglycaemic Hyperosmola Syndrome (HHS) ......................................................................................................... 11 Steroids and Diabetes .................................................................................................................................................. 11 Sick day management plan .......................................................................................................................................... 11 Complications of Diabetes ........................................................................................................................................... 12 Diabetic ulcers ............................................................................................................................................................. 13 Kidney failure ............................................................................................................................................................... 14 Eye complications ........................................................................................................................................................ 14
Nutrition ............................................................................................................................................................ 15 Healthy weight range, waist circumference and BMI ................................................................................................. 17
Importance of exercise ....................................................................................................................................... 18 Lifestyle changes ................................................................................................................................................ 19 Team management of diabetes .......................................................................................................................... 19 Diabetes references and resources ..................................................................................................................... 21 Notes ................................................................................................................................................................. 22 Appendices ........................................................................................................................................................ 23
Appendix 1 – Blood Glucose/Ketone Monitor Operation ........................................................................................... 23 Appendix 2 – Baker IDI Nutritional plate model .......................................................................................................... 25

Diabetes management workbook
Doc: PHDDMWKB.15 Version: 1 Issued: Dec 2015 Page 3 of 25
Training and assessment information Welcome Welcome to your course and Premium Health. The aim of this resource is to provide the essential knowledge and skills you require to effectively manage residents with diabetes. Helping you to succeed in your course We believe learning should be an enjoyable and challenging process and we understand that each learner is different. A variety of methods such as class participation, group discussion, scenarios, workbook exercises and opportunities for practice will help you to achieve Work Ready status. We select our Premium Health trainers and assessors carefully. All are nurses or paramedics with appropriate qualifications, technical expertise and experience in both education and emergency first aid and in the disability or health care sector. This enables them to provide you with quality training which is grounded in experience and knowledge of the field. Performance outcomes On completion of this course you will be able to:
• Describe the classification of diabetes and its medical management • Identify the signs, symptoms and first aid management of Hyperglycaemia • Identify the signs, symptoms and first aid management of Hypoglycaemia • Describe the common complications of diabetes • Explain the main function of glucose in the body • Describe the function of Insulin • Identify common diabetic medications • Identify risk factors for developing Diabetes • Demonstrate blood glucose monitoring
Statement of Participation A Statement of Participation will be issued upon successful achievement of the assessment tasks in this non-accredited course. Evaluation of the course A student feedback form is provided at the back of the workbook. Your feedback is important to us as we use this as part of our continuous improvement cycle. Please complete the form at the end of your course. Premium Health’s customer service We offer you an on-going service in relation to course information and invite you to call our office on 1300 72 12 92 or email us on [email protected]. For more information about Premium Health specialised health and first aid courses, products, services and policies, access our website www.premiumhealth.com.au

Diabetes management workbook
Doc: PHDDMWKB.15 Version: 1 Issued: Dec 2015 Page 4 of 25
Diabetes Diabetes mellitus is a condition where there is too much glucose (sugar) in the blood. Currently nearly 1 million Australians have this disease, a figure which has doubled since the 1990’s. The body is like an engine, with glucose being the main and most efficient fuel the body uses to generate its energy. To provide this energy, the sugar from the food we eat is transformed into glucose. Glucose travels in the blood and is delivered to the cells with the help of a substance called insulin. Insulin is a hormone produced by the pancreas and it allows for the body to be able to use glucose for energy. Diabetes interrupts this process in various ways depending on the type of diabetes a person has. When there is no insulin or when insulin doesn't work effectively, glucose remains in the blood stream, blood glucose levels (BGLs) become too high and diabetes results. Diabetes mellitus is a chronic condition which can result in disability or early death. Management of the condition involves the person with diabetes actively managing their condition by controlling blood glucose levels, having an appropriate diet balanced by exercise and with the support and consultation of a therapeutic team which involves their doctor, specialist physician, diabetes educator, dietician, podiatrist and eye specialist. The aim of good diabetes management as stated by the Royal Australian College of General Practitioners is:
• Improvement in the duration and quality of life of patients • Encouraging patients to participate and take an active role in the management of their diabetes • To ensure that all other preventative health care activities are included while maintaining good diabetes
health care. Cause of diabetes In diabetes, either the pancreas no longer makes insulin (type 1 diabetes), or the cells don’t respond to the insulin properly (insulin resistance) or the pancreas produces inadequate insulin for the body’s increased needs (type 2 diabetes). Insulin carries glucose through cell walls into cells to be used as energy. After eating, the blood glucose level rises, which triggers a release of insulin which moves glucose into the cells and blood glucose levels (BGLs) fall.
Source: John Hopkins Medicine

Diabetes management workbook
Doc: PHDDMWKB.15 Version: 1 Issued: Dec 2015 Page 5 of 25
Classification of diabetes Diabetes is classified as:
1) Type 1 diabetes 2) Type 2 diabetes 3) Gestational diabetes and 4) Pre-diabetes.
Treatment goals include:
• Attain and maintain optimal BGLs, usually between 4.0 – 6.0mmol/L (fasting). • Attain and maintain optimal HbA1c <7% • Reduce cardiovascular risk • Achieve weight control • Encourage self-monitoring and management • Physical exercise - At least 30 minutes walking (or equivalent) 5 or more days/week (Total ≥150
minutes/week) Type 1 diabetes Type 1 diabetes was previously known as Insulin Dependent Diabetes (IDDM) or Juvenile onset diabetes. In Type 1 diabetes the body cannot make its own insulin. The immune system of a person with type 1 diabetes attacks the insulin-producing cells of the pancreas. Type 1 diabetes can occur at any point in life, but most commonly develops in childhood or the teen years. This type of diabetes cannot be prevented. In Australia, it affects 1 in 10 people, approximately 129 000 people. Type 1 diabetes requires insulin for survival. Currently this is best achieved via injection. Type 2 diabetes Type 2 diabetes was previously known as Non-Insulin Dependent Diabetes (NIDDM) or Maturity Onset Diabetes. It is a chronic condition where the body produces insulin but cells of the body become less responsive to that insulin. This is often referred to as insulin resistance. Excess weight, particularly around the waist, contributes to insulin resistance. 90% of people diagnosed with diabetes have Type 2 diabetes. It usually develops later in life, but it can affect all ages. Lifestyle changes can delay the need for medication to stabilise blood glucose levels. Risk factors for Type 2 diabetes include:
• Pre-diabetes • Overweight • Aboriginal or Torres Strait Islander over 35 years old • Older than 45 year, close relative with type 2 diabetes • Previous gestational diabetes
Gestational diabetes This is a temporary form of diabetes that occurs during pregnancy. During pregnancy the body must produce 2-3 times the normal amount of insulin. If the mother cannot produce that much insulin, or if she is insulin resistant, her blood glucose levels will rise. It affects between 5% and 8% of pregnant women. In Australia, about 15 000 women develop gestational diabetes every year. Once the baby is born the need for insulin drops and symptoms usually disappear. Having gestational diabetes means both the mother and the child have a higher risk of developing type 2 diabetes later in life.

Diabetes management workbook
Doc: PHDDMWKB.15 Version: 1 Issued: Dec 2015 Page 6 of 25
Pre-diabetes Pre-diabetes is a condition in which blood glucose levels are higher than normal, although not high enough to cause diabetes. Pre-diabetes has no symptoms, but has a range of risk factors including obesity, smoking, heart disease, polycystic ovarian syndrome and high blood pressure. Without treatment, about one in three people with pre-diabetes will develop type 2 diabetes. Treatment medication Insulin Everyone with Type 1 diabetes needs to use insulin to keep their blood glucose levels as normal as possible. Insulin may also be required to help manage type 2 diabetes when diabetes tablets, together with healthy eating and regular physical activity, are not enough to keep blood glucose levels within the recommended target range. Insulin must be taken by injection. It cannot be taken orally because it is destroyed by the digestive chemicals in the stomach. Insulin types There are 5 types of insulin ranging from short to long acting. Often people need varying amounts of both short and longer acting insulin. 1. Rapid onset – fast acting insulin
• Clear in appearance and start to work within 1 - 20 minutes • Peak time is 1 hour and lasts 3 - 5 hours • Examples: NovoRapid®, Humalog®, Apidra® • Very important to eat immediately after injecting
2. Short acting insulin
• Clear in appearance, works within half an hour, so need to have injection half an hour before eating • Peak time is 2- 4 hours and lasts for 6 - 8 hours • Examples: Actrapid®, Humulin®R and Hypurin® Natural (beef)
3. Intermediate acting insulin
• Cloudy in appearance, works within 1 ½ hours • Peak around 4-12 hours and lasts for 16-24 hours • Examples: Protaphane®, Humulin® NPH, Hypurine Isophane® (beef)
4. Mixed insulin
• Cloudy in appearance (contain pre-mixed combinations of either rapid onset or short acting) • Examples: NovoMix® 30 (30% insulin aspart and 70% Protamine crystallised insulin aspart), Humalog® mix 25
(25% Insulin lispro, 75% insulin lispro Protamine suspension), Humalog® mix 50 (50% Insulin lispro, 50% insulin lispro Protamine suspension)
• Types of mixed insulins containing a short acting insulin currently available are: Mixtard®30/70, Mixtard®50/50 and Humulin®30/70
5. Long acting insulin
• Clear in appearance (injected once or twice daily injection lasting up to 24 hours) • Provide“Basal or background insulin”. Needs to be supplemented with short or rapid onset-fast acting in
Type 1 diabetics. • Examples: Lantus® (insulin glargine) and Levermir® (insulin detemir)
Methods of insulin administration
• Injection with an insulin pen • Insulin pump • Injection with a needle and syringe
Insulin pens make injecting simpler and more convenient. Some insulin pens are disposable and come pre-filled with insulin. Other pens are reusable and have a small cartridge that can be replaced. All insulin pens use disposable

Diabetes management workbook
Doc: PHDDMWKB.15 Version: 1 Issued: Dec 2015 Page 7 of 25
needles, which should be changed after each use. Reusable insulin pens are used with 3ml insulin cartridges. Each cartridge contains 300 units of insulin. Insulin pens are made to fit specific brands of insulin. They are not interchangeable. Disposable insulin pen devices are prefilled with 300 units of insulin and discarded when empty. Reusable pens – NovoPen 4, NovoPen 3 Demi, HumaPen Luxura, HumaPen Luxura HD, HumaPen Memoir, ClikSTAR Disposable pens – FlexPen, InnoLet, KwikPen, SoloStar Insulin pumps are battery operated devices that deliver a continuous small dose of insulin with extra insulin given with meals. They hold a reservoir of insulin that can be programmed to deliver different insulin doses throughout the day. A thin tube brings the insulin to a plastic cannula, which is placed under the skin. The cannula may be kept in place for up to 3 days. Syringes may be used if two types of insulin need to be mixed in special amounts. Syringes come in 0.3 ml (30 units), 0.5 ml (50 units) and 1ml (100 units) sizes. Syringes and needles are made to be used only once and then discarded. Insulin is injected through the skin into the subcutaneous layer (fatty tissue) – most suitable sites are generally those indicated below. The tummy or abdomen absorbs insulin the fastest and is the site used by most people.
www.diabeteskidsandteens.com.au
Type 2 diabetes People with Type 2 diabetes are often given tablets (oral hypoglycaemics) to help control their blood glucose levels. These tablets are not an oral form of insulin. This medication aims to increase the sensitivity of target organs to insulin and decrease the rate at which glucose is absorbed from the gastrointestinal tract. It is used in conjunction with healthy eating and regular physical activity. In Australia there are seven classes of medicines used to treat Type 2 diabetes.
1) Biguanides (Metformin) • They help to lower BGL’s by reducing the amount of stored glucose released by the liver, slowing the
absorption of glucose from the gut and helping the body to become more sensitive to insulin
2) Sulphonylureas (Gliclazide, Glibenclamide, Glipizide, Glimepiride) • They lower BGL’s by stimulating the pancreas to release more insulin • They can course hypoglycaemia
3) Thiazolidinediones (glitazones) • They help to lower blood glucose levels by increasing the effect of the insulin, especially on muscle and fat
cells (they aim to improve insulin resistance) • Their effect is slow, taking days to weeks to begin working and one to two months for their full effect
4) Alpha glucosidase inhibitor (Acarbose)
They help to slow down the digestion and absorption of certain dietary carbohydrates in the gut.
5) DPPP-4 inhibitors (Linagliptin, Saxagliptin, Sitagliptin, Vildagliptin) • They work by inhibiting the enzyme DPP-4. This enhances the levels of active incretin hormones which
act to lower blood glucose levels by increasing insulin secretion and decreasing glucagon secretion.

Diabetes management workbook
Doc: PHDDMWKB.15 Version: 1 Issued: Dec 2015 Page 8 of 25
6) Incretin mimetics (Exenatide) • New class of drug used to treat type 2 diabetes. Given by injection. • Help to lower blood glucose levels by:
- Stimulating the pancreas to release insulin – but only when blood glucose levels are high - Reducing the amount of glucose released into the bloodstream by the liver. - Slowing down gastric emptying - Helping to feel full and reducing appetite
7) Sodium-glucose transporter (SGLT2) inhibitors (Canagliflozin, Dapagliflozin) • New class of oral drugs • Lowers blood glucose levels by decreasing the amount of glucose that is reabsorbed from the kidneys so
that it goes out through the urine rather than staying in the blood. Blood glucose levels No matter the type of diabetes, tracking blood glucose levels is the key to managing the condition. Blood glucose levels can be tested with a drop of blood obtained by pricking the finger with a sharp needle, or as part of an oral glucose tolerance test ordered by a doctor. The aim is to maintain as close to normal blood glucose levels as possible. Blood glucose tests are usually done before meals or two hours after meals. It is recommended, that those with diabetes regularly monitor their blood glucose levels. Over time the reading will provide valuable information to determine the best management strategies for that individual. Regular testing of BGLs assists in adjustment of medication dosages to best manage the diabetes. Maintaining good blood glucose control is the best defence to reduce the chances of developing complications from diabetes. Blood glucose targets Before a meal After a meal
Type 1 diabetes 4-6.7 mmol/L 5-10 mmom/L
Type 2 diabetes 6.1-8 mmol/L 6-10 mmol/L
Gestational 4-5.5 mmol/L 4-7 mmol/L
Accurate blood glucose results depend on:
• The machine working properly • Doing the test correctly • Using strips which are in date and undamaged • Calibrating the machine
These may be checked by doing a control test with a special solution. Common reasons for incorrect results:
• Using the wrong strip or strips that have expired or have been stored incorrectly • Not washing hands before testing (handling sweet foods such as jam or fruit can give higher results) • Incorrect calibration or set up • Not enough blood on the strip – this will give lower results with some machines
BGLs should be tested more often when:
• The person is sick – increase frequency of testing to 2 - 4 hourly • When adjusting tablet or insulin doses or • When blood glucose levels are high, for example - over 15 mmol/l

Diabetes management workbook
Doc: PHDDMWKB.15 Version: 1 Issued: Dec 2015 Page 9 of 25
Glycosylated haemoglobin (HbA1c) test The HbA1c test shows an average of a person’s blood glucose level over the past 10-12 weeks and should be arranged by their doctor every 3-6 months. The HbA1c test does not replace the BGL testing but is used as an added tool in giving the overall picture of blood glucose management. An HbA1c test is possible because red blood cells are continuously being made by the long bones of the body and released into circulation. When these cells are released, they pick up glucose in the blood stream at that time. Each red blood cell lasts about 120 days. Therefor any blood sample will have a range of cells released over the previous 120 days with different amounts of glucose attached. The HbA1c test gives a good guide to the average. In general, people with all types of diabetes should try to keep their HBA1c numbers below 7%. Hypoglycaemia Means “low blood glucose” and is often referred to as a “Hypo”. It occurs when the blood glucose level drops to less than 4mmol/L or when symptoms are being experienced at a level close to 4mmol/L. Signs & symptoms
• Feeling shaky or nervous • Pounding heart • Rapid pulse • Sweating • Chills • Feeling irritable • Headache • Hunger • Weakness • Tingling or numbness in lips or tongue • Confusion or lack of concentrations
If left untreated, hypoglycaemia may lead to fainting or seizures. Possible causes
• Insufficient food or delayed meals or snacks • Excess insulin or diabetes tablets taken • Alcohol consumed without food or in excessive amounts • Extra physical activity without sufficient carbohydrate or insulin adjustment
Treatment for hypoglycaemic episode If conscious Give:
a sugary drink - e.g. 100mls Lucozade or Lemonade, or 6-8 large jelly beans
Then: Check blood glucose levels & repeat in 5–10 mins Follow with a carbohydrate snack e.g. fruit, sandwich or glass of milk
Repeat BGLs until levels improve Seek medical aid if required If unconscious Manage using first aid priority action plan:
DRSABCD – position on side (nil by mouth) Stay with casualty until medical aid arrives

Diabetes management workbook
Doc: PHDDMWKB.15 Version: 1 Issued: Dec 2015 Page 10 of 25
Hyperglycaemia Means there is an excessively high blood glucose level. Over the long term, hyperglycaemia can lead to diabetic neuropathy, cystitis, kidney damage and possibly ketoacidosis. Signs & symptoms
• Thirsty • Hungry • Need to frequently urinate • Extremely tired • Nauseated • Blurred vision • Flushed red face
Possible causes
• Emotional Stress • Change in other medications (e.g. cortisone can raise BGLs) • Wrong or missed dose of insulin or tablets • Insufficient daily exercise • Changes to eating pattern • Other illness - urinary tract infections, throat infections, or chest infections will cause a rise in BGLs
Treatment for hyperglycaemic episode
• Test BGLs frequently • If hyperglycaemia persists, contact doctor so treatment can be reviewed – identify cause/initiate treatment
e.g. medication change • Send for medical help if:
o Vomiting stops them from drinking and makes eating difficult o Blood glucose levels remain high o Moderate to large ketones are present in the urine
For Type 2 diabetes it is normal for blood glucose levels to go up and down throughout the day. An occasional high blood glucose level is not a problem. But if the blood glucose level remains above 15 mmol/L for more than 12 hours contact the doctor or Diabetes Educator. If a blood glucose level reads 20 mmol/L or above contact the doctor immediately or the Diabetes Educator. In type 1 diabetes, high blood glucose levels can progress to a serious condition called Ketoacidosis. Ketoacidosis Ketoacidosis is a serious condition associated with illness or very high blood glucose levels in type 1 diabetes. It develops gradually over hours or days. It is a sign of insufficient insulin. Most cases of ketoacidosis occur in people with type 1, it very rarely occurs in people with type 2. Without enough insulin, the body’s cells cannot use glucose for energy. To make up for this, the body begins to burn fat for energy instead. This leads to accumulation of dangerous chemical substances in the blood called ketones, which also appear in the urine. The symptoms of ketoacidosis include:
• All the symptoms for hyperglycaemia • Loss of appetite • Stomach pains • Nausea or vomiting • Extreme tiredness • A fruity smell on the breath
If the person looks unwell, is apathetic, dehydrated and has ketones in the urine, seek medical assistance immediately.

Diabetes management workbook
Doc: PHDDMWKB.15 Version: 1 Issued: Dec 2015 Page 11 of 25
Hyperglycaemic Hyperosmola Syndrome (HHS) If someone has very poorly controlled Type 2 diabetes, they can develop a life threatening condition called Hyperglycaemic Hyperosmola Syndrome. In this condition, very high glucose levels draw fluid out of the body’s tissues. They body becomes very dehydrated; this can lead to a coma if not treated. The symptoms include:
• Thirst • Passing lots of urine • Muscle cramps • Slow heavy breathing • Extreme tiredness
Steroids and Diabetes Corticosteroids (steroids) are hormones similar to those naturally occurring in the body that are produced to fight stress, injury and disease. They are useful anti-inflammatory medications and can be used to treat asthma, arthritis, dermatitis and to prevent nausea during medical procedures such as chemotherapy. Certain forms of steroids can affect blood glucose levels in people with and without diabetes. Often people who have diabetes and are taking large doses of steroids prescribed by their doctor for a medical condition, need to temporarily commence or increase diabetes tablets or insulin injections. Steroids raise blood glucose levels in three ways:
1) They block the action of insulin which causes insulin resistance 2) They make glucose less able to move out of the blood stream to be taken up by the muscles 3) They cause the liver to start releasing extra glucose into the blood stream.
People with type 1 or type 2 diabetes need to monitor their blood glucose levels more often if they are taking oral steroids, to check if and when their levels are rising. You should report any changes or symptoms to your health care team. Never stop steroid medication abruptly. Steroids that are taken for a short period of time will usually be started at a high dose and then slowly reduced every day or so. Steroids that are taken for longer than 7-10 days need to be reduced slowly and safely. An abrupt stop to steroid medication can cause someone to become very unwell. Sick day management plan Australian Diabetes Education Association advises that common illness such as urinary tract, ear and chest infections and viral illnesses place stress on the body of a diabetic person. The result of this stress is that blood glucose levels will rise and may become quite high. It is really important for people with diabetes to have a Sick Day Management plan in place. This requires putting a plan in place before the person becomes sick and preparing an Action Plan in conjunction with their doctor. When sick, the advice from the Australian Diabetes Education Association is:
• Continue taking the diabetes medication as prescribed • Monitor blood glucose levels more frequently, usually every 2 hours • Ask for help early from your GP or local hospital • Keep drinking and eat if possible • Go to hospital if:
o blood glucose is greater than 15mmol/L for more than 12 hours or if it continues to rise o If the person is feeling drowsy, confused, having difficulty breathing or has severe abdominal pain o If the person has hypoglycemia or if the blood glucose cannot be kept above 4mmol/L o If the person is too unwell to carry out their self-monitoring o If the person if vomiting or diarrhoea continues for more than 12 hours

Diabetes management workbook
Doc: PHDDMWKB.15 Version: 1 Issued: Dec 2015 Page 12 of 25
Sick day action plan sample (Source: www.adea.com.au) Sick say action plan Date: Any special instructions for when to commence using guidelines
Details of whom to contact
Action to take if unable to contact the numbers above
Any special instructions for diabetes medication
Any special instructions for types of fluids to have
Instructions for use of insulin
Instructions for managing low blood glucose levels
When to seek medical care
Other Complications of Diabetes In the long term, untreated diabetes raises the risk for complications, such as:
• Heart disease and stroke (four times more common in people with diabetes) • Blindness and other eye problems (diabetes is a leading cause of adult blindness in Australia) • Nerve damage • Nerve pain • Kidney failure • Amputation
These problems can be prevented or greatly reduced by maintaining good blood glucose control and regular check-ups.

Diabetes management workbook
Doc: PHDDMWKB.15 Version: 1 Issued: Dec 2015 Page 13 of 25
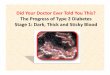
Diabetic ulcers Diabetic foot problems occur as a result of various factors such as ulcerations, infections and gangrene. They are the most common cause of hospitalisation amongst people with diabetes. In people with diabetic foot ulcers, peripheral sensory neuropathy, deformity and trauma are commonly presenting risk factors. All three of these risk factors are present in 65% of diabetic foot ulcers. Calluses, oedema, and peripheral vascular disease have also been identified as factors in the development of diabetic foot ulcers. Diabetic peripheral neuropathy is thought to be the result of vascular disease. Diabetic peripheral neuropathy is present in 60% of diabetic persons and in 80% of diabetic persons with foot ulcers. It is the greatest risk factor for foot ulceration. The result of loss of sensation in the foot is unnoticed injuries and fractures; structural foot deformity, such as hammertoes, bunions, metatarsal deformities, or Charcot foot; further stress and eventual tissue breakdown. Excessive heat or cold, pressure from a poorly fitting shoes or damage from a blunt or sharp object may cause blistering and ulceration because it is not noticed due to the loss of sensation. These factors increase risk of limb loss to a high risk level.
Charcot deformity with mal perforans ulcer of plantar midfoot. Among patients with diabetes, 15% develop a foot ulcer and 12-24% of individuals with a foot ulcer require amputation. Fifty per cent of the people with amputations will develop ulcerations and infections in the other limb within 18 months. Fifty eight per cent will have an amputation of the other limb 3-5 years after the first amputation. In addition, the 3-year mortality after a first amputation has been estimated as high as 20-50%. Note: It is recommended best practice that complex or chronic wounds, such as diabetic ulcers, are managed by a qualified wound specialist. This person will either manage the wound directly or will supervise designated staff in the management of the wound. Ulcer assessment Diabetic ulcers tend to occur in the following areas:
• Areas most subjected to weight bearing, such as the heel, plantar metatarsal head areas, the tips of the most prominent toes (usually the first or second), and the tips of hammer toes
• Areas most subjected to stress, such as the dorsal portion of hammer toes. Ulcers also occur over the malleoli because these areas are commonly subjected to trauma.
Other physical findings include the following:
• Hypertrophic calluses • Brittle nails • Hammer toes • Fissures
Diabetic foot ulcer

Diabetes management workbook
Doc: PHDDMWKB.15 Version: 1 Issued: Dec 2015 Page 14 of 25
Signs of diabetic ulcers Sign Symptom/appearance
Neuropathic pain Burning, stinging, shooting and stabbing (non-stimulus dependent)
Local pain Deep infection or Charcot joint
Size Length, width, depth and location, preferably with clinical photograph
Wound bed Appearance: • Black (necrosis) • Yellow, red, pink • Undermined
Infection signs Odour Some signs (fever, pain, increased white blood count/ ESR) may be absent. Evaluate the ulcer for signs of infection, inflammation and oedema.
Exudate Copious, moderate, mild, none
Wound edge Callus and scale, maceration, erythema, oedema Acknowledgement: This table is courtesy of Coloplast – Improved Patient Outcomes for Diabetic Foot Ulcers – A Pocket Guide
Gangrene Pressure sores
Kidney failure Over time, the high levels of sugar in the blood can damage the millions of tiny filtering units within each kidney. This eventually leads to kidney failure. Around 20 to 30 per cent of people with diabetes develop kidney disease (diabetic nephropathy), although not all of these will progress to kidney failure. A person with diabetes is susceptible to nephropathy whether they use insulin or not. The risk is related to the length of time the person has diabetes. For people with diabetes, kidney problems are usually picked up during a check-up by their doctor. At first, the only sign is high protein levels in the urine, but this has no symptoms. It may be years before the kidneys are damaged severely enough to cause symptoms. Some of the symptoms may include:
• Fluid retention (oedema of the legs or face) • Fatigue • Headache • Nausea • Vomiting.
Eye complications People with diabetes do have a higher risk of blindness than people without diabetes. But most people who have diabetes have nothing more than minor eye disorders. People with diabetes are 40% more likely to suffer from glaucoma than people without diabetes. The longer someone has had diabetes, the more common glaucoma is. Risk also increases with age.

Diabetes management workbook
Doc: PHDDMWKB.15 Version: 1 Issued: Dec 2015 Page 15 of 25
Glaucoma occurs when pressure builds up in the eye. The pressure pinches the blood vessels that carry blood to the retina and optic nerve. Vision is gradually lost because the retina and nerve are damaged. There are several treatments for glaucoma. Some use drugs to reduce pressure in the eye, while others involve surgery. Many people without diabetes get cataracts, but people with diabetes are 60% more likely to develop this eye condition. People with diabetes also tend to get cataracts at a younger age and have them progress faster. With cataracts, the eye's clear lens clouds, blocking light. Diabetic retinopathy is a diabetes complication that affects eyes. It's caused by damage to the blood vessels of the light-sensitive tissue at the back of the eye (retina). At first, diabetic retinopathy may cause no symptoms or only mild vision problems. Eventually, it can cause blindness. Nutrition Nutrition management goals in diabetes are:
• Attain and maintain optimal BGLs, usually between 4.0 – 10.0mmol/L. In the elderly, a higher upper reading may be acceptable.
• Reduce cardiovascular risk • Achieve weight control • Encourage physical activity – planned exercise program. Exercise improves glucose regulation. • Eat a balanced diet comprised predominantly of foods that have a low Glycaemic Index
A resident’s diet should be designed in consultation with a qualified dietician. The aims of the diet may also include weight loss as well as diabetes management. Constant reinforcement of dietary advice usually has the effect of better compliance with the diet. Studies have shown that a person’s food choices are significantly improved when people have nutrition education and know what constitute appropriate foods. Glycaemic index Carbohydrates (CHO) are digested to produce glucose. Some are slowly absorbed, others more quickly. The glycaemic index or GI ranks carbohydrates according to their effect on blood glucose levels. The lower the GI, the slower the rise in blood glucose levels will be when the food is consumed. The effect may differ from person to person. It is recommended that people with diabetes have moderate amounts of carbohydrate and include high fibre foods that also have a low GI (not all high fibre foods have a low GI). Some research has shown that by eating a diet with a lower GI, people with diabetes can reduce their average blood glucose levels. This is important in reducing the risk of developing diabetes-related complications. The recommendation is to eat more low GI foods, but not to exclude high GI foods. The GI is only a small part of the healthy eating plan for people with diabetes.

Diabetes management workbook
Doc: PHDDMWKB.15 Version: 1 Issued: Dec 2015 Page 16 of 25
Glycaemic index reference table (Baker institute)

Diabetes management workbook
Doc: PHDDMWKB.15 Version: 1 Issued: Dec 2015 Page 17 of 25
Healthy weight range, waist circumference and BMI Most Australian adults and around a quarter of our children are now overweight or obese. Being overweight greatly increases the risk of high blood pressure, muscle, bone and respiratory disorders and chronic disease including type 2 diabetes. Being underweight also carries health risks. Waist circumference A way for adults to measure their weight-related health risk is with a tape measure. This can be done by measuring between the lowest rib and the top of the hip bone, roughly in line with the belly button.
BMI chart for adults Body mass index (BMI) is one method used to estimate total amount of body fat. It is calculated by dividing your weight in kilograms by your height in metres squared (m2). Differences in BMI between people of the same age and sex are usually due to body fat. However, there are exceptions to this rule, which means a BMI figure may not be accurate. BMI is not the best measure of weight and health risk. A person’s waist circumference is a better predictor of health risk than BMI. BMI calculations will overestimate the amount of body fat for:
• Body builders • Some high performance athletes • Pregnant women.
BMI calculations will underestimate the amount of body fat for:
• The elderly • People with a physical disability who are unable to walk and may have muscle wasting.
Adults can use the following graph as a rough guide to assess weight status. It may not be appropriate for those who have a high muscle mass due to elite sport of physical activity.
1) Find your weight on the left and your height at the bottom of the chart 2) From your height and weight, trace along the lines until they meet 3) The point where the lines meet will tell you what BMI range you are in.

Diabetes management workbook
Doc: PHDDMWKB.15 Version: 1 Issued: Dec 2015 Page 18 of 25
Importance of exercise The human body generally responds well to physical exercise and substantial improvements may be anticipated in heart and lung function, muscular strength and endurance and flexibility. Some of the more noticeable changes from exercise may include:
• Improved glucose regulation • Increased ability to perform physical work • Improved sense of well being • Increased muscular strength • Decreased blood pressure • Improved sleep patterns and levels of anxiety
Exercise can have a profound effect with the most "unfit" person usually experiencing the greatest benefits. Before commencing any program of physical activity, a medical check-up with a Doctor is advised. Other tips for commencing an exercise program include:
• Ease steadily and gently into an exercise program - begin with low intensity, low frequency activity and proceed slowly
• Choose an exercise activity that is enjoyed • Start a regular routine by exercising every other day • Exercise in a group setting as this is more socially enjoyable • Avoid any exercise that hurts. Movements should be gentle and comfortable

Diabetes management workbook
Doc: PHDDMWKB.15 Version: 1 Issued: Dec 2015 Page 19 of 25
Importantly: • Always check the feet, including soles, for any injury before exercising • Check BGL before commencing exercise • Carry identification and wear a medical identification bracelet • Carry some sugary food and carbohydrate food in case a hypo is experienced
WARNING: • Stop exercising and consult your Doctor if any of the following occur: nausea, dizziness,
breathlessness, tightness in the chest or persistent muscle soreness. • Remember that there is there is no benefit in continuing exercise when it hurts.
Lifestyle changes The diagnosis of diabetes can be very stressful for both younger and older patients. Initial denial of the condition is normal. Patients, whose difficulties with accepting the diagnosis compromise their treatment, may benefit from psychological interventions. General practitioners can engage the help of a psychologist, social worker or counsellor. These practitioners may be accessed as part of a Team Care Arrangement within a General Practice Management Plan or under the Better Access to Psychiatrists, Psychologists and General Practitioners through the Medicare Benefits Scheme Initiative. The younger patient needs to become familiar with their condition, insulin and diet changes. They will have to learn to cope with feelings that come with depending on medication for survival. The older patient faces increasing vulnerability to sickness, disability and loss of function. Fears may include job security, physical disfigurement and loss of ability to contribute to present relationships. The diagnosis of diabetes may have a profound effect on people engaged in certain occupations, eg: machinery operators, pilots, heavy vehicle drivers, divers, etc. While not always prohibiting many of these occupations, the diagnosis of diabetes may require careful career counselling. It is important for the patient to have all the information available so that a common sense of purpose between the health care professionals and the patient can develop. This takes time and some patients may decide to reject advice. Professionals need to maintain an open approach and emphasise that help is available when required. Team management of diabetes The focus of the team management is the person diagnosed with diabetes. Medicare subsidies are available for group education sessions involving diabetes educators, dieticians and exercise physiologists. Knowledgeable support, practical help and encouragement to live healthy, active lives will do much to prevent further complications from this disease in residents. Education is ongoing and needs to continue for the rest of the person’s life. Diabetes knowledge, especially self-care skills such as blood glucose monitoring, foot care, and insulin administration need to be assessed regularly at the twelve monthly GP review. Lifestyles which have been established for many years are not easy to change and health care professionals cannot expect immediate adherence to the plan of management. Assess the SNAP risk factors (Smoking, Nutrition, Alcohol and Physical activity) and establish a long term lifestyle plan. Diabetes educator Qualified diabetes educators can support the resident in assisting them to develop knowledge of their condition, how to self-monitor, manage their eating plans and foot care, how to use their medication appropriately and exercise plans. A newly diagnosed person will benefit from early referral to a diabetes educator. This enables them to learn about and put into place informed actions on how to manage and improve their glycaemic control.

Diabetes management workbook
Doc: PHDDMWKB.15 Version: 1 Issued: Dec 2015 Page 20 of 25
Dietician Lifestyle changes such as a healthy diet, regular exercise and any necessary weight loss is often sufficient to gain control of diabetes in the majority of newly diagnosed people. The sooner a newly diagnosed person sees a dietician, the sooner the person can learn about and put into place informed actions regarding their diet to improve glycaemic control. Endocrinologist An Endocrinologist is a specialist doctor who has done years of training in diabetes. Many people with type 1 diabetes see an endocrinologist. People with type 2 diabetes may see an endocrinologist if they are having trouble with their diabetes management or if they are having other health problems impacting on their diabetes. General practitioner The GP is usually the first point of contact and will be intimately involved in the ongoing care, playing a central role in managing and supporting a person with a chronic condition like diabetes. Pharmacist Pharmacists are often a first point of contact for people asking for advice on a wide range of health issues. They are able to provide a free information leaflet for all prescription medications called Consumer Medicine Information (CMI). An annual review of a person’s medication can be conducted by authorised Pharmacists, known as Home Medicines Review (HMR). These reviews are funded by the Australian Government. The aim of the review is to look at a person’s medication regime and to identify whether there is a risk of drug side effects, interactions, long-term side effects or possible toxicity and to make recommendations about safe medication orders to the resident’s doctor. Podiatrist A diabetic person is at significant risk of foot problems due to compromised circulation and sensation. Podiatrists provide preventative care and also assist in the management of diabetic foot ulcers or calluses. Diabetic foot complications are the most common cause of non-traumatic amputation. Eye specialist A diabetic person is at risk of vision loss due to diabetes retinopathy. This is caused by damage to the very small blood vessels on the back of the eye. Diabetes retinopathy can occur regardless of the type of diabetes, age or BGL control of the resident. However; good BGLs, blood pressure and regular screening can greatly reduce the risk of complications. Everyone with diabetes should have their eyes checked regularly, from when first diagnosed and then at least every two years after that.

Diabetes management workbook
Doc: PHDDMWKB.15 Version: 1 Issued: Dec 2015 Page 21 of 25
Diabetes references and resources Diabetes Australia www.diabetesaustralia.com.au/ Victoria Office and retail store address: 570 Elizabeth Street Melbourne VIC 3000 Customer Service: 1300 136 588 Direct Business Calls: (03) 9667 1777 Opening hours: Mon to Fri 8:30am - 5:00pm Fax: (03) 9667 1778 email: [email protected] http://www.diabetesvic.org.au/contact-us Diabetes Research Foundation http://www.diabetesresearchfoundation.asn.au/site/ Juvenile Diabetes Research Foundation http://www.jdrf.org.au/ Royal Children’s Hospital, Melbourne Fact sheet: Diabetes manual, Diabetes manual type 2 diabetes http://www.rch.org.au Department of Health, Victoria Home Page Keyword search: Diabetes www.health.vic.gov.au Department of Human Services, Victoria Home Page Keyword search: Diabetes www.dhs.vic.gov.au/home Better Health Channel, Victoria Home Page: A-Z of Conditions: Diabetes Fact Sheets www.betterhealthchannel.vic.gov.au/ Department of Education and Early Childhood Development Home Page keyword search: Diabetes – information on medical condition guidelines, Safety guidelines for Education Outdoors emergency response procedures; Student safety and risk management etc. http://www.education.vic.gov.au/

Diabetes management workbook
Doc: PHDDMWKB.15 Version: 1 Issued: Dec 2015 Page 22 of 25
Notes

Diabetes management workbook
Doc: PHDDMWKB.15 Version: 1 Issued: Dec 2015 Page 23 of 25
Appendices Appendix 1 – Blood Glucose/Ketone Monitor Operation Although similar, all blood glucose monitors will have different operating instructions in relation to calibration and use. The following instructions and notes are for the MediSense Optimum Xceed blood glucose monitor which also has the capacity to monitor blood ketones.
• Three types of tests strips may be used with MediSense Optimum Xceed blood glucose monitor machine – blood glucose, ketone and calibration MediSense (Abbott) test strips
• When a test strip is inserted into the strip port (sensor), an icon corresponding to the test strip type shows
on the display window, e.g. a blood drop icon displays for a blood glucose strip, a circle for ketones.
• When a blood sample or control solution sample is applied to the test strip, depending on the strip being used, either glucose or ketones present in the sample react with the chemicals on the test strip. This reaction produces a small electrical current that is measured by the machine. The test result is shown on the display window.
A carry case is used to store and carry the monitor and other supplies of testing strips, lancing device and small number of disposable lancets. Strip port This is where any of the following are be inserted, depending on the test being conducted:
• Glucose calibration strips • Ketone calibration strips • Blood glucose test strips • Blood ketone test strips • Data cable used for uploading results onto a computer (not available for training sessions)
Mode button This button is used to:
• Turn the monitor ON or OFF • Access monitor setup options • Access and save monitor settings • Access previous results and averages
Battery When the monitor screen fails to turn on, check to see if the battery is installed correctly. The battery icon will display on the screen when the battery is getting low or it needs to be replaced. A CR 2032 Lithium (coin cell) battery is used and needs to be inserted with the plus + sign facing up1. Testing strips MediSense strips (Abbott) are the only blood glucose, blood ketone or calibration strips that may be used in the MediSense Optimum Xceed monitor Operation Each time the monitor is turned on, a full display shows. It is important to check that the “full display” window is displaying correctly each time the machine is turned on and before testing a blood sample. All information should
1 A spare battery is provided with the machine. Trainers are to contact the Training Support Officer when a battery is changed to ensure replacement and sufficient power during next training sessions.

Diabetes management workbook
Doc: PHDDMWKB.15 Version: 1 Issued: Dec 2015 Page 24 of 25
appear completely in the display window. Note the “full display” screen is only visible on the display window for a short amount of time. Calibration The monitor is calibrated using the calibration strip provided with each new packet of MediSense blood glucose or ketone test strips. This is necessary so the machine recognises the new batch of strips. Calibration is carried out when:
• When a new packet of blood glucose or blood ketone test strips are used • When changing strip type e.g. from blood glucose to blood ketone or calibration strips
Control Test Control tests are carried out to ensure the sensor is giving a correct reading using solutions of known quantities of the substance being measured, e.g. glucose. Testing is carried out when:
• A new packet of blood glucose or blood ketone test strips are used • Changing strip type e.g. from blood glucose to blood ketone or calibration strips • There is doubt about the blood glucose or ketone reading obtained • Diabetic medication plans are adjusted or changed to ensure baseline
Control test - trainer to demonstrate procedure
• 2 solutions are used for a control test - one marked LO and one marked HI • It is important not to use a control test solution that has exceeded its expiry date - each solution will last for
approx 90 days from opening • An LOT number is provided at the bottom of the instruction leaflet accompanying each new packets of test
strips • For a control test using the LO solution - the result needs to be within the LOT number parameters for the LO
solution • For a control test using the HI solution – the result needs to be within the LOT number parameters for the HI
solution Troubleshooting and error messages E – 1 Temperature is too hot or too cold for the system to work properly
move to warmer or cooler area and try again
E – 2 Sensor error turn sensor OFF and try again
E – 3 There may be a problem with the test strip
use new test strip and try again
E – 4 Blood glucose result may be too high to be read by the system or there may be a problem with the test strip Try again with a new test strip If happens again consult the supervising medical professional immediately
E – 5 Blood applied to test strip too soon Try again with a new test strip
E – 6 Calibration/Test strip error
Repeat calibration using the calibrator that came with the test strips you are using, check the expiry of the test strips, if error keeps occurring contact the supplier2
E – 7 Test strip error - test strip is damaged, has been used or the sensor does not recognise it
Use a test strip designed for the monitor and ensure it is a new test strip
E – 8 Sensor Error remove the test strip, turn the monitor OFF and try again)
2 Trainers, please notify Training Support Officer of this or any monitor malfunction

Diabetes management workbook
Doc: PHDDMWKB.15 Version: 1 Issued: Dec 2015 Page 25 of 25
Appendix 2 – Baker IDI Nutritional plate model