Embed Size (px)
Citation preview

Developing a Personal Protective Equipment
Selection Matrix for Preventing Occupational
Exposure to Ebola Virus
Christopher K. Brown, Denise L. Matthews, Richard J. Thomas, and Amanda L. Edens
In response to the 2014 Ebola outbreak in West Africa and resulting cases in the United States, the Occupational Safety and
Health Administration developed a personal protective equipment selection matrix to help employers protect workers from
exposure to Ebola virus in the event of additional US cases. Now, the world’s second largest Ebola outbreak on record continues
to expand in the Democratic Republic of Congo, where more than 70 Ebola-infected healthcare workers serve as reminders of
the importance of robust infection prevention measures in keeping infectious disease responders from becoming victims
themselves. Toward facilitating preparedness for cases associated with the ongoing or future outbreaks, this article discusses the
matrix of personal protective equipment recommendations. The matrix applies to a variety of job tasks in health care, labora-
tories, waste handling, janitorial services, travel and transportation, and other sectors where workers may be exposed to the Ebola
virus during outbreak events. A discussion of the information sources and decision-making process for developing the matrix
forms the basis of the recommendations. The article then emphasizes challenges and considerations for formulating the matrix,
including identifying information sources to help characterize occupational exposures, aligning recommendations among
stakeholders with varying viewpoints, and balancing worker protections with feasibility concerns. These considerations highlight
issues that remain relevant for preparedness efforts ahead of future US cases of Ebola or other emerging infectious diseases.
Keywords: Personal protective equipment, Ebola virus disease, Occupational health, Respiratory protection
The Ebola virus (EBV) outbreak in the DemocraticRepublic of Congo (DRC), now the second largest
on record after the West Africa epidemic approximately 5years ago, continues to expand. As of March 10, 2019,there have been more than 900 confirmed or probablecases and at least 582 deaths among confirmed cases.1
More than 70 healthcare workers are among those in-fected, 26 of whom have died. These worker infectionsare reminders of the importance of robust infection pre-vention measures, including personal protective equipment(PPE), in keeping infectious disease responders from becom-ing victims themselves.
Christopher K. Brown, PhD, MPH, CPH, is Senior Health Scientist, and Denise L. Matthews, MSPH, is Director, both in the Officeof Emergency Management and Preparedness; Richard J. Thomas, MD, MPH, is Deputy Director, Office of Occupational Medicineand Nursing; and Amanda L. Edens, MSPH, is Director; all in the Directorate of Technical Support and Emergency Management,Occupational Safety and Health Administration, US Department of Labor, Washington, DC.
Health SecurityVolume 17, Number 3, 2019 ª Mary Ann Liebert, Inc.DOI: 10.1089/hs.2019.0014
1

Although the current outbreak has been contained in theDRC thus far, preparing for domestic cases remains criticalto ensuring a safe and successful public health response ifinfected individuals again reach the United States. In ad-dition to several aid workers whom the US governmenttransported from abroad for observation or treatment at theNebraska Medical Center, Emory University Hospital, andthe National Institutes of Health (NIH) since the start ofthe West Africa outbreak, 2 other individuals presented inTexas and New York with Ebola virus disease (EVD) in2014 after arriving in the United States on their own. TheTexas case spread EBV to 2 healthcare workers.
While well-equipped biocontainment facilities withteams that have undergone intensive training in infectionprevention are typically activated to care for intentionallyrepatriated patients, other healthcare facilities and theirworkers could encounter spontaneously presenting EBV-infected individuals at any time. Because of their job tasks,workers in laboratories, environmental services (ie, clean-ing), law enforcement, air travel and other transportationoperations, and waste management, among other sectors,may also be at risk for EBV exposure if cases reach theUnited States. As such, employers of workers who mightevaluate, isolate, handle materials from or contaminated by,or otherwise interact with EBV-infected individuals shouldhave plans to protect employees with appropriate controls,including PPE.
In this article, we describe development of an Occupa-tional Safety and Health Administration (OSHA) EBVPPE selection matrix during the response to the West Africaepidemic and resulting US cases.2 While we discuss theprocess for creating the matrix, this article emphasizeschallenges and considerations for developing the guidance,especially those relevant to continued preparedness efforts.Understanding the basis of OSHA’s PPE matrix and theissues the agency considered in preparing it may facilitateuser efforts to incorporate the recommendations into theirown workplace planning efforts.
Methods
OSHA aimed to develop adaptable PPE recommendationsfor safeguarding workers in a variety of different jobs fromoccupational exposure to EBV in the United States. Weorganized this information into a matrix that links worktasks with appropriate equipment, an approach consistentwith PPE-related communications the agency has issued forother types of emergencies.3,4
Before making equipment recommendations, OSHAneeded to assess exposure scenarios warranting PPE. Toidentify job tasks with possible EBV exposure, we adaptedthe Centers for Disease Control and Prevention (CDC)EBV-specific epidemiologic risk factors framework.5 Itcovered most types of exposures we anticipated addressingin the PPE matrix, and it allowed us to identify workers
likely to have at least some EBV exposure risk during anoutbreak in the United States. Those included workers withtasks that could result in, among other things:
� Close contact with an individual while the personexhibited EVD symptoms;
� Percutaneous (eg, needlestick) or mucous membraneexposure to blood or body fluids of a symptomaticperson with EVD;
� Contact or droplet exposure to the blood or bodyfluids of a symptomatic person with EVD;
� Direct contact with a dead body (considering otherfactors about the decedent and exposure); and
� Other low- but not no-risk exposures.
These risk factors focus on contact transmission (ie, ex-posure to EBV contained in blood, body fluids, or otherpotentially infectious materials). However, some evidencesuggests that aerosols containing infectious particles of avariety of sizes suspended in the air also present exposurehazards.6-8 Without empirical support for excluding thistransmission route, OSHA also considered job tasks thatcould result in EBV exposure in aerosols, including aerosol-generating procedures in healthcare and laboratory workand aerosols generated by maintenance, janitorial, andwaste management operations. For all tasks evaluated, ouraim was to identify PPE that would prevent contact ofexposed skin and mucous membranes with blood, bodyfluids, or other potentially infectious materials that couldcontain EBV. We also offered recommendations for re-spiratory protection when we believed workers might en-counter potentially infectious aerosols. In general, activitieswith lower risks of exposure to potentially infectious blood,body fluids, and other potentially infectious materials re-quired lower levels and/or fewer pieces of PPE, such assingle pairs of gloves or facemasks. As exposure likelihoodor intensity increased or aerosols became a concern, weadded additional PPE, including barrier garments andrespirators.
Scarce, up-to-date, peer-reviewed information on PPEfor EBV at the time we developed this matrix (ie, early inthe 2014-15 West Africa outbreak) forced us to rely fre-quently on other data sources in assessing hazards andidentifying the types of equipment workers would need toprevent exposures. In some cases, well-accepted federalguidelines for infection prevention proved to be readilyadaptable to the matrix. For example, we incorporatedrecommendations for standard and transmission-basedprecautions that were already routinely followed in hospi-tals and other healthcare facilities.9 For laboratories, weused recommended biosafety protocols from the CDC/NIH publication Biosafety in Microbiological and Biomedi-cal Laboratories (BMBL), including biosafety level (BSL)-4guidelines for PPE and physical containment of EBVsamples.10 The BMBL guidance is well accepted and nearlyuniversally followed as the gold standard for laboratory
DEVELOPING A PERSONAL PROTECTIVE EQUIPMENT SELECTION MATRIX
2 Health Security

biosafety. It provided a basis of recommendations to whichwe added flexibilities that considered alternative practicesfrom the literature concerned with clinical laboratory re-sponse to EVD cases.
For other potential occupational exposures, these types ofuniversal guidelines did not exist. In particular, there wasvirtually no information on which to base PPE recommen-dations for tasks associated with waste handling, cleaning,and maintenance operations. We identified very little in-formation about biological agent exposures among thesetypes of workers, especially in the US waste and environ-mental services industries.
To gather perspectives about hazards and controls in theseand other types of jobs, OSHA also met with labor andindustry representatives, state and local government agencies,and federal partners with expertise in airline and other publicand mass transportation operations, public safety and emer-gency response, public health, waste management, and deathcare (ie, mortuary and other postmortem) services—in ad-dition to healthcare and laboratory operations. These stake-holder interactions, though largely informal, were particularlyuseful in providing anecdotal information about job tasks andexposure hazards that were not available from other sources(ie, the scholarly literature). In collaborating with federalpartners, OSHA also worked to ensure alignment of rec-ommendations and requirements across agencies, includingwhen CDC and its National Institute for OccupationalSafety and Health (NIOSH) also developed guidance appli-cable to tasks to which our matrix applies.11-17 Additionally,we considered manufacturer guidelines and industry con-sensus standards (eg, ASTM standards for breakthroughtesting) for various pieces of PPE to ensure the capabilities ofsuch equipment matched the protection we aimed to achievewhen including it in the matrix.
An overarching goal in designing the matrix was to en-sure that recommendations would help employers complywith their obligations under the Occupational Safety andHealth (OSH) Act, to provide workers safe and healthyworking conditions. Whenever EBV and related hazards(eg, cleaning chemicals) pose workplace hazards, employerslikely need to comply with provisions from a combinationof OSHA requirements, including standards for blood-borne pathogens, PPE, and respiratory protection and thegeneral duty clause, Section 5(a)(1), of the OSH Act.18-21
For many of the exposure scenarios and PPE options weconsidered, there was no apparent consensus among avail-able scientific publications, government guidance, andstakeholder views to inform a clear way forward for rec-ommendations. To distill competing information streamsinto a single set of guidelines, we often had little choice butto defer to the collective knowledge of the authors and otherOSHA staff involved in the Ebola response. The authorshave infection prevention, industrial hygiene, epidemiology,and occupational medicine expertise, for example. Given theneed to issue guidance quickly, we considered the evidenceand made what we believed was the best decision possible
for various types of fluid-resistant or impermeable garments,respirators, and other types of PPE. Typically, our approachwas to discuss possible hazards and available controls andmake a recommendation that satisfied our team members’collective concerns for worker health. In these instances, wealso developed accompanying notes to explain additionalfactors that employers should consider when assessing haz-ards or identifying exposures, selecting PPE for workers, andimplementing elements of a comprehensive infection pre-vention and worker protection program.
In addition to explanatory notes, the matrix also includesflexible PPE options for most tasks it covers. These optionsidentify which equipment should be used at a minimumand which items might be needed during higher-risk worktasks. Users can also move between different PPE ensembleswithin the matrix as workers’ job tasks change. Wheneverpossible, we also considered alternative approaches for workpractices that could allow for varying levels of PPE for tasksin which exposures were controlled by other means. Con-sistent with OSHA standards requiring employers to per-form hazard analyses and provide appropriate PPE toprotect workers (eg, those for bloodborne pathogens, PPE,and respiratory protection), the PPE matrix leaves it up toemployers to recognize when tasks, such as aerosol-gener-ating procedures or exposures to large amounts of bodyfluids, warrant different or additional PPE, or when engi-neering and administrative controls reduce the need forprotective clothing and equipment.18-20
Results
Workers Without AppreciableEBV Exposure RiskWhile it was apparent that many workers performing taskscovered by OSHA’s matrix were at elevated risk for occu-pational EBV exposure, it was also clear that the majority ofUS workers had—and continue to have—low or no iden-tifiable risk for such exposure. Most types of employeeswork in office environments or other settings in which theyperform tasks that generally do not require them to wearPPE for infectious diseases.22 For workers in some of thesectors with the highest employment, such as manufactur-ing and construction occupations, there was no reason toanticipate EBV exposures, so no new or additional PPE iswarranted (beyond anything those workers already mightrequire for protection against routine job hazards). OSHAemphasized this point by including a column in its matrixfor workers without exposure.
General Work TasksFor general work tasks with possible EBV exposures, OSHA’srecommendations reflect the kind and severity of anticipated
BROWN ET AL
Volume 17, Number 3, 2019 3
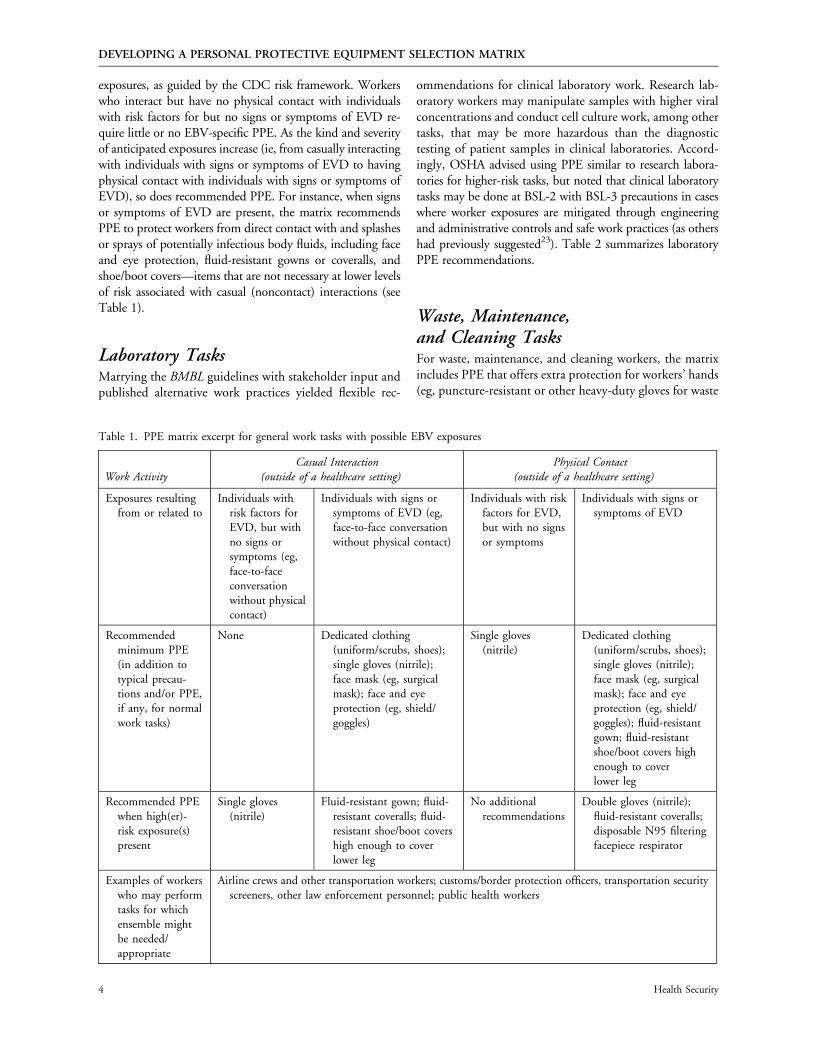
exposures, as guided by the CDC risk framework. Workerswho interact but have no physical contact with individualswith risk factors for but no signs or symptoms of EVD re-quire little or no EBV-specific PPE. As the kind and severityof anticipated exposures increase (ie, from casually interactingwith individuals with signs or symptoms of EVD to havingphysical contact with individuals with signs or symptoms ofEVD), so does recommended PPE. For instance, when signsor symptoms of EVD are present, the matrix recommendsPPE to protect workers from direct contact with and splashesor sprays of potentially infectious body fluids, including faceand eye protection, fluid-resistant gowns or coveralls, andshoe/boot covers—items that are not necessary at lower levelsof risk associated with casual (noncontact) interactions (seeTable 1).
Laboratory TasksMarrying the BMBL guidelines with stakeholder input andpublished alternative work practices yielded flexible rec-
ommendations for clinical laboratory work. Research lab-oratory workers may manipulate samples with higher viralconcentrations and conduct cell culture work, among othertasks, that may be more hazardous than the diagnostictesting of patient samples in clinical laboratories. Accord-ingly, OSHA advised using PPE similar to research labora-tories for higher-risk tasks, but noted that clinical laboratorytasks may be done at BSL-2 with BSL-3 precautions in caseswhere worker exposures are mitigated through engineeringand administrative controls and safe work practices (as othershad previously suggested23). Table 2 summarizes laboratoryPPE recommendations.
Waste, Maintenance,and Cleaning TasksFor waste, maintenance, and cleaning workers, the matrixincludes PPE that offers extra protection for workers’ hands(eg, puncture-resistant or other heavy-duty gloves for waste
Table 1. PPE matrix excerpt for general work tasks with possible EBV exposures
Work ActivityCasual Interaction
(outside of a healthcare setting)Physical Contact
(outside of a healthcare setting)
Exposures resultingfrom or related to
Individuals withrisk factors forEVD, but withno signs orsymptoms (eg,face-to-faceconversationwithout physicalcontact)
Individuals with signs orsymptoms of EVD (eg,face-to-face conversationwithout physical contact)
Individuals with riskfactors for EVD,but with no signsor symptoms
Individuals with signs orsymptoms of EVD
Recommendedminimum PPE(in addition totypical precau-tions and/or PPE,if any, for normalwork tasks)
None Dedicated clothing(uniform/scrubs, shoes);single gloves (nitrile);face mask (eg, surgicalmask); face and eyeprotection (eg, shield/goggles)
Single gloves(nitrile)
Dedicated clothing(uniform/scrubs, shoes);single gloves (nitrile);face mask (eg, surgicalmask); face and eyeprotection (eg, shield/goggles); fluid-resistantgown; fluid-resistantshoe/boot covers highenough to coverlower leg
Recommended PPEwhen high(er)-risk exposure(s)present
Single gloves(nitrile)
Fluid-resistant gown; fluid-resistant coveralls; fluid-resistant shoe/boot covershigh enough to coverlower leg
No additionalrecommendations
Double gloves (nitrile);fluid-resistant coveralls;disposable N95 filteringfacepiece respirator
Examples of workerswho may performtasks for whichensemble mightbe needed/appropriate
Airline crews and other transportation workers; customs/border protection officers, transportation securityscreeners, other law enforcement personnel; public health workers
DEVELOPING A PERSONAL PROTECTIVE EQUIPMENT SELECTION MATRIX
4 Health Security
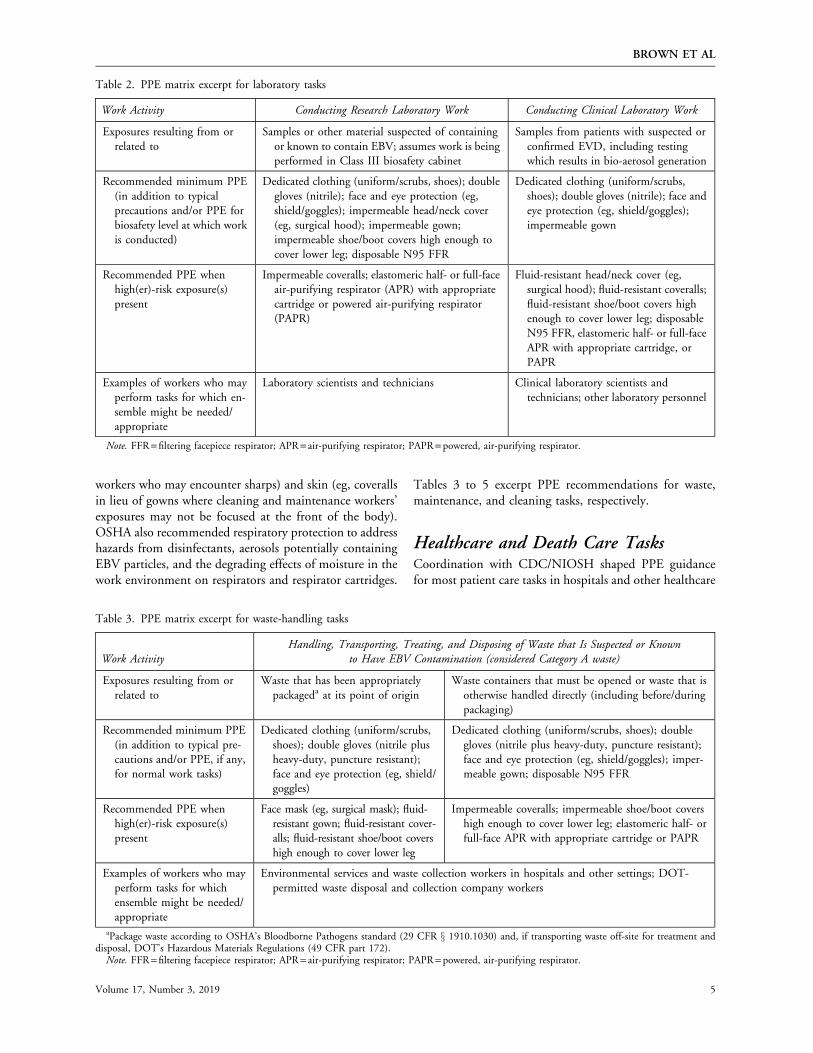
workers who may encounter sharps) and skin (eg, coverallsin lieu of gowns where cleaning and maintenance workers’exposures may not be focused at the front of the body).OSHA also recommended respiratory protection to addresshazards from disinfectants, aerosols potentially containingEBV particles, and the degrading effects of moisture in thework environment on respirators and respirator cartridges.
Tables 3 to 5 excerpt PPE recommendations for waste,maintenance, and cleaning tasks, respectively.
Healthcare and Death Care TasksCoordination with CDC/NIOSH shaped PPE guidancefor most patient care tasks in hospitals and other healthcare
Table 2. PPE matrix excerpt for laboratory tasks
Work Activity Conducting Research Laboratory Work Conducting Clinical Laboratory Work
Exposures resulting from orrelated to
Samples or other material suspected of containingor known to contain EBV; assumes work is beingperformed in Class III biosafety cabinet
Samples from patients with suspected orconfirmed EVD, including testingwhich results in bio-aerosol generation
Recommended minimum PPE(in addition to typicalprecautions and/or PPE forbiosafety level at which workis conducted)
Dedicated clothing (uniform/scrubs, shoes); doublegloves (nitrile); face and eye protection (eg,shield/goggles); impermeable head/neck cover(eg, surgical hood); impermeable gown;impermeable shoe/boot covers high enough tocover lower leg; disposable N95 FFR
Dedicated clothing (uniform/scrubs,shoes); double gloves (nitrile); face andeye protection (eg, shield/goggles);impermeable gown
Recommended PPE whenhigh(er)-risk exposure(s)present
Impermeable coveralls; elastomeric half- or full-faceair-purifying respirator (APR) with appropriatecartridge or powered air-purifying respirator(PAPR)
Fluid-resistant head/neck cover (eg,surgical hood); fluid-resistant coveralls;fluid-resistant shoe/boot covers highenough to cover lower leg; disposableN95 FFR, elastomeric half- or full-faceAPR with appropriate cartridge, orPAPR
Examples of workers who mayperform tasks for which en-semble might be needed/appropriate
Laboratory scientists and technicians Clinical laboratory scientists andtechnicians; other laboratory personnel
Note. FFR = filtering facepiece respirator; APR = air-purifying respirator; PAPR = powered, air-purifying respirator.
Table 3. PPE matrix excerpt for waste-handling tasks
Work ActivityHandling, Transporting, Treating, and Disposing of Waste that Is Suspected or Known
to Have EBV Contamination (considered Category A waste)
Exposures resulting from orrelated to
Waste that has been appropriatelypackageda at its point of origin
Waste containers that must be opened or waste that isotherwise handled directly (including before/duringpackaging)
Recommended minimum PPE(in addition to typical pre-cautions and/or PPE, if any,for normal work tasks)
Dedicated clothing (uniform/scrubs,shoes); double gloves (nitrile plusheavy-duty, puncture resistant);face and eye protection (eg, shield/goggles)
Dedicated clothing (uniform/scrubs, shoes); doublegloves (nitrile plus heavy-duty, puncture resistant);face and eye protection (eg, shield/goggles); imper-meable gown; disposable N95 FFR
Recommended PPE whenhigh(er)-risk exposure(s)present
Face mask (eg, surgical mask); fluid-resistant gown; fluid-resistant cover-alls; fluid-resistant shoe/boot covershigh enough to cover lower leg
Impermeable coveralls; impermeable shoe/boot covershigh enough to cover lower leg; elastomeric half- orfull-face APR with appropriate cartridge or PAPR
Examples of workers who mayperform tasks for whichensemble might be needed/appropriate
Environmental services and waste collection workers in hospitals and other settings; DOT-permitted waste disposal and collection company workers
aPackage waste according to OSHA’s Bloodborne Pathogens standard (29 CFR x 1910.1030) and, if transporting waste off-site for treatment anddisposal, DOT’s Hazardous Materials Regulations (49 CFR part 172).
Note. FFR = filtering facepiece respirator; APR = air-purifying respirator; PAPR = powered, air-purifying respirator.
BROWN ET AL
Volume 17, Number 3, 2019 5

Table 4. PPE matrix excerpt for maintenance tasks
Work Activity Performing Maintenance Work
Exposures resulting from orrelated to
Work in areas that have beenfully and appropriatelydecontaminated in a waythat eliminates EBV
Work in areas suspected or known to have EBV contamination,which have not been fully and appropriately decontaminatedin a way that eliminates EBV (eg, in emergencies)
Recommended minimum PPE(in addition to typical pre-cautions and/or PPE, if any,for normal work tasks)
None Dedicated clothing (uniform/scrubs, shoes); double gloves(nitrile plus heavy duty, as appropriate for hazard); face andeye protection (eg, shield/goggles); impermeable coveralls;impermeable shoe/boot covers high enough to cover lowerleg; elastomeric half- or full-face APR with appropriatecartridge
Recommended PPE whenhigh(er)-risk exposure(s)present
Dedicated clothing (uniform/scrubs, shoes)
Impermeable head/neck cover (eg, surgical hood); PAPR
Examples of workers who mayperform tasks for which en-semble might be needed/appropriate
Maintenance workers in all settings
Note. FFR = filtering facepiece respirator; APR = air-purifying respirator; PAPR = powered, air-purifying respirator.
Table 5. PPE matrix excerpt for cleaning (environmental services) tasks
Work Activity Cleaning and Disinfecting Environments
Exposures resultingfrom or related to
Environments with suspected orconfirmed EBV contamina-tion, but without significant,visible contamination fromblood or other body fluids
Environments with suspected orconfirmed EBV contaminationthat includes significant, visiblecontamination from blood orother body fluids
Environments with suspectedor confirmed EBV contam-ination and using disinfec-tants which may pose achemical hazard
Recommended min-imum PPE (inaddition to typicalprecautions and/or PPE, if any, fornormal worktasks)
Dedicated clothing (uniform/scrubs, shoes); double gloves(nitrile); face mask (eg, surgi-cal mask); face and eye pro-tection (eg, shield/goggles);fluid-resistant gown; fluid-resistant shoe/boot covershigh enough to cover lowerleg
Dedicated clothing (uniform/scrubs, shoes); double gloves (ni-trile plus heavy duty for chemicalprotection); face and eye protec-tion (eg, shield/goggles); imper-meable head/neck cover (eg,surgical hood); impermeablegown or coveralls (garmentshould fully cover skin); imper-meable apron; impermeable shoe/boot covers high enough to coverlower leg; elastomeric half- orfull-face APR with appropriatecartridge
Dedicated clothing (uniform/scrubs, shoes); double gloves(nitrile plus heavy duty forchemical protection); faceand eye protection (eg,shield/goggles); imperme-able head/neck cover(eg, surgical hood); imper-meable gown; impermeableshoe/boot covers highenough to cover lower leg;elastomeric half- or full-faceAPR with appropriatecartridge
Recommended PPEwhen high(er)-risk exposure(s)present
Double gloves (nitrile plus heavyduty); impermeable head/neck cover (eg, surgical hood);fluid-resistant coveralls; dis-posable N95 FFR or elasto-meric half- or full-face APRwith appropriate cartridge
PAPR Impermeable coveralls; imper-meable apron; PAPR
Examples of workerswho may performtasks for whichensemble mightbe needed or ap-propriate
Environmental services workers in all settings, including hospitals, aircraft and airports, and other areas
Note. FFR = filtering facepiece respirator; APR = air-purifying respirator; PAPR = powered, air-purifying respirator.
6 Health Security

settings, including those involving individuals with or underinvestigation for EVD. The matrix and CDC’s guidance foremergency department evaluation and management of pa-tients under investigation for EVD consistently describe PPEfor initial assessment of both symptomatic and asymptom-atic individuals.14 Similarly, the matrix is generally congru-ent with CDC’s guidance for healthcare workers duringmanagement of patients with confirmed EVD or EVD-likesymptoms.16 Exceptions to this centered on OSHA’s rec-ommendations and options for respiratory protection andmore protective guidelines for garments like coveralls,aprons, and head covers in some scenarios. Table 6 sum-marizes PPE recommendations for patient care tasks. Thediscussion section of this article further examines differencesbetween OSHA’s matrix and CDC’s guidelines.
Death care tasks, including packaging and transferringremains of individuals suspected of dying or known to havedied of EVD, are likely to involve exposure risks similar tosome healthcare tasks also covered in the matrix. Because ofthis, the matrix’s column of recommendations for deathcare activities closely follows adjacent columns for patientcare and transport tasks. Table 7 captures PPE recom-mendations for death care tasks.
OSHA’s full PPE selection matrix is available as part ofOSHA Fact Sheet 3761, ‘‘PPE Selection Matrix for Oc-cupational Exposure to Ebola Virus: Guidance for Com-mon Exposure Scenarios’’ (www.osha.gov/Publications/OSHA3761.pdf). A version of the matrix and explanatorynotes are also provided in Figure 1.
Discussion
General Approach to Developing PPERecommendationsPlanning the matrix initially required determining the ex-tent to which PPE should be used for worker protectionagainst EBV exposures, particularly given that the hierarchyof controls prioritizes elimination and substitution of haz-ards and reliance on engineering and administrative con-trols and safe work practices before requiring PPE. Indeed,we agree that these other elements of the hierarchy ofcontrols should be implemented before relying on PPE, ifat all possible. However, our extensive PPE recommenda-tions reflect the idea that expanded PPE use offers a morefeasible option for protecting workers in healthcare facili-ties, airports, and waste processing plants; aboard aircraft,ambulances, and other vehicles; and in other workplaceswhere EBV exposures are most likely during outbreaks.24 Insome cases, using PPE may be quicker and more realisticthan retrofitting workplaces with engineering controls (eg,installing negative-pressure isolation rooms with anteroomsin hospitals where they do not exist and where the need forthem may never arise) during an ongoing outbreak whenEBV hazards pose an immediate threat to worker health.
Using PPE as part of a comprehensive infection pre-vention program also enables workers to continue inter-acting with patients in healthcare settings, travelersrequiring entry screening at borders, and other potentiallyinfectious people without the use of certain engineeringcontrols, like physical barriers, that can preclude directpatient care, body temperature checks, and other interactivetasks. Although some occupational health practitioners maybe reluctant to turn to PPE instead of relying on the otherelements of the hierarchy, we also note that we are not thefirst to suggest that available options for preventing workerexposures to emerging pathogens like EBV may be limited,thus necessitating expanded PPE use.24
Evidence Gaps and StakeholderDisagreementsAs we noted in the methods section, the limited availableliterature relevant to worker protection against infectiousdiseases was a major hurdle to developing PPE recom-mendations, especially outside of health care and labora-tories. For employees handling infectious waste, forexample, we found only 1 study describing transmission ofinfectious agents (specifically, Mycobacterium tuberculosis)to US workers.25 Various studies from abroad describedgeneral waste handling work practices, hazards, and pre-cautions, but working conditions frequently differed fromthose in the United States. PPE recommendations for wastehandling, cleaning, and maintenance tasks were furthercomplicated by the fact that exposure to EBV was not theonly hazard these types of work pose. Additional chemical,physical, and safety hazards needed to be addressedalongside EBV exposures, a consideration reflected in thematrix’s inclusion of heavy-duty gloves and more protectiverespirators for these types of workers.
Even when published literature and other resources wereavailable to inform our PPE recommendations, we foundthat there was rarely full agreement among informationsources about what equipment to use. Despite our effort toinclude with the matrix robust explanatory notes aboutdifferent ways to implement OSHA’s guidance while stillprotecting workers, stakeholder viewpoints in particularwere strong and varied. Some workers wanted protectionsbeyond what OSHA deemed necessary. Some employersbelieved recommended precautions would be difficult toimplement. In other cases, employers may have providedworkers with overly protective equipment to be cautious,even though authoritative sources recommended lesserprotections. Specifically, several stakeholders advocated forstronger recommendations for respiratory protection wherenone were advised by or being considered for inclusion inguidance from federal agencies. This included during tasksother than medical and supportive care of hospitalizedpatients with EVD or other higher-risk exposure scenariosOSHA considered as triggers for recommending respiratory
Volume 17, Number 3, 2019 7
BROWN ET AL

Tab
le6.
PP
Em
atri
xex
cerp
tfo
rp
atie
nt
care
task
s
Wor
kA
ctiv
ity
Pro
vidi
ngM
edic
alan
dSu
ppor
tive
Car
e
Exp
osu
res
resu
ltin
gfr
omor
rela
ted
toC
are
ofin
div
idu
als
wit
hn
osi
gns,
sym
pto
ms,
orri
skfa
ctor
sfo
rE
VD
Car
eof
ind
ivid
ual
sw
ith
risk
fact
ors
for
EV
D,
but
wit
hn
osi
gns
orsy
mp
tom
s
Init
ial
eval
uat
ion
ofin
di-
vid
ual
sw
ith
susp
ecte
dE
VD
(in
clu
din
gth
ose
wit
hso
me
sign
sor
sym
pto
ms)
,bu
tw
ith
out
obvi
ous
blee
din
g,vo
m-
itin
g,or
dia
rrh
ea
Init
ial
eval
uat
ion
ofin
div
id-
ual
sw
ith
susp
ecte
dE
VD
wh
oh
ave
blee
din
g,vo
m-
itin
g,or
dia
rrh
ea,
orw
hen
thes
esy
mp
tom
sar
eli
kely
tod
evel
op;
ord
ur-
ing
hos
pit
aliz
atio
nof
in-
div
idu
als
wit
hsu
spec
ted
orco
nfi
rmed
EV
D
Car
eof
ind
ivid
ual
sw
ith
susp
ecte
dor
con
firm
edE
VD
,w
hic
hin
volv
esp
erfo
rmin
gae
roso
l-ge
n-
erat
ing
pro
ced
ure
s
Tra
nsp
orti
ng
sick
ind
ivid
u-
als
wit
hri
skfa
ctor
sfo
rE
VD
orw
ho
are
sus-
pec
ted
orco
nfi
rmed
toh
ave
EV
D
Rec
omm
end
edm
inim
um
PP
E(i
nad
dit
ion
toot
her
asp
ects
ofst
and
ard
pre
cau
tion
sfo
rh
ealt
hca
re)
Non
eN
one
Ded
icat
edcl
oth
ing
(un
i-fo
rm/s
cru
bs,
shoe
s);
dou
ble
glov
es(n
itri
le);
face
mas
k(e
g,su
rgic
alm
ask)
;fa
cean
dey
ep
ro-
tect
ion
(eg,
shie
ld/g
og-
gles
);fl
uid
-res
ista
nt
gow
nor
cove
ralls
(gar
-m
ent
shou
ldfu
llyco
ver
skin
)
Ded
icat
edcl
oth
ing
(un
i-fo
rm/s
cru
bs,
shoe
s);
dou
-bl
egl
oves
(nit
rile
);fa
cean
dey
ep
rote
ctio
n(e
g,sh
ield
/gog
gles
);im
per
me-
able
hea
d/n
eck
cove
r(e
g,su
rgic
alh
ood
);ap
pro
pri
-at
ely
flu
id-r
esis
tan
tor
im-
per
mea
ble
gow
nor
cove
ralls
(gar
men
tsh
ould
fully
cove
rsk
in);
imp
er-
mea
ble
apro
n;
imp
erm
e-ab
lesh
oe/b
oot
cove
rsh
igh
enou
ghto
cove
rlo
wer
leg;
dis
pos
able
N95
FF
R,
elas
tom
eric
hal
f-or
full-
face
AP
Rw
ith
app
rop
riat
eca
rtri
dge
,or
PA
PR
Ded
icat
edcl
oth
ing
(un
i-fo
rm/s
cru
bs,
shoe
s);
dou
ble
glov
es(n
itri
le);
face
and
eye
pro
tect
ion
(eg,
shie
ld/g
oggl
es);
im-
per
mea
ble
hea
d/n
eck
cove
r(e
g,su
rgic
alh
ood
);im
per
mea
ble
gow
nor
cove
ralls
(gar
men
tsh
ould
fully
cove
rsk
in);
imp
erm
eabl
eap
ron
;im
-p
erm
eabl
esh
oe/b
oot
cove
rsh
igh
enou
ghto
cove
rlo
wer
leg;
dis
pos
-ab
leN
95F
FR
,el
asto
-m
eric
hal
f-or
full-
face
AP
Rw
ith
app
rop
riat
eca
rtri
dge
,or
PA
PR
Ded
icat
edcl
oth
ing
(un
i-fo
rm/s
cru
bs,
shoe
s);
dou
-bl
egl
oves
(nit
rile
);fa
cean
dey
ep
rote
ctio
n(e
g,sh
ield
/gog
gles
);im
per
me-
able
hea
d/n
eck
cove
r(e
g,su
rgic
alh
ood
);im
per
me-
able
gow
nor
cove
ralls
(gar
men
tsh
ould
fully
cove
rsk
in);
imp
erm
eabl
eap
ron
;im
per
mea
ble
shoe
/bo
otco
vers
hig
hen
ough
toco
ver
low
erle
g;d
is-
pos
able
N95
FF
R,
elas
to-
mer
ich
alf-
orfu
ll-fa
ceA
PR
wit
hap
pro
pri
ate
cart
rid
ge,
orP
AP
R
Rec
omm
end
edP
PE
wh
enh
igh
(er)
-ris
kex
pos
ure
(s)
pre
sen
t
Non
eD
edic
ated
clot
hin
g(u
nif
orm
/sc
rubs
,sh
oes)
;si
ngl
egl
oves
(nit
rile
)
Flu
id-r
esis
tan
tap
ron
;d
is-
pos
able
N95
FF
R,
elas
-to
mer
ich
alf-
orfu
ll-fa
ceA
PR
wit
hap
pro
pri
ate
cart
rid
ge,
orP
AP
R
Non
eN
one
Non
e
Exa
mp
les
ofw
orke
rsw
ho
may
per
form
task
sfo
rw
hic
hen
sem
ble
mig
ht
ben
eed
ed/a
pp
rop
riat
e
Hea
lth
care
wor
kers
,in
clu
din
gp
hys
icia
ns,
nu
rses
,an
dot
her
s;ai
dw
orke
rs;
airl
ine
and
oth
ertr
ansp
orta
tion
wor
kers
Hea
lth
care
wor
kers
,in
clu
din
gp
hys
icia
ns,
nu
rses
,an
dot
her
sA
irm
edic
altr
ansp
ort
wor
k-er
s,em
erge
ncy
med
ical
serv
ices
(EM
S)w
orke
rs
Not
e.F
FR
=fi
lter
ing
face
piec
ere
spir
ator
;A
PR
=ai
r-p
urif
yin
gre
spir
ator
;P
AP
R=
pow
ered
,ai
r-p
urif
yin
gre
spir
ator
.
8 Health Security

protection (eg, during aerosol-generating healthcare andlaboratory procedures or cleaning and disinfection tasksthat could generate aerosols).
Differing views on respirators likely arise from thecomplexity of choosing which type of respirator to use forbiological agent exposures. There is no permissible expo-sure limit for biological agents. Identifying sources of ex-posure, determining how far from a source a worker mightbe exposed, and characterizing for how long and on whatenvironmental surfaces biological agents remain viablefurther that challenge. Existing tools for respiratory pro-tection selection generally require users to know at least theoccupational exposure limit and expected concentration ofthe respiratory hazard and, ideally, the concentration atwhich the hazard is immediately dangerous to life andhealth. For biological agents, those inputs may not be clearor available. Other gaps in information, including a greaterunderstanding about how EBV is transmitted, its infectionprocess, and determinants of clinical versus subclinicaloutcomes of exposure also complicate recommendationsfor PPE and other controls.26
In the interest of protecting workers, considering stake-holder input, and providing flexibility to employers in se-lecting specific PPE, OSHA’s matrix includes a widervariety of options for respirators than what sometimes ap-pears in other healthcare worker–focused guidance releasedover the course of the West Africa outbreak response.Specifically, OSHA determined that, though the assignedprotection factors of N95 filtering facepiece respirators,half- or full-face air-purifying respirators, and powered air-purifying respirators are different, any of these devicescould be used to protect workers from EBV exposure forcertain tasks, namely in health care and death care. Some UShospitals have successfully treated EBV-infected patientsusing various PPE ensembles and without nosocomial in-fection of participating healthcare workers or ancillary staff.
Accounts from such facilities suggest that even the leastprotective respirator among those mentioned—the N95filtering facepiece respirator—can be used in a PPE en-semble that successfully protects healthcare workers.27
Where chemical hazards or excessive moisture would makeusing a disposable N95 filtering facepiece respirator inap-propriate (eg, during cleaning tasks involving significantamounts of disinfectants or other liquids that could impairfiltration), OSHA recommended more durable and pro-tective respirators with cartridges designed for the hazard(s)of concern (eg, a combination chemical/particulate car-tridge).
For laboratory tasks, using the existing BMBL recom-mendations as the basis for corresponding sections of thePPE matrix satisfied stakeholders with interests in this area.Importantly, it also provided a reliable roadmap for navi-gating incongruent CDC and American Society of Mi-crobiology guidance for managing laboratory specimenspotentially containing EBV.28,29 Laboratory guidelinesfrom the BMBL manual provided high levels of protectionwhile also having a history of acceptability to and practi-cability for laboratory workers, managers, and otherstakeholders. Research facilities have operated for severaldecades with well accepted and widely practiced biosafetyprotocols, including exceptional capacity for agent con-tainment and worker protection when needed. Adaptationof BMBL recommendations allowed clear comparison ofcontrols, including PPE, between various biosafety levelsthat are routinely implemented in laboratories throughoutthe country.
CDC and OSHA RecommendationsTo help employers comply easily with OSHA requirementswhile also following other federal recommendations forprotecting public health and delivering clinical care, we
Table 7. PPE matrix excerpt for death care tasks
Work Activity Handling Dead Bodies
Exposures resulting from orrelated to
Work with bodies of individuals suspected of dying or known to have died of EVD, such asduring packaging of remains in an appropriate containment bag or transferring of packagedremains to a crematory
Recommended minimum PPE(in addition to typical pre-cautions and/or PPE, if any,for normal work tasks)
Dedicated clothing (uniform/scrubs, shoes); double gloves (nitrile); face and eye protection (eg,shield/goggles); impermeable head/neck cover (eg, surgical hood); impermeable coveralls;impermeable apron; impermeable shoe/boot covers high enough to cover lower leg; disposableN95 FFR, elastomeric half- or full-face APR with appropriate cartridge, or PAPR
Recommended PPE whenhigh(er)-risk exposure(s)present
None
Examples of workers who mayperform tasks for which en-semble might be needed/appropriate
Morticians; coroners; medical examiners; forensic scientists
Note. FFR = filtering facepiece respirator; APR = air-purifying respirator; PAPR = powered, air-purifying respirator.
BROWN ET AL
Volume 17, Number 3, 2019 9

Figure 1. OSHA’s full PPE selection matrix
DEVELOPING A PERSONAL PROTECTIVE EQUIPMENT SELECTION MATRIX
10 Health Security

BROWN ET AL
Volume 17, Number 3, 2019 11

aimed to align the PPE matrix as much as possible withCDC recommendations. However, there are still differ-ences between the matrix and CDC’s guidelines, as weunderstand them, and employers need to consider thesewhen developing their own workplace infection preventionprograms. For example, some CDC guidance for healthcareworkers calls for using N95 or better respirators but, whenspecifying what that means, describes an N95 filteringfacepiece respirator or powered air-purifying respirator.16
For similar exposures, OSHA’s matrix includes options forusing elastomeric air-purifying respirators with appropriatecartridges (in addition to N95 filtering facepiece respiratorsor powered air-purifying respirators). An elastomeric air-purifying respirator with at a least a half facepiece and anassigned protection factor of 10 or higher would be expectedto provide at least as much protection as a disposable N95
filtering facepiece respirator. Elastomeric air-purifying respi-rators also can be decontaminated for reuse—a benefit whendisposable N95 filtering facepiece respirators are scarce—andare appropriate when workers are using cleaning chemicalsfor which a combination particulate/chemical cartridge isneeded or where moisture would degrade the effectivenessof a disposable N95 filtering facepiece respirator.
It was not just the inclusion of elastomeric respiratorsthat separated the respiratory protection recommendationsin OSHA’s matrix from those of the CDC guidance. OSHA’smatrix recommends using respirators in several situationswhere CDC does not: for healthcare workers evaluating pa-tients suspected of having EVD but who are clinically stableand do not have bleeding, vomiting, or diarrhea;30 fortesting laboratory specimens that may contain EBV;29 andfor managing body fluid contamination in commercial
aMost workers in office environments normally do not require personal protective equipment (PPE) to perform their job tasks safely.In settings where there is no reason to anticipate exposure to Ebola virus (EBV), no new or additional PPE is warranted.bRisk factors for Ebola virus disease (EVD) include contact with blood or other body fluids or human remains of a patient known tohave or suspected of having EVD; residence in or travel to an area where EBV transmission is active; and direct handling of bats ornonhuman primates from disease-endemic areas.cSigns and symptoms of EVD include fever, severe headache, muscle pain, weakness, diarrhea, vomiting, abdominal (stomach) pain,and unexplained hemorrhage (bleeding or bruising).dHandling of samples from individuals with suspected or confirmed EVD, or research samples of EBV, should be done in containment(eg, in a biosafety cabinet, or BSC) to protect workers and to prevent contamination of surfaces outside the BSC. The OccupationalSafety and Health Administration (OSHA) recommends that clinical laboratory testing work be conducted, at a minimum, at BSL-2with BSL-3 precautions, using at least a Class II BSC, and that research work be conducted at BSL-4, using a Class III BSC. Followinga risk assessment and development of a comprehensive strategy for mitigating lab worker exposures, some types of specimens fromindividuals with suspected or confirmed EVD may be safely handled and tested in the core clinical laboratory (ie, at levels lower thanBSL-2 with 3 precautions) using an integrated approach. Such an approach may involve decontaminating and packaging samples incontainment in an EVD patient care area; use of specialized equipment that does not require opening/uncapping tubes, centrifugation,or other aerosol-generating procedures; training on and use of appropriate PPE; and proper waste handling and disposal techniques.ePackage waste according to OSHA’s Bloodborne Pathogens standard (29 CFR x 1910.1030) and, if transporting waste off-site fortreatment and disposal, the US Department of Transportation (DOT) Hazardous Materials Regulations (49 CFR part 172).fConsider the amount of vomit and watery excrement a patient is producing when selecting these items. Material thickness, fluidresistance, seam integrity, and the amount of time a worker can comfortably wear a protective garment should be considered whenselecting gowns, coveralls, and aprons. When the anticipated risk of exposure to blood and body fluids is low, employers shouldprovide workers with fluid-resistant garments. Fluid-resistant gowns should meet American National Standards Institute (ANSI)/Association for the Advancement of Medical Instrumentation (AAMI) PB70 Level 3 requirements. Fluid-resistant coveralls should bemade of fabric and constructed with seams that pass: (1) American Association of Textile Chemists and Colorists (AATCC) 42 ImpactPenetration Test at 1 g or below and AATCC 127 Hydrostatic Head Test at 50 cm or above, or (2) EN 20811 Hydrostatic Head Testat 50 cm or above, or (3) American Society for Testing and Materials (ASTM) F1670 Synthetic Blood Penetration Resistance Test, or(4) International Organization for Standardization (ISO) 16603 Synthetic Blood Penetration Resistance Test (at 3.5 kilopascal [kPa]or above). When the anticipated risk of exposure to blood and body fluids is high, employers should provide workers with imper-meable garments. Impermeable isolation or surgical gowns should meet the ANSI/AAMI PB70 Level 4 requirements. Impermeablecoveralls should be made of fabric and constructed with seams that pass ASTM F1671 Bloodborne Pathogen Penetration ResistanceTest or ISO 16604 Bloodborne Pathogen Penetration Resistance Test (at 14 kPa or higher). In the absence of manufacturer-provideddata on seams, select a garment constructed with an appropriate seaming technique (eg, taped seams).gIn instances where workers may be exposed to aerosols (eg, as a result of spraying liquids or air during cleaning) suspected of or knownto contain EBV, medically qualified workers must use, at a minimum, a National Institute for Occupational Safety and Health(NIOSH)–approved, fit-tested N95 respirator. A full-face elastomeric respirator or powered air-purifying respirator (PAPR) offers ahigher level of protection (ie, greater assigned protection factor) than a half-mask elastomeric respirator or disposable N95 filteringfacepiece respirator. When using elastomeric respirators or PAPRs while using disinfectants that may pose a chemical hazard, acombination particulate/chemical cartridge may be necessary to protect workers from exposure to the chemicals in addition to EBVparticles. Note that disposable N95 respirators and certain cartridges for elastomeric respirators may be adversely affected by an increasein moisture and spray from certain work tasks, including during cleaning and decontamination. In such instances, or during other tasksto improve worker comfort, a supplied-air respirator may be an alternative.
DEVELOPING A PERSONAL PROTECTIVE EQUIPMENT SELECTION MATRIX
12 Health Security

passenger aircraft.31 We believe that the uncertainty aboutpotential sources of infection in these situations and, again,the transmission routes through which EBV may spread,warrant respiratory protection: Patients, travelers, and speci-mens may expose workers to infectious particles if aerosols aregenerated through natural (eg, a person vomiting) or me-chanical (eg, vortexing a sample, disturbing material whilecleaning) processes. OSHA also recommends respirators inthe matrix’s column for workers handling dead bodies ofindividuals who may have died from EVD, while CDCdoes not; however, CDC’s guidelines apply to handling ofremains that are already packaged in a healthcare setting (eg,by healthcare workers in higher level PPE), whereas OSHA’srecommendations cover a broader range of death care tasks.15
Workers handling dead bodies may be at similar exposure riskas healthcare workers until the remains are in sealed, decon-taminated packaging.
Other differences between the OSHA matrix and CDC’srecommendations involve the extent to which the 2 agen-cies recommend skin and mucous membrane protection forvarious workers. Keeping with OSHA’s strategy of mini-mizing exposed skin that could come into contact withEBV in blood, body fluids, or other potentially infectiousmaterials, OSHA sometimes recommends more extensivebarrier protection compared to CDC’s recommendations.For healthcare workers evaluating clinically stable patientssuspected of having Ebola, OSHA recommends using agown or coverall along with an apron for higher-risk ex-posures and to protect against unexpected bulk contami-nation (eg, vomitus, feces), whereas CDC’s guidelines noteonly a gown or coverall.30 For workers testing clinicalspecimens that may contain EBV, OSHA included doubleinstead of single gloves, along with a head covering, shoe/boot covers, and coveralls for higher-risk exposures. Theseitems were not part of CDC’s recommended ensemble forsimilar activities, which includes gloves, fluid-resistant orimpermeable gown, face mask, and eye protection.29 Otherdifferences not specifically discussed here may also resultfrom how workers’ tasks are categorized. For example, thetask-based matrix may prompt airline personnel managingpotentially infectious body fluids to use different PPE, suchas heavy-duty gloves and additional barrier protections,than they would when following CDC’s occupation-basedEVD guidance.31
Matrix ApplicationIn using the final matrix, employers and workers must bemindful that the guidance presents combinations of PPEitems selected for certain types of work tasks and sources ofexposure. Particularly in cases where skin or mucousmembrane exposure to infectious blood or other bodyfluids is likely, each column of the matrix recommendsusing items together in a way that we believe will providesufficient coverage of the skin, eyes, nose, and mouth. Fortasks in which aerosol exposures are concerns, the matrix
recommends equipment that functions to prevent contactexposures while also protecting workers from inhaling EBVparticles or hazardous chemicals. When implementing therecommendations using various brands or types of PPE,employers should ensure that the individual items still meetthis objective and that fit-testing supports the use of specificitems together, such as a certain face shield or surgical hoodwith a certain respirator. That may require a qualified in-dustrial hygienist to manage quantitative and qualitativerespirator fit testing protocols for workers in full ensemblesof PPE.
Importantly, PPE for high-consequence hazards, includ-ing EBV, is only effective when workers properly put it onand remove it. This is shown in lessons learned from traininginitiatives in which healthcare workers failed to demonstratecompetency in PPE donning or doffing during training andassessment, including when fluorescent or chemiluminescentdyes applied to PPE were used as markers of would-be ex-posures under real-life work conditions.32 However, as theaim of OSHA’s PPE matrix is to help employers identify thetypes of PPE their workers may need for various jobs wherewe foresaw potential EBV exposure, describing a full don-ning and doffing regimen was outside the scope both of thatwork and this article. Other sources, such as CDC, offerprotocols for donning and doffing certain PPE ensembles,including for healthcare workers.
The amount of time a worker can wear a PPE ensembleor a particular piece of PPE needed for a task is anotherimportant consideration for ensuring the safety and healthof workers, particularly when they are at risk for exposure toEBV and related hazards if there are breaches in establishedwork protocols or the PPE itself. Worker stay time in PPEdepends on a number of factors, some of which may bedifficult to ascertain, including the severity of the hazard thePPE must withstand; the degradation rate or point of PPEfailure (ie, permeation rate, breakthrough time from initialexposure until virus particles and/or fluid reach the inside ofa garment); an individual worker’s physical condition andtolerance for the PPE; heat stress caused or made worse bythe PPE; and overall level of worker fatigue, which may alsobe made worse by the PPE or may compromise a worker’sability to use the PPE properly or remove the ensemblewithout contaminating him- or herself.
For all tasks where OSHA recommends wearing fluid-resistant or impermeable garments, considering the amountof blood, vomit, and watery excrement (eg, diarrhea) apatient is producing or that is in a contaminated environ-ment should influence user selection of specific fluid-re-sistant or impermeable items. In accordance with NIOSH’sfluid-resistant or impermeable garment document, OSHArecommends providing workers with fluid-resistant gar-ments when the anticipated risk of exposure to blood andbody fluids is low and impermeable garments when theanticipated risk of exposure to blood and body fluids ishigh.17 Because the PPE matrix cannot describe everypossible exposure scenario, it indicates to employers
BROWN ET AL
Volume 17, Number 3, 2019 13

whether specific garments should be fluid-resistant or fluid-and virus-impermeable based on generally anticipated ex-posures. Employers should determine where exposures arefocused (eg, on the center of the body, where the additionof an apron might be most protective, versus on the limbs,where coveralls or shoe/boot covers might be more use-ful). Examination of a variety of commercially availableprotective garments also indicated that other consider-ations beyond fluid-resistant or impermeable coatings onfabric affect the overall resistance or impermeability ofthe garment, including material thickness and seam andzipper construction and placement. Employers also needto consider other extenuating factors, such as fluid pen-etration at pressure points, permeation rate and break-through time, and garment or equipment performanceunder the standardized testing conditions NIOSH’s re-search identified.
Providing flexible PPE options whenever possible madethe most sense for addressing the practicability challenges aswell as for ensuring employers could use different variationsof PPE while still protecting their workers. The PPE matrixconsolidates a set of recommendations for protectiveequipment and garments for workers performing a range ofwork tasks, with those tasks and sources of exposure typi-cally described in ways that allow for employers to selecteither enhanced PPE for higher-risk exposures or selectdifferent PPE items as a worker’s tasks or exposure(s) movehim or her to a different column of the matrix. Flexibilityin how employers assess and control worker exposure isconsistent with the philosophy of the hierarchy of controlsitself, in that it allows for decision making in the risk-control process rather than adopting a rigid frameworkfor hazard abatement.33 An employer should provide PPEto workers using the task- and exposure-based categoriesof the matrix. If work tasks or sources of exposure change,an employer can look at the recommended equipment forhigher-risk exposures or across the other columns of thematrix and provide different or more protective PPE forworkers as needed. In some instances, such as when lab-oratory or waste workers perform job functions similar tothose of healthcare workers, the flexible, task-based de-sign of the matrix allows users to follow recommenda-tions that most closely align with their job duties, ratherthan job title, at any given time.
Conclusions
Protective measures, including PPE, for preventing occu-pational exposure to EBV depend on the type of work, riskof encountering sources of EBV, and the nature of otherpotential hazards to which workers may be simultaneouslyexposed. OSHA developed consolidated PPE recommen-dations applicable to most workers in the United Stateswho are likely to have EBV exposure. When the PPE matrixwas originally published, there was insufficient information
in the scholarly literature on which to base the recom-mendations. However, consideration of job hazards andexposure risks alongside stakeholder needs and expert inputyielded recommendations suitable for a broad range ofwork tasks that may be associated with EBV exposure.
Continued debate over what PPE is appropriate forcertain work tasks and exposure scenarios highlights re-maining gaps in knowledge. Particularly, more research isneeded to explore EBV’s routes of transmission, includingcontrolled studies to explore the possibility for near- andfar-field aerosol transmission that would warrant enhancedrespiratory protection for workers performing tasks currentlyconsidered to be less hazardous, such as casual (noncontact)interaction outside of healthcare settings with individualswith signs or symptoms of EVD. More work is also neededto inform decision making about worker stay times in PPEensembles, as well as to identify PPE that minimizes heatstress, worker fatigue, and other undesired side effects ofwearing such equipment.
Given these gaps, PPE recommendations and other typesof infection prevention guidelines must continue to beupdated if and when new trials or other robust studies offerbetter data to support them. In the meantime, OSHA’sPPE matrix remains applicable for preparedness and plan-ning for safe and effective response to possible future do-mestic EVD cases.
Acknowledgments
The authors thank their OSHA and interagency col-leagues who were involved in the development of guid-ance on which the matrix was based and who contributedtheir expertise to development of the matrix and reviewof this manuscript. In particular, the authors thank for-mer OSHA Assistant Secretary Dr. David Michaels andformer Deputy Assistant Secretary Jordan Barab for theirinput on the matrix and drafts of this manuscript. Theauthors also thank Drs. Thomas Nerad and MargyLambert for their input on the matrix. The opinionsexpressed in this article are those of the authors and donot necessarily represent the views of the US Departmentof Labor (DOL)/OSHA. Mention(s) of products do notconstitute endorsements by DOL/OSHA or the authorsand are included only as examples of types of PPE.
References
1. World Health Organization. Ebola Virus Disease: Demo-cratic Republic of the Congo. External Situation Report 32.March 12, 2019. https://apps.who.int/iris/bitstream/handle/10665/311242/SITREP_EVD_DRC_20190310-eng.pdf?ua=1.Accessed March 14, 2019.
2. Occupational Safety and Health Administration. PPE selectionmatrix for occupational exposure to Ebola virus. OSHA-3761.
DEVELOPING A PERSONAL PROTECTIVE EQUIPMENT SELECTION MATRIX
14 Health Security

November 24, 2014. https://www.osha.gov/Publications/OSHA3761.pdf. Accessed January 16, 2019.
3. Occupational Safety and Health Administration. Disastercleanup and recovery PPE matrix. OSHA-3898. October2016. https://www.osha.gov/Publications/OSHA3898.pdf.Accessed January 16, 2019.
4. Occupational Safety and Health Administration. OSHA/NIOSH Interim Guidance (April 2005). Chemical - Biological- Radiological - Nuclear (CBRN) Personal ProtectiveEquipment Selection Matrix for Emergency Responders.2005. https://www.osha.gov/SLTC/emergencypreparedness/cbrnmatrix/index.html. Accessed January 16, 2019.
5. Centers for Disease Control and Prevention. Epidemiologicrisk factors to consider when evaluating a person for exposureto Ebola virus. October 27, 2014. https://web.archive.org/web/20141028031924/http://www.cdc.gov/vhf/ebola/exposure/risk-factors-when-evaluating-person-for-exposure.html. Ac-cessed January 16, 2019.
6. Mekibib B, Arien KK. Aerosol transmission of filoviruses.Viruses 2016;8(5):E148.
7. Jaax N, Jahrling P, Geisbert T, et al. Transmission of Ebolavirus (Zaire strain) to uninfected control monkeys in a bio-containment laboratory. Lancet 1995;346(8991-8992):1669-1671.
8. Brosseau LM, Jones R. Health workers need optimal respiratoryprotection for Ebola. CIDRAP September 17, 2014. http://www.cidrap.umn.edu/news-perspective/2014/09/commentary-health-workers-need-optimal-respiratory-protection-ebola. Ac-cessed January 16, 2019.
9. Siegel JD, Rhinehart E, Jackson M, Chiarello L; Health CareInfection Control Practices Advisory Committee. 2007 Guide-line for isolation precautions: preventing transmission of infec-tious agents in health care settings. Am J Infect Control 2007;35(10 Suppl 2):S65-S164.
10. Chosewood LC, Wilson DE, eds. Biosafety in Microbiologicaland Biomedical Laboratories. 5th ed. Washington, DC: USDepartment of Health and Human Services; 2009.
11. Centers for Disease Control and Prevention. Infection preven-tion and control recommendations for hospitalized patientsunder investigation (PUIs) for Ebola virus disease (EVD) in U.S.hospitals. Updated September 3, 2015. http://www.cdc.gov/vhf/ebola/healthcare-us/hospitals/infection-control.html. AccessedJanuary 16, 2019.
12. Centers for Disease Control and Prevention. Interim guid-ance about Ebola virus infection for airline flight crews,cleaning personnel, and cargo personnel. Updated August 2,2014. https://web.archive.org/web/20140803034710/http://www.cdc.gov/quarantine/air/managing-sick-travelers/ebola-guidance-airlines.html. Accessed January 16, 2019.
13. Centers for Disease Control and Prevention. Guidance forcollection, transport, and submission of specimens for Ebolavirus testing. Reviewed June 1, 2018. http://www.cdc.gov/vhf/ebola/hcp/interim-guidance-specimen-collection-submission-patients-suspected-infection-ebola.html. Accessed January 16,2019.
14. Centers for Disease Control and Prevention. Identify, isolate,inform: emergency department evaluation and managementfor patients under investigation (PUIs) for Ebola virus dis-ease (EVD). Updated December 29, 2015. https://www.cdc.gov/vhf/ebola/healthcare-us/emergency-services/emergency-departments.html. Accessed January 16, 2019.
15. Centers for Disease Control and Prevention. Guidance for safehandling of human remains of Ebola patients in U.S. hospitalsand mortuaries. Updated February 11, 2015. https://www.cdc.gov/vhf/ebola/healthcare-us/hospitals/handling-human-remains.html. Accessed January 16, 2019.
16. Centers for Disease Control and Prevention. Guidance onpersonal protective equipment (PPE) to be used by health-care workers during management of patients with confirmedEbola or persons under investigation (PUIs) for Ebola whoare clinically unstable or have bleeding, vomiting, or diarrheain U.S. hospitals, including procedures for donning anddoffing PPE. Updated November 17, 2015. http://www.cdc.gov/vhf/ebola/hcp/procedures-for-ppe.html. Accessed Janu-ary 16, 2019.
17. National Institute for Occupational Safety and Health. Con-siderations for selecting protective clothing used in healthcarefor protection against microorganisms in blood and bodyfluids. January 30, 2018. https://www.cdc.gov/niosh/npptl/topics/protectiveclothing/default.html. Accessed January 16,2019.
18. Respiratory Protection. 29 C.F.R. Sect. 1910.134. 2012.19. Bloodborne Pathogens. 29 C.F.R. Sect. 1910.1030. 2012.20. Personal Protective Equipment. 29 C.F.R. Sect. 1910 Sub-
part I. 2016.21. Occupational Safety and Health Act. U.S. Code. Sect. Ch.
15 et seq. 1970.22. Bureau of Labor Statistics. National Occupational Employ-
ment and Wage Estimates. May 2017. https://www.bls.gov/oes/current/oes_nat.htm#00-0000. Accessed January 17, 2019.
23. Iwen PC, Garrett JL, Gibbs SG, et al. An integrated ap-proach to laboratory testing for patients with Ebola virusdisease. Lab Med 2014;45(4):e146-e151.
24. Ringen K, Landrigan PJ, Stull JO, Duffy R, Melius J,McDiarmid MA. Occupational safety and health protectionsagainst Ebola virus disease. Am J Ind Med 2015;58(7):703-714.
25. Johnson KR, Braden CR, Cairns KL, et al. Transmission ofMycobacterium tuberculosis from medical waste. JAMA2000;284(13):1683-1688.
26. Judson S, Prescott J, Munster V. Understanding Ebola virustransmission. Viruses 2015;7(2):511-521.
27. Hewlett AL, Varkey JB, Smith PW, Ribner BS. Ebola virusdisease: preparedness and infection control lessons learnedfrom two biocontainment units. Curr Opin Infect Dis 2015;28(4):343-348.
28. American Society for Microbiology. Interim laboratory guide-lines for handling/testing specimens from cases or suspectedcases of hemorrhagic fever virus (HFV). September 10, 2014.https://smlc.cl/sitio/ebola/ASM-HFV-Ebola-Laboratory-Interim-Guidance.pdf. Accessed January 16, 2019.
29. Centers for Disease Control and Prevention. Guidance forU.S. laboratories for managing and testing routine clinicalspecimens when there is a concern about Ebola virus disease.June 1, 2018. https://www.cdc.gov/vhf/ebola/laboratory-personnel/safe-specimen-management.html. Accessed January16, 2019.
30. Centers for Disease Control and Prevention. For U.S.healthcare settings: donning and doffing personal protectiveequipment (PPE) for evaluating persons under investigation(PUIs) for Ebola who are clinically stable and do not havebleeding, vomiting, or diarrhea. November 7, 2015. https://
BROWN ET AL
Volume 17, Number 3, 2019 15

www.cdc.gov/vhf/ebola/healthcare-us/ppe/guidance-clinically-stable-puis.html. Accessed January 16, 2019.
31. Centers for Disease Control and Prevention. Interimguidance for Ebola virus cleaning, disinfection, and wastedisposal in commercial passenger aircraft. February 18, 2016.https://www.cdc.gov/vhf/ebola/prevention/cleaning-commercial-passenger-aircraft.html. Accessed January 16, 2019.
32. Bell T, Smoot J, Patterson J, Smalligan R, Jordan R. Ebola virusdisease: the use of fluorescents as markers of contamination forpersonal protective equipment. IDCases 2014;2(1):27-30.
33. Winder C, Makin AM. Going beyond OSH risk assessmentsusing matrices. In: Aven T, Vinnem JE, eds. Risk, Reliability,and Societal Safety. London, UK: Taylor and Francis; 2007.
Manuscript received January 23, 2019;revision returned March 15, 2019;accepted for publication March 18, 2019.
Address correspondence to:Christopher K. Brown, PhD, MPH, CPH
Directorate of Technical Support and Emergency ManagementOccupational Safety and Health Administration
US Department of Labor200 Constitution Ave., NW
Washington, DC 20210
Email: [email protected]
DEVELOPING A PERSONAL PROTECTIVE EQUIPMENT SELECTION MATRIX
16 Health Security





























