Embed Size (px)
Citation preview

DEVELOPMENT OF
AUTOIMMUNITY
ARPAD LANYI PhD

CENTRAL AND PERIPHERAL TOLERANCE
TO SELF ANTIGENS
Central tolerance:
Elimination of self-reactive clones.
BUT!!! Some clones escape.
Peripheral tolerance:
Elimination of „fugitive” or altered clones is an important
role for regulatory T-cells.

Normal tissue cells do not express MHC class II
NO SIGNAL 1. for CD4+ Th activation
Normal tissue cells do not express co-stimulatory molecules
and do not produce T-cell differentiating cytokines
NO SIGNAL 2. for CD4+ Th activation
Migration of naive T lymphocytes to normal tissues is limited
Antigen presenting cells are not activated in normal tissues
UNDER NORMAL CIRCUMSTANCES PERIPHERAL TISSUES ARE PROTECTED
FROM IMMUNE RESPONSE
IMMUNE RESPONSES ARE NOT INITIATED IN THE PERIPHERY

GENERAL FEATURES OF AUTOIMMUNE DISORDERS
Autoimmune diseases may be either systemic or organ specific, depending on the distribution of the autoantigens that are recognized.
• Circulating immune complexes – SLE • Autoantibodies or T-cell responses against self antigens
with restricted tissue distribution - Type 1 diabetes
Various effector mechanisms are responsible for tissue injury in different autoimmune diseases.
• Autoantibodies• Immune complexes• Autoreactive T lymphocytes
All autoimmune diseases involve breaking T-cell tolerance.

AUTOANTIBODY PRODUCTION IS DEPENDENT ON THE
AVAILABILITY OF AUTOREACTIVE T-CELLS
Practically all autoimmune diseases
involve some T-cell defects
In the absence of T-cell help autoreactive
B-cells are retained in the T-cell zone and
die by apoptosis

SINGLE GENE MUTATIONS CAUSE AUTOIMMUNITY
• AIRE - Failure of central tolerance - APECED

AUTOIMMUN REGULATOR (AIRE)A transcription factor expressed by thymic medullary
epithelial cells and induces expression of many tissue-specific genes
Deficiency in establishing central T-cell tolerance
allows too many
self reactive T-cell clones to leave the thymus
AUTOIMMUNE POLYENDOCRINOPATHY-
CANDIDIASIS-ECTODERMAL DYSTROPHY
(APECED)
Rare disease, but more frequently seen in inbred
populations
Finnish, Iranian Jews and in the island of Sardine

SYMPTOMS OF APECED
• Anti-Th17 specific antibodies!!!!!
• Role of Th17 discovered by studying a rare immunodeficiency
• https:///jimneydandme.wordpress.com/james-story

SINGLE GENE MUTATIONS CAUSE AUTOIMMUNITY
• AIRE - Failure of central tolerance - APECED•FOXP3 – Deficiency of functional regulatory T cells - IPEX•CTLA4 - Failure of anergy in CD4+ T cells; defective function of regulatory T cells - several autoimmune disorders•CD25 - Defective development, survival, or function of regulatory T-cells – IPEX-like•C4 - Defective clearance of immune complexes; failure of B cell tolerance – SLE•FAS/FASL - Defective deletion of anergic self-reactive B cells; reduced deletion of mature CD4+T cells - Autoimmune lymphoproliferative syndrome (ALPS)
These genes are associated with rare autoimmune diseases, their identification
has provided valuable information about the importance of various molecular
pathways in the maintenance of self-tolerance.

MOST AUTOIMMUNE DISEASES ARECOMPLEX
POLYGENIC TRAITS
MULTIPLE INHERITED GENETIC POLYMORPHISMSCONTRIBUTE TO
DISEASE SUSCEPTIBILITY

HLA IS THE DOMINANT GENETIC FACTOR AFFECTING
SUSCEPTIBILITYTO AUTOIMMUNE DISEASE
Family studies reveal that HLA type
correlateswith susceptibility to type 1
diabetes
Similar results are seen for manyautoimmune diseases
Haplotype is a group of genes within an
organism that was inherited together from a single parent

ASSOCIATIONS OF HLA ALLOTYPES WITH AUTOIMMUNE DISEASE
HLA associations reflect the
importance of T-cell
tolerance in preventing
autoimmunity
Many more autoimmune
diseases are associated with
HLA II than with HLA I
indicating that CD4+T-cells are
inherently more likely
to lose tolerance to a self antigen
than are CD8+T-cells

PREFERENTIAL ALLELE ASSOCIATIONS:
LINKAGE DISEQUILIBRIUMParticular alleles of the different polymorphic genes
arecombined in HLA haplotypes at frequencies higher
than expected by chanceA1–B8–DR3–DQ2 haplotype, which includes alleles for HLA-A, -B, -C, -DR, and -DQ is characteristic of Caucasian populations (up to 11%).
Association with several common autoimmune diseases: type 1 diabetes, SLE, myasthenia gravis, autoimmune hepatitis, primary biliary cirrhosis.

COMBINATIONS OF HLA CLASS IIALLOTYPES CONFER
SUSCEPTIBILITY TO TYPE 1 DIABETES
Common Caucasian HLA haplotypes that encode either the DQ2 or the DQ8 allotype confer susceptibility to type 1 diabetes.
Heterozygous individuals are more susceptible to diabetes.
This augmented susceptibility is due to a novel HLA-DQ heterodimer consisting of the DQ8 α-chain and the DQ2 β-chain.

POLYMORPHISMS IN NON-HLA GENES ASSOCIATED WITH AUTOIMMUNITY

GENETIC PREDISPOSITION IS NOT EQUAL TO AUTOIMMUNE DISEASE
INDIVIDUALS WITH GENETIC PREDISPOSITION
DEVELOP AUTOIMMUNE DISEASE
WITH A MAXIMUM FREQUENCY OF 20%
ENVIRONMENTAL FACTORS PLAY AROLE
IN DEVELOPING OF AUTOIMMUNITY

DRUG INDUCED HEMOLYTIC ANEMIA
• Alpha methyldopa therapy results in the formation of red blood cell autoantibodies in 10-20% of patients taking the drug for longer than 4 months. True autoantibodies: directed against an autoantigen on the red
blood cell membrane, not against the drug The target membrane antigen is usually within the Rhesus system
• Drug-dependent Abs Penicillin, cefotetan: covalently bind to rbc membrane proteins.
o Anti-drug Ab (usually IgG) - attaches to the drug-coated RBCs - clearance by macrophages
Ceftriaxone: binds non-specifically to RBC membrane proteinso Abs are formed to the combined membrane-drug (hapten)
complex, can be IgM or IgG, and often activate complement - acute rapid intravascular hemolysis

SMOKING
Smoking damages the mucosa of the airways and exacerbates many diseases.
All patients with Goodpasture’s syndrome develop glomerulonephritis, but only those who habitually smoke cigarettes develop pulmonary hemorrhage.
In nonsmokers, the basement membranes of lung alveoli are inaccessible to antibodies.
In smokers the lack of integrity gives circulating antibodies access to the basement membranes.

PHYSICAL TRAUMA

INFECTIONS:
ENVIRONMENTAL FACTORS THAT CAN TRIGGER
AUTOIMMUNE DISEASE

ROLE OF INFECTIONS IN THE DEVELOPMENT OF AUTOIMMUNITY
MOLECULAR MIMICRY MAY LEAD TO SEVERE AUTOIMMUNE
REACTIONS

INFECTIONS ASSOCIATED WITH THE START OF AUTOIMMUNITY

ANTIBODIES AGAINST STREPTOCOCCAL CELL-WALL ANTIGENSCROSS-REACT WITH ANTIGENS ON HEART TISSUE

• In response to IFN-γ MHCII expression is induced on thyroid cells (on the β cells of the pancreas as well as on microglia).
• Insufficient for the activation of naive T-cells (not normally present in the periphery anyway), BUT effector T-cells cross-reacting with autoantigens may be activated.
INDUCTION OF HLA CLASS II EXPRESSION ON TISSUE CELLS
FACILITATES AUTOIMMUNITY

GENETIC AND ENVIRONMENTAL FACTORSACT TOGETHER
TO CAUSE AUTOIMMUNITY

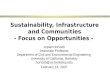
smokers
nonsmokers
Smoking, HLA-DR4 and an
immune response to citrullinated proteins are all tied together in
the same disease-causing
mechanism
Basic residues in the peptide-binding groove of the DRβ*04 chain are
necessary to confer susceptibility to
rheumatoid arthritis
Smoking is the major environmental factor
associated with rheumatoid arthritis
ACPA+: strong association with
HLA-DR4 and smoking
APCA-: no association
RHEUMATOID ARTHRITIS IS INFLUENCEDBY GENETIC AND ENVIRONMENTAL FACTORS

INTERPLAY BETWEEN GENETIC AND ENVIRONMENTAL FACTORS:
CELIAC DISEASEStrong genetic predisposition: DQ2, DQ8 allotypes – celiac disease - 80% DQ2 (the same DQ allotypes that predispose to type 1 diabetes)
Caucasian populations • bread: staple• DQ2:30%• Celiac disease: 0.5-1%• The concordance rate in monozygotic twins: 75-
80%
Environmental factors:• Antibodies, memory T-cells – cross-reaction• Repeated infections with rotavirus• IFN-γ therapy (hepatitis)• Gluten introduction – maternal IgA

ROLE OF THE GUT MICROBIOTA IN AUTOIMMUNITY
doi:10.1038/nri3430
doi:10.1038/nri3430

doi:10.1038/nri3430
doi:10.1038/nm0911-1055
ROLE OF THE GUT MICROBIOTA IN AUTOIMMUNITY

ROLE OF OTHER INTRINSIC FACTORS IN AUTOIMMUNITY

Most autoimmune diseases are more prevalent in women than men.
Conservative estimates indicate that nearly 80% of
individuals with autoimmune diseases are women.
Ankylosing spondylitis occurs more frequently in men.
HORMONES

SENESCENCE OF THE THYMUS
AND THE T-CELL POPULATIONCONTRIBUTES TOAUTOIMMUNITYT-cell populations are dynamic:
• T-cells must divide periodically to survive.
• 1% of the body’s T-cells being replaced each day.
Once the thymus can no longer fulfill the demand for naive T-cells, the immune system compensates:
• expanding the size of existing T-cell clones
• altering the properties of T-cells - make them more resistant to apoptosis; CD28 - KIRRA: large clones of expanded autoreactive CD4 T-
cells
• lack of CD28
• express NK-cell receptors - KIR2DS2
• produce large amounts of IFN-γ
• not anergic

Self antigens are persistent, and once an immune response starts,
many amplification mechanisms are activated that perpetuate the
response Tissue injures result in the release and alterations of other tissue
antigens, activation of lymphocytes specific for these other antigens,
and exacerbation of the disease
AUTOIMMUNE DISEASES TEND TO BE CHRONIC, PROGRESSIVE AND SELF-
PERPETUATING

MECHANISMS OF CHRONICITY OF AUTOIMMUNE DISEASES

PEMPHIGUS FOLIACEUS
INTRAMOLECULAR EPITOPE SPREADING

INTERMOLECULAR EPITOPE SPREADING IN SLE

DYSFUNCTION OF REGULATORY T-CELLS

FOXP3 deficiency: IPEX
)
IL-6 mediated resistance in psoriasis
Autoimmunity in Dry Eye:
qualitative Treg defect – resistance Th17 cells
CTLA-4 haploinsufficiency: autoimmunity
IL-10: severe colitis
doi:10.1038/nri2889
LOSS OF REGULATION OF AUTOREACTIVE T-CELLS RESULTS IN AUTOIMMUNITY

Average Pixel Density within Indicated Cellsa
Average Pixel Density within Keratinocytesa pb
Fold Increase over
Keratinocytesc
CD11c+ 966.5 ± 30.3 587.1 ± 30.6 0.039 1.98 ± 0.37
CD3+ 914.1 ± 35.7 676.2 ± 21.3 0.0044 1.38 ± 0.09
Mac387+ 1014.0 ± 38.4 958.9 ± 28.7 0.4056 1.08 ± 0.06
CD31+ 1495.2 ± 81.2 832.3 ± 36.3 0.0015 1.87 ± 0.23
IL-6 MEDIATED RESISTANCE IN PSORIASIS
IL-6 is overexpressed in
lesional psoriatic skin
Immune cell subsets including DCs, as well as CD31+ endothelial cells, represent major sources of IL-6 in lesional psoriatic skin
IL-6 is necessary and
sufficient for reversal
of Treg suppressive
function
10.4049/jimmunol.0803721

AUTOIMMUNITY IN DRY EYE: DEFECT IN TREGS IS QUALITATIVE NOT QUANTITATIVE
doi: 10.4049/jimmunol.182.3.1247

THANK YOU

ROLE OF INFECTIONS IN THE DEVELOPMENT OF AUTOIMMUNITY
MOLECULAR MIMICRY MAY LEAD TO SEVERE AUTOIMMUNE
REACTIONS

smokers
nonsmokers
Smoking, HLA-DR4 and an
immune response to citrullinated proteins are all tied together in
the same disease-causing
mechanism
Basic residues in the peptide-binding groove of the DRβ*04 chain are
necessary to confer susceptibility to
rheumatoid arthritis
Smoking is the major environmental factor
associated with rheumatoid arthritis
ACPA+: strong association with
HLA-DR4 and smoking
APCA-: no association
RHEUMATOID ARTHRITIS IS INFLUENCEDBY GENETIC AND ENVIRONMENTAL FACTORS