Embed Size (px)
Citation preview

European guidelines: diabetes and cardiovascular disease
Diabetes and Hyperlipidemia
State of the art 2010
Lars RydénKarolinska InstitutetStockholm, Sweden

European guidelines: diabetes and cardiovascular disease
Diabetes and hyperlipidemia

European guidelines: diabetes and cardiovascular disease
Treatment targets
Diabetes and hyperlipidemia

European guidelines: diabetes and cardiovascular disease
Treatment targets
(Rydén, Standl et al Europ Heart J 2007; 28:88 )
Lipid category mmol/l mg/dl
Cholesterol
Total 4.5 <175
LDL ≤1.8 ≤70
HDL men >1.0 >40women >1.2 >46
Triglycerides <1.7 <150
Total/HDL cholesterol <3

European guidelines: diabetes and cardiovascular disease
Treatment targets
Epidemiology and cardiovascular risk
Diabetes and hyperlipidemia

European guidelines: diabetes and cardiovascular disease
(Isomaa et al Diabetes Care 2001;24:683)
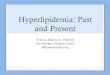
Dyslipidemia - common in diabetes
The BOTNIA studyn 4 483
age years 35–70
Glucose tolerance
Normal 1 988
IFG/IGT 7 98
Diabetes 1 697
DyslipidemiaTG ≥1.7 mmol/l
(≥ 66 mg/dl)
and/or
HDL
men/women <0.9 mmol/l
(35 mg/dl)
women <1.0 mmol/l
(39 mg/dl)
100
80
60
40
20
0
Glucose metabolism
Normal IFG/IGT Diabetes
Male
Female
Pre
vale
nce d
yslip
idem
ia(%
)29 16
45 31
54 56

European guidelines: diabetes and cardiovascular disease
Lipid profile in patients with and without diabetes (1)
(UKPDS Diabetes Care 1997; 20:1663)
DM
No
DM
No
DM DM
Total cholesterol
5.0 193
5.4 206
5.8 224
6.0 232
mmol/l mg/dl
5.6 216
5.2 201
Men Women
LDL-Cholesterol
DM
No
DM
No
DM DM
Men
3.0 116
3.2 124
3.4 131
4.0 154
3.8 147
3.6 139
Women
p<0.001
mmol/l mg/dl

European guidelines: diabetes and cardiovascular disease
Lipid profile in patients with and without diabetes (2)
1 89
1.2 106
1.4 124
1.6 142
1.8 159
2.0 177
Triglycerides
No
DMDM DM
No
DM1.0 39
1.2 46
1.4 54
1.6 62
HDL- Cholesterol
DM DM
No
DM
No
DM
Men
p<0.02
Women
p<0.001
Men
p<0.001
Women
p<0.001
(UKPDS Diabetes Care 1997; 20:1663)
mmol/l mg/dl mmol/l mg/dl

European guidelines: diabetes and cardiovascular disease
Risk factors and diabetes
(Stamler et al. Diabetes Care 1993;16:434)
80
60
40
30
10
5
Serum cholesterol (mmol/L)
No diabetes
Diabetes
4 5 6 7
Vulnerability to
hypercholesterolemia
by diabetic state
10 year CHD mortality
(per 103)
10 y
ear
CH
D m
ort
alit
y
Rate

European guidelines: diabetes and cardiovascular disease
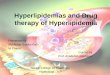
(Turner et al. UKPDS 23. BMJ 1993;98:316)
LDL mmol/l HDL mmol/l Age (years)
0.1 mmol/l (4 mg/dl) increase in HDL
= 15% decrease in CVD endpoints
HbA1c (%) Syst BP (mm Hg) Smoking
Risk factors and diabetes
Estimated
Hazard Ratio
for coronary
artery disease
3 055 patients
with type 2
diabetes in UKPDS

European guidelines: diabetes and cardiovascular disease
Treatment targets
Epidemiology and cardiovascular risk
Statin therapy
Secondary and primary prevention
Diabetes and hyperlipidemia

European guidelines: diabetes and cardiovascular disease
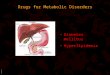
Heart Protection Study – subgroup with diabetes
(HPS Collaborative Group: Lancet 2003; 361: 2005)
Patients
Diabetes n = 5 963
Simvastatin 40 mg/day or placebo
Proportionate reduction %
Coronary mortality 20
Stroke 24
Revascularization 17
Major vascular events 22Simvastatin
Placebo
P<0.0001
Follow up (years)
Majo
r C
V e
vents
(%
)

European guidelines: diabetes and cardiovascular disease
(CTT Collaborators Lancet 2008; 371:117 )
Lancet 2008; 371:117
Risk reduction by LDL reduction and diabetic state
Diabetes (no) 18 686
Type 2 17 220
Events 3 247
Follow up (mean years) 4.3
Outcome measure
Effect of decreasing LDL by 1 mmol/l

European guidelines: diabetes and cardiovascular disease
(CTT Collaborators Lancet 2008; 371:117 )
Reduction by
1 mmol/l (39 mg/dl) decrease in LDL-cholesterol
Event Diabetes No diabetes
Total mortality 0.91 (0.82-1.01) 0.87 (0.82-0.92)
Major vascular 0.79 (0.72-0.86) 0.79 (0.76-0.82)
Major coronary 0.78 (0.69-0.87) 0.77 (0.73-0.81)
Overall reduction 20%
Risk reduction by LDL reduction and diabetic state

European guidelines: diabetes and cardiovascular disease
(CTT Collaborators Lancet 2008; 371:117 )
Reduction by
1 mmol/l (39 mg/dl) decrease in LDL-cholesterol
Subgroups with similar overall reduction
Diabetes type 1 or 2 BMI
Age and sex Smoking status
Blood pressure Other blood lipids
Hypertension Level of CV risk
Initial LDL level down to 2.6 mmol/l (100 mg/dl)
Risk reduction by LDL reduction and diabetic state

European guidelines: diabetes and cardiovascular disease
Statins in patients with and without diabetes
From the 4 S and CARE trials
(Kreisberg RA et al. Am J Cardiol 1998;82:67U)
Diabetes
LDL-Cholesterol
10
2.6100
20
30
40
Majo
r coro
nary
events
(%
) 60
70
3.9 150
5.2200
50
CARE - pravastatin
placebo
4S - simvastatin
statin
mmol/lmg/dl
No diabetes

European guidelines: diabetes and cardiovascular disease
Treating to New Targets – subgroup with diabetes
(Shephard et al: Diabetes care 2006; 29:1220)
Patients n= 1 501Diabetes + CAD + LDL <3.4 mmol/l (<130 mg/dl)
Atorvastatin 10 or 80 mg/day
Follow up (median) 4.9 years
EndpointFirst major CV-event
LDL cholesterol at end of treatmentAtorvastatin 10 2.5 mmol/l (99 mg/dl)
Atorvastatin 80 2.0 mmol/l (77 mg/dl)

European guidelines: diabetes and cardiovascular disease
Treating to New Targets – subgroup with diabetes
(Shephard et al: Diabetes care 2006; 29:1220)
Follow up (years)
Pro
port
ion w
ith m
ajo
r C
V e
vents
(%
)
Atorvastatin 10 mg 18%
Atorvastatin 80 mg 14%
HR 0.75 (95% CI 0.58-0.97)
p = 0.026

European guidelines: diabetes and cardiovascular disease
Guideline recommendations
Secondary prevention Class Level
Elevated LDL- and low HDL are important risk I A
factors in patients with diabetes mellitus
Statins are first line agents for lowering LDL-
cholesterol in diabetic patients I A
In diabetic patients with CVD statin therapy should be I B
initiated regardless of baseline LDL-cholesterol with
a treatment target of ≤1.8-2.0 mmol/l (70-77 mg/dl)
(Rydén, Standl et al Europ Heart J 2007; 28:88 )

European guidelines: diabetes and cardiovascular disease
Patients with type 2 diabetes
Age (years) 40-75
Baseline LDL mmol/l (mg/dl) 3.0 (116)
CVD-manifestation None
Risk factor for CVD ≥1
retinopathy or albuminuria or smoker or hypertension
Randomised treatment
Atorvastatin 10 mg/day n=1 428
Placebo n=1 410
(Colhoun HM et al. Lancet 2004;364:685)
Primary prevention with statins in diabetesThe Collaborative Atorvastatin Diabetes Study (CARDS)

European guidelines: diabetes and cardiovascular disease
Primary prevention with statins in diabetesThe Collaborative Atorvastatin Diabetes Study (CARDS)
(Colhoun HM et al. Lancet 2004;364:685)
0
5
10
15
0 1 2 3 4 4.75
Atorvastatin
Placebo
Follow up (years)
Majo
r coro
nary
events
(%
)
Primary endpoint - major coronary event
-37% (95 CI: -52 to -17; p=0.001)

European guidelines: diabetes and cardiovascular disease
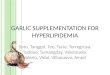
Primary prevention with statins in diabetesThe CARDS trial
(Colhoun HM et al. Lancet 2004;364:685)
Primary
ACS
Coron revasc
Stroke
Mortality
Any CVE
Treatment effects
primary and secondary endpoints
Major CVE
All cause mortality
Any CVE

European guidelines: diabetes and cardiovascular disease
Guideline recommendations
Primary prevention Class Level
Given the high lifetime risk of CVD, it is suggested IIb C
that all type 1 patients above age 40 years should
be considered for statin therapy.
In patients 18-39 years (type 1 or 2), statin therapy
should be considered when other risk factors are
present (e.g. microvasc complications, poor glycemic
control, hypertension, family history….)
(Rydén, Standl et al Europ Heart J 2007; 28:88 )

European guidelines: diabetes and cardiovascular disease
Guideline recommendations
Primary prevention Class Level
Statin therapy should be considered in adult patients IIb B
with type 2 diabetes without CVD if total
cholesterol is >3.5 mmol/l (>135 mg/dl)
targeting a LDL-cholesterol reduction of 30-40%
(Rydén, Standl et al Europ Heart J 2007; 28:88 )

European guidelines: diabetes and cardiovascular disease
Treatment targets
Epidemiology and cardiovascular risk
Statin therapy
Secondary and primary prevention
Fibrates
Diabetes and hyperlipidemia

European guidelines: diabetes and cardiovascular disease
Atheroprotective effects of HDL
(After Barter et al 1999;Harwood Acad Publ)
Promotion of cholesterol efflux
Inhibition of adhesion molecule expression
Inhibition of LDLoxidation

European guidelines: diabetes and cardiovascular disease
Proportionate risk reduction in major fibrate trialsSecondary prevention in patients with diabetes
RR: 68% - MI or sudden death (ns)
GemfibrozilHelsinki Heart Study
RR 23% - combined cardiac endpoints (ns)
DAIS
RR: 70% - definite CHD events (p=0.01)
SENDCAP
Clinical OutcomesFibrateStudy
VA-HIT RR: 32% - composite endpoint (p=0.004)
Patients no
135
Bezafibrate
Gemfibrozil 769
164
Fenofibrate 418
(Koskinen et al. Diabetes Care 1992;15:820. Elkeles et al. Diabetes Care 1998;21:64.
Rubins et al. Arch Int Med 2002;162:2597. DAIS Investigators. Lancet 2001;357:905)

European guidelines: diabetes and cardiovascular disease
Fenofibrate Intervention and Event Lowering in DiabetesThe FIELD trial
PatientsDiabetes ± CVDn = 9 795No statins at entryFenofibrate 200 mg/dayPlacebo
(The FIELD Study Investigators. Lancet 2005; 366:1849)
Coronary deaths or
myocardial infarction
Cum
ula
tive r
isk (
%)

European guidelines: diabetes and cardiovascular disease
Patientsn = 5,518 type 2 diabetes
Simvastatin +Fenofibrate 200 mg/day
PlaceboMean follow up 4.7 years
Endpoint CV death or nonfatal MI or stroke
Accord Study group. New Engl J Med 2010; 362: 1563
The effect of combination lipid therapy in T2 DMThe ACCORD trial

European guidelines: diabetes and cardiovascular disease
Accord Study group. New Engl J Med 2010; 362: 1563
The effect of combination lipid therapy in T2 DMThe ACCORD trial

European guidelines: diabetes and cardiovascular disease
Guideline recommendations
Secondary prevention Class Level
In diabetic patients with hypercholesterolaemia IIb B
>2mmol/l (177 mg/dl) after having reached the
LDL target with statin therapy, statin therapy
should be increased to reduce the secondary target
of non-HDL cholesterol.
In some cases, combination therapy with the
addition of ezetemibe, nicotinic acid or fibrates
may be considered
(Rydén, Standl et al Europ Heart J 2007; 28:88 )

European guidelines: diabetes and cardiovascular disease
Treatment targets
Epidemiology and cardiovascular risk
Statin therapy
Secondary and primary prevention
Fibrates
Multifactorial management
Diabetes and hyperlipidemia

European guidelines: diabetes and cardiovascular disease
Statins in patients with and without diabetes
From the 4 S and CARE trials
(Kreisberg RA et al. Am J Cardiol 1998;82:67U)
Diabetes
LDL-Cholesterol
10
2.6100
20
30
40
Majo
r coro
nary
events
(%
) 60
70
3.9 150
5.2200
50
CARE - pravastatin
placebo
4S - simvastatin
statin
mmol/lmg/dl
No diabetes

European guidelines: diabetes and cardiovascular disease
Diabetes and Hyperlipidemia
Concluding remarks
Diabetes and hyperlipidemia
common combination
with special characteristics
statin treatment rewarding
need for HDL-increasing drugs
Treatment
part of a multifactorial management
present practice far from satisfactory

European guidelines: diabetes and cardiovascular disease
Diabetes and Hyperlipidemia
State of the art
Thanks for the attention!