Embed Size (px)
Citation preview

Dextrocardia
PGI Gamboa, Milrose D.

DEXTROCARDIA
S.A. 35 yr. old Female Molo, Iloilo City CC: Vaginal Spotting Diagnosis: Incomplete Abortion Non-induced
Non-Septic S/P Completion Curettage

Patient has been asymptomatic and was diagnosed to have Dextrocardia on her 3rd pregnancy.
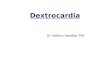
Chest X-ray PA view was requested.


Developmentally, the atria are a continuation of the pulmonary and systemic vasculature; thus, their position is almost always the same as that of the viscera

• Situs describes the position of the cardiac atria and viscera
• Situs solitus is the normal position
• Cardiac situs is determined by the atrial location.

the standard anatomy of situs solitus A) and the mirror image of situs inversus (B). The right lung (RL), left lung (LL), right atrium (RA), and left atrium (LA) are shown.

The term situs inversus is a short
form of the Latin phrase "situs
inversus viscerum," meaning "inverted
position of the internal organs

Situs Inversus Marco Severino first recognized dextrocardia in 1643 Matthew Baillie described the complete mirror-image
reversal of the thoracic and abdominal organs in situs inversus
First seen and drawn by Leonardo da Vinci in 1452–1519 The prevalence of situs inversus varies among different
populations but is less than 1 in 10,000 people.
Situs inversus is present in 0.01% of the population

Situs inversus (also called situs transversus or oppositus) is a congenital condition in which the major visceral organs are reversed or mirrored from their normal positions.
The normal arrangement is known as situs solitus
situs ambiguus or heterotaxy, situs cannot be determined

Effect on Anatomy Generally, the organs are simply transposed through the
sagittal plane In situs inversus, the morphologic right atrium is on the
left, and the morphologic left atrium is on the right. The normal pulmonary anatomy is also reversed so that
the left lung has 3 lobes and the right lung has 2 lobes. In addition, the liver and gallbladder are located on the left, whereas the spleen and stomach are located on the right.
The remaining internal structures are also a mirror image of the normal.


Embryonic Development
Sidedness is one of the earliest changes noted in normal embryologic development
Two symmetrical groups of cells known as precardiac cells migrate toward the central node (an infolding along the primitive streak) and join to form the primitive heart tube
The embryo is symmetric until just after the heart tube is formed.

Shortly thereafter, the heart tube begins to bend to the right.
The primitive heart tube folds and remodels during weeks 4 through 7, gradually becoming the 4-chambered heart and great vessels.
It typically rotates toward the right at the 22nd to 23rd day of development, and the apex moves to the left

Types of situs inversus
Situs inversus can be classified further into: situs inversus with levocardia situs inversus with dextrocardia
independent of the cardiac apical position

The terms levocardia and dextrocardia indicate only the direction of the cardiac apex at birth; do not imply the orientation of the cardiac chambers
Levocardia the base-to-apex axis points to the left
Dextrocardia the axis is reversed

Isolated dextrocardia is also termed situs solitus with dextrocardia The cardiac apex points to the right, the viscera are otherwise in their usual
positions
Situs inversus with dextrocardia is also termed situs inversus totalis The cardiac position, as well as the atrial
chambers and abdominal viscera, is a mirror image of the normal anatomy

Situs ambiguous or heterotaxy situs cannot be determined the liver may be midline, the spleen absent or
multiple, the atrial morphology unclear, and the bowel malrotated.
Often, normally unilateral structures are duplicated or absent
The 2 primary subtypes of situs ambiguous (1) right isomerism, or asplenia syndrome (2) left isomerism, or polysplenia syndrome

Classic right isomerism, or asplenia, bilateral right-sidedness bilateral right atria, a centrally located liver, and an
absent spleen, and both lungs have 3 lobes The descending aorta and inferior vena cava are on the
same side of the spine.
In left isomerism, or polysplenia, bilateral left-sidedness bilateral left atria and multiple spleens, and both lungs
have 2 lobes Interruption of the inferior vena cava with azygous or
hemiazygous continuation is often present

Other features of situs inversus
Situs inversus occurs more commonly with dextrocardia. A 3-5% incidence of congenital heart disease is observed
in situs inversus with dextrocardia, usually with transposition of the great vessels
Of these patients, 80% have a right-sided aortic arch
Situs inversus with levocardia is rare, almost always associated with congenital heart disease Kartagener syndrome is typified by bronchiectasis,
sinusitis, and situs inversus and affects 20% of patients with situs inversus; however, only 50% of patients with Kartagener syndrome have situs inversus

Diagnosis
Segmental approach for evaluating cardiac anatomy in the patient with a congenital heart abnormality:
Determine the position of the atria, viscera, right and left ventricles, and great vessels

(Atria)
Positioning is described as levocardia if the heart is on the left, dextrocardia if on the right, and mesocardia if in the center
Dextroposition Displacement of the heart to the right as a
result of another condition, such as scoliosis or a hypoplastic lung

(Viscera)
When the internal abdominal organs, atria, and lungs are positioned normally, it is called situs solitus.
If the position of the viscera, lungs, and atria is reversed, it is called situs inversus. The term situs ambiguus is used to describe an indeterminate visceroatrial sidedness.

Situs ambiguus is further divided according to its occurrence with asplenia or with polysplenia.
In situs ambiguus with asplenia, there is usually a central liver, 2 right lungs, and no spleen.
In situs ambiguus with polysplenia, there are 2 left lungs, multiple small spleens, and anomalous development of the intrahepatic vena cava.
These 2 variations are sometimes thought of as having bilateral left (polysplenia) or right (asplenia) sides.

(Ventricles) D-loop
the orientation of the right and left ventricles is normal the right ventricular inflow tract is to the right of the left
ventricle.
L-loop the position of the ventricles is reversed and therefore the right
ventricle is to the left of the left ventricle
X-loop In situs ambiguus, neither an L-loop nor D-loop can be identified,
The loops can be further described as concordant if their position matches the visceroatrial situs and discordant if they do not

(Vessels) The vessels are designated as normal if the pulmonary artery
arises from the right ventricle and the aorta from the left ventricle
In levocardia, the position is referred to as solitus normal, or D-normal;
In dextrocardia, it is inverted normal, or L-normal. The vessels are transposed if the aorta arises from the right
ventricle and the pulmonary artery from the left ventricle. The vessels may also demonstrate double-outlet right ventricle,
double-outlet left ventricle, truncus arteriosis, or other abnormal positioning, which has been referred to as malposition.

Significance

Situs inversus is generally an autosomal recessive condition, although it can be X-linked or found in identical "mirror" twins

In the absence of congenital heart defects, individuals with situs inversus are phenotypically unimpaired, and can lead normal healthy lives, without any complications related to their medical condition.
There is a 5–10% prevalence of congenital heart disease in individuals with situs inversus totalis, most commonly transposition of the great vessels
The incidence of congenital heart disease is 95% in situs inversus with levocardia.

The exact cause of dextrocardia with situs inversus is not known, but the condition results from the abnormal positioning of the internal organs during fetal development.
More than 40 genes have been identified as being required for the positioning and patterning of the organs in the body.

Mutations in 9 different genes have been reported in individuals with either heterotaxy syndrome or situs inversus totalis, which suggests that in at least some individuals with either of these conditions, the cause may be genetic.
However, because a specific genetic cause has not been identified (and inheritance patterns have not been confirmed), it is difficult to estimate recurrence risks for the condition.

Kartagener Syndrome
About 25% of individuals with situs inversus have an underlying condition known as primary ciliary dyskinesia (PCD) dysfunction of the cilia that manifests itself during
the embryologic phase of development. Normally-functioning cilia determine the position
of the internal organs during early embryological development, and so individuals with PCD have a 50% chance of developing situs inversus.
Kartagener syndrome characterized by the triad of situs inversus,
chronic sinusitis, and bronchiectasis

Primary ciliary dyskinesia to result from mutations in several different
genes, but in many cases, the cause of the disorder is unknown.
This condition is typically inherited in an autosomal recessive pattern, which means both copies of the gene in each cell have mutations.

Radiography
In most patients with situs inversus, chest radiography shows dextrocardia, with the cardiac apex pointing to the right and the aortic arch and stomach bubble located on the right as well

Posteroanterior chest radiograph in a 40-year-old man with situs inversus and dextrocardia. This image shows that the cardiac apex (*) points to the right. A right-sided aortic arch (A) is associated with slight deviation of the trachea (T) to the left. The stomach (S) bubble is visible in the right upper quadrant.

Confirming a mirror-image position of the atria allows confident diagnosis of situs inversus if the viscera are also reverse
The atrial morphology cannot be discerned on chest radiographs, but it can be determined indirectly by evaluating the bronchi
the side of the morphologic bronchus corresponds to the side of the morphologic atrium
If a minor fissure can be identified, by inference, an eparterial bronchus and morphologic right atrium exist on that side.

Upper and lower gastrointestinal examinations are usually not performed for the diagnosis of situs inversus
However, situs inversus may be found incidentally during such examinations
In an upper gastrointestinal examination in a patient with situs inversus, the stomach is on the right, with the C loop of the duodenum curving to the left
The liver and spleen are also in mirror-image locations compared with their normal position.
In a barium enema examination, the sigmoid colon curves to the right, leading to a right-sided descending colon and terminating in a left-sided cecum


The degree of confidence of radiographs is high. CT scan findings can be used to resolve any remaining questions.

Long-term Sequelae
Long-term prognosis depends on associated congenital defects and the presence of cardiovascular compromise.
Most patients with dextrocardia with situs inversus do not have any significant cardiac defects, and their life expectancy is normal.
Those who have ciliary defects require frequent treatment for chronic pulmonary infections and complications.

Situs ambiguus is almost always associated with severe cardiovascular impairment; often, congenital anomalies occur in other organ systems as well.
Patients with asplenia have the additional problem of recurrent, severe infections that contribute to their higher mortality rate.

Electrocardiographic (ECG) differences can be minimized by reversing the precordial leads and the right and left arm leads.
The P waves, QRS complex, and T waves are all inverted in lead I.
Patients with heterotaxy who need cardiac evaluation should undergo echocardiography and/or cardiac catheterization when possible because of their high incidence of cardiac anomalies.

Angiography
Angiography is unnecessary for the diagnosis of situs inversus. In fact, noninvasive methods are preferred.
Although the atrial morphology can be analyzed to determine atrial situs, angiography is usually reserved for the evaluation of congenital heart disease

Thank you!



![Dextrocardia with Situs Inversus, Atrio-ventricular and ...dextrocardia to be associated with situs solitus in 64%, situs inversus in 27%, and situs ambiguous in 9% [2]. In our case](https://img.pdfslide.us/doc/110x75/608c25297b80eb7d6b550573/dextrocardia-with-situs-inversus-atrio-ventricular-and-dextrocardia-to-be-associated.jpg)





![New technique Right Anterior Small Thoracotomy (RAST ... · fore operating on a patient with dextrocardia through a right thoracotomy[4], ... he had PTCA stents two times in 1996](https://img.pdfslide.us/doc/110x75/5e527b73d5ff46443a61ad6f/new-technique-right-anterior-small-thoracotomy-rast-fore-operating-on-a-patient.jpg)