Embed Size (px)
Citation preview

Xiaomei Lu
Spring 2019
Master thesis 1, 15 ECTS
Master’s in Economics
Determinants of health care
expenditure in Sweden
Xiaomei Lu

Abstract
Sweden faces increasing pressures on health funding. Total expenditure on health
care currently accounts for about 10.92% of GDP, which suggests an increase of about
twofold over the last five decades. This paper examines the short-run and long-run
relationship between income and health care expenditure in Sweden during the period
1980–2017. The study focused on the differences between short- and long-term
elasticities. Consistent with the conventional findings, the income elasticity for health
care is found to be greater than one, suggesting that health care is a luxury good in
Sweden. Additionally, the age structure variable is found to have a significant positive
impact on health care expenditure. Finally, the importance of another non-income
variable, relative price, is also confirmed, an increase in relative price is associated with
lower quantity of health care expenditure.

Table of content
Ⅰ. Introduction ................................................................................................................ 1
Ⅱ. Theoretical bases ....................................................................................................... 3
Ⅲ. Data and analytical framework .................................................................................4
Ⅳ. Econometric methodology and results..................................................................... 5
Ⅳ.Ⅰ Unit root and stationarity tests.......................................................................…. 5
Ⅳ.Ⅱ Co-integration test ..............................................................................................6
Ⅳ.Ⅲ Error Correction Model ......................................................................................7
Ⅴ. Summary and conclusions ........................................................................................9
Acknowledgement........................................................................................................10
References....................................................................................................................11
Appendix......................................................................................................................13
List of tables
Table 1. Unit root test .....................................................................................................6
Table 2.OLS regression on lnqt.......................................................................................6
Table 3. Estimation results, error correction models ......................................................8
Graph The change trend of quantity of total health care expenditure, per capital GDP,
relative price and percentage of population above 65years old during 1980-2017 in
Sweden ...........................................................................................................................5

1
Ⅰ Introduction
The objective of this article is to examine the short- and long-run effects of income
and prices of health care expenditure in Sweden, using 1980-2017 annual time-series
data.
A series of studies1 have focused on using cross-sectional data and panel data to
investigate the relationship between the health care expenditure and the determinants
across countries. These studies differ in terms of the time period covered, determinates
selected, country chosen and econometric techniques employed in the estimation.
Obviously, these studies provide meaningful and useful guide to understand the reason
why health care expenditure varies significantly across countries, but on the other hand,
they cannot be generalized to individual country since the aggregate level empirical
analyses are less able to capture the complexity and peculiarity of the economic
environments of each individual country. Hence, any inferences derived from these
studies can only provide a general understanding of the broad relationship between
these variables.
In this spirit, country-specific case studies may give more exact description on how
income and prices affect health care expenditure in the studied countries. Gbesemete
and Gerdtham (1992); Ang (2010); Seshamani and Gray (2004); Murthy and Okunade
(2016) and Morgan, Gmeinder and Wilkens (2017) examine the evolution and
determinants of health care expenditure in specific country by using systematic time-
series data. To some extent, the main finding of these studies offers guidance and
constructive suggestions for policy formulation in the country-specific studied.
The literature about the relationship between health spending and GDP have been
popularized by the early work of professor Joseph Newhouse (1997). He inferred that
over 90 percent of the sample variation between countries in HE could be explained by
variations in per capita GDP, with an income elasticity in the range 1.15 to 1.31.
Subsequently, other economists have been attracted to the study of international
comparisons of health expenditure and empirical studies2 have supported the hypothesis
that there is strong positive relationship between per capita health spending and per
capita GDP.
1.see e.g. Newhouse (1977), Hitiris (1997), Cuyler (1989), Gerdtham and Löthgren
(2000), Gerdtam and Jönsson (1991), Gerdtham and Johannesson (1999), Hitiris and
Posnett (1992), Lago-Peñas, Cantarero-Prieto, and Blázquez-Fernández (2013),
Mladenović et al (2016), Narayan, Narayan, and Mishra (2010), Braendle and
Colombier (2016), Lorenzoni and Koechlin (2017),etc. 2. see e.g. Gerdtham and Jönsson (1991), Milne and Molana (1991), Hitiris (1997),
Cuyler (1989), Gerdtham and Löthgren (2000), Lorenzoni and Koechlin(2017),
Baltagi and Moscone (2010), Blomqvist and Carter (1996), etc.

2
Other than the GDP per capita, economists are also interested in the non-income
determinants of health care expenditure. A group of studies3have found that the age
structure of the population (usually measured by the percentage of population over age
65) are significantly associated with health care expenditure.
In addition to GDP and the age structure of the population, the relative price of health
care can also be viewed as an determinant that affect the demand of health care.4 In the
literature, Lorenzoni and Koechlin (2017) argued that “health-specific price levels play
an important role in explaining differences in per capita health care volumes across
countries. Hospital price levels for 2014 are for the first time available for all OECD
countries (http://stats.oecd.org/Index.aspx?DataSetCode=PPP2014).” Considering
relative price of health care is related to the quantity of health care funding, such non-
income variable may also be treated indirectly as determinants of health care.
As mentioned above the aim of this article is to examine the short- and long-run
relationship between the health care expenditure and its determinants in Sweden by
using 1980-2017 annual time-series data. In studying the relationship between the
quantity of health care expenditure (qt), the real income(GDP per capita/consumer price
index) (yt) , the relative price (pt) of health care and demographics (OLDt), defined as
the percentage of the population 65 years old and older, this study applied unit root test
and co-integration theory to analyze the econometric relationship between time series
and then adopt the error correction model to unravel the short and long-run relationship
among the variables.
The study’s objective was achieved in three steps. Firstly, non-stationarity of each
observed time-series was tested by using the standard approaches which are to estimate
augmented Dickey–Fuller ADF regression (ADF test) and Phillips–Perron test(PP), and
then ascertain the order of integration of the data series. Secondly, by applying Engle-
Granger two-step method, results were obtained regarding the existence of long-run
cointegration relationships between the variables in the data. Thirdly, the short and
long-run elasticities of real income (yt) and relative price (pt) were estimated by
adopting an Error Correction Model (ECM).
Briefly foreshadowing the main conclusions, the present study finds that the quantity
of health care expenditure(qt), the real income (yt), the relative price (pt) of health care
and demographics (OLDt) are integrated of order one and are cointegrated in the Engle-
Granger cointegration test. The long-run results reveal that while real income (yt) and
demographics (OLDt) have a positive and statistically significant effect on the quantity
of health care (qt), relative price (pt) is also statistically significant but with a negative
effect as expected. More specifically, the current study finds that the short-run elasticity
of quantity of health care with respect to real income is below one, around 0.81-0.88,
while the long-run elasticity is above one, in the range of 1.42-1.64, which suggest that
health care in long-run is a luxury good in Sweden.
3see e.g. Hitiris and Posnett (1992), Lago-Peñas, Cantarero-Prieto, and Blázquez-
Fernández(2013), Ang (2010), Braendle and Colombier (2016).
4see Milne and Molana(1991), Leu (1986), Gerdtham and Jönsson (1991b), Gerdtham
and Jönsson (1991a) .

3
This paper is most closely related to Ang (2010) who studied the determinants of
health care expenditure using Australian data from 1960 to 2003 and found that the
determinants, including real income, demographic structure (both percentage of
population above 65years old and below 15years old), density of health care services
and public finance on health care expenditure, impose an a significant positive influence
on health care expenditure. Specifically, pointing out the long-run elasticities of health
care expenditure with respect to real income are found to be in the range of 1.207–1.252
implying that health care is luxury good in Australia. The present paper contributes by
introducing in the relative price which is assumed to have an impact on the quantity of
health care, and using relatively new Swedish data.
The rest of this article is organized as follows: Section II analyses the theories on
which this paper is based. In section III, the data and analytical framework for
modelling was described. In section Ⅳ the econometric techniques employed in this
study are described, and also the results are presented and analyzed. The last section
summarizes and concludes.
Ⅱ Theoretical bases
The paper is based on a few fundamental economic theories.
The theory of consumer demand is applicable for explaining the relationship between
the health care expenditure and real income, also the relative price of health care. The
income effect is a phenomenon observed through changes in purchasing power,
revealing the change in quantity demanded brought by a change in real income. In
general, the relationship between income and quantity demanded is positive, while
classic economics predicts that quantity demanded decreases with increasing price.
As we know, normal goods are those goods for which the demand rises as income
rises, while inferior goods are goods whose demand decreases as consumer income
rises (or demand increases when consumer income decreases). (Jurion, B.J. 1978)
Obviously, health care appears to be a normal good. On the other hand, a luxury good is
a good for which demand increases by a greater proportion than income. (Varian,
Hal 1992) In contrast, a necessary good is a good for which demand increases by a
smaller proportion than income. For the long-run elasticity is found to be above one, in
the range of 1.41-1.64, which suggests that health care in long-run is a luxury good in
Sweden.
For most goods, elasticities are often lower in the short run than in the long run.
Changes that just are not possible to make in a short amount of time are realistic over
a longer time. In the short-run, the health care expenditure is lagging behind GDP
growth. Adjustments for demanding and supplying need a certain period of time to be
realistic. For instance, the increase in health care centers, medical personnel and
hospital beds etc. takes time to adjust after observing the increasing in the economic
growth.

4
Ⅲ Data and analytical framework
In the previous health economics studies, per capita GDP, the proportion of
population under 15 and/or over 65 have been identified as the key determinants of
health care expenditure. Other than these two determinants, this study introduces the
relative price of health care into the analytical framework, since economic theory
predict that the relative price of a good should affect the quantity for a normal good.
The formulation of the empirical specification of the health care demand equation
was given in Equation 1.
lnqt=ƒ(lnyt, lnpt, OLDt) (1)
where qt is the ratio of total health care expenditure per capital to the producer price
index PPI(2015=100) of medical and dental instruments and supplies; yt is the ratio of
per capital GDP to the consumer price index CPI(1980=100); pt is the producer price
index (2015=100) of medical and dental instruments and supplies divided by the
consumer price index CPI; and OLDt is the percentage of population aged over 65.
All variables (other than OLDt) are expressed in natural logarithms for the usual
statistical reasons. The reason for using producer price index (2015=100) of medical
and dental instruments and supplies instead of the consumer price index of medical care
to derive the relative price is that the household out-of-pocket payment of the total
health care expenditure account for a small proportion, around 15%. However, up to
56% of the total health care expenditure in Sweden is funded by the county councils
and enterprises owned by the county councils and about 25% is funded by
municipalities. In such particular circumstance, the consumer price index does not fully
reveal the relative price trend of the health care, but the producer price index is an
appropriate alternative choice. Annual data covering the period 1980–2017 in Sweden
were used in the estimation. All data were gathered from OECD Health Data (2018)
and SCB, (except that the PPI during the period 1980-1990 is estimated on CPI 1980-
1990 through OLS regression, because of the lack of data resource for it, as explained
in the appendix.)
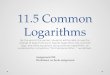
A graph of the changing trend of quantity of the total health care expenditure (lnqt),
per capital GDP (lnyt), the relative price (lnpt) and the percentage of population above
65years old (OLDt) is presented as follow. In general, the growth rate of quantity of the
total health care expenditure (lnqt) and per capital GDP (lnyt) is similar as predicted,
while the relative price (lnpt) and the percentage of population above 65years old (OLDt)
appears comparatively constant.

5
Ⅳ Econometric Methodology and results
Ⅳ. Ⅰunit root and stationarity tests
Before adopting any time series model, stationary tests for all variables are necessary
in order to detect and avoid spurious regressions. A unit root test is used to study if a
time series variable is non-stationary and possesses a unit root. In general, there are
several tests for it, including augmented Dickey–Fuller test(ADF), Phillips–Perron test,
KPSS test, ADF-GLS test. In this article, augmented Dickey–Fuller test(ADF) and
Phillips–Perron test(PP), which are the most common unit root test, were used to test
the stationarity of the time series. With this aim, ADF test and PP test for lnqt, lnyt, lnpt
and OLDt have been carried out. A summary of results is reported in Table 1. The null
hypothesis (H0) that the tested series has a unit root is accepted in the level of all series
which indicates that lnqt, lnyt, lnpt and OLDt are all non-stationary. This results are the
same as Gerdtham and Löthgren (2000) reported for health expenditure and GDP.
However according to both of ADF test and PP test, all series of lnqt, lnyt, lnpt and OLDt
are stationary process after first order difference. Hence all series may be treated as I(1).
-4
-2
0
2
4
6
1980 1985 1990 1995 2000 2005 2010 2015
lnqt lnyt
lnpt OLD1
The change trend of quantity of total health care expenditure, per capita GDP,
relative price and percentage of population above 65years old
during 1980-2017 in Sweden

6
Table1 unit root test
lnqt lnyt lnpt OLDt
test types(c t m) t-statistic t-statistic t-statistic t-statistic
ADF test
(0,0,0)
(c,0,0)
(c,t,0)
(0,0,1)
(c,0,1)
(c,t,1)
1.33
0.483
-1.99
-4.7***
-4.84***
-5.41***
1.32
0.39
-1.69
-3.33***
-3.59***
-4.19***
-1.39
-2.23
-2.88
-6.42***
-6.65***
-6.58***
0.72
-2.03
-3.68**
-3.14***
-3.23***
-4.24***
PP test
(0,0,0)
(c,0,0)
(c,t,0)
(0,0,1)
(c,0,1)
(c,t,1)
1.09
0.19
-1.99
-4.74***
-4.82***
-5.41***
1.30
0.51
-1.63
-3.24***
-3.59**
-4.22***
-1.23
-2.05
-2.80
-6.69***
-7.09***
-6.98***
1.89
-0.21
-0.99
-4.20***
-5.69***
-8.67***
Notes: For ADF, AIC was used to select the lag length and the maximum number of
lags was set to be nine. For PP, AR spectral-GLS detrend was used as the spectral
estimation method. *, ** and *** denote significance at the 10%, 5% and 1% levels,
respectively. For the test type (c,t,m) , c denotes with intercept, t with intercept and
trend, and m indicates lagged differences.
Ⅳ.Ⅱ Co-integration test
Since all series are stationary process after first order difference, there might exist
cointegration relationships between the variables. By applying the Engle-Granger two-
step method, results can be obtained regarding the existence of long-run cointegration
relationships between the variables in the data.
In the first step, OLS regression was conducted with lnqt as the explained variable
and lnyt, lnpt and OLDt as the explanatory variables. The regression result is
presented as follow (Table2):
Table 2 OLS regression on lnqt
Variable Coefficient Std. Error t-Statistic Prob.
C -6.14 0.65 -9.396 0.0000lnyt 1.42 0.082 17.22 0.0000lnpt -1.23 0.36 -3.41 0.0017
OLDt 7.72 2.18 3.55 0.0012
R-squared 0.958 Mean dependent var 3.468Adjusted R-squared 0.955 S.D. dependent var 0.304S.E. of regression 0.064 Akaike info criterion -2.54Sum squared resid 0.142 Schwarz criterion -2.367Log likelihood 52.25 Hannan-Quinn criter. -2.478F-statistic 261.64 Durbin-Watson stat 0.73Prob(F-statistic) 0.000000

7
In the second step, the residual series is made out from the OLS regression above
and then conducted the ADF test for the residual series generated. The t-statistic value
of the residual series in the ADF test is -2.86, less than the critical value of the 1%
significance level, -2.63. Therefore, it can be considered that the residual error series
is stationary, indicating the existence of long-run cointegration relationships between
the variables in the data.
Ⅳ.Ⅲ Error Correction Model
Since the residual of the OLS regression is considered to be stationary in the
cointegration analysis, which indicates the existence of long-run cointegration
relationships between the variables. The error correction model (ECM) can be adopted
to estimate the long-run equilibrium relationship between quantity of health care
expenditure and its determinants. By applying the ECM, the short-run dynamic
adjustment has also been revealed, which are critical in any time-series investigation.
The effects of the determinants of health care expenditure are often different in the short
and long run.
Below the error correction model (ECM) was set out, by just formulating one
equation Δlnqt=α0+α1Δlnyt+α2Δlnpt+α3ΔOLDt+λlnqt-1+β1lnyt-1+β2lnpt-1+β3OLDt-1+еt
(referred as model A) and by using Engle-Granger two-step approach (referred as
model B), respectively.
In model A, the short-run elasticities of all the determinants can be obtained
directly from the estimated result, including the real income elasticity, the price
elasticity and demographic semi-elasticity. The corresponding long-run elasticities
can be derived indirectly by adopting βK/-λ, for k=1,2,3. When applying this model,
the error correction term is not necessary to be generated during the regression
process.
On the other hand, while adopting model B, it is necessary to obtain the error
correction term first, by regressing the long-run steady-state model in the first step
and making residuals out of it. The long-run elasticities are obtained directly during
first step. While in the second step, by bringing in the error correction term, error
correction model (ECM) is set out and short-run elasticities can be obtained.
Firstly, the following long-run steady-state solution is obtained in the co-
integration test. lnqt=-6.14+1.42 lnyt-1.23 lnpt+7.72 OLDt (refer to Table 2)
Next, the Error-Correction Term (ECT) can be obtained by taking lnqt-1-a0–b1lnyt-1
- b2lnpt-1 +b3OLDt-1 to formulate the error correction model (ECM) as shown in
Equation Δlnqt=δ1Δlnyt+δ2Δlnpt+δ3ΔOLDt-μ(ecm t-1)+еt .Where ecmt-1 = lnqt-1-a0–
b1lnyt-1 - b2lnpt-1 +b3OLDt-1. The ECT captures the health care expenditure evolution
process by which agents adjust for prediction errors made in the last period. The
stationarity of the ECT provides evidence that the long-run relationship exists.
Slightly different results are acquired from the two models. The results are
presented in Table 3. But in general, all long-run effects are significant at the
conventional levels and have the expected signs and reasonable magnitudes.

8
Table 3 Estimation results, error correction models
Model A
Model B
(Engle-Granger two-step approach)
Variable parameter coefficient Std.error Prob. parameter coefficient Std.error Prob.
Panel 1 the long-run equilibrium level relationship
c
lnyt
lnpt
OLDt
β1 /-λ
β2 /-λ
β3 /-λ
1.64
-3.07
12.79
0.31
1.68
6.97
0.000
0.068
0.067
a0
b1
b2
b3
-6.14
1.42
-1.23
7.72
0.65
0.08
0.36
2.18
0.000
0.000
0.001
0.001
Panel 2 the short-run relationship
c
Δlnyt
Δlnpt
ΔOLDt
lnqt-1
lnyt-1
lnpt-1
OLDt-1
ecmt-1
α0
α1
α2
α3
λ
β1
β2
β3
-2.81
0.81
-1.34
-2.91
-0.27
0.45
-0.84
3.49
1.02
0.24
0.34
8.4
0.13
0.19
0.38
1.98
0.009
0.001
0.0004
0.731
0.045
0.029
0.038
0.089
δ1
δ2
δ3
μ
0.88
-1.01
7.58
-0.303
0.21
0.25
4.46
0.126
0.000
0.000
0.099
0.021
Model A
Model B(1-step)
Model B(2-step)
R-squared
0.62
0.958
0.58
Adjusted R-squared
0.52
0.955
0.54
F-statistic
6.66
261.64
Prob(F-statistic)
0.000
0.000
S.E of regression
0.046
0.06
0.045
(1) The regression results for model A, reported in panel 2 of Table 3, provide the
short-run dynamic changes pattern. Other than the demographic variable (OLDt) which
indicates no short-run inference can be made about this variable, all other coefficients
are statistically significant at the 5% level. In the first differenced form, real income(lnyt)
and relative price (lnpt), appear to be statistically significant at the 1% level, and
therefore short-run inference can be made. The short-run income elasticity is 0.81,
indicating when per capital GDP grows 1%, the quantity of health care will increase by
0.81% in the current year. The short-run price elasticity has the expected negative sign
and implies that an increase in relative price of health care by 1% will decrease the
quantity consumed by 1.34%.
The coefficient on lnyt-1 is about 0.45, indicating the quantity of health care in the
previous year increasing by 1% will lead to the quantity in current year rising by
0.45% .The possible explanation is that the fixed assets and personnel investment
proposed in the previous year in health care have a stimulating effect on the health care
expenditure in the following period of time.
The long-run elasticity of quantity of health care with respect to per capita GDP is
around 1.64 with standard error 0.31, suggesting that the real income long-run elasticity
is above 1. The result implies that health care in long-run is a luxury good in Sweden.

9
Such a finding is consistent with a number of previous studies, including Newhouse
(1977), Leu (1986), Gerdtham and Jönsson (1991), Milne and Molana (1991), Hitiris
(1997) and Ang (2010). The long-run price elasticity is around -3.07 with standard error
1.68. This point estimated is below that reported by Gerdtham and Jönsson (1991),
Marc Pomp and Sunčica Vujić(2008), in which the relative price elasticities are between
minus one and zero. However due to the large standard error, the 95% confidence
interval range from -6.43 to -0.29, and therefore do not contradict that the true effect is
between minus one and zero. The possible explanation is that the use of predicted prices
for some years resulting in the large standard error. And the use of different approaches
to derive the relative price of the health care could be another reason.
(2) Engle-Granger two-step approach (model B)
The regression results for model B are presented in table 3.
The coefficients on ecmt-1 is -0.303, which measure the speed at which adjustment
returns to the long-run equilibrium value, is statistically significant at the 1% level
with the expected negative sign. This indicates that the quantity of health care adjusts
at the speed of 30.3% every year to restore equilibrium when there is a shock to the
steady-state relationship.
While the estimated short-run income elasticity δ1 is around 0.88, the long-run
elasticity is 1.42 with standard error 0.08. This result also suggests that health care in
long-run is a luxury good in Sweden. And while the estimated short-run price elasticity
δ2 is around -1.01, the long-run elasticity is -1.23 with standard error 0.36. The
magnitudes of the coefficients for relative price are slightly different from that obtained
in model A, and closer to that found in previous studies.
The coefficient on OLDt is found to be around 7.58 with the expected (positive)
sign and statistically significant at the 1% level. The result suggests that the quantity
of health care expenditure rises significantly with the increase in elderly population
(over 65) relative to total population, which is expected. To this extent, the results
support the view that demographic factors are crucial in explaining the variations in
health care expenditure, as reported by the previous studies of Gerdtham and Jönsson
(1991a),Hitiris( 1997) ,Gerdtham et al. (1992) and Murthy and Ukpolo (1994)
Ⅴ Summary and conclusions
Sweden faces increasing pressures on health funding. Total expenditure on health
care currently accounts for about 10.92% of GDP in Sweden, suggesting an increase of
about twofold over the last five decades. It is crucial to examine the underlying causes
of this increase and provide some fundamental guidelines for health policy designing.
This paper investigated the short and long-run economic relationship between
quantity of health care and its determinants, including per capital GDP, relative price
and age structure (the percentage of population above 65years old). Using a time-series
data of Sweden followed about 39 years, this paper has studied the non-stationarity and
cointegration properties of all the series. The analysis indicates that health care
expenditure and the three determinants studied are non-stationary, but there exists long-

10
run cointegration between the variables. Our results show that there exists strong
positive relationship between quantity of health care and per capita GDP as reported in
previous studies, and also indicate that health care in long-run is a luxury good in
Sweden, with a long-run income elasticity greater than one, consistent with the previous
studies Newhouse(1977). As for non-income determinants, our analysis indicates the
percentage of population above 65yeas old plays a quite important role in explaining
health expenditure variations as previous studies implied. And finally, from the results
obtained, relative price is also an important determinant of the demand for health care
since its coefficient is significant at 1% level in both models.
Several limitations of this study need to be acknowledged. One limitation concerns
the fact that there may be some omitted variables which affect the demand for health.
This could lead to omitted variables bias. Another limitation concerns issues of data.
Because of lacking for relative price from 1980 to 1990, it had to be imputed. On the
other hand, future studies on health care expenditure growth may further expand the
study by empirically test different variables and related health indexes with GDP. And
it may be worthwhile to try using longer time series to study if the elasticities have
changed over time.
Acknowledgement
In the acknowledgement of this thesis, I would like to thank different people who
directly or indirectly contributed to my thesis via their time, efforts, knowledge,
expertise. Particularly I would like to thank my supervisor, David Granlund, for his
efforts, support and guidance. David has provided his feedback and supervision
throughout the research work in a professional manner. His criticism and suggestions
were always constructive as far as the improvements in the thesis were concerned. I
also would like to thank those who supported me throughout the process.

11
References
Newhouse P. Joseph (1977), Medical-Care Expenditure: A Cross-National Survey, The
Journal of Human Resources, Vol. 12, No. 1 (Winter, 1977), pp. 115-125
Gerdtham ULF -G, Jes Sørgaard, Fredrik Andersson, and Bengt Jönsson (1991) , An
econometric analysis of health care expenditure: A cross-section study of the
OECD countries. Journal of Health Economics I1 (1992) 63-84 North-Holland
Gerdtham ULF -G and Bengt Jonsson (1991), Price and quantity in international
comparisons of health care expenditure. Applied Economics, 1991, 23, 1519-1528
Gerdtham ULF -G and Jonssön Bengt (1991), Conversion factor instability in
international comparisons of health care expenditure. Journal of Health Economics 10
(1991) 227-234. North-Holland
Gerdtham ULF -G and Johannesson Magnus (1997), New estimates of the demand for
health: results based on a categorical health measure and Swedish micro data.
Working Paper Series in Economics and Finance No. 205 November 1997
Gerdtham. Ulf-G and Löthgren Mickael (2000), On stationarity and cointegration of
international health expenditure and GDP, Journal of Health Economics 19 2000 461–
475
Lago-Peñas, Cantarero-Prieto, Blázquez-Fernández (2013) On the relationship
between GDP and health care expenditure: A new look. Economic Modelling 32 (2013)
124–129
Morgan David, Gmeinder Michael and Wilkens Jens (2017) An OECD analysis of
health spending in Norway. OECD Health Working Papers No. 91
Culyer, A.J (1989), Cost Containment in Europe. Health Care Financ Rev. 1989 Dec;
1989(Suppl): 21–32.
Gbesemete Kwamep and Gerdtham Ulf-G (1992), Determinants of Health Care
Expenditure in Africa: A Cross-Sectional Study. World Development Vol. 20. No. 2. pp.
303-30X. 1992 .
Murthy N.R. Vasudeva, Okunade A. Albert (2016), Determinants of U.S. health
expenditure: Evidence from autoregressive distributed lag (ARDL) approach to
cointegration. Economic Modelling 59 (2016) 67–73
Baltagi H. Badi and Moscone Francesco (2010) Health care expenditure and income
in the OECD reconsidered: Evidence from panel data. Economic Modelling 27 (2010)
804–811
Ellis P. Randall, Martins Bruno and Zhu Wenjia (2017), Health care demand
elasticities by type of service. Journal of Health Economics 55 (2017) 232–243
Hitiris. Theo (1997), Health care expenditure and integration in the countries of the
European Union, Applied Economics, 29:1, 1-6, DOI: 10.1080/000368497327335
Hitiris. Theo and Posnett John (1992), The determinants and effects of health
expenditure in developed countries, Journal of Health Economics 11 (1992) 173-18 1.
North-Holland

12
Getzen E. Thomas (2000), Health care is an individual necessity and a national
luxury: applying multilevel decision models to the analysis of health care
expenditures.Journal of Health Economics 19 2000 259–270
Mladenović Igor, Miloš, Milovančević, Svetlana Sokolov Mladenović , Vladislav
Marjanović, Petković (2016) Analyzing and management of health care expenditure
and gross domestic product (GDP) growth rate by adaptive neuro-fuzzy technique,
Computers in Human Behavior 64 (2016) 524e530
Lorenzoni Luca, Koechlin Francette (2017) , International Comparisons of Health
Prices and Volumes: New Findings, OECD Directorate for Employment, Labour and
Social Affairs.
Blomqvist, Å.G and Carter. R.A.L (1997), Is health care really a luxury? Journal of
Health Economics 16 (1997) 207-229
Abdul Azeez Oluwanisola Abdul Wahab and Zurina Kefeli (2016), Projecting a Long
Term Expenditure Growth in Healthcare Service: A Literature Review, Procedia
Economics and Finance 37 ( 2016 ) 152 – 157
Gerdtham.Ulf-G and Löthgren Mickael (2000), On stationarity and cointegration of
international health expenditure and GDP, Journal of Health Economics 19 2000 461–
475
Schieber J. George and Poullier Jean-Pierre (1989), Overview of international
comparisons of health care expenditures, Health Care Financ Rev. 1989 Dec;
1989(Suppl): 1–7.
Leu, R. E. (1986) The public–private mix and international health care costs, in Public
and Private Health Services (Eds) A. J. Culyer and B. Jonsson, Basil Blackwell,
Oxford, pp. 41–63.
Murthy N. R. Vasudeva & Ukpolo Victor(1994), Aggregate health care expenditure in
the United States: evidence from cointegration tests. Applied Economics Volume 26,
1994-Issue 8
Milne R and Molana H (1991), On the effect of income and relative price on demand
for health care: EC evidence. Applied Economics (1991) 23(7) 1221-1226
Seshamani Meena and Gray Alastair (2004), Ageing and health‐care expenditure: the
red herring argument revisited. Health Economics Volume13, Issue4 April 2004 Pages 303-
314
Ang B James (2010), The determinants of health care expenditure in Australia, Applied
Economics Letters, 17: 7, 639 — 644, First published on: 01 June 2009 (iFirst)
Braendle Thomas and Colombier Carsten (2016), What drives public health care
expenditure growth? Evidence from Swiss cantons, 1970–2012, Health Policy 120
(2016) 1051–1060
Wang Kuan-Min (2011), Health care expenditure and economic growth: Quantile
panel-type analysis, Economic Modelling 28 (2011) 1536–1549
Narayan Seema, Narayan Kumar Paresh and Mishra Sagarika (2010), Investigating
the relationship between health and economic growth: Empirical evidence from a
panel of 5 Asian countries, Journal of Asian Economics 21 (2010) 404–411

13
Liang Li-Lin and Mirelman J.Andrew (2014), Why do some countries spend more for
health? An assessment of sociopolitical determinants and international aid for
government health expenditures, Social Science & Medicine 114 (2014) 161e168
Duarte Fabian (2012), Price elasticity of expenditure across health care services,
Journal of Health Economics 31 (2012) 824–841
Zhou Zhongliang, Su Yanfang, Gao Jianmin, Xu Ling, Zhang Yaoguang (2011), New
estimates of elasticity of demand for healthcare in rural China, Health Policy 103
(2011) 255–265
Appendix
Data of the consumer price index and producer price index was collected from
SCB. While the CPI is presented from 1980 to 2017, the PPI only presented from
1990 to 2017. Considering that the PPI generally appears to have similar trend as CPI.
PPI in the period of 1980-1990 is predicted by using data of CPI.
Firstly, set out regression equation lnPPI=α+βlnCPI, following results were obtained.
lnPPI Coef. St.Err. t-value p-value [95% Conf Interval]
lnCPI 1.054 0.065 16.23 0.000 0.921 1.188
Constant -1.520 0.365 -4.17 0.000 -2.270 -0.770
Mean dependent var 4.403 SD dependent var 0.126
R-squared 0.910 Number of obs 28.000
F-test 263.561 Prob > F 0.000
Akaike crit. (AIC) -100.859 Bayesian crit. (BIC) -98.194
*** p<0.01, ** p<0.05, * p<0.1
Next, PPI was predicted by using the reported regression model. PPI during the period
of 1980-1990 is obtain then.
The data of total health care expenditure and GPD is collected from OECD health
care database.