Embed Size (px)
Citation preview
Development of a novel endothelial cell-seededendovascular stent for intracranial aneurysm therapy
Wei Zhu,1,2 Yanlong Tian,1 Liang-Fu Zhou,1 Yang Wang,3,4 Donglei Song,1 Ying Mao,1 Guo-Yuan Yang21Department of Neurosurgery, Huashan Hospital of Fudan University, Shanghai, China2Center for Cerebrovascular Research, Department of Anesthesia and Perioperative Care, University of California,San Francisco, San Francisco, California3Department of Anatomy, Shanghai Medical School, Fudan University, Shanghai, China4Department of Histology and Embryology, Shanghai Medical School, Fudan University, Shanghai, China
Received 13 April 2007; revised 30 May 2007; accepted 18 June 2007Published online 17 September 2007 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/jbm.a.31592
Abstract: The metallic stent has been widely used in endo-vascular treatment of intracranial aneurysms and arterial ste-nosis. Endothelialization at the neck of the aneurysm or ste-notic lesion after stent deployment plays a pivotal role in pre-venting aneurysm recurrence, as well as local thrombusformation and restenosis. To deliver autologous endothelialcells and to promote the endothelialization on the luminalwall of the parent artery, we established an endothelial cell-seeded intracranial stent device. Endothelial cells were iso-lated from canine jugular vein and identified by FACS assayand immunohistochemistry. We demonstrated that theseeded endothelial cells formed a confluent endothelial layer
on the stent’s surface. After being brushed with 100 dyne/cm2 of shear stress, we found that this endothelial layerremained intact for at least 48 h on the heparinized polymercoated stent, rather than the poly-lactic-acid coated stent (p <0.05). The results suggest that an autologous endothelialcell-seeded stent may be a feasible and optimal tool for endo-thelial delivery during stenting and may overcome somelimitations of the traditional bare stent in the treatment ofintracranial aneurysms and arterial stenosis. � 2007 WileyPeriodicals, Inc. J BiomedMater Res 85A: 715–721, 2008
Key words: endothelial cell; endothelialization; stent
INTRODUCTION
Intracranial aneurysms are common vascular dis-orders in the brain, and ruptured aneurysm usuallycauses subarachnoid hemorrhage, which is vital ininducing morbidity and mortality.1 The pathophysi-ology underlying aneurysm formation, progression,and rupture is not clearly understood.2,3 As a mini-mally invasive neurosurgical technique, endovascu-lar coiling was introduced in 1990 and has beenwidely used in the treatment of intracranial aneu-rysm.4,5
Endovascular techniques for intracranial aneur-ysms treatment and arterial stenosis have greatlyimproved since the last decade.5 Guglielmi electro-lytically detachable coils (GDC) and platinum intra-cranial stents have been used with excellent clinical
results in a large number of cases6,7; however, intrin-sic technical problems remain, especially in the treat-ment of giant or broad-necked aneurysms. Further-more, embolization of these stubborn aneurysmswith GDC or bare metallic stents may cause throm-boembolic complication in the parent artery orinduce a long-term recurrence of the aneurysm.8,9
Vascular endothelium plays a significant role inthe biological regulation of vessels: it provides anon-thrombogenic surface, serves as a physical andbiochemical barrier, and secretes bioactive substan-ces controlling vascular tone and blood flow.10–12
The formation of endothelium at the neck of the an-eurysm may isolate the aneurysm cavity from bloodflow and, as a result, prevent a recurrence.
If rapid re-endothialization occurs at the neck ofthe aneurysm after embolization, the luminal surfaceof the parent artery may be reconstructed. Problemssuch as aneurysm recurrence and restenosis of theparent artery may also be minimized. However, it isdifficult to induce circulating endothelial progenitorcells to migrate, adhere to and home on the luminalsurface of the aneurismal neck because of fast bloodflow and high shear stress. Several studies involving
Correspondence to: G.-Y. Yang; e-mail: [email protected] grant sponsor: Chinese Nature and Science
Foundation; contract grant number: 30300361 (WZ)
' 2007 Wiley Periodicals, Inc.
animals have demonstrated that endothelial cell-seeding in the atherosclerotic lesions reduced reste-nosis in the injured arteries,13,14 suggesting thatendothelial cell-seeding may provide a feasibleapproach to the modification of the stent. On the ba-sis of our understanding of the characteristics of en-dothelial cells and stents, we designed an endothelialcell-seeded stent and tested this novel device withina shear stress brushing system in vitro.
MATERIALS AND METHODS
Endothelial cells culture
All animal experiments complied with the guidelinesof the Committee on Ethics in Animal Experiments,Fudan University, Shanghai, China. Canine jugular veinendothelial cells were isolated with a modified methodreported by Smith et al.15 A 10-cm segment of caninejugular vein was ligated and separated. The vein wascannulated and the blood was washed out with D-Hankssolution (Sigma, St. Louis, MO). Subsequently, the veinwas incubated in 1% type I collagenase (Sigma) and0.125% pancreatin (Sigma) in a serum-free DMEM (Invi-trogen, Carlsbad, CA) for 20 min at 378C, then centri-fuged at 800g for 5 min at 258C. The pellets were washedand resuspended in DMEM supplemented with 20% fe-tal bovine serum (Gibco, Invitrogen) and 20 ng/mLVEGF (Invitrogen). The endothelial cells were seeded onpoly-lactic-acid (PLA)-coated culture plate at 1 3 106
cells/mL in a humidified atmosphere of 5% CO2 at 378C.The culture medium was changed twice a week. Thecells were used for studies in passengers 5–8.
Immunostaining
The cultured cells were seeded onto 8-well chamberslides and grown to 75% confluence before the experi-ments. The cells were fixed in 2% paraformaldehyde andincubated for 30 min in 5% goat serum (Sigma) with 0.1%triton. Anti-vWF polyclonal antibody (1:200 dilution,DAKO, Carpentaria, CA) was applied at 48C overnight,and then FITC-conjugated goat-anti-rabbit IgG was used assecond antibody (1:1000, Molecular Probe, Invitrogen) atroom temperature for 1 h. The sections were then mountedand photographed using a fluorescent microscope(Olympus Company, NY). Negative controls were per-formed by omitting the primary antibody during immuno-staining.
Flow cytometry assay
The cultured cells were trypsinized and washed thricewith FACS buffer (Invitrogen), resuspended in 3% BSA(Sigma), and incubated for 30 min in FITC-labeled goatanti-mouse vWF IgG (HþL) monoclonal antibody (1:200dilution, DAKO) diluted in 3% BSA on ice. The mouse
isotope IgG (HþL) was used as a negative control. Thecells were washed with FACS buffer thrice by centrifugeat 250g for 5 min, and finally resuspended in a 2% parafor-maldehyde for flow cytometry detection.
Tube formation assay
A 24-well culture plate was coated with 300 mL ofMatrigel (Chemicon, Temecula, CA) per well and thenallowed to polymerize for 30 min at 378C. Total 5 3 104
cells/well were seeded on the matrix in 200 mL of 0.1%BSA/DMEM with 10 ng/mL VEGF (Invitrogen) or without(control), and were then incubated at 378C with 5% CO2
for 18 h. After being washed, microphotographs weretaken with a light microscope (Leica, Wetzlar, Germany).
Endothelialization of vascular stent
A stainless steel stent was commercially obtained fromWeichuang Company (Weichuang Company, Shanghai,China), the surface of which was coated with the hepari-nized polymer using an electronic balance. The hepari-nized polymer contained lactone, a derivation of morpho-line-dione, and was made with the modified methoddescribed by Magoshi and Matsuda.16 The coated stentwas rinsed thrice with sterilized water and dried over-night. Sterilized with ethylene oxide gas, the heparinizedpolymer coated stent was placed in 6-well culture plates,and then 1 3 106 canine endothelial cells in 1 mL DMEMmedium plus 20% FBS and 20 ng/mL VEGF were added.After 1 h of incubation, the stent was rotated 1808 aroundits longitudinal axis and another cell suspension wasadded in the same manner. After repeating this procedurethrice, the stent was incubated for an additional threedays. As a control, canine endothelial cells were alsoseeded on the PLA-coated stent using the same procedure.Finally, a JEOL JSM-T300 scanning electron microscope(Tokyo, Japan) was used to morphologically evaluate theendothelialization of the stent surface.
Shear stress brushing test
A blood flow mimicking device system (Zhongshan,Shanghai, China) was induced to evaluate the success ofthe endothelialized stent. This system was connected to aperfusion pump, which could generate and adjust the flowvolume and flow rate during the experiment. Briefly, thecanine endothelial cell-seeded stent was placed in the sys-tem and was immersed in a DMEM plus 20% FBS and20 ng/mL VEGF medium. Then the stent was treated witha mimicking blood flow with 100 dyne/cm2 shear stressfor 0, 12, 24, and 48 h. The entire procedure was per-formed in an incubator with 5% CO2 at 378C. Finally, thestent was washed thrice with PBS and the endothelial cellsin five random regions on the surface were countedthrough a light microscope (Leica). For semi-quantitatingthe endothelial cell count on the surface of the stent, fiverandom regions on each stent were photographed using a310 objective and cell counting was performed on these
716 ZHU ET AL.
Journal of Biomedical Materials Research Part A
photographs by using image analysis system (NationalInstitute of Health, Image J). A thresholding procedurewas established to determine the cell signal on the surfaceof the stent in each image. The same parameter wasapplied to all images that were obtained at equal objectivesand light intensities. The data were presented as a sum ofcells from the five images.
Statistical analysis
All the experiments were performed at least threetimes. The data are represented as mean 6 standarddeviation (SD). One-way ANOVA with Fisher’s compari-son tests were used to compare the endothelial cellcount among different groups. A random probabilityvalue less than 0.05 was considered statistically signifi-cant for the comparisons.
RESULTS
Endothelial cell isolation, culture, andcharacterization
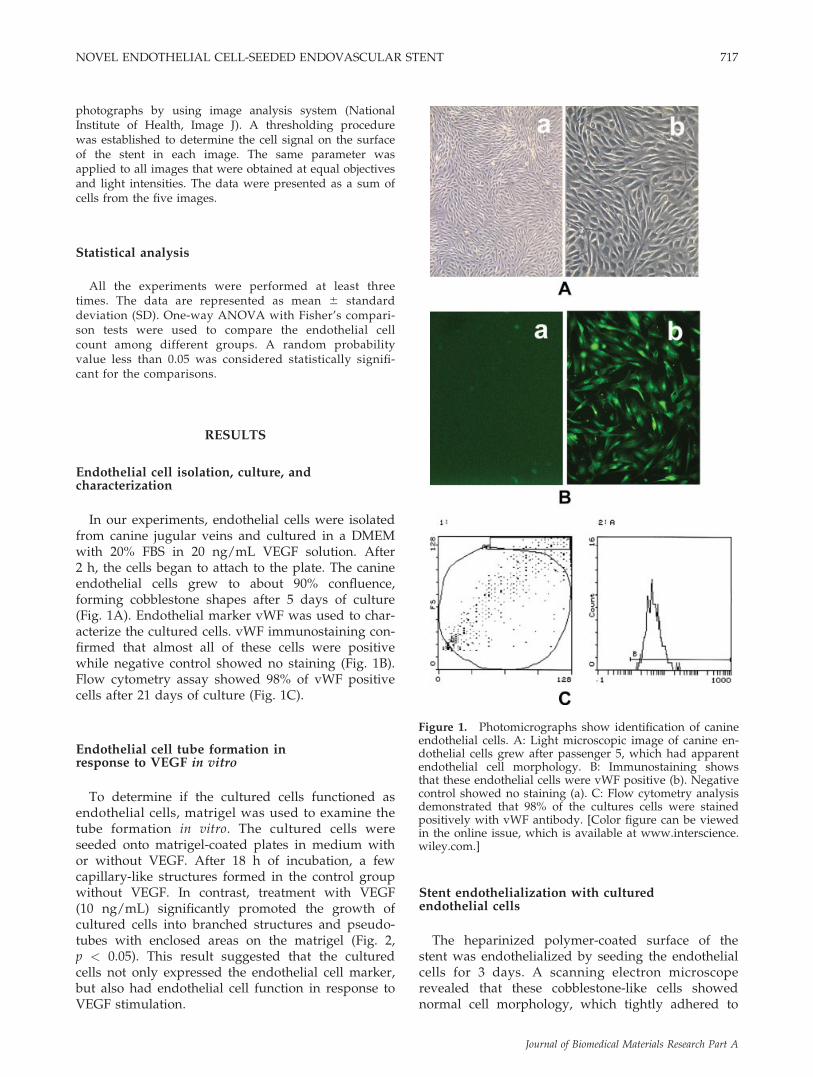
In our experiments, endothelial cells were isolatedfrom canine jugular veins and cultured in a DMEMwith 20% FBS in 20 ng/mL VEGF solution. After2 h, the cells began to attach to the plate. The canineendothelial cells grew to about 90% confluence,forming cobblestone shapes after 5 days of culture(Fig. 1A). Endothelial marker vWF was used to char-acterize the cultured cells. vWF immunostaining con-firmed that almost all of these cells were positivewhile negative control showed no staining (Fig. 1B).Flow cytometry assay showed 98% of vWF positivecells after 21 days of culture (Fig. 1C).
Endothelial cell tube formation inresponse to VEGF in vitro
To determine if the cultured cells functioned asendothelial cells, matrigel was used to examine thetube formation in vitro. The cultured cells wereseeded onto matrigel-coated plates in medium withor without VEGF. After 18 h of incubation, a fewcapillary-like structures formed in the control groupwithout VEGF. In contrast, treatment with VEGF(10 ng/mL) significantly promoted the growth ofcultured cells into branched structures and pseudo-tubes with enclosed areas on the matrigel (Fig. 2,p < 0.05). This result suggested that the culturedcells not only expressed the endothelial cell marker,but also had endothelial cell function in response toVEGF stimulation.
Stent endothelialization with culturedendothelial cells
The heparinized polymer-coated surface of thestent was endothelialized by seeding the endothelialcells for 3 days. A scanning electron microscoperevealed that these cobblestone-like cells showednormal cell morphology, which tightly adhered to
Figure 1. Photomicrographs show identification of canineendothelial cells. A: Light microscopic image of canine en-dothelial cells grew after passenger 5, which had apparentendothelial cell morphology. B: Immunostaining showsthat these endothelial cells were vWF positive (b). Negativecontrol showed no staining (a). C: Flow cytometry analysisdemonstrated that 98% of the cultures cells were stainedpositively with vWF antibody. [Color figure can be viewedin the online issue, which is available at www.interscience.wiley.com.]
NOVEL ENDOTHELIAL CELL-SEEDED ENDOVASCULAR STENT 717
Journal of Biomedical Materials Research Part A
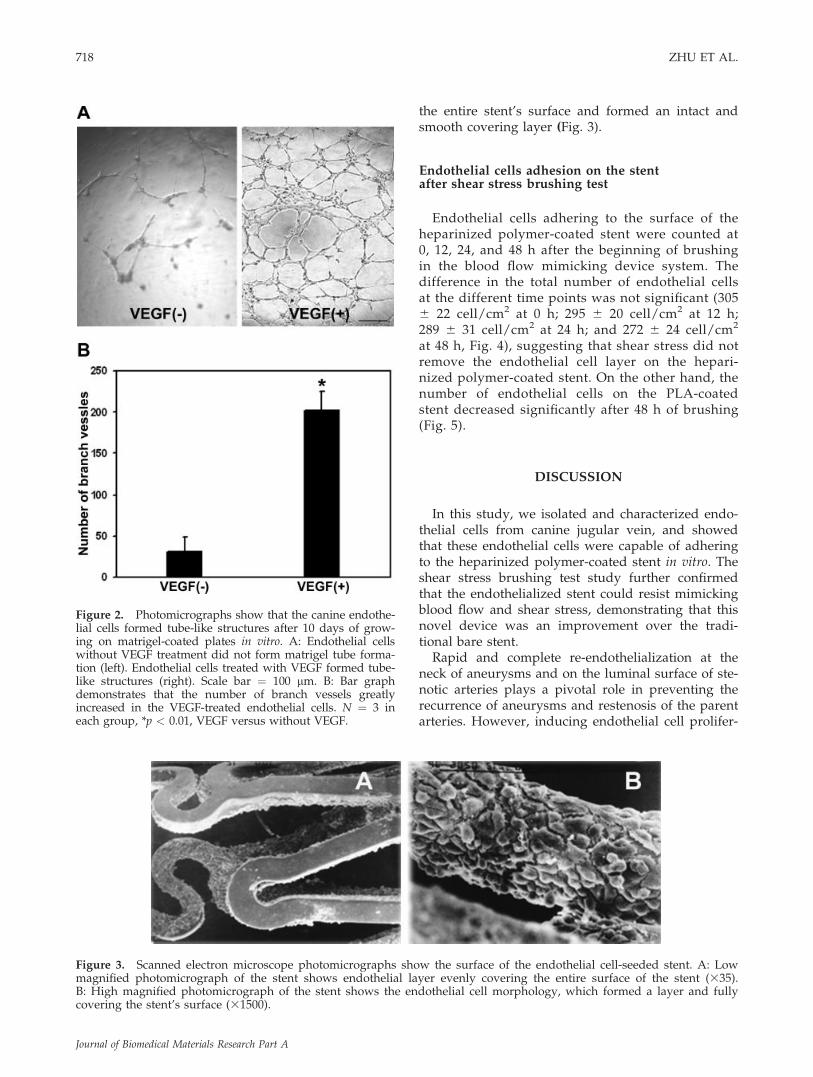
the entire stent’s surface and formed an intact andsmooth covering layer (Fig. 3).
Endothelial cells adhesion on the stentafter shear stress brushing test
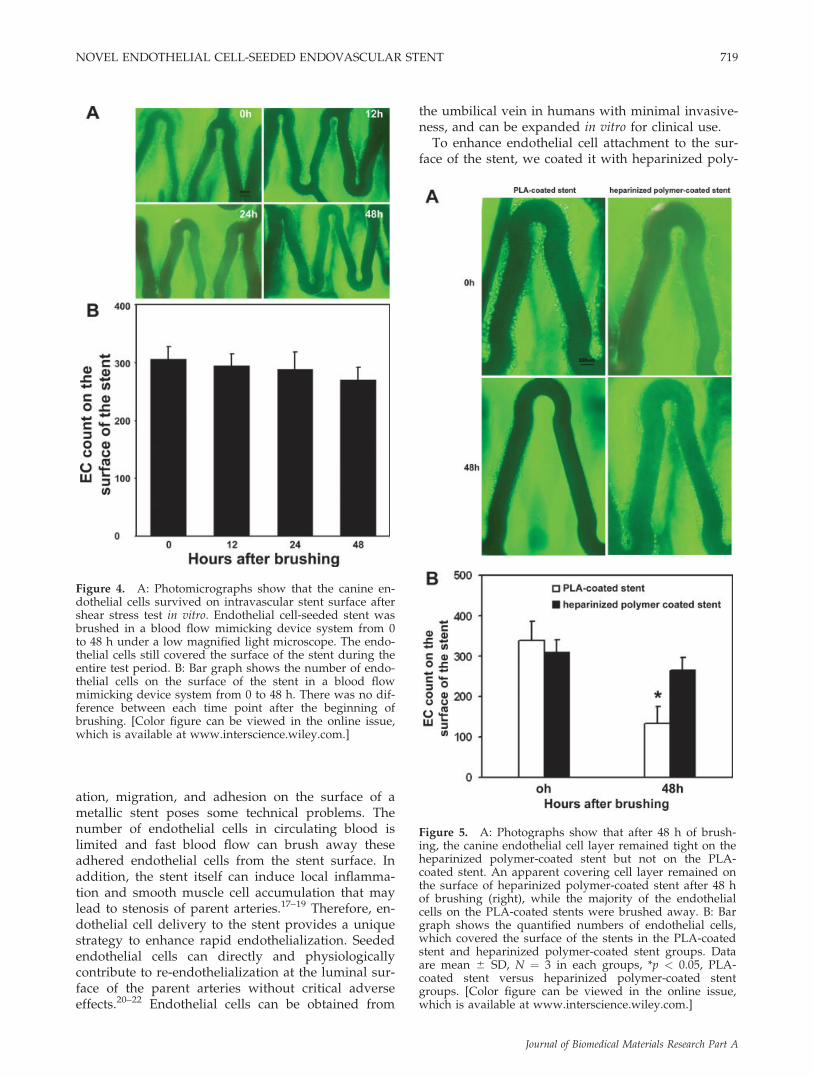
Endothelial cells adhering to the surface of theheparinized polymer-coated stent were counted at0, 12, 24, and 48 h after the beginning of brushingin the blood flow mimicking device system. Thedifference in the total number of endothelial cellsat the different time points was not significant (3056 22 cell/cm2 at 0 h; 295 6 20 cell/cm2 at 12 h;289 6 31 cell/cm2 at 24 h; and 272 6 24 cell/cm2
at 48 h, Fig. 4), suggesting that shear stress did notremove the endothelial cell layer on the hepari-nized polymer-coated stent. On the other hand, thenumber of endothelial cells on the PLA-coatedstent decreased significantly after 48 h of brushing(Fig. 5).
DISCUSSION
In this study, we isolated and characterized endo-thelial cells from canine jugular vein, and showedthat these endothelial cells were capable of adheringto the heparinized polymer-coated stent in vitro. Theshear stress brushing test study further confirmedthat the endothelialized stent could resist mimickingblood flow and shear stress, demonstrating that thisnovel device was an improvement over the tradi-tional bare stent.
Rapid and complete re-endothelialization at theneck of aneurysms and on the luminal surface of ste-notic arteries plays a pivotal role in preventing therecurrence of aneurysms and restenosis of the parentarteries. However, inducing endothelial cell prolifer-
Figure 2. Photomicrographs show that the canine endothe-lial cells formed tube-like structures after 10 days of grow-ing on matrigel-coated plates in vitro. A: Endothelial cellswithout VEGF treatment did not form matrigel tube forma-tion (left). Endothelial cells treated with VEGF formed tube-like structures (right). Scale bar ¼ 100 lm. B: Bar graphdemonstrates that the number of branch vessels greatlyincreased in the VEGF-treated endothelial cells. N ¼ 3 ineach group, *p < 0.01, VEGF versus without VEGF.
Figure 3. Scanned electron microscope photomicrographs show the surface of the endothelial cell-seeded stent. A: Lowmagnified photomicrograph of the stent shows endothelial layer evenly covering the entire surface of the stent (335).B: High magnified photomicrograph of the stent shows the endothelial cell morphology, which formed a layer and fullycovering the stent’s surface (31500).
718 ZHU ET AL.
Journal of Biomedical Materials Research Part A
ation, migration, and adhesion on the surface of ametallic stent poses some technical problems. Thenumber of endothelial cells in circulating blood islimited and fast blood flow can brush away theseadhered endothelial cells from the stent surface. Inaddition, the stent itself can induce local inflamma-tion and smooth muscle cell accumulation that maylead to stenosis of parent arteries.17–19 Therefore, en-dothelial cell delivery to the stent provides a uniquestrategy to enhance rapid endothelialization. Seededendothelial cells can directly and physiologicallycontribute to re-endothelialization at the luminal sur-face of the parent arteries without critical adverseeffects.20–22 Endothelial cells can be obtained from
the umbilical vein in humans with minimal invasive-ness, and can be expanded in vitro for clinical use.
To enhance endothelial cell attachment to the sur-face of the stent, we coated it with heparinized poly-
Figure 4. A: Photomicrographs show that the canine en-dothelial cells survived on intravascular stent surface aftershear stress test in vitro. Endothelial cell-seeded stent wasbrushed in a blood flow mimicking device system from 0to 48 h under a low magnified light microscope. The endo-thelial cells still covered the surface of the stent during theentire test period. B: Bar graph shows the number of endo-thelial cells on the surface of the stent in a blood flowmimicking device system from 0 to 48 h. There was no dif-ference between each time point after the beginning ofbrushing. [Color figure can be viewed in the online issue,which is available at www.interscience.wiley.com.]
Figure 5. A: Photographs show that after 48 h of brush-ing, the canine endothelial cell layer remained tight on theheparinized polymer-coated stent but not on the PLA-coated stent. An apparent covering cell layer remained onthe surface of heparinized polymer-coated stent after 48 hof brushing (right), while the majority of the endothelialcells on the PLA-coated stents were brushed away. B: Bargraph shows the quantified numbers of endothelial cells,which covered the surface of the stents in the PLA-coatedstent and heparinized polymer-coated stent groups. Dataare mean 6 SD, N ¼ 3 in each groups, *p < 0.05, PLA-coated stent versus heparinized polymer-coated stentgroups. [Color figure can be viewed in the online issue,which is available at www.interscience.wiley.com.]
NOVEL ENDOTHELIAL CELL-SEEDED ENDOVASCULAR STENT 719
Journal of Biomedical Materials Research Part A

mer, which could help the cells to adhere butnot affect their growth.16 Using a scanning electronmicroscope, we found that endothelial cells formedan intact and smooth layer on the stent’s surface,indicating that the heparinized polymer promotedendothelial cell adhesion. The heparinized polymerwould degrade in approximately a month (data notshown). The heparinized polymer-coated stent couldsignificantly reduce the platelet adhesion16 and fur-ther prevent thrombosis at the early stage after stent-ing.23 The SEM observation indicated that the seededendothelial cells adhered to the stent and formed acomplete layer that could prevent platelet and leu-kocyte adhesion from the blood. Endothelializationcould further reduce neointimal hyperplasia.24,25 Webelieve that this is an important step in endothelialcell delivery, although the long-term effect of hepari-nized polymer coated stents needs further study.
To observe the response of the endothelial cells onthe surface of the stent to the blood flow, we used ablood flow mimicking device system. The endothe-lialized stent was subjected to a 100 dyne/cm2 shearstress flow, which was stronger than the flow forcein intracranial arteries, and a feasible way to evalu-ate the stability of cells on the stent’s surface at dif-ferent time points.26 After 48 h of brushing, the ma-jority of the cells on the surface remained attached,indicating that these seeded endothelial cells couldremain adhered to the stent and contribute to futureendothelialization.
In conclusion, for endothelial cell delivery duringstenting, we attached autologous endothelial cells onthe surface of a heparinized polymer-coated metalstent. These cells formed a confluent endotheliallayer on the stent’s surface, which remained intactfor at least 48 h under high shear stress brushing.Further in vivo studies need to be performed todetermine whether this novel device can enhance en-dothelialization at the neck of the aneurysm and theluminal surface of the stenotic artery after stenting.
The authors thank Dr. Yongfeng Fan, from the Centerfor Cerebrovascular Research at the University of Califor-nia, San Francisco for editorial assistance and helpfulinsight.
References
1. Forget TR Jr, Benitez R, Veznedaroglu E, Sharan A, MitchellW, Silva M, Rosenwasser RH. A review of size and locationof ruptured intracranial aneurysms. Neurosurgery 2001;49:1322–1325; discussion 1325–1326.
2. Juvela S, Poussa K, Porras M. Factors affecting formation andgrowth of intracranial aneurysms: A long-term follow-upstudy. Stroke 2001;32:485–491.
3. Juvela S. Natural history of unruptured intracranial aneur-ysms: Risks for aneurysm formation, growth, and rupture.Acta Neurochir Suppl 2002;82:27–30.
4. Brettler S. Endovascular coiling for cerebral aneurysms.AACN Clin Issues 2005;16:515–525.
5. Qureshi AI. Endovascular treatment of cerebrovasculardiseases and intracranial neoplasms. Lancet 2004;363:804–813.
6. Aletich VA, Debrun GM, Misra M, Charbel F, Ausman JI.The remodeling technique of balloon-assisted Guglielmidetachable coil placement in wide-necked aneurysms: Experi-ence at the University of Illinois at Chicago. J Neurosurg2000;93:388–396.
7. Tong FC, Cloft HJ, Dion JE. Endovascular treatment ofintracranial aneurysms with Guglielmi detachable coils:Emphasis on new techniques. J Clin Neurosci 2000;7:244–253.
8. Biondi A, Jean B, Vivas E, Le Jean L, Boch AL, Chiras J, VanEffenterre R. Giant and large peripheral cerebral aneurysms:Etiopathologic considerations, endovascular treatment, andlong-term follow-up. AJNR Am J Neuroradiol 2006;27:1685–1692.
9. Thompson MM, Smith JL, Bell PR. Thromboembolic compli-cations during endovascular aneurysm repair. Semin VascSurg 1999;12:215–219.
10. Raymond J, Sauvageau E, Salazkin I, Ribourtout E, Gevry G,Desfaits AC. Role of the endothelial lining in persistence ofresidual lesions and growth of recurrences after endovas-cular treatment of experimental aneurysms. Stroke 2002;33:850–855.
11. Raymond J, Guilbert F, Metcalfe A, Gevry G, Salazkin I,Robledo O. Role of the endothelial lining in recurrences aftercoil embolization: Prevention of recanalization by endothelialdenudation. Stroke 2004;35:1471–1475.
12. Stiver SI, Porter PJ, Willinsky RA, Wallace MC. Acute humanhistopathology of an intracranial aneurysm treated usingGuglielmi detachable coils: Case report and review of the lit-erature. Neurosurgery 1998;43:1203–1208.
13. Kipshidze N, Ferguson JJ III, Keelan MH Jr, Sahota H,Komorowski R, Shankar LR, Chawla PS, Haudenschild CC,Nikolaychik V, Moses JW. Endoluminal reconstruction of thearterial wall with endothelial cell/glue matrix reduces reste-nosis in an atherosclerotic rabbit. J Am Coll Cardiol2000;36:1396–1403.
14. Methe H, Nugent HM, Groothuis A, Seifert P, Sayegh MH,Edelman ER. Matrix embedding alters the immune responseagainst endothelial cells in vitro and in vivo. Circulation2005;112(9 Suppl):I89–I95.
15. Smith JM, Meinkoth JH, Hochstatter T, Meyers KM. Differen-tial distribution of von Willebrand factor in canine vascularendothelium. Am J Vet Res 1996;57:750–755.
16. Magoshi T, Matsuda T. Formation of polymerized mixedheparin/albumin surface layer and cellular adhesionalresponses. Biomacromolecules 2002;3:976–983.
17. Ganaha F, Kao EY, Wong H, Elkins CJ, Lee J, Modanlou S,Rhee C, Kuo MD, Yuksel E, Cifra PN, Waugh JM, Dake MD.Stent-based controlled release of intravascular angiostatin tolimit plaque progression and in-stent restenosis. J Vasc IntervRadiol 2004;15:601–608.
18. Tardif JC, Gregoire J, L’Allier PL. Prevention of restenosiswith antioxidants: Mechanisms and implications. Am J Cardi-ovasc Drugs 2002;2:323–334.
19. Welt FG, Rogers C. Inflammation and restenosis in the stentera. Arterioscler Thromb Vasc Biol 2002;22:1769–1776.
20. Prasad CK, Resmi KR, Krishnan LK, Vaishnav R. Survival ofendothelial cells in vitro on Paclitaxel-loaded coronary stents.J Biomater Appl 2005;19:271–286.
21. Shirota T, Yasui H, Shimokawa H, Matsuda T. Fabrication ofendothelial progenitor cell (EPC)-seeded intravascular stentdevices and in vitro endothelialization on hybrid vascular tis-sue. Biomaterials 2003;24:2295–2302.
720 ZHU ET AL.
Journal of Biomedical Materials Research Part A

22. Koren B, Weisz A, Fischer L, Gluzman Z, Preis M, Avramo-vitch N, Cohen T, Cosset FL, Lewis BS, Flugelman MY. Effi-cient transduction and seeding of human endothelial cellsonto metallic stents using bicistronic pseudo-typed retroviralvectors encoding vascular endothelial growth factor. Cardio-vasc Revasc Med 2006;7:173–178.
23. Wissink MJ, Beernink R, Pieper JS, Poot AA, Engbers GH,Beugeling T, van Aken WG, Feijen J. Binding and release ofbasic fibroblast growth factor from heparinized collagen mat-rices. Biomaterials 2001;22:2291–2299.
24. Tull SP, Anderson SI, Hughan SC, Watson SP, Nash GB,Rainger GE. Cellular pathology of atherosclerosis: Smoothmuscle cells promote adhesion of platelets to cocultured en-dothelial cells. Circ Res 2006;98:98–104.
25. Amoroso G, van Veldhuisen DJ, Tio RA, Mariani M. Patho-physiology of vascular endothelium and circulating platelets:Implications for coronary revascularisation and treatment. IntJ Cardiol 2001;79:265–275.
26. Davies PF, Tripathi SC. Mechanical stress mechanisms andthe cell. An endothelial paradigm. Circ Res 1993;72:239–245.
NOVEL ENDOTHELIAL CELL-SEEDED ENDOVASCULAR STENT 721
Journal of Biomedical Materials Research Part A