Embed Size (px)
Citation preview

American University of Armenia
School of Public Health
Determinants of Iron Deficiency Anemia among
Hospitalized Children Aged 6-59 Months in Armenia
A Case-Control Study
Master of Public Health Integrating Experience Project
Professional Publication Framework
By
Anush Mnatsakanyan, MD
Advising Team:
Anahit Demirchyan, MD, MPH
Haroutune Armenian, MD, DrPH
Kristina Akopyan, MD, MPH
Yerevan, Armenia
2016

i
Acknowledgements
I would like to express my sincere gratitude to my advising team for making this project
real, for guiding and supporting me throughout this long way to the goal.
My deep appreciation to Dr. Anahit Demirchyan for her continuous help, smart ideas and
advice and for clarifying every doubt in a very kind and friendly way.
I would like to express my thankfulness to Dr. Haroutune Armenian for his expert
opinion and for sharing his inspiring philosophic approach towards the research.
My heartfelt gratitude to Dr. Kristina Akopyan for her enthusiasm, motivation and
encouragement. She was the one who made me feel confident, believe that everything is doable,
and success is inevitable.
I would like to express my grateful thanks to Dr. Varduhi Petrosyan for her parental
support and encouragement. I would expand my thankfulness to all the faculty members and
professors for sharing their knowledge and making us professionals.
I would like to thank the administration and staff of Arabkir JMC, Muratsan UH and
Hematology Center after Prof. Yeolyan for giving their permission and making this study
possible.
This project would not be possible without my friends. Thanks to all of my MPH friends,
especially Zaruhi Arakelyan, Tatevik Movsesyan, Nare Navasardyan and Vahe Krmoyan for
their dedication. I am very grateful to my pediatrician friends Azatuhi Ashotyan and Tehmine
Ghalechyan for their devoted help and support.
My deepest appreciation to my parents and brothers for making my wishes and dreams
come true, and to my sister Mariam for her great support. My warmest thanks to Vahe for his
love and infinite encouragement.
Thanks to my life for the opportunity to achieve my goals.

ii
List of Abbreviations
CI Confidence interval
CRP C-reactive protein
DALY Disability adjusted life years
DNA Deoxyribonucleic acid
FFQ Food frequency questionnaire
Hb Hemoglobin
ID Iron deficiency
IDA Iron deficiency anemia
IRB Institutional review board
MCV Mean corpuscular volume
OR Odds ratio
RBC Red blood cells
SD Standard deviation
SES Socioeconomic status
SF Serum ferritin
WHO World Health Organization
YLD Years lived with disability

iii
Table of Content
Abstract ........................................................................................................................................... v
1. Introduction/Literature Review ............................................................................................... 1
1.1 Anemia ............................................................................................................................. 1
1.2 Iron Deficiency Anemia ................................................................................................... 1
1.3 Prevalence and Disease Burden ....................................................................................... 2
1.4 Diagnosis .......................................................................................................................... 3
1.5 Consequences of Iron Deficiency Anemia ....................................................................... 4
1.6 Risk Factors ...................................................................................................................... 5
1.7 Situation in Armenia ........................................................................................................ 6
1.8 Rationale for the current study ......................................................................................... 6
1.9 Aims of the Study and Research Question ............................................................................ 7
2. Methods ................................................................................................................................... 7
2.1 Study Design .................................................................................................................... 7
2.2 Study Population .............................................................................................................. 7
2.3 Sample Size ...................................................................................................................... 9
2.4 Data Collection ................................................................................................................. 9
2.5 Study Instrument ............................................................................................................ 11
2.6 Study Variables .............................................................................................................. 11
2.7 Analysis .......................................................................................................................... 12
2.8 Ethical Considerations.................................................................................................... 12
3. Results ................................................................................................................................... 13
3.2 Descriptive statistics ............................................................................................................ 14
3.3 Simple Logistic Regression ................................................................................................. 15
3.4 Multiple Logistic Regression .............................................................................................. 16
4. Discussion .............................................................................................................................. 17
4.1 Strengths of the study ..................................................................................................... 17
4.2 Study Limitations ........................................................................................................... 18
4.3 Main Findings ................................................................................................................ 19
5. Recommendations ................................................................................................................. 22
6. Conclusion ............................................................................................................................. 23

iv
References ..................................................................................................................................... 24
Table 1. Descriptive Statistics of Children 6-59 Months of Age with IDA vs. without Anemia 32
Table 2. ORs, CIs and p-values from simple logistic regression and age-adjusted multiple
logistic regression analyses between IDA status and independent variables ............................... 37
Table 3. Multiple logistic regression model of determinants of IDA among hospitalized children
6-59 months of age........................................................................................................................ 41
Appendix 1. Medical Record Review Form ................................................................................ 42
Appendix 2. Journal Form ........................................................................................................... 43
Appendix 3. Questionnaire for Telephone Interview with Mothers ............................................ 44
Appendix 4. Informed Consent Form .......................................................................................... 60

v
Abstract
Background: Anemia is a problem of public health significance worldwide with 32.9%
prevalence globally. Preschool children and pregnant women are the most vulnerable groups
regarding anemia. According to the latest data from Armenia, the prevalence of anemia among
children 6-59 months of age is about 37%. Iron deficiency is the most common nutritional
disorder worldwide and, globally, it is responsible for 60% of anemia cases. Iron deficiency
anemia (IDA) results in impairment of motor and mental development of the child and has long-
lasting health consequences. Lack of data about iron deficiency anemia and its risk factors
among children in Armenia stood as a rationale to conduct the current study.
Aim: To identify independent risk factors of iron-deficient anemia among hospitalized children
aged 6-59 months in Armenia.
Methods: The study utilized case-control design, where the cases were hospitalized children
aged 6-59 months with IDA and controls were children without any type of anemia from the
same population group. Study settings were the two major pediatric hospitals and the specialized
hematology center in Yerevan city, which are referral hospitals throughout Armenia. Data was
collected from hospital records and mothers of sampled children through telephone interview.
Collected data has been analyzed descriptively, which was followed by bivariate and
multivariate logistic regression analyses in order to find independent risk factors of IDA among
the study population.
Results: Overall, 213 participants – 71 cases and 142 controls were included in the study. The
study identified six independent risk factors of IDA. Younger children (OR=0.89; p<0.001), as
well as children with lower birth weight (OR=0.99; p<0.001) had higher odds of having IDA.
Consumed amount of cow’s milk per day measured in cups (OR=1.51; p=0.030) and previous
history of child’s anemia (OR=3.43; p=0.043) were both independently related to higher odds of
having IDA, while higher frequency of consuming sweets per week (OR=0.78; p=0.006) and
higher food diversity score (OR=0.76; p=0.034) reduced the odds of having IDA.
Conclusion: The independent risk factors of IDA among hospitalized children aged 6-59 months
in Armenia found in this study were somewhat expected and have been previously reported in
the literature. The study findings indicated the need to pay more attention to preventing iron
deficiency among younger children and those born low birth weight and to completely treat any
identified anemia among children. Counseling of mothers on child nutrition, which should
include promotion of diverse diet and avoidance of cow’s milk, could have positive reflection in
prevention of IDA. The protective effect of higher weekly frequency of sweets consumption on
IDA found in this study needs further investigation and more rigorous measurement, as literature
provides contradicting results on this association.

1
1. Introduction/Literature Review
1.1 Anemia
Anemia is a condition defined as decreased hemoglobin level or red blood cell (RBC)
mass below the threshold, which is insufficient to meet the body’s physiological demand.1,2
According to World Health Organization, in public health terms anemia is referred to low
hemoglobin level.1 The normal range of hemoglobin values varies according to age, sex,
smoking status, pregnancy, residential altitude above sea level, etc.1 Anemia is one of the most
prevalent disorders worldwide and stands as a huge public health problem in non-industrialized
and even in many industrialized countries.3 Anemia affects about 2 billion people worldwide,
which is almost 33% of global population.4 Three major groups of factors lead to anemia: genetic
disorders, infectious diseases and inadequate nutrition. Iron, folic acid, vitamin B12, vitamin A,
protein energy malnutrition are the most common nutritional factors contributing to anemia
status.5
1.2 Iron Deficiency Anemia
Iron deficiency (ID) is the top cause of anemia.6 Moreover, iron deficiency is the most
common single-nutrient deficiency in the world, mainly in developing countries.2,7 Iron is one of
the most important micronutrients for the human organism. It is a key element, playing role in
different biological processes such as respiration, energy generation, DNA synthesis, cell
proliferation, etc.8 Iron is a determining element in hemoglobin molecule structure5, hence, iron-
deficiency can stand as a direct cause of anemia.9 Iron deficiency is a condition, when body iron
stores are reduced, but are sufficient for adequate hemoglobin synthesis. Iron deficiency anemia
refers to more severe condition, when iron stores are not enough to produce the required level of
hemoglobin. This results in anemia and microcytic (reduced cell volume) hypochromic red

2
cells.6 Iron deficiency can be a result of inadequate iron intake and absorption, increased iron
demand or excessive iron losses (i.e. with blood loss).5,6,10 About 80% of iron stock in a term
newborn is accumulated during the third trimester of pregnancy. It is a source for iron supply in
children until 4-6 months of age. Children up to 6 months of age are relatively protected from
iron-deficiency. After 6 months iron stores are depleted, though child’s rapid growth continues.
This results in scarcity of iron supply from the internal stock, therefore, in the case of inadequate
iron consumption, child develops iron deficiency and consequently iron deficiency anemia.2,7
1.3 Prevalence and Disease Burden
Anemia is a global public health problem in low, middle and even high-income
countries.11 According to 2010 data on worldwide prevalence of anemia, 32.9% of the global
population suffered from anemia. The disease burden for anemia is 68.3 million years lived with
disability (YLDs).4 Preschool children and pregnant women are the groups mostly affected from
anemia. The World Health Organization’s Database on Anemia for 1993-2005, which covered
almost half of the worldwide population, revealed 1.62 billion people to be anemic globally. It
also demonstrated that 47.4% of preschool-age children and 41.8% of pregnant women had
anemia.11 Another data from 2011 showed a slightly reduced prevalence of anemia, which was
43% (273 million) among children and 38% (32 million) among pregnant women worldwide.12
Children under 5 years old have the highest prevalence of anemia, as well as the least noticeable
change in it during 1990-2010.4 Anemia is related to perinatal mortality as well as maternal
mortality. A systematic analyses showed that one unit increase in hemoglobin level reduces the
relative risk of perinatal and maternal mortality by 28% and 25%, respectively.
Iron deficiency is responsible for almost 60% of anemia cases in non-malaria regions,
and 50% in malaria regions. Iron deficiency is a more common cause of anemia mainly in low-

3
and middle-income countries.13,14 The proportion of ID among anemia causes varies by regions.
The higher rates have been estimated in Central and South Asia (64.7% and 54.8%) and Latin
America (62.3%) in contrast to North America and Europe, where the proportions of anemia
attributable to iron deficiency are 2.9% and 20-30%, respectively.13 Iron deficiency is
responsible for 591,000 perinatal deaths and 115,000 maternal deaths globally.15,16 The total
global burden of iron deficiency anemia equals to 19.7 million disability-adjusted life years
(DALYs), which is 1.3% of the global total DALYs.14
1.4 Diagnosis
According to WHO, anemia refers to low hemoglobin (Hb) level below the threshold
defined for each population group.1 For the children 6-59 months of age the hemoglobin cut-off
level is 11g/dL (110 g/L). Besides, there is a classification of severity of anemia, according to
which anemia is classified as mild (Hb 100-109g/L), moderate (Hb 70-99g/L) and severe
(Hb<70g/L).17 Considering the existing correlation between hemoglobin level and different
factors, such as age, gender, altitude, smoking, and pregnancy, WHO provided adjustments to
hemoglobin concentration for mentioned factors. For example, in case of altitude, higher altitude
above sea level assumes higher hemoglobin level.17 Hemoglobin level alone is not a measure of
iron deficiency anemia.17 As such, it has low sensitivity and specificity, because there might be
other causes of anemia (Vitamin B12, Vitamin A deficiency, sickle cell disease, etc.). Iron
deficiency anemia is responsible for around 50% of cases of anemia. Thus, the hemoglobin
measurement alone cannot provide realistic estimates for iron-deficiency anemia.18 In addition to
hemoglobin level, iron-deficiency anemia (IDA) evaluation requires complete blood count
(including red blood cell count) and serum iron markers.19,20 World Health Organization
recommends the use of serum ferritin (SF) level as a an indicator of body iron stores depletion.

4
For children under 5 years old iron store depletion corresponds to serum ferritin level below
12ng/ml.21 However, serum ferritin is an acute phase reactant, thus it could be elevated in the
presence of inflammation regardless of iron deficiency. Therefore, to control for false negative
elevation of SF for the diagnosis of iron-deficiency, C-reactive protein (CRP) is also measured,
which is another acute phase reactant. Correspondingly, decreased level of SF is considered to
be caused by iron deficiency when there is no increase in CRP.22 Microcytic erythrocytes (red
blood cells) are also indicators of iron deficiency.20 Their presence can be measured by mean
corpuscular volume (MCV), which reflects the average red blood cell volume.2,7,20 Microcytic
anemia is diagnosed when the mean corpuscular volume of erythrocytes is below the mean
volume of normal cells for the specific age group by 2 standard deviations or more. In
particular, for children from 6 months to 2 years of age, the volume threshold is 75fL, and for 2-
6 years old age group - 70 fL.23,24
1.5 Consequences of Iron Deficiency Anemia
Anemia has serious and considerable effect on human health, as well as on social and
economic development of society.11 Iron is involved in different processes taking place in human
organism, therefore its deficiency may result in a number of consequences for human health,
including physical and mental retardation, behavioral changes, etc.25 Preschool children are the
most vulnerable group regarding anemia, as it has many long-term effects on them.4 Different
epidemiological studies conducted during the last two decades have proved that severe anemia
has negative effect on child’s motor and mental development.26 A population-based study
conducted in Florida, US showed that children suffering from anemia since early childhood have
higher risk of mild or moderate mental retardation as a long-term health effect (after 10 years).26
Iron deficiency anemia affects maturation of central neural system.27 It influences child’s motor

5
activity and cognitive development, as well as school performance.28–30 Infants with iron
deficiency anemia have lower motor development scores compare to non-anemic iron-sufficient
infants.29 Changes in child behavior are among the other health effects of IDA.31,32 A
longitudinal follow-up study revealed that former iron-deficient children had lower arithmetic
achievements and poorer writing skills compared to those without iron-deficiency history.
Moreover, those with ID are found to be more problematic, anxious or depressed, as well as
having social and attention problems.33 Other consequences of iron deficiency anemia are
child’s linear growth retardation,34 poor physical activity,25 as well as low tolerance to infections
due to impaired immune system, mainly cell-mediated immunity.35,36
1.6 Risk Factors
Iron deficiency anemia is the most widespread nutritional disorder in the world,
especially in developing countries.2 Many studies have been conducted on iron-deficiency
anemia in different countries, and many of them have identified the risk factors of iron
deficiency and iron deficiency anemia.
Nutritional iron deficiency occurs when iron intake in the diet does not meet
physiological iron demands of the body.22 Iron stock accumulated in the body of the fetus during
the third trimester of pregnancy is sufficient until 4-6 months of age for term infants.7 Moreover,
exclusive breastfeeding protects the child from IDA during the first four months of life.37
Afterwards, iron stores of the infant get depleted and diet becomes the dominant source of iron
intake.2,22 Low-iron containing or iron-inhibiting diet stands as risk factor for ID and IDA.
Cow’s milk consumption is one of the most well known risk factors of iron deficiency and IDA,
as cow’s milk inhibits iron absorption. Many studies have proven that early introduction and
excessive intake of cow’s milk are statistically significantly related to ID/IDA.22,38–41,42 The

6
presence of red meat and ascorbic acid in the diet increase iron absorption.22 Children who
consumed red meat more than two times per week had lower risk of ID and IDA compared to
those who eat red meat less than two times per week.40,43–46 Other dietary factors, such as
prolonged bottle-feeding38,47, juice, soda, junk food intake, lack of cereals in the diet, etc. are
associated with ID/IDA.40,46,48 Overweight children are more likely to develop ID and IDA
compared to non-overweight children.48,49,41 Other risk factors associated with anemia include
child’s younger age and male sex, low birth weight, maternal anemia during pregnancy50,
family’s low socioeconomic status42,51, family’s food insecurity52, child’s malnutrition53, , blood
lose, hookworm infection2,54, early umbilical cord clamping,55,7 and using inefficient biofuel for
household heating.44,56
1.7 Situation in Armenia
There is very limited information about anemia prevalence and its risk factors in
Armenia. The latest country-wide survey evaluating anemia rates among women and children is
the 2005 Demographic and Health Survey, according to which anemia prevalence among
children aged 6-59 months in Armenia is about 37%.57 This is higher than the prevalence of
anemia among the same age group in 2000 (about 24%).58 The most recent study in Armenia on
anemia among children was conducted in 2015 in a rural region of Talin. Findings of this study
revealed the prevalence of anemia among children up to 5 years old in Talin region to be
32.4%.44 There is no data about iron deficiency anemia for Armenia.
1.8 Rationale for the current study
Anemia is a major public health problem worldwide. Armenia also faces this issue, as
described above. A recent study conducted in Armenia identified risk factors of childhood
anemia.44 However, this study focused on anemia in general (measured by low hemoglobin

7
level) without specifying the type of it. There is no data specifically on iron deficiency anemia
in Armenia. Current study will be the first one in Armenia focusing on risk factors of iron
deficiency anemia.
1.9 Aims of the Study and Research Question
The aim of the study is to identify the risk factors of iron deficiency anemia among
hospitalized children aged 6-59 months in Armenia.
The research questions are the following:
What are the independent risk factors of iron-deficiency anemia among hospitalized
children aged 6-59 months in Armenia.
What are the barriers to access iron-rich food for families of hospitalized children 6-59
months of age in Armenia?
2. Methods
2.1 Study Design
Current study utilized case-control design to address the research question. This study
design is a valuable tool for identifying factors associated with the outcome of interest. This
research method is also convenient by its cost and speed.
2.2 Study Population
The target population were children 6-59 months of age being hospitalized in Arabkir
Joint Medical Center, Muratsan University Hospital, or Hematology Center after Prof. Yeolyan
during the period from 1 January 2015 to 8 April 2016. The first two hospitals are major
pediatric inpatient clinics in Yerevan city, the third center is the major specialized hematological
hospital in Armenia, also located in Yerevan. These hospitals were chosen as the main referral

8
centers for pediatric patients throughout Armenia that could provide the required laboratory data
to identify the study cases.
Cases: Study cases were children 6-59 months of age admitted to the selected hospitals
during the period of 1 January 2015 to 8 April 2016, who were diagnosed with iron deficiency
anemia (IDA). The student investigator identified the cases according to the following
diagnostic criteria: blood hemoglobin level less than 110g/L, mean corpuscular volume of 70fL
or less, serum ferritin level less than 12 ng/mL. IDA diagnosis was confirmed if all the three
criteria were present at the same time.
Controls: The study controls were children of the same age group admitted to Arabkir
Joint Medical Center during the same period without any type of anemia or microcytosis, i.e.
with blood hemoglobin level of 110 g/L or higher and mean corpuscular volume above 70 fL. In
all three hospitals, serum ferritin is usually checked if the child has low hemoglobin level,
therefore the inclusion of this marker for the control selection was not possible.
Arabkir Joint Medical Center was chosen for selecting the study controls mainly due to
feasibility issues, as this center is the only one keeping electronic record forms for each patient,
which contain all the necessary data for control selection, including birth date, main clinical
diagnosis, admission/discharge date, and contact information.
In order to control for the potential bias on the anemia status caused by the main disease
(for which the child was hospitalized), cases and controls were selected from the pool of children
with the same main clinical diagnosis, its stage and severity, except for iron deficiency anemia.
Exclusion criteria: Those caregivers who were not fluent in Armenian were excluded
from the study.

9
2.3 Sample Size
The sample size was calculated using the formula for comparison of proportions between
two groups, with the ratio of cases and controls taken as 1:2 to increase the study power, as the
number of cases was limited in the selected study sites during the targeted period of time. A
recent study conducted in a rural region of Armenia showed that meat consumption during the
last 24 hours was 64.4% among anemic children, and that this variable was an independent risk
factor for anemia.44 Aiming to detect a 15% difference in this variable between cases and
controls with 95% confidence level and a study power of 0.8, the estimated sample size was
calculated to be 345 with 115 cases and 230 controls.
n1 =
(𝑧∝/2 √𝑝𝑞̅̅ ̅̅ (𝜆+1)
𝜆+𝑧𝛽√
𝑝1𝑞1+𝑝2𝑞2𝜆
)
2
∆2 = 𝑛1
(1.96 √0.44∗0.56̅̅ ̅̅ ̅̅ ̅̅ ̅̅ ̅̅ ̅̅ (2+1)
2+0.84√
0.51∗0.49+0.36∗0.64
2)
2
0.152 ≈ 115
n2 = λ * n1 = 115*2 = 230, where λ=2 (2 controls per case)
Total sample size = 230+115 = 345 (2)
2.4 Data Collection
During the first stage of data collection, the student-investigator conducted medical
record review in the three study sites: Arabkir JMC, Muratsan University Hospital and
Hematology center after Prof. Yeolyan, after getting permission from the hospital
administrations.
Case selection in Arabkir JMC and Muratsan UH started from reviewing the laboratory
test results on ferritin level. Those children who were checked for serum ferritin level and met
the inclusion criterion of having ≤12ng/mL ferritin, were further investigated for other inclusion
criteria such as age, blood hemoglobin level and MCV in medical records. In the Hematology

10
Center after Prof. Yeolyan, cases were identified by checking all the medical records completed
during the selected period in order to find eligible participants. Due to preliminary information
about the limited number of cases, a census of children meeting the inclusion criteria was
sampled (for cases).
Afterwards, medical record review of the selected potential cases was conducted in order
to obtain the remaining necessary data (demographic characteristics, main clinical diagnosis,
comorbidities, and laboratory data on each selected child). The clinical data was extracted in the
Medical Record Review Form (Appendix 1), while the identifiable data and contact information
were recorded in the Journal Form (Appendix 2). Overall, 90 cases were identified from the
three study sites.
All the controls were selected from Arabkir JMC. As it was described above, cases and
controls were selected from the pool of children with the same main clinical diagnosis, its stage
and severity, except for iron deficiency anemia. From the electronic database of Arabkir JMC,
the student-investigator identified all the 6-59 months old patients with appropriate main clinical
diagnosis who utilized inpatient or outpatient services of the center within the selected period (1
January 2015 to 8 April 2016). As a result, almost 5000 hospitalized children were identified
and selected from the database. To achieve random selection of controls while giving a
preference to more recently tested children, a random number was chosen between 1-20 (in our
case, the random number was 8) to identify the index child, after which the student-investigator
moved backward from the index child selecting each 8th child from the list of potential controls
after making sure that the selected child meets the inclusion criteria for controls. All the required
information on each selected control was extracted in the Journal and Medical Record Review
forms (Appendices 1 and 2). The process continued till 232 eligible controls were selected.

11
During the second stage of the data collection, telephone interviews were conducted with
the mothers of identified cases and controls. Three attempts were made to contact each mother.
Student-investigator and seven trained interviewers accomplished data collection during the
period of 9 April to 6 May, 2016.
2.5 Study Instrument
The same interviewer-administrated questionnaire (Appendix 3) was applied to mothers
of both cases and controls. The student investigator developed the questionnaire using adapted
items and scales from different studies conducted to identify risk factors of anemia or iron
deficiency anemia among young children.38,43,44,59–61 The questionnaire includes the following
domains: 1. Child’s birth history (including pregnancy), 2. Breastfeeding and feeding during the
first year of life, 3. Child’s current diet (FFQ), 4. Child care and health, 5. Child’s food
security, 6. Mother’s knowledge and counseling received on iron rich/iron absorption inhibiting
diet, 7. Barriers to iron rich food faced by family, and 8. Socioeconomic and demographic
characteristics of mother and family. Before starting the data collection, the questionnaire was
pre-tested among three mothers of 6-59 months old children hospitalized in Arabkir JMC. Based
on these interviews, appropriate changes were made in the final instrument.
2.6 Study Variables
The dependent variable of the study is the presence of iron-deficiency anemia in a child
aged 6-59 months.
Independent variables are potential risk factors of iron deficiency, including child’s
characteristics (age, gender, birth weight and length); family’s socioeconomic and demographic
features (socioeconomic status, parents’ education and employment, household size, number of
children in the family, family’s monthly expenditure); pregnancy-related factors (maternal

12
anemia during pregnancy, mother’s coffee consumption during pregnancy, number of deliveries,
delivery type, child’s birth order); child’s nutrition patterns (breastfeeding initiation and
duration, formula feeding, bottle feeding, frequency of iron rich/inhibiting food consumption per
week); living/environmental conditions (child’s food security, household heating means, day
care center attendance); child health related conditions (diagnosis of hookworm infection, blood
loss, diarrhea during the last year); mother’s knowledge about iron rich/inhibiting food and
whether nutritional counseling on these received; and barriers to iron rich food.
2.7 Analysis
The student investigator did single data entry; afterwards data was cleaned by identifying
outlying values through proportion and frequency checks. Data analysis was conducted using
SPSS 13.0 software.
The samples of cases and controls were compared descriptively in terms of all study
variables. Independent sample’s t-test was used to compare means for continuous variables and
chi-square test to compare proportions for categorical variables. Simple logistic regression
analysis was conducted to assess the relation of each independent variable with the outcome
(IDA status). Afterwards, multiple logistic regression analysis was conducted to assess the
relation of each independent variable with the outcome while controlling for potential
confounders. The best fitting logistic regression model with the outcome of IDA status was
constructed to identify the factors independently associated with the outcome. The model fit was
tested using Hosmer – Lemeshow goodness of fit test.
2.8 Ethical Considerations
The Institutional Review Board (IRB) within the School of Public Health of American
University of Armenia reviewed and approved the study protocol. Data collection started after

13
the approval. Permission was obtained from all selected hospitals in order to conduct medical
record review.
Oral consent form was presented to participants (interviewees) for getting their consent to
participate in the study while informing them about the importance of their contribution, as well
as their rights (Appendix 4). Each participant was given a right to skip any question or stop the
interview at any time. The interviews started after obtaining oral consent from the participants.
All the identifiable information was collected in journal forms and kept separate from the
questionnaires and medical record review forms to avoid disclosure of any information collected
during the study.
3. Results
3.1 Response rate
The research team identified 322 eligible participants during the medical record review stage (90
cases and 232 controls). Approximately one-third (33.9%) of the identified population (109
participants) were not interviewed for different reasons (failure to contact, caregiver unavailable
at the time of data collection, refusal to participate, not fluent in Armenian). Among those
contacted, the response rate was 97.3% for cases and 95.6% for controls. As a result, 213
mothers of eligible children were interviewed, of which 71 were cases and 142 controls. With
this sample size, the study power for identifying 15% difference in proportions of independent
variables was calculated as 0.65.

14
3.2 Descriptive statistics
About 25.3% of the cases (n=18) were from Arabkir Joint Medical Center, 16.9% (n=12)
from Muratsan University Hospital, and the rest (n=41) from Hematology Center after Prof.
Yeolyan. All 142 controls were from Arabkir JMC.
The mean blood hemoglobin level was 85.45 g/L among cases and 126.78 g/L among
controls. In the group of cases, the proportion of children with mild anemia was 26.8%,
moderate 50.7%, and severe 22.5%.
The mean age of children was 14.4 months (SD 9.6 ) for the cases and 36.2 months
(SD14.8) for the controls with statistically significant difference between the two groups
(p<0.001). There were more males among cases compared to controls (64.8% vs. 48.6%,
p=0.025). Table 1 presents descriptive statistics for all independent variables. Statistically
significant difference was detected between cases and controls regarding birth weight and length,
with the cases having lower birth weight and length than controls. Maternal anemia and coffee
consumption during pregnancy were more frequently reported among cases than controls. The
proportion of children born with cesarean section and with higher birth order were higher among
cases compared to controls. Higher proportion of cases than controls reported current bottle-
feeding, frequent consumption of cow’s milk and tea/coffee in a weekly diet. Early initiation of
breastfeeding, mean weekly frequency of consuming meat, legumes, nuts, dairy products,
vegetables, fruits, sweets, and bread were higher among controls than the cases. Compared to
mothers of controls, mothers of cases reported more frequently having anemia among family
members, experiencing child food insecurity, having lower socioeconomic status, using biofuel
for heating, facing food cost as a barrier to iron rich food, and having more difficulty with
feeding the child with iron-rich food.

15
3.3 Simple Logistic Regression
Table 2 shows the results of univariate analysis between child’s IDA status and each
independent variable. The estimated crude OR between child’s age and IDA status was 0.87
(95% CI: 0.84-0.91; p<0.001). Child’s lower birth weight and height were associated with IDA
status (OR=0.99, 95% CI: 0.99-0.99; p<0.001, and OR=0.925, 95% CI: 0.86-0.99; p=0.030,
respectively). Unadjusted OR for cesarean section was 2.44 (95% CI: 1.34-4.44; p=0.003), and
for child’s higher birth order 1.56 (95% CI: 1.04-2.34; p<0.001) indicating the possibility for
both being risk factors for IDA. Lower weekly consumption of meat, legumes, nuts, citrus fruits,
sweets, and bread (measured in times per week) were also significantly associated with IDA.
Consuming more cow’s milk per day (measured in cups) was associated with higher odds of
having IDA with crude OR of 1.29 (95% CI: 1.02-1.62; p=0.030). Higher food diversity score
was associated with lower risk of childhood IDA with crud OR of 0.61 (95% CI: 0.51-.72;
p<0.001). Presence of anemia among family members (OR=3.39; 95% CI: 1.63-7.04; p=0.001)
and child’s previous history of anemia (OR=2.11; 95% CI: 0.98-4.56; p=0.058) were both
significantly associated with child’s IDA status. Food cost and food availability as barriers to
use iron rich food had positive association with the likelihood of having IDA (OR=2.76, 95% CI:
1.51-5.05; p=0.001, and OR=2.26; 95% CI: 1.13-4.52; p=0.021, respectively). Child’s family’s
socioeconomic status score was associated with lower risk for a child to have IDA with crude
OR of 0.83 (95% CI: 0.71-0.98; p=0.023). Household heating with biofuel was associated with
higher odds (OR=2.74, 95% CI: 1.46-5.17; p=0.002) for a child to have IDA. The following
factors were also significantly associated with the IDA status of a child in the univariate analysis:
maternal coffee consumption during pregnancy, lower gestational age, long duration of
predominant breastfeeding, presence of cow’s milk and tea/coffee in child’s diet, child’s

16
previous history of hookworm infection, child’s lower food security, and parents’ lower
educational level.
3.4 Multiple Logistic Regression
As age is a confounder in the association between IDA and other risk factors according to
the literature,62 and since the mean age of the cases and controls in this sample were significantly
different, the next step in our analysis was calculating age-adjusted associations between the IDA
status and the dependent variables of interest (Table 2). When controlling for child’s age, birth
weight and birth length were both associated with less chance for a child to have IDA
(OR=0.998; 95% CI: 0.998-0.999; p<0.001 and OR=0.91; (95% CI: 0.83-0.99; p=0.035,
respectively). The age-adjusted OR for the association between cesarean section and IDA status
was 2.25 (95% CI: 1.01-4.97; p=0.048), indicating higher chance of being anemic among those
children born with cesarean section. From weekly dietary items, more frequent consumption of
meat (OR=0.79, 95% CI: 0.67-0.94; p=0.006) and sweets (OR=0.81, 95% CI: 0.70-0.93;
p=0.003) were associated with lower likelihood of IDA, while consuming more cow’s milk per
day was associated with higher risk of IDA (OR=1.38, 95% CI: 1.03-1.86; p=0.032). Higher
food diversity score was still associated with lower risk of having IDA (OR=0.69, 95% CI: 0.56-
0.86; p=0.001), while household heating with biofuel (OR=2.17, 95% CI: 0.92-5.15; p=0.078)
and SES-score (OR=0.89, 95% CI: 0.72-1.09; p=0.252) lost their significance after adjusting for
child’s age. As for barriers to iron rich food, food cost and availability were no longer
significantly associated with the likelihood of IDA in age-adjusted analysis.
All the variables that were statistically significant after adjusting for age, as well as some
other potential risk factors supported by literature were further tested in the multivariate analysis
to find independent risk factors of IDA among selected sample. For this purpose, the research

17
team developed best fitting final model for IDA status. In this process, all the variables that were
not statistically significant after controlling for other variables in the model were excluded. As a
result, the final model included the following set of independent factors: child’s age (OR=0.89,
95% CI: 0.85-0.93; p<0.001), birth weight (OR=0.99, 95% CI: 0.997-0.999; p<0.001), consumed
amount of cow’s milk per day in cups (OR=1.51, 95% CI: 1.04-2.19; p=0.030), weekly
frequency of consuming sweets (OR=0.78, 95% CI: 0.65-0.93; p=0.006), food diversity score
(OR=0.76, 95% CI: 0.58-0.98; p=0.034), and previous history of anemia (OR=3.43, 95% CI:
1.04-11.27; p=0.043). The final model reached very good model fit indices (Table 3).
According to it, each month increase in child’s age was associated with 11% lower chance for
him to have IDA, each one gram increase in child’s birth weight was associated with 0.2% lower
odds of having IDA, one point higher food diversity score decreased the odds of having iron
deficiency anemia by 24%, each additional cup of cow’s milk consumed daily was associated
with 1.5 times higher odds of having iron deficiency anemia, while an additional day in a week
when sweets were consumed was associated with 22% lower odds of having IDA. Also, having
previous history of anemia produced 3.4 times higher odds of having current IDA among the
study population.
4. Discussion
4.1 Strengths of the study
To our knowledge, this is the first study conducted in Armenia specifically investigating
iron deficiency anemia risk factors among 6-59 months old children, with the iron-deficiency
anemia status confirmed with a combination of three indicators – levels of serum ferritin, blood
hemoglobin, and mean corpuscular volume of erythrocytes.

18
Another strength was that the study did not rely on the diagnoses of children in the
medical records to identify their case/control status. Instead, the student investigator applied
specific diagnostic criteria to make the selection, which assured a uniform diagnostic approach to
all the study participants.
The controls were selected from the same pool of hospitalized children to reduce the
selection bias. From the list of potential controls, the study participants were selected in a
random manner while giving a preference to more recently hospitalized children to reduce the
recall bias among them.
To avoid the potential bias from having more “anemia of inflammation” among cases
(low hemoglobin level in presence of infection or other inflammatory process in the body)63 than
among controls, for the cases with the main clinical diagnosis other than IDA, the student
investigator chose a proportionate number of controls with the same main diagnosis in the same
stage and severity.
4.2 Study Limitations
One of the limitations of this study is its limited generalizability, as it selected cases
among hospitalized children, not among general population. Also, the study included only three
hospitals in Yerevan, and all the controls were selected from one hospital. However, all three
hospitals are referral centers serving children throughout the country.
In our study, controls were not checked for serum ferritin level to confirm the lack of
initial stages of iron deficiency. Although the mean corpuscular volume was checked among
them to control for microcytosis, which is mainly caused by iron deficiency,23 children in the
control group could still be iron deficient without anemia, which could lead to misclassification
bias. However, as this bias is unidirectional (only controls could be iron-deficient, cases cannot

19
be iron-sufficient), this could introduce an effect of making the identified associations weaker in
our study, than they could have been in the reality.
The other limitation of the current study is the possibility of recall bias due to long
interval between hospitalization and the interview (maximum 1 year and 3 months).64 Questions
asked to mothers (on diet, health related conditions) were mainly related to the period before the
hospitalization, and the items on child feeding practices during the first year of life were related
to even earlier period. In order to minimize the recall bias at least for controls, we had chosen
more recent patients applied to the hospital.
During the data collection, we faced with limited number of cases. Hence, we could not
achieve the estimated sample size for the cases. For the actual sample size, the study power was
0.65, meaning that some associations could be statistically insignificant due to small sample size.
4.3 Main Findings
The prior studies and surveys conducted in Armenia where designed to identify the
prevalence and risk factors of anemia in general, by only measuring blood hemoglobin
level.44,57,58 As there was no data about iron deficiency anemia in the country, the current study
aimed to reveal independent risk factors of iron deficiency anemia among hospitalized children
aged 6-59 months in Armenia, as well as to find the barriers for accessing iron rich food among
families of those children.
The finding of this study on younger age being a risk factor of IDA in children is
consistent with the existing literature.65–73 In a number of studies, 6-24 months old children have
shown to be at higher risk of having IDA.53,74 This could be explained by continuing rapid
growth and high iron demand for brain growth and maturation in the period when breast milk or
iron-fortified infant formula is replaced by non-fortified table food and even by cow’s milk. In

20
addition, child’s likes or dislikes make their feeding more difficult during this transition period.
Overall, these factors put younger children under higher risk of iron deficiency, and
consequently iron deficiency anemia.74,75
In this study, we were able to find an association between cow’s milk consumption and
iron deficiency anemia for children 6-59 months of age. The time of introduction of cow’s milk
into child’s diet was not significantly associated with IDA. However, our study detected
significant association between daily-consumed amount of cow’s milk in cups and iron
deficiency anemia. This result is consistent with the literature, as in many studies conducted in
different countries cow’s milk consumption was significant risk factor for IDA among children.
In a British study conducted among 1.5-4.5 years old children, those who consumed more than
400g milk and milk products daily, were less likely to have iron-rich products (meat, fish, fruit,
nuts) in their diet, which subsequently lead to iron deficiency and later to IDA.66 The positive
relationship between cow’s milk consumption and iron deficiency anemia could be explained by
several mechanisms. First, cow’s milk itself is a poor source of iron.76 Second, it contains
calcium and protein called casein, both of which have inhibitory effect on iron absorption and
bioavailability.77–82 Finally, cow’s milk may cause intestinal blood loss, which in turn leads to
iron loss and anemia.83 According to recommendations of American Academy of Pediatrics,
cow’s milk should not be introduced before the age of 12 months. When introduced, the amount
of cow’s milk should not exceed two cups (400-500ml) per day.84
Our study findings demonstrated that child’s low birth weight is a risk factor of childhood
IDA. This finding is strongly supported by literature, as many studies have shown significant
association between low birth weight and iron deficiency anemia.39,42,47,48,85 Children with low
birth weight have insufficient iron stores, hence, their iron requirement is higher to maintain

21
appropriate growth during the first months of life. This explains the potential relationship
between low birth weight and IDA.5,7,86,87 Furthermore, in many studies iron supplementation of
low birth weight infants has been shown as an effective way to prevent further iron deficiency
and IDA.88–90
One of the findings of the current study is the association between food diversity score
and IDA, such that more diverse diet protects a child from IDA. Several studies found a relation
between diverse diet and micronutrient, especially, iron intake, which was reflected in the
increased level of serum ferritin.62,91–95 Possibly, diverse diet includes iron rich foods as well as
products that increase iron bioavailability, which in turn prevents iron deficiency and IDA. The
recent study conducted among under-five children in Armenia (Talin region) also found that
higher food diversity score was protective against anemia.44
According to our study findings, previous history of anemia stands as an independent risk
factor of current iron deficiency anemia. There are some studies indicating that the past history
of anemia is associated with anemia in children without specifying the type of it.96 However,
larger number of studies report lack of such association.97,98 A case-control study conducted
among women showed significant association between their past history of IDA and current IDA
status.99 In this study, we did not ask about the type of anemia in the past.
A contradicting finding of this study was that the higher frequency of consuming sweets
per week was a protective factor from IDA. We could not find relevant studies that showed a
negative (protective) association between sweet consumption and IDA. However, there are
scientific papers on sugar’s effect in increasing iron bioavailability, which somehow could stand
as an explanation to our finding.100,101 In opposite, many studies on IDA risk factors either did

22
not find any association between sweet consumption and IDA status, or have found positive
association between those two.66,102
This study was unable to find significant associations between the studied barriers to iron
rich food (food availability, cost, family’s socio-economic status, etc.) and IDA. The lower-
than-targeted power of the study or low diversity of the studied sample in terms of families’
socio-economic status could possibly be the underlying factors for this lack of association.
5. Recommendations
Based on our findings, younger children are at higher risk of IDA, thus preventive
interventions should target those children. Infants with low birth weight are also vulnerable
regarding ID and IDA. Nutritional counseling should be given to mothers of low birth weight
infants, in order to ensure that their diet contains sufficient iron to prevent IDA. Prematurity of
the infant is associated with low birth weight. American Academy of Pediatrics recommends to
give iron supplements to preterm infants starting from four months of age.7 In addition to these
points, there is also a need for making dietary recommendations to the caregivers of young
children, mainly focusing on discouraging cow’s milk consumption and ensuring food diversity,
so that child’s diet includes all the main food groups with appropriate frequency.
Further research is recommended to identify the prevalence of IDA among children in
Armenia. The finding on the negative association between sweet consumption and IDA also
needs further investigation.

23
6. Conclusion
Current study identified the determinants of IDA among hospitalized children 6-59
months of age in Armenia. According to our findings, child’s younger age, lower birth weight,
previous history of anemia, low food diversity, and higher daily consumption of cow’s milk
where independently associated with IDA. High weekly frequency of sweets and sugary
products was found to be protective factor from IDA.
This was the first study investigating the determinants of iron deficiency anemia among
children 6-59 months in Armenia. It resulted in findings that are consistent with the literature,
and in ideas for future research in this field.

24
References
1. WHO, CDC. Assessing the Iron Status of Populations. Geneva; 2007.
2. Kliegman RM, Stanton BF, Schor NF, Geme JWS. Nelson Textbook of Pediatrics. 20th
ed. Philadelpia, PA: Elsevieer; 2016.
3. McLean E, Cogswell M, Egli I, Wojdyla D, de Benoist B. Worldwide prevalence of
anaemia, WHO Vitamin and Mineral Nutrition Information System, 1993–2005. Public
Health Nutr. 2009;12(04):444. doi:10.1017/S1368980008002401.
4. Kassebaum NJ, Jasrasaria R, Naghavi M, et al. A systematic analysis of global anemia
burden from 1990 to 2010. Blood. 2014; 123(5):615-625. doi:10.1182/blood-2013-06-
508325.
5. Balarajan Y, Ramakrishnan U, Özaltin E, Shankar AH, Subramanian S. Anaemia in low-
income and middle-income countries. Lancet. 2011;378(9809):2123-2135.
doi:10.1016/S0140-6736(10)62304-5.
6. Longo DL, Camaschella C. Iron-Deficiency Anemia. N Engl J Med. 2015;372(19):1832-
1843. doi:10.1056/NEJMra1401038.
7. Baker RD, Greer FR, The Committee on Nutrition. Diagnosis and Prevention of Iron
Deficiency and Iron-Deficiency Anemia in Infants and Young Children (0 – 3 Years of
Age). Pediatrics. 2010;125(5):1040-1050. doi:10.1542/peds.2010-2576.
8. Hentze MW, Muckenthaler MU, Galy B, Camaschella C. Two to Tango: Regulation of
Mammalian Iron Metabolism. Cell. 2010;142(1):24-38. doi:10.1016/j.cell.2010.06.028.
9. Schechter AN. Hemoglobin research and the origins of molecular medicine. Blood.
2008;112(10):3927-3938. doi:10.1182/blood-2008-04-078188.
10. Pasricha S, Drakesmith H, Black J, Hipgrave D, Biggs B. Control of iron deficiency
anemia in low- and middle-income countries. 2015;121(14):1-3. doi:10.1182/blood-2012-
09-453522.
11. WHO. Worldwide prevalence of anaemia. WHO Rep. 2005:51.
doi:10.1017/S1368980008002401.
12. Stevens GA, Finucane MM, De-Regil LM, et al. Global, regional, and national trends in
haemoglobin concentration and prevalence of total and severe anaemia in children and
pregnant and non-pregnant women for 1995–2011: a systematic analysis of population-
representative data. Lancet Glob Heal. 2013;1(1):e16-e25. doi:10.1016/S2214-
109X(13)70001-9.
13. World Health Organization. The Global Burden of Disease: 2004 update. Geneva; 2008.
14. World Health Organization. Global Health Risks: Mortality and burden of disease
attributable to selected major risks. Geneva; 2009.
15. World Health Organization. Comparative Quantification of Health Risks. Global and
Regional Burden of Disease Attributable to Selected Major Risk Factors. Geneva; 2004.
16. Scott S, Chen-Edinboro L, Caulfield L, Murray-Kolb L. The Impact of Anemia on Child
Mortality: An Updated Review. Nutrients. 2014;6(12):5915-5932.

25
doi:10.3390/nu6125915.
17. WHO. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of
Severity. Geneva; 2011. doi:WHO/NMH/NHD/MNM/11.1.
18. White KC. Anemia is a poor predictor of iron deficiency among toddlers in the United
States: for heme the bell tolls. Pediatrics. 2005;115(2):315-320. doi:10.1542/peds.2004-
1488.
19. Mei Z, Cogswell ME, Parvanta I, et al. Hemoglobin and ferritin are currently the most
efficient indicators of population response to iron interventions: an analysis of nine
randomized controlled trials. J Nutr. 2005;135(8):1974-1980.
20. Johnson-Wimbley TD, Graham DY. Diagnosis and management of iron deficiency
anemia in the 21st century. Therap Adv Gastroenterol. 2011;4(3):177-184.
doi:10.1177/1756283X11398736.
21. WHO. Serum ferritin concentrations for the assessment of iron status and iron deficiency
in populations. Vitamin and Mineral Nutrition Information System. WHO. 2011:1-5.
doi:(WHO/NMH/NHD/MNM/11.2).
22. Zimmermann MB, Hurrell RF. Nutritional iron deficiency. Lancet. 2007;370(9586):511-
520. doi:10.1016/S0140-6736(07)61235-5.
23. Richardson M. Microcytic anemia. Pediatr Rev. 2007;28(1):5-14. doi:10.1542/pir.28-1-5.
24. Janus J, Moerschel SK. Evaluation of anemia in children. Am Fam Physician.
2010;81(12):1462-1471.
25. Beard J. Iron Biology in Immune Function, Muscle Metabolism and Neuronal
Functioning. J Nutr. 2001;131(2):568S-580S.
26. Hurtado EK, Claussen AH, Scott KG. Early Childhood Anemia and Mild or Moderate
Mental Retardation. Am J Clin Nutr. 1999;69(1):115-119.
27. Ayala R, Otero GA, Porcayo Mercado R, Pliego-Rivero FB. Delayed CNS Maturation in
Iron-Deficient Anaemic Infants. Nutr Neurosci. 2008;11(2):61-68.
doi:10.1179/147683008X301342.
28. Shafir T, Angulo-Barroso R, Su J, Jacobson SW, Lozoff B. Iron Deficiency Anemia in
Infancy and Reach and Grasp Development. Infant Behav Dev. 2009;32(4):366-375.
doi:10.1016/j.infbeh.2009.06.002.
29. Shafir T, Angulo-Barroso R, Angelilli ML, Jing Y, Jacobson SW, Lozoff B. Iron
Deficiency and Infant Motor Development. Early Hum Dev. 2008;84(7):479-485.
doi:10.1016/j.earlhumdev.2007.12.009.
30. Grantham-Mcgregor S, Ani C. A Review of Studies on the Effect of Iron Deficiency on
Cognitive Development in Children. J Nutr. 2001;131(2):649S-668S.
31. McCann JC, Ames BN. An overview of evidence for a causal relation between iron
deficiency during development and deficits in cognitive or behavioral function. Am J Clin
Nutr. 2007;85(4):931-945.

26
32. Lozoff B, Corapci F, Burden MJ, et al. Preschool-Aged Children with Iron Deficiency
Anemia Show Altered Affect and Behavior. J Nutr. 2007;137(3):683-689.
33. Lozoff B, Jimenez E, Hagen J, Mollen E, Wolf AW. Poorer behavioral and
developmental outcome more than 10 years after treatment for iron deficiency in infancy.
Pediatrics. 2000;105(4):E51.
34. Kumar T, Taneja S, Yajnik CS, Bhandari N, Strand TA. Prevalence and predictors of
anemia in a population of North Indian children. Nutrition. 2014;30(5):531-537.
doi:10.1016/j.nut.2013.09.015.
35. Oppenheimer S. Iron and Its Relation to Immunity and Infectious Disease. J Nutr.
2001;131(2):616S-635S.
36. Sadeghian M, Keramati M, Ayatollahi H, Manavifar L, Enaiati H, Mahmoudi M. Serum
Immunoglobulins in Patients with Iron Deficiency Anemia. Indian J Hematol Blood
Transfus. 2010;26(2):45-48. doi:10.1007/s12288-010-0025-3.
37. Marques RFSV, Taddei JAAC, Lopez FA, Braga JAP. Breastfeeding exclusively and iron
deficiency anemia during the first 6 months of age. Rev Assoc Med Bras. 2014;60(1):18-
22. doi:10.1590/1806-9282.60.01.006.
38. Parkin PC, DeGroot J, Maguire JL, Birken CS, Zlotkin S. Severe iron-deficiency anaemia
and feeding practices in young children. Public Health Nutr. 2016;19(4):716-722.
doi:10.1017/S1368980015001639.
39. Uijterschout L, Vloemans J, Vos R, et al. Prevalence and Risk Factors of Iron Deficiency
in Healthy Young Children in the Southwestern Region of the Netherlands. J Pediatr
Gastroenterol Nutr. 2014;58(2):193-198. doi:10.1097/MPG.0000000000000216.
40. Christofides A, Schauer C, Zlotkin SH. Iron Deficiency and Anemia Prevalence and
Associated Etiologic Risk Factors in First Nations and Inuit Communities in Northern
Ontario. Can J Public Health. 2016;96(4):304-307. doi:10.17269/cjph.96.630.
41. Ferrara M, Bertocco F, Ricciardi A, Ferrara D, Incarnato L, Capozzi L. Iron deficiency
screening in the first three years of life: A three-decade-long retrospective case study.
Hematology. 2014;19(4):239-243. doi:10.1179/1607845413Y.0000000124.
42. Male C, Persson LA, Freeman V, Guerra A, van’t Hof MA, Haschke F. Prevalence of
iron deficiency in 12-mo-old infants from 11 European areas and influence of dietary
factors on iron status (Euro-Growth study). Acta Paediatr. 2001;90(5):492-498.
43. Bogen DL, Duggan AK, Dover GJ, Wilson MH. Screening for Iron Deficiency Anemia by
Dietary History in a High-Risk Population. Pediatrics. 2000;105(6):1254-1259. doi:
10.1542/peds.105.6.1254
44. Demirchyan A, Petrosyan V, Sargsyan V, Hekimian K. Prevalence and Determinants of
Anemia among Children Aged 0-59 Months in a Rural Region of Armenia: A Case-
Control Study. Public Health Nutr. 2015:1-10. doi: 10.1017/S1368980015002451.
45. Moshe G, Amitai Y, Korchia G, et al. Anemia and Iron Deficiency in Children:
Association With Red Meat and Poultry Consumption. J Pediatr Gastroenterol Nutr.
2013;57(6):722-727. doi:10.1097/MPG.0b013e3182a80c42.

27
46. Boutry M, Needlman R. Use of Diet History in the Screening of Iron Deficiency.
Pediatrics. 1996;98(6):1138-1142.
47. Brotanek JM, Halterman JS, Auinger P, Flores G, Weitzman M. Iron deficiency,
prolonged bottle-feeding, and racial/ethnic disparities in young children. Arch Pediatr
Adolesc Med. 2005;159(11):1038-1042. doi:10.1001/archpedi.159.11.1038.
48. Brotanek JM, Gosz J, Weitzman M, Flores G. Iron deficiency in early childhood in the
United States: risk factors and racial/ethnic disparities. Pediatrics. 2007;120(3):568-575.
doi:10.1542/peds.2007-0572.
49. Nead KG, Halterman JS, Kaczorowski JM, Auinger P, Weitzman M. Overweight Children
and Adolescents: A Risk Group for Iron Deficiency. Pediatrics. 2010;114(1):104-108.
doi: 10.1542/peds.114.1.104
50. Wang J, Wang H, Chang S, Zhao L, Fu P, Yu W. The Influence of Malnutrition and
Micronutrient Status on Anemic Risk in Children under 3 Years Old in Poor Areas in
China. PLoS One. 2015:1-13. doi:10.1371/journal.pone.0140840.
51. Leite MS, Cardoso AM, Ea C, et al. Prevalence of anemia and associated factors among
indigenous children in Brazil: results from the First National Survey of Indigenous
People’s Health and Nutrition. Nutr J. 2013;12(1):69:1-11. doi:10.1186/1475-2891-12-69.
52. Skalicky A, Meyers AF, Adams WG, Yang Z, Cook JT, Frank DA. Child food insecurity
and iron deficiency anemia in low-income infants and toddlers in the United States.
Matern Child Health J. 2006;10(2):177-185. doi:10.1007/s10995-005-0036-0.
53. Adish AA, Esrey SA, Gyorkos TW, Johns T. Risk factors for iron deficiency anaemia in
preschool children in northern Ethiopia. Public Health Nutr. 1999;2(3):243-252.
54. Helena F, Zanin C, Adalton C, et al. Determinants of Iron Deficiency Anemia in a Cohort
of Children Aged 6-71 Months Living in the Northeast of Minas Gerais, Brazil. PLoS
One. 2015:1-14. doi:10.1371/journal.pone.0139555.
55. Andersson O, Domellof M, Andersson D, Hellstrom-Westas. Effect of Delayed vs Early
Umbilical Cord Clamping on Iron Status and Neurodevelopment at Age 12 Months. A
Randomized Clinical Trial. JAMA Pediatr. 2014;168(6):547-554.
doi:10.1001/jamapediatrics.2013.4639.
56. Mishra V, Retherford RD. Does biofuel smoke contribute to anaemia and stunting in
early childhood? Int J Epidemiol. 2007;36(1):117-129. doi:10.1093/ije/dyl234.
57. National Statistical Service of Republic of Armenia, Ministry of Health of Armenia, ORC
Macro Calverton. Armenia Demographic and Health Survey. Yerevan; 2005.
58. National Statistical Service of the Republic of Armenia, Ministry of Health of Armenia,
ORC Macro Calverton. Armenia Demographic and Health Survey. Yerevan; 2000.
59. Huybrechts I, De Backer G, De Bacquer D, Maes L, De Henauw S. Relative validity and
reproducibility of a food-frequency questionnaire for estimating food intakes Among
flemish preschoolers. Int J Environ Res Public Health. 2009;6(1):382-399.
doi:10.3390/ijerph6010382.

28
60. Walton J. National Pre-School Nutrition Survey. Summary Report on: Food and Nutrient
Intakes, Physical Measurements and Healthy Eating. Dublin; 2012.
http://www.iuna.net/wp-
content/uploads/2012/06/Summary_Report_National_PreSchool_Nutrition_Survey_June_
2012.pdf.
61. United States Department of Agriculture. U.S. Household Food Security Survey Module:
Three-Stage Design, With Screeners. 2012.
http://www.ers.usda.gov/datafiles/Food_Security_in_the_United_States/Food_Security_S
urvey_Modules/hh2012.pdf.
62. Siegel EH, Stoltzfus RJ, Khatry SK, Leclerq SC, Katz J, Tielsch JM. Epidemiology of
anemia among 4- to 17-month-old children living in south central Nepal. Eur J Clin Nutr.
2006;60(2):228-235.
63. Roy CN. Anemia of inflammation. Hematology Am Soc Hematol Educ Program.
2010;2010(1):276-280. doi: 10.1182/asheducation-2010.1.276.
64. Armenian HK. The Case-Control Method. Design and Application. New York: Oxford
University Press; 2009.
65. Schneider JM, Fujii ML, Lamp CL, Lönnerdal B, Dewey KG, Zidenberg-cherr S. The use
of multiple logistic regression to identify risk factors associated with anemia and iron
deficiency in a convenience sample of 12 – 36-mo-old children from low-income families.
Am J Clin Nutr. 2008;87(1):614-620.
66. Thane CW, Walmsley CM, Bates CJ, Prentice A, Cole TJ. Risk factors for poor iron status
in British toddlers: further analysis of data from the National Diet and Nutrition Survey of
children aged 1.5-4.5 years. Public Health Nutr. 2000;3(4):433-440.
67. Soh P, Ferguson EL, McKenzie JE, Homs MYV, Gibson RS. Iron deficiency and risk
factors for lower iron stores in 6-24-month-old New Zealanders. Eur J Clin Nutr.
2004;58(1):71-79. doi:10.1038/sj.ejcn.1601751.
68. Lisbôa MBM de C, Oliveira EO, Lamounier JA, Silva CAM, Freitas RN. Prevalence of
iron-deficiency anemia in children aged less than 60 months: A population-based study
from the state of Minas Gerais, Brazil. Rev Nutr. 2015;28(2):121-131. doi:10.1590/1415-
52732015000200001.
69. Alvarez-Uria G, Naik PK, Midde M, Yalla PS, Pakam R. Prevalence and severity of
anaemia stratified by age and gender in rural India. Anemia. 2014;2014:1-6.
doi:10.1155/2014/176182.
70. Woldie H, Kebede Y, Tariku A. Factors Associated with Anemia among Children Aged 6-
23 Months Attending Growth Monitoring at Tsitsika Health Center, Wag-Himra Zone,
Northeast Ethiopia. J Nutr Metab. 2015;2015. doi:10.1155/2015/928632.
71. Bortolini GA, Vitolo MR. Relationship between iron deficiency and anemia in children
younger than 4 years. J Pediatr (Rio J). 2010;86(6):488-492. doi:10.2223/JPED.2039.
72. Zhao A, Zhang Y, Peng Y, et al. Prevalence of anemia and its risk factors among children
6-36 months Old in Burma. Am J Trop Med Hyg. 2012;87(2):306-311.

29
doi:10.4269/ajtmh.2012.11-0660.
73. Gompakis N, Economou M, Tsantali C, Kouloulias V, Keramida M, Athanasiou-Metaxa
M. The effect of dietary habits and socioeconomic status on the prevalence of iron
deficiency in children of northern Greece. Acta Haematol. 2007;117(4):200-204.
doi:10.1159/000098273.
74. Paoletti G, Bogen DL, Ritchey AK. Severe Iron-Deficiency Anemia Still an Issue in
Toddlers. Clin Pediatr (Phila). 2014;53:1352-1358. doi:10.1177/0009922814540990.
75. Eden A, Mir M. Iron deficiency in 1- to 3-year-old children. A pediatric failure? Arch
Pediatr Adolesc Med. 1997;151(10):986-988.
76. Agostoni C, Turck D. Is Cows’ Milk Harmful for a Childʼs Health? J Pediatr
Gastroenterol Nutr. 2011;53(6):594-600. doi:10.1097/MPG.0b013e318235b23e.
77. Hallberg L, Rossander-Hultén L, Brune M, Gleerup A. Bioavailability in man of iron in
human milk and cow’s milk in relation to their calcium contents. Pediatr Res.
1992;31(5):524-527. doi:10.1203/00006450-199205000-00024.
78. Saarinen UM, Siimes M. Iron Absorption from Breast Milk, Cow’s Milk, and Iron-
supplemented Formula: An Opportunistic Use of Changes in Total Body Iron Determined
by Hemoglobin, Ferritin, and Body Weight in 132 Infants. Pediatr Res. 1979;13(3):143-
147. doi:10.1203/00006450-197903000-00001.
79. Roughead ZK, Zito CA, Hunt JR. Inhibitory effects of dietary calcium on the initial
uptake and subsequent retention of heme and nonheme iron in humans: Comparisons
using an intestinal lavage method. Am J Clin Nutr. 2005;82(3):589-597.
80. Hallberg L, Hulthén L. Prediction of dietary iron absorption an algorithm for calculating
absorption and bioavailability. Am J Clin Nutr. 2000;71(5):1147-1160.
81. Domellöf M. Iron requirements, absorption and metabolism in infancy and childhood.
Curr Opin Clin Nutr Metab Care. 2007;10(3):329-335.
doi:10.1097/MCO.0b013e3280523aaf.
82. Ziegler EE. Consumption of cow’s milk as a cause of iron deficiency in infants and
toddlers. Nutr Rev. 2011;69(1):S37-S42. doi:10.1111/j.1753-4887.2011.00431.x.
83. Jiang T, Jeter JM, Nelson SE, Ziegler EE. Intestinal blood loss during cow milk feeding in
older infants: quantitative measurements. Arch Pediatr Adolesc Med. 2000;154(7):673-
678. doi:10.1001/archpedi.154.7.673.
84. Maguire JL, Lebovic G, Kandasamy S, et al. The relationship between cow’s milk and
stores of vitamin D and iron in early childhood. Pediatrics. 2013;131(1):e144-e151.
doi:10.1542/peds.2012-1793.
85. Lozoff B, Kaciroti N, Walter T. Iron deficiency in infancy: Applying a physiologic
framework for prediction. Am J Clin Nutr. 2006;84(6):1412-1421.
86. Domellof M. Iron and other micronutrient deficiencies in low-birthweight infants. Nestle
Nutr Inst Workshop Ser. 2013;74:197-206. doi:10.1159/000348772.
87. Chaparro CM. Setting the Stage for Child Health and Development: Prevention of Iron

30
Deficiency in Early Infancy. J Nutr. 2008;138(12):2529-2533.
88. Berglund S, Westrup B, Domellof M. Iron supplements reduce the risk of iron deficiency
anemia in marginally low birth weight infants. Pediatrics. 2010;126(4):e874-e883.
doi:10.1542/peds.2009-3624.
89. Jin H-X, Wang R-S, Chen S-J, Wang A-P, Liu X-Y. Early and late Iron supplementation
for low birth weight infants: a meta-analysis. Ital J Pediatr. 2015;41:16.
doi:10.1186/s13052-015-0121-y.
90. Long H, Yi JM, Hu PL, et al. Benefits of iron supplementation for low birth weight
infants: a systematic review. BMC Pediatr. 2012;12:99. doi:10.1186/1471-2431-12-99.
91. Nti CA. Dietary Diversity is Associated with Nutrient Intakes and Nutritional Status of
Children in Ghana. Asian J Med Sci. 2011;2(2):105-109. doi:10.3126/ajms.v2i2.4179.
92. Rani V, Arends DE, Brouwer ID. Dietary diversity as an indicator of micronutrient
adequacy of the diet of five to eight year old Indian rural children. Nutr Food Sci.
2010;40(5):466-476. doi:10.1108/00346651011076974.
93. Acham H, Tumuhimbise GA, Kikafunda JK. Simple Food Group Diversity as a Proxy
Indicator for Iron and Vitamin A Status of Rural Primary School Children in Uganda.
Food Nutr Sci. 2013;4(12):1271-1280. doi: 10.4236/fns.2013.412163.
94. Demment MW, Young MM, Sensenig RL. Providing Micronutrients through Food-Based
Solutions: A Key to Human and National Development. J Nutr. 2003;133(5):3879S-
3885S.
95. Kennedy GL, Pedro MR, Seghieri C, Nantel G, Brouwer I. Dietary diversity score is a
useful indicator of micronutrient intake in non-breast-feeding Filipino children. J Nutr.
2007;137(2):472-477.
96. Cotta RMM, Oliveira F de CC, Magalhaes KA, et al. Social and biological determinants
of iron deficiency anemia. Cad Saude Publica. 2011;27(2):S309-S320.
doi:10.1590/S0102-311X2011001400017
97. Rocha DDS, Capanema FD, Netto MP, Franceschini SCC, Lamounier JA. Prevalence
and risk factors of anemia in children attending daycare centers in Belo Horizonte-MG.
Rev Bras Epidemiol. 2012;15(3):675-684. doi: 10.1590/S1415-790X2012000300020.
98. Zuffo CRK, Schmidt ST, Taconeli CA, Osório MM, Almeida CCB, da Silva BHC.
Prevalence and risk factors of anemia in children. J Pediatr (Rio J). 2015.
doi:10.1016/j.jped.2015.09.007.
99. Al-Quaiz JM. Iron deficiency anemia. A study of risk factors. Saudi Med J.
2001;22(6):490-496.
100. Christides T, Sharp P. Sugars increase non-heme iron bioavailability in human epithelial
intestinal and liver cells. PLoS One. 2013;8(12):e83031.
doi:10.1371/journal.pone.0083031.
101. Pollack S, Kaufman RM, Crosby WH. Iron Absorption: Effects of Sugars and Reducing
Agents. Blood. 1963;24(5):577-581.

31
102. Maunder EMW, Nel JH, Steyn NP, Kruger HS, Labadarios D. Added sugar, macro- and
micronutrient intakes and anthropometry of children in a developing world context. PLoS
One. 2015;10(11):1-24. doi:10.1371/journal.pone.0142059.

32
Table 1. Descriptive Statistics of Children 6-59 Months of Age with IDA vs.
without Anemia
Variable N Case Control p-value
Child Characteristics
Age (months), mean (SD) 213 14.4 (9.6) 36.2 (14.8) 0.000
Gender: Female, % 213 35.2 51.4 0.025
Male, % 64.8 48.6
Weight on admission (kg), mean (SD) 124 9.7 (2.1) 13.6 (3.1) 0.000
Height on admission(cm), mean (SD) 102 75.9 (8.5) 90.6 (11.0) 0.000
Birth History
Birth weight (g), mean (SD) 212 2602.7 (701.2) 3172.8 (517.4) 0.000
Birth length (cm), mean (SD) 201 48.0 (4.5) 49.6 (4.3) 0.020
Gestational age, mean (SD) 213 37.4 (3.3) 38.9 (2.0) 0.000
Maternal anemia: Yes, % 210 30.4 17.7 0.037
No, % 69.6 82.3
Coffee consumption during pregnancy:
Never, %
212
19.7
38.3
0.024
1-2 cups, % 63.4 48.2
More than 3 cups, % 16.9 13.5
Delivery number (total) , mean (SD) 213 1.8 (0.8) 1.8 (0.6)
Child’s birth order, mean (SD) 213 1.78 (0.8) 1.6 (0.6) 0.028
Delivery interval, mean (SD) 110 53.3 (39.2) 54.0 (33.4) 0.097
Delivery type: Natural, % 212 53.5 73.8 0.003
Cesarean section, % 46.5 26.2
Feeding Practice During the First Year of Life
Breastfeeding initiation: Immediately% 213 16.9 33.8 0.013
During the first day % 46.5 42.3
After the first day % 35.2 21.1
Never % 2.8 0.0
Breastfeeding (total) duration, mean (SD) 213 8.5 (4.5) 9.6 (8.5) 0.271
Breastfeeding (exclusive) duration, mean
(SD)
212 2.7 (2.8) 2.7 (2.6) 0.982
Breastfeeding (mostly) duration, mean (SD) 212 2.5 (2.8) 1.4 (2.5) 0.004
Infant formula: Yes, % 210 40.6 51.8 0.127
No, % 59.4 48.2
Complementary food initiation 212 6.5 (2.1) 6.0 (2.3) 0.160
Tea consumption: Yes, % 206 22.7 59.3 0.000
No, % 77.3 40.7
Cow’s milk consumption: Yes, % 212 34.3 60.6 0.000
No, % 65.7 39.4
Bottle feeding: Yes, % 211 54.3 32.6 0.000
Stopped, % 8.6 38.3
Never, % 37.1 29.1

33
Variable N Case Control p-value Bottle in bed: Occasionally, % 213 9.9 4.2 0.127
Most of the time, % 36.6 47.9
No, % 53.5 47.9
Weekly Food Frequency
Red meat, mean (SD) 213 1.9 (2.1) 2.6 (1.8) 0.043
Other types of meat, mean (SD) 213 1.2 (1.3) 2.3 (1.7) 0.000
Meat (all) , mean (SD) 213 2.9 (2.6) 4.4 (2.1) 0.000
Legume, mean (SD) 213 1.0 (1.7) 1.6 (1.8) 0.031
Commercial baby food, mean (SD) 213 1.6 (2.6) 0.7 (1.8) 0.002
Homemade grain, mean (SD) 213 3.8 (2.6) 3.9 (2.2) 0.662
Nuts, mean (SD) 213 0.6 (1.5) 1.1 (1.6) 0.044
Cow’s milk (# of cups per day), mean (SD) 213 1.1 (1.5) 0.7 (1.0) 0.027
Dairy, mean (SD) 213 3.6 (2.9) 4.9 (2.3) 0.000
Green vegetables, mean (SD) 213 1.8 (2.3) 2.2 (2.3) 0.192
Other vegetables, mean (SD) 213 2.8 (2.5) 4.4 (2.3) 0.000
Citrus fruits, mean (SD) 213 1.8 (2.5) 3.1 (2.4) 0.000
Other fruits, mean (SD) 213 4.7 (2.5) 5.6 (2.0) 0.003
Tea/coffee, mean (SD) 123 1.2 (2.5) 2.9 (2.9) 0.000
Sweet soda, mean (SD) 213 0.5 (1.5) 0.8 (1.7) 0.340
Sweets, mean (SD) 213 2.7 (2.9) 5.6 (2.2) 0.000
Bread, mean (SD) 213 4.9 (2.8) 6.4 (1.5) 0.000
Child Health and Care
Smoking in presence of the child:
Every day, %
213
23.9
26.8
0.442
Several times per week, % 9.9 15.5
Several times per month, % 14.1 7.7
Once per month or less, % 19.7 15.5
Never, % 32.4 34.5
Anemia among family members: Yes, % 209 30.4 11.4 0.001
No, % 69.6 88.6
Past history of child anemia: Yes, % 213 21.1 11.3 0.054
No, % 78.9 88.7
History of hookworm infection: Yes, % 205 11.7 15.3 0.040
No, % 88.3 84.7
History of diarrhea: Yes, % 213 2.8 8.5 0.247
No, % 97.2 91.5
History of blood loss: Yes, % 213 1.4 2.8 0.657
No, % 98.6 97.2
Presence of main caregiver: Yes, % 213 97.2 93.0 0.207
No, % 2.8 7.0
Day care center attendance: Yes, % 213 5.6 50.7 0.000
No, % 94.4 49.3
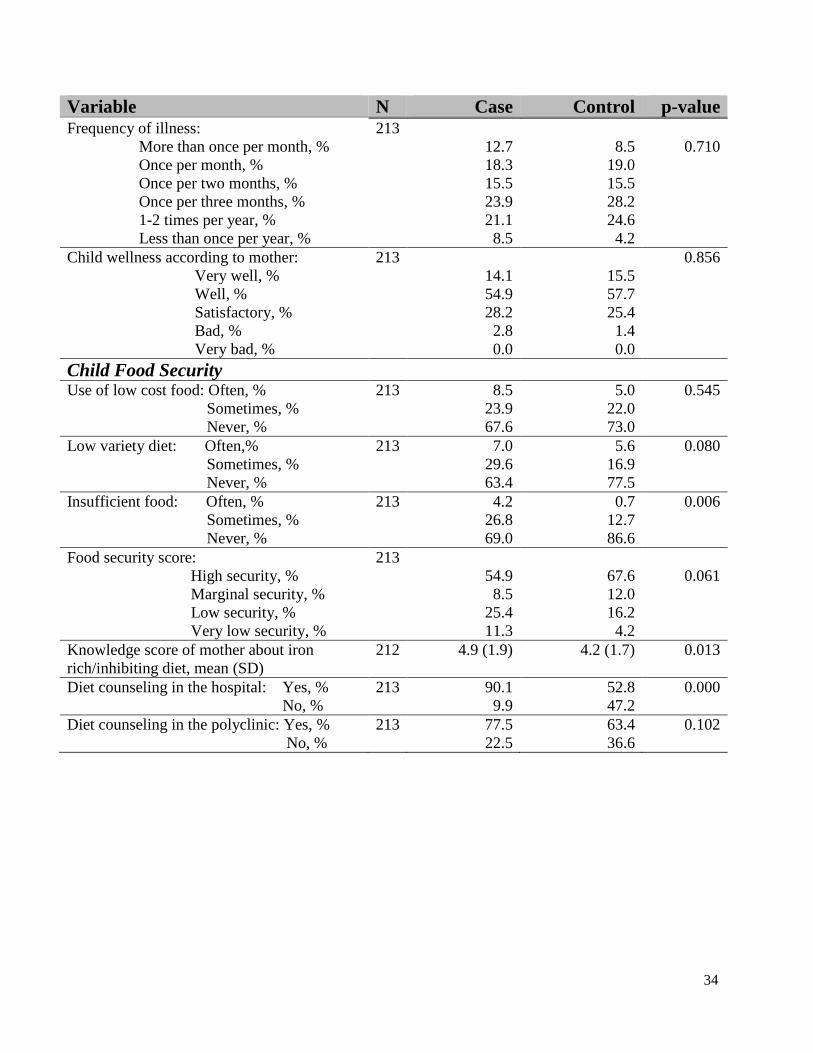
34
Variable N Case Control p-value Frequency of illness:
More than once per month, %
213
12.7
8.5
0.710
Once per month, % 18.3 19.0
Once per two months, % 15.5 15.5
Once per three months, % 23.9 28.2
1-2 times per year, % 21.1 24.6
Less than once per year, % 8.5 4.2
Child wellness according to mother:
Very well, %
213
14.1
15.5
0.856
Well, % 54.9 57.7
Satisfactory, % 28.2 25.4
Bad, % 2.8 1.4
Very bad, % 0.0 0.0
Child Food Security
Use of low cost food: Often, % 213 8.5 5.0 0.545
Sometimes, % 23.9 22.0
Never, % 67.6 73.0
Low variety diet: Often,% 213 7.0 5.6 0.080
Sometimes, % 29.6 16.9
Never, % 63.4 77.5
Insufficient food: Often, % 213 4.2 0.7 0.006
Sometimes, % 26.8 12.7
Never, % 69.0 86.6
Food security score:
High security, %
213
54.9
67.6
0.061
Marginal security, % 8.5 12.0
Low security, % 25.4 16.2
Very low security, % 11.3 4.2
Knowledge score of mother about iron
rich/inhibiting diet, mean (SD)
212 4.9 (1.9) 4.2 (1.7) 0.013
Diet counseling in the hospital: Yes, % 213 90.1 52.8 0.000
No, % 9.9 47.2
Diet counseling in the polyclinic: Yes, % 213 77.5 63.4 0.102
No, % 22.5 36.6

35
Barriers to Iron Rich Food N Case Control p-value
Diet improvement is needed: Yes, % 212 58.6 64.1 0.436
No, % 41.4 35.9
Difficulties in feeding with beef/liver:
Yes, %
213
11.3
15.5
0.645
Sometimes, % 19.7 21.1
No, % 69.0 63.4
Difficulties in feeding with fish/seafood:
Yes, %
213
15.5
16.2
0.017
Sometimes, % 36.6 19.0
No, % 47.9 64.8
Difficulties in feeding with poultry/pork:
Yes, %
213
9.9
7.7
0.208
Sometimes, % 25.4 16.2
No, % 64.8 76.1
Difficulties in feeding with green veg-s:
Yes, %
213
1.4
16.9
0.003
Sometimes, % 21.1 14.8
No, % 77.5 68.3
Difficulties in feeding with citrus fruits:
Yes, %
213
8.5
5.6
0.041
Sometimes, % 29.6 16.2
No, % 62.0 78.2
Difficulties in feeding with legume:
Yes, %
212
5.6
13.5
0.117
Sometimes, % 9.9 14.2
No, % 84.5 72.3
Difficulties in feeding with all mentioned:
Yes, %
213
7.0
6.3
0.883
Sometimes, % 33.8 31.0
No, % 59.2 62.7
Child likes/dislikes: Yes, % 213 76.1 81.7 0.334
No, % 23.9 18.3
Food cost: Yes, % 213 46.5 23.9 0.001
No, % 53.5 76.1
Convenience: Yes, % 213 14.1 5.6 0.037
No, % 85.9 94.4
Availability: Yes, % 213 28.2 14.8 0.020
No, % 71.8 85.2
Advertisement: Yes,% 213 8.5 17.6 0.074
No, % 91.5 82.4
Others minding the child: Yes, % 213 19.7 16.9 0.613
No, % 80.3 83.1

36
Socio-demographic Characteristics of
Parents and Family N Case Control p-value
Mother’s age, mean (SD) 213 28.5 (5.1) 29.6 (5.1) 0.133
Presence of both parents: Yes, % 213 91.5 97.9 0.030
No, % 8.5 2.1
Mother’s education:
Incomplete secondary, %
213
1.4
0.0
0.041
Secondary, % 46.5 40.0
Professional technical, % 11.3 18.3
University, % 40.8 52.8
Postgraduate, % 0.0 0.7
Father’s education:
Incomplete secondary, %
205
3.1
0.0
0.052
Secondary, % 56.9 42.1
Professional technical, % 10.8 15.0
University, % 29.2 42.1
Postgraduate, % 0.0 0.7
Mother’s employment:
Employed, %
213
14.1
27.5
0.260
In maternity leave, % 18.3 14.1
Unemployed, % 64.8 55.6
Works at home, % 1.4 2.1
Seasonal employee/farm worker, % 0.0 0.0
Student, % 1.4 0.7
Father’s employment:
Employed, %
205
66.2
76.4
0.292
Unemployed, % 9.2 10.0
Works at home, % 3.1 0.7
Seasonal employee/farm worker, % 10.8 5.0
Migratory worker, % 10.8 7.9
Student, % 0.0 0.0
Household heating system:
Electricity, %
201
18.6
11.3
0.000
Hot water, % 22.0 46.5
Wood, % 37.3 26.1
Animal dung, % 11.9 0.0
Gas heater, % 10.2 16.2
Household size, mean (SD) 213 5.8 (2.0) 5.5 (1.8) 0.209
Number of children in household, mean (SD) 213 2.1 (1.2) 1.9 (0.7) 0.269
Socioeconomic status score, mean (SD) 213 5.2 (1.7) 5.8 (1.9) 0.021
Resident of : Yerevan, % 213 36.6 46.5 0.171
Region, % 63.4 53.5
Residency: Urban, % 213 71.8 73.9 0.743
Rural, % 28.2 26.1

37
Table 2. ORs, CIs and p-values from simple logistic regression and age-adjusted multiple logistic regression
analyses between IDA status and independent variables
Unadjusted analysis Age-adjusted analysis
Variable OR CI P-value OR CI P-value
Child Characteristics
Age (months) 0.87 0.84-0.91 0.000
Gender: Male
Female
1.00
0.03
0.29-0.93
0.026
1.00
0.75
0.35-0.61
0.462
Birth History
Birth weight 0.998 0.998-0.999 0.000 0.998 0.998-0.999 0.000
Birth length 0.93 0.86-0.99 0.030 0.91 0.83-0.99 0.035
Maternal anemia during pregnancy 2.03 1.04-3.97 0.039 1.65 0.69-3.96 0.261
Maternal coffee consumption during pregnancy:
None
1.00
1-2 cups 0.41 0.16-1.04 0.061
3 cups and more 1.05 0.46-2.37 0.911
Gestational age 0.80 0.72-0.90 0.000 0.83 0.71-0.98 0.024
Delivery type 2.44 1.34-4.44 0.003 2.24 1.01-4.97 0.048
Birth order 1.56 1.04-2.33 0.030 1.16 0.66-2.04 0.603
Feeding Practice During the First Year of Life
Breastfeeding (predominantly) duration 1.17 1.05-1.31 0.006 1.11 0.97-1.28 0.124
Cow’s milk consumption 0.34 0.19-0.62 0.000 1.08 0.48-2.46 0.850
Tea/coffee consumption 0.20 0.10-0.39 0.000 0.64 0.27-1.52 0.320
Bottle feeding: Never 1.00 1.00
Stopped 0.18 0.07-0.47 0.000 0.30 0.09-0.95 0.041
Till now 1.30 0.68-2.21 0.427 1.14 0.48-2.7 0.764
Bottle in bed: Never 1.00
Occasionally 0.18 0.07-0.47 0.000 1.00
Most of the time 1.30 0.68-2.50 0.427 3.89 0.69-21.9 0.123
Weekly food frequency
Read meat in diet 0.85 0.72-1.00 0.045 0.84 0.70-1.02 0.071

38
Unadjusted analysis Age-adjusted analysis
Variable OR CI P-value OR CI P-value Other meat in diet 0.58 0.46-0.74 0.000 0.65 0.49-0.87 0.003
Meat in diet 0.76 0.67-0.87 0.000 0.79 0.67-0.94 0.006
Legume 0.78 0.63-0.96 0.017 1.04 0.80-1.35 0.755
Commercial baby food 1.22 1.07-1.39 0.003 1.10 0.93-1.29 0.280
Nuts 0.80 0.63-1.00 0.051 0.99 0.77-1.28 0.994
Cow’s milk (N of cups per day) 1.29 1.02-1.62 0.030 1.38 1.03-1.86 0.032
Dairy 0.81 0.72-0.90 0.000 0.91 0.79-1.06 0.217
Other vegetables 0.75 0.66-0.86 0.000 0.80 0.66-0.93 0.005
Citrus fruits 0.78 0.68-0.89 0.000 0.90 0.78-1.05 0.183
Other fruits 0.83 0.73-0.94 0.004 0.85 0.72-1.01 0.058
Tea/coffee 0.79 0.70-0.89 0.000 0.98 0.84-1.14 0.787
Sweets 0.68 0.61-0.77 0.000 0.81 0.70-0.93 0.003
Bread 0.73 0.64-0.84 0.000 0.78 0.63-0.95 0.014
Food diversity score 0.61 0.51-0.72 0.000 0.70 0.56-0.86 0.001
Child Health and Care
Smoking in presence of the child:
Less than once per month 1.00 1.00
Several times per month 0.77 0.41-1.42 0.402 0.80 0.36-1.79 0.590
Several times per week and more 1.74 0.68-4.48 0.248 3.22 0.83-12.48 0.090
Anemia among family members 3.39 1.63-7.04 0.001 2.48 0.98-6.30 0.056
Past history of anemia of the child 2.11 0.98-4.56 0.058 2.44 0.83-7.16 0.105

39
Unadjusted analysis Age-adjusted analysis
Variable OR CI P-value OR CI P-value History of hookworm infection 0.26 0.07-0.89 0.032 0.66 0.14-2.91 0.567
Daycare attendance 0.06 0.02-0.17 0.000 0.53 0.14-1.94 0.335
Food security-combined
High security 1.00 1.00
Low security 1.97 0.97-3.99 0.061 1.21 0.50-3.06 0.686
Very low security 3.35 1.10-10.20 0.033 2.91 0.66-12.79 0.156
Knowledge score 1.23 1.04-1.46 0.015 1.14 1.92-1.40 0.226
Barriers to iron rich food
Difficulties in feeding with fish/seafood:
No 1.00
Sometimes 1.29 0.57-2.94 0.537
Yes 2.61 1.34-5.08 0.005
Difficulties in feeding with poultry/pork:
No 1.00
Sometimes 1.49 0.55-4.10 0.435
Yes 1.84 0.91-3.73 0.092
Difficulties in feeding with green vegetables:
No 1.00
Sometimes 0.07 0.01-0.56 0.012
Yes 1.26 0.60-2.64 0.541
Difficulties in feeding with citrus fruits:
No 1.00
Sometimes 1.89 0.62-5.77 0.262
Yes 2.30 1.16-4.58 0.017

40
Unadjusted analysis Age-adjusted analysis
Variable OR CI P-value OR CI P-value Food cost 2.76 1.51-5.05 0.001 1.82 0.82-4.03 0.139
Convenience 2.75 1.03-7.30 0.043 2.04 0.54-7.72 0.292
Availability 2.26 1.13-4.52 0.021 1.84 0.72-4.66 0.201
Advertisement 0.43 1.17-1.11 0.080 0.48 1.51-1.55 0.482
Sociodemographic Characteristics of Parents and Family
Mother’s employment 0.66 0.36-1.12 0.168 0.84 0.39-1.82 0.657
Mother’s education: Secondary 1.00 1.00
Professional technical 0.36 0.15-0.90 0.029 0.49 0.15-1.64 0.246
University 0.45 0.24-0.84 0.012 0.45 0.22-1.13 0.097
Father’s education: Secondary 1.00 1.00
Professional technical 0.50 0.20-1.30 0.156 0.80 0.20-3.22 0.749
University 0.48 0.25-0.92 0.028 0.53 0.22-1.25 0.147
Household size 1.10 0.95-1.28 0.209 1.21 0.92-1.39 0.263
Number of children in household 1.20 0.87-1.61 0.269 1.19 0.81-1.76 0.381
Heating system: Non- biofuel
Biofuel
1.00
0.002
1.00
2.74 1.46-5.17 2.17 0.92-5.15 0.078
SES score 0.83 0.71-0.98 0.023 0.89 0.72-1.09 0.252
Residency: Yerevan
Regions
1.00
1.50
0.84-2.00
0.172
1.00
1.64
0.63-2.96
0.425
The age-adjusted analysis was conducted for all those variables that were associated with the outcome in the unadjusted analysis at p≤0.25 level of significance.

41
Table 3. Multiple logistic regression model of determinants of IDA among
hospitalized children 6-59 months of age
Characteristics OR 95% CI P value
Child’s age (months) 0.89 0.85 - 0.93 0.000
Child’s birth weight (grams) 0.99 0.997 - 0.999 0.000
Cow’s milk consumption (# of cups per day) 1.51 1.04 - 2.19 0.030
Sweet in diet (# of times per week) 0.78 0.65 - 0.93 0.006
Child’s food diversity score 0.76 0.58 - 0.98 0.034
Previous history of child’s anemia 3.43 1.04-11.27 0.043
Model’s fit statistics: Hosmer & Lemeshow goodness of fit test,
p=0.862
R-square=0.709

42
Appendix 1. Medical Record Review Form
General Information
ID# ____|____|____
Date of birth ____/____/_______
Patient sex Male___ Female___
Date of admission ____/____/_______ Date of discharge ____/____/_______
Main clinical diagnosis _____________________________________________
Having chronic disease No___ Yes______________________________________(name of the disease)
Patient weight_______ kg height_________ cm (at the time of admission)
Anemia Status
Hemoglobin level ___________ g/L
Mean corpuscular volume (MCV) ___________ fL
Serum Ferritin __________ ng/mL
CRP __________mg/L or __________ (-/+)

43
Appendix 2. Journal Form
Interviewer’s name (first, last), _______________________________________
RESULT CODES (RC)
1. Completed interview
2. No such case (wrong name, wrong address)
3. Mother or caretaker is not available
4. No response (nobody answers the call)
5. Refusal
6. Respondent doesn’t understand Armenian
7. Postponed interview
8. Incomplete interview
9. Other _____________________________________________________
ID # Name of the child (first, last) Child’s address Child’s phone Adm.
date
Disch.
date
Birth
date
Hosp
ital
Att
1
Att
2
Att
3
Case/
control

44
Appendix 3. Questionnaire for Telephone Interview with Mothers
# Ընդհանուր տեղեկություններ երեխայի մասին
Մորը հայտնել, որ հաջորդ հարցերը վերաբերում են տվյալ երեխային (անունը):
1. Ի՞նչ քաշով և հասակով է ծնվել երեխան: 1ա․_________ գրամ 1բ․ ______ սմ
88. Չգիտեմ
2. Այս երեխայով հղիության ընթացքում Դուք
ունեցե՞լ եք սակավարյունություն (արյան
պակաս):
1. Այո
2. Ոչ
88. Չգիտեմ
3. Միջին հաշվով, օրական քանի՞ բաժակ սուրճ եք
խմել այս երեխայով հղիության ժամանակ:
1. Ոչ մի բաժակ
2. 1-2 բաժակ
3. 3 բաժակ և ավելի
88․Չգիտեմ
4. Հղիության ո՞րերորդ շաբաթում է ծնվել երեխան: _______-րդ
5. Ինչպե՞ս եք ծննդաբերել այս երեխային:
(Կարդա՛լ պատասխանները) 1. Բնական ճանապարհով
2. Կեսարյան հատումով
6. Մինչև այժմ Դուք քանի՞ ծննդաբերություն եք
ունեցել: _______ (Եթե 1՝ անցում Հ․9)
7. Այս երեխան Ձեր ո՞րերորդ ծննդաբերությունից է: _______-րդ (Եթե 1-ին՝ անցում Հ․9)
8. Այս երեխայի ծննդից որքա՞ն ժամանակ առաջ է
եղել Ձեր նախորդ ծննդաբերությունը: ______ տարի ______ ամիս
Հայաստանում երկաթ դեֆիցիտային անեմիայի որոշիչ գործոնները
6-59 ամսական հոսպիտալացված երեխաների շրջանում
Հարցազրուցավարի ID ____|____
Մասնակցի ID ____|____|____
Ամսաթիվ ____/____/________
Սկիզբ ____:____ Ավարտ ____:____

45
# Սնուցում և կրծքով կերակրում կյանքի առաջին տարում
9. Ծննդաբերությունից հետո որքա՞ն ժամանակ
անց եք երեխային մոտեցրել կրծքին:
(Կարդա՛լ պատասխանները)
1. Անմիջապես (առաջին ժամում)
2. Առաջին օրվա ընթացքում
3. Առաջին օրվանից հետո
4. Ընդհանրապես չեմ մոտեցրել
5. Չեմ հիշում
10. Որքա՞ն ժամանակ է երեխան կերակրվել կրծքով: 1. Չի կերակրվել……….(Անցում Հ․13)
2. Մինչև մեկ շաբաթ
3. ________ ամիս
4. Մինչև հիմա կերակրվում է
11. Որքա՞ն ժամանակ է երեխան կերակրվել միայն
կրծքի կաթով` չստանալով ո´չ ջուր, ո´չ այլ
հեղուկ կամ սնունդ:
1. Չի կերակրվել
2. Մինչև մեկ շաբաթ
3. ________ ամիս
4. Մինչև հիմա………….(Անցում Հ․35)
12. Որքա՞ն ժամանակ է երեխան կերակրվել
գերազանցապես կրծքի կաթով (հնարավոր է
նաև`ջուր կամ սամիթի ջուր):
1. Չի կերակրվել
2. Մինչև մեկ շաբաթ
3. ________ ամիս
4. Մինչև հիմա………….(Անցում Հ․35)
13. Ե՞րբ եք սկսել երեխային մանկական
կաթնախառնուրդ տալ (օրինակ՝ Հիփ, Նան,
Սիմիլակ):
1. _____ ամս-ում`_______________
2. Չեմ տվել (կաթնախառն.-ի անունը)
88. Չեմ հիշում
14. Ե՞րբ եք սկսել երեխային հավելյալ սնունդ տալ
(կիսաջրիկ կամ պինդ սնունդ, օր.` շիլա, պյուրե):
1. _______ ամսականում
2. Չեմ տվել
88. Չեմ հիշում
15. Ե՞րբ եք սկսել երեխային սև թեյ կամ սուրճ տալ: 1. _________ ամսականում
2. Չեմ տվել
88. Չեմ հիշում
16. Ե՞րբ եք սկսել երեխային կովի կամ այլ
կենդանական կաթ տալ (արտադրված, փոշի,
խտացրած կամ տնական):
1. ______ ամսականում
2. Չեմ տվել
88. Չեմ հիշում
17. Արդյո՞ք երեխան կերակրվում (կերակրվել) է
շշով օրվա ընթացքում:
1. Այո
2. Երբևէ չի կերակրվել…………(Անցում Հ.19) 3. Այժմ չի կերակրվում___________
(նշել դադարեցնելու տարիքը) 4. Չգիտեմ………………………..(Անցում Հ.19)
18. Արդյո՞ք երեխան կերակրվում (կերակրվել) է
շշով անկողնում (օրինակ` քնելուց առաջ)
1. Հազվադեպ
2. Հաճախ
3. Ոչ
4. Չգիտեմ

46
Սնուցման գործելակերպ
Կարդա՛լ․«Հաջորդ հարցերը վերաբերում են երեխայի սննդակարգին մինչ հիվանդանոց դիմելը»
19. Շաբաթվա ընթացքում քանի՞ անգամ է երեխան օգտագործում տավարի միս
կամ լյարդ՝ բացառությամբ երշիկի, նրբերշիկի:
_______ անգամ
20. Շաբաթվա ընթացքում քանի՞ անգամ է երեխան օգտագործում թռչնամիս, ձուկ,
խոզի միս՝ բացառությամբ երշիկի, նրբերշիկի:
_______ անգամ
21. Շաբաթվա ընթացքում քանի՞ անգամ է երեխան օգտագործում լոբազգիներ
(լոբի, ոսպ, սիսեռ, ոլոռ):
_______ անգամ
22. Շաբաթվա ընթացքում քանի՞ անգամ է երեխան օգտագործում պատրաստի
մանկական կերակրատեսակներ (շիլաներ, բանջարեղենային պյուրեներ):
_______ անգամ
23. Շաբաթվա ընթացքում քանի՞ անգամ է երեխան ուտում տան պայմաններում
ձավարեղենից պատրաստված սնունդ (հնդկացորեն, վարսակ, բլղուր, բրինձ):
_______ անգամ
24. Շաբաթվա ընթացքում քանի՞ անգամ է երեխան օգտագործում ընդեղեն (ընկույզ,
նուշ, պնդուկ և այլն):
_______ անգամ
25. Միջինում օրեկան քանի՞ բաժակ (200մլ) կովի կաթ է խմում երեխան, այդ թվում
նաև` պատրաստված կաթի փոշուց կամ խտացրած կաթից:
_______ բաժակ
26. Շաբաթվա ընթացքում քանի՞ անգամ է երեխան օգտագործում այլ կաթնամթերք
(պանիր, կաթնաշոռ, մածուն կամ այլ կաթնամթերք):
_______ անգամ
27. Շաբաթվա ընթացքում քանի՞ անգամ է երեխան օգտագործում կանաչեղեն,
ինչպես նաև կանաչ բանջարեղեն, օրինակ՝ բրոկոլի, սպանախ, մառոլ, շուշան։
_______ անգամ
28. Շաբաթվա ընթացքում քանի՞ անգամ է երեխան օգտագործում այլ բանջարեղեն,
օրինակ՝ պղպեղ, լոլիկ, գազար, բացառությամբ կարտոֆիլի։
_______անգամ
29. Շաբաթվա ընթացքում քանի՞ անգամ է երեխան օգտագործում ցիտրուսային
մրգեր և մրգահյութեր (նարինջ, թուրինջ, մանդարին, կիտրոն):
_______ անգամ
30. Շաբաթվա ընթացքում քանի՞ անգամ է երեխան օգտագործում մրգեր
(բացառությամբ՝ ցիտրուսների) կամ մրգաչիր:
_______ անգամ
31. Շաբաթվա ընթացքում քանի՞ անգամ է երեխան օգտագործում թեյ/սուրճ։ _______ անգամ
32. Շաբաթվա ընթացքում քանի՞ անգամ է երեխան խմում լիմոնադ, կոկա-կոլա,
ֆանտա կամ այլ քաղցր գազավորված ընպելիք:
_______ անգամ
33. Շաբաթվա ընթացքում քանի՞ անգամ է երեխան օգտագործում կոնֆետ, շաքար,
կամ շաքարից պատրաստած այլ քաղցրավենիք:
_______ անգամ
34. Շաբաթվա ընթացքում քանի՞ անգամ է երեխան օգտագործում հաց: _______ անգամ

47
Երեխայի՝ սննդով ապահովվածություն
Կարդա՛լ․ «Հիմա ես կնկարագրեմ մի քանի իրավիճակ` կապված երեխայի համար սնունդ
ձեքբերելու հետ։ Խնդրում եմ պատասխանեք՝ վերջին 12 ամսվա ընթացքում Դուք որքա՞ն հաճախ
եք եղել այդպիսի իրավիճակներում` ՀԱՃԱ՞Խ, ԵՐԲԵ՞ՄՆ, թե՞ ԵՐԲԵՔ» ։
35. «Ես/Մենք օգտագործում ենք միայն որոշ ցածր արժողությամբ
մթերքներ երեխային կերակրելու համար, քանի որ կան
սնունդ գնելու ֆինանսական դժվարություններ»։ Այս իրավիճակը որքա՞ն հաճախ է հանդիպել վերջին 12
ամսվա ընթացքում։
1. Հաճախ
2. Երբեմն
3. Երբեք
4. Չգիտեմ/Հրաժարվում եմ
պատասխանել
36. «Ես/Մենք չենք կարողանում կերակրել երեխային բազմազան
սննդով, քանի որ չենք կարող ձեռք բերել այն:»
Այս իրավիճակը որքա՞ն հաճախ է հանդիպել վերջին 12
ամսվա ընթացքում։
1. Հաճախ
2. Երբեմն
3. Երբեք
4. Չգիտեմ/Հրաժարվում եմ
պատասխանել
37. «Մեր երեխան բավարար քանակությամբ չի սնվում, քանի որ
չենք կարող ձեռք բերել բավարար քանակությամբ սնունդ։»
Այս իրավիճակը որքա՞ն հաճախ է հանդիպել վերջին 12
ամսվա ընթացքում։
1. Հաճախ
2. Երբեմն
3. Երբեք
4. Չգիտեմ/Հրաժարվում եմ
պատասխանել
Եթե տրվել է մեկ կամ ավել դրական պատասխան («հաճախ» կամ «երբեմն»), հարցնել նաև 48-51 հարցերը, այլապես անցնել հարց 52-ին:
38. Վերջին 12 ամսվա ըննթացքում դուք երբևէ կրճատե՞լ եք
երեխայի սննդի չափաբաժինը` սնունդ գնելու ֆինանսական
դժվարությունների պատճառով
1. Այո
2. Ոչ
3. Չգիտեմ
39. Վերջին 12 ամսվա ընթացքում երբևէ երեխան բաց թողե՞լ է
սնվելը` սնունդ գնելու ֆինանսական դժվարությունների
պատճառով:
1. Այո
2. Ոչ……(անցում Հ․50)
3. Չգիտեմ…. (անցում Հ․50)
49ա․
Որքա՞ն հաճախ է հանդիպում այդ իրավիճակը:
1. Գրեթե ամեն ամիս
2. Որոշ ամիսների
ընթացքում, ոչ բոլոր
3. Միայն 1 կամ 2 ամիս
4. Չգիտեմ
40. Վերջին 12 ամսվա ընթացքում երբևէ եղե՞լ է, որ երեխան
քաղցած լինի, սակայն դուք չկարողանաքլ ձեռք բերել ավելի
շատ սնունդ:
1. Այո
2. Ոչ
3. Չգիտեմ
41. Վերջին 12 ամսվա ընթացքում երբևէ երեխան եղե՞լ է քաղցած
ամբողջ օրվա ընթացքում` սնունդ գնելու ֆինանսական
դժվարությունների պատճառով:
1. Այո
2. Ոչ
3. Չգիտեմ
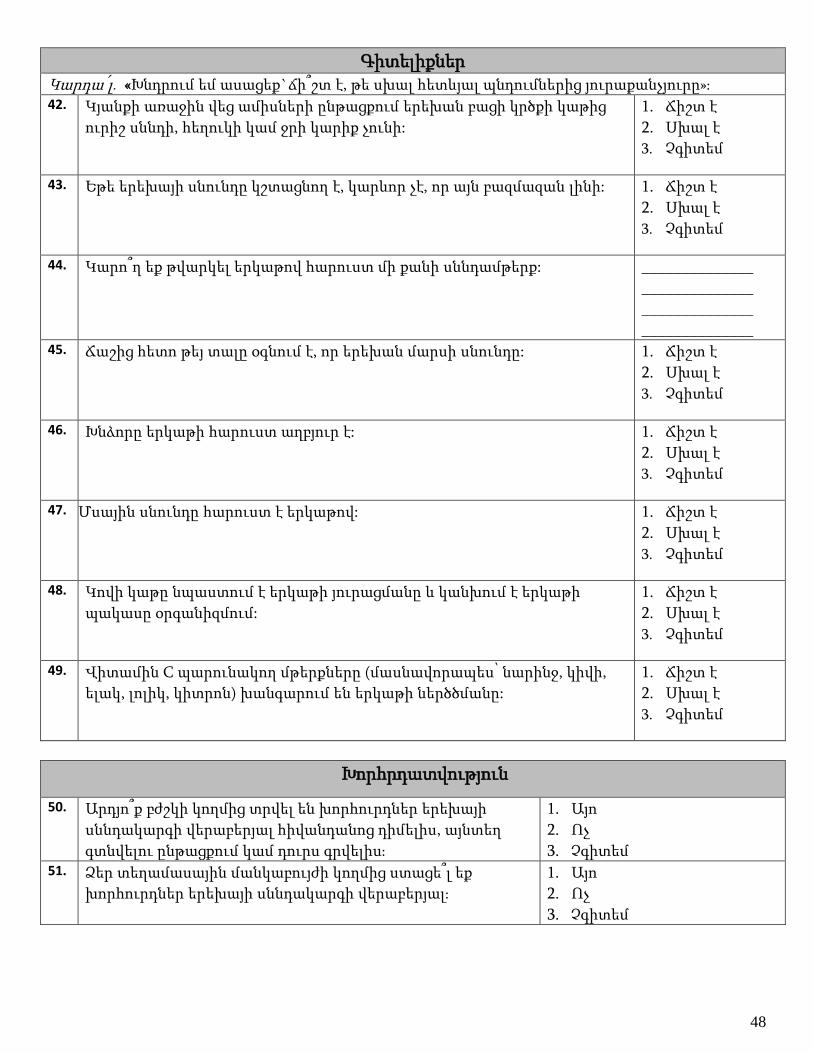
48
Գիտելիքներ
Կարդա՛լ․ «Խնդրում եմ ասացեք`ճի՞շտ է, թե սխալ հետևյալ պնդումներից յուրաքանչյուրը»։ 42. Կյանքի առաջին վեց ամիսների ընթացքում երեխան բացի կրծքի կաթից
ուրիշ սննդի, հեղուկի կամ ջրի կարիք չունի:
1. Ճիշտ է
2. Սխալ է
3. Չգիտեմ
43. Եթե երեխայի սնունդը կշտացնող է, կարևոր չէ, որ այն բազմազան լինի: 1. Ճիշտ է
2. Սխալ է
3. Չգիտեմ
44. Կարո՞ղ եք թվարկել երկաթով հարուստ մի քանի սննդամթերք: ______________
______________
______________
______________ 45. Ճաշից հետո թեյ տալը օգնում է, որ երեխան մարսի սնունդը: 1. Ճիշտ է
2. Սխալ է
3. Չգիտեմ
46. Խնձորը երկաթի հարուստ աղբյուր է: 1. Ճիշտ է
2. Սխալ է
3. Չգիտեմ
47. Մսային սնունդը հարուստ է երկաթով: 1. Ճիշտ է
2. Սխալ է
3. Չգիտեմ
48. Կովի կաթը նպաստում է երկաթի յուրացմանը և կանխում է երկաթի
պակասը օրգանիզմում:
1. Ճիշտ է
2. Սխալ է
3. Չգիտեմ
49. Վիտամին C պարունակող մթերքները (մասնավորապես՝ նարինջ, կիվի,
ելակ, լոլիկ, կիտրոն) խանգարում են երկաթի ներծծմանը:
1. Ճիշտ է
2. Սխալ է
3. Չգիտեմ
Խորհրդատվություն
50. Արդյո՞ք բժշկի կողմից տրվել են խորհուրդներ երեխայի
սննդակարգի վերաբերյալ հիվանդանոց դիմելիս, այնտեղ
գտնվելու ընթացքում կամ դուրս գրվելիս։
1. Այո
2. Ոչ
3. Չգիտեմ 51. Ձեր տեղամասային մանկաբույժի կողմից ստացե՞լ եք
խորհուրդներ երեխայի սննդակարգի վերաբերյալ։
1. Այո
2. Ոչ
3. Չգիտեմ

49
Երեխայի խնամք և առողջություն
52. Որքա՞ն հաճախ են մարդիկ ծխում երեխայի
ներկայությամբ` նույն սենյակում:
(Կարդա՛լ պատասխանները)
1. Ամեն օր
2. Շաբաթը մի քանի անգամ
3. Ամիսը մի քանի անգամ
4. Ամիսը մեկ կամ պակաս
5. Երբեք
53. Ձեր ընտանիքում որևէ մեկն ունի՞
սակավարյունություն (արյան պակաս) :
1. Այո __________(36ա.Ազգակց. կապը երեխայի հետ)
2. Ոչ
88. Չգիտեմ
54. Նախկինում երեխայի մոտ ախտորոշվե՞լ է
սակավարյունություն (արյան պակաս) մինչ
հիվանդանոց ընդունվելը։
1. Այո ________(37ա.Երեխայի տարիքը ախտորոշման ժ-կ)
2. Ոչ
88. Չգիտեմ
55. Վերջին տարվա ընթացքում երեխան ունեցե՞լ
է ճիճվակրություն:
1. Այո, հիվանդանոց դիմելուց առաջ
2. Այո, հիվանդանոց դիմելուց հետո
3. Ոչ
88. Չգիտեմ
56. Վերջին տարվա ընթացքում երեխան ունեցե՞լ
է տևական (2 շաբաթից ավել տևող),
հաճախակի (ամիսը 3-4 անգամ) կամ
արյունային փորլուծություն:
1. Այո, հիվանդանոց դիմելուց առաջ
2. Այո, հիվանդանոց դիմելուց հետո
3. Ոչ
88․ Չգիտեմ
57. Վերջին տարվա ընթացքում երեխան ունեցե՞լ
է արյան զգալի կորուստ վիրահատության
կամ արյունահոսության հետևանքով (օր․`
քթից)
1. Այո, հիվանդանոց դիմելուց առաջ
2. Այո, հիվանդանոց դիմելուց հետո
3. Ոչ
88. Չգիտեմ
58. Երեխան ունի՞ մեկ հիմնական խնամող, որը
նրա հետ է ամեն օր` օրվա մեծ մասը:
1. Այո _______________(41ա.կապը երեխայի հետ)
2. Ոչ
88. Չգիտեմ
59. Երեխան հաճախու՞մ է ցերեկային խնամքի
որևէ հաստատություն:
1. Այո
2. Ոչ
60. Որքա՞ն հաճախ է երեխան հիվանդանում:
(Կարդա՛լ պատասխանները)
1. Ամիսը մեկ անգամից հաճախ
2. Ամիսը մեկ անգամ
3. Երկու ամիսը մեկ անգամ
4. Երեք ամիսը մեկ անգամ
5. Տարեկան մեկ-երկու անգամ
6. Տարեկան մեկ անգամից քիչ
61. Ընդհանուր առմամբ, ինչպե՞ս կգնահատեիք
երեխայի առողջությունը ներկայումս:
(Կարդալ՛ պատասխանները)
1. Շատ լավ
2. Լավ
3. Բավարար
4. Վատ
5. Շատ վատ

50
Խոչընդոտներ
62. Ձեր կարծիքով, կարո՞ղ էր Ձեր երեխայի
սննդակարգն ավելի առողջ լինել, քան` հիմա։
1. Այո
2. Ոչ
63. Ձեզ համար դժվա՞ր է երեխային կերակրել
հետևյալ սննդատեսակներով․
(ես կթվարկեմ դրանք, իսկ դուք
պատասխանեք այո/երբեմն/ոչ)
այո երբեմն ոչ 1. Տավարի միս, լյարդ
2. Ձուկ/ծովամթերք այո երբեմն ոչ
3. Հավի/խոզի միս այո երբեմն ոչ
4. Կանաչ բանջարեղեն այո երբեմն ոչ
5. Ցիտրուսային մրգեր այո երբեմն ոչ
6. Լոբազգիներ(ոսպ,լոբի) այո երբեմն ոչ
7. Ընդհանուր առմամբ,
բոլոր նշված մթեքները այո երբեմն ոչ
64. Նշված գործոններից որո՞նք կարող են նշված
սննդատեսակներով (օր.՝ միս, կանաչ բանջ.,
ցիտրուսային մրգեր, լոբազգիներ) երեխային
չկերակրելու պատճառ հանդիսանալ ։
Կարող եք նշել մի քանի ճիշտ պատասխան։
1. Երեխայի նախասիրությունները
2. Սննդատեսակի գինը
3. Հարմարությունը
4. Հասանելիությունը
5. Գովազդը
6. Այլ մարդկանց ազդեցությունը երեխայի վրա
7. Ալերգիան
8. Այլ________________(նշե՛լ)
Սոցիալտնտեսական և ժողովրդագրական տվյալներ մոր և ընտանիքի մասին
65. Քանի՞ տարեկան եք:
(Մոր կամ խնամակալի լրացրած տարիների թիվը)
______ տարեկան * _____________________
(*Եթե մայր չունի, նշեք խնամակալի կապը երեխայի հետ):
66. Արդյո՞ք երկու ծնողներն էլ մասնակցում են
երեխայի խնամքին։
1. Այո
2. Ոչ ___________________________________
_________________________(նշե՛լ պատճառը)
67. Ի՞նչ կրթություն ունեք:(մայրը)
(Կարդա՛լ պատասխանները)
1. Թերի միջնակարգ (10 տարուց քիչ)
2. Միջնակարգ (10 տարի)
3. Միջնակարգ մասնագիտական (10-13 տարի)
4. Բարձրագույն
5. Հետդիպլոմային
68. Ի՞նչ կրթություն ունի երեխայի հայրը:
(Կարդա՛լ պատասխանները)
1. Թերի միջնակարգ (10 տարուց քիչ)
2. Միջնակարգ (10 տարի)
3. Միջնակարգ մասնագիտական (10-13 տարի)
4. Բարձրագույն
5. Հետդիպլոմային

51
Շնորհակալություն Ձեր մասնակցության և տրամադրած ժամանակի համար։
69. Ո՞րն է Ձեր ( երեխայի մոր) ներկայիս
զբաղվածությունը:
(Կարդա՛լ պատասխանները)
1. Աշխատում եմ
2. Աշխատում եմ, բայց ֆիզ. արձակուրդում եմ
3. Չեմ աշխատոււմ
4. Տանն եմ աշխատում
5. Սեզոնային աշխատող եմ կամ հողագործ
6. Ուսանող եմ
7. Այլ (նշեք) ________________________
70. Ո՞րն է երեխայի հոր ներկայիս
զբաղվածությունը:
(Կարդա՛լ պատասխանները)
1. Աշխատում է
2. Չի աշխատում
3. Տանն է աշխատում
4. Սեզոնային աշխատող է կամ հողագործ
5. Արտագնա աշխատող է
6. Ուսանող է
7. Այլ (նշեք) ________________________
71. Քանի՞ անձ է բնակվում Ձեր տանը` ներառյալ
Դուք:
_________
72. Մինչև 18 տարեկան քանի՞ երեխա է բնակվում
Ձեր տանը:
_________
73. Հիմնականում ինչպե՞ս է ջեռուցվում Ձեր
տունը:
1. _______________________________ (նշե՛լ)
2. Չի ջեռուցվում
74. Միջինում ամսական որքա՞ն գումար է
ծախսում Ձեր ընտանիքը:
1. 25 000 դրամից պակաս
2. 25 000-ից 50 000 դրամ
3. 50 001- 100 000 դրամ
4. 100 001-200 000 դրամ
5. 200 001-300 000 դրամ
6. 300 000 դրամից ավել
7. Չգիտեմ
75. Ձեր ընտանիքում քանի՞ հոգի է աշխատում
(հաշվեք նաև Ձեզ և նրանց, ովքեր աշխատում
են տանը, զբաղվում են հողագործությամբ,
սեզոնային և արտագնա աշխատանքով):
_________

52
# General Information about the Child
Inform mother, that next questions are about this child (name)
1. Child’s birth weight and height. 1a․_________ g 1b․ ______ cm
88. Don’t know
2. Did you have anemia during the pregnancy with this
child?
3. Yes
4. No
89. Don't know
3. In average, how many cups of coffee did you consume
per day during the pregnancy with this child?
4. None
5. 1-2 cups
6. 3 cups and more
88․Don’t know
4. Child’s gestational age. _______ (weeks)
5. How was this child delivered?
(Read the options) 3. Natural type
4. Cesarean section
6. How many deliveries have you had till now? _______ ……..(If 1, skip to Q.9)
7. Which delivery is this child from? _______ ……..(If 1, skip to Q.9)
8. When was your previous delivery before this child? ______ year(s)______ month(s)
Determinants of Iron Deficiency Anemia
among Hospitalized Children Aged 6-59 Months in Armenia
Interviewer ID ____|____
Interviewee ID ____|____|____
Date ____/____/________
Start ____:____ End____:____

53
# Feeding and Breastfeeding during the first year of life
9. When did you breastfeed your child for the first time
after delivery?
(Read the options)
6. Immediately (during the first hour)
7. During the first day
8. After the first day
9. Never
10. Don't know
10. How long your child has been breastfed? 5. Never……….(Skip to Q.13) 6. Until 1 week
7. ________ month(s)
8. Till now
11. How long your child has been exclusively breastfed
without receiving water, other liquids or food?
5. Never
6. Until 1 week
7. ________ month(s)
8. Till now ………….(Skip to Q.35)
12. How long your child has been mostly breastfed
(possibly water or fennel tea)?
5. Never
6. Until 1 week
7. ________ month(s)
8. Till now ………….(Skip to Q.35)
13. When have you started feeding your child with
infant formula (e.g. Hipp, Nan, Similac)?
3. _____ months_______________
4. Never (the name of formula)
88. Don’t know
14. When have you started feeding your child with
complementary food (semi-liquid or solid food, e.g.
porridge, puree)?
3. _______ months
4. Never
88. Don’t know
15. When have you started to give your child tea or
coffee?
1. _______ months
2. Never
88. Don’t know
16. When have you started to give your child cow’s or
other animal’s milk (produced, powder, evaporated
or homemade)?
1. _______ months
2. Never
88. Don’t know
17. Does the child use the bottle during the day? 5. Yes
6. Never used……………..(Skip to Q.19) 7. Stopped_______________
(age, when stopped) 8. Don’t know ……………(Skip to Q.19)
18. Does the child use a bottle in bed? (e.g. before
sleeping)
5. Occasionally
6. Most of the time
7. No
8. Don’t know

54
Feeding Practice
Read: ”Next questions are about your child’s diet before the admission to the hospital”
19. How many times does your child eat beef or liver except for sausages, during a week
_______ times
20. How many times does your child eat poultry, fish, pork except for sausages during a
week
_______ times
21. How many times does your child eat legume (bean, lentils, peas, chickpeas) during a
week?
_______ times
22. How many times does your child eat commercial baby food (porridges, purees) during
a week?
_______ times
23. How many times does your child eat homemade grain porridges (buckwheat, oats,
bulgur, rice) during a week?
_______ times
24. How many times does your child eat nuts (walnut, almond, hazelnut, etc.) during a
week?
_______ times
25. In average, how many glasses (200ml) of cow’s milk (including made from powder or
evaporated milk) does your child drink per day?
_______ times
26. How many times does your child eat other dairy products (cheese, curd, yoghurt, etc.)
during a week?
_______ times
27. How many times does your child eat greens and green vegetables (broccoli, spinach,
lettuce, shoushan) during a week?
_______ times
28. How many times does your child eat other vegetables (e.g. pepper, tomatoes, carrot,
except potatoes) during a week?
_______ times
29. How many times does your child use citrus fruits and juices (orange, grapefruit,
tangerine, lemon) during a week?
_______ times
30. How many times does your child eat fruits, juices and dried fruits except citruses
during a week?
_______ times
31. How many times does your child use tea or coffee during a week? _______ times
32. How many times does your child use lemonade, Coca-Cola, Fanta or other sweet soda
drinks during a week?
_______ times
33. How many times does your child use candy, sugar or other sugar based products
during a week?
_______ times
34. How many times does your child use bread during a week?
_______ times

55
Child Care and Health
35. How often people smoke in the presence of your
child in the same room?
(Read the options)
6. Every day
7. Several times per week
8. Several times per month
9. Once per month or less
10. Never
36. Does anybody have anemia in your family? 3. Yes __________(36a. Relationship to the child)
4. No
88. Don’t know
37. Has your child ever been diagnosed with anemia
before admission to the hospital?
3. Yes ________(37a. Age, when diagnosed)
4. No
88. Don’t know
38. Did your child have hookworm infection during
the last year?
4. Yes, before the hospitalization
5. Yes, after the hospitalization
6. No
89. Don’t know
39. Did your child have persistent (more than 2
weeks), frequent (2-4 times per moth) or bloody
diarrhea during the last year?
1. Yes, before the hospitalization
2. Yes, after the hospitalization
3. No
88. Don’t know
40. Did your child have notable blood loss due to
surgery or bleeding (e.g. nasal bleeding)?
4. Yes, before the hospitalization
5. Yes, after the hospitalization
6. No
89. Don’t know
41. Does your child have main caregiver, who stays
with the child most of the time every day?
3. Yes _______________(41a.relationship to child)
4. No
89. Don’t know
42. Does your child attend any day care center? 3. Yes
4. No
43. How often does your child get sick?
(Read the options)
7. More than once per month
8. Once per month
9. Once per 2 months
10. Once per 3 months
11. 1-2 times per year
12. Less than once per year
44. In general, how would you assess current health
status of your child?
(Read the options)
6. Very well
7. Well
8. Satisfactory
9. Bad
10. Very bad

56
Child Food Security
Read: “Now I'm going to read you several statements that people have made about the food situation of their children. For these statements, please tell me whether the statement was OFTEN true, SOMETIMES
true, or NEVER true in the last 12 months for”
45. “(I/we) relied on only a few kinds of low-cost food to feed
(my/our) child/the children) because (I was/we were)
running out of money to buy food.”
How often does this situation happen during the last 12
months?
5. Often
6. Sometimes
7. Never
8. Don’t know/ Refused
46. “(I/We) couldn’t feed (my/our) child a balanced and diverse
meal, because (I/we) couldn’t afford that.”
How often does this situation happen during the last 12
months?
5. Often
6. Sometimes
7. Never
8. Don’t know/ Refused
47. “Our child does not eat enough because we just couldn't
afford enough food."
How often does this situation happen during the last 12
months?
5. Often
6. Sometimes
7. Never
8. Don’t know/ Refused
If affirmative response (i.e., "often true" or "sometimes true") to one or more of questions, then continue to questions 48-51; otherwise skip to question 52.
48. In the last 12 months, did you ever cut the size of your child’s
meals because there wasn't enough money for food? 4. Yes
5. No
6. Don't know
49. In the last 12 months, did your child ever skip meals because
there wasn't enough money for food? 4. Yes
5. No………….. (skip to Q.50) 6. Don’t know…(skip to Q.50)
49a
How often did this happen? 5. Almost every month
6. Some months but not every month
7. Only 1 or 2 months
8. Don’t know
50. In the last 12 months, was your child ever hungry but you just
couldn't afford more food? 4. Yes
5. No
6. Don’t know
51. In the last 12 months, did your child ever not eat for a whole
day because there wasn't enough money for food? 4. Yes
5. No
6. Don't know

57
Knowledge
Read: ”Please answer, are the following statements true or false?”․
52. During the first six months of life child don’t need other food, liquid or water,
besides breast milk.
4. True
5. False
6. Don't know
53. If child’s food is filling, food diversity is not important. 4. True
5. False
6. Don't know
54. Can you list some iron rich foods? ______________
______________
______________
______________ 55. Tea after meal helps child to digest the food. 4. True
5. False
6. Don't know
56. Apple is iron rich source. 4. True
5. False
6. Don't know
57. Meat is rich in iron. 4. True
5. False
6. Don't know
58. Cow’s milk increases iron absorption and prevents iron deficiency. 4. True
5. False
6. Don't know
59. Vitamin C containing foods (orange, kiwi, strawberry, tomatoes, and lemon)
inhibit iron absorption.
4. True
5. False
6. Don't know
Counseling
60. Did the doctor give you recommendations about child diet during the hospital
stay or discharge?
4. Yes
5. No
6. Don't know 61. Have you received recommendation about your child diet from your primary
care physician?
4. Yes
5. No
6. Don't know

58
Barriers to Iron Rich Food
62. In your opinion, could your child’s diet be
healthier than now?
3. Yes
4. No
63. Is it difficult to feed your child with the following
foods?
(I will list them. Please answer
yes/sometimes/no)
yes sometimes no 8. Beef/ Liver
9. Fish/ Seafood yes sometimes no
10. Poultry/Pork yes sometimes no
11. Green vegetables yes sometimes no
12. Citrus fruits yes sometimes no
13. Legume(bean, lentils) yes sometimes no
14. In general, mentioned
above foods yes sometimes no
64. From the mentioned factors, which can be the
reason for not feeding the child with the
following foods (meat, green vegetables, citrus
fruits, legume)
Mention all answers that apply.
9. Child likes/dislikes
10. Cost of the food
11. Convenience
12. Availability
13. Advertising
14. Other people minding your child
15. Allergy
16. Other________________
Socioeconomic and Demographic Characteristics of Mother and Family
65. What is your age?
(Completed years age of mother or caregiver)
______ years * ________________________
(*If no mother, mention relationship of caregiver to child)
66. Do both parents take care of the child? 1. Yes
2. No ___________________________________
_________________________(mention the reason)
67. What is the highest level of education you
completed (mother)?
(Read the options)
1. Incomplete secondary
2. Secondary
3. Professional technical
4. University
5. Postgraduate
88. Don’t know
68. What is the highest level of education child’s father
completed?
(Read the options)
1. Incomplete secondary
2. Secondary
3. Professional technical
4. University
5. Postgraduate
88. Don’t know

59
Thank you for your participation and time!
69. What is your (mother’s) current occupational
status?
(Read the options)
1. Employed
2. Employed, but currently in maternity leave
3. Unemployed
4. Working at home
5. Seasonal employee or farm worker
6. Student
7. Other ________________________
70. What is father's current occupational status?
(Read the options)
1. Employed
2. Unemployed
3. Working at home
4. Seasonal employee or farm worker
5. Migratory worker
6. Student
7. Other ________________________
71. How many people live in your house including
you?
_________
72. How many children under age of 18 live in your
house?
_________
73. How is your house mainly heated? 1. _____________________(specify)
2. Not heated
74. In average, how much money does your family
spend?
1. Less than 25 000 AMD
2. 25 000-50 000 AMD
3. 50 001- 100 000 AMD
4. 100 001-200 000 AMD
5. 200 001-300 000 AMD
6. More than 300 000 AMD
7. Don't know
75. How many people are employed in your family
(including you and those, who works at home,
who are farm workers or seasonal and
migratory workers)
_________

60
Appendix 4. Informed Consent Form
American University of Armenia
School of Public Health
Institutional Review Board #1
Determinants of Iron Deficiency Anemia among Hospitalized Children Aged 6-59 Months in Armenia
Consent form
Hello, my name is Anush. I am a physician and graduate student of the Master of Public Health program at the
American University of Armenia. We are conducting a study to investigate determinants of iron deficiency
anemia among children 6-59 months of age in Armenia. The research is conducted among children who were
hospitalized in Arabkir Medical Center or in Muratsan University Hospital during January 1 2015 to April 8
2016. We obtained permission from the administration of these hospitals to obtain access to your contact
information from medical record. I have contacted you as you are one of the 345 mothers/care givers of
children who were hospitalized in mentioned hospitals during January 1 2015 to April 8 2016.. I would like to
ask you to participate in this study to share with us some additional details, mainly about child care and dietary
habits.
Your participation in this study is voluntary. There will be no consequences if you refuse to participate in this
study. Your participation will limited by 15-20 minutes telephone interview. You can skip any questions you
do not want to answer and stop the interview at any time.
Your participation in the study poses no risk for you and your child, as well as will not affect on future
provision of any type of health care services to your child. There is no direct benefit from the participation in
this study, but your participation will contribute to better understanding the risk factors iron deficiency anemia
among children, which later could lead to improved management and better prevention of iron deficiency
anemia in Armenia. The information provided by you and the data obtained from the medical records are fully
confidential and will be used only for the study. Only the general findings will be presented in the final report.
Your and your child’s personal and contact information will not appear anywhere. All your and child’s
identifiable information will be destroyed upon the completion of data collection.
If you have any questions about this study you can call to the study investigator Dr. Anahit Demirchyan, (374
60) 61 25 62 . If you feel you have not been treated fairly or think you have been hurt by joining the study you
should contact the primary member of Institutional Review Board of the American University of Armenia Dr.
Varduhi Petrosyan, (37460) 61 25 92.
Do you agree to participate? Thank you.

61
Հայաստանի Ամերիկյան Համալսարան
Հանրային առողջապահության բաժին
Գիտահետազոտական էթիկայի թիվ 1 հանձնաժողով
Հայաստանում երկաթ դեֆիցիտային անեմիայի որոշիչ գործոնները 6-59 ամսական
հոսպիտալացված երեխաների շրջանում
Իրազեկ համաձայնության ձև
Բարև Ձեզ, իմ անունն Անուշ է։ Ես բժիշկ եմ և Հայաստանի Ամերիկյան Համալսարանի Հանրային
առողջապահության բաժնի ավարտական կուրսի ուսանող: Մենք իրականացնում ենք հետազոտություն,
որի նպատակն է բացահայտել Հայաստանում երկաթի պակասով պայմանավորված սակավարյունության
որոշիչ գործոնները 6-59 ամսական երեխաների մոտ: Հետազոտությունն իրականացվում է այն երեխաների
շրջանում, ովքեր հոսպիտալացվել են Արաբկիր բժշկական համալիրում կամ Մուրացան
համալսարանական հիվանդանոցում 2015 թ-ի հունվարի 1-ից մինչև 2016 թ-ի ապրիլի 8-ը: Ձեր
հեռախոսահամարը վերցվել է Արաբկիր բժշկական համալիրի/Մուրացան համալսարանական
հիվանդանոցի բժշկական քարտից: Ես զանգահարել եմ Ձեզ, քանի որ դուք հանդիսանում եք 345
երեխաներից մեկի մայրը/խնամակալը, որոնք հոսպիտալացվել են նշված հիվանդանոցներում 2015 թ-ի
հունվարի 1-ից մինչև 2016 թ-ի ապրիլի 8-ը: Ես կխնդրեի Ձեզ մասնակցել այս հետազոտությանը, որպեսզի
ստանամ մի քանի լրացուցիչ տվյալ Ձեր երեխայի մասին, մասնավորապես` երեխայի խնամքի և
սննդակարգի վերաբերյալ։
Ձեր մասնակցությունն այս հետազոտությանը կամավոր է: Մասնակցությունից հրաժարվելը չի
ունենա որևէ հետևանք Ձեզ համար։ Ձեր մասնակցությունը սահմանափակվում է 15-20 րոպե տևողությամբ
հեռախոսային հարցազրույցով: Դուք կարող եք չպատասխանել ցանկացած հարցի, եթե չեք ցանկանում,
կամ ցանկացած պահի ընդհատել հարցազրույցը:
Ձեր մասնակցությունն այս հետազոտությանը որևէ վտանգ չի ներկայացնում Ձեզ և Ձեր երեխայի
համար, ինչպես նաև չի խոչընդոտի հետագայում բժշկական ծառայություններից օգտվելուն։ Այս
հարցազրույցին Ձեր մասնակցությունը չի ենթադրում որևէ ուղղակի շահ Ձեզ համար, բայց այն կարող է
օգնել ավելի լավ հասկանալու երեխաների շրջանում երկաթի պակասով պայմանավորված
սակավարյունության ռիսկի գործոնները, որը հետագայում կարող է նպաստել Հայաստանում արդյունվետ
ծրագրերի իրականցմանն ու այս տիպի սակավարյունության կանխարգելմանը։ Ձեր տրամադրած
տվյալները, ինչպես նաև բժշկական քարտից վերցված տվյալները գաղտնի են պահվելու և օգտագործվելու
են միայն հետազոտության նպատակով: Վերջնական զեկույցում կներկայացվեն միայն ընդհանուր
տվյալներ։ Ձեր և երեխայի որևէ անձնական և կոնտակտային տվյալ (անուն, հասցե և այլն) որևէ տեղ չեն
ներկայացվելու: Ձեր և երեխայի անձը բացահայտող բոլոր տվյալները ոչնչացվելու են տվյալների
հավաքագրումից անմիջապես հետո:
Այս հետազոտության վերաբերյալ հարցեր ունենալու դեպքում կարող եք կապ
հաստատել հետազոտության համակարգողի` Անահիտ Դեմիրճյանի հետ հետեւյալ հեռախոսահամարով`
060 61 25 62: Եթե Դուք կարծում եք, որ այս հետազոտությանը մասնակցելու ընթացքում Ձեզ լավ չեն
վերաբերվել, կամ մասնակցությունը Ձեզ վնաս է պատճառել, կարող եք զանգահարել Հայաստանի
ամերիկյան համալսարանի գիտական էթիկայի հանձնաժողովի ներկայացուցիչ՝ Վարդուհի
Պետրոսյանին հետեւյալ հեռախոսահամարով` 060 61 25 92 ։
Համաձա՞յն եք մասնակցել: Շնորհակալություն:





























