Embed Size (px)
DESCRIPTION
typhoid lecture.ppt
Citation preview

Enteric Fever
Dr Paul Collini

TYPHOID
= smoke
i.e. stupor or clouding of mind
unfortunatley ricketssial disease also does this and is called ‘typhus’
We are concerned with Enteric fever
Typhoid or paratyphoid

Organisms
• Salmonella – gram negative bacillus– flagellated
• Antigens– somatic o antigen– flagella H antigen– Surface Vi antigen

Types of Salmonella
• Salmonella typhi• Salmonella paratyphi A,B,(sometimes C)• remember other forms of salmonella ‘non-
typhopidal salmonellae or NTS’– salmonella typhimurium, salmonella enteritidis
– cause diarrhoeal illness but not severe enteric fever (except in immunocompromised)

Epidemiology• typhoid salmonellae bacteria are endemic in all parts of
the 'developing' world– tend to be found in the tropics only because those are
the same areas with poor sanitation.– incidence higher in dry season or times of flood
• 12-20 M cases annually worldwide, India especially– Annual incidence 0.5-1% population in endemic area– Children and Young Adults predominantly
• MR 5-20%• NTS more prevelant as cause of enteric fever in areas of
high HIV prevalence

reservoir of infection
• only in man• are asymptomatic human carriers.
– bacteria continue a low level infection in the gall bladder, and with bile are excreted into the faeces.
– water supply contaminated by faeces– low standfard of self hygiene– extra problem if carrier is food worker / handler

Infection• is via ingestion of bacteria• bacteria are either in water supply or contaminate food• food kept at the right temperature (i.e. not refrigerated)
allows for multiplication of bacteria• infecting dose is impotrtant
– 10^3 organisms rarely cause disaese
– 10^5 organisms 25% attack rate
– 10^9 organisms 95% attack rate
• gastric acid can neutralise the bacteria to some extent, thus those on PPI / H2 blockers may be at more risk

Pathophysiology
ingestion bacilli attach to and penetrate mucosa of small intestine enter lymphatics and taken to mesenteric glands here multiplication of bacteria occurs drainage from lymphatic system to blood stream via thoracic
duct lead to a first, transient bacteraemia

Pathophysiology
infection travels to liver, gall bladder, spleen and bone marrow further multiplication in the spleen and liver second bacteraemia as organisms re-enter blood this coincides with start of symptoms i.e. the end of the
incubation period Bile is infected and excreted into the lumen of the intestine
resulting in a secondary invasion of the bowel mucosa
(if pre existing Gall Bladder disease - e.g. stones there is a greatly increased risk of chronic carriage)

Pathophysiology• The bacilli avoid immune system largely because they infect but
don't kill macrophages. – The organism multiplies within the macrophage during jopurney through
lymphatics and blood, while evading phagocytosis
– further multiplication occurs in the lymphoreticular system
– as the immune system responds foci of inflammation are seen.
– these foci of infection/inflammation are called typhoid nodules
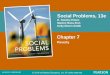
• Peyer's Patches– focus of inflammation in gut lymphoid tissue
– if no resolution, by 7-10 days necrosis occurs and subsequent ulceration
– these intestinal ulcers are responsible for GI bleeding and at times gut perforation

Ulcerated Peyers Patches due to Enteric S typhi

Ulceration in S typhi

Pathophysiology
• Effects on other organs are mediated by a non specific toxin– heart
– muscle
– central nervous system

Clincal: Enteric fever
• Incubation period 7 -21 days, usually 14• untreated course of illness isusually 3 weeks but
may continue for months• few signs or symtpoms are consistently seen other
than– Fever and Headache most common = 90%

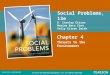
Fever in typhoid
• first week – stepwise increase
• second week – remittant
• third week – falling again
• can be high i.e. 40 degrees • often the patient has a relative bradycardia

others symptoms:
• abdominal pain• constipation• diarrhoea• deafness• cough• psychiatric: psychosis or depression

Signs
• Fever• relative bradycardia• abdominal distension common• hepatomegaly, splenomegaly 25-50%• mental change: confusion, ataxia, tremors, apathy• rose spots (from day 7), red macules that blanch• deafness, meningism• SHOCK if severe e.g. perforation

Presentation
early: fairly well patient, alert not dehydrated
late: toxic, confused and very dehydrated
any system can be involved, so presentation can vary very widely: always suspect

Complications• Perforation
– 5% most likely in 3rd week
• Haemorrhage– from ulcerated Peyer’s patches
• Metastatic infection– abscess or bone infection, poss years later
• Carriage– flukes / stones encourage– Carcinoma of GB late complication

Diagnosis
• Culture
• Serology
• Other tests

Culture
• Blood Culture 40 - 70% sensitivity
– best option to yield result in first week– can be positive at any point in illness– lysis centrifugation )macrophage fraction) more sensitive
• Bone Marrow Culture 95% sensitivity (even if antibiotics)
• Stool Culture– can be positive in first four days after infection (i.e. during
incubation period when patient asymptomatic)– and if diarrhoea present (usually second week)– sensitivity can be increased to 86% using a string capsule
• Rose spot Aspirate, CSF culture, Pus from abscess

SerologyWIDAL TEST
measures antibodies to the somatic 'O' antigen + flagellar 'H' antigen
it is largely useless, especially in an endemic setting
– it is NON SPECIFIC other salmonella infection (even asymptomatic) will give high titres
– titres will be high from previous exposure or immunisation
– four fold increase between illness and convalescence is unhelpful:•titres rise greatly during incubation period and not much thereafter
•the diagnosis is made after the illness has finished
•how many patients will return and pay for a second widal when better
– some culture proven typhoid patients have a 'negative' widal.
antigen based tests are still in development

Other
• WBC – is often normal but both leucocytosis and ‘classic’
leucopaenia are seen.
– if WBC is raised tend to be lymphocytosis
– may have thrombocytopenia
• Chemistry– no specific findings but can get raised transaminases
and bilirubin

Management
• supportive– nursing care is paramount to ensure fluid intake,
sanitation (barrier nurse) and pressure area care
• fluid and electrolyte balance are critical• Antibiotics• Specific interventions

Antimicrobial Therapy
• CHLORAMPHENICOL
• AMOXYCILLIN
• SMP-TMX 'SEPTRIN'
• CIPROFLOXACIN
• CEPHALOSPORINS
• AZITHROMYCIN

‘first line’ agentsChloramphenicol, amoxycillin and cotrimoxazole
– rapid improvement in symptoms– defervessence in 3-5 days
chloramphenicol : 500mg 4 hourly then 6 hourly after defervessence: 14 days total
Co-trimoxazole : 960mg bd– useful for empirical treatment– available and affordable– resistance in Asia, has been seen in Kenya but little
solid data elsewhere

Ciprofloxacinhighly effective
– defervessence 3-5 days– lower rate of carriage and rare relapse– 500mg bd x 14 – very good oral absorption– (only IV required if vomiting or diarrhoea is present)
not recommended in children and pregnancy
resistance emerging already
more costly, not always available

Cephalosporins 3rd genas effectiveall IV and all expensivebut share resistance with first line
AzithromycinVery good tissue penetration and oral preparationworks as well as all otherseffective in resistant casesno problem for children but expensive

specific issues• perforation / haemorrhage
– full iv resuscitation +/- blood– cover for G-ve and anaerobic– EARLY surgery
• typhoid shock– high dose steroids early
• relapse– not due to resistance but recrudescence from GB
• carriers– up to a month of cipropfloxacin