-
CHILDRENS HEALTH CARE, 35(4), 349363Copyright 2006, Lawrence
Erlbaum Associates, Inc.
Diabetes Management andMetabolic Control in School-Age
Children With Type 1 Diabetes
Maureen A. FreyCarmen and Ann Adams Department of Pediatrics
Wayne State University
Deborah EllisDepartment of Psychiatry and Behavioral
Neurosciences
Wayne State University
Tom TemplinCollege of Nursing
Wayne State University
Sylvie Naar-KingCarmen and Ann Adams Department of
Pediatrics
Wayne State University
James P. GutaiDepartment of Community Medicine
Wayne State University
This study investigated the effect of mothers coping resources,
cognitive resources,family stress, and demographic variables on
diabetes management and the mediat-ing role of diabetes management
on metabolic control among children with dia-betes. Mothers (N =
59) completed self-report measures. HbA1c was obtained fromthe
medical records. Although cognitive resources, coping resources,
and familystress accounted for 30% of the variance in diabetes
management, the hypothesis of
Correspondence should be sent to Maureen A. Frey, Critical Care
Medicine4134 CHM, 3901Beaubien, Detroit, MI 48201-2119. E-mail:
[email protected]
Chap 05.qxd 10/23/2006 5:30 PM Page 349
-
mediation was not supported. The only significant predictor of
HbA1c was AfricanAmerican race/ethnicity. The findings identify
modifiable targets for practice andhighlight the increased risk for
poor metabolic control for minority children.
Type 1 diabetes, the most common endocrine disorder in the
pediatric popula-tion, affects 1 in every 400 to 600 children and
adolescents (National DiabetesInformation Clearing House, n.d.).
Type 1 diabetes requires lifelong administrationof exogenous
insulin, daily blood glucose testing, continual attention to
dietaryintake, and increased physical activity to maintain adequate
metabolic control.Although diabetes management and metabolic
control have been extensively inves-tigated in adolescent
populations, much less is known about predictors of
diabetesmanagement and metabolic control in younger children. Yet
the first years afterdiagnosis are critical in terms of
establishing adequate patterns of diabetes manage-ment. The role of
parents of young children with diabetes is also becoming
increas-ingly important as intensive insulin therapy, with its
higher level of complexity, isinitiated earlier in the course of
the disease. In addition, because the microvascularcomplications of
diabetes are directly related to duration of diagnosis, young
chil-dren are at increased risk for such complications compared
with those diagnosed ata later age (Donaghue et al., 2003). The
lack of research with school-age and pread-olescent children with
diabetes is a significant barrier to the development of
healthpromotion and risk reduction interventions with this
population. Accordingly, thepurpose of this study is to identify
predictors of diabetes management among moth-ers of 6- to
13-year-old children with type 1 diabetes and subsequently to
determinethe relationship between diabetes management and metabolic
control.
Descriptive studies with children and adolescents show that
younger childrenhave better metabolic control than do older
children (Johnson et al., 1992; La Greca,Follansbee, & Skyler,
1990; Palta, Shen, Allen, Klein, & DAlessio, 1996).
However,others have noted that many school-age and younger children
show evidence ofless than adequate metabolic control. For example,
Davis et al. (2001) reportedthat 43% of their sample had a
glycohemoglobin level four standard deviationsabove the normal
range, indicating fair to poor glycemic control. Garrison
andcolleagues (Garrison, Biggs, & Williams, 1990) reported that
23% of their sampleshowed poor glycemic control for at least 1 year
prior to study entry. In addition,29% of the sample showed fair to
poor regimen adherence. These studies areimportant because all of
the participants were younger than 11 years of age. Inaddition,
there is evidence that patterns of metabolic control are
established earlyin the course of the disease, often within 2 years
of diagnosis (Forsander et al.,1998; Jacobson et al., 1990). Both
cross-sectional and longitudinal studies showthat early patterns of
metabolic control tend to remain stable over time (Seiffge-Krenke,
& Stemmler, 2003).
Studies of school-age children with diabetes are limited
compared with studies ofadolescents with diabetes (Anderson &
Laffel, 1997). Family support for diabetes
350 FREY, ELLIS, TEMPLIN, NAAR-KING, GUTAI
Chap 05.qxd 10/23/2006 5:30 PM Page 350
-
(Waller et al., 1986), family conflict (Jacobson et al., 1990),
and family stress(Viner, McGrath, & Trudinger, 1996) have been
related to metabolic control, andparent involvement with diabetes
management has been related to adherence inchildren (La Greca et
al., 1990). However, in view of the more primary role of
thecaregiver in the management of diabetes at this age, caregiver
factors might beparticularly important. Therefore, Davis and
colleagues (2001) investigated par-enting style in mothers of 4- to
10-year-old children with diabetes. Parentalwarmth was a
significant predictor of adherence. However, neither adherence
norparental warmth was predictive of metabolic control. In
examining maternal tem-perament variables related to young
childrens adherence and metabolic control,Garrison et al. (1990)
reported that maternal characteristics related to child out-comes
in a differential manner. That is, maternal temperament was
associatedwith metabolic control but not with adherence. Maternal
temperament character-istics that were found to be associated with
poor metabolic control were negativemood, high social withdrawal,
high rigidity, and lower activity level. The authorsconcluded that
further attention to individual characteristics of parents as
predic-tors of diabetes management in children was warranted.
As has been found in studies of adolescents, studies with
younger childrendemonstrate that diabetes management has not always
been closely linked tometabolic control. In one of the few studies
to include children younger than8 years of age, diabetes
management, measured as a single-item parent rating ofthe extent to
which You or your child follow the diabetes regimen, was notrelated
to metabolic control (Auslander, Anderson, Bubb, Jung, &
Santiago,1990). Johnson and associates (1992) also failed to show a
relationship betweenadherence and metabolic control in school-age
children despite considerablemethodological rigor and use of the
well-established 24-Hour Recall Interview tomeasure adherence.
A significant gap in the research is lack of attention to the
cognitive ability ofcaregivers. Diabetes management is complex and
requires considerable problemsolving and decision making. The
cognitive ability of adolescents is a criticalfactor in determining
readiness for and ability to manage self-care (Brandt,1998).
Likewise, the cognitive ability of caretakers may affect their
ability tomake decisions regarding insulin adjustments or dietary
changes. Cognitive abil-ity is also related to health literacy or
to the ability to process and act on healthinformation. Parents
with poor health literacy may struggle to carry out
recom-mendations made by medical personnel for management of their
childs care(Schillinger et al., 2002).
Some of the strongest and most consistent predictors of
metabolic control inchildren and adolescents are the
sociodemographic characteristics of race/ethnicity,family income,
and family composition. Poor metabolic control is associatedwith
minority status, low family income, and single-parent headed
households(Auslander, Thompson, Dreitzer, White, & Santiago,
1997; Delamater, Albrecht,
DIABETES MANAGEMENT AND METABOLIC CONTROL 351
Chap 05.qxd 10/23/2006 5:30 PM Page 351
-
Postellon, & Gutai, 1991; Delamater et al., 1999; Harris,
Greco, Wysocki,Elder-Danda, & White, 1999; Harris &
Mertlich, 2003; Overstreet, Holmes,Dunlap, & Frentz, 1996;
Thompson, Auslander, & White, 2001). However, in stud-ies in
which the effects of race/ethnicity and socioeconomic status were
controlled,the most significant risk factor for poor metabolic
control was living in a single-parent household (Harris et al.,
1999; Overstreet et al., 1996; Thompson et al.,2001). Auslander et
al. (1990) also found that African American mothers reportedlower
adherence to diet and frequency of blood glucose testing than did
EuropeanAmerican mothers. However, there is limited research on
other caregiver charac-teristics or behaviors that might account
for differences in health outcome.
Kings Conceptual System (King, 1981, 1995) provides an
ecological frameworkfor understanding and organizing factors that
may influence diabetes manage-ment and metabolic control. The
framework includes personal systems (individu-als), interpersonal
systems (families and other small groups), and social systems(large
community groups). It is interactions within and between the three
systemsthat influence behavior. Behavior, in turn, influences
health outcomes. Knowledgeof interactions comes from concepts such
as stress, coping, resources, and health.The empirical literature
has also suggested that these concepts are important
inunderstanding diabetes management.
In summary, research with caregivers of school-age children is
very limiteddespite the acknowledged importance of diabetes
management and metaboliccontrol for this age group. Research has
suggested that some parent characteris-tics and demographic factors
may influence metabolic control directly and indi-rectly through
management of diabetes. Accordingly, the aim of our study is
toinvestigate the effects of family stress, mothers coping
resources, mothers cog-nitive resources, and selected demographic
variables on diabetes management in6- to 13-year-old children with
type 1 diabetes. A secondary aim was to determineif diabetes
management mediated the effects of family stress, mothers
copingresources, mothers cognitive resources, and selected
demographic variables onmetabolic control in this population.
METHOD
ParticipantsParticipants for this descriptive cross-sectional
study were recruited from auniversity-affiliated pediatric diabetes
clinic. Participants were seen clinically formedical visits by a
multidisciplinary team at 3- to 4-month intervals. The
sampleconsisted of 59 motherchild dyads who met the following
eligibility criteria:child between 6 and 12.9 years of age, who had
been diagnosed for at least 1 yearwith type I diabetes, and no
known developmental delay or other chronic med-ical conditions.
Given the young age of children in the sample, all children
were
352 FREY, ELLIS, TEMPLIN, NAAR-KING, GUTAI
Chap 05.qxd 10/23/2006 5:30 PM Page 352
-
managed by injected insulin rather than insulin pump. They were
expected to testblood glucose three to four times per day and were
provided with individualizedmeal plans. All maternalchild dyads
were English speaking. Data were collectedat the time of a
regularly scheduled clinic appointment with the assistance of
atrained data collector. Sixty-three percent of the eligible
individuals agreed to par-ticipate. The most frequent reason for
nonparticipation was the extra time duringthe clinic appointment
needed to complete the research measures. All data wereobtained by
maternal report.
Characteristics of the participants for the total sample and by
race/ethnicity areshown in Table 1. Approximately two thirds of the
sample was of minorityrace/ethnicity: 27% were African American, 3%
were American Indian, 15%were biracial, and 15% selected Other.
Three mothers, 5% of the sample, didnot provide race/ethnic
information. Overall, the demographics of the samplewere
representative of the diverse urban population served by the clinic
whereparticipants were recruited. Analyses of variance indicated no
significant differ-ences between the racial/ethnic subsamples on
mothers age, mothers education,or childs age. Pearson chi-square
analyses indicated no significant differences inchilds gender.
There was a difference in mothers marital status and familyincome.
A significantly smaller percent of African American mothers (29%)
weremarried compared with the European American (70%) or the Other
(61%) group.Family income was also significantly lower for African
Americans.
The mean age of the children was somewhat skewed toward the
upper end ofthe eligibility age range, which is consistent with the
typical age of onset of type 1diabetes. On average, children had
been diagnosed with diabetes for 3 to 4 years.
DIABETES MANAGEMENT AND METABOLIC CONTROL 353
TABLE 1Sample Characteristics by Race/Ethnicity
African European Characteristic Totala Americansb Americansc
Otherd
ChildAge 9.45 (2.48) 10.15 (2.68) 9.49 (2.20) 9.17 (2.58)Female
(%) 61 69 45 67Duration of 3.52 (2.53) 3.59 (2.88) 4.06 (2.92) 2.99
(1.82)
diabetesMother
Age 37.50 (5.80) 38.79 (7.02) 38.20 (5.56) 35.72 (4.93)Education
(years) 13.56 (1.80) 13.19 (1.22) 14.30 (2.22) 13.18 (1.72)Married
(%) 61 31 70 78Income (yearly) $32,198 ($16,293) $19,893 ($16,908)
$38,525 ($13,629) $34,605 ($14,000)
Note. Values are mean (SD) or percentage.aN = 59. bn = 16 (27%).
cn = 20 (34%). dn = 23 (39%).
Chap 05.qxd 10/23/2006 5:30 PM Page 353
-
Measures
Family Inventory of Life Events and Changes (FILE; McCubbin
& Patterson,1987). The FILE is a 71-item parent-report scale
designed to assess both acuteand chronic stressful events in the
family system over the previous 12 months.Positive responses are
summed to form a total stress score. Higher scores indicatehigher
levels of stress. Testretest reliability of .80 and evidence of
good con-struct validity has been reported. The scale has been
extensively used with diversepopulations.
The Shipley Institute of Living Scale. This 60-item
parent-report scale iscomposed of two brief subtests: vocabulary
and abstract thinking, which are cog-nitive resources correlated
with general cognitive ability (Zackery, 1991). Respondentsselect
words with similar meaning from a list and fill in numbers or
letters to logi-cally complete given sequences (abstract thinking).
The scale requires minimalassistance to complete and can be
administered in small groups. High split-half(.84) and testretest
(.78) reliability coefficients have been reported. The Shipleyscale
(Zackery, 1991) correlates highly with full-scale IQ scores as
obtained byinstruments such as the Wechsler Adult Intelligence
ScaleRevised (Wechsler,1981). Total scores were used in our
analyses.
The Coping Resources Inventory (CRI). This 60-item
parent-reportscale quantifies the availability of five resources
for coping: cognitive, social,emotional, spiritual/philosophical,
and physical (Hammer & Marting, 1988).Responses are on a
4-point scale, ranging 1 (never), 2 (rarely), 3 (always), and4
(almost always), in the previous 6 months. Cronbachs alpha
coefficients of .71to .84 for the subscales and .91 for the scale
total have been reported. In this study,Cronbachs alpha
coefficients ranged from .48 to .89 for the subscales and .92
forthe scale total. In this study, the total score was used in the
analyses.
The Diabetes Management ScaleParent Report (DMSPR). TheDMSPR was
used to measure diabetes management (Frey, Ellis, Naar-King,
&Greger, 2004; Schilling, Grey, & Knafl, 2002). The scale
taps blood glucose test-ing; insulin injections; dietary
considerations; symptom management; exercise;and parent/adult
supervision, assistance, and overall responsibility for
manage-ment. Mothers were asked What percent of the time ? various
componentsof management were completed in the past 3 months. The
response scale rangedfrom 0% to 100%. Items are summed to obtain a
total score; higher scores reflectmore completed diabetes care for
the child. A previous study showed that theDMSPR was sensitive to
differences in both age and level of metabolic control.Internal
consistency of the DMSPR in this study was .78.
354 FREY, ELLIS, TEMPLIN, NAAR-KING, GUTAI
Chap 05.qxd 10/23/2006 5:30 PM Page 354
-
Metabolic control. HbA1c was obtained at each visit as part of
standardcare. The HbA1c value obtained at the time of study
recruitment was used inanalysis. The range of HbA1c for the sample
was 5.76% to 15.99%, with a meanof 9.00% (SD = 1.95%).
The demographic characteristics of race/ethnicity, family
income, motherseducation (highest grade completed), and marital
status were obtained bymothers self-report. Income and education
were considered proxy measures ofsocioeconomic status.
Procedures
The study received human participants approval from the
Institutional ReviewBoard. All mothers provided written informed
consent, and children older than7 years of age gave verbal assent
to participate. Most potential participants werenotified of the
study by letter or by telephone prior to a scheduled medical
appoint-ment, although some were approached in the waiting area at
the time of theirappointment. Mothers completed the questionnaires
in the clinic and received $10to compensate for additional time in
the clinic.
Analytic ApproachWe used structural equation modeling (SEM) with
AMOS Version 5.0 (Arbuckle& Wothke, 2003) to determine
predictors of mothers diabetes management andto test for mediation.
A manifest model was specified because all constructs weremeasured
as single indicators. SEM is considered more appropriate than
tradi-tional multivariate analyses for testing mediation because it
allows both theassessment of goodness of fit of a specified model
and the testing of each esti-mated path coefficient (Satorra &
Saris, 1985). In the past, use of SEM wasrestricted to studies with
large samples. However, bootstrap analysis allowsmodel testing with
small samples by using the actual data to estimate standarderror
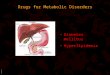
(Shrout & Bolger, 2002). The theoretical model tested is shown
in Figure 1and contains three exogenous variables and two
endogenous variables. Wehypothesized that maternal cognitive
resources, maternal coping resources, andfamily stress would be
predictors of diabetes management. In this model,
diabetesmanagement fully mediates the relationship between maternal
and family vari-ables and metabolic control.
Demographic covariates were added to the SEM model empirically
after ananalysis of residuals was performed. Potential covariates
were family income,mothers education (highest grade completed),
childs gender, childs race/ethnicity,and family composition. Family
composition was dichotomized as single parent
DIABETES MANAGEMENT AND METABOLIC CONTROL 355
Chap 05.qxd 10/23/2006 5:30 PM Page 355
-
and two parent. Two-parent families included two biological
parents, a stepparentand biological parent, and parents living with
a partner. The contrasts used forrace/ethnicity were African
American versus all others and European Americanversus all others.
In this analysis, residual error for each endogenous
variable(diabetes management and metabolic control) was first
computed. The pattern ofcorrelation between each residual and each
potential covariate was then exam-ined. Those covariates that were
significantly related to the residuals and to
theexogenous/predictor variables were included in the model to
reduce bias andpotential confounding effects. Family income and
African American race/ethnicitymet these criteria.
RESULTS
Bivariate correlations between variables are shown in Table 2.
The demographicvariables of family income, family composition, and
race/ethnicity were signifi-cantly intercorrelated indicating that
African American children were more likelyto be from single-parent
lower income families compared with White and otherrace/ethnic
children. There were no significant correlations between the
predictorvariables of mothers cognitive resources, mothers coping
resources, and familystress. However, several demographic variables
were significantly related to thepredictor variables.
Race/ethnicity, family income, and mothers education
weresignificantly related to mothers cognitive resources, and
family income wasalso related to mothers coping resources. Mothers
who reported lower cogni-tive resources also reported lower family
income, lower education, and AfricanAmerican race/ethnicity. Family
stress (r = .30, p = .022) and coping resources(r = .30, p = .009)
were significantly associated with diabetes management anddiabetes
management was significantly associated with metabolic control (r =
.26,p = .047). Mothers who reported lower stress and higher coping
resources also
356 FREY, ELLIS, TEMPLIN, NAAR-KING, GUTAI
MothersCognitiveResources
FamilyStress
MothersCopingResources
MothersDiabetesManagement
ChildsMetabolicControl
FIGURE 1 Theoretical model.
Chap 05.qxd 10/23/2006 5:30 PM Page 356
-
TABL
E 2
Corre
latio
ns A
mon
g Varia
bles
Vari
able
Age
Race
/Eth
nici
tya
Dur
atio
nH
gA1c
Inco
me
Educ
atio
nM
arri
edb
FILE
Ship
leyCR
I
Child A
ge
Rac
e/et
hnic
ity.15
Dur
atio
n.37
**.02
HbA
1c.33
**.56
**.09
Mot
her
Inco
me
.02
.37
**.23
.40
**
Educ
atio
n (ye
ars)
.11
.13
.04
.03
.18
Mar
ried
.10
.30
**.17
.17
.52
**.08
FILE
.05
.06
.05
.10
.04
.17
.21
Ship
ley
.11
.34
**.28
**.10
.48
**.42
**.24
.14
CRI
.03
.16
< .0
1.04
.27
.09
.07
.10
.16
DM
SPR
.19
.10
.21
.26
*.11
.03
.10
.34
**.17
.30
**
Note
.FI
LE =
Fam
ily In
ven
tory
of L
ife E
vents
and
Cha
nges
; Shi
pley
= S
hipl
ey In
stitu
te o
f Liv
ing
Scal
e; C
RI =
Cop
ing
Reso
urce
s Inv
ento
ry; D
MS
PR =
Dia
bete
s Man
agem
ent S
cale
Par
ent R
epor
t.a A
frica
n Am
eric
an =
1,a
ll ot
hers
= 0
. bM
arrie
d =
1,al
l oth
ers =
0.
*p
< .0
5. *
*p