Embed Size (px)
Citation preview

British lournal of Haematology. 1989. 73, 403-409
Desferrioxamine ototoxicity: evaluation of risk factors in thalassaemic patients and guidelines for safe dosage
JOHN B. PORTER, MERVYN S. JASWON, ERNST R . HUEHNS. CHARLES A. EAST* AND JONATHAN W. P . HAZELL* Department of Clinical'Haematology, University College and Middlesex School of Medicine, London WCl E 6 H X , and *Department of Otolaryngology, Royal Ear Hospital, London WCl E 6AU
Received 5 May 1989; accepted for publication 17 July 1 989
Summary. Forty-seven patients with thalassaemia have been studied to define risk factors for development of sensorineural hearing loss, and to establish guidelines for safe chelation. Sensorineural hearing loss was only present in patients who had previously received desferrioxamine (DFO). The two most signilkant risk factors were the maximum dose of DFO previously received (P<O.Ol), and a serum ferriti of <2000 pg/l at that time (P<O.OOl). A therapeutic index
obtained from the ratio of the mean daily dose of DFO mg/kg divided by the serum ferritin identifies patients with a ratio of >0.025 as at risk of sensorineural hearing loss (P<O.OOl) and can be used as a guideline for safe DFO dosage. Follow-up audiometry of the affected patients over a 2-year period indicated that adjustment of the dose to a therapeutic index of <0.025 resulted in the stabilization of hearing loss in seven patients and improvement in two.
The chelator desferrioxamine (DFO) has been used since the late 1960s to increase iron excretion and hence reduce iron overload. With the use of higher doses of DFO and its administration to less iron overloaded patients, this drug has recently been implicated as a cause of both retinal (Davies et al, 1983: Borgna-Pignatti et al. 1984; Oliveri et al, 1986) and auditory toxicity in man (Zipursky, 1985; Orton et al. 1985: Guerin et al. 1985: Oliveri et al. 1986). In view of the importance of this drug in delaying the fatal consequences of iron overload (Barry et aJ, 1974: Pippard et d, 1978), it is clearly undesirable to reduce or withdraw the administration of this drug unless absolutely necessary. However, the contradictory evidence regarding the relationship between DFO administration and auditory toxicity can make these decisions dBcult. Some investigators have identified a high degree of iron overload as a possible risk factor (De Virgilis et al, 1979). whereas others suggest that high DFO doses associated with low serum ferritin values and young age are risk factors (Oliveri et al, 1986). Furthermore, audiometric abnormalities associated with extramedullary bone marrow expansion have been described in patients with thalassaemia not receiving DFO (Hazel1 i? Modell. 1976: Mchtosh. 1976). There is no evidence in animal models for DFO mediated
Correspondence: Dr J. B. Porter. Department of Clinical Haemato- logy. University College and Middlesex School of Medicine, London WClE 6AX.
ototoxicity (Shirane i? Harrison, 1987), in contrast to the good evidence for DFO mediated visual toxicity (Arden, 1986). An additional uncertainty is what action to take if auditory abnormalities are identified in a patient receiving DFO.
In an attempt to clarify these points this study has investigated a number of factors. Firstly, risk factors for the development of abnormal audiometric function, such as dose of DFO. age, iron overload status and possible extramedullary bony expansion have been identified. Secondly, a therapeutic safety index for the use of DFO has been derived, combining the risk factors for ototoxicity that we have identified as the most important. so that guidelines for the further use of DFO can be given. Finally, patients with auditory abnormalities have been followed for 2 years to determine the influence of DFO dose modification on the evolution of auditory function,
PATIENTS AND METHODS
47 patients with thalassaemia attending the Haematology Department of University College Hospital, London. were studied (Table I). 30 patients had fl-thalassaemia major (age range 5-28 years: 13 male, 17 female) and 17 patients had thalassaemia intermedia (age range 5-62 years: 7 male, 10 female). Patients with thalassaemia major were transfused regularly to maintain their haemoglobin above 11 g/dl, whilst those with thalassaemia intermedia received trans- fusions intermittently for varying periods of t i e for specific
403

404 indications, e.g. to help induce puberty or during pregnancy.
Initially the serum ferritin and DFO dose, at the time of suspected ototoxicity. were examined. However, for reasons discussed later, the maximum dose of DFO ever received by the patient, together with the serum ferritin at that time, were also determined. DFO dose was expressed as follows: the total amount of DFO in milligrammes (mg) received over the course of a week was divided by 7 and stated in mg/kg/24 h. This entailed some degree of approximation, as it relied on patients’ accounts of their compliance. Most patients received chelation 5 nights per week.
In total, 37 patients had previously received DFO, this comprised all 30 patients with thalassaemia major and seven patients with thalassaemia intermedia. The remaining 10 patients with thalassaemia intermedia had only rarely been transfused, e.g. pre-operatively and never received DFO. The doses ofDFO ranged betwen 14 and 98 mg/kg 24 h, and were administered as an infusion subcutaneously, or intrave- nously via an indwelling catheter (Portacath) in three patients. All patients received ascorbic acid on days when they were chelated, in a dose of between 50 and 200 mg orally, apart from those patients commencing high dose desferrioxamine (Porter & Huehns, 1989).
An otological history was taken and pure tone audiometry (PTA) performed on all patients as well as impedance audiometry when indicated. Bone conduction thresholds were performed where the PTA was abnormal to determine whether the hearing loss was conductive or sensorineural. For the purposes of this study, normal hearing was classified as being between 0 and 20 decibels (dB), moderate hearing loss between 20 and 45 dB, and severe when greater than 45 dB. In order to localize the anatomical site of sensorineural damage auditory brainstem responses (ABR) (Mason et al, 1988) were recorded in two patients with severe hearing loss. ABRs could not be obtained from the other two patients with severe hearing loss as their hearing deficit at the frequency measured by the test (3 kHz) was too profound. In the two patients with both thalassaemia intermedia and sensori- neural hearing loss polytomography of the temporal bone was performed to see whether marrow expansion was present, as they had other radiological evidence of this process (X-ray mandible with widened medulla and nar- rowed cortex). Follow-up audiometry was performed in patients with sensorineural hearing loss at approximately 6- monthly intervals for a 2-year period. A variation of greater than 10 dB between follow-up tests on PTA was accepted as significant.
In all patients with evidence of progressive sensorineural hearing loss receiving DFO, their dose was reduced, and in one patient where deterioration continued despite this, the drug was withdrawn completely for 1 month before restart- ing at a reduced dose.
The degree of iron overload was calculated for each patient from the mean serum ferritin levels over a period of 6 months prior to audiometry. Ferritin measurement was by an in- house radioimmunoassay (second antibody precipitation): all values for ferritin are referrable to the WHO International Standard (Human Liver) 80-602. kindly provided by the
Iohn B. Porter et al National Institute for Biological Standards and Control, London, England (ICSH, 1985).
Statistical analysis was performed using the Chi-squared test. unless otherwise stated.
RESULTS
Audiological investigations Nine of the 37 patients (Table 11) who had received DFO (24%) had abnormal audiograms and displayed bilateral symmetrical high frequency sensorineural hearing loss. Four of these patients (I, 2 , 4 and 9) developed severe symptomatic hearing loss which in patients 2 and 4 was greater than 45 dB from 0.2 5 to 6.0 kHz, worse in the higher frequencies, and they now require powerful hearing aids. Patient 1 had a rapid fall off to 80 dB at 8 kHz, and patient 9 a fall off to 100 dB at 6- 8 kHz. Two patients (1 and 2) developed tinnitus. and patient 2 a vestibular neuropathy. Auditory brainstem responses in patients 1 and 9 showed no delay in conduction with preservation of the normal wave pattern. Polytomography of the temporal bone in patients 8 and 9 showed no evidence of narrowing of the internal auditory meatus.
Three of the patients (3, 5 and 8) on DFO with sensori- neural hearing loss also had a conductive hearing loss due to secretory otitis media and a fourth patient on DFO had a conductive hearing loss due to otosclerosis. Of the 10 patients who had not received DFO, none had a high frequency sensorineural hearing loss, but two had a conductive hearing loss, in one associated with secretory otitis media and in the other with a high jugular bulb which filled the lower part of the middle ear. Therefore, within the total group of 47 patients, six had a conductive hearing loss detected by audiometry (1 3%).
Risk factors for ototoxicity The relationship between the following parameters and sensorineural hearing loss was looked at in order to define risk factors for ototoxicity: age, dose of DFO. and degree of iron overload (Table I). There was no association between the age of the patient and hearing loss. Sensorineural hearing loss was only present in patients who had received DFO. At the time ototoxicity was suspected there was no relationship between the current dose of DFO and hearing loss. However, when the highest dose of DFO ever received by each patient was related to hearing loss a clear trend was observed. AII patients with severe sensorineural hearing loss had received a maximum DFO dose > 3 5 mg/kg/24 h for at least 3 months (P< 0.01). However, this dose was not invariably associated with hearing loss as 12 patients with normal hearing had received in excess of this dose. When the degree of iron overload was looked at it was found that a low serum ferritin was also a risk factor for sensorineural hearing loss. All patients with sensorineural hearing loss had a serum ferritin of <2000 pg/l at the time of the maximum dose of DFO previously received (P<O.OOl ) (Fig 1). However, a low ferritin was not invariably associated with hearing loss as six patients with normal hearing had serum femtiis of < 2000 yg/l when receiving their maximum DFO dose (Table I).
Desferrioxamine Dosage and Ototoxicity 405
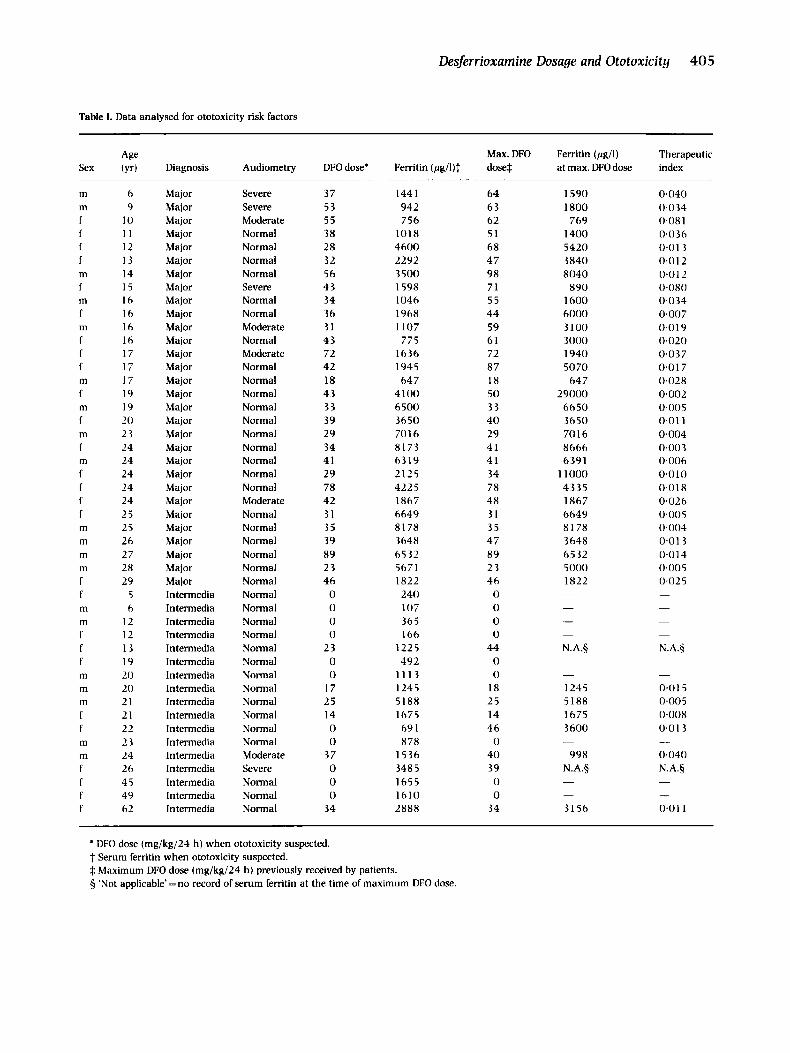
Table I. Data analysed for ototoxicity risk factors
Sex
m m f f f f m f m f m f f f m f m f m f m f f f f m rn rn rn f f m m f f f m m m f f m m f f f f
-
Age (Yr)
6 9
10 11 12 13 14 15 16 I6 I6 16 17 17 17 19 19 20 23 24 24 24 24 24 25 25 26 27 28 29
5 6
12 12 13 19 20 20 21 21 22 23 24 26 45 49 62
- Diagnosis
Major Major Major Major Major Major Major Major Major Major Major Major Major Major Major Major Major Major Major Major Major Major Major Major Major Major Major Major Major Major Intermedia Intermedia Intermedia Intermedia Intermedia Intermedia Intermedia Intermedia Intermedia Intermedia Intermedia Intermedia Intermedia Intermedia Intermedia Intermedia Intermedia
Audiometry
Severe Severe Moderate Normal Normal Normal Normal Severe Normal Normal Moderate Normal Moderate Normal Normal Normal Normal Normal Normal Normal Normal Normal Normal Moderate Normal Normal Normal Normal Normal Normal Normal Normal Normal Normal Normal Normal Normal Normal Normal Normal Normal Normal Moderate Severe Normal Normal Normal
DFO dose'
37 53 55 38 28 32 56 43 34 36 31 43 72 42 18 43 33 39 29 34 41 29
42 31 35 39 89 23 46 0 0 0 0
2 3 0 0
1 7 25 14 0 0
37 0 0 0
34
78
Max. DFO Ferritin (&I)? dose$
- 1441 942 756
1018 4600 2292 3 500 1598 1046 1968 1107
775 1636 1945
647 4100 6500 3650 7016 8173 6319 2125 422 5 1867 6649 81 78 3648 6532 5671 1822
240 107 365 166
1225 492
1113 1245 5188 1675 69 1 878
1536 348 5 1655 1610 2888
64 63 62 51 68 47 98 71 55 44 59 61 72 8 7 18 50 33 4 0 29 41 41 34 78 48 31 35 47 8 9 23 4 6 0 0 0 0
44 0 0
18 25 1 4 46 0
4 0 39 0 0
34
Ferritin (&I) Therapeutic at max. DFO dose index
1590
769 1400 5420 3840 8040
890 1600 6000 3100 3000 1940 5070
64 7 29000
6650 3650 7016 8666 6391
1 1000 4335 1867 6649 81 78 3648 6532 5000 1822
1 no0
-
- - -
N.A.S -
-
1245 5188 1675 3600
998 N.A.5
-
- -
31 56
0.040 0.034 0.08 1 0.036 0.01 3 0.0 12 0 . 0 1 2 0.080 0.034 0.007 0.019 0.020 0.037 0.01 7 0.028 0.002 0.005 0.01 1 0.004 0.003 0.006 0.01 0 0.01 8 0.026 0.005 0.004 0.01 3 0.014 0.005 0.025 -
-
-
-
N.A.S -
-
0.01 5 04105 0.008 0.01 3
0.040 N.A.5
-
- - 0 . 0 1 1
* UFO dose (mg/kg/24 h) when ototoxicity suspected. t Serum ferritin when ototoxicity suspected. $ Maximum DFO dose (mg/kg/24 h) previously received by patients. 5 'Not applicable' =no record of serum ferritin at the time of maximum DFO dose.
k
0
m
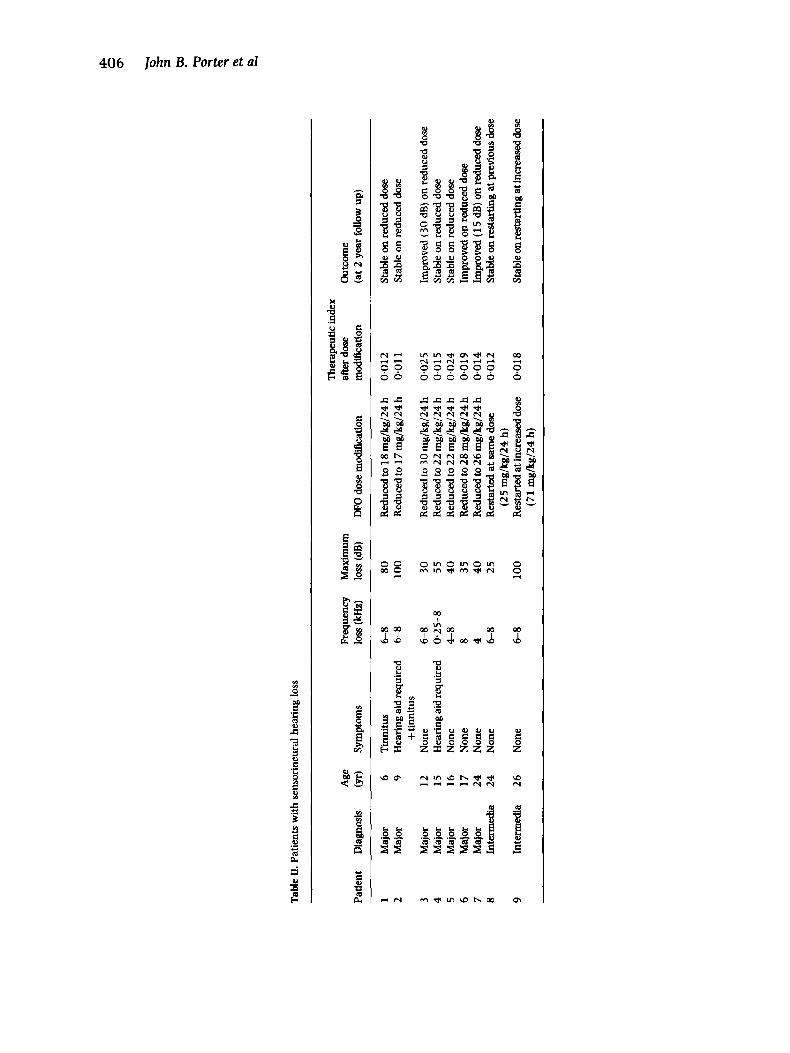
Tab
le II.
Pat
ient
s with
sen
sori
neur
al h
eari
ng lo
ss
The
rape
utic
inde
x A
ge
Freq
uenc
y M
axim
um
afte
r dos
e O
utco
me
Patie
nt
Dia
gnos
is
(yr)
Sy
mpt
oms
loss
(kH
z)
loss
(dB)
DFO
dose
mod
ific
atio
n m
odiic
atio
n (a
t 2 y
ear follow u
p)
1
2 9
Maj
or
Maj
or
Maj
or
Maj
or
Maj
or
Maj
or
Maj
or
Inte
rmed
ia
Inte
rmed
ia
6 9
12
15
16
17
24
24
26
Tin
nitu
s H
eari
ng ai
d re
quir
ed
Non
e H
eari
ng ai
d re
quir
ed
Non
e N
one
Non
e N
one + tin
nitu
s
Non
e
6-8
6-8
6-8
0.25
-8
4-8
8 4 6-8
6-8
80
10
0
30
55
4
0
35
40
25
100
Red
uced
to 1
8 rn
g/kg
/24
h R
educ
ed to
17
mg/
kg/2
4 h
Red
uced
to 3
0 m
g/kg
/24
h R
educ
ed to
22
mg/
kg/2
4 h
Red
uced
to 2
2 m
g/kg
/24
h R
educ
ed to
28
mg/
kg/2
4 h
Red
uced
to 2
6 m
g/kg
/24
h R
esta
rted
at s
ame
dose
Res
tart
ed a
t inc
reas
ed do
se
(25
mg/
kg/2
4 h)
(71
m/k
g/2
4 h
)
0.01
2 0.
01 1
0.02
5 0.
01 5
0.02
4 0.019
0.01
4 0.
012
0.01
8
Stab
le o
n re
duce
d do
se
Stab
le o
n re
duce
d do
se
Impr
oved
(30
dB) o
n re
duce
d do
se
Stab
le o
n re
duce
d do
se
Stab
le o
n re
duce
d do
se
Impr
oved
on
redu
ced
dose
Im
prov
ed (
1 5 dB) o
n re
duce
d do
se
Stab
le on
restarting a
t pre
viou
s dos
e
Stab
le on
restarting a
t inc
reas
ed do
se
Desferrioxamine Dosage and Ototoxicity 40 7
11000-
10000 -
9000 - - d . m 8000 - 3.
P)
-0
5 6000-
Y m E 5000-
C
k 4WO- Q)
Y
g 7 w o -
E .-
.- - .- - 3000 -
2000 - 1000 -
30000 1-
0-
normal moderate severe
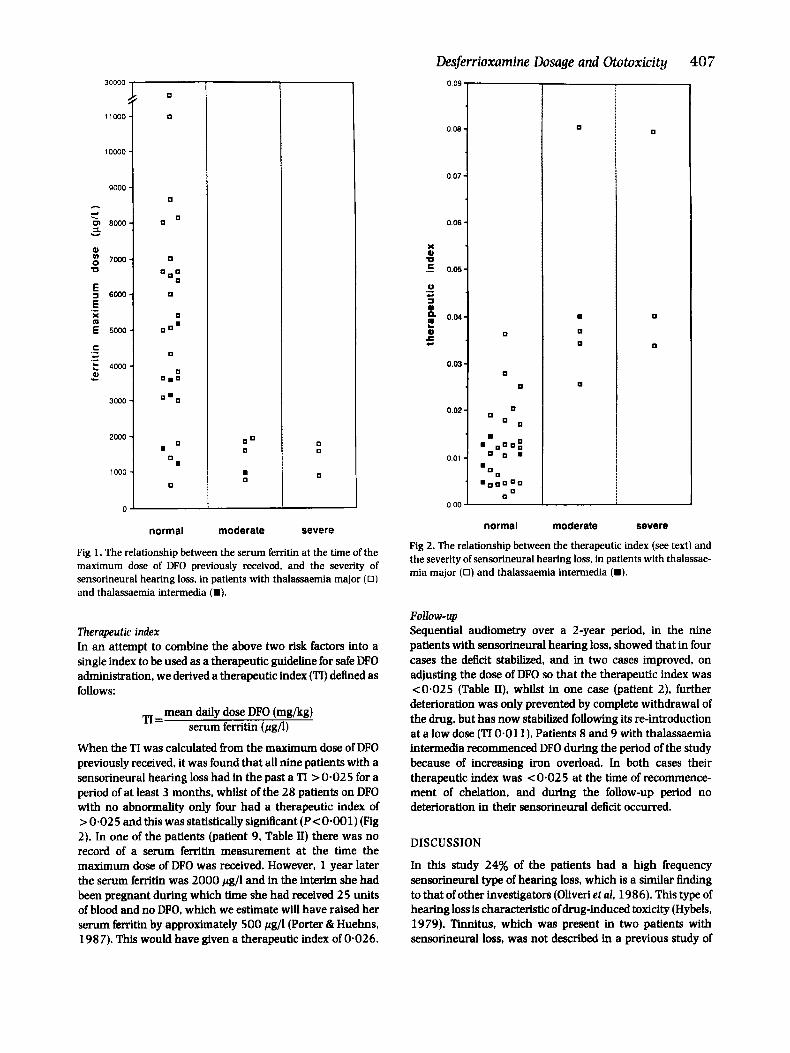
Fig 1. The relationship between the serum ferritin at the time of the maximum dose of DFO previously received, and the severity of sensorineural hearing loss, in patients with thalassaemia major (0 ) and thalassaemia intermedia (m).
Therapeutic index In an attempt to combine the above two risk factors into a single index to be used as a therapeutic guideline for safe DFO administration, we derived a therapeutic index (TI) defined as follows:
mean daily dose DFO (mg/kg) serum ferritin (pg/l) TI=
When the TI was calculated from the maximum dose of DFO previously received, it was found that all nine patients with a sensorineural hearing loss had in the past a TI > 0.02 5 for a period of at least 3 months, whilst of the 28 patients on DFO with no abnormality only four had a therapeutic index of >0.025 and this was statistically significant (P<O.OOl) (Fig 2). In one of the patients (patient 9, Table II) there was no record of a serum ferritin measurement at the time the maximum dose of DFO was received. However, 1 year later the serum ferritin was 2000 pg/l and in the interim she had been pregnant during which time she had received 25 units of blood and no DPO. which we estimate will have raised her serum ferritin by approximately 500 pg/l (Porter & Huehns, 1987). This would have given a therapeutic index of 0.026.
0 09 7
normal moderate severe
Fig 2. The relationship between the therapeutic index (see text) and the severity of sensorineural hearing loss, in patients with thalassae- mia major (0) and thalassaemia intermedia (m).
FOllOW-Up Sequential audiometry over a 2-year period, in the nine patients with sensorineural hearing loss, showed that in four cases the deficit stabilized, and in two cases improved, on adjusting the dose of DFO so that the therapeutic index was <0.025 (Table II), whilst in one case (patient 2), further deterioration was only prevented by complete withdrawal of the drug, but has now stabilized following its re-introduction at a low dose (TI 0.011). Patients 8 and 9 with thalassaemia intermedia recommenced DFO during the period of the study because of increasing iron overload. In both cases their therapeutic index was < 0.02 5 at the time of recommence- ment of chelation, and during the follow-up period no deterioration in their sensorineural deficit occurred.
DISCUSSION
In this study 24% of the patients had a high frequency sensorineural type of hearing loss, which is a similar 6nding to that of other investigators (Ohveri et al, 1986). This type of hearing loss is characteristic of drug-induced toxicity (Hybels, 1979). Tinnitus, which was present in two patients with sensorineural loss, was not described in a previous study of

408 89 patients (Oliveri et al. 1986) but was noted by Marsh et a1 (1981) in a patient with thalassaemia intermedia treated with subcutaneous DFO. The additional Rnding of conductive hearing loss in 13% of patients demonstrates that such abnormalities are more frequent in this group of patients than the general population and must be distinguished from a sensorineural deficit.
Assessment of the risk factors in this study has shown evidence of sensorineural abnormalities only in patients who had previously received DFO. The finding that the maximum dose of DFO previously received for a period of at least 3 months was significantly associated with sensorineural hearing loss, rather than the dose at the time abnormality was detected, suggests that there may be long-term damage following relatively high doses of the drug. Insufficient data was available concerning the exact duration for which the maximum dose of DFO was received, and it is possible that this may be an additional risk factor. The absence of sensorinerural loss in patients with serum ferritin values >2000 pg/l at the time of maximum DFO administration (Fig 1) suggests that a high degree of iron overload protects against the ototoxic effects of DFO.
The younger patients with thalassaemia major have shown the most severe sensorineural damage following relatively high DFO dosage: however, they have been better chelated compared with the older patients (subcutaneous DFO was unavailable 10 years ago) and therefore have lower serum ferritin values. It is therefore unnecessary to invoke age per se as a risk factor. Furthermore, older patients are also susceptible to the effects of DFO as we have investigated one 44-year-old patient with acquired sideroblastic anaemia and only mild iron overload (serum ferritin 400 pg/l) who developed reversible high frequency sensorineural loss on comparatively low doses of DFO (30 mg/kg/24 h).
If the risk factors of maximum DFO dosage and low serum femtin at that time are considered separately, it is unclear how best to adjust the dose of DFO to treat a given degree of iron overload. In both our series and that of Oliveri, a number of patients with low serum ferritin receiving DFO had normal audiometry (Table I). Furthermore, there were a number of patients receiving high doses of DFO without evidence of auditory abnormalities. It is likely that some interaction of DFO dose and iron overload status is important in the genesis of DFO associated toxicity. By combining the two risk factors of maximum dose DFO and serum femtin at that time into a single therapeutic index, it was found that no patient with a ratio of <0.025 had a sensorineural deficit (P<O.OOl). Using this therapeutic index as a guideline for the DFO dose to be administered, it is possible to give large doses of DFO with minimal risk of ototoxicity to severely iron overloaded patients with reduction of dosage being necessary only as the serum ferritin begins to fall. The safe dose can be calculated from the product of serum ferritin x 0.025. For example, a patient with a ferritin of 2000 pg/l, the maximum safe dose will be either 50 mg/kg/24 h 7 d a week, or 70 mg/kg/24 h 5 d a week. As the therapeutic index for ototoxicity has been derived for patients receiving DFO three to seven times per week it would seem prudent to apply it only to patients receiving DFO at similar time intervals, as doses above 120
John B. Porter et al mg/kg/24 h may be associated with retinal (Davies et al. 1983) as well as other toxicities (Porter & Huehns, 1989).
By following the audiometry over a 2-year period, at approximately 6-monthly intervals, it was possible to investi- gate the effect of dose modification of DFO on the sensori- neural hearing loss. In all patients with deteriorating sensori- neural loss, the dose of DFO was reduced so that the TI was <0.025 (patients 1-6, Table 11). The finding that audiometry either stabilized or improved on dose reduction in all these patients is strong circumstantial evidence of a causal link between DFO use and ototoxicity. This stabilization or improvement was paralleled with a reduction of the thera- peutic index from > 0.02 5 to <Om02 5 in each of the above cases. The clinical value of the therapeutic index is also illustrated by patient 9. This patient required further inten- sive chelation, and DFO was recommenced intravenously at 100 mg/kg/24 h for 5 d periods at 2-4-weekly intervals (therapeutic index <0.025). There was no change in audiometry over a 5-month follow-up suggesting that pro- vided that DFO dose to ferritin ratios are not excessive (i.e. >0.025) DFO can be given without compromising auditory function even in patients with an existing sensorineural deficit.
It has been suggested that such patients with abnormal auditory function should be changed to diethylenetriamine- pentaacetic acid (DTPA) (Jackson et al, 1983). However, DTPA has a number of disadvantages over DFO. most importantly its relative lack of selectivity for ferric iron. Whilst most attention has been drawn to its afEnity for zinc, resulting in a variety of symptoms including acrodermatitis enteropathica. it must be remembered that DTPA also has a relatively high stability constant for other metals such as copper and manganese (Waxman & Brown. 1969). Although it has been claimed that the concurrent adminis- tration of zinc reduces the toxicity of this compound (Wonke et al, 1989). the zinc sulphate is unpalatable, needs to be taken in large amounts, and some authors have found toxicity despite the concurrent administration of zinc (Pip pard et al, 1986). Thus if DFO can be continued without deleterious effects, this would be advantageous. Our results suggest that following dose modification this can be achieved in most patients.
A possible mechanism for DFO associated toxicity is that in less severely iron overloaded patients, more of the iron-free drug is available to chelate trace metals in the cochlea, thereby inhibiting important metalloenzymes such as tyrosi- nase or lipoxygenase. Alternatively, there may be a direct toxic effect on the cochlea (Simon et d, 1983). The only reported study which has examined the effect of DFO on the animal cochlea (Shirane & Harrison, 1987) failed to demon- strate changes in the sensory epithelium following a DFO dose of 100 mg/kg/24 h for 64 d in non iron overloaded animals. Furthermore, in a preliminary study, no evidence of cochlea damage on electron microscopy in normal or iron overloaded mice receiving DFO at 200 mg/kg/24 h for 2 months has been observed (authors’ unpublished observa- tions).
The risk factors for ototoxicity appear to be somewhat Merent from those of visual toxicity suggesting that the

Desferrioxamine Dosage and Ototoxicity 409 A., Mdardi, V. & Puxeddu, P. (1979) Auditory involvement in thalassaemia major. Acta Haernatologica, 61, 209-2 15.
Guerin A., London. G.. Marchais. S.. Metivier. F. & Pelisse. j-M. ( 198 5) Acute deafness and desfemoxamine. Lancet. ii. 39-40.
Hazell. J.W.P. & Modell. C.B. (1976) ENT involvement in thalassae- mia major. journal OfLaryngology and Otology. 90, 877-881.
Hybels, R.L. (1979) Drug toxicity of the inner ear. Medical Clinics of North America, 63, 309-319.
International Committee on Standards in Haematology (1985) Proposed international standard of human ferritin assay. British journal of Haernatology. 61, 61-63.
Jackson. M.J.. Brenton. D.P. & Modell. B. (1983) DTPA in the management of iron overload in thalassaemia. Iournal oflnheriled Metabolic Diseases, 6. 97-98.
Marsh, M.N.. Holbrwk. I.B.. Clark, C. & Shder. J.L. (1981) Tinnitus in a patient with beta-thalassaemia intermedia on long-term treatment with desfemoxamine. Postgraduate Medical journal. 57,
Mason. S.. McCormick. B. & Wood, S. (1988) Auditory brainstem response in paediatric audiology. Archives ofDisease in Childhood, 63,465-467.
McIntosh. N. (1976) Beneflcial effects of transfusing a patient with non-transfusion dependent thalassaemia major. Archives of Disease in Childhood. 51,471.
Oliveri, N.F., Buncie, J.R.. Chew, E.. Gallanti. T.. Harrison, R.V., Keenan, N.. Logan, W.. Mitchell. D., Ricci. G., Skarf. B.. Taylor, M. & Freedman, M.H. (1986) Visual and auditory neurotoxicity in patients receiving subcutaneous defroxamine infusions. New England journal of Medicine. 314. 869-873.
Orton. R.B.. de Veber. L.L. & Sulk, H.M.B. ( 1 985) Ocular and auditory toxicity of long-term high-dose subcutaneous desferrioxamine therapy. Canadian journal of Ophthalmology. 20, 1 5 3-1 56.
Pippard. M.J.. Jackson. M.J.. Hoffman. K., Petrou. M. & Modell. B. ( 1 986) Iron chelation using subcutaneous infusions of diethylene triamine penta-acetic acid (DTPA). Scandinavian journal of Haema-
Pippard, M.J.. Letsky, E.A.. Callender, S.T. & Weatherall. D.J. ( 1978) Prevention of iron loading in transfusion-dependent thalassaemia. Lancet. i, 1178-1181.
Porter, J.B. & Huehns. E.R. (1987) Transfusion and exchange transfusion in sickle cell anaemia, with particular reference to iron metabolism. Actn Haernatologica. 78, 198-205.
Porter, J.B. & Huehns, E.R. (1989) The toxic effects of desfemoxa- mine. Clinics in Haernatology-Balliere’s Clinical Haernatology, 2, (2) 4 59-4 74.
Shuane, M. & Harrison, R.V. (1987) The eKects of deferoxamine mesylate and hypoxea on the cochlea. Acta Otolarynglogica. 104,
Simon, P.. Ang. K.S., Meyrier, A., Allain, P. & Mauras. Y. (1983) Desferrioxamine, ocular toxicity and trace metals. Lancet. ii. 5 12- 513.
Waxman, H.S. & Brown, E.B. (1969) Clinical usefulness of iron chelating agents. Progress in Haernatology, 6, 338-373.
Wonke. B.. Aldouri. M.A..Flynn. D.M..Stearns. M.P.. Warner, P.Y.& Hofibrand. A.V. (1989) Auditory neurotoxicity in patients receiv- ing subcutaneous desferrioxamine treatment and the use of calcium diethylene triamine penta acetic acid (DTPA) as an alternative chelator. Archives of Disease in Childhood, 64, 77-82.
Zipursky. A. (1985) Deferoxamine: eye and ear damage threat Selecta. (D). 15, 1347-1348.
582-584.
tology. 36, 466-472.
99-107.
mechanisms may be different. Retinal toxicity has been observed at high doses of DFO (Davies et al, 198 3, Oliveri et al. 1986) whereas ototoxicity may occur at lower doses particu- larly where there is minimal iron overload (Guerin et al. 1985). This may be because DFO, being hydrophilic with a lipid/water partition coefficient of 0.01 is unable to penetrate the blood retinal barrier unless very high doses of DFO are given, or the blood retinal barrier is breached in some way. This may occur by the co-administration of drugs which facilitate transit of metals across biomembranes (Blake et al. 1985) or following physical damage to the retina, as for example, in diabetes mellitus (Arden et al, 1984). By contrast DFO may be able to penetrate the cochlea in the absence of these factors, and accumulate there due to the slow removal of endolymph (Marsh et al, 1981). None of the patients with auditory sensorineural abnormalities in this series had diabetes or evidence of retinal malfunction on electroretino-
It is concluded that the optimal safe dose of DFO must be tailored to each patient on the basis of the degree of iron overload at that time, and that the therapeutic index is a useful guideline in this aspect of patient management. The presence of sensorineural abnormalities is not an absolute indication for stopping DFO, and it can be continued at a dose adjusted to the degree of iron overload without further deterioration or with improvement in audiometric function in some cases. Further work on the mechanism of DFO mediated ototoxicity is required so that patients with modest degrees of iron overload can be safely treated.
g w h y .
ACKNOWLEDGMENT J. W. P. Hazell is supported by a grant from the Royal National Insitute for the Deaf, London.
REFERENCES Arden, G.B. (1 986) Desfemoxamine administered intravenously by
infusion causes a loss of retinal sensitivity in rabbits anaesthetised with methane. Human Toxicology. 5, 229-236.
Arden, G.B.. Wonke. B.. Kennedy, C. & Huehns. E.R. (1984) Ocular changes in patients undergoing long-term desferrioxamine treat- ment. British journal of Ophthalmology, 68, 873-877.
Barry, M.. Flynn. D.M.. Letsky. E.A. &Risdon. R.A. (1974) Long-term chelation therapy in thalassaemia major: EfTect on liver iron concentration, liver histology and clinical progress. British Medical journal. ii, 16-20.
Blake, D.R.. Winyard. P.. Lunec. J . . Williams, A,. Good, P.A.. Crewes. S.J.. Gutteridge. J.M.C.. Rowley. D.. Halliwell. B.. Cornish, A. & Hider, R.C. (1985) Cerebral and ocular toxicity induced by desferrioxamine. Quarterly journal of Medicine. 56, 345-35 5.
Borgna-Pignatti, C.. de Stefano. P. & Broglia. A.M. (1984) Visual loss in patient on high-dose subcutaneous desferrioxamine. Iltnret. i.
Davies. S.C.. Hungerford. J.L.. Arden.G.B., Marcus, R.E., Miller. M.H. & Huehns. E.R. (1983) Ocular toxicity of highdose intravenous desfemoxamine. Lncet, ii, 181-184.
De Vigilis. S.. Argiolon. F., Sanna, G.. Cornacchia. G.. Cossu. P.. Cao.
681.