Embed Size (px)
Citation preview
426
Azathioprine 100 mg daily was added but soon withdrawn becauseof neutropenia. During the next month his disease flared and amononeuritis multiplex affected the motor and sensory nerves inboth legs and left hand. In addition he had a necrotising scleritiswith a corneal melt in the right eye. He was referred to the VasculitisClinic at our hospital. Haemoglobin was 10-8 g/dl, WCC18.1 x 109/1, ESR 90 mm/h, C-reactive protein (CRP) 110 mg/1(normal < 10). Antineutrophil cytoplasmic antibodies (ANCA) titrewas 320 with a cytoplasmic staining pattern. Radiography(cavitating lesions) and nasal mucosa biopsy (necrotisinggranulomatous vasculitic lesions) led to the diagnosis of WG.
Intravenous cyclophosphamide with mesna, and intravenousmethylprednisolone and oral prednisolone led to improvement,especially in the necrotising scleritis and neurological deficits. Hewas maintained on oral cyclophosphamide until thrombocytopeniaoccurred, and normal values returned after switching to intravenouscyclophosphamide. The cavitating pulmonary lesions resolvedalmost completely and he remained well for a year.The disease then flared. Despite six fortnightly pulses of
cyclophosphamide 750-1000 mg, he became severely ill with
widespread vasculitic lesions and the pulmonary nodules returned.He was given three 2 litre plasma exchanges, intravenous
cyclophosphamide, doxorubicin and vincristine, and oral
prednisolone, with no response to two courses. The cutaneousvasculitic lesions became widespread and were associated withpyrexia, arthralgia, scleritis, and sinusitis. ESR, CRP, and ANCAtests were abnormal.
Oral etoposide 100 mg daily for 7 days every 3 weeks was started.Within a month gradual improvement was apparent and he hasbeen in complete clinical remission on monthly courses of etoposidefor a year with no adverse effects.
Other approaches in WG, besides cyclophosphamide, includeplasmapharesis with immunosuppressives, intravenous
immunoglobulins,l and monoclonal antibodies against T-cell
antigens,2 with varying degees of success. Etoposide3 arrests DNAreplication, apparently by inducing single-strand DNA breaks inthe premitotic phase. It is most often used in combination regimensin small-cell lung cancers, testicular teratomas, and lymphomas.The main adverse effects include bone-marrow suppression with aleucocyte nadir after 15 days, nausea and vomiting, reversiblealopecia, transient disturbances of liver function, and occasionally amild peripheral neuropathy.4
Lupus Arthritis Research Unitand Department of Oncology,
St Thomas’s Hospital,London SE1 7EH, UK
D. D’CRUZH. PAYNEA. TIMOTHYG. R. V. HUGHES
1. Jayne DRW, Davies MJ, Fox CJV, Black CM, Lockwood CM. Treatment ofsystemic vasculitis with pooled intravenous immunoglobulin. Lancet 1991; 337:1137.
2. Mathieson PW, Cobbold SP, Hale G, et al Monoclonal-antibody therapy in systemicvasculitis. N Engl J Med 1990; 323: 250-56.
3. Vogelsang NJ, Raghavan D, Kennedy BJ. VP-16-213 (Etoposide): the mandrake rootfrom Issyk-Kul. Am J Med 1982, 72: 136-44.
4. Issell BF, Muggia FM, Carter SK, eds Etoposide (VP-16)—current status and newdevelopments. New York: Academic Press, 1984.
Magnesium and chronic fatigue syndromeSIR,-Dr Clague and colleagues (July 11, p 124) report normal
magnesium status in 12 patients with chronic fatigue syndrome(CFS). We agree that magnesium deficiency is not the cause ofCFS, but it is a factor in many of the patients we see.CFS patients, who are referred to us for nutrient status
investigations by general practitioners and consultants from manycentres, have often been investigated elsewhere. This preselectionwill skew our patient population, but we are nonetheless surprisedthat Clague et al did not find any magnesium deficiencies. In theinvestigation of several hundred CFS patients we have never seen12 consecutive people with normal magnesium values. We usewhite cell magnesium and magnesium retention tests as well asmeasurement of red-cell magnesium when necessary. That
Clague’s patients did not show any improvement in symptoms afterintravenous magnesium should not be surprising since no patientwas deficient in magnesium. We find that at least half the patients
who are deficient benefit from oral supplementation, although a fewdo also need intramuscular magnesium. We support the use ofmagnesium for CFS patients whenever there is a proven deficiency.
In your May 30 note (p 1349), you correctly state the importanceof recognising CFS patients with a major depressive illness. Webelieve that it is equally important to identify those with essentialnutrient deficiencies. In our experience deficiencies of magnesium,vitamin Bl, and essential fatty acids are quite common. Correction isoften accompanied by clinical improvement. You also say thatalterations in muscle physiology are not seen in CFS patients.Although this is certainly true with many techniques that look atmuscle contraction, one of us (J. M. H.) has previously reportedchanges in relaxation and resting indices with myothermography onpatients with magnesium deficiency. We are finding a goodcorrelation between this test and magnesium status in CFS patients.Improvements in the test results also parallel clinical improvement.
BIOLAB Medical Unit,9 Weymouth Street,London W1N 3FF, UK
JOHN MCLAREN HOWARDSTEPHEN DAVIESADRIAN HUNNISETT
1. Howard J. Muscle action, trace elements and related nutrients the myothermogramIn: Chazot G, Abdulla M, Arnaud P, eds. Current trends in trace element research.proceedings m international symposium on trace elements. Pans, 1987 London.Smith-Gordon, 1989: 79-85.
Detection of long-lasting antibody tohepatitis E virus in a US traveller to Pakistan
SiR,—Most waterbome hepatitis due to infection with hepatitisE virus (HEV) has occurred in developing countries, such as India,Pakistan, Burma, Algeria, Somalia, and Ethiopia.1 There have beenisolated reports of HEV infection among travellers to India andSaudi Arabia and in a traveller to Mexico.’ Here we reportserological antibodies to HEV in a US traveller to Pakistan.A 54-year-old, previously healthy, well-nourished man
developed malaise and jaundice on Jan 12, 1988, about 1 monthafter returning from Pakistan. There was no serological evidence foracute hepatitis due to hepatitis A or B virus, or to cytomegalovirus;non-A, non-B hepatitis (NANBH) was presumed. The patient hada hepatocellular involvement (aspartate aminotransferase [AST]5000 IU, total bilirubin 10-7 mgfdl, direct bilirubin 7-2 mgldl,alkaline phosphatase 267 IU) which progressed to a cholestaticpattern (AST 387 IU, alanine aminotransferase 574 IU, totalbilirubin 30 mg/dl, direct bilirubin 16-1 mg/dl, alkaline phosphatase196 IU). He was admitted for intravenous hydration and supportivecare, and was discharged on Feb 21.The patient was readmitted 4 days later with persistent nausea
and vomiting, despite treatment with prochlorperazine and
metoclopramide, and progressive weight loss. He was started onperipheral hyperalimentation, but because of severe venous
irritation from the catheter, tube feeding was initiated. Bilirubinandliver enzyme concentrations decreased and on March 4, the patientwas discharged.
In July, 1991, a panel of twenty specimens from patientsdiagnosed with acute NANBH, including one from the patient
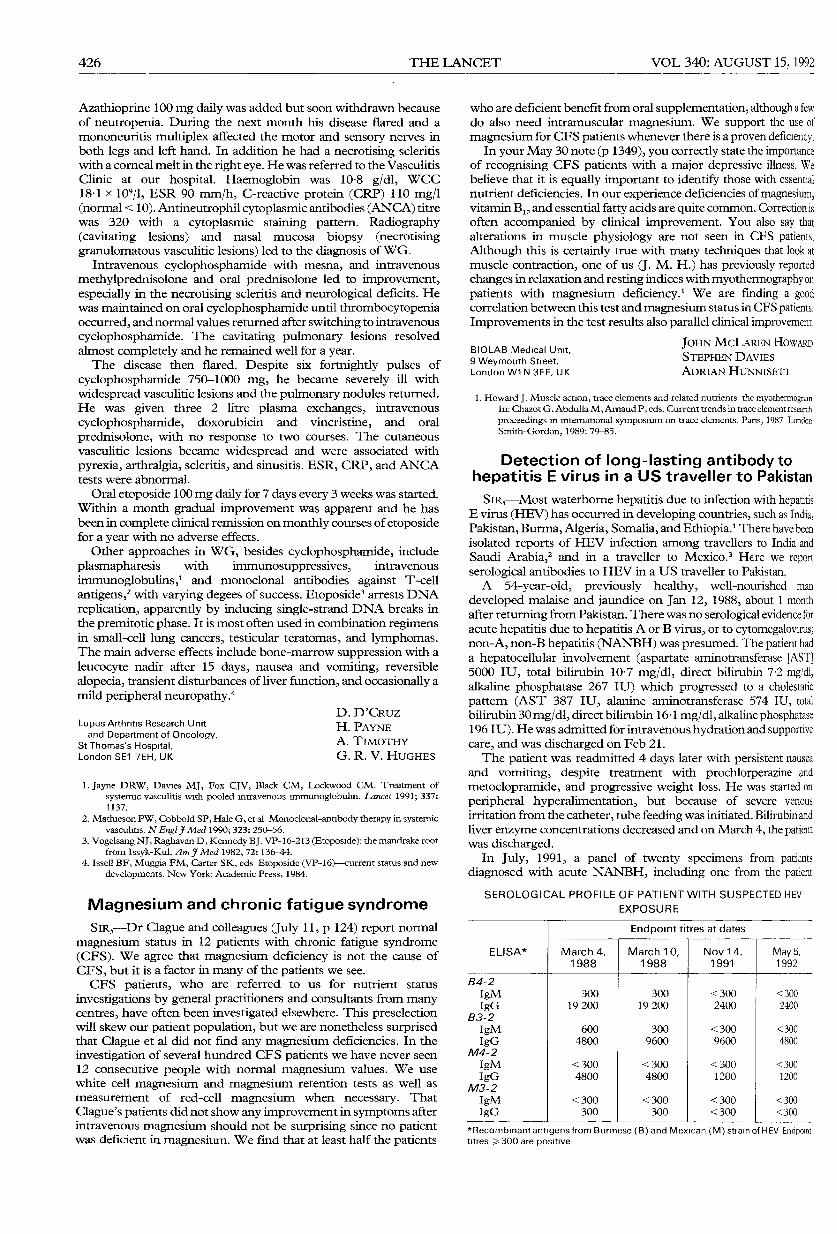
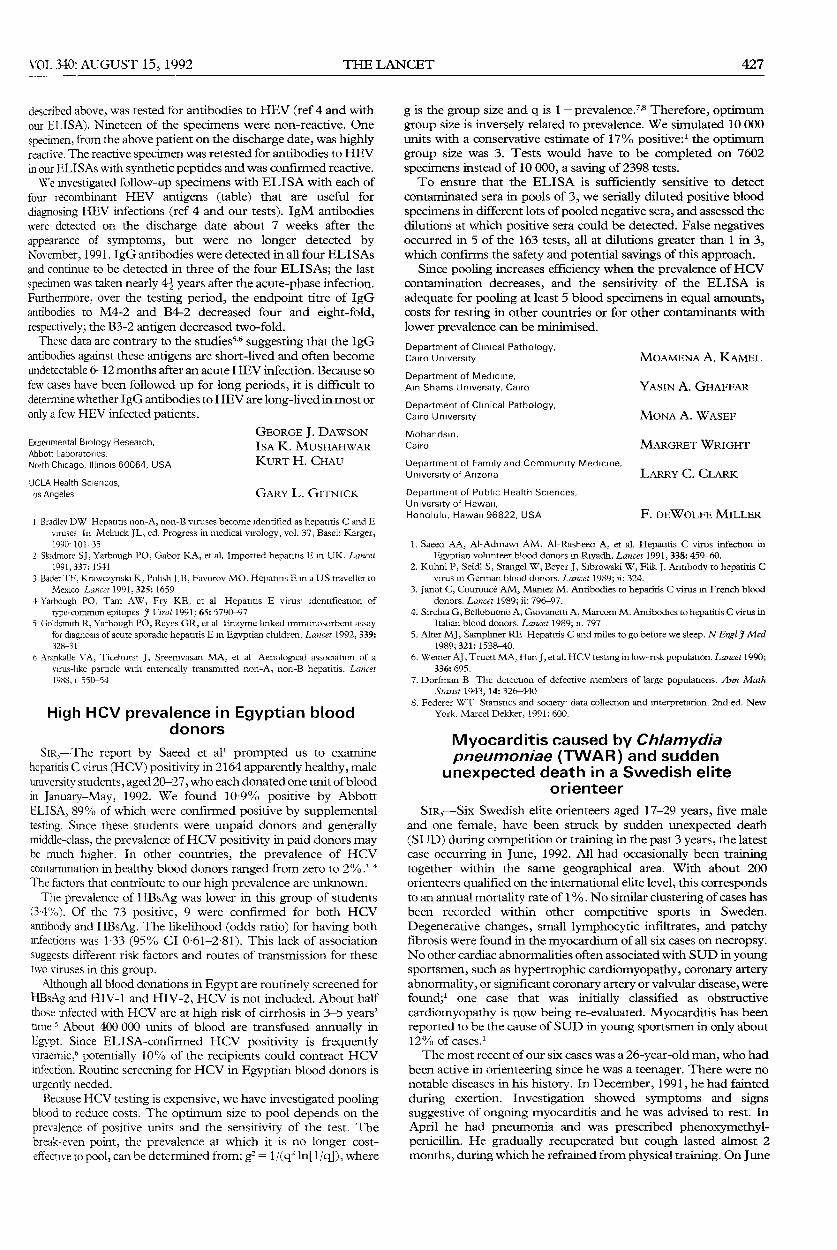
SEROLOGICAL PROFILE OF PATIENT WITH SUSPECTED HEV
EXPOSURE
*Recombinant antigens from Burmese (B) and Mexican (M)stra of HEV Endpointtltres ?o 300 are positive
427
described above, was tested for antibodies to HEV (ref 4 and withour ELISA). Nineteen of the specimens were non-reactive. Onespecimen, from the above patient on the discharge date, was highlyreactive. The reactive specimen was retested for antibodies to HEVin our ELISAs with synthetic peptides and was confirmed reactive.We investigated follow-up specimens with ELISA with each of
four recombinant HEV antigens (table) that are useful for
diagnosing HEV infections (ref 4 and our tests). IgM antibodieswere detected on the discharge date about 7 weeks after theappearance of symptoms, but were no longer detected byinovember, 1991. IgG antibodies were detected in all four ELISAsand continue to be detected in three of the four ELISAs; the lastspecimen was taken nearly 41 years after the acute-phase infection.Furthermore, over the testing period, the endpoint titre of IgGantibodies to M4-2 and B4-2 decreased four and eight-fold,respectively; the B3-2 antigen decreased two-fold.These data are contrary to the studiess,6 suggesting that the IgG
antibodies against these antigens are short-lived and often becomeundetectable 6-12 months after an acute HEV infection. Because sofew cases have been followed up for long periods, it is difficult todetermine whether IgG antibodies to HEV are long-lived in most oronly a few HEV infected patients.
Experimental Biology Research,Abbott Laboratories,North Chicago, Illinois 60064, USA
UCLA Health Sciences,Los Angeles
GEORGE J. DAWSONISA K. MUSHAHWARKURT H. CHAU
GARY L. GITNICK
1 Bradley DW Hepatitis non-A, non-B viruses become identified as hepatitis C and Eviruses In Melnick JL, ed. Progress in medical virology, vol. 37, Basel: Karger,1990; 101-35
2. Skidmore SJ, Yarbough PO, Gabor KA, et al. Imported hepatitis E in UK. Lancet1991; 337: 1541
3 Bader TF, Krawczynski K, Polish LB, Favorov MO. Hepatitis E m a US traveller toMexico Lancet 1991, 325: 1659
4 Yarbough PO, Tarn AW, Fry KE, et al Hepatitis E virus; identification of
type-common epitopes J Virol 1991; 65: 5790-975 Goldsmith R, Yarbough PO, Reyes GR, et al Enzyme linked immunosorbent assay
for diagnosis of acute sporadic hepatitis E in Egyptian children. Lancet 1992, 339:328-31
b Arankalle B’A, Ticehurst J, Sreenivasan MA, et al Aetiological association of avirus-like particle with enterically transmitted non-A, non-B hepatitis. Lancet1988; i: 550-54
High HCV prevalence in Egyptian blooddonors
SiR,—The report by Saeed et all prompted us to examinehepatitis C virus (HCV) positivity in 2164 apparently healthy, maleuruversity students, aged 20-27, who each donated one unit of bloodin January-May, 1992. We found 10-9% positive by AbbottELISA, 89% of which were confirmed positive by supplementaltesting. Since these students were unpaid donors and generallymiddle-class, the prevalence of HCV positivity in paid donors maybe much higher. In other countries, the prevalence of HCVcontamination in healthy blood donors ranged from zero to 2%.*The factors that contribute to our high prevalence are unknown.The prevalence of HBsAg was lower in this group of students
(3-4%). Of the 73 positive, 9 were confirmed for both HCVantibody and HBsAg. The likelihood (odds ratio) for having bothinfections was 1-33 (95% CI 0’61-2’81). This lack of associationsuggests different risk factors and routes of transmission for thesetwo viruses in this group.Although all blood donations in Egypt are routinely screened for
HBsAg and HIV-1 and HIV-2, HCV is not included. About halfthose infected with HCV are at high risk of cirrhosis in 3-5 years’time.’ About 400 000 units of blood are transfused annually inEgypt. Since ELISA-confirmed HCV positivity is frequentlyviraemic,6 potentially 10% of the recipients could contract HCVinfection. Routine screening for HCV in Egyptian blood donors isurgently needed.
Because HCV testing is expensive, we have investigated poolingblood to reduce costs. The optimum size to pool depends on theprevalence of positive units and the sensitivity of the test. Thebreak-even point, the prevalence at which it is no longer cost-effective to pool, can be determined from: g2 = 1 /(qZ In[l/q]), where
g is the group size and q is 1 - prevalenCe.7,8 Therefore, optimumgroup size is inversely related to prevalence. We simulated 10 000units with a conservative estimate of 17% positive:1 the optimumgroup size was 3. Tests would have to be completed on 7602specimens instead of 10 000, a saving of 2398 tests.To ensure that the ELISA is sufficiently sensitive to detect
contaminated sera in pools of 3, we serially diluted positive bloodspecimens in different lots of pooled negative sera, and assessed thedilutions at which positive sera could be detected. False negativesoccurred in 5 of the 163 tests, all at dilutions greater than 1 in 3,which confirms the safety and potential savings of this approach.
Since pooling increases efficiency when the prevalence of HCVcontamination decreases, and the sensitivity of the ELISA is
adequate for pooling at least 5 blood specimens in equal amounts,costs for testing in other countries or for other contaminants withlower prevalence can be minimised.
Department of Clinical Pathology,Cairo University MOAMENA A. KAMEL
Department of Medicine,Ain Shams University, Cairo YASIN A. GHAFFAR
Department of Clinical Pathology,Cairo University MONA A. WASEF
Mohandsm,Cairo MARGRET WRIGHT
Department of Family and Community Medicine,University of Arizona LARRY C. CLARK
Department of Public Health Sciences,University of Hawaii,Honolulu, Hawaii 96822, USA F. DEWOLFE MILLER
1. Saeed AA, Al-Admawi AM, Al-Rasheed A, et al. Hepatitis C virus infection inEgyptian volunteer blood donors m Riyadh. Lancet 1991, 338: 459-60.
2. Kuhnl P, Seidl S, Stangel W, Beyer J, Sibrowski W, Flik J. Antibody to hepatitis Cvirus in German blood donors. Lancet 1989; ii: 324.
3. Janot C, Couroucé AM, Maniez M. Antibodies to hepatitis C virus in French blooddonors. Lancet 1989; ii: 796-97.
4. Sirchia G, Bellobuono A, Giovanetti A, Marconi M. Antibodies to hepatitis C virus inItalian blood donors. Lancet 1989; ii: 797
5. Alter MJ, Sampliner RE Hepatitis C and miles to go before we sleep. N Engl J Med1989; 321: 1538-40.
6. Weiner AJ, Truett MA, Han J, et al. HCV testing in low-risk population. Lancet 1990;336: 695.
7. Dorfman B The detection of defective members of large populations. Ann MathStatist 1943, 14: 326-440
8. Federer WT Statistics and society data collection and interpretation. 2nd ed. NewYork. Marcel Dekker, 1991: 600.
Myocarditis caused by Chlamydiapneumoniae (TWAR) and sudden
unexpected death in a Swedish eliteorienteer
SiR,—Six Swedish elite orienteers aged 17-29 years, five maleand one female, have been struck by sudden unexpected death(SUD) during competition or training in the past 3 years, the latestcase occurring in June, 1992. All had occasionally been trainingtogether within the same geographical area. With about 200orienteers qualified on the international elite level, this correspondsto an annual mortality rate of 1 %. No similar clustering of cases hasbeen recorded within other competitive sports in Sweden.
Degenerative changes, small lymphocytic infiltrates, and patchyfibrosis were found in the myocardium of all six cases on necropsy.No other cardiac abnormalities often associated with SUD in youngsportsmen, such as hypertrophic cardiomyopathy, coronary arteryabnormality, or significant coronary artery or valvular disease, werefound;’ one case that was initially classified as obstructive
cardiomyopathy is now being re-evaluated. Myocarditis has beenreported to be the cause of SUD in young sportsmen in only about12% of cases.’The most recent of our six cases was a 26-year-old man, who had
been active in orienteering since he was a teenager. There were nonotable diseases in his history. In December, 1991, he had faintedduring exertion. Investigation showed symptoms and signssuggestive of ongoing myocarditis and he was advised to rest. InApril he had pneumonia and was prescribed phenoxymethyl-penicillin. He gradually recuperated but cough lasted almost 2months, during which he refrained from physical training. On June