Embed Size (px)
Citation preview

Int J Clin Exp Med 2015;8(2):3006-3009www.ijcem.com /ISSN:1940-5901/IJCEM0004468
Case ReportAtypical, multilevel and noncontiguous tuberculous spondylitis that affected the vertebrae of thoracic, lumbar and sacrum: a case report
Yi Shen1*, Weiye Zhong1, Dan Peng1*, Chang Lu1, Guangzhong Xiong2, Duo Li3, Youwen Deng1, Lihua Tan4
Departments of 1Orthopaedic Surgery, 2Neurosurgery, 3Pathology, 4Radiology, The 2nd Xiangya Hospital of Central South University, 410011, Hunan, China. *Equal contributors.
Received December 5, 2014; Accepted February 8, 2015; Epub February 15, 2015; Published February 28, 2015
Abstract: Aim: Tuberculous spondylitis (TS, also called Spinal tuberculosis, Pott’s spine or Pott’s disease) is a com-mon extrapulmonary manifestation of tuberculosis (TB), but multilevel, noncontiguous TS cases are rare. Methods: Physical examination, CT, MRI imaging, percutaneous biopsy and other lab tests were used to confirm the diagnosis. Result: we report a rare case of atypical, multilevel and noncontiguous TS in a 50-year-old woman. We found four noncontiguous osteolytic lesions in her spine that affected the Intervertebral joints of T10/11, L1/2, L3/4 and L5/S1. Patient was then treated conservatively with anti-TB drugs and was followed-up for about 1 year. The treatment turned out to be successful. Conclusion: The conservative anti-TB treatment was enough at least for this particular patient.
Keywords: Tuberculous spondylitis (spinal tuberculosis), multilevel, noncontiguous, Pott’s disease
Introduction
Tuberculous spondylitis (TS, also called Spinal tuberculosis, Pott’s spine or Pott’s disease) is a common extrapulmonary manifestation of tu- berculosis (TB), accounting for 50% of skeletal TB [1]. Since the symptoms and the features of individual TS vary greatly, TS is often misdiag-nosed. Furthermore, even though it is tho- ught that TS could spread through hematoge-nous route, in most reported cases, however, there were no more than 2 lesions sites in spine in each TS patient [2, 3]. So far, only two report-ed multilevel, noncontiguous TS cases in En- glish literatures [4, 5]. In these two cases, more than 3 lesions were found in each patient and some lesions affected multiple joints. The unique features of our current case are that there are four noncontiguous lesions, and each lesion affected only one joint, and the lesions are more or less evenly distribute in the entire spine, including the vertebrae of thoracic lum-bar, and sacrum.
Case report
A 50-year-old woman was hospitalized for chronicle back pain (lasting about 4 months).
Two months before admission to the hospital, her back pain was significantly aggravated, which caused her to have difficulty in walking. One month before her admission, she was mis-diagnosed as regular spondylitis, and received regular antibiotic (cephalosporins) treatment for about one month, but the treatment failed to alleviate her back pain and other symptoms. On her admission to our hospital, there were no typical symptoms of TB, such as afternoon fever, night sweating, or weight loss, even th- ough she had pulmonary TB history.
Physical examination found that she could move her lower limbs freely without feeling pain, numbless or fatigue, when she lay in bed. Her reflexes of knee and ankle were normal. Ankle clonus (-), Lasegue test (-), muscle str- ength and tension of lower limbs were normal without obvious symptoms of neurological dam-ages. The chief complaint was the abnormal percussion tenderness of lower back.
The lab test results were: the erythrocyte sedi-mentation rate (ESR) was 99 mm/h (higher than normal) and the C-Reactive Protein (CRP) was 13.30 mg/l (higher than normal). The blood
Conservative treatment successful on atypical multilevel tuberculous spondylitis
3007 Int J Clin Exp Med 2015;8(2):3006-3009
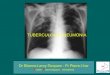
Figure 1. Coronal (A), sagittal (B) and axial (C-F) CT imaging at the time of admission showed that the osteolytic le-sions are located at the joins of the vertebrae of T10/11 (C), L1/2 (D), L3/4 (E) and L5/S1 (F). Note in (A & B), the intervertebral spaces between affected vertebrae are narrowed or expended irregularly, with isolated, small sand-like sequestra. The obvious irregular osteolytic lesions of endplates of affected vertebrae were also found in axial images (C-F). No paraspinal abscess was found in any of these images.
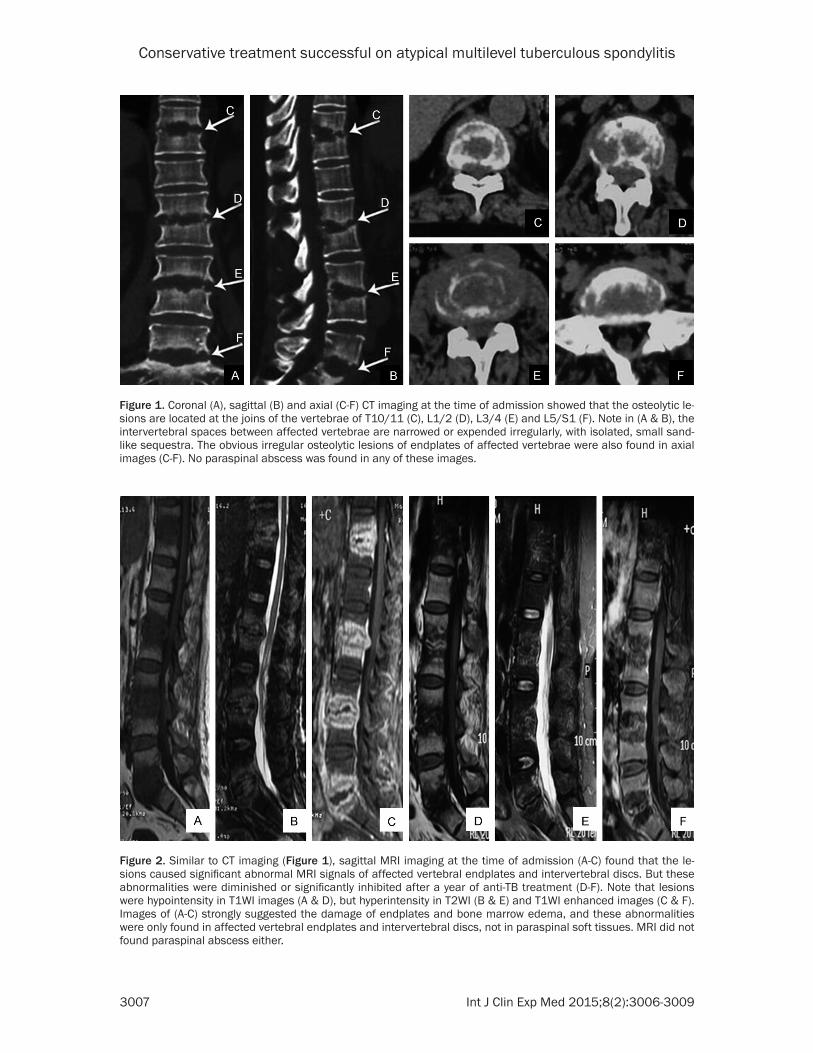
Figure 2. Similar to CT imaging (Figure 1), sagittal MRI imaging at the time of admission (A-C) found that the le-sions caused significant abnormal MRI signals of affected vertebral endplates and intervertebral discs. But these abnormalities were diminished or significantly inhibited after a year of anti-TB treatment (D-F). Note that lesions were hypointensity in T1WI images (A & D), but hyperintensity in T2WI (B & E) and T1WI enhanced images (C & F). Images of (A-C) strongly suggested the damage of endplates and bone marrow edema, and these abnormalities were only found in affected vertebral endplates and intervertebral discs, not in paraspinal soft tissues. MRI did not found paraspinal abscess either.
Conservative treatment successful on atypical multilevel tuberculous spondylitis
3008 Int J Clin Exp Med 2015;8(2):3006-3009
bacterial culture, the blood fungal culture and the serologic test of HIV were all negative, but the tuberculosis spot test was positive.
Four noncontiguous lesions were found in her spine by CT imaging, at the time of her admis-sion, which irregularly narrowed the interverte-bral spaces between affected vertebrae of T10/11, L1/2, L3/4 and L5/S1, respectively. Further detailed imaging study found that the osteolytic lesions were mainly at the joints of vertebrae, especially at the edges of the end-plates that directly contact with annulus fibro-sus of intervertebral discs (Figure 1).
MRI imaging found that the signals of the lesions are hypointense in T1WI but hyperin-tense in T2WI and T1WI enhanced (Gadolinium-enhanced) images. Gadolinium-enhanced MRI imaging further found a significant disruption of the fine structure of the affected intervertebral discs and the end plates of affected vertebrae. However, MRI did not find clear abnormality in paraspinal soft tissues, such as paraspinal abscess (Figure 2).
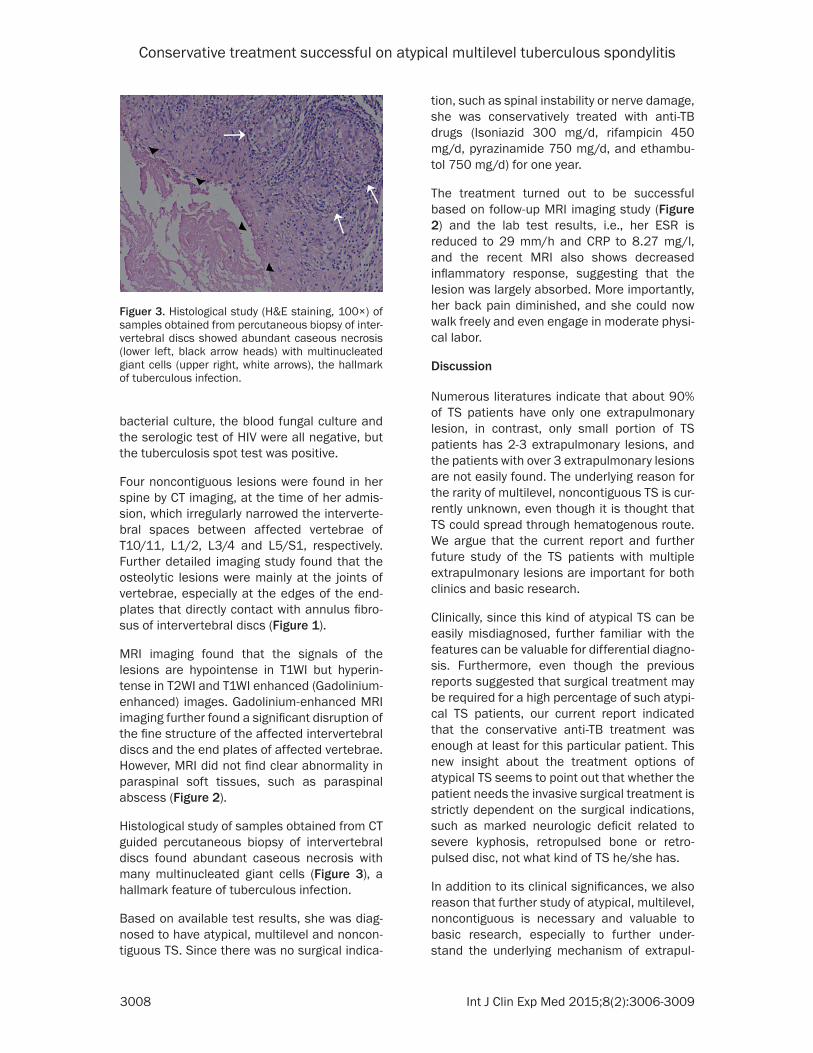
Histological study of samples obtained from CT guided percutaneous biopsy of intervertebral discs found abundant caseous necrosis with many multinucleated giant cells (Figure 3), a hallmark feature of tuberculous infection.
Based on available test results, she was diag-nosed to have atypical, multilevel and noncon-tiguous TS. Since there was no surgical indica-
tion, such as spinal instability or nerve damage, she was conservatively treated with anti-TB drugs (Isoniazid 300 mg/d, rifampicin 450 mg/d, pyrazinamide 750 mg/d, and ethambu-tol 750 mg/d) for one year.
The treatment turned out to be successful based on follow-up MRI imaging study (Figure 2) and the lab test results, i.e., her ESR is reduced to 29 mm/h and CRP to 8.27 mg/l, and the recent MRI also shows decreased inflammatory response, suggesting that the lesion was largely absorbed. More importantly, her back pain diminished, and she could now walk freely and even engage in moderate physi-cal labor.
Discussion
Numerous literatures indicate that about 90% of TS patients have only one extrapulmonary lesion, in contrast, only small portion of TS patients has 2-3 extrapulmonary lesions, and the patients with over 3 extrapulmonary lesions are not easily found. The underlying reason for the rarity of multilevel, noncontiguous TS is cur-rently unknown, even though it is thought that TS could spread through hematogenous route. We argue that the current report and further future study of the TS patients with multiple extrapulmonary lesions are important for both clinics and basic research.
Clinically, since this kind of atypical TS can be easily misdiagnosed, further familiar with the features can be valuable for differential diagno-sis. Furthermore, even though the previous reports suggested that surgical treatment may be required for a high percentage of such atypi-cal TS patients, our current report indicated that the conservative anti-TB treatment was enough at least for this particular patient. This new insight about the treatment options of atypical TS seems to point out that whether the patient needs the invasive surgical treatment is strictly dependent on the surgical indications, such as marked neurologic deficit related to severe kyphosis, retropulsed bone or retro-pulsed disc, not what kind of TS he/she has.
In addition to its clinical significances, we also reason that further study of atypical, multilevel, noncontiguous is necessary and valuable to basic research, especially to further under-stand the underlying mechanism of extrapul-
Figuer 3. Histological study (H&E staining, 100×) of samples obtained from percutaneous biopsy of inter-vertebral discs showed abundant caseous necrosis (lower left, black arrow heads) with multinucleated giant cells (upper right, white arrows), the hallmark of tuberculous infection.
Conservative treatment successful on atypical multilevel tuberculous spondylitis
3009 Int J Clin Exp Med 2015;8(2):3006-3009
monary lesion formation and the spreading route of TS. This hopefully will eventually answer the key question: why are the cases of multi-level, noncontiguous TS so rare, despite the seemly open hematogenous spreading route?
Disclosure of conflict of interest
None.
Address correspondence to: Lihua Tan, Department of Radiology, The 2nd Xiangya Hospital of Central South University, 139 Renmin Road, Changsha 410011, P. R. China. Tel: +86073185576046; Fax: +86073188339796; E-mail: [email protected]
References
[1] Ansari S, Amanullah MF, Ahmad K and Ra- uniyar RK. Pott’s Spine: Diagnostic Imaging Modalities and Technology Advancements. N Am J Med Sci 2013; 5: 04-11.
[2] Kulali A, Cobanoglu S and Ozyilmaz F. Spinal tuberculosis with circumferential involvement of two noncontiguous isolated vertebral levels: case report. Neurosurgery 1994; 35: 154-8.
[3] Janssens JP and de Haller R. Spinal tuberculo-sis in a developed country. A review of 26 cas-es with special emphasis on abscesses and neurologic complications. Clin Orthop Relat R 1990; 257: 7-75.
[4] Turgut M. Multifocal extensive spinal tubercu-losis (Pott’s disease) involving cervical, thorac-ic and lumbar vertebrae. Bri J Neurosurgery 2001; 15: 42-6.
[5] Emel E, Guzey FK, Guzey D, Bas NS, Sel B and Alatas I. Non-contiguous multifocal spinal tu-berculosis involving cervical, thoracic, lumbar and sacral segments: a case report. Eur Spine J 2006; 15: 1019-24.


![Follow Sipi cantpancreatitis · tuberculous]Tuberculous 38. 2010167550 lymphaderioPathy [lymph Fallow Up: 4 Korea Republ.. 09-Sep- node 11. tuberculosis]Tuberculous Pleural effusion](https://img.pdfslide.us/doc/110x75/5f7d6a51d573d133e30b0217/follow-sipi-tuberculoustuberculous-38-2010167550-lymphaderiopathy-lymph-fallow.jpg)