Embed Size (px)
Citation preview

Description of the Characteristics of CasesWith Noncontiguous Neural Tube DefectsIdentified in a Series of Consecutive BirthsM.-L. MARTINEZ-FRIAS,1,2* A. SANCHIS,3 P. APARICIO,4 M. BLANCO,5 M.J. GARCIA,6
J. GOMEZ-ULLATE,7 V. FELIX,8 H. HUERTAS,9 N. JIMENEZ,10 J.A. LOPEZ,11
J.J. MARCO,12 M. MARTIN,13 G. PALACIOS,14 D. ROMERO,15 AND M.S. VAZQUEZ16
1ECEMC, Facultad de Medicina, Universidad Complutense, Madrid, Spain2Departamento de Farmacologıa, Facultad de Medicina, Universidad Complutense, Madrid, Spain3Servicio de Pediatrıa, Hospital Dr. Peset de Valencia, Valencia, Spain4Servicio de Pediatrıa, Hospital General Yague de Burgos, Burgos, Spain5Servicio de Pediatrıa, Hospital Xeral de Vigo, Vigo, Spain6Servicio de Pediatrıa, Hospital Virgen de la Luz de Cuenca, Cuenca, Spain7Servicio de Pediatrıa, Hospital Marques de Valdecilla de Cantabria, Santander, Spain8Servicio de Pediatrıa, Hospital Virgen de la Salud de Toledo, Toledo, Spain9Servicio de Pediatrıa, Hospital Gutierrez Ortega de Valdepenas, Valdepenas, Spain10Servicio de Obstetricia-Ginecologıa, Hospital General de Segovia, Segovia, Spain11Servicio de Pediatrıa, Hospital Rafael Mendez de Lorca, Lorca, Spain12Servicio de Pediatrıa, Hospital Arnau de Vilanova de Lleida, Lleida, Spain13Servicio de Pediatrıa, Hospital Rıo Hortega de Valladolid, Valladolid, Spain14Servicio de Pediatrıa, Hospital Infanta Elena de Orense, Orense, Spain15Servicio de Pediatrıa, Hospital General de Segovia, Segovia, Spain16Servicio de Neonatologıa, Hospital General de Albacete, Albacete, Spain
ABSTRACT Van Allen et al. [(1973) Am. J.Med. Genet. 47:723–743] provided evidence for mul-tisite closure of the neural tube in humans. Reynolds etal. [(1995) Proceedings of the greewood Genetic Cen-ter 14:70–71] and Seller [(1995) J. Med. Genet.32:205–207] described 13 and seven cases of noncon-tiguous neural tube defects (NTDs) respectively andconcluded that the presence of noncontiguous NTDscannot be explained on the basis of the model of asingle initiation site with bidirectional closure. Here wepresent a series of 14 consecutive infants with noncon-tiguous NTDs, describing their characteristics. Theseshow that noncontiguous NTDs are clinically heteroge-neous, may have differences in sex ratio, and couldhave causal heterogeneity. The different combinationsof closure failure defects have shown proportions in ourpopulation that are different from those in the popula-tions studied by Reynolds et al. and Seller. Teratology57:13–16, 1998 r 1998 Wiley-Liss, Inc.
Van Allen et al. (’93) provided evidence for multisiteclosure of the neural tube in humans similar to theintermittent pattern of neural tube closure observed inexperimental animals (Golden and Chernoff, ’93). Rey-nolds et al. (’95) and Seller (’95a) described 13 andseven cases of noncontiguous neural tube defects (NTDs)respectively, and concluded that the presence of noncon-tiguous NTDs cannot be explained on the basis of themodel of a single initiation site with bidirectionalclosure. We observed that the prevalence of noncontigu-
ous NTDs is 0.13 per 10,000 livebirths in our population(Martınez-Frıas et al., ’96).
Here we describe the consecutive cases with noncon-tiguous NTDs observed among 948 live and stillborninfants with NTDs. We have considered as noncontigu-ous NTDs those cases in which the lesion involved atleast two noncontiguous sites, i.e. a case with sites 2 1 4and 1 affected (holoacrania and noncontiguous spinabifida).
MATERIALS AND METHODS
The live and stillborn cases with NTDs derived fromthe Spanish Collaborative Study of Congenital Malfor-mations (ECEMC). This is an ongoing hospital-basedcase-control study and surveillance system with amethodology aimed not only at the surveillance ofcongenital anomalies, but also at investigating theircharacteristics, the clusters of congenital malforma-tions, and the causes of congenital defects. All childrenborn in about 70 participating hospitals from all overSpain are examined by pediatricians who, being inter-ested in the problem of congenital defects, collaboratewith the ECEMC program and accept its unique strictmethodology.
Contract grant sponsors: Direccion General de Salud Publica, Ministe-rio de Sanidad y Consumo of Spain, Fundacion ONCE of Spain.
*Correspondence to: Dr. M.-L. Martınez-Frıas, ECEMC, Facultad deMedicina, Universidad Complutense, 28040, Madrid, Spain.
Received 29 May 1997; Accepted 13 November 1997
TERATOLOGY 57:13–16 (1998)
r 1998 WILEY-LISS, INC.

Malformed infants (cases)
The collaborating physicians examine all the new-born infants in each participating hospital during thefirst 3 days of life to identify those with major and/orminor/mild congenital defects, making a detailed de-scription of each congenital anomaly. In many instancesphotographs, karyotypes, imaging studies, pathologyreports, and results of other studies are also availablefor review.
We modified the ICD-8 code for congenital defects byadding two more digits in order to obtain more specific-ity. The ECEMC coding system has different levels toidentify congenital defects and clinical patterns (Mar-tınez-Frıas, ’94; Martınez-Frıas and Urioste, ’94). Wehave expanded the code for each type of NTD (Martınez-Frıas et al., ’96) in order to specify the location of thelesion according to Van Allen et al.’s (’93) proposal.
Control children
For each malformed infant (case), the next nonmal-formed infant of the same sex born in the same hospitalis selected as a control subject, from whom we collectthe same data as for the malformed infant.
Descriptions of the ECEMC methodology have beenpublished repeatedly (Martınez-Frıas, ’94, ’95; Martınez-Frıas and Urioste, ’94).
From April 1976 to March 1995, the ECEMC sur-veilled a total of 1,222,698 livebirths, and from January1980 a total of 8,066 stillbirths. We identified 784 and164 children with NTDs among liveborn and stillbirths,respectively. In 14 of 948 consecutive infants withNTDs there were different closure sites affected(Table 1).
We consider as noncontiguous NTDs the presence ofat least two NTDs in one individual separated by aregion of normally closed neural tube. Van Allen et al.(’93) proposed five closure regions. The initial closure isat the cervical region (number 1), which is bidirectional.
Closure number 2 begins at the prosencephalon-mesencephalon junction and is also bidirectional. Clo-sure 3 starts at the stomodeum and is unidirectional tomeet the descending rostral part of the closure site 2.The junction of sites 2 and 3 represents the anteriorneuropore. Closure 4 is over the rhombencephalon andis unidirectional towards the rostral part of the embryo.Finally, closure number 5 affects the extreme caudalend of the neural tube, and is also unidirectional tomeet the descending part of closure site 1. The areabetween closures 1 and 5 represents the posteriorneuropore. We have numbered the different NTDs bythe number of the affected closure region. For instance,meroacrania is considered as closure defect 2, butholoacrania is (2 1 4). Frontal encephalocele arises atthe junction of closures 2 and 3 and it is considered as(2 1 3).
RESULTS
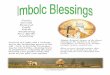
Table 1 shows the description of the different lesionswith respect to clinical presentation, sex and cause (ifknown), birth weight and gestational age in each one ofthe 14 cases with different closure site defects. In one ofthe 14 noncontiguous NTDs cases the closure sites werenot specified clearly. All cases of anencephaly hadholoacrania (2 1 4). None of the cases had meroacrania.Among 13 cases with specified site of lesion, 10 includesite 2 (79.92%), six (46.15%) include site 3, all of themwith frontal encephalocele, and five (38.46%) includesite 4, as one of the two lesions. Five (83.33%) of the sixcases with frontal encephalocele were females. Two ofthree cases with anencephaly were females. There werea female case and a male case with occipital encephalo-cele (site 4). Nine cases were isolated, three presented anonsyndromal multiple congenital anomaly (MCA) pat-tern. Among the six cases with frontal encephalocele,two (33.33%) had trisomy 18, and in another case wesuspected trisomy 18, but lacked a karyotype. Among
TABLE 1. Description of the lesions in cases with different closure sites involved and clinicalpresentation/cause
Case Lesion 1 Lesion 2 Sex
Clinicalpresent./
Cause
Birthweight
(g)
Gestationalage
(weeks)
1 Occipital encephalocele (4) Lumbar myeloeningocele (1) Male Isolated 2,920 382 Frontal encephalocele (312) Lumbar myelomeningocele (1) Male Isolated 3,400 403 Frontal encephalocele (312) Lumbar myelomeningocele (1) Female T-18 NS 374 Thoracic meningocele (1) Lumbo-sacral myelomeningocele (115) Absence Multiple 2,370 365 Frontal encephalocele (312) Lumbar myelomeningocele (1) Female Isolated 2,900 396 Anencephaly (214) Myelomeningocele NS Female Isolated 3,100 427 Occipital encephalocele (4) Lumbar myelomeningocele (1) Female Isolated 2,845 428 Frontal encephalocele (312) Lumbar myelomeningocele (1) Female Multiple1 2,500 399 Frontal encephalocele (312) Lumbar myelomeningocele (1) Female Isolated 4,240 39
10 Frontal encephalocele (312) Lumbar myelomeningocele (1) Female T-18 2,040 4111 Parietal encephalocele (2) Lumbo-sacral myelomeningocele (115) Female Isolated 2,750 3712 Anencephaly (214) Lumbar myelomeningocele (1) Male Isolated NS 4113 Anencephaly (214) Sacral myelomeningocele (5) Male Multiple 1,453 3014 Encephalocele NS Myelomeningocele NS Male Isolated 2,900 40
Present. 5 presentation; T-18 5 trisomy 18; NS 5 not specified.1Suspected trisomy 18.
14 M.-L. MARTINEZ-FRIAS ET AL.

the total infants with trisomy 18 identified in theECEMC data, 10 cases had NTD and in two of them(20%) the NTDs were noncontiguous.
In order to further delineate the characteristics ofthese noncontiguous NTDs, Table 1 also presents thebirth weight and gestational age of each affected child.Only four of the 12 cases with specified data (cases 4,10, 12 and 13) had low birth weight (,2,500 g) and oneof them was premature (,37 weeks of gestation). Threeof the four cases had an MCA pattern, one of them wasborn to a diabetic mother, and the last one had trisomy18. On the other hand, none of the other cases waspremature.
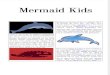
Table 2 indicates the number of cases and the percent-age of the different closure site defect combinationsobserved by Reynolds et al. (’95), Seller (’95a) and thepresent study. Only one group of noncontiguous closuresite defects was observed in the three series but withhigher proportion in the series of Reynolds et al. (’95).This group is: occipital meningoencephalocele plus spinabifida (closure site defects 4 1 1). Two types, frontalencephalocele plus spina bifida (closure site defects(3 1 2) 1 1) and holoacrania plus spina bifida (closuresite defects (2 1 4) 1 1), were observed only by Rey-nolds et al. (’95) and the present study, but withdifferent proportions; and also two types, holoacraniaplus spina bifida (2 1 4) 1 (1 1 5) and meroacraniaplus sacral spina bifida (type 2 1 5), were observed bySeller (’95a) and Reynolds et al. (’95). The closure sitedefect (4 1 1) was commonest in the series of Reynoldset al. (’95), while in the series of Seller (’95a) thecommonest were types 4 1 4 1 1 (constituted by thepresence of two separate but closely placed meningoen-cephaloceles associated with spina bifida in one case,and a small lesion in the occipital bone together with alarge cervical meningocele, and spina bifida in the othercase) and (2 1 4 1 1) 1 (1 1 5), and in our series themost frequent was (3 1 2) 1 1 (frontal encephaloceleplus lumbar myelomeningocele).
None of our cases was prenatally exposed to knownteratogens. Other characteristics such as maternal andpaternal ages (excluding cases with trisomy 18) do notdiffer from the controls (maternal age in cases, n 5 12,X 5 27.25, SD 5 7.39; maternal age in the controlgroup, n 5 23,776, X 5 27.48, SD 5 5.34; paternal agein cases, n 5 10, X 5 30.7, SD 5 5.16; paternal age inthe control group, n 5 23,282, X 5 30.36, SD 5 5.74).
DISCUSSION
Noncontiguous NTDs are rare. In fact, the prevalencein our population is 0.13/10,000 livebirths (Martınez-Frıas et al., ’96). The present analysis suggests a higherprevalence of noncontiguous NTDs among stillborninfants (cases number 12, 13) of 2.48/10,000. This is aminimum estimate since the voluntary interruption ofpregnancy due to congenital defects has been legal inSpain since 1985. However, in spite of rarity (1.48% ofthe total NTDs; 14/948), the presence of noncontiguousNTDs cannot be explained on the basis of the model of a
single initiation site with bidirectional closure, andsupports the multisite model of neural tube closure, aspostulated by Van Allen et al. (’93), Reynolds et al. (’95)and Seller (’95a). This is also stated by Busam et al.(’93) from a case with two separate anterior NTDsinvolving two contiguous sites (2 and 4), which wereseparated by a bony and cutaneous bridge. Thus, studyof the different types of noncontiguous NTDs, theirclinical presentation and causes, as well as their propor-tions and characteristics in different populations, couldgive us some clues about neural tube closure biology.
We have shown that the different noncontiguousNTDs are heterogeneous in clinical presentation andcause. Nine (64.29%) of the 14 cases were isolatedNTDs, three (21.43%) had anomalies other than NTD(nonsyndromal), and two (14.29%) were aneuploidies.Two of the three cases with an MCA pattern had a widespectrum of anomalies affecting different systems. Theother one presented with defects of biliary ducts, thy-mus and adrenal glands. All seven cases described bySeller (’95a) were nonsyndromal. There is no informa-tion on the clinical presentation in the two previouspublished data on this topic (Van Allen et al., ’93;Reynolds et al., ’95). It seems that the case of Busam etal. (’93) only had an associated cleft of the soft palate.
Our data of noncontiguous NTDs suggest that theyare causally heterogeneous. Twenty percent of theNTDs observed in cases of trisomy 18 are noncontigu-ous, and all of them affect sites (3 1 2) 1 1. Reynolds etal. (’95) observed one case related to alcohol exposure.From a series of recurrent NTD after maternal folatesupplementation studied by Seller (’95b) it is suggestedthat the effect of the folate supplementation is notrelated to a particular region of the neural tube;however, the number of this series is very small.
In relation to the type of closure failure, the sitesmost frequently involved in our data were sites 2 and 3
TABLE 2. Comparison of the closure site defectsobserved by Reynolds et al. (1995), Seller (1995a),
and the present study
Closure site defects
Reynoldset al. Seller
Presentstudy
N % N % N %
21(115) 0 — 0 — 1 7.69(214)1(115) 1 7.69 1 14.29 0 —(214)11 3 23.08 0 — 1 7.69(312)11 11 7.69 0 — 6 46.15(214)15 0 — 0 — 1 7.69211 1 7.69 0 — 0 —215 1 7.69 1 14.29 0 —411 6 46.15 1 14.29 2 15.3811(115) 0 — 0 — 1 7.69(214)1NS 0 — 0 — 1 7.6941411 0 — 2 28.57 0 —(21411)1(115) 0 — 2 28.57 0 —
Total 13 100 7 100 13 100
NS 5 nonspecified closure site defects.1Although Reynolds et al. coded this case as 311, it is a frontalencephalocele (as in our cases) plus lumbar meningocele.Thus, we consider it as (312)11.
NONCONTIGUOUS NTD 15

in six (46.15%) of 13 cases with specified data, while acombination of sites 2 and 4 was observed in three(23.08%) cases. This is different from that observed inthe series of Reynolds et al. (’95) and Seller (’95a),where the most frequently affected site was 4 (10 of 13cases), combined with site 2 in four of 10 cases in theseries of Reynolds et al. (’95) and also site 4 (in six ofseven cases) in that of Seller (’95a) that was combinedin six instances with site 1. Although frontal NTDseems to be common in South East Asia (Thu and Kyu,’84), they are very rare in the western world (Seller,’95a). Thus it is very interesting the high proportion ofcases that we observed (42.86%, 6/14) in our series ofconsecutive children with noncontiguous NTDs. Thepresence of more severe cases with three different typesof closure failure sites in the series of Seller (’95a) couldwell be due to the fact that this is a series based inprenatal diagnosis of NTDs and voluntary interruptionof pregnancies, instead of consecutive births. Thus,some of the types of noncontiguous NTDs identified bySeller (’95a) could have been spontaneous or inducedabortions in our series. Nevertheless, the differences inthe types of closure failure observed between the seriesof Reynolds et al. (’95), Seller (’95a) and the presentstudy suggest that genetic differences in the popula-tions could account for the variation in the frequency ofthe different types of noncontiguous NTD. Although thenumbers are small, the observed sex ratios also supportthe possibility that the different closure sites are underdifferent genetic controls. Similarly to the results ob-served by Seller (’95c) for parietal or occipital encepha-loceles, our data show (Table 1) that frontal encephalo-cele (closure sites 3 1 2) is observed more frequently infemales than in males (five of six). This result isdifferent from that of Thu and Kyu (’84) for fronto-nasalencephalomeningoceles that were more frequent inmales in Burma. Seller (’95c) observed similar sex ratiofor isolated failure of closure 2. Since our numbers aresmall, and there is only a previous analysis of sex ratioin the different types of closure failure (Seller, ’95c),
these observations on sex ratios should be analyzed inlarger series to confirm the suggested sex differences.
The analysis of noncontiguous NTD series from otherpopulations will enhance our knowledge on their char-acteristics and biology.
ACKNOWLEDGMENTS
This work was supported in part by a grant fromDireccion General de Salud Publica, Ministerio deSanidad y Consumo of Spain, and by Fundacion ONCEof Spain.
LITERATURE CITEDBusam, K.J., D.J. Roberts, and J.A. Golden (1993) Clinical teratology
counseling and consultation case report: Two distinct anteriorneural tube defects in a human fetus: Evidence for an intermittentpattern of neural tube closure. Teratology, 48:399–403.
Golden, J.A., and G.F. Chernoff (1993) Intermittent pattern of neuraltube closure in two strains of mice. Teratology, 47:73–80.
Martınez-Frıas, M.-L. (1994) Developmental field defects and associa-tions: Epidemiological evidence of their relationship. Am. J. Med.Genet., 49:45–51.
Martınez-Frıas, M.-L. (1995) Primary midline developmental field. I.Clinical and epidemiological characteristics. Am. J. Med. Genet.,56:374–381.
Martınez-Frıas, M.-L. and M. Urioste (1994) Segmentation anomaliesof the vertebras and ribs: A developmental field defect: Epidemio-logic evidence. Am. J. Med. Genet., 49:36–44.
Martınez-Frıas, M.-L., M. Urioste, E. Bermejo, A. Sanchıs, and E.Rodrıguez-Pinilla (1996) Epidemiological analysis of multi-site clo-sure failure of neural tube in humans. Am. J. Med. Genet., 66:64–68.
Reynolds, J.F., C.A. Moore, S. Li, Sx. Hong, Z. Li, R.J. Berry, D.McFadden, and M.I. Van Allen (1995) Noncontiguous neural tubedefects. Proceedings of the Greewood Genetic Center 14:70–71.
Seller, M.J. (1995a) Further evidence for an intermittent pattern ofneural tube closure in humans. J. Med. Genet. 32:205–207.
Seller, M.J. (1995b): Multi-site neural tube closure in humans andmaternal folate supplementation. Am. J. Med. Genet. 58:222–224.
Seller, M.J. (1995c) Sex, neural tube defects, and multisite closure ofthe human neural tube. Am. J. Med. Genet. 58:332–336.
Thu, A. and H. Kyu (1984) Epidemiology of frontoethmoidal encephalo-meningocoeles in Burma. J. Epidemiol. Community Health 38:89–98.
Van Allen, M.I., D.K. Kalousek, G.F. Chernoff, D. Juriloff, M. Harris,B.C. McGillivray, S.L. Yong, S. Langlois, P.M. MacLeod, D. Chitayat,J.M. Friedman, R.D. Wilson, D. McFadden, J. Pantzar, S. Ritchie,and J.G. Hall (1993) Evidence for multi-site closure of the neuraltube in humans. Am. J. Med. Genet., 47:723–743.
16 M.-L. MARTINEZ-FRIAS ET AL.