Embed Size (px)
Citation preview

Cervical Radiculopathy and Cervical Radiculopathy and MyelopathyMyelopathy
Wayne Cheng, MDWayne Cheng, MDInstructorInstructor
Loma Linda University Medical CenterLoma Linda University Medical CenterDepartment of Orthopaedic SurgeryDepartment of Orthopaedic Surgery


OverviewOverview• AnatomyAnatomy• EpidemiologyEpidemiology• Natural HistoryNatural History• Clinical PresentationClinical Presentation• RadiologyRadiology• TreatmentTreatment
– Non-OpNon-Op– OperativeOperative
• OITE QuestionsOITE Questions

AnatomyAnatomy
• OcciputOcciput
• C1 AtlasC1 Atlas
• C2 AxisC2 Axis
• C3-C7C3-C7

AnatomyAnatomy
• Vertebral bodies of C3-C7 are similar Vertebral bodies of C3-C7 are similar – Function and appearanceFunction and appearance

AnatomyAnatomy

AnatomyAnatomy
• Occipital atlantal joint Occipital atlantal joint – 50% flexion extension50% flexion extension
• Atlantoaxial jointAtlantoaxial joint– 50% cervical rotation50% cervical rotation

AnatomyAnatomy
C3C4-5
C6
Lower Mandible C2

AnatomyAnatomy
C3C4-5
C6
Lower Mandible C2

AnatomyAnatomy
C3C4-5
C6
Lower Mandible C2

AnatomyAnatomy
C3C4-5
C6
Lower Mandible C2

AnatomyAnatomy
C3C4-5
C6
Lower Mandible C2

AnatomyAnatomy
• Disc between bodies of Disc between bodies of C2-C7C2-C7– Outer annulus fibrosusOuter annulus fibrosus– Inner nucleus pulposusInner nucleus pulposus
• Force dissipatersForce dissipaters
• Thicker anteriorly, cervical Thicker anteriorly, cervical lordosislordosis

AnatomyAnatomy• Cervical nerve roots exit Cervical nerve roots exit aboveabove
corresponding vertebral body C1-C7corresponding vertebral body C1-C7– C1 exits b/t occiput & C1 bodyC1 exits b/t occiput & C1 body
– C8 exits below C7C8 exits below C7

AnatomyAnatomy NeuroforaminaNeuroforamina
• Anteromedially uncovertebral jointAnteromedially uncovertebral joint
• Posterolaterally facet jointPosterolaterally facet joint
• Superiorly pedicle of above vertebraeSuperiorly pedicle of above vertebrae
• Inferiorly pedicle of below vertebraeInferiorly pedicle of below vertebrae
• Medially edge vertebral end plates & Medially edge vertebral end plates & intervertebral discsintervertebral discs

AnatomyAnatomy NeuroforaminaNeuroforamina
• Foramina largest at C2-3Foramina largest at C2-3
• Progressive decrease in Progressive decrease in size to the C6-7 levelsize to the C6-7 level
• Nerve root occupies 25-Nerve root occupies 25-33% foraminal space33% foraminal space

DefinitionDefinition
• RadiculopathyRadiculopathy– Functional disturbance of spinal nerve rootFunctional disturbance of spinal nerve root
• MyelopathyMyelopathy– Functional disturbance of the spinal cordFunctional disturbance of the spinal cord

Vs.Vs.
RadiculopathyRadiculopathyIncidence
Natural History
Diagnosis ?
MyelopathyMyelopathy

Cervical RadiculopathyCervical RadiculopathyRisk FactorsRisk Factors
• Heavy lifting Heavy lifting – > 25lbs repetitively> 25lbs repetitively
• SmokingSmoking
• Driving/operating Driving/operating vibrating equipmentvibrating equipment
• Previous trauma 15%Previous trauma 15%

Cervical RadiculopathyCervical Radiculopathy EpidemiologyEpidemiology
• Annual Annual incidence .85/1000incidence .85/1000– Peak 4Peak 4thth & 5 & 5thth decades decades– 2.1/1000 incidence2.1/1000 incidence
• Prevalence 3.3/1000Prevalence 3.3/1000– Less frequent than Less frequent than
lumbar spinelumbar spine
• M > F ?M > F ?
• C6 & C7 rootsC6 & C7 roots – most commonly affectedmost commonly affected
• Degenerative changes Degenerative changes > disc herniation> disc herniation

Cervical RadiculopathyCervical Radiculopathy EpidemiologyEpidemiology
• Younger patientsYounger patients– ““SoftSoft” disc herniation” disc herniation– Acute injury causing Acute injury causing
foraminal foraminal impingementimpingement
• Older patientsOlder patients– Foraminal narrowing Foraminal narrowing
from from osteophytesosteophytes– More axial neck & More axial neck &
interscapular paininterscapular pain

Natural HistoryNatural History
• RadiculopathyRadiculopathy– 43% no sx after 4 43% no sx after 4
wkswks– 30% mild sx.30% mild sx.– 27% continue to 27% continue to
have significant sx.have significant sx.
• Lee and Turner 1963 Lee and Turner 1963 BMJBMJ
• MyelopathyMyelopathy– Epstein: Epstein:
• 36% improve• 20% deteriorated
– Symon:• 67% relentless
progression
– Clark & Robinson:• 50% deteriorated.

Differential DiagnosisDifferential Diagnosis Cervical RadiculopathyCervical Radiculopathy
• TumorsTumors– IntracranialIntracranial– Axillary schwannomaAxillary schwannoma– OsteochondromaOsteochondroma
• UE mononeuropathiesUE mononeuropathies– RadialRadial– MedianMedian– UlnarUlnar
• Thoracic Outlet SyndromeThoracic Outlet Syndrome

Differential DiagnosisDifferential Diagnosis Cervical RadiculopathyCervical Radiculopathy
• Brachial Plexus disordersBrachial Plexus disorders• Primary shoulder diseasePrimary shoulder disease
– Rotator cuffRotator cuff– Adhesive capsulitisAdhesive capsulitis– Glenoid cystGlenoid cyst
• Epidural varicose veinsEpidural varicose veins• Vertebral artery dissectionVertebral artery dissection• InfectionsInfections

Referred Pain DistributionReferred Pain Distribution
– OsteophytesOsteophytes• Uncovertebral or Uncovertebral or
Facet jointsFacet joints
– Disc herniationDisc herniation• Central or Lateral Central or Lateral
extrusionextrusion
– CombinationCombination

Clinical PresentationClinical PresentationHistoryHistory
• Radiating arm painRadiating arm pain• Sensibility lossSensibility loss• Motor deficitsMotor deficits• Reflex changesReflex changes

Clinical PresentationClinical PresentationHistoryHistory
• Disc herniation afterDisc herniation after – TraumaTrauma– Repetitive activityRepetitive activity– Awaken at nightAwaken at night
• PainPain– SevereSevere– BurningBurning– Tooth-ache qualityTooth-ache quality
• DysphagiaDysphagia

Clinical PresentationClinical PresentationHistoryHistory
• Dermatomal distributionDermatomal distribution• Example: C5-C6 DiscExample: C5-C6 Disc
– b/t vertebral body C5 + C6 b/t vertebral body C5 + C6 – C6 nerve root compressionC6 nerve root compression
• Presenting symptoms Presenting symptoms – Level of nerve compressionLevel of nerve compression

HISTORYHISTORY
• 65 year old male , failed 65 year old male , failed B. CTR and B. RCT B. CTR and B. RCT Surgery.Surgery.
• 54 year old male, WC, 54 year old male, WC, failed posterior failed posterior foraminotomy.foraminotomy.

Physical ExamPhysical Exam• SensationSensation• Motor strengthMotor strength• Range of motionRange of motion• Deep tendon reflexesDeep tendon reflexes

Physical ExamPhysical ExamC4 RadiculopathyC4 Radiculopathy
• C3-4 levelC3-4 level
• UncommonUncommon
• Weak deltoidWeak deltoid
• Variable sensory loss Variable sensory loss
• Often severe radiating painOften severe radiating pain – shoulder & scapulashoulder & scapula
• Rule out rotator cuff dzRule out rotator cuff dz

Physical ExamPhysical ExamC5 RadiculopathyC5 Radiculopathy
• C4-5 levelC4-5 level– 33rdrd most common most common
• Weak deltoid, shoulder Weak deltoid, shoulder external rotatorsexternal rotators– perhaps biceps perhaps biceps
• Biceps reflexBiceps reflex• Pain & Sensory loss Pain & Sensory loss
– lateral shoulderlateral shoulder– lateral brachiumlateral brachium

Physical ExamPhysical ExamC6 RadiculopathyC6 Radiculopathy
• C5-6 levelC5-6 level• Weak biceps & wrist Weak biceps & wrist
extensionextension• Brachioradialis reflexBrachioradialis reflex• Pain & sensory loss Pain & sensory loss
– radial handradial hand– lateral brachiumlateral brachium

Physical ExamPhysical ExamC7 RadiculopathyC7 Radiculopathy
• C6-7 levelC6-7 level• Weak triceps, wrist Weak triceps, wrist
flexion, finger ext flexion, finger ext • Triceps reflexTriceps reflex• Pain & sensory lossPain & sensory loss
– middle fingermiddle finger– posterolateral armposterolateral arm

Physical ExamPhysical ExamC8 RadiculopathyC8 Radiculopathy
• C7-T1 levelC7-T1 level– InfrequentInfrequent
• Weak gripWeak grip• Pain & sensory loss Pain & sensory loss
– ulnar handulnar hand– forearmforearm

Physical ExamPhysical ExamT1 RadiculopathyT1 Radiculopathy
• T1-2 levelT1-2 level– Very uncommonVery uncommon
• Weak hand intrinsicsWeak hand intrinsics• Pain & sensory loss Pain & sensory loss
– ulnar forearmulnar forearm– elbowelbow

Physical ExamPhysical ExamProvocative TestsProvocative Tests
• Spurling TestSpurling Test• Manual Cervical DistractionManual Cervical Distraction• Valsalva ManeuverValsalva Maneuver• Shoulder Abduction SignShoulder Abduction Sign• L’hermitte’s SignL’hermitte’s Sign

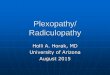
Physical ExamPhysical ExamSpurling TestSpurling Test
• Extending the neckExtending the neck• Rotating headRotating head• Downward pressure on headDownward pressure on head• Positive if pain radiates to Positive if pain radiates to
side patient’s head is pointedside patient’s head is pointed– Positive Spurling in 71% football Positive Spurling in 71% football
players c recent burner players c recent burner (Levitz et al (Levitz et al AM J Sp MedAM J Sp Med 1997) 1997)

Physical ExamPhysical ExamManual Cervical DistractionManual Cervical Distraction
• Supine patientSupine patient
• Gentle manual axial Gentle manual axial distractiondistraction– Up to ~30lbsUp to ~30lbs
• Positive response Positive response reduction neck and reduction neck and limb symptomslimb symptoms

Physical ExamPhysical ExamValsalva TestValsalva Test
• Patient bears downPatient bears down• Increased intrathecal Increased intrathecal
pressure pressure • Symptoms reproducedSymptoms reproduced

Physical ExamPhysical ExamShoulder Abduction SignShoulder Abduction Sign
• While sitting, patient places hand of While sitting, patient places hand of affected extremity on headaffected extremity on head
• Support of extremity in scapular Support of extremity in scapular planeplane
• Positive test is reduction of Positive test is reduction of symptomssymptoms

Physical ExamPhysical ExamL’hermitte’s SignL’hermitte’s Sign
• Neck flexionNeck flexion• Electric-like sensation radiating Electric-like sensation radiating
down spine and/or extremitiesdown spine and/or extremities– Cervical spondylosisCervical spondylosis– Multiple sclerosisMultiple sclerosis– TumorTumor

Clinical PresentationClinical PresentationMyelopathyMyelopathy
• Gait changesGait changes• Bowel(18%) or Bowel(18%) or
bladder(15%)dysfunctionbladder(15%)dysfunction• Simultaneous LE Simultaneous LE
changeschanges– sensory or motorsensory or motor
• Diffuse hyperreflexiaDiffuse hyperreflexia– Upper motor neuron changesUpper motor neuron changes
• 20% no neck or arm pain20% no neck or arm pain

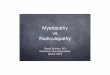
Hoffman’s ReflexHoffman’s ReflexMyelopathyMyelopathy
• Suddenly extend Suddenly extend middle finger DIPmiddle finger DIP
• Reflex finger flexionReflex finger flexion• When asymmetric When asymmetric
indicative spinal cord indicative spinal cord impingementimpingement

Inverted Radial ReflexInverted Radial ReflexMyelopathyMyelopathy
• Tapping of distal Tapping of distal brachioradialis brachioradialis tendon tendon
• Spastic contraction Spastic contraction of finger flexorsof finger flexors

Grip & Release TestGrip & Release TestMyelopathyMyelopathy
• Form fist and Form fist and extend fingers extend fingers rapidlyrapidly
• Repeat 20x in 10 Repeat 20x in 10 secondsseconds

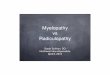
Finger Escape SignFinger Escape SignMyelopathyMyelopathy
• Hold fingers adducted Hold fingers adducted and extendedand extended
• Small & ring fingers fall Small & ring fingers fall into flexion abductioninto flexion abduction– Usually within 30 secondsUsually within 30 seconds

RadiologyRadiology
• RadiographsRadiographs• MyelogramMyelogram• CT ScanCT Scan• CT MyelogramCT Myelogram• MRIMRI• ElectrodiagnosticsElectrodiagnostics

RadiographsRadiographsCervical RadiculopathyCervical Radiculopathy
• Only initial screening toolOnly initial screening tool– Rule out other insidious diseasesRule out other insidious diseases
• OsteophytesOsteophytes– Oblique viewsOblique views
• Uncovertebral hypertrophyUncovertebral hypertrophy
• SubluxationSubluxation– Lateral flexion extensionLateral flexion extension

RadiographsRadiographsCervical RadiculopathyCervical Radiculopathy
• 30% asymptomatic individuals over 30 yo 30% asymptomatic individuals over 30 yo will have degenerative changeswill have degenerative changes
• 70% by 70 yo will have degenerative 70% by 70 yo will have degenerative changes on x-raychanges on x-ray

MyelogramMyelogram Cervical RadiculopathyCervical Radiculopathy
• Intrathecal contrast then X-rayIntrathecal contrast then X-ray• Assess space occupying lesions by Assess space occupying lesions by
changes in contourchanges in contour– Dural sacDural sac– Nerve rootsNerve roots– Spinal cordSpinal cord

MyelogramMyelogram Cervical RadiculopathyCervical Radiculopathy
• Infection risk Infection risk • Difficulty distinguish nature of defectDifficulty distinguish nature of defect
– Cervical disc herniationCervical disc herniation– OsteophyteOsteophyte
• Often used in Often used in conjunction with CTconjunction with CT

CTCTCervical RadiculopathyCervical Radiculopathy
• More sensitive than MRI to More sensitive than MRI to bony changesbony changes
• Limited ability to detect Limited ability to detect soft tissue lesionssoft tissue lesions
• Ionizing radiationIonizing radiation

CT MyelogramCT Myelogram Cervical RadiculopathyCervical Radiculopathy
• Myelography followed by CT scanMyelography followed by CT scan• Better detect bony and space Better detect bony and space
occupying lesionsoccupying lesions– Better anatomic information than MRI?Better anatomic information than MRI?
• Risk radiation & infectionRisk radiation & infection

MRIMRICervical RadiculopathyCervical Radiculopathy
• Noninvasive, often only study neededNoninvasive, often only study needed
• More sensitive to changes disc, More sensitive to changes disc, spinal cord, nerve root & surrounding spinal cord, nerve root & surrounding soft tissuessoft tissues– 25% asymptomatic patients > 40yo findings of 25% asymptomatic patients > 40yo findings of
HNP or foraminal stenosisHNP or foraminal stenosis

Radiology DataRadiology DataCervical RadiculopathyCervical Radiculopathy
• Blinded retrospectiveBlinded retrospective• Correctly predicted cervical spine Correctly predicted cervical spine
surgical pathology surgical pathology – MRI MRI 88%88%– CT Myelo CT Myelo 81%81%– Myelography alone Myelography alone 58%58%– CT alone CT alone 50%50%
Brown et al Brown et al Am J NeuroradiologyAm J Neuroradiology 1988 1988

Treatment Treatment Non-Operative Non-Operative Operative Operative• RestRest
• ImmobilizationImmobilization
• MedicationMedication
• Physical TherapyPhysical Therapy
• Cervical tractionCervical traction
• InjectionsInjections
• IndicationsIndications
• Anterior ApproachAnterior Approach
• Posterior ApproachPosterior Approach
• ResultsResults

Non-Operative TreatmentNon-Operative TreatmentCervical RadiculopathyCervical Radiculopathy
• First line therapyFirst line therapy– Neck painNeck pain– Cervical radiculopathyCervical radiculopathy
• Most do well in 6 weeksMost do well in 6 weeks– 25% persistent or worsening of symptoms25% persistent or worsening of symptoms

ImmobilizationImmobilizationCervical RadiculopathyCervical Radiculopathy
• Soft cervical collarSoft cervical collar• Limits range of motionLimits range of motion• Minimize nerve root irritationMinimize nerve root irritation• Relieve paraspinal muscle spasmRelieve paraspinal muscle spasm
– Hopefully reduce inflammationHopefully reduce inflammation

MedicationsMedicationsCervical RadiculopathyCervical Radiculopathy
• NSAIDsNSAIDs– First choiceFirst choice– Reduce nerve root inflammationReduce nerve root inflammation
• NarcoticsNarcotics• Oral steroidsOral steroids• Local steroidsLocal steroids• Epidural steroidsEpidural steroids

InjectionsInjectionsCervical RadiculopathyCervical Radiculopathy
• Epidural steroidsEpidural steroids• Root injectionsRoot injections• Facet blocksFacet blocks
– Less often than in lumbar Less often than in lumbar spinespine
– Anatomic considerationsAnatomic considerations– Experienced staffExperienced staff

Physical TherapyPhysical TherapyCervical RadiculopathyCervical Radiculopathy
• Cervical TractionCervical Traction
• Aerobic exerciseAerobic exercise
• Postural awarenessPostural awareness
• Spinal extensor strengtheningSpinal extensor strengthening
• ThermotherapyThermotherapy
• AcupunctureAcupuncture

Cervical TractionCervical TractionCervical RadiculopathyCervical Radiculopathy
• Soft disc herniationsSoft disc herniations– Often younger patientsOften younger patients
• Less successfulLess successful– SpondylosisSpondylosis– Narrow spinal canalsNarrow spinal canals
• 20-30lb usually effective distractive force20-30lb usually effective distractive force• Long-term basisLong-term basis
– select patientsselect patients

Non-Operative TreatmentNon-Operative TreatmentCervical RadiculopathyCervical Radiculopathy
• Response in days to weeksResponse in days to weeks• Protracted non-op care Protracted non-op care notnot
recommended in presence ofrecommended in presence of– Persistent, severe painPersistent, severe pain– WeaknessWeakness– Major sensibility lossMajor sensibility loss– Myelopathy with obvious cord findingsMyelopathy with obvious cord findings

Operative TreatmentOperative TreatmentIndicationsIndications
• Compression of nerve Compression of nerve root or spinal cordroot or spinal cord
• InstabilityInstability– SpondylolisthesisSpondylolisthesis– RetrolisthesisRetrolisthesis
• DeformityDeformity
• Failed medical Failed medical managementmanagement
• Significant neurologic Significant neurologic deficitdeficit– motor weaknessmotor weakness
• Severe cervical Severe cervical myelopathymyelopathy

ApproachApproach• AnteriorAnterior
– ACDFACDF– CorpectomyCorpectomy
– 1 or 2 level dz. 1 or 2 level dz. • (central or lateral)(central or lateral)• Hard or soft discHard or soft disc
– KyphosisKyphosis
• PosteriorPosterior– ForaminotomyForaminotomy
• Soft lateral disc.Soft lateral disc.
– LaminectomyLaminectomy– Laminectomy + fusionLaminectomy + fusion– LaminoplastyLaminoplasty– 3 or more levels with 3 or more levels with
preservation of lordosis.preservation of lordosis.

Anterior ApproachAnterior ApproachCervical RadiculopathyCervical Radiculopathy
• Supine on tableSupine on table• Left sided approach Left sided approach
– if C4-5 or lowerif C4-5 or lower– Recurrent laryngeal Recurrent laryngeal
nervenerve
• Can utilize either side Can utilize either side if above C4if above C4

Anterior ApproachAnterior ApproachCervical RadiculopathyCervical Radiculopathy
• Recurrent laryngeal Recurrent laryngeal nerve on leftnerve on left– Predictable coursePredictable course– Between trachea and Between trachea and
esophagusesophagus– Ascends from looping Ascends from looping
around aortic archaround aortic arch

Anterior ApproachAnterior ApproachCervical RadiculopathyCervical Radiculopathy
• Once at spine level, spinal needle place into Once at spine level, spinal needle place into disc spacedisc space
• Lateral radiograph take to confirm locationLateral radiograph take to confirm location

Anterior ApproachAnterior ApproachCervical RadiculopathyCervical Radiculopathy
• Technique described by Robinson & Technique described by Robinson & Smith 1955Smith 1955– Use tricortical iliac crest graftUse tricortical iliac crest graft

Cloward Technique Cloward Technique Cervical RadiculopathyCervical Radiculopathy
• Dowel type graftDowel type graft• Variable size, bicorticalVariable size, bicortical• Sized drill hole carefully placed into Sized drill hole carefully placed into
center involved disc spacecenter involved disc space

Bailey & BadgleyBailey & BadgleyCervical RadiculopathyCervical Radiculopathy
• Trough made into vertebral bodiesTrough made into vertebral bodies– Above and below involved discAbove and below involved disc
• Unicortical Unicortical – ½ inch width½ inch width– 3/16 inch depth3/16 inch depth

Simmons & BhallaSimmons & BhallaCervical RadiculopathyCervical Radiculopathy
• Keyhole techniqueKeyhole technique• Beveled bicortical graftBeveled bicortical graft
– 14-18 degrees ideal14-18 degrees ideal– Bevel up for superior vertebral bodyBevel up for superior vertebral body– Bevel down for inferior vertebral bodyBevel down for inferior vertebral body

ACDFACDF
• 42 yo with both C6 42 yo with both C6 and C7 and C7 radiculopathyradiculopathy

Posterior ApproachPosterior ApproachCervical RadiculopathyCervical Radiculopathy
• Described two decades Described two decades b/f anterior popularizedb/f anterior popularized
• Utilized in numerous Utilized in numerous situationssituations– Lateral soft disc herniationLateral soft disc herniation– Midline spondylotic Midline spondylotic
myelopathymyelopathy

Posterior ApproachPosterior ApproachCervical RadiculopathyCervical Radiculopathy
• Radiculopathy Radiculopathy without neck painwithout neck pain
• Keyhole Keyhole foraminotomyforaminotomy– Lateral discsLateral discs

Posterior ApproachPosterior ApproachCervical RadiculopathyCervical Radiculopathy
Raynor et al Raynor et al NeurosurgNeurosurg 1983 1983
• 3-5mm nerve root exposure3-5mm nerve root exposure• 1/3 removal facet joint1/3 removal facet joint
• Similar anterior Similar anterior decompressiondecompression– work outside direct visionwork outside direct vision

Posterior ApproachPosterior ApproachCervical RadiculopathyCervical RadiculopathyRaynor et al Raynor et al J NeurosurgJ Neurosurg 1985 1985
• 50% B facetectomies50% B facetectomies• 5mm nerve root 5mm nerve root
– exposureexposure
• Spinal stability intactSpinal stability intact
• 70% B facetectomies70% B facetectomies
• 8-10mm nerve root 8-10mm nerve root – exposureexposure
• Significant reduction Significant reduction of spine stability to of spine stability to shearshear

ANT. CORPECTOMY & ANT. CORPECTOMY & POST FORAMINOTOMYPOST FORAMINOTOMY
• 59 yo businessman 59 yo businessman with severe R. arm with severe R. arm pain. pain.


Posterior ApproachPosterior ApproachCervical MyelopathyCervical Myelopathy
• LaminoplastyLaminoplasty– Stenosis Stenosis

Cervical LaminoplastyCervical Laminoplasty
• 81 year old with 81 year old with quadriparesis, loss quadriparesis, loss of function of all 4, of function of all 4, worse with BUE worse with BUE than BLE.than BLE.

CombinedCombined
• 42 year old with 42 year old with progressive progressive quadriplegia in the quadriplegia in the ERER

CombinedCombined

CombinedCombined
• 64 year old male, 64 year old male, loss function of loss function of right arm, unsteady right arm, unsteady gait.gait.

CombinedCombined

OITEOITE

OITE 2000-#73OITE 2000-#73• A 45yo man has had spontaneous neck and right arm pain for the A 45yo man has had spontaneous neck and right arm pain for the
past 2 days, and he states that the pain is relieved when he places his past 2 days, and he states that the pain is relieved when he places his hand on the top of his head. Examination reveals decreased hand on the top of his head. Examination reveals decreased sensation on the dorsum of the first web space, weakness in the sensation on the dorsum of the first web space, weakness in the wrist extensors, and an absent brachioradialis reflex. The remainder wrist extensors, and an absent brachioradialis reflex. The remainder of the exam is unremarkable. What is the most likely diagnosis?of the exam is unremarkable. What is the most likely diagnosis?1—Double-crush phenomenon with carpal tunnel syndrome & cervical disk 1—Double-crush phenomenon with carpal tunnel syndrome & cervical disk herniation at C5-6herniation at C5-62—Cervical disk herniation at C6-72—Cervical disk herniation at C6-73—Cervical disk herniation at C5-6 with myelopathy3—Cervical disk herniation at C5-6 with myelopathy4—Acute cervical disk herniation at C5-64—Acute cervical disk herniation at C5-65—A shoulder impingement lesion & cervical disk herniation at C6-75—A shoulder impingement lesion & cervical disk herniation at C6-7

OITE 2000-#73OITE 2000-#73• A 45yo man has had spontaneous neck and right arm pain for the A 45yo man has had spontaneous neck and right arm pain for the
past 2 days, and he states that the pain is relieved when he places his past 2 days, and he states that the pain is relieved when he places his hand on the top of his head. Examination reveals decreased hand on the top of his head. Examination reveals decreased sensation on the dorsum of the first web space, weakness in the sensation on the dorsum of the first web space, weakness in the wrist extensors, and an absent brachioradialis reflex. The remainder wrist extensors, and an absent brachioradialis reflex. The remainder of the exam is unremarkable. What is the most likely diagnosis?of the exam is unremarkable. What is the most likely diagnosis?1—Double-crush phenomenon with carpal tunnel syndrome & cervical disk 1—Double-crush phenomenon with carpal tunnel syndrome & cervical disk herniation at C5-6herniation at C5-62—Cervical disk herniation at C6-72—Cervical disk herniation at C6-73—Cervical disk herniation at C5-6 with myelopathy3—Cervical disk herniation at C5-6 with myelopathy4—Acute cervical disk herniation at C5-64—Acute cervical disk herniation at C5-65—A shoulder impingement lesion & cervical disk herniation at C6-75—A shoulder impingement lesion & cervical disk herniation at C6-7

SAE Spine 2000 #2SAE Spine 2000 #2• A 60yo man underwent an anterior diskectomy and fusion for C4-A 60yo man underwent an anterior diskectomy and fusion for C4-
5 disk disease using a left-sided approach 1 week ago. He now 5 disk disease using a left-sided approach 1 week ago. He now reports a persistent dry cough and mild horseness. Pulmonary reports a persistent dry cough and mild horseness. Pulmonary evaluation shows evidence of a mild aspiration, and ear, nose, evaluation shows evidence of a mild aspiration, and ear, nose, and throat visualization shows laxity of the vocal cord on the left and throat visualization shows laxity of the vocal cord on the left side. What is the most likely explanation for these findings?side. What is the most likely explanation for these findings?1—Traction on the recurrent laryngeal nerve1—Traction on the recurrent laryngeal nerve2—Traction on the superior laryngeal nerve2—Traction on the superior laryngeal nerve3—Injury to the pharyngeal nerve branches when ligating the superior 3—Injury to the pharyngeal nerve branches when ligating the superior thyroid arterythyroid artery4—Direct trauma to the larynx from retractor blades4—Direct trauma to the larynx from retractor blades5—Direct injury to the vocal cords from endotracheal intubation5—Direct injury to the vocal cords from endotracheal intubation

SAE Spine 2000 #2SAE Spine 2000 #2• A 60yo man underwent an anterior diskectomy and fusion for C4-A 60yo man underwent an anterior diskectomy and fusion for C4-
5 disk disease using a left-sided approach 1 week ago. He now 5 disk disease using a left-sided approach 1 week ago. He now reports a persistent dry cough and mild horseness. Pulmonary reports a persistent dry cough and mild horseness. Pulmonary evaluation shows evidence of a mild aspiration, and ear, nose, evaluation shows evidence of a mild aspiration, and ear, nose, and throat visualization shows laxity of the vocal cord on the left and throat visualization shows laxity of the vocal cord on the left side. What is the most likely explanation for these findings?side. What is the most likely explanation for these findings?1—Traction on the recurrent laryngeal nerve1—Traction on the recurrent laryngeal nerve2—Traction on the superior laryngeal nerve2—Traction on the superior laryngeal nerve3—Injury to the pharyngeal nerve branches when ligating the superior 3—Injury to the pharyngeal nerve branches when ligating the superior thyroid arterythyroid artery4—Direct trauma to the larynx from retractor blades4—Direct trauma to the larynx from retractor blades5—Direct injury to the vocal cords from endotracheal intubation5—Direct injury to the vocal cords from endotracheal intubation

OITE 1999-#24OITE 1999-#24• An otherwise healthy 79yo woman has had An otherwise healthy 79yo woman has had
deteriorating function in her hands for the past 6 deteriorating function in her hands for the past 6 months when she is knitting or buttoning. She also months when she is knitting or buttoning. She also reports neck pain and stiffness and diminished reports neck pain and stiffness and diminished sensation in the left hand. Examination reveals a sensation in the left hand. Examination reveals a broad-based gait, weakness in the interossei in the left broad-based gait, weakness in the interossei in the left hand, a positive left Hoffman sign, and bilateral hand, a positive left Hoffman sign, and bilateral upgoing toes. What is the most likely diagnosis?upgoing toes. What is the most likely diagnosis?1—Syringomyelia1—Syringomyelia2—Pathologic fracture of C4 with incomplete spinal cord injury2—Pathologic fracture of C4 with incomplete spinal cord injury3—Amytrophic lateral sclerosis3—Amytrophic lateral sclerosis4—Multiple sclerosis4—Multiple sclerosis5—Cervical spondylotic myelopathy5—Cervical spondylotic myelopathy

OITE 1999-#24OITE 1999-#24• An otherwise healthy 79yo woman has had deteriorating An otherwise healthy 79yo woman has had deteriorating
function in her hands for the past 6 months when she is function in her hands for the past 6 months when she is knitting or buttoning. She also reports neck pain and knitting or buttoning. She also reports neck pain and stiffness and diminished sensation in the left hand. stiffness and diminished sensation in the left hand. Examination reveals a broad-based gait, weakness in the Examination reveals a broad-based gait, weakness in the interossei in the left hand, a positive left Hoffman sign, and interossei in the left hand, a positive left Hoffman sign, and bilateral upgoing toes. What is the most likely diagnosis?bilateral upgoing toes. What is the most likely diagnosis?1—Syringomyelia1—Syringomyelia2—Pathologic fracture of C4 with incomplete spinal cord injury2—Pathologic fracture of C4 with incomplete spinal cord injury3—Amytrophic lateral sclerosis3—Amytrophic lateral sclerosis4—Multiple sclerosis4—Multiple sclerosis5—Cervical spondylotic myelopathy5—Cervical spondylotic myelopathy