Embed Size (px)
Citation preview

Despite the success of endovascular repair of the descending thoracic aorta, surgeons face limitations in deploying this technology for pararenal, paravisceral and thoracoabdominal aortic aneurysms. In these instances, a conventional endograft would typically not have a sufficient landing zone to seal the aneurysm and would likely occlude blood flow to an aortic branch.
Two approaches were developed to allow physicians to treat a wider range of patients with aortic aneurysms: fenestrated endografts and branched endografts.
Fenestrated endografts have openings in the grafts that are positioned at the ostia of the aortic branches and through which smaller stents are deployed into the arterial branches. Detailed preprocedure imaging informs the customized design of each endograft and the deployment of these endografts must be precise. Fenestrated
endografts can currently treat juxtarenal aortic aneurysms and are now available at the Aortic Center.
Branched endografts are designed as a single system of main stent graft and attached branch stent graft. Currently approved endografts for EVAR and TEVAR are being updated with branched technology. These endografts have been available in Europe for over five years. Trials are planned in the near future in the hope of bringing this technology to patients in the United States.
Mortality rates associated with fenestrated or branched endovascular repair of abdominal andthoracoabdominal aortic aneurysms are generally lower than conventional open surgical repair. Endoleaks, in which blood flows outside the lumen of the endograft, occur at approximately the same rate with fenestrated or branched endovascular repair as in open surgical repair.9
W I N T E R 2 0 1 5
THELEADINGEDGE
USC CardioVascular Thoracic Institute
CLINICAL TRIALSThe USC Comprehensive Aortic Center has dedicated research coordinators to evaluate patients, discuss trial participation and enroll patients in clinical trials.
Currently, the Aortic Center is enrolling or following patients in the studies below:
Global Registry for Endovascular Aortic Treatment - This is a prospective observational cohort registry designed to obtain data on device performance and clinical outcomes of patients treated with Gore endovascular aortic products. (NCT01658787)
NTA3CT - The primary aim of this study is to determine if doxycycline will inhibit the increase in greatest transverse diameter of small abdominal aortic aneurysms over a 24-month period of observation in comparison to a placebo-treated control group. (NCT01756833)
Endovascular Management of Aortic DiseaseThe USC Comprehensive Aortic Center at the Keck Medical Center of USC was created to provide the best and most advanced care for patients with aortic disease. The Aortic Center employs the recognized expertise of the cardiac and vascular surgeons of Keck Medical Center of USC to provide the full complement of endovascular and open aortic procedures.
The Aortic Center possesses a full spectrum of techniques and technology to treat all aortic pathologies including aneurysms, dissections and occlusive disease. Aortic disease management requires a collaborative, multidisciplinary approach and longitudinal care for the life of the patient.
The management of aortic disease by endovascular aortic repair (EVAR) and thoracic endovascular aortic repair (TEVAR) revolutionized the treatment of
the aorta. At Keck Medical Center of USC, an estimated 70 percent of patients with aortic disease are now treated with either TEVAR or EVAR. These procedures utilize catheter-based, minimally-invasive vascular access and endografts to treat aortic disease.
For the minority of patients with aortic disease not amenable to treatment with EVAR or TEVAR, the USC Comprehensive Aortic Center has experienced cardiac and vascular surgeons with recognized expertise in the open surgical repair of arch, thoraco-abdominal and pararenal aortic disease. Keck Medical Center of USC cardiac surgeons use antegrade cerebral perfusion instead of deep hypothermic circulatory arrest to maintain cerebral protection while reducing the time to rewarm patients from an operation that treats type A aortic dissections and complex aortic arch repairs.
See Endovascular, page 4 See Clinical Trials, page 6
THE LEADING EDGEUSC CardioVascular Thoracic Institute
University of Southern California SST-2830, 2011 N. Soto St. Los Angeles, CA 90032
© 2015 Keck Medicine of USC
For more information, call theUSC CardioVascular Thoracic Institute at: (323) 442-5849 Or visit: aortic.KeckMedicine.orgFor urgent patient referrals and transfers, call: (866) 65-AORTA (866-652-6782)
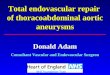
Figure 4Diagram of a deployed, fenestrated stent graft in the abdominal aorta with covered stents inserted into the renal arteries.
TECHNOLOGY SPOTLIGHTNext Generation of Endografts are Branched and Fenestrated
NONPROFIT ORGU.S. POSTaGe
PaIDUNIveRSITy OF
SOUTheRN CalIFORNIa
University of Southern California SST-2830, 2011 N. Soto Street Los Angeles, CA 90032
Image courtesy of Cook Medical

MESSAGE FROM THE C0-DIRECTORSDear Colleague:
The team of experts at the USC Comprehensive Aortic Center is ready to work closely with you in the care of your patients with aortic disease.
The strong collaboration between our vascular and cardiothoracic surgeons and cardiovascular medicine specialists allows us to provide the most comprehensive care to our patients by treating the entire aorta. Our skilled physicians have performed hundreds of cases, and have been regional leaders in the development of endovascular aneurysm repair and thoracic endovascular aortic repair therapies. In addition to being at the forefront of endovascular technology, the Aortic Center is the largest referral center in Southern California for the evaluation and treatment of aortic emergencies, including ruptured aortic aneurysms and acute aortic dissection.
Because time is of the essence for most aortic patients, Keck Medicine of USC offers immediate access to lifesaving care for patients in need of emergent treatment through its Rapid Transfer Program.
To further acquaint you with the USC Comprehensive Aortic Center, we have created this publication that explains our approach to care and services we offer. For more information or to refer a patient, please call (866) 65-AORTA (866-652-6782).
We are committed to partnering with you in the management of your patients. It is our pleasure to ensure the best possible outcomes are delivered with compassion.
2 USC CardioVascular Thoracic Institute: (323) 442-5849 cvti.KeckMedicine.org 3
THE LEADING EDGEUSC CardioVascular Thoracic Institute
Fred A. Weaver, MD, MMMProfessor of SurgeryKeck School of Medicine of USC
Co-directorUSC CardioVascular Thoracic Institute
Co-directorUSC Comprehensive Aortic Center
Fernando Fleischman, MD Assistant Professor of SurgeryKeck School of Medicine of USC
Co-directorUSC Comprehensive Aortic Center
Aortic dissections involve a tear and dissection of the layers within the aortic wall. Type A aortic dissections involve the ascending aorta, and type B dissections do not. If any portion of the dissection involves the ascending aorta, it is classified as a type A, even if the dissection extends into the descending aorta. When the aortic wall dissects, a false lumen develops in the aortic media.
Patients with type B aortic dissections are typically treated medically. While the immediate success of medical therapy is high, approximately 60 percent of patients will develop aortic aneurysms of the most challenging variety.1 The rationale for using TEVAR in patients with type B aortic dissections is that by covering
the proximal aortic entry tear with the aortic endograft, blood flow is excluded from the false lumen and redirected into the true lumen (Figure 1).
Prospective, randomized trials of TEVAR for patients with type B aortic dissections showed lower rates of aortic-related complications and mortality, and improved remodeling of the false lumen compared to patients receiving medical care alone.2,3 Recent data published in JAMA Surgery show the results from patients treated with TEVAR at the USC Comprehensive Aortic Center.4
The data demonstrate that TEVAR promotes favorable remodeling of the thoracic and abdominal aorta.
A 67-year-old man was referred to the Aortic Center with a type B aortic dissection. At the referring hospital, his chief concerns were chest pain, midline back pain and pain in his right thigh on ambulation. Upon arriving at Keck Medical Center of USC, the patient underwent CT imaging that revealed a type B aortic dissection that extended from the subclavian arteries to both of the common iliac arteries. Physicians at the USC Comprehensive Aortic Center initially managed the patient’s aortic dissection medically and monitored the dissection with repeat CT imaging. During a
period of nine months after the aortic dissection occurred, CT imaging showed that the proximal thoracic portion of the dissection expanded in size from 4.1 cm to 5.5 cm. Physicians at the Aortic Center felt that the patient needed to be treated surgically to mitigate any future risk and that the patient was a good candidate for TEVAR.
In November 2010, the patient underwent thoracic endovascular repair of his aortic dissection. In preparation for the TEVAR procedure, the left subclavian artery was transposed onto the left common carotid artery to increase the proximal landing zone in the aortic arch for TEVAR. Both femoral arteries were catheterized and a subsequent arch aortogram showed the extent of the dissection and the location of the arch
vessels. A thoracic stent graft, 34 mm in diameter by 15 cm in length, was inserted through the right femoral artery and advanced into the aortic arch. An arch aortogram precisely localized the stent graft relative to the dissection and the stent graft was deployed just distal to the origin of the left common carotid artery.
After deployment, another arch aortogram demonstrated that the stent graft decreased blood flow into the false lumen by ~95 percent. The celiac artery, which could not be visualized on a preprocedure aortogram, was now visualized, indicating that flow was restored to the previously stenosed artery.
CASE STUDY
TEVAR in a Chronic Type B Aortic Dissection
Figure 1CT images before and after TEVAR. (left) The preprocedure CT image shows a large aortic dissection with aneurysmal degeneration (note the lighter gray shading that indicates the enlarged area of blood flow). (right) The postprocedure CT image shows that the stent graft confines the blood flow to the true lumen. These are representative images that were not taken from the patient described.
PROCEDURE SHOWCASE AND OUTCOMES
Treatment of Type B Aortic Dissection with TEVAR

4 USC CardioVascular Thoracic Institute: (323) 442-5849 cvti.KeckMedicine.org 5
THE LEADING EDGEUSC CardioVascular Thoracic Institute
Advanced imaging technology is essential to EVAR and TEVAR. Each patient’s preoperative CT images are transformed into a 3D reconstruction of the aorta to better inform surgeons with endovascular device selection and placement (Figure 3).
Intravascular ultrasound is used during EVAR and TEVAR to help visualize aortic branches, endoluminal aortic morphology, and aortic fenestrations, which allows for more accurate placement of the endograft and reduces contrast nephrotoxicity.
In the near future, branched EVAR devices will expand the endovascular treatment options for many patients with complex aortic disease (see Technology Spotlight below). This technology will allow treatment of patients with thoracoabdominal aortic aneurysms. Ascending aorta designs of TEVAR devices are being developed to treat some patients with type A aortic dissections. Additionally, there is growing use of TEVAR to repair blunt traumatic aortic injury. Keck Medicine of USC is the only center on the West Coast and only one of five centers in the United States that performs robotic endovascular procedures, which have the potential to improve the safety and efficacy of EVAR, FEVAR and TEVAR procedures.
The USC Comprehensive Aortic Center was created to integrate the complementary expertise of cardiac surgeons, vascular surgeons, cardiovascular medicine specialists, radiologists, vascular technologists and nurses in the treatment of aortic disease from the arch to the bifurcation. The Aortic Center has a unique, dedicated line, (866) 65-AORTA (866-652-6782), for physicians to receive an
emergency, comprehensive evaluation of patients over the phone. A phone call to the Aortic Center line gets immediate attention and decision-making in the triage of patients to Keck Medical Center of USC. Aortic Center staff will facilitate patient transport through the Keck Hospital of USC Rapid Transport service. Aortic Center staff provide patient updates and follow-up to referring physicians after a transfer has taken place.
The Rapid Transport service is designed to bring patients by ambulance or helicopter to Keck Medical Center of USC within two hours or less. The faster patients are brought to the Aortic Center, the better their outcomes. For example, in pathologies of the ascending aorta, a patient’s mortality rises progressively for every minute that they are not yet treated surgically.
PROVIDING IMMEDIATE ACCESS 24/7Call (866) 65-AORTA (866-652-6782) to reach the physicians at the USC Comprehensive Aortic Center for:
• Consultationonan urgent aortic case
• Transportationofa patient to Keck Medical Center of USC to treat their aortic condition
Figure 33D reconstruction of the heart, aorta and major branching blood vessels used to plan TEVAR procedure. The image was reconstructed from preprocedure CT imaging.
More recently, FEVAR (fenestrated endovascular aortic repair) has been utilized to treat juxtarenal and pararenal aortic aneurysms. TEVAR, as performed at Keck Medical Center of USC, is achieved with the complementary talents of cardiac and vascular surgeons.
In 2004, the USC Comprehensive Aortic Center became the first group in Southern California to perform TEVAR for a thoracic aortic aneurysm. Since 2004, more than 240 TEVAR procedures have been
performed by the Aortic Center team.
EVAR and TEVAR are performed in one of two hybrid operating rooms at Keck Medical Center of USC where angiography and intravascular ultrasound are seamlessly integrated into the procedure (Figure 2).
EVAR and TEVAR were pioneered as approaches to reduce the morbidity and mortality associated with open surgical repair of aortic aneurysms, dissections and trauma. In addition, EVAR and TEVAR
offer treatment options for patients who are deemed too high risk to undergo open surgical repair. EVAR and TEVAR are now the treatments of choice for most aortic disease.
Prospective clinical trials of EVAR and TEVAR have shown that endovascular procedures to treat aortic pathologies have fewer complications5 and lower rates of aneurysm-related mortality6,7 than conventional open surgical repair of aortic aneurysms. The USC Comprehensive Aortic Center has extensive experience with hybrid aortic procedures that combine EVAR or TEVAR with open surgical procedures to treat complex aortic arch and thoracoabdominal aortic pathology.8
Endovascular Management of Aortic Disease
Figure 2 Still image taken from video of TEVAR procedure. The inset photo shows the catheter insertion by the surgeon. The black and white photo is an intraoperative aortogram showing the delivery catheter and the TEVAR stent graft before deployment inserted into the aorta.
Since 1999, Keck Medicine of USC vascular surgeons have employed EVAR for abdominal aortic aneurysms. The experienced vascular surgery team has performed more than 500 EVARs to date.
Continued from page 1

USC Comprehensive Aortic Center Team
References1. Tsai TT, Fattori R, Trimarchi S. Long-term survival in patients presenting with type B acute aortic dissection: insights from the International Registry of Acute
Aortic Dissection. Circulation. 2006;114(21):2226-2231.
2. Nienaber CA, Kische S, Rousseau H, et al. Endovascular repair of type B aortic dissection: long-term results of the randomized investigation of stent grafts in aortic dissection trial. Circ Cardiovasc Interv. 2013;6(4):407-416.
3. Brunkwall J, Kasprzak P, Verhoeven E, Heijmen R, Taylor P. Endovascular repair of acute uncomplicated type B dissection promotes aortic remodeling: 1 year results of the ADSORB trial. Eur J Vasc Endovasc Surg. 2014;48(3):285-291.
4. Sigman MM, Palmer OP, Ham SW, Cunningham M, Weaver FA. Aortic morphologic findings after thoracic endovascular aortic repair for type B aortic dissection. JAMA Surg. 2014;149(9):977-983.
5. Prinssen M, Verhoeven ELG, Buth J, Cuypers PWM, Grobbee DE, Blankensteijn J. A randomized trial comparing conventional and endovascular repair of abdominal aortic aneurysms. N Engl J Med. 2004;351(16):1607-1618.
6. Makaroun MS, Dillavou ED, Wheatley GH, Cambria RP. Five-year results of endovascular treatment with the Gore TAG device compared with open repair of thoracic aortic aneurysms. J Vasc Surg. 2008;47(5):912-918.
7. Matsumura JS, Melissano G, Cambria RP, et al. Five-year results of thoracic endovascular aortic repair with the Zenith TX2. J Vasc Surg. 2014;60(1):1-10.
8. Ham SW, Chong T, Moos J, et al. Arch and visceral/renal debranching combined with endovascular repair for thoracic and thoracoabdominal aortic aneurysms. J Vasc Surg. 2011;54(1):30-41.
9. Bakoyiannis CN, Economopoulous KP, Georgopoulos S, et al. Fenestrated and branched endografts for the treatment of thoracoabdominal aortic aneurysms: a systematic review. J Endovasc Ther. 2010;17(2):201-209.
USC CardioVascular Thoracic Institute: (323) 442-5849 cvti.KeckMedicine.org 7
Gore Excluder Iliac Branch Graft - The prospective, nonrandomized, multicenter, single-arm study will assess the safety and efficacy of the iliac branch endoprosthesis device in subjects with common iliac artery aneurysms or aorto-iliac aneurysms. (NCT01883999)
The Aortic Center is also participating in these clinical trials, which are not yet enrolling patients:
Valor II - This study is evaluating the clinical performance of Medtronic’s Valiant Thoracic Stent Graft System to treat descending thoracic aneurysms of degenerative etiology in subjects that are candidates for endovascular repair. (NCT00413231)
Anaconda - This Phase II clinical study, sponsored by Terumo, is assessing the safety and efficacy of the Anaconda Stent Graft System in subjects presenting with an infrarenal abdominal aortic aneurysm. (NCT00612924)
Gore Conformable TAG - This study is evaluating the Gore Conformable TAG Thoracic Endoprosthesis for the primary treatment of descending thoracic aortic aneurysms. (NCT00874250)
Gore Trauma TAG - The prospective, multicenter, single-arm study will evaluate the use of the Conformable TAG Endoprosthesis in traumatic transection of the descending thoracic aorta. (NCT00917852)
VITALITY - The purpose of this post-market study is to examine the long-term safety and efficacy of endovascular repair with Medtronic’s Talent Abdominal Stent Graft System in patients with an abdominal aortic aneurysm. (NCT00816062)
CLINICAL TRIALS
For urgent patient referrals and transfers, call: (866) 65-AORTA (866-652-6782)
THE LEADING EDGEUSC CardioVascular Thoracic Institute
6
RECENT ACCOMPLISHMENTSFred A. Weaver, MD, MMM, professor of Surgery, Keck School of Medicine of USC, Co-director of the CardioVascular Thoracic Institute and Co-director of the USC Comprehensive Aortic Center is the senior author on a recent publication in JAMA Surgery on type B aortic dissections (Sigman MM, et al. Aortic morphologic findings after thoracic endovascular aortic repair for type B aortic dissection. JAMA Surg. 2014; 149(9):977-983.)
Fernando Fleischman, MD, assistant professor of Surgery, Keck School of Medicine of USC, Co-director of the USC Comprehensive Aortic Center, authored a 2013 publication on CT angiography for surgical planning. (Shinbane JS, et al. Anomalous coronary arteries: cardiovascular computed tomographic
angiography for surgical decisions and planning. World J Pediatr Congenit Heart Surg. 2013; 4(2): 142-154.)
Dr. Weaver was selected to give the 2013 William Hunter Harridge Lecture to the Midwest Surgical Association. In 2014, he served as President of the Pacific Coast Surgical Association and the Society for Clinical Vascular Surgery.
Dr. Weaver was the senior author on a paper presented at the 28th annual meeting of the Western Vascular Society. (Wartman SM, et al. Outcomes after abdominal aortic aneurysm repair requiring a suprarenal cross-clamp. J Vasc Surg. 2014; 54(1): 30-41.)
Continued from page 1
Vascular SurgeryFred A. Weaver, MD, MMMProfessor of SurgeryCo-director, USC Comprehensive Aortic Center
Sukgu M. Han, MDAssistant Professor of Surgery
William M. Lee, MDAssistant Professor of Surgery
Mitra K. Nadim, MDAssociate Professor of Clinical Medicine Director, USC Hypertension Center
Christian J. Ochoa, MDAssistant Professor of SurgeryAssistant Director, Critical Limb Ischemia Program
Vincent L. Rowe, MD, FACS Professor of Surgery
Sung Wan Ham, MD Assistant Professor of Surgery
Karen Woo, MD, MS, FACS Assistant Professor of Surgery
Laura Sjoberg, RN, MSN, ACNP-BC Nurse Practitioner
RadiologyFarhood Saremi, MDProfessor of Radiology
Alison Wilcox, MD, FSCCTAssistant Professor of RadiologyDirector, Cardiothoracic Imaging
Cardiothoracic SurgeryFernando Fleischman, MDAssistant Professor of SurgeryCo-director, USC Comprehensive Aortic Center
Vaughn A. Starnes, MDHastings Distinguished Professor and Chair Department of SurgeryExecutive Director, USC CardioVascular Thoracic Institute
Craig J. Baker, MD Associate Professor of Surgery
Michael E. Bowdish, MDAssistant Professor of SurgeryDirector, Mechanical Circulatory Support
Robbin G. Cohen, MD, MMM Associate Professor of Surgery
Mark J. Cunningham, MD Associate Professor of SurgerySurgical Director, Heart Transplant Program Amy Hackmann, MD Assistant Professor of Surgery
Sophia Lam, RN, MSN, CNS, ACNP-BC Nurse Practitioner
For more information on any of the clinical trials or to inquire about enrolling a patient, please contact Stephanie Mullin, RN, Research Coordinator Supervisor, at (323) 442-6226 or: [email protected]