Embed Size (px)
Citation preview

Detection of Myocardial Ischemia by Automated,Motion-Corrected, Color-Encoded Perfusion Maps Compared
With Visual Analysis of Adenosine Stress CardiovascularMagnetic Resonance Imaging at 3 T
A Pilot Study
Christina Doesch, MD,* Theano Papavassiliu, MD,* Henrik J. Michaely, MD,ÞUlrike I. Attenberger, MD,Þ Christopher Glielmi, PhD,þ Tim Suselbeck, MD,* Christian Fink, MD,Þ
Martin Borggrefe, MD,* and Stefan O. Schoenberg, MDÞ
Purpose: The purpose of this study was to compare automated, motion-corrected, color-encoded (AMC) perfusion maps with qualitative visual analysisof adenosine stress cardiovascular magnetic resonance imaging for detection offlow-limiting stenoses.Materials and Methods: Myocardial perfusion measurements applying thestandard adenosine stress imaging protocol and a saturation-recovery temporalgeneralized autocalibrating partially parallel acquisition (t-GRAPPA) turbo fastlow angle shot (Turbo FLASH) magnetic resonance imaging sequence were per-formed in 25 patients using a 3.0-T MAGNETOM Skyra (Siemens HealthcareSector, Erlangen, Germany). Perfusion studies were analyzed using AMC per-fusion maps and qualitative visual analysis. Angiographically detected coronaryartery (CA) stenoses greater than 75% or 50% or more with a myocardial per-fusion reserve index less than 1.5 were considered as hemodynamically relevant.Diagnostic performance and time requirement for both methods were compared.Interobserver and intraobserver reliability were also assessed.Results: A total of 29 CA stenoses were included in the analysis. Sensitivity,specificity, positive predictive value, negative predictive value, and accuracyfor detection of ischemia on a per-patient basis were comparable using theAMC perfusion maps compared to visual analysis. On a perYCA territorybasis, the attribution of an ischemia to the respective vessel was facilitatedusing the AMC perfusion maps. Interobserver and intraobserver reliabilitywere better for the AMC perfusion maps (concordance correlation coefficient,0.94 and 0.93, respectively) compared to visual analysis (concordance corre-lation coefficient, 0.73 and 0.79, respectively). In addition, in comparison tovisual analysis, the AMC perfusion maps were able to significantly reduceanalysis time from 7.7 (3.1) to 3.2 (1.9) minutes (P G 0.0001).Conclusions: The AMC perfusion maps yielded a diagnostic performance ona per-patient and on a perYCA territory basis comparable with the visualanalysis. Furthermore, this approach demonstrated higher interobserver andintraobserver reliability as well as a better time efficiency when compared tovisual analysis.
Key Words: cardiovascular magnetic resonance imaging, myocardialischemia, CA disease, AMC color-encoded perfusion maps
(Invest Radiol 2013;48: 678Y686)
F irst-pass perfusion cardiovascular magnetic resonance imaging(CMR) allows a noninvasive hemodynamic assessment with ex-
cellent results for the detection of coronary angiography (CA) disease(CAD) compared with conventional CA.1Y4
In clinical routine practice, qualitative visual analysis, viewingadenosine stress and rest perfusion images side by side, is the mostwidespread evaluation method. The combination of quantitative stress-rest perfusion and late gadolinium enhancement (LGE) enables detec-tion of CAD with a sensitivity of 89% and a specificity of 87%.5
However, the identification of perfusion deficits (PDs) using qualita-tive analysis is highly dependent on the observers and their experi-ence. Therefore, more objective evaluation methods using quantitative1,6
or semiquantitative7Y9 analysis have been investigated.Semiquantitative assessment determines the signal intensity-
time curves for stress and rest perfusion for each myocardial seg-ment and permits calculation of the myocardial perfusion reserveindex (MPRI). The MPRI analysis has demonstrated high accuracycompared to fractional flow reserve, determined by intracoronaryflow wire measurements,9 but has been shown to underestimate themyocardial blood flow compared to quantitative analysis.10 Quantita-tive analysis allows the absolute quantification of myocardial bloodflow in milliliter/gram/minute and the determination of the myocar-dial perfusion from the time-intensity curves of the myocardium arte-rial input function using deconvolution.6 However, because of theextensive required postprocessing, quantitative1,6 and semiquantitativeanalysis7Y9 are time-consuming; therefore, their use is mostly constrainedto clinical studies.
Retrospective respiratory triggering for motion correction oftime-resolved 2-dimensional perfusion measurements has recentlybeen described for the kidney.11 Now, a new postprocessing softwarehas become available, generating voxelwise color-encoded upslopevalues on the basis of motion-corrected data, accounting for motion orbreath-hold difficulty and requiring no user interaction. In contrast toprevious quantitative1,6 and semiquantitative analysis7Y9 approachescalculating the myocardial perfusion over groups of voxels within amyocardial segment, this approach enables, for the first time, the eval-uation of the myocardial blood flow within a single voxel with the po-tential for a more reliable quantification of the extent and the locationof the PD.
The aim of our pilot study was to compare these new auto-mated, motion-corrected, color-encoded (AMC) perfusion maps withvisual qualitative analysis of adenosine stress CMR in symptomaticpatients for the detection of flow-limiting stenoses.
ORIGINAL ARTICLE
678 www.investigativeradiology.com Investigative Radiology & Volume 48, Number 9, September 2013
Received for publication March 14, 2012; and accepted for publication, after re-vision, February 2, 2013.
From the *First Department of Medicine, and †Department of Clinical Radiologyand Nuclear Medicine, University Medical Center Mannheim, Medical FacultyMannheim, University of Heidelberg, Mannheim, Germany; and ‡SiemensHealthcare, Cardiovascular Magnetic Resonance Research and Development,Chicago, IL.
Conflicts of interest and sources of funding: none declared.Supplemental digital contents are available for this article. Direct URL citations
appear in the printed text and are provided in the HTML and PDF versions of thisarticle on the journal’s Web site (www.investigativeradiology.com).
Reprints: Christina Doesch, MD, First Department of Medicine, University MedicalCentre Mannheim, Medical Faculty Mannheim, University of Heidelberg, Theodor-Kutzer-Ufer 1Y3, 68167Mannheim, Germany. E-mail: [email protected].
Copyright * 2013 by Lippincott Williams & WilkinsISSN: 0020-9996/13/4809Y0678
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

MATERIALS AND METHODS
Study PopulationAfter institutional review board approval, 25 patients who
were referred for elective CA were prospectively recruited betweenJanuary 2011 and October 2011. Table 1 summarizes the baselineand clinical characteristics. Indication for referral was stable anginapectoris Canadian Cardiovascular Society classifications I to III.Exclusion criteria were standard CMR contraindications. Writteninformed consent was obtained from all patients.
Cardiovascular Magnetic Resonance ImagingThe patients underwent adenosine stress and rest perfusion
using a 3.0-T MAGNETOM Skyra (Siemens Healthcare Sector,Erlangen, Germany) with an 18-element body matrix coil. Duringimaging, the patients were instructed to hold their breath as long aspossible at the end of expiration.
For myocardial perfusion measurements, 3 short-axis slicesin the basal, midventricular, and apical location to cover the American
Heart Association segmental model (segments 1Y16) plus an additional4-chamber view (segment 17)12 were obtained.
Pharmacological stress administering 140 Kg/kg of body weight(BW) more than 4 to 5 minutes under electrocardiographic monitoringwas performed. After injection of 0.05-mmol/kg BW gadoterate meg-lumine (Dotarem, Guerbet, France) with a flow of 4 mL/s, perfusionimages were obtained by using a saturation-recovery temporal general-ized autocalibrating partially parallel acquisition (t-GRAPPA) turbo fastlow angle shot (Turbo FLASH) magnetic resonance imaging sequence(field of view, 350 mm � 350 mm; effective repetition time, 2.5 milli-seconds; acquisition time, 190.5 milliseconds; echo time, 1.04 millisec-onds; flip angle, 10 degrees; matrix, 192� 44; slice thickness, 7mm; andin-plane resolution, 1.8 � 2.4 � 7 mm) with an acceleration factor of3 acquiring 4 slices per heart cycle.
Ten minutes after the stress examination, a second bolus of0.05-mmol/kg BW gadoterate meglumine was injected with a flow of4 mL/s and the rest perfusion images were obtained with the sameorientation and position as those of the stress perfusion images.
Late Gadolinium EnhancementThen, another bolus of 0.1-mmol/kg BW gadoterate meglumine
was given and the LGE images were acquired 10 minutes after therest perfusion. An inversion time scout was performed to choose theoptimal inversion time between 200 and 360 milliseconds. The LGEimages were acquired using a phase-sensitive inversion recoverytrue fast imaging with steady state precession sequence13: field ofview, 290 mm� 260 mm; repetition time, 2.2 milliseconds; echo time,1.1 milliseconds; flip angle, 50 degrees; matrix, 140 � 192; slicethickness, 6 mm; and in-plane resolution, 1.4 � 1.9 � 6 mm.
Coronary AngiographyAll patients underwent coronary angiography, with imaging ac-
quired in multiple projections. If more than 1 CA stenosis was presentwithin the same perfusion territory, the most severe stenosis was used.14
Visual analysis estimation of stenosis severity, not quantitativecoronary angiography, was used to categorize CA stenoses as less than50%, 50% to 75%, or 75% or more. Significant disease was defined as50% or more stenosis of a CA or major branches or bypass. The extentof CAD (angiographic 1-, 2-, or 3-vessel disease) was quantified usingthe number of vessels with 50% or more stenosis. A CA stenosis withan angiographic lumen reduction of 75% or more was considered he-modynamically significant. In patients with angiographic stenoses ofintermediate severity (Q50% and G75%), the definition of the hemody-namic relevance was made on the basis of the MPRI determined byCMR. In these patients, an MPRI less than 1.5 was considered to beflow-limiting and, thus, hemodynamically relevant,9 whereas an MPRIof 1.5 or more was regarded as hemodynamically nonrelevant. The cor-onary angiograms were analyzed by the consensus of 2 board-certifiedcardiologists with more than 10 years of experience in interventionalcardiology who were unaware of the CMR results.
Image AnalysisFor the visual analysis of PDs, the images for stress and rest
perfusion were displayed side by side using the syngoARGUS Viewer,VD 11 (Siemens Healthcare Sector, Erlangen, Germany). An abnormalCMR study was defined by the presence of a PD during adenosineinfusion persisting more than 5 images beyond the initial peak en-hancement of the segment, which seemed almost normal. Myocardialischemia was defined as a segment with a PD only at stress and nohyperenhancement at LGE. In segments with LGE less than 75% sub-tended by CA stenosis 50% or more, a PD only at stress was relevantif it exceeded the preexisting LGE. A myocardial scar was defined asa segment with a hyperenhancement at LGE. Myocardial segmentswere assigned to the 3 coronary arterial territories in accordance with the17-segment segmentation model of the American Heart Association.12
TABLE 1. Baseline and Clinical Characteristics
All Patients(N = 25)
Age, mean (SD), y 68.3 (7.5)
Men, n (%) 21 (84)
Arrhythmia, n (%) 3 (12)
Asynchrony, n (%) 2 (8)
Angina, n (%)
CCS I 2 (8)
CCS II 18 (72)
CCS III 5 (20)
CCS IV 0
No significant CAD, n (%) 3 (12)
1-vessel disease, n (%) 5 (20)
2-vessel disease, n (%) 11 (44)
3-vessel disease, n (%) 6 (44)
Previous myocardial infarction, n (%) 11 (44)
Previous CABG, n (%) 3 (12)
Cardiovascular magnetic resonance parameters
LV function, mean (SD), % 52.3 (12.0)
LV end-diastolic volume, mean (SD), mL 155.4 (47.7)
LV end-systolic volume, mean (SD), mL 77.1 (43.2)
LV end-diastolic mass, mean (SD), g 152.2 (41.6)
LGE extent, mean (SD), % 14.9 (12.5)
LV end-diastolic mass, mean (SD), g 152.2 (41.6)
% LGE extent 14.9 (12.5)
Hemodynamic data
Duration of adenosine administration, min) 4.7 (0.4)
Heart rate (beats per minute)
At rest, mean (SD) 67.2 (9.2)
During adenosine stress, mean (SD) 93.3 (9.9)
Symptoms during peak adenosine stress, n (%)
Angina 9 (36)
Dyspnea 4 (16)
Discontinuation of adenosine due to adverse effects 0 (0)
CABG indicates coronary artery bypasss graft; CAD, coronary artery dis-ease; CCS, Canadian Cardiovascular Society classification; LGE, late gado-linium enhancement; LV, left ventricular.
Investigative Radiology & Volume 48, Number 9, September 2013 Detection of Myocardial Ischemia by AMC Perfusion Maps
* 2013 Lippincott Williams & Wilkins www.investigativeradiology.com 679
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

For the AMC perfusion maps, voxelwise upslope values areencoded using a color look-up table.15,16 Details about AMC imageregistration, motion correction, and processing of pixel-based dataare provided in Supplemental Appendix A1 (Supplemental DigitalContent 1, http://links.lww.com/RLI/A80). All processing steps in-cluding motion correction, noise suppression, and map generationare implemented in the Image Calculation Environment (SiemensHealthcare Sector, Erlangen, Germany) of the CMR scanner pro-viding automated data sets with no user interaction. The analysis ofthe AMC stress and rest perfusion maps was done offline on theMAGNETOM Skyra Multimodality Workplace (Siemens HealthcareSector, Erlangen, Germany). According to the color look-up table,dark blue to black color indicates myocardial segments with reducedupslope values during myocardial perfusion and was therefore de-fined as abnormal.
Analysis at random order on a per-patient basis and a per-CAterritory basis was performed by a consensus of 2 readers blinded tothe MPRI and CA results for the visual analysis and using the AMCperfusion maps.
The extent of the PD was graded with regard to its transmuralextent using the visual analysis and the AMC perfusion maps (0,normal perfusion; transmural extent: G25%, 1; 25Y50%, 2; 950%Y75%,3; and 975%, 4). As a global measure for the transmural PD, thetransmural perfusion deficit index (TPDI) was calculated as the sumof all segmental transmurality scores divided by 17.17
For the interobserver reproducibility of TPDI, 2 blindedreaders independently classified the extent of ischemia during thestress and rest perfusion using the AMC perfusion maps and the vi-sual analysis. One of them repeated the analysis 3 months later toassess the intraobserver reproducibility.
The manual MPRI analysis was performed by means of acommercially available dedicated software tool (Dynamic SignalAnalysis, Argus; Siemens Healthcare Sector). For each signalintensity-time curve, the foot point and the point of signal maximumwere determined by the software. Both data points (foot point andsignal maximum) were corrected interactively if necessary. The sig-nal intensity-time curve of the left ventricular (LV) cavity served asthe input function. The upslope values of all segments were dividedby the upslope value of the signal intensity-time curve that is auto-matically generated by the Argus software in the LV cavity. TheMPRI was calculated by dividing the upslope of the stress examinationnormalized to the upslope of the LV cavity by the correspondingsegment’s upslope value of the rest examination normalized to the up-slope of the LV cavity [MPRI: upslopestress corrected/upsloperest corrected].7
The manual semiquantitative MPRI analysis was performed by a thirdreader blinded to the results of the angiograms and the visual analysis.
To evaluate the influence of motion correction on the deter-mination of the myocardial perfusion, the MPRI and the stress-restTPDI were calculated for 10 randomly selected patients. These re-sults were then compared with those obtained using the nonYmotioncorrected data.
Analysis of LGEThe LGE images were analyzed visually, and bright segments
from subendocardial to epicardial were classified as fibrotic becauseof myocardial infarction.
Image QualityTo determine image quality, the readers reviewed the images
for the nonYcorrected stress and rest perfusion and LGE using a 5-point grading scale, with 1 as nondiagnostic; 2, severely impaired(severe artifacts, severe signal inhomogeneity); 3, moderately im-paired (some artifacts, some signal inhomogeneity); 4, slightly im-paired (very little artifacts, very little signal inhomogeneity); and 5,excellent.
Statistical AnalysisContinuous parameters are reported as mean (SD). Differences
in the continuous parameters were assessed using a paired Student ttest. Categorical variables were tested with the W2 or the Fisher exacttest. Receiver-operating characteristics (ROC) curve analysis wasperformed to compare the diagnostic performance of the visualanalysis and the AMC perfusion maps to detect myocardial ischemiaduring adenosine stress. Sensitivity, specificity, accuracy, and pre-dictive values were calculated according to standard formulae.
Intraobserver and interobserver reliability for stress-rest TPDIusing the visual analysis or the AMC perfusion maps were assessedusing the Lin concordance correlation coefficient (CCC)18 and themethod of Bland-Altman analysis.19 P G 0.05 was considered to in-dicate a significant difference. All data analyses were performedusing the Statistical Package for the Social Sciences for Windows11.0.1 (SPSS, Inc).
Power calculation was performed on the first 10 participants[2-sided paired t test performed using the SAS, version 8.2 soft-ware (SAS Institute, Cary, NC)] to assess the sample sizes neededto establish a power of 90% (with > = 0.05) for differences in stress-rest TPDI of 0.1 for the comparison of the visual analysis and theanalysis using the AMC perfusion maps. According to this calcula-tion, the number of participants needed was 18.
RESULTSIn our 25 patients, a total of 75 coronary arteries were exam-
ined. A normal coronary angiogram was found in 27 of the 75 cor-onary arteries (36%). In the remaining coronary arteries, 48 CAstenoses were detected: 3 of the 75 (4%) with an angiographic lumenreduction less than 50% and 45 of the 75 (60%) with an angio-graphic stenoses 50% or more. Table 2 displays the percentage ofthe LGE extent in the myocardial segments supplied by the 45 cor-onary arteries with stenoses of 50% or more.
Among the 45 coronary stenoses with a lumen reduction of50% or more, a total of 19 presented with an angiographically sig-nificant CA stenoses of 75% or more and 22 coronary arteriespresented with stenoses of angiographically intermediate severity(Q50% and G75%). Ten of the coronary arteries with angiographicallyintermediate stenoses revealed a reduced MPRI less than 1.5 deter-mined by CMR in the myocardial segments subtended by this CAand were therefore classified as hemodynamically relevant. TwelveCA stenoses of intermediate angiographic severity had an MPRI of1.5 or more and were therefore regarded as hemodynamicallynonrelevant. Four CA stenoses supplied myocardial segments withan LGE of 75% or more and were therefore excluded from theanalysis. In summary, 29 hemodynamically relevant CA stenoses wereincluded in the analysis. Figure 1 provides an overview of the CA ste-noses and their location.
Cardiovascular magnetic resonance imaging was successfullyperformed in all 25 patients, giving 400 myocardial segments that
TABLE 2. Late Gadolinium Enhancement Extent in MyocardialSegments Supplied by Coronary Arteries With StenosesQ50% (n = 45)
NonYLGE AHA Segments 16/45 (36%)
LGE (infarcted) AHA segments 29/45 (64%)
G50% transmural LGE extent 18/45 (40%)
Q50% to G100% transmural LGE extent 7/45 (16%)
Transmural scar (LGE extent, 100%),excluded from the analysis
4/45 (9%)
AHA indicates AmericanHeart Association; LGE, late gadolinium enhancement.
Doesch et al Investigative Radiology & Volume 48, Number 9, September 2013
680 www.investigativeradiology.com * 2013 Lippincott Williams & Wilkins
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

were analyzed by calculating the MPRI. The mean (SD) MPRI was1.9 (0.7) (range, 0.5Y3.5). A total of 130 myocardial segments(32.5%) presented with an MPRI less than 1.5; the remaining 270myocardial segments (67.5%) showed an MPRI of 1.5 or more. Asignificant inverse correlation was observed between the angio-graphically determined CA stenoses and the MPRI determined byCMR (r = j0.741; P G 0.0001; Fig. 2).
ReliabilityWhen all stenoses were considered, the analysis using the AMC
perfusion maps provided a slightly better sensitivity, positive predic-tive value (PPV), negative predictive value (NPV), and accuracy for thedetection of hemodynamically significant CA stenoses when com-pared to the visual analysis (Table 3A). Figures 3 to 6 demonstratepatient examples for the diagnosis of ischemia using AMC perfusionmaps (Figs. 3Y6A, B) and visual analysis (Figs. 3Y6C, D). The ROCanalysis revealed better diagnostic performance of the AMC perfusionmaps as compared to visual analysis to identify hemodynamically rele-vant CA stenoses (area under the curve, 0.97 vs 0.83; P = 0.04; Fig. 7).The attribution of an ischemic segment to the anatomic location of thehemodynamically relevant CA stenosis (Table 3B) was also slightly su-perior using the AMC perfusion maps compared to visual analysis.
ReproducibilityThe interobserver and intraobserver reproducibility were better
for the AMC perfusion maps (CCC, 0.94 and 0.93, respectively)compared with the visual analysis (CCC, 0.73 and 0.79, respectively).The Bland-Altman plots of stress-rest TPDI between the 2 observers(P = 0.3) and at 2 different time points (P = 0.2) revealed a compa-rable mean bias for both methods, but the analysis using the AMCperfusion maps showed lower limits of agreement (Fig. 8).
Workflow ImpactsThe time requirement for the analysis of the first-pass perfu-
sion using the AMC perfusion maps was found to be significantlyreduced compared with the visual analysis and the calculation of theMPRI using noncorrected data [3.2 (1.9) minutes vs 7.7 (3.1) minutes(P G 0.0001) vs 19.0 (6.0) minutes (P G 0.0001), respectively].
Impact of Motion Correction on Image Analysisand Workflow
Because the analysis of the AMC perfusion maps is based onmotion-corrected perfusion scans, we additionally analyzed the stress-rest TPDI and the MPRI in 10 randomly selected patients and com-pared the results with those obtained using noncorrected data sets.Comparison of the results of stress-rest TPDI between the noncorrected
FIGURE 1. Overview of the severity of coronary artery stenoses and their location. Overview of the angiographically examined CAand the detected stenoses divided according to the diameter stenoses and their hemodynamical significance determined by CMR.Moreover, the location of all stenoses is indicated. RCA indicates right CA.
Investigative Radiology & Volume 48, Number 9, September 2013 Detection of Myocardial Ischemia by AMC Perfusion Maps
* 2013 Lippincott Williams & Wilkins www.investigativeradiology.com 681
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

TABLE 3. Diagnostic Performance to Detect HemodynamicallySignificant Coronary Artery Stenoses
On a Per-Patient Basis
Visual Analysis AMC Perfusion Maps
Sensitivity 87.5% 93.8%
Specificity 77.8% 100.0%
Positive predictive value 87.5% 100.0%
Negative predictive value 77.8% 90.0%
Accuracy 84.0% 96.0%
True positive 14/16 15/16
False negative 2/16 1/16
False positive 2/9 0/9
True negative 7/9 9/9
On a PerYCoronary Artery Territory Basis
Visual Analysis AMC Perfusion Maps
RCA LAD LCX RCA LAD LCX
Sensitivity 57.1% 54.5% 63.6% 57.1% 63.6% 90.9%
Specificity 77.8% 85.7% 71.4% 94.4% 100% 85.7%
Positive predictive value 50.0% 75.0% 63.6% 80.0% 100% 83.3%
Negative predictive value 82.4% 70.6% 71.4% 85.0% 77.8% 92.3%
Accuracy 72.0% 72.0% 68.0% 84.0% 84.4% 88.0%
True positive 4/7 6/11 7/11 4/7 7/11 10/11
False negative 3/7 5/11 4/11 3/7 4/11 1/11
False positive 4/18 2/14 4/14 1/18 0/14 2/14
True negative 14/18 12/14 10/14 17/18 14/14 12/14
AMC indicates automated, motion-corrected, color-encoded; LAD, leftanterior descending; LCX, left circumflex; RCA, right coronary artery.
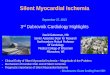
FIGURE 3. True-positive detection of myocardial ischemia bythe AMC perfusion maps and the visual analysis in a patientpresenting with a new left anterior descending arteryreocclusion. A patient with known infarction of the anteriorwall 3 years ago presented with new onset angina. Automated,motion-corrected, color-encoded perfusion maps of stress (A)versus rest perfusion (B). The dark blue color of the septal andinferior septal midventricular and apical wall only during stressperfusion (white arrows) are indicative of myocardial ischemiain the LAD territory and can easily be identified at a singleglance. Visual analysis of stress (C) versus rest perfusion (D).The basal stress perfusion image shows a dark-rim artifact (darkgray arrow), and the stress-induced PD of the septal andinferior septal midventricular and apical wall (white arrows) ismuch more difficult to detect by visual analysis. The LGE CMR(E) shows a scar of the anterior wall (gray arrows). Coronaryangiographic findings (F) revealed reocclusion of the proximalLAD (white arrow), the cause of septal ischemia.
FIGURE 2. Correlation of the angiographically determineddegree of the CA stenoses and MPRI. This graph shows asignificant inverse correlation between the diameter stenosesby angiography and the MPRI determined by CMR.
Doesch et al Investigative Radiology & Volume 48, Number 9, September 2013
682 www.investigativeradiology.com * 2013 Lippincott Williams & Wilkins
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

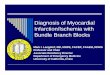
FIGURE 4. True-positive detection of myocardial ischemia bythe AMC perfusion maps and the visual analysis in a patientpresenting with intermediate CA stenoses. The patientpresented with stable angina (Canadian CardiovascularSociety classification II) for more than one year and new onsetdyspnea on exertion. Automated, motion-corrected,color-encoded perfusion maps of stress (A) versus restperfusion (B). The dark blue color of the basal andmidventicular septal and wall only during stress perfusion(white arrows) is consistent with myocardial ischemia in theLAD territory. Visual analysis of stress (C) versus rest perfusion(D). The visual analysis provides equally good detection of themyocardial ischemia of the basal and midventicular septal wallonly during stress perfusion (white arrows). The patient did notshow delayed enhancement (E). Coronary angiographicfindings (F) revealed a new 75% stenosis of the LAD with anFFR of 0.6, indicating an ischemic stenosis and a 70% stenosisof the LCX with an FFR of 0.8, proving a nonischemic stenosis.FFR indicates fractional flow reserve.
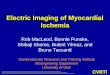
FIGURE 5. True-negative AMC perfusion maps andfalse-positive detection of myocardial ischemia by visualanalysis in a patient without significant CA stenoses. Thepatient presented with a new sense of weakness andbreathlessness on exertion. Automated, motion-corrected,color-encoded perfusion maps of stress (A) versus restperfusion (B). The identical blue to green color during stressand rest perfusion excludes myocardial ischemia during stressand rest perfusion. Visual analysis of stress (C) versus restperfusion (D). The basal stress perfusion image shows adark-rim artifact (dark gray arrow). The midventricular septalwall shows myocardial ischemia only during stress perfusion(white arrow), thus representing a false-positive result. The LGEdid not show myocardial scar (E). Coronary angiographicfindings (F) did not show significant CA stenoses.
Investigative Radiology & Volume 48, Number 9, September 2013 Detection of Myocardial Ischemia by AMC Perfusion Maps
* 2013 Lippincott Williams & Wilkins www.investigativeradiology.com 683
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

and corrected data showed a significant linear correlation (r = 0.981;P G 0.001). The Bland-Altman plots revealed a low mean (j0.7) andnarrow limits of agreement (upper limit of agreement, 1.9; lower limitof agreement, j3.3). Linear regression analysis for the MPRI calcu-lated on the noncorrected and corrected data also indicated a significantcorrelation (r = 0.877; P G 0.0001). The Bland-Altman plots showed alow mean difference (j0.01) and narrow limits of agreement (upperlimit of agreement, 0.82; lower limit of agreement,j0.85).
Application of motion-corrected data resulted in a significantlyreduced time requirement from 19.0 (6.0) minutes to 14.1 (3.6) (P =0.02) for the MPRI analysis because of improved automatic detectionof the nadir and the point of the signal maximum.
Image Analysis and ArtifactsAll images acquired were of sufficient quality for the analysis,
and no images were excluded. On a 5-point scale, the mean (SD)image quality for stress perfusion, rest perfusion, and LGE accountedfor 4.8 (0.4), 4.8 (0.4), and 4.8 (0.5), respectively. Stress-rest perfu-sion was mainly impaired by dark-rim artifacts20 observed in 4 patientsand ghosting artifacts detected in 2 patients. The LGE quality was af-fected by metal artifacts because of sternal cerclage after coronary arterybypasss graft (n = 3), chemical shift artifacts (n = 1), and frequency shiftartifacts (n = 2).
DISCUSSIONOur results demonstrated, for the first time, that the detection
of myocardial ischemia in patients with known CAD using AMCperfusion maps is feasible. Hemodynamically relevant CA stenosescould accurately be diagnosed using AMC perfusion maps in a rou-tine clinical setting. The values for sensitivity, specificity, PPV, NPV,and accuracy on a per-patient basis were comparable to visual analysis,and the AMC perfusion maps also revealed a higher diagnostic perfor-mance on a perYCA territory basis. In addition, the results showed im-proved interobserver and intraobserver reliability. The time requirementwas significantly reduced.
In our study, the AMC perfusion maps revealed a slightly bettersensitivity, specificity, PPV, NPV, and accuracy compared with the vi-sual analysis. Besides, the analysis on a perYCA territory basis alsoshowed a trend toward higher sensitivities to attribute a PD to the leftanterior descending (LAD) (63.6% vs 54.5%) or the left circumflexartery (LCX) territory (90.9% vs 63.6%) using the AMC perfusion maps.
FIGURE 6. True-positive detection of myocardial ischemiausing the AMC perfusion maps and the false-negative result bythe visual analysis in a patient with intermediate CA stenoses. Apatient presenting with a progressive angina on exertion at ouroutpatient clinic. Automated, motion-corrected,color-encoded perfusion maps of stress (A) versus restperfusion (B). Stress perfusion showed a midventricular darkblue to dark green myocardial segment inferolaterally (whitearrow), indicatingmyocardial ischemia in the LCX territory thatwas detected as true positive using the AMC perfusion maps.Visual analysis of stress (C) versus rest perfusion (D). The visualanalysis of stress and rest perfusion did not reveal myocardialischemia and therefore resulted in a false-negative result. TheLGE did not show myocardial scar (E). Coronary angiographicfindings (F) revealed a hemodynamically 75% ramuscircumflex stenosis and a nonischemic 75% stenosis of theramus diagonalis 1.
FIGURE 7. Receiver-operating characteristic curve. The ROCcurves for the AMC perfusion maps versus the visual analysisrevealed better diagnostic performance of the AMC perfusionmaps (gray line) comparedwith the visual analysis (dotted line)in identifying the hemodynamically relevant CA stenoses (areaunder the curve, 0.97 vs 0.83; P = 0.04).
Doesch et al Investigative Radiology & Volume 48, Number 9, September 2013
684 www.investigativeradiology.com * 2013 Lippincott Williams & Wilkins
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Results for the visual analysis are in line with previouslypublished data (see Supplemental Appendix A2, Supplemental Dig-ital Content 2, http://links.lww.com/RLI/A81). Preliminary adenosinestress studies at 3.0 T yielded a sensitivity of 93% to 98% for detectionof CAD.21 In a study by Thomas et al,22 the vessel-to-vessel analysisyielded the lowest sensitivities for detection of significant CAD in theLAD territory (sensitivity, 69%; specificity, 94%). The AMC perfusionmaps evaluated in this study may represent a new alternative to analyzeperfusion studies combining the precision of semiquantitative anal-ysis with the simplicity of visual analysis. Our preliminary result usingAMC perfusion maps additionally suggests that this approach couldfacilitate the attribution of an ischemia to the respective CA territory.However, the study was not powered for this comparison.
The clinical value of a specific analysis method is determinednot only by its reliability but also by its reproducibility. The inter-observer and intraobserver reliabilities to detect stress-rest TPDI usingthe AMC perfusion maps were higher as compared with the visual
analysis. This is most probably caused by the easier detection of myo-cardial ischemia. First, AMC perfusion maps seem to be less proneto artifacts. Because of the automated motion correction, the mainchallenge of qualitative analysis representing cardiac and respiratorymotion is minimized and facilitates the correct interpretation of dataespecially in patients with arrhythmia, in patients with asynchrony, orin those who are not able to breathe shallowly at peak exertion.
Second, AMC perfusion maps graphically display the peaksignal intensities and therefore make it easier to detect hypoperfusedmyocardium. Third, AMC perfusion maps allow detection of areas ofhypoperfusion by a simple quick assessment, whereas visual analysisrequires detection of areas of hypoperfusion at stress lasting for morethan 5 images beyond the initial peak enhancement, which requiresmore experience and time of the observer.
Many efforts have been made to optimize first-pass contrast-enhanced CMR for the detection of myocardial ischemia with re-gard to accuracy and robustness23,24 since the initial description of
FIGURE 8. Bland-Altman plots for the interobserver and intraobserver variability of stress-rest TPDI. A, The visual analysisinterobserver variability. The Bland-Altman plot of observer 1 versus that of observer 2 for the visual analysis of stress-rest TPDI.B, The visual analysis intraobserver variability. The Bland-Altman plot for the analysis at 2 different time points for the visual analysisof stress-rest TPDI. C, The AMC perfusionmaps interobserver variability. The Bland-Altman plot of observer 1 versus that of observer2 for the AMC perfusion maps of stress-rest TPDI. D, The AMC perfusion maps intraobserver variability. The Bland-Altman plotfor the analysis at 2 different time points for the AMC perfusion maps of stress-rest TPDI. LLA indicates lower limit of agreement;ULA, upper limit of agreement.
Investigative Radiology & Volume 48, Number 9, September 2013 Detection of Myocardial Ischemia by AMC Perfusion Maps
* 2013 Lippincott Williams & Wilkins www.investigativeradiology.com 685
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

this method by Atkinson et al.25 However, postprocessing remainedvery time-consuming, limiting its application.
The AMC perfusion maps evaluated in this study may re-present a new alternative to analyze perfusion studies combining theprecision of semiquantitative analysis with the simplicity of visualanalysis. Comparing stress-rest TPDI and MPRI in our study betweennoncorrected and corrected data showed a significant correlation. There-fore, we assume that motion correction has little impact either on theabsolute myocardial perfusion expressed by the stress-rest TPDI or onthe MPRI analysis.
Like in our study, a previous work by Wollny et al26 usingautomated motion correction designed for free breathing also dem-onstrated improved intensity-time curves. In our study, the use ofmotion-corrected data improved the automatic determination of thenadir and the point of the signal maximum of the signal intensity-time curves by the software requiring less user interaction and there-fore significantly reduced the time for the MPRI analysis.
LimitationsLimitations of the present study relate to the relatively small
study cohort. However, the pilot study showed promising results thatneed to be confirmed in larger trials including patients with variousdegrees of CAD.
We did enroll patients with a very high probability of CAD (ie,those with already known CAD, previous myocardial infarction, andcoronary artery bypasss graft), a referral bias that can raise test sen-sitivity and/or specificity.27 However, this bias occurred for both anal-ysis algorithms. Moreover, the examined patient population reflectedbest the patient population referred to adenosine stress perfusion CMRin our tertiary referral university hospital.
CONCLUSIONSIn our pilot study, the AMC perfusion maps yielded a diagnostic
performance on a per-patient and on a perYcoronary artery territorybasis comparable to visual analysis. Furthermore, it showed higherinterobserver and intraoberserver reliability as well as a better timeefficiency.
ACKNOWLEDGMENTThe authors thank Uwe Mattler and Katrin Koziel for their
technical assistance in this project.
REFERENCES1. Schwitter J, Nanz D, Kneifel S, et al. Assessment of myocardial perfusion in
coronary artery disease by magnetic resonance: a comparison with positronemission tomography and coronary angiography. Circulation. 2001;103:2230Y2235.
2. Doesch C, Seeger A, Hoevelborn T, et al. Adenosine stress cardiac magneticresonance imaging for the assessment of ischemic heart disease. Clin ResCardiol. 2008;97:905Y912.
3. Seeger A, Doesch C, Klumpp B, et al. MR stress perfusion for the detection offlow-limiting stenoses in symptomatic patients with known coronary artery dis-ease and history of stent implantation [in German]. Rofo. 2007;179:1068Y1073.
4. Jahnke C, Nagel E, Gebker R, et al. Prognostic value of cardiac magneticresonance stress tests: adenosine stress perfusion and dobutamine stress wallmotion imaging. Circulation. 2007;115:1769Y1776.
5. Klem I, Heitner JF, Shah DJ, et al. Improved detection of coronary artery dis-ease by stress perfusion cardiovascular magnetic resonance with the use of de-layed enhancement infarction imaging. J Am Coll Cardiol. 2006;47:1630Y1638.
6. Wilke N, Jerosch-Herold M, Wang Y, et al. Myocardial perfusion reserve: as-sessment with multisection, quantitative, first-pass MR imaging. Radiology.1997;204:373Y384.
7. Al-Saadi N, Nagel E, Gross M, et al. Noninvasive detection of myocardial is-chemia from perfusion reserve based on cardiovascular magnetic resonance.Circulation. 2000;101:1379Y1383.
8. Fenchel M, Kramer U, Helber U, et al. Semiquantitative assessment of myo-cardial perfusion using magnetic resonance imaging: evaluation of appropriatethresholds and segmentation models. Invest Radiol. 2004;39:572Y581.
9. Rieber J, Huber A, Erhard I, et al. Cardiac magnetic resonance perfusion im-aging for the functional assessment of coronary artery disease: a comparisonwith coronary angiography and fractional flow reserve. Eur Heart J. 2006;27:1465Y1471.
10. Hsu LY, Rhoads KL, Holly JE, et al. Quantitative myocardial perfusion analy-sis with a dual-bolus contrast-enhanced first-pass MRI technique in humans.J Magn Reson Imaging. 2006;23:315Y322.
11. Attenberger UI, Sourbron SP, Michaely HJ, et al. Retrospective respiratorytriggering renal perfusion MRI. Acta Radiol. 2010;51:1163Y1171.
12. Cerqueira MD, Weissman NJ, Dilsizian V, et al. Standardized myocardial seg-mentation and nomenclature for tomographic imaging of the heart: a statementfor healthcare professionals from the Cardiac Imaging Committee of the Councilon Clinical Cardiology of the American Heart Association. Circulation. 2002;105:539Y542.
13. Huber A, Bauner K, Wintersperger BJ, et al. Phase-sensitive inversion recovery(PSIR) single-shot TrueFISP for assessment of myocardial infarction at 3 tesla.Invest Radiol. 2006;41:148Y153.
14. Galbraith JE, Murphy ML, de Soyza N. Coronary angiogram interpretation.Interobserver variability. JAMA. 1978;240:2053Y2056.
15. Yang GZ, Hawkes D, Rueckert D, et al, eds. Unsupervised inline analysis ofcardiac perfusion MRI. MICCAI 2009, Part II, LNCS 5762. Berlin, Heidelberg(Germany): Springer-Verlag Berlin Heidelberg; 2009:741Y749.
16. Lindeberg T. Edge detection and ridge detection with automatic scale selection.Int J Comput Vis. 1998;30:117Y154.
17. Paetsch I, Jahnke C, Wahl A, et al. Comparison of dobutamine stress magneticresonance, adenosine stress magnetic resonance, and adenosine stress magneticresonance perfusion. Circulation. 2004;110:835Y842.
18. Lin LI. A concordance correlation coefficient to evaluate reproducibility.Biometrics. 1989;45:255Y268.
19. Bland JM, Altman DG. Statistical methods for assessing agreement betweentwo methods of clinical measurement. Lancet. 1986;1:307Y310.
20. Di Bella EV, Parker DL, Sinusas AJ. On the dark rim artifact in dynamic contrast-enhanced MRI myocardial perfusion studies. Magn Reson Med. 2005;54:1295Y1299.
21. Cheng AS, Pegg TJ, Karamitsos TD, et al. Cardiovascular magnetic resonanceperfusion imaging at 3-tesla for the detection of coronary artery disease: a com-parison with 1.5-tesla. J Am Coll Cardiol. 2007;49:2440Y2449.
22. Thomas D, Strach K, Meyer C, et al. Combined myocardial stress perfusionimaging and myocardial stress tagging for detection of coronary artery diseaseat 3 tesla. J Cardiovasc Magn Reson. 2008;10:59.
23. Elkington AG, He T, Gatehouse PD, et al. Optimization of the arterial inputfunction for myocardial perfusion cardiovascular magnetic resonance. J MagnReson Imaging. 2005;21:354Y359.
24. Utz W, Niendorf T, Wassmuth R, et al. Contrast-dose relation in first-passmyocardial MR perfusion imaging. J Magn Reson Imaging. 2007;25:1131Y1135.
25. Atkinson DJ, Burstein D, Edelman RR. First-pass cardiac perfusion: evaluationwith ultrafast MR imaging. Radiology. 1990;174:757Y762.
26. Wollny G, Ledesma-Carbayo MJ, Kellman P, et al. Exploiting quasiperiodicityin motion correction of free-breathing myocardial perfusion MRI. IEEE TransMed Imaging. 2010;29:1516Y1527.
27. Ransohoff DF, Feinstein AR. Problems of spectrum and bias in evaluating theefficacy of diagnostic tests. N Engl J Med. 1978;299:926Y930.
Doesch et al Investigative Radiology & Volume 48, Number 9, September 2013
686 www.investigativeradiology.com * 2013 Lippincott Williams & Wilkins
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.