Embed Size (px)
Citation preview

In the name of Allah the Beneficent the Merciful

Detecting the Differences
Radiculopathy, Myelopathy and Peripheral Neuropathy
Dr Zafar Iqbal
Department of Neurosurgery
Abbasi Shaheed Hospital Karachi

Points to note …..
Radiculopathy, myelopathy, and peripheral neuropathy have common overlapping symptoms, but each has a unique physiological mechanism underlying the sensory and motor disturbances associated with each disorder.

Points to note …..
While the physical exam should reveal characteristics that differentiate one pathology from another, in order to prevent an incorrect diagnosis, the list of differential diagnoses should be examined before treatment is started.

Points to note …..
Further work-up may be necessitated by other disease processes that present with common symptoms, if the patient does not respond to well regarded treatment or new symptoms develop during treatment.

Radiculopathy
Radiculopathy occurs as a result of biomechanical pressure on a nerve root with subsequent biochemical release of inflammatory mediators
(Starkweather, Witek-Janusek & Mathews, 2005).

Radiculopathy
Biomechanical pressure at the point of the dorsal root ganglion (nerve root that directly dissects from the spinal cord) or peripheral nerve can be caused by
disc tissue, tumors, or bone.

Radiculopathy
often has a quick onset and is characterized by a shooting pain that radiates down the extremity.
Patients often present with symptoms present upon awakening in the morning, without identifiable trauma or stress.

Radiculopathy
Clinical findings include pain, dermatomal sensory disturbances, weakness, and hypoactive muscle stretch reflexes in the
distribution of the affected nerve root

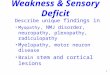
Radiculopathy
cervical herniated disc is the most common reason for upper extremity radiculopathy


Radiculopathy

Radiculopathy
Motor and sensory loss will be specific to the nerve root involved

Radiculopathy

Almost all herniated cervical discs cause painful limitation of neck motion, with aggravation of pain during neck extension.


Radiculopathy
Left C–6 radiculopathy occasionally presents with chest or scapular pain
C–8 and T–1 nerve root involvement may cause a partial Horner’s syndrome due to interruption distal to the superior cervical ganglion.

Over 90% of patient with acute cervical radiculopathy due to cervical disc herniation will improve without surgery (Saal, Saal, &Yurth, 1996).

The recovery period can be treated with adequate pain medication, mainly non-steroidal anti-inflammatory types and muscle relaxants. Short course tapered steroids and intermittent cervical traction (10–15 pounds for 10–15 minutes 2–3 times daily) may also be used.

In patients that have progressive neurological deficits (i.e. weakness) of the affected muscle groups, however, surgery may provide the best long-term outcomes

cervical discectomy
Anterior cervical discectomy with fusion (ACDF) or without fusion (ACD) or posterior cervical foraminotomy may be used for resection of a cervical disc herniation

selection of the surgical procedure
reasonably be based on the preference of the surgeon and tailored to the individual patient.

cervical disc replacement
may likely be available to the general public in the near future. Clinical trials on the efficacy of disc replacement surgery have continued with promising outcomes (Phillips & Garfan, 2005).

Cervical disc replacement
preserves motion at the instrumented level/s and can potentially improve load transfer to the adjacent levels compared with fusion. There are several different models that are presently seeking FDA approval

Risks associated with surgery
neurological injury, dural tear, infectionthe

Risks
long-term voice disturbances dysphasia. incidence of new-onset dysphasia after
surgery is 29.8% at three months, 6.9% at six months, and 6.6% at two years.

Risks
The use of plates resulted in a 1.6-times higher incidence and higher rates were noted following multi-level procedures and at more cephalic levels.
a smaller and smoother plate profile reduced the incidence and severity of post-operative dysphasia.

plating affects the adjacent levels Most plate designs use oblong holes, and,
as settling occurs, the plate translates toward the next adjacent non-fused level (Cervical Spine Research Society, 2005). Plates within 5 mm of non-fused disc spaces have been associated with adjacent-level disc ossification.

Risks
This phenomenon, when occurring within three months after surgery, is likely to be progressive. However, Rao and colleagues (2005) suggest that fusion does not generally affect adjacent levels in the cervical spine.

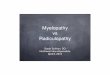
Myelopathy
Functional disturbance or pathological change in the spinal cord is referred to as myelopathy

Myelopathy
It is often caused by pressure around the spinal cord. This syndrome usually has a prolonged onset, occurring over months to years

Differential Diagnosis

Patients may present with
an inability to button their clothes, turn doorknobs and may complain of dropping objects often.

CSM
Cervical spondylosis is the most common cause of myelopathy in patients over 55 years of age (Greenberg, 2006). Spondylosis, a term used to describe widespread degenerative condition of the discs and vertebrae, can cause direct cord compression.

Cervical spondylotic myelopathy
develops in almost all patients with over 30% narrowing of the cross-sectional area of the cervical spinal canal, although some patients with severe cord compression do not develop myelopathy.

CSM
Osteophytes and hypertrophy or enfolding of the ligamentum flavum may also contribute to spinal cord compression


These processes
narrow the canal causing ischemia of the cord and degeneration of the central grey matter at the level of compression

Damage
to the posterior columns above the lesion and demyelination in the lateral columns, especially the corticospinal tracts, below the lesion, causes
changes in sensory and motor function. Thus, a mixture of
upper motor and lower motor neuron findings in cervical
myelopathy may be found.

Clinical Features
There may be weakness and wasting of hand muscles with slow, stiff opening and closing of the
fists, resembling arthritis.

Clinical Features
Clumsiness with fine motor skillsproximal weakness of the lower
extremities, notably iliopsoas weakness occurs in 54%, and
spasticity of the lower extremities with most having hyperactive reflexes (clonus and Babinski’s sign).
.

Clinical Features
Glove distribution sensory loss in the hands may be present and most have loss of vibratory sense in the lower extremities

Amyotrophic lateral sclerosis (ALS)
is commonly misdiagnosed as cervical spondylosis.

Common findings of ALS
include: atrophic weakness of the hands and forearms mild lower extremity spasticity and diffuse hyperreflexia, but sensory changes are absent. Dysarthria or hyperactive jaw-jerk may be the first clue. Hyperactive jaw jerk indicates upper motor neuron
lesion above the midpons and distinguishes long tract findings above the foramen magnum from those below. Fasciculation of the tongue or in the lower extremities may also occur in ALS.

Electromyelography (EMG)
Electromyelography (EMG) is the diagnostic test used to confirm ALS.

MRI
Careful consideration of chiari malformation, syringomyelia, hydrocephalus and cervical spondylosis with cord compression were used when evaluating the films.

Surgery
cervical laminoplasty, a procedure to decompress the spinal canal by removing a part of the lamina of the affecting vertebrae.
Anterior cervical discectomy or vertebrectomy with or without fusion may be used to treat
anterior disease up to three levels. The posterior approach, Decompressive cervical laminectomy with or without fusion may be used if the
disease is primarily posterior or if surgery is required in more than three levels.

cervical laminoplasty
was associated with better clinical outcomes (functioning, pain) and less complications than decompression and fusion.




Indications for surgery
are primarily patients with radiological evidence of spondylotic degeneration of the cervical spine with progressive symptoms, and/or pain.

Severity and Progression
Thus, the importance of determining severity and progression of symptoms is vital as the goal of surgery is to stop the progression, while recovery of symptoms is variable.

Laminoplasty
has gained in popularity for the treatment of cervical myelopathy secondary to
ossification of the posterior longitudinal ligament and
spondylosis with spinal stenosis

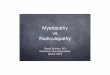
Peripheral neuropathy
Peripheral neuropathy occurs as nerve roots, which extend to the distal portion of each extremity, are damaged.

Etiology
The exact cause is unknown but is thought to be mediated by inflammation, ischemia and demyelination of the larger peripheral nerves

Etiology
Diabetes, alcohol and Guillain-Barre
accounting for 90% of cases


Evaluation
for the initial workup for peripheral neuropathies of unknown etiology should include
Hgb-A1C, TSH, ESR, vitamin B12 and EMG studies.

Over 50% of patients with diabetes mellitus (type I and type II)
develop neuropathic symptoms (Perkins, 2002). Diabetic neuropathy may be slowed with tight glucose control, while in patients with impaired glucose tolerance; diet and exercise have been shown to significantly improve neuropathic pain (Laino, 2004)..

Even in patients that have diabetes, evaluation of other causes for neuropathy is advocated. Gorson and Ropper (2006) found that 53% of 103 diabetic patients with polyneuropathy had additional causes, such as
vitamin B deficiencies, renal disease, alcohol overuse, and neurotoxin medications

Drugs
Thalidomide Metronidazole (Flagyl) Phenytoin (Dilantin), Amitriptyline (Elavil), Dapsone Nitrofurantoin (Macrodantin) Cholesterol Lowering Drugs Such As 1. Lovastatin (Mevacor)2. Indapamide (Lozol) 3. Gemfibrozil (Lopid) Thallium, And Chemotherapy (Cisplatin, Vincristine)

Guillain-Barre syndrome
presents as an acute onset of peripheral neuropathy with progressive and symmetric muscle weakness (more severe proximally) with areflexia.

Guillain-Barre syndrome
This occurs with focal segmental demyelination with endoneurial monocytic infiltration; the exact cause of the disease, however, remains unknown. Patients are diagnosed based on presentation and progression of symptoms, nerve conduction studies and through cerebral spinal fluid analysis

Perioperative neuropathies
Most sensory neuropathies that develop perioperatively or after cardiac catheterization resolve over time, but motor neuropathies can be transient or permanent

Gabapentin
a neuroleptic drug, has been advocated for treatment of neuropathic pain including peripheral nerve injury (National Guideline Clearinghouse, 2003).


Nerve Growth Factor
Recombinant human Nerve Growth Factor (rhNGF) may be the first treatment that actually repairs nerves
rhNGF is a manufactured form of a naturally produced chemical that signals the body to produce, repair and strengthen small nerves

Conclusion
Patients presenting with radiculopathy, myelopathy or peripheral neuropathy may have several overlapping symptoms. The physical exam should provide the practitioner with a differential diagnoses scheme that will allow correct diagnosis and treatment

………
In general, the absence of weakness should allow the practitioner time for an adequate work-up of the most common diagnoses through laboratory or radiological tests. It is imperative that the practitioner continues to evaluate treatment regimens for their effectiveness and revisit the differential diagnoses so that the patient does not continue down the wrong treatment path. In addition, helping patients to recognize healthy life style habits that may affect their symptoms is crucial