Embed Size (px)
Citation preview

Paediatrics
Developmental anatomy of the airwayedward doyle
Abstractthe airway develops from the primitive foregut and a number of
congenital anomalies may result when this process is abnormal. the
anatomy of the neonatal airway is significantly different from older
children and adults. the larynx is cephalad, the epiglottis large and
the cricoid cartilage is the narrowest part of the upper airway. the
technique of endotracheal intubation is significantly different in ne-
onates compared with older children and adults. a straight-bladed
laryngoscope and an uncuffed endotracheal tube are usually used.
during the first years of life the anatomy gradually becomes more
like that of adults. By the age of 8–10 years normal children have an
airway that is anatomically adult in most ways other than absolute
size. the technique used for endotracheal intubation in adults is ap-
propriate, including the use of a Macintosh laryngoscope blade and a
cuffed endotracheal tube.
Keywords endotracheal tube; epiglottis; paediatric airway
Embryonic development
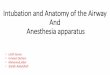
Development of the human airway starts during the 4th week of gestation. The airway originates from the median laryngotracheal groove, an anterior feature of the primitive pharynx. The groove deepens and its lips fuse to form a septum converting the groove into the laryngotracheal tube. The tube is lined with endoderm, and from this the epithelial lining of the respiratory tract develops. The cranial end of the tube forms the larynx, its succeeding part the trachea. From the caudal end two lateral outgrowths arise and form the stem bronchi as well as the left and right lung buds. By 6 weeks of gestation it is possible to identify the rudimentary epiglottis and arytenoids. If epithelial fusion between the two sides of the developing larynx fails to regress the clinical manifestation is a degree of laryngeal atresia ranging from an anterior laryngeal web to complete occlusion of the larynx (Figure 1). A laryngeal cleft is the result of incomplete fusion of the tracheooesophageal septum or cricoid cartilage. Abnormal development of the tracheooesophageal septum results in a tracheooesophageal fistula.
Edward Doyle, MD, FRCA, is a consultant paediatric anaesthetist at the
Royal Hospital for Sick Children, Edinburgh, UK. Conflicts of interest:
none declared.
aNaestHesia aNd iNteNsiVe care MediciNe 10:4 183
The airway at birth
At birth the cricoid cartilage lies at the level of C3/4. The view at direct laryngoscopy is often described as anterior but is in fact cephalad. The epiglottis is well developed (often described as omega shaped) and prominent, projecting backwards at an angle of 45° to the vertical. The mandible is relatively underdeveloped and is combined with a prominent midface that results in a degree of micrognathia. To facilitate suckling, the tongue is large in relation to the oral cavity. Neonates are unable to interrupt ventilation while suckling and swallowing and must be able to suckle and breathe simultaneously. The apposition of epiglottis and uvula in the midline effectively separates a midline pathway into the trachea for air (neonates are nasal breathers) and two lateral channels (piriform fossae) leading into the oesophagus for milk. Infants have a relatively large head with a prominent occiput. The autoflexion that results may make the view at direct laryngoscopy incomplete. This may be countered by supporting the shoulders. The combination of relative micrognathia and a large tongue can make mask ventilation difficult. The large tongue, micrognathia, prominent occiput, cephalad larynx and prominent epiglottis can make laryngoscopy and endotracheal intubation awkward for those more familiar with adult anatomy. This combination of factors means that a straightbladed laryngoscope, used with the tip of the blade on the underside of the epiglottis, is the appropriate technique for laryngoscopy.
Weak intercostal and diaphragmatic muscles (owing to a lack of type I fibres) with a more horizontal attachment and a protuberant abdomen result in less efficient ventilation than in adults. There is limited respiratory reserve and earlier onset of fatigue if the work of ventilation increases during anaesthesia or illness. Specific compliance of the respiratory system is similar in different age groups. Chest wallspecific compliance, however, is higher in neonates and infants (0.06 ml/cm/ml H2O compared with 0.04 ml/cm/ml H2O) because of the cartilaginous ribs and lack of chest wall musculature. This explains why intercostal recession or even sternal recession occur so readily in neonates and young infants with increased respiratory effort and during episodes of airway obstruction.
Figure 1 endoscopic view of the larynx of an infant with stridor,
showing an anterior web occupying at least 90% of the glottis. a Fused
vocal cords; b airway.
reproduced, with permission, from Kubba M, Moores t. Anaesthesia
and Intensive Care Medicine 2006; 7: 158–60.
© 2009 elsevier Ltd. all rights reserved.
Paediatrics
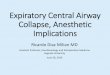
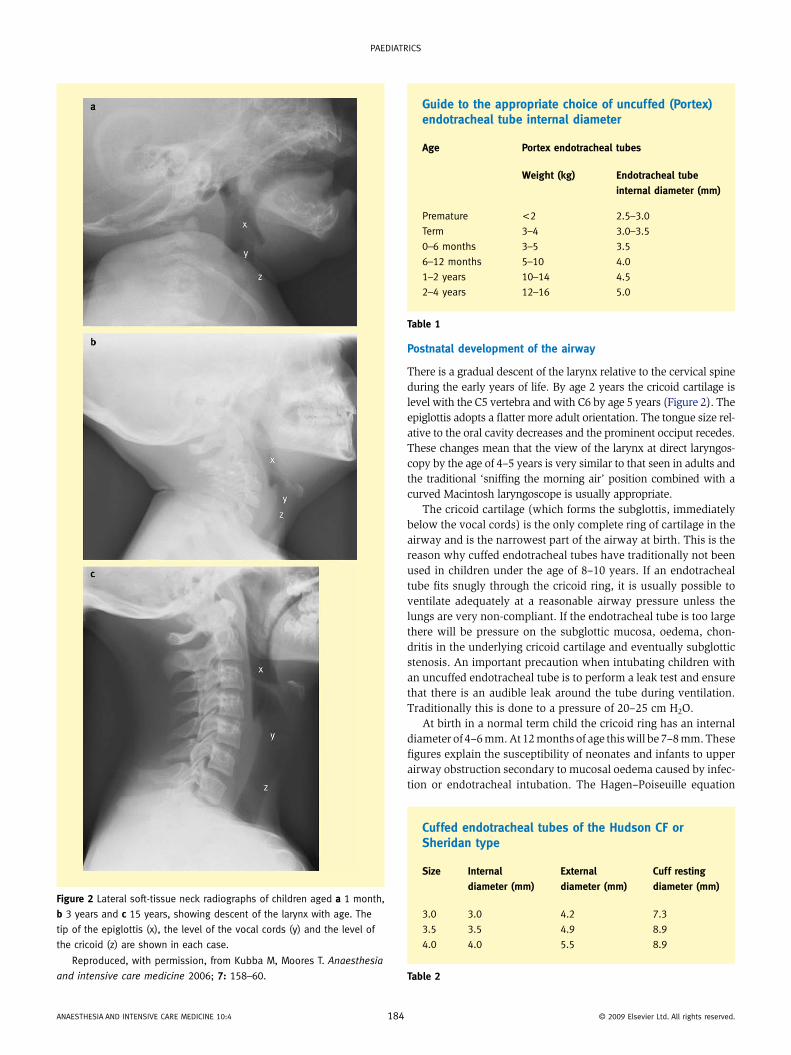
Figure 2 Lateral soft-tissue neck radiographs of children aged a 1 month,
b 3 years and c 15 years, showing descent of the larynx with age. the
tip of the epiglottis (x), the level of the vocal cords (y) and the level of
the cricoid (z) are shown in each case.
reproduced, with permission, from Kubba M, Moores t. Anaesthesia
and intensive care medicine 2006; 7: 158–60.
aNaestHesia aNd iNteNsiVe care MediciNe 10:4 18
Postnatal development of the airway
There is a gradual descent of the larynx relative to the cervical spine during the early years of life. By age 2 years the cricoid cartilage is level with the C5 vertebra and with C6 by age 5 years (Figure 2). The epiglottis adopts a flatter more adult orientation. The tongue size relative to the oral cavity decreases and the prominent occiput recedes. These changes mean that the view of the larynx at direct laryngoscopy by the age of 4–5 years is very similar to that seen in adults and the traditional ‘sniffing the morning air’ position combined with a curved Macintosh laryngoscope is usually appropriate.
The cricoid cartilage (which forms the subglottis, immediately below the vocal cords) is the only complete ring of cartilage in the airway and is the narrowest part of the airway at birth. This is the reason why cuffed endotracheal tubes have traditionally not been used in children under the age of 8–10 years. If an endotracheal tube fits snugly through the cricoid ring, it is usually possible to ventilate adequately at a reasonable airway pressure unless the lungs are very noncompliant. If the endotracheal tube is too large there will be pressure on the subglottic mucosa, oedema, chondritis in the underlying cricoid cartilage and eventually subglottic stenosis. An important precaution when intubating children with an uncuffed endotracheal tube is to perform a leak test and ensure that there is an audible leak around the tube during ventilation. Traditionally this is done to a pressure of 20– 25 cm H2O.
At birth in a normal term child the cricoid ring has an internal diameter of 4–6 mm. At 12 months of age this will be 7–8 mm. These figures explain the susceptibility of neonates and infants to upper airway obstruction secondary to mucosal oedema caused by infection or endotracheal intubation. The Hagen–Poiseuille equation
Guide to the appropriate choice of uncuffed (Portex) endotracheal tube internal diameter
Age Portex endotracheal tubes
Weight (kg) Endotracheal tube
internal diameter (mm)
Premature <2 2.5–3.0
term 3–4 3.0–3.5
0–6 months 3–5 3.5
6–12 months 5–10 4.0
1–2 years 10–14 4.5
2–4 years 12–16 5.0
Table 1
Cuffed endotracheal tubes of the Hudson CF or Sheridan type
Size Internal
diameter (mm)
External
diameter (mm)
Cuff resting
diameter (mm)
3.0 3.0 4.2 7.3
3.5 3.5 4.9 8.9
4.0 4.0 5.5 8.9
Table 2
4 © 2009 elsevier Ltd. all rights reserved.
Paediatrics
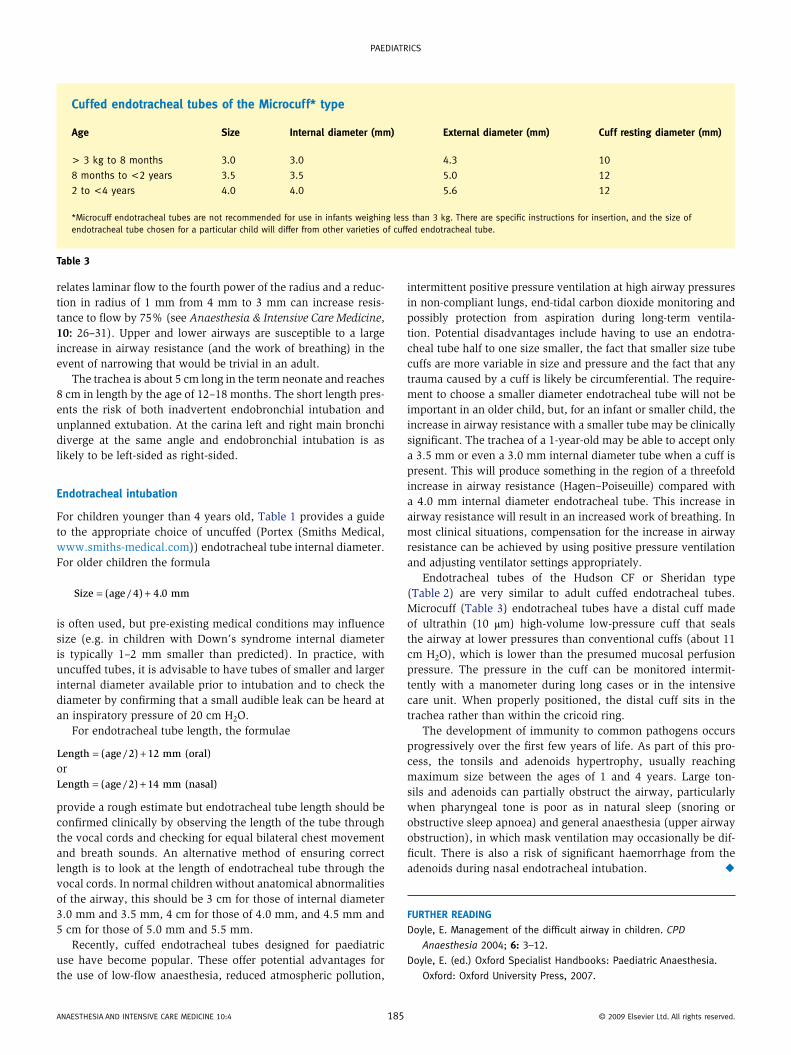
Cuffed endotracheal tubes of the Microcuff* type
Age Size Internal diameter (mm) External diameter (mm) Cuff resting diameter (mm)
> 3 kg to 8 months 3.0 3.0 4.3 10
8 months to <2 years 3.5 3.5 5.0 12
2 to <4 years 4.0 4.0 5.6 12
*Microcuff endotracheal tubes are not recommended for use in infants weighing less than 3 kg. there are specific instructions for insertion, and the size of endotracheal tube chosen for a particular child will differ from other varieties of cuffed endotracheal tube.
Table 3
relates laminar flow to the fourth power of the radius and a reduction in radius of 1 mm from 4 mm to 3 mm can increase resistance to flow by 75% (see Anaesthesia & Intensive Care Medicine, 10: 26–31). Upper and lower airways are susceptible to a large increase in airway resistance (and the work of breathing) in the event of narrowing that would be trivial in an adult.
The trachea is about 5 cm long in the term neonate and reaches 8 cm in length by the age of 12–18 months. The short length presents the risk of both inadvertent endobronchial intubation and unplanned extubation. At the carina left and right main bronchi diverge at the same angle and endobronchial intubation is as likely to be leftsided as rightsided.
Endotracheal intubation
For children younger than 4 years old, Table 1 provides a guide to the appropriate choice of uncuffed (Portex (Smiths Medical, www.smithsmedical.com)) endotracheal tube internal diameter. For older children the formula
Size age . mm= +( / )4 4 0
is often used, but preexisting medical conditions may influence size (e.g. in children with Down’s syndrome internal diameter is typically 1–2 mm smaller than predicted). In practice, with uncuffed tubes, it is advisable to have tubes of smaller and larger internal diameter available prior to intubation and to check the diameter by confirming that a small audible leak can be heard at an inspiratory pressure of 20 cm H2O.
For endotracheal tube length, the formulae
Length age mm (oral)= +( / )2 12orLength age mm (nasal)= +( / )2 14
provide a rough estimate but endotracheal tube length should be confirmed clinically by observing the length of the tube through the vocal cords and checking for equal bilateral chest movement and breath sounds. An alternative method of ensuring correct length is to look at the length of endotracheal tube through the vocal cords. In normal children without anatomical abnormalities of the airway, this should be 3 cm for those of internal diameter 3.0 mm and 3.5 mm, 4 cm for those of 4.0 mm, and 4.5 mm and 5 cm for those of 5.0 mm and 5.5 mm.
Recently, cuffed endotracheal tubes designed for paediatric use have become popular. These offer potential advantages for the use of lowflow anaesthesia, reduced atmospheric pollution,
aNaestHesia aNd iNteNsiVe care MediciNe 10:4 18
intermittent positive pressure ventilation at high airway pressures in noncompliant lungs, endtidal carbon dioxide monitoring and possibly protection from aspiration during longterm ventilation. Potential disadvantages include having to use an endotracheal tube half to one size smaller, the fact that smaller size tube cuffs are more variable in size and pressure and the fact that any trauma caused by a cuff is likely be circumferential. The requirement to choose a smaller diameter endotracheal tube will not be important in an older child, but, for an infant or smaller child, the increase in airway resistance with a smaller tube may be clinically significant. The trachea of a 1yearold may be able to accept only a 3.5 mm or even a 3.0 mm internal diameter tube when a cuff is present. This will produce something in the region of a threefold increase in airway resistance (Hagen–Poiseuille) compared with a 4.0 mm internal diameter endotracheal tube. This increase in airway resistance will result in an increased work of breathing. In most clinical situations, compensation for the increase in airway resistance can be achieved by using positive pressure ventilation and adjusting ventilator settings appropriately.
Endotracheal tubes of the Hudson CF or Sheridan type (Table 2) are very similar to adult cuffed endotracheal tubes. Microcuff (Table 3) endotracheal tubes have a distal cuff made of ultrathin (10 μm) highvolume lowpressure cuff that seals the airway at lower pressures than conventional cuffs (about 11 cm H2O), which is lower than the presumed mucosal perfusion pressure. The pressure in the cuff can be monitored intermittently with a manometer during long cases or in the intensive care unit. When properly positioned, the distal cuff sits in the trachea rather than within the cricoid ring.
The development of immunity to common pathogens occurs progressively over the first few years of life. As part of this process, the tonsils and adenoids hypertrophy, usually reaching maximum size between the ages of 1 and 4 years. Large tonsils and adenoids can partially obstruct the airway, particularly when pharyngeal tone is poor as in natural sleep (snoring or obstructive sleep apnoea) and general anaesthesia (upper airway obstruction), in which mask ventilation may occasionally be difficult. There is also a risk of significant haemorrhage from the adenoids during nasal endotracheal intubation. ◆
FurTHEr rEADInG
doyle, e. Management of the difficult airway in children. CPD
Anaesthesia 2004; 6: 3–12.
doyle, e. (ed.) Oxford specialist Handbooks: Paediatric anaesthesia.
Oxford: Oxford University Press, 2007.
5 © 2009 elsevier Ltd. all rights reserved.