Embed Size (px)
Citation preview
Department of Plastic Surgery, Helsinki University Central Hospital
Wihuri Research Institute
Helsinki, Finland
ACUTE ARTERIAL THROMBOSIS IN MICROSURGERY - CLINICAL AND
EXPERIMENTAL STUDIES
Eija Olsson
Academic dissertation
To be presented, with the permission of the Medical Faculty of the University of Helsinki, for
public examination in the lecture hall of Töölö Hospital, Helsinki University Central Hospital,
Helsinki, on December 14th, 2001, at 12 noon.
Helsinki 2001
SUPERVISED BY:
Docent Riitta Lassila, M.D.
Wihuri Research Institute and Department of Internal Medicine
Helsinki University Central Hospital
Helsinki, Finland
Professor Sirpa Asko-Seljavaara, M.D.
Department of Plastic Surgery
University of Helsinki
Helsinki, Finland
REVIEWED BY:
Docent Disa Lidman, M.D.
Department of Plastic Surgery, Hand Surgery, and Burns
University Hospital
Linköping, Sweden
Docent Jari Petäjä, M.D.
Hospital for Children and Adolescents
University of Helsinki
Helsinki, Finland
ISBN 952-91-4165-3 (nid.)
ISBN 952-10-0234-4 (PDF)
Yliopistopaino
Helsinki 2001
3
CONTENTS
ABBREVIATIONS 5 ORIGINAL PUBLICATIONS 6 ABSTRACT 7 1. INTRODUCTION 10 2. REVIEW OF THE LITERATURE 12 2.1. The thrombotic process 12 2.2. Activation of blood coagulation and fibrinolysis 14 The plasma markers for coagulation and fibrinolysis 14 The hypercoagulable state 15 The effect of surgery on coagulation and fibrinolysis 17 Coagulation and fibrinolysis activation in thrombotic manifestations 18
2.3. Anti-thrombotic agents and HEP-PG 19 Heparins: unfractionated heparin and low-molecular-weight heparin 19 Antiplatelet agents 22 Dextran 23 Thrombolytic agents 24 Other agents 24 HEP-PG 26 2.4. Experimental thrombosis research 27 Experimental thrombosis models 27 Methods for thrombosis evaluation 28 2.5. Histopathology of microvascular anastomoses 29 Histopathology in experimental microvascular models 29 Histopathology of human microvascular anastomoses 31 3. AIMS OF THE STUDY 33 4. MATERIALS AND METHODS 34 4.1. PATIENTS AND METHODS; CLINICAL PART - Studies I, II and III 34 4.1.1 Patients and microsurgical procedures (Studies I, II and III) 34 The TRAM group (study I) 37 The lower extremity trauma group (study II) 37 The cancer group (study III) 38 The vessel sample group (study I) 38 4.1.2. Blood sampling and analysis (Studies I, II and III) 39 4.1.3. Vessel samples and their histopathological and immunohistochemical analysis (Study I) 40 Vessel samples and associated clinical manifestations 40 Sample preparation 40 Immunohistochemistry 41 Immunohistochemical markers 41 Staining procedure 41 Evaluation of immunoreactivities 41
4
4.1.4. Statistics (Studies I, II and III) 42 4.2. ANIMALS AND METHODS; EXPERIMENTAL PART - Study IV 43 4.2.1. Animals and thrombosis models in experiments I-III 43 Experiments I-III 43 Animals and operating technique 43 Thrombosis models 45
Irrigation solutions and thrombin time 46 4.2.2. Methods for thrombosis evaluation 46 Patency testing (experiments I, II and III) 46 Scanning electron micrographs (SEM) (experiments I and III) 47 Measurement of Indium 111-labelled platelets (experiment II) 47 Platelet preparation and labelling 47 Blood sampling and injection of Indium 111-labelled platelets 48 Vessel samples and measurement of radioactivity 48 4.2.3. Statistics 48 5. RESULTS 49
5.1. Activation of coagulation and fibrinolysis in free flap surgery – association with flap failure (Studies I, II and III) 49
Outcome of the patients and intra- and postoperative thrombotic events 49 Preoperative hypercoagulable state 50 The time course of coagulation and fibrinolytic parameters 51
Thrombotic events and their correlation with operative factors and plasma markers 56
The overall correlation of plasma markers 59 The effect of LMWH (dalteparin) 62 5.2. Histopathology and immunohistochemistry of failed human
anastomoses (Study I) 63 Overall vessel morphology 63 Immunohistochemistry 64 Histopathology 66 5.3. Local anti-thrombotic effect of HEP-PG (Study IV) 66 Thrombin times and bleeding times 66 Patency rates 67 SEM analysis 68 Deposition of Indium 111-labelled platelets 70 6. DISCUSSION 71 7. CONCLUSIONS 78 8. ACKNOWLEDGEMENTS 79 9. REFERENCES 81

5
ABBREVIATIONS
ABC avidin-biotin complex
ACD acidic citrated dextrose
ADP adenosine 5´-diphosphate
ANOVA analysis of variance
ASA acetylsalicylicacid, aspirin
ASO arteriosclerosis obliterans
a-v arteriovenous
c-AMP adenosine 3´,5´-cyclic monophosphate
CRP C-reactive protein
ELISA enzyme-linked immunosorbent assay
FG fibrinogen
F1+2 prothrombin fragment 1+2
GP glycoprotein
HEP-PG heparin proteoglycan
LD latissimus dorsi
LMWH low molecular weight heparin
MFH malignant fibrous histiocytoma
MTS modified Tyrode Solution
PAI plasminogen activator inhibitor
PBS phosphate-buffered saline
PECAM platelet-endothelial cell adhesion molecule
PPP platelet-poor plasma
PRP platelet-rich plasma
SE standard error of mean
SEM scanning electron microscopy
TAT thrombin-antithrombin III complex
TFL tensor fasciae latae
tPA tissue-type plasminogen activator
TRAM transversus rectus abdominis musculocutaneous
UFH unfractionated heparin
vWF von Willebrand factor
6
ORIGINAL PUBLICATIONS
This thesis is based on the following original publications, which are referred to in the text by
their Roman numerals.
I Olsson E, Sarlomo-Rikala M, Böhling T, Asko-Seljavaara S, Lassila R.
Immunohistochemical evaluation of failed vessel anastomoses in clinical
microsurgery. Br J Plast Surg 2000; 53: 567-573.
II Olsson E, Svartling N, Asko-Seljavaara S, Lassila R. Activation of coagulation and
fibrinolysis in microsurgical reconstructions in lower extremities. Br J Plast Surg
2001; 54: 597-603.
III Olsson E, Svartling N, Asko-Seljavaara S, Lassila R. Activation of coagulation and
fibrinolysis during reconstructive microsurgery in patients with cancer.
Microsurgery 2001; 21: 208-213.
IV Olsson E, Asko-Seljavaara S, Lassila R. Topically administered macromolecular
heparin proteoglycans inhibit thrombus growth in microvascular anastomoses.
Thromb Haemost (in press, 2002).

7
ABSTRACT
Altough microvascular surgery is routine nowadays, the problem of intra- or postoperative
thrombosis still exists in under 5 % to 25 % of cases. The search for an ideal topical
antithrombotic agent therefore goes on. The aims of the present study were threefold: first, to
test sensitive new markers for coagulation and fibrinolysis during and after reconstructive
microsurgery in humans to see if there was any association with failures. Second, the failed
anastomoses were subjected to immunohistochemical analysis. Finally, a promising new
topical antithrombotic agent, native heparin proteoglycan (HEP-PG), was experimentally
tested in vivo in an anastomosis model in rats.
Coagulation and fibrinolytic markers were analysed in 24 patients in three different groups:
patients undergoing late breast reconstruction with a TRAM flap, patients with trauma or
chronic ulcer in the lower extremities, and patients with cancer in the oral cavity or the
extremities. The plasma markers analysed included fibrinogen, TAT, F1+2, D-dimer, tPA and
PAI-1. When assessed during microsurgical tissue transfers, thrombin generation as measured
by TAT and F1+2 associated with threatening flap failure and following reoperation. These
markers could also be used for the postoperative follow-up and evaluation of patients in need
of more intense antithrombotic therapy in order to avoid reoperations. Thrombin generation
was already seen before the operation in half of the TRAM patients with intraoperative
thrombosis, and at the time of thrombosis both thrombin generation and fibrinolysis activation
were evident in patients with obvious intraoperative thrombosis. Moreover, distinct thrombin
generation was observed at 24 h in one patient with subsequent edge necrosis. Patients with
lower extremity trauma who were in a hypercoagulable state before the operation and who
required reoperation showed consistent thrombin generation at the end of primary surgery,
which in part reflected coagulation activation due to excessive intraoperative bleeding.
Meticulous hemostasis during surgery might therefore help to diminish the need for
reoperations. Four out of seven patients with active cancer showed a preoperative
hypercoagulable state, and two of them also had a thrombotic event with consistent activation
of coagulation and fibrinolysis.
All patients had been given thrombosis prophylaxis with LMWH, dalteparin. The level of
anti-factor Xa activity was assessed as the indicator of the efficacy of LMWH. The level of

8
anti-factor Xa was under the recommended limit of 0.3 U/ml in all of the patients who had
received anticoagulation with LMWH, dalteparin, the previous evening, and even some of
those who had received it a few hours before the operation. Preoperative recognition of the
hypercoagulable state, especially in patients with recent trauma or active cancer, could
facilitate the targeting of meticulous antithrombotic protection perioperatively in these
patients. Thus, a question remaining for new studies is: could a better perioperative
anticoagulation control with LMWH help to reduce the risk of thrombotic events?
A total of 17 vessel samples were collected from 13 patients and subjected to
histopathological and immunohistochemical analyses. Analysis of the failed anastomoses
revealed that technical failures are rare. Immunohistochemical studies showed a lack of
endothelial cells adjacent to the anastomosis site as recognised by absent PECAM-1 staining,
and colocalised recruitment of platelets and fibrin. Of interest was the finding that PECAM-1
staining was absent in the single adherent layers of platelets but was found positive in micro
and larger thrombi. This suggests a difference in behaviour between thrombosis that retains
mural and thrombosis that extends to the lumen. The secondary thrombi at reoperations
showed clear inflammatory signs in vessels that could be associated with enhanced
coagulation and formation of fibrin-rich thrombi. Refined surgical techniques are essential to
minimise the anastomotic injury responsible for the local thrombotic response, but it should
be borne in mind that nearly all compromised anastomoses can be saved by having them
redone by an experienced microsurgical team. Enhanced antithrombotic treatment might also
support this salvage.
Finally, the antithrombotic effect of native macromolecular HEP-PG was tested in an
anastomosis model in rat common femoral arteries both acute and long term. We show that
topically applied native macromolecular HEP-PG (10 µg/ml) effectively inhibit thrombus
formation in microvascular arterial anastomoses in rats. The platelet thrombi induced during
this experimental microvascular surgery were minimal shortly (10 min) after the
thrombogenic challenge and remained so in the long term (72 h), too. These findings were
confirmed by SEM analysis and quantified with Indium 111-labelled platelets when compared
with saline, whereas unfractionated heparin at a 100-fold higher concentration failed to
markedly reduce the thrombotic response. The local antithrombotic effect of HEP-PG led to
neither prolonged anastomotic bleeding nor a systemic influence on platelet counts or
thrombin time. HEP-PG, by having a strongly retaining bond to extracellular matrix, seem to

9
have potential as a locally active antithrombotic agent in arterial circulation. This strategy is
applicable to microvascular surgery and to arteriovenous shunts, which frequently tend to
occlude in patients with renal failure needing permanent access to dialysis.

10
1. INTRODUCTION
Free microvascular tissue transplantations have become routine in plastic surgery, with
success rates ranging from 90 % to 99 % (Harashina 1988, Percival et al. 1989, Khouri 1992,
Suominen and Asko-Seljavaara 1995, Nieminen et al. 1999). According to the above authors,
re-exploration is needed in 6-25% of cases, the most common findings being either arterial
thrombosis or bleeding. The anastomosis itself promotes platelet adhesion and aggregation at
the needle holes and, in the event of severe vessel injury, a platelet thrombus will form
(Acland 1973, Yu-dong et al. 1989). Partial, dynamic thrombosis at the site of anastomosis
can seed microemboli downstream to the flap. These cause vasospasm mediated by platelet
metabolites, which can lead to secondary thrombosis (Barker et al. 1992, Weinzweig and
Gonzalez 1995). Kinking of vessels or compression due to haematoma, oedema or too tight
closure may also lead to diminished flow and secondary thrombosis (Percival et al. 1989,
Suominen and Asko-Seljavaara 1995, Rieck et al. 1995). In some cases, even the experienced
microsurgeon may have to redo an anastomosis several times during the primary operation
because of recurrent thrombosis without an obvious cause. This could reflect the procoagulant
state of the patient and insufficient anticoagulation therapy.
An increased risk of thromboembolic events threatens patients with recent trauma or
operation, infection or malignancy, who are in a hypercoagulable state before surgery
(Kudrjashov et al. 1969, Bennet and Towler 1985, Hoffman 1991, Falanga et al. 1993). Many
patients undergoing free flap transfer belong to this group. In addition, the surgery itself with
subsequent bleeding activates the coagulation and fibrinolytic systems not only at the wound
sites but also systemically (Brozovic 1977, Fujii et al. 1994, Komuro et al. 1998, Niemi et al.
1998). To evaluate the activation of the coagulation and fibrinolytic systems perioperatively,
highly specific and sensitive plasma markers for coagulation and fibrinolysis activity can be
measured by means of recently developed ELISA-based immunoassays (Yoda and Tsukasa
1981, Derlerck et al. 1987, Pelzer et al. 1988, Kluft and Verheijen 1990, Pelzer et al. 1991,
Merlini et al. 1998). We wanted to find out how the hypercoagulable state, which is thought
to be present in many patients, and the surgery itself affect the plasma markers, and also how
anastomotic failures, which are expected to occur in some patients, further affect these
markers. Furthermore, thrombosed anastomoses were subjected to histopathological and
immunohistochemical analyses. More insight into the pathophysiology of clot formation and

11
its dissolution is needed to enable us to target optimal therapeutic interventions in
microsurgery and thus to further reduce the risk of thrombotic events.
While thrombosis remains a problem in microsurgery, thrombosis research has focused on
antithrombotic and vasoactive agents (Buckley et al. 1994). Opinions about the use of
antithrombotic agents in free flap surgery and also the practice differ around the world
(Davies 1982, Salemark 1991, Siegel 1991). Systemic antithrombotic treatment with heparin,
dextran and ASA is commonplace, as is local irrigation with heparinised saline. However,
since systemic drugs may be used in excess and cause bleeding, research has lately focused on
topically applied agents, and the search for the ideal topical antithrombotic agent continues
(Cooley and Gould 1991, Das and Miller 1994). Recent studies on rat serosal mast cell -
derived heparin proteoglycans (HEP-PG) have shown that soluble or immobilised HEP-PG
can completely inhibit collagen-induced platelet aggregation in human blood in vitro (Lassila
et al. 1997). In this study we tested the inhibitory capacity of HEP-PG in vivo.
12
2. REVIEW OF THE LITERATURE
2.1. The thrombotic process
Thrombosis is a pathophysiological haemostatic response to vessel trauma. Numerous factors
affect the thrombotic process in arteries, e.g. the amount of injury on the vessel wall,
circulating blood platelets, the coagulation and fibrinolytic system and shear forces (Acland
1973, Nievelstein and de Groot 1988, Lassila et al. 1990, Johnson et al. 1993, Maraganore
1993, Barker et al. 1995, Ware and Coller 1995, Ruggeri 1997, Bassiouny et al. 1998). The
most important initial interactions occur with circulating blood platelets and subendothelial
layers of the injured vessel (Nievelstein and de Groot 1988, Tangelder et al. 1989, Ware and
Coller 1995).
Under normal conditions the intact endothelium presents a nonthrombogenic surface for
flowing blood. Endothelial cells do not only form a barrier; they can also synthesise, secrete,
bind and convert many substances involved in platelet function, coagulation and fibrinolysis.
Prostacyclin and nitric oxide are two known potent inhibitors of platelet activation secreted by
endothelial cells (Nievelstein and de Groot 1988, Ware and Coller 1995, Makhoul et al.
1999). The intact endothelium can, however, become a site for platelet adherence, e.g. when
inflammation, infection, cancer or some other chronic disease is present or when there is a
toxic reaction to certain drugs (Brozovic 1977, Nievelstein and de Groot 1988, Zacharski et
al. 1992, Donati 1995, Karpatkin et al. 1996, ten Cate et al. 1997, Makhoul et al.1999).
In microvascular anastomoses, the needle holes are the most thrombogenic sites for platelet
adherence (Acland 1973, Rosenbaum and Sundt 1977, Yo-dong et al. 1989). Once the
endothelium is damaged and the subendothelium or deeper layers are exposed, platelets will
rapidly adhere. Interstitial collagens of types I and III, which are located in the deeper layers,
are known to be the strongest inducers of platelet adhesion and aggregation (Kehrel 1995). In
small vessels, shear rates are high and platelet adhesion is enhanced (Ruggeri 1997). At high
shear rates, von Willebrand factor (vWF) mediates the initial binding of platelets to the
subendothelium via platelet membrane glycoprotein (GP) Ib (Nievelstein and de Groot 1988,
Ruggeri and Ware 1993, Ware and Coller 1995, Ruggeri 1997). Platelets can also adhere to
13
the exposed collagen direct via glycoprotein Ia/IIa-receptor (Ware and Coller 1995, Ruggeri
1997). Subsequently, the platelets are activated and cover the exposed surfaces by spreading
(Nightingale et al. 1980, Ruggeri and Ware 1993).
vWF and fibrinogen bind to the activated platelets, linking one to another via glycoprotein
IIb/IIIa-receptors in a process known as aggregation. Platelets are strongly activated when
adhesion to collagen or other subendothelial elements occurs, but also when thrombin is
formed (Ware and Coller 1995, Ruggeri 1997). Most of the activators are released and
synthesised locally at the site of injury. Activated platelets themselves are capable of secreting
proaggregatory substances, e.g. ADP and serotonin, of enzymatically converting arachinodic
acid to thromboxane A2, and of generating thrombin on their membrane phospholipids, thus
further promoting the growth of a sticky platelet plug (Nievelstein and de Groot 1988,
Maraganore 1993, Ware and Coller 1995).
The latticework of the thrombus is composed of fibrin strands. Activated platelets help to
convert fibrinogen into fibrin via the generation of thrombin. Thrombin, being the clotting
factor that is a potent physiological agonist activating platelets and inducing platelet
aggregation, mediates the thrombotic process in arteries (Maraganore 1993, Ware and Coller
1995). The amount of thrombin generated must be sufficient to overcome the inhibitory
mechanisms of the nearby endothelial cells, and other local and systemic anticoagulant
factors. Activated platelets accelerate thrombin formation on their membrane surface via the
activation of factor X by factors IXa and VIIIa, and via the activation of prothrombin by
factors Xa and Va. Membrane-associated thrombin generation is much faster than that
occurring in plasma, and membrane phospholipids contribute mainly to procoagulant
responses. Thrombin may also act locally at the site of arterial injury and cause vasospasm by
inducing contraction of vascular smooth muscle (Brophy et al. 1998). The initiation of
platelet contraction, resulting in clot retraction, is also caused by thrombin (Ware and Coller
1995).

14
2.2. Activation of blood coagulation and fibrinolysis
The plasma markers for coagulation and fibrinolysis
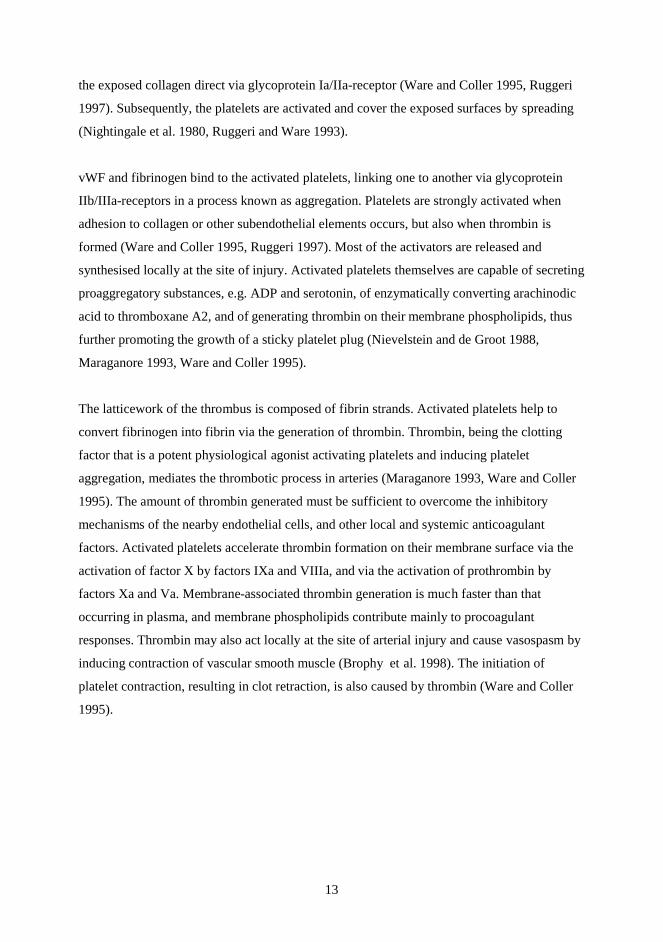
The complex system of blood coagulation cascade includes extrinsic or tissue factor pathway,
which is currently thought to be the principal initiating pathway, intrinsic pathway and final
common pathway leading to the generation of thrombin, see Figure 1 (Colman et al. 1994).
Fibrinogen is an acute phase protein and the source of fibrin formation (Kwaan and Barlow
1973, Brozovic 1977, Bennett and Towler 1985). Analysis of the generation of thrombin, the
enzyme which converts fibrinogen into fibrin, includes fibrinopeptide A (FPA), prothrombin
fragment 1+2 (F1+2), thrombin-antithrombin III complex (TAT) and activated protein C
(APC) (Pelzer et al. 1988, Pelzer et al. 1991, Szczeklik et al. 1992, Merlini et al. 1998). When
prothrombin is converted to thrombin via a proteolytic reaction, inactive prothrombin
fragment 1+2 (F1+2) is released (Merlini et al. 1998). As thrombin converts fibrinogen into
fibrin, fibrinopeptides A and B are released. The natural inhibitor of thrombin in plasma is
antithrombin III, which forms a complex with thrombin (TAT) (Colman et al. 1994, Merlini
et al. 1998). Thrombin can also bind to thrombomodulin on endothelial cells, leading to
activation of protein C, which is a circulating anticoagulant (Fernandez et al. 1997, Merlini et
al. 1998, Dahlbäck 2000). Besides these two inhibitors, tissue factor pathway inhibitor is of
great importance in regulating coagulation activation (Broze 1995).
The main function of the fibrinolytic system is to limit clot formation and degrade the fibrin
deposits formed (Colman et al. 1994). The key enzyme capable of doing this is plasmin,
which is formed from plasminogen after proteolytic activation (Lijnen and Collen 1995).
Analysis of plasmin generation consists of D-dimer, a fibrin degradation product reflecting
fibrinolysis, and the activity of tissue-type plasminogen activator (tPA) and plasminogen
activator inhibitor-1 (PAI-1), the two regulators of fibrinolysis (Bennett and Towler 1985,
Rånby et al. 1986, Derlerck et al. 1987, Kluft and Verheijen 1990, Lijnen and Collen 1995).
D-dimer, reflecting in part thrombin action before clot formation as well as ongoing
fibrinolysis, is formed after crosslinked fibrin is digested by plasmin (Colman et al. 1994).
Tissue-type plasminogen activator is the main activator of circulating plasminogen and is
released from endothelial cells. The activation is inhibited by plasminogen activator inhibitors
(PAI), of which PAI-1 is the most important. These serve to facilitate fibrin formation during
15
the period when hemostatic plug is formed. Fibrinolytic system can also be inhibited via α2-
antiplasmin or thrombin-activatable fibrinolysis inhibitor (TAFI) (Colman et al. 1994, Bajzar
et al. 1995).
Figure 1. Schematic, simplified presentation of the coagulation and fibrinolytic systems relevant to this study. The plasma markers measured here are in shaded boxes. Of the inhibitors of the coagulation system only antithrombin is presented, and of the inhibitors of plasminogen activators only PAI-1, which is the most important.
The hypercoagulable state
Hypercoagulable states are classified as either primary or secondary. Primary
hypercoagulable states are mostly due to inherited mutations of physiological antithrombotic
factors leading to antithrombin/heparin disorders, protein C/protein S disorders or fibrinolytic
Prothrombin
Prothrombin fragment 1+2 (F 1+2)
Tissue factor (extrinsic), intrinsic, and
common pathways
Thrombin
Antithrombin III
Trombin-antithrombin complex (TAT)
Fibrinogen Fibrin
Fibrin degradation products, D-dimer
Plasminogen Plasmin
Tissue-type plasminogen activator (tPA)
Plasminogen activator inhibitor 1 (PAI-1)

16
disorders. Secondary hypercoagulable states are mostly acquired, multifactorial and complex
abnormalities of the haemostatic system. In secondary hypercoaglulable states diverse
abnormalities in blood flow, blood composition and vessel wall can be found, e.g. in obesity,
trauma, pregnancy, cancer and diabetes (Schafer 1997). According to a broad definition, in a
hypercoagulable state the coagulation mechanism is activated in the blood without signs of
thrombosis, and in the presence of additional prothrombotic stimuli it may develop into an
overt thrombotic event (Schafer 1997, Merlini et al. 1998). Such additional prothrombotic
stimuli could be stress, operation or other trauma, the last two subsequently followed by an
acute phase reaction and a period of posttraumatic hypercoagulability (Brozovic 1977,
Bennett and Towler 1985, Hoffmann 1991).
The hypercoagulable or thrombophilic state in cancer patients has long been recognised
(Kudrjashov et al. 1969, Yoda and Abe 1981, Rickles et al. 1992, Falanga et al. 1993, Donati
1996, Karpatkin et al. 1996, Falanga and Rickles 1999, Kaviani and Organ Jr 1999).
Procoagulant activation is revealed in many cancer patients by elevated levels of fibrinogen,
fibrinopeptide A, F1+2, TAT and D-dimer (Yoda and Abe 1981, Zacharski et al. 1992,
Falanga et al. 1993, Donati 1996, von Tempelhoff et al. 1997, Gouin-Thibault and Samama
1999, López et al. 1999, Kalweit et al. 2000); in some patients also enhanced fibrinolytic
activation is shown by intensified tPA and PAI activity (Zacharski et al. 1992, Schmitt et al.
1997, von Tempelhoff et al. 1997, Carroll and Binder 1999). These markers are now known
to be prognostically associated (Gouin-Thibault and Samama 1999). Enhanced
anticoagulation therapy is therefore recommended in cancer patients in the context of surgery
or chemotherapy (Rickles et al. 1992, Falanga et al. 1993, Donati 1995, Gondret et al. 1995,
Zacharski and Ornstein 1998, Bona 1999, Gouin-Thibault and Samama 1999, Lee and Levine
1999).
In both acute and chronic cardiovascular diseases, the activation of blood coagulation can be
measured by elevated fibrinogen, FPA, F1+2, TAT and /or D-dimer (Lassila et al. 1993,
Merlini et al. 1994, Peltonen et al. 1995, Ernofsson et al. 1998, Merlini et al. 1998,
Holmberg et al. 1999, López et al 1999). Here, treatment with LMWH was found to diminish
both thrombin generation and activity (Ernofsson 1998). Thrombi stability is counteracted by
the fibrinolytic system, tPA and PAI-1, which have also been reported to be related to well
known cardiovascular risk factors, e.g. age, sex, blood pressure and centrally located body fat
(Rånby et al. 1986, Sundell et al. 1989). Elevated levels of tPA have been recorded in

17
arteriosclerotic patients with aneurysmal and occlusive aorta (Shireman et al 1997). Also,
upregulation of PAI-1 has been observed in patients with patent venous grafts (Peltonen et
al.1996).
In severe injuries such as pelvic and long bone fractures and abdominal and chest injuries,
elevation of D-dimer has been reported in the majority of patients on the 1st day after trauma,
the levels correlating with the injury severity score (Chen et al. 1999, Peetz et al 2000). PAI-1
activity was also elevated in trauma patients at admission and was followed by a progressive
decline from day 2 onwards (Chen et al. 1999). On the 1st day after burn trauma, both
hypercoagulability and hyperfibrinolysis have occurred with elevated TAT, D-dimer and tPA,
the hypercoagulability persisting for at least 1 week after trauma. Also, non-survivors were
found to have higher levels of TAT and tPA than survivors on the 1st day after trauma
(Garcia-Avello et al. 1998). Furthermore, in acute infections such as sepsis and endotoxaemia,
activation of coagulation has been reported with elevated F1+2 and TAT levels (ten Cate et al.
1997).
The effect of surgery on coagulation and fibrinolysis
During surgery, fibrinogen levels have been shown to decrease partly due to haemodilution
and bleeding (Murray et al. 1988, Strauss et al. 1988, Fujii et al. 1994, Peltonen et al. 1996,
Egli et al. 1997, Niemi et al. 1997, Peltonen et al. 1997), but a protracted increase in
fibrinogen and FPA levels has been found to persist for a week or more after operation or
trauma (Brozovic 1977, Bennett and Towler 1985, Fujii et al. 1994, Moor et al. 2000). Both
thrombin generation, as measured by TAT and F1+2, and fibrinolysis, as measured by D-
dimer and tPA, are activated during surgery. The short-lived elevation of tPA is followed by a
marked reduction on the 1st postoperative day. This condition, known as fibrinolytic
shutdown, is mostly due to increased levels of PAI-1 (D’Angelo et al. 1985, Kluft et al.
1985).
During intracranial surgery, transient activation of coagulation has been reported with
elevated TAT levels, as well as activation of fibrinolysis in response to trauma with elevated
D-dimer, tPA and PAI-1 (Fujii et al. 1994, Peltonen et al. 1997). After laparoscopic
cholecystectomy, activation of coagulation and increased fibrin turnover were found with
18
elevated F1+2, D-dimer and fibrin degradation products, whereas tPA activity was found to
be increased intraoperatively (Rahr et al. 1999). Patients with pulmonary malignancies
showed an intraoperative increase in F1+2 and D-dimer levels, whereas TAT remained
unchanged during the operation (Kalweit et al. 2000). In neonates, increased levels of F1+2,
tPA and PAI-1 were reported during cardiopulmonary bypass, and tPA remained elevated on
the 3rd postoperative day when D-dimer levels were also elevated (Petäjä et al. 1996). After
coronary artery bypass grafting, activation of coagulation was shown by elevated TAT on the
3rd postoperative day, and an increase in plasminogen activator inhibitor-1 levels on the 1st
postoperative day predicted graft failure (Moor et al. 2000). In orthopaedic surgery, elevated
TAT on the 1st postoperative day was followed by a continuous decrease, whereas D-dimer
decreased on the 1st postoperative day followed by a continuous increase up to the 8th
postoperative day. D-dimer levels above 2 mg/l on the 4th postoperative day were related to
thromboembolic complications, and D-dimer levels were monitored to adjust the dose of
LMWH (Peetz et al. 2000). Anticoagulant treatment has also been shown to lower the levels
of thrombin generation, F1+2 and TAT, during the perioperative period when there is
considerable need for thrombosis prophylaxis (Amelsberg et al. 1992, van Wersch et al.
1992).
Activation of both coagulation and fibrinolysis is also seen during ischaemia and reperfusion.
Activation of the coagulation system, measured by F1+2, TAT and soluble fibrin levels, was
reported during open abdominal aortic surgery and persisted 1 week after the operation. Here,
thrombin generation was stimulated mainly by ischaemia and reperfusion of the lower part of
the body (Holmberg et al. 1999). After supraceliac aortic clamping, activation of fibrinolysis
has been shown by elevated levels of tPA (Illig et al. 1997). Venous occlusion and the use of
a tourniquet followed by ischaemia have been noted to enhance fibrinolysis by elevating D-
dimer, tPA and PAI levels, as well (Petäjä et al. 1987, Syrjälä et al. 1993, Niemi et al. 1996).
Coagulation and fibrinolysis activation in thrombotic manifestations
In acute myocardial infarction, thrombin generation is reflected in increased FPA, F1+2 and
TAT levels in plasma, and a persistent hypercoagulable state, as measured with F1+2,
continues for up to 6 months after the acute phase (Szczeklik et al. 1992, Merlini et al. 1994).
In brain infarction, activation of coagulation and fibrinolysis varies in different subtypes: in

19
cardioembolic stroke, the elevation in TAT and D-dimer occurs within 48 h and persists for 1
month, whereas in atherothrombotic stroke there is an increase only in D-dimer 1 week after
onset (Takano et al. 1992). When patients with sudden arterial occlusion in the lower
extremities were compared with patients with stable peripheral arterial occlusive disease, both
coagulation and fibrinolysis, as measured by TAT, D-dimer, tPA and PAI-1 levels, were
clearly activated during the occlusion, and increased levels of TAT and PAI-1 correlated with
a poor outcome (Peltonen et al. 1995). Also, during acute deep vein thrombosis and
pulmonary embolism, activation of coagulation can be detected as elevated F1+2 and TAT
levels, and the activation of fibrinolysis as increasing levels of soluble D-dimer and tPA
(Declerck et al. 1987, Pelzer et al. 1988, Boneu et al. 1991, Pelzer et al. 1991, Meissner et al.
2000). Local thrombotic events in microsurgery have so far been studied in a limited number
of patients, and here only two patients showed an increase in F1+2 and TAT, the markers of
thrombin generation, at the time of threatening or obvious thrombosis and subsequent flap
failure (Komuro et al. 1998).
2.3. Antithrombotic agents and HEP-PG
Antithrombotic agents act by reducing platelet aggregation, by inhibiting the coagulation
cascade or by augmenting fibrinolysis (Tangelder et al. 1989, Johnson and Barker 1992,
Maraganore 1993). In microsurgery, the agents are used either systemically or locally. The
systemic agents inlude anticoagulants, antiplatelet drugs, plasma expanders and thrombolytic
agents. In addition, agents causing peripheral vasodilatation are used. Locally administered
agents include anticoagulants and thrombolytic agents, and are used either topically or as
intra-arterial infusion (Salemark 1991, Siegel 1991, Johnson and Barker 1992).
Heparins: unfractionated heparin and low-molecular-weight heparin
Unfractionated heparin (UFH), the traditional golden standard anticoagulant, is a
heterogeneous preparation of glycosaminoglycans derived from porcine intestinal mucosa
with molecular weights ranging from 3000 to 30,000 (Murray et al. 1936, Ehrlich and Stivala
1973, Salzman et al. 1980, Hirsh et al. 2001). It acts indirectly by inhibiting the conversion of
fibrinogen into fibrin through interaction with antithrombin III (Salzman et al. 1980, Hirsh et
20
al. 1998). Heparin-antithrombin III complex inactivates thrombin and factor Xa and also
many other factors in the clotting cascade (Jeske and Fareed 1993, Hirsh et al. 1998). The
binding of heparin to antithrombin III is reversible and time-dependent, the half-life of its
anticoagulant activity being 1-1.5 h (Ehrlich and Stivala 1973, Dawes 1993).
Heparin can also reduce tissue factor production by binding to monocytes, and release tissue
factor pathway inhibitor amplifying anticoagulation independent of antithrombin III (Dawes
1993, Engelberg 1996). Endothelial cells take up heparin against a concentration gradient, and
by increasing the negative surface charge heparin can also prevent platelet and red cell
attachment to the endothelium (Hiebert and Jaques 1976). Heparin can lower plasma viscocity
by lowering plasma fibrinogen levels, and it also enhances fibrinolysis (Ehrlich and Stivala
1973, Engelberg 1996).
The inhibitory capacity of heparin against thrombin could be beneficial in hindering tumour
cell growth, as thrombin is known to enhance the progression of many tumours. The
antioxidant effects of heparin may also play a role in malignancy (Karpatkin et al. 1996,
Zacharski and Ornstein 1998). Heparin has anti-inflammatory properties as well.
Despite its anticoagulant properties, heparin has limited effect on the arterial thrombotic
process. Both fibrin- and subendothelial matrix-bound thrombin have shown resistance to the
inactivating effect of heparin-antithrombin III complex, and circulating heparin may thus be
incapable of preventing thrombosis (Maraganore 1993, Hirsh et al. 1998). Heparin also exerts
prothrombotic effects on platelets as a result of saturable, specific and reversible binding
between heparin and platelets (Dawes 1993). Activated platelets secrete platelet factor 4,
which is capable of neutralising the effect of heparin. This in part explains the limited
antithrombotic effect of heparin on platelet-rich thrombi (Maraganore 1993, Ware and Coller
1995, Arnljots et al. 1997). Also, in some diseases, e.g. ischaemic coronary syndromes,
variable responses, even resistance, to heparin have been observed making the therapy
unpredictable and less than optimal (Maraganore 1993, Hirsh et al. 2001).
In clinical microsurgery, heparin has mostly been used systemically perioperatively to prevent
thrombosis or in the event of obvious thrombosis, intraoperatively or at reoperation (Salemark
1991, Johnson and Barker 1992). Complications during parenteral high-dose heparin therapy,
haematoma and bleeding, have been reported to occur especially in combination with dextran
21
or ASA (Salemark 1991, Kroll et al. 1995). At some centres heparin is given systemically in
low doses or boluses during the perioperative period, a practice considered safer as the rate of
complications has not increased (Kroll et al. 1995). In experimental microsurgery, however,
the effect of heparin boluses has been found doubtful (Arnljots and Bergqvist 1995). Heparin
has also been administered successfully as a continuous, local intra-arterial infusion both
experimentally and clinically (Fukui et al. 1989, May and Rothkopf 1989, Maeda et al. 1990).
In a recent study, postoperative treatment with heparin alone or in combination with dextran
did not improve the survival of free tissue transfers (Deutinger et al. 1998).
Local instillation of heparin is commonly used at anastomosis either alone or in combination
with other systemic agents, e.g. dextran (Salemark 1991, Johnson and Barker 1992).
Experimental studies have shown that local instillation of heparin hinders thrombosis in
microanastomoses and traumatised vessels, although contradictory results have also been
obtained (Rosenbaum and Sundt 1977, Sinclair 1980, Zinberg et al. 1989, Wieslander and
Dougan 1990, Cox et al. 1992, Das and Miller 1994, Chen et al. 1996). Applied topically, in
concentrations of at least 50 U/ml, heparin has successfully inhibited thrombin activity on the
damaged vessel wall, but this was not found when heparin was used systemically in optimal,
safe concentrations (Johnson and Barker 1992). Administered systemically, heparin is capable
of inhibiting only soluble thrombin, not thrombin already bound to fibrin and subendothelial
matrix; therefore the application of heparin locally at anastomosis could be a valid option.
Low molecular-weight heparins (LMWH) are chemically obtained fragments of
unfractionated heparin with a mean molecular weight of 5000. Their half-life is 2-4 times
longer than that of UFH; they have dose-independent clearance and are almost completely
absorbed when injected subcutaneously, thus making the anticoagulant response more
predictable than that of UFH (Bergqvist et al. 1983, Bergqvist 1996, Weitz 1997, Hirsh et al.
1998, Nader et al. 1999). Like unfractionated heparins, LMWH bind to and activate
antithrombin III, but LWMH have greater activity against factor Xa than against factor IIa
(thrombin) when compared with UFH (Serra et al. 1997, Hirsh et al. 1998). If thrombin is
fibrin-bound, LMWH cannot inactivate it, either. Also, like unfractionated heparin, LMWH
can release tissue factor pathway inhibitor, thus enhancing their anticoagulant activity (Weitz
1997). The selective decline in circulating antithrombin and tissue factor pathway inhibitor
during infusion of UFH, but not during subcutaneous LMWH treatment, might also explain
the better efficacy of LMWH over UFH (Hansen J-B and Sandset PM 1998). The LMWH
22
affinity for cell receptors is lower than that of UFH, and their effects are more likely mediated
through mechanisms other than cellular interactions, which accounts for their better
bioavailability (Dawes 1993, Weitz 1997). LMWH have also been shown to be less active
than UFH in inducing platelet aggregation (Salzman et al. 1980). LMWH have fewer side
effects than UFH. They have been reported to cause less bleeding, since platelet function and
the platelet-vessel wall interaction are less inhibited, and microvascular permeability is not
increased (Weitz 1997, Zacharski and Ornstein 1998). Moreover, the risk of heparin-induced
thrombocytopaenia, as well as osteoporosis, seems to be lower when LMWH are used (Weitz
1997). LMWH, like UFH, possess anti-inflammatory properties (Downing et al.1998).
In clinics, LMWH are used as subcutaneous injections to prevent and treat thromboembolic
events, that is, deep vein thrombosis and pulmonary embolism, in the context of surgery and
trauma and also to treat unstable angina and acute myocardial ischaemia (Gondret et al. 1995,
Weitz 1997, Turpie 1999). To date, their effect in hindering arterial thrombosis at the level of
microanastomoses, whether in systemic or topical use, has been demonstrated only in animal
studies (Zhang and Wieslander 1992, Zhang et al. 1993, Chen et al. 1995, Kroll et al. 1995).
Antiplatelet agents
Acetylsalicylic acid (ASA) is the traditional, most widely used antiplatelet agent (Nichter and
Bindiger 1988, Tangelder et al. 1989, Johnson and Barker 1992, Ware and Coller 1995).
Platelet aggregation is inhibited through the arachinodic acid pathway. Via the irreversible
inhibition of cyclo-oxygenase prostaglandin synthesis and the production of
proaggregant/vasoconstrictor, thromboxane A2 is blocked for the whole lifespan of platelets
treated with small amounts (> 50 mg) of peroral ASA. A sign of the antiplatelet effect is
prolonged bleeding time. Large doses of ASA inhibit cyclo-oxygenase -dependent
prostacyclin production in endothelial cells but only temporarily, due to rapid synthesis. As
anucleic platelets lack the machinery for synthesis, the effect of ASA is eliminated only in
platelets newly liberated from bone marrow megakaryocytes (Ware and Coller 1995).
With its 25-30% secondary preventive efficacy on atherothrombotic events clinics have long
used ASA in prevention of cardio- and cerebrovascular diseases [Antithrombotic Trialists’
(ATT) Collaboration 2001]. As a new antiplatelet alternative, clopidogrel, an ADP-receptor

23
antagonist, offers secondary prevention for patients insensitive or unresponsive to ASA
(Gachet 2000). In experimental microsurgical studies, ASA has effectively hindered platelet
aggregation but not necessarily thrombus formation (Folts et al. 1976, Rosenbaum and Sundt
1977, Cooley et al. 1987, Buckley et al. 1994). Many microsurgical centres use ASA
perioperatively, often in combination with dextran. (Salemark 1991, Siegel 1991, Johnson and
Barker 1992).
Other antiplatelet agents are prostacyclin and its analogues. Prostacyclin is a platelet
antiaggregator endogenously formed by endothelial cells from arachinodic acid (Tangelder et
al. 1989). It acts by increasing the level of c-AMP in platelets, thus inhibiting the activation,
as well as aggregation, of platelets. It is also vasodilatory. As exogenous prostacyclin is
unstable and has a short half-life, more stable analogues have been developed. Dipyridamole,
a phosphodiesterase inhibitor, works not only on the level of c-AMP but by raising the level
of platelet antagonist adenosine in plasma. In experimental microsurgical studies the effects
have been contradictory, and only some centres use them, either postoperatively alone or in
combination with ASA (Salemark 1991, Salemark et al. 1991, Savoie et al. 1991, Siegel
1991, Salemark et al. 1995).
Dextran
Dextran is a polysaccharide normally used as a plasma expander. It has both low-molecular
weight (40,000) and high molecular weight forms (70,000) (Ljungström K-G 1988). Its
antithrombotic properties are due to a reduction in platelet adhesion, a decrease in factor VIII-
related antigen activity, a reduction in platelet aggregation and a decrease in blood viscosity.
Fibrin formation and stabilisation are also impaired (Batlle et al 1985, Wieslander et al. 1986,
Johnson and Barker 1992, Wolfort et al. 1992, Buckley et al. 1994). Dextran causes fewer
haemorrhagic complications than heparin. Due to its antigenicity, however, allergic reactions
can occur, but they are rare (Ljungström K-G 1988, Siegel 1991).
The antithrombotic efficacy of dextran in preventing deep vein thrombosis and pulmonary
enbolism in the context of surgery is well known (Ljungström K-G 1988). In experimental
microsurgery, both short- and long-term studies have shown that dextran is effective in
hindering arterial thrombosis either alone or in combination with other antithrombotic agents
24
(Savoie et al. 1991, Wolfort et al. 1992, Zhang and Wieslander 1993, Buckley et al. 1994,
Rooks et al. 1994). In clinical microsurgical pratice, dextran is widely used intra- and
postoperatively alone or in combination with heparin or ASA (Salemark 1991, Siegel 1991).
Thrombolytic agents
The thrombolytic drugs streptokinase and tPA activate the endogenous fibrinolytic system.
They activate fibrinolysis by converting plasminogen to plasmin. The proteolytic enzyme
plasmin then lyses fibrin in clots. Streptokinase activates plasminogen in circulation and tPA
on the clot surface. Streptokinase lacks selectivity for fibrin, causing fibrinogen depletion.
Streptokinase can thus cause complications such as bleeding and allergic reactions (Johnson
and Tillett 1952, Goldberg et al. 1989, Rooks et al. 1994, Hashim et al. 1996). The advantages
of tissue plasminogen activator over streptokinase are that it binds specifically to fibrin and
not to circulating fibrinogen, initiating fibrinolysis only locally and leaving fibrinogen largely
undepleted, which diminishes the risk of haemorrage. Also, tPA is nonantigenic and has a
shorter half-life than streptokinase (Hashim et al. 1996, Lykoudis et al. 2000).
In routine clinical practice, they are used to treat acute myocardial infarction. Microsurgical
experimental studies have demonstrated their efficacy in hindering stable thrombus formation
or in lysing clots either alone or in combination with other antithrombotic agents, but
contradictory results have also been presented (Johnson and Tillett 1952, Levy et al. 1991,
Savoie et al. 1991, Arnljots et al. 1994, Rooks et al. 1994, Chen et al. 1995). In clinical
microsurgery, these agents are used mainly in the event of manifest thrombosis (Fukui et al.
1989, Goldberg et al. 1989, Salemark 1991, Siegel 1991, Hussein et al. 1996, Theile and
Coombs 1996).
Other agents
A variety of other substances have been tested experimentally and found to improve
microvascular patency. The most potent inhibitors of thrombin are hirudin and its
recombinant form (Arnljots and Bergqvist 1995, Zhang and Wieslander 1996, Hirsh and
Weitz 1999). Like heparin, hirudin is capable of inhibiting circulating thrombin in plasma.
Hirudin exerts its inhibitory effect on thrombin via a direct active-site mechanism whereas

25
heparin needs a cofactor, antithrombin III. In addition to this, hirudin can inhibit fibrin-bound
thrombin but heparin can only attack the circulating enzyme. The antithrombotic effects of
hirudin have been found even after its plasma clearance, implying that treatment with single
boluses could be effective in hindering thrombus formation.
Tissue factor pathway inhibitor, a protein inhibitor naturally secreted from platelets and
bound to plasma lipoproteins, exerts its effect on the extrinsic pathway of coagulation by
binding to and inhibiting tissue factor and factor VIIa and also factor Xa (Ware and Coller
1995). It has specific binding sites on the injured vessel wall when topically applied, and as a
topical antithrombotic agent it is more effective than heparin (Ozbeck et al. 1995). In a large,
multicentre clinical study, topically applied recombinant human tissue factor pathway
inhibitor was as efficacious as locally instilled heparin in preventing thrombosis in free flap
surgery (Khouri et al. 2001).
Another agent that works on the level of the extrinsic pathway is active site-inactivated factor
VIIa (Arnljots et al. 1997). Normally the extrinsic pathway of coagulation is initiated after
tissue factor from the injured vessel wall binds to factor VIIa, the complex further activating
factor IX and factor X, and finally leading to thrombin generation. Here, thrombin formation
could be blocked at the very first step by using modified factor VIIa, which is capable of
binding to tissue factor but has an inactivated enzymatic site. Here, too, the antithrombotic
effect of the agent when topically applied was better than that of heparin boluses and there
were no haemorragic side effects. A recent study found this effect with systemic
administration, too (Söderström et al. 2001). An earlier study, however, reported an increase
in duration and episodes of anastomotic bleeding (Sørensen et al. 1999).
Pentoxifylline, a haemorrheologic agent normally used in clinics to treat claudication,
increases erythrocyte flexibility and microcirculatory flow, and reduces blood viscosity. It
also decreases platelet hyperactivity, and may lower fibrinogen levels. Pentoxyfylline has
further been shown to decrease levels of platelet-activating factor and thereby to reduce the
amount of tissue injury caused by ischaemia-reperfusion (Adams et al. 1995). A significant
improvement on patencies has been seen in severe trauma models in animals treated with this
agent, and it is used at some microsurgical centres (Siegel 1991, Kronen et al. 1994).
In addition to these, vasodilatory agents have been found to improve microvascular patency.

26
Phentolamine, which dilates vascular smooth muscle, has been beneficial in experimental
studies when topically applied (Reichel et al. 1988). At clinics some centres use vasodilators
intraoperatively, e.g. xylocaine and papaverine, to treat spasm or postoperatively, e.g.
chlorpromatzine, to enhance peripheral circulation (Siegel 1991, Khouri 1992).
HEP-PG
The soluble heparin proteoglycans (HEP-PG) are released from mast cell cytoplasmic
secretory granules after their exocytosis, and have a molecular weight of 750 000 (Yurt et al.
1977). They contain heparin and chondroitin sulphate glycosaminoglycan chains, one HEP-
PG monomer consisting of approximately 10 heparin glycosaminoglycan chains (MW 75
000) (Lindstedt et al. 1992, Lassila et al. 1997). In vitro HEP-PG were found to totally inhibit
collagen-induced platelet aggregation and subsequent serotonin release, due to the heparin
glycosaminoglycan component and HEP-PG macromolecular structure. This inhibitory effect
is lacking or minimal in standard heparins, see Table 1. HEP-PG did not block glycoprotein
Ia/IIa-mediated platelet adhesion at high shear rates, but they did reduce GPIa/IIa –induced
activation. Also, thrombin-induced platelet aggregation and von Willebrand factor binding to
glycoprotein receptor IIb/IIIa were reduced (Lassila et al. 1997). Recently, similar results
were obtained with HEP-PG immobilised together with collagen (Kauhanen et al. 1998).
HEP-PG inhibited release reaction from the adherent platelets as well. HEP-PG have further
been shown to have an inhibitory effect on rat aortic smooth muscle cell proliferation (Wang
and Kovanen 1999). When cutaneous mast cells were stimulated by subjecting them to an
allergenic challenge, bleeding time was prolonged and thrombin generation reduced
(Kauhanen et al. 1998).
27
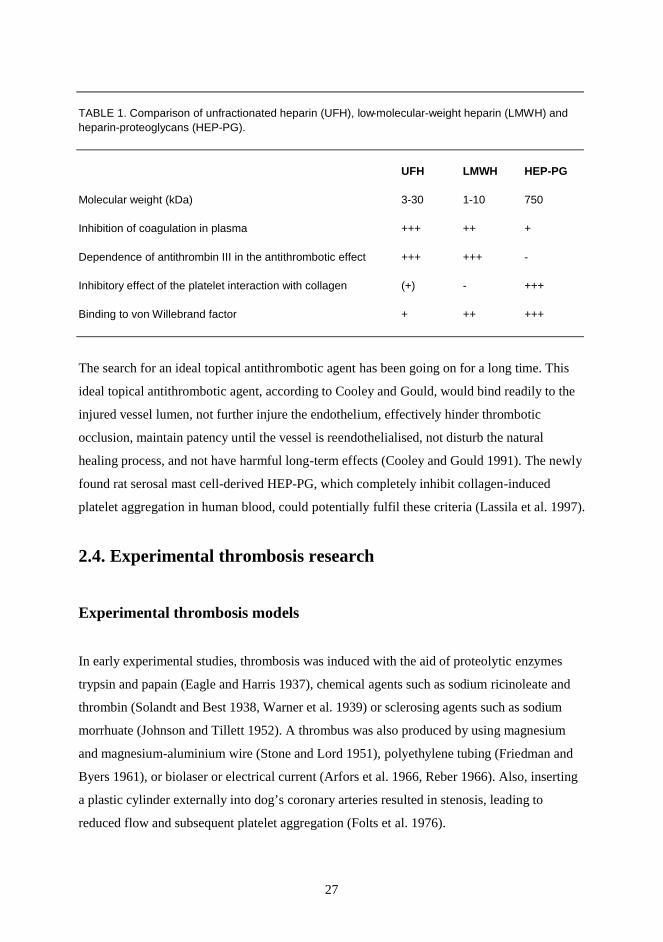
TABLE 1. Comparison of unfractionated heparin (UFH), low-molecular-weight heparin (LMWH) and heparin-proteoglycans (HEP-PG).
UFH LMWH HEP-PG
Molecular weight (kDa) 3-30 1-10 750
Inhibition of coagulation in plasma +++ ++ +
Dependence of antithrombin III in the antithrombotic effect +++ +++ -
Inhibitory effect of the platelet interaction with collagen (+) - +++
Binding to von Willebrand factor + ++ +++
The search for an ideal topical antithrombotic agent has been going on for a long time. This
ideal topical antithrombotic agent, according to Cooley and Gould, would bind readily to the
injured vessel lumen, not further injure the endothelium, effectively hinder thrombotic
occlusion, maintain patency until the vessel is reendothelialised, not disturb the natural
healing process, and not have harmful long-term effects (Cooley and Gould 1991). The newly
found rat serosal mast cell-derived HEP-PG, which completely inhibit collagen-induced
platelet aggregation in human blood, could potentially fulfil these criteria (Lassila et al. 1997).
2.4. Experimental thrombosis research
Experimental thrombosis models
In early experimental studies, thrombosis was induced with the aid of proteolytic enzymes
trypsin and papain (Eagle and Harris 1937), chemical agents such as sodium ricinoleate and
thrombin (Solandt and Best 1938, Warner et al. 1939) or sclerosing agents such as sodium
morrhuate (Johnson and Tillett 1952). A thrombus was also produced by using magnesium
and magnesium-aluminium wire (Stone and Lord 1951), polyethylene tubing (Friedman and
Byers 1961), or biolaser or electrical current (Arfors et al. 1966, Reber 1966). Also, inserting
a plastic cylinder externally into dog’s coronary arteries resulted in stenosis, leading to
reduced flow and subsequent platelet aggregation (Folts et al. 1976).

28
In the early years of clinical microsurgery Acland made experiments on the effects of
different surgical traumas on rat femoral vessels including pinching, pulling, scraping,
incising and suturing the vessels, and came to the conclusion that the greatest trauma was
created by an incision closed by a single suture (Acland 1973). The anastomosis model was
one of the first to be used and still is favoured in various contexts (Baxter et al. 1972, Acland
and Trachtenberg 1977, Rosenbaum and Sundt 1977, Nightingale et al. 1980, Wieslander et
al. 1982, Yu-dong et al. 1989, Johnson et al. 1993, Boeckx et al. 1994, Sigurbjörnsson et al.
1994). Since then, various new models have been developed and used to study thrombus
formation and the effects of trauma and to test the effect of new antithrombotic agents. The
arterial inversion graft model has been used alone or in combination with crush injury (Kersh
et al. 1989, Kronen et al. 1994). Crush injury combined with arteriotomy, intimal abrasion
and stasis (Davidson et al. 1990, Buckley et al. 1994), crush injury and venotomy (L evy et al.
1991), crush-avulsion injury (Cooley et al. 1987, Rooks et al. 1993, Fu et al. 1995) and crush
injury alone or combined with anastomosis have all been used during the past decade
(Stockmans et al. 1991, Chen et al. 1996). Other methods have included arteriotomy
combined with intimectomy (Wieslander et al. 1990, Zhang and Wieslander 1996),
arteriotomy and an inverted flap (Barker et al. 1992), anastomosis with a twisted pedicle
(Ozbek et al. 1994, Atchabahian and Masquelet 1996), intimal abrasion with a twisted pedicle
(Brown et al. 1995), clamp injury alone or combined with stasis (Jackiewicz et al. 1996,
Thomson et al. 1998), clip ligature (Kashyap et al. 2001), the erroneous placing of a stitch in a
vein and venous anastomosis with a knotted sut ure (Lan et al. 1992, Tonken et al. 1995).
Thrombosis has also been induced photochemically with green light and rose Bengal injection
(Kikuchi et al. 1998).
Methods for thrombosis evaluation
To start with, light microscopy with different stainings was used to evaluate the healing
process and histopathology of microanastomoses or to compare the effect of different
irrigation solutions or pharmacological agents (Baxter et al. 1972, Acland and Trachtenberg
1977, Acland et al. 1980). Later, scanning electron microscopy was often employed in the
evaluation of trauma-induced endothelial changes or thrombus formation, in the evaluation of
the normal healing process of microvascular anastomoses or endothelial regeneration of
microvascular prostheses and in studies of vascular intimal thickening (Dujovny et al. 1979,
29
Nightingale et al. 1980, Cooley et al. 1987, Levy et al. 1991, Savoie et al. 1991, Boeckx et al.
1994, Fu et al. 1995, Lanzetta and Owen 1996, Kikuchi et al. 1998, Kashyap et al. 2001).
Electron microscopy has also been applied to evaluate regeneration of the endothelium with
its intracytoplasmic structure, intercellular junctions and smooth muscle cells after clamping
injury and in studies of myofibroblasts in intimal hyperplasia (Jackiewicz et al. 1996, Yang et
al. 1998).
During the last two decades, radiolabelled platelets have been used in studies of thrombus
kinetics in injured vessels (Wieslander et al. 1982, Wieslander et al. 1986, Lassila et al. 1990,
Stockmans et al. 1991, Zhang et al. 1993). The new methods involve direct on line
visualisation of thrombus formation at the anastomosis area and measurements of emboli in
the downstream microcirculation by means of video camera, monitor and recorder (Barker et
al. 1992, Andresen et al. 1994, O´Shaughnessy et al. 1994, Barker et al. 1995, Sørensen et al.
1999).
2.5. Histopathology of microvascular anastomoses
Histopathology in experimental microvascular models
Baxter and his colleagues studied the histopathology of rabbit microanastomoses in biopsies
obtained from the 3rd postoperative day up to the 18th postoperative week (Baxter et al.
1972). If the cut vessel edges were in accurate apposition, only a thin layer of mural thrombus
was found on the luminal surface from the 3rd day on, and the thrombus shrank during the
2nd week followed by invasion of smooth muscle cells, elastin and collagen fibres, and
endothelial cells. If accurate alignment was not achieved, the thrombus spread and, in some
cases, became obstructive. Some of these obstructive thrombi recanalised after a week, but in
others the recanalisation failed to take place. Medial disruption was greatest in the vessels that
had too many sutures, and were unevenly positioned, causing tension. The normal restoration
process comprising subintimal hyperplasia started in the 1st postoperative week, and was
dependent on the amount of viable media; loss of media led to thrombosis without
regeneration in one-third or more cases.
Acland and Trachtenberg studied the histology of longitudinally cut sections of patent rat
30
anastomoses, from 1 h to 3 weeks postoperatively (Acland and Trachtenberg 1977). They
found intimal loss all the way between the clamps, but the internal elastic lamina was intact.
In most of the samples, medial necrosis was widespread, extending for 2 mm on either side of
the anastomosis area; as in the study made by Baxter et al. it was not found to correlate with
suture placement. No regeneration or invasion of the necrotic media was seen up to the 3rd
postoperative week. Depending on the time of sample collection, thrombi caused narrowing
of the lumen at 1 h in most samples; after a week the narrowing was due to fibrous ingrowth
in some samples.
As endothelial damage was widespread on patent anastomoses in early histological studies,
the cause was sought by means of comparative histological work on different irrigation
solutions. The conclusion reached was that normal saline produced more severe endothelial
damage, and cytoplasmic and nuclear changes, than did physiological buffered solutions such
as lactated Ringer´s solution and Normosol (Acland et al. 1980). However, all the vessels
revealed endothelial hyperplasia and platelet deposits, even control vessels that were only
dissected free from the surroundings without the use of irrigation solution.
Lidman and Daniel studied the normal healing process of rabbits´ microanastomoses during a
3-month period (Lidman and Daniel 1981). At first, the damage associated with the
anastomoses included endothelial loss, and necrosis in the media and adventitia under the ties,
but the internal elastic lamina was mostly intact. During the follow-up period the endothelium
and adventitia were restored, but the part of the media that was necrotic failed to regenerate.
The vessel wall maintained its thickness thanks to reactive intimal hyperplasia. A thick layer
of cells with elongated nuclei, resembling smooth muscle cells, developed in the vessel wall
between a single endothelial cell layer and medial smooth muscle cells. Later, in a 12-month
follow-up study showed that the temporary arterial hypertrophic response was greatest at the
3rd month postoperatively, declining thereafter (Lidman et al. 1984).
The development of intimal hyperplasia by myofibroblasts in healing microanastomoses has
been studied in greater detail recently with the aid of electron microscopy. In that study,
spindleshaped immature fibroblasts were seen on the intima at the end of the 1st postoperative
week, and only after a month did they become mature (Yang et al. 1998). In another study on
endothelial injury, smooth muscle cell migration from the media to the neointima occurred a
week after the injury; the formation of neointima reached its maximun 3 weeks after the
31
injury and remained unchanged for up to 42 days (Kikuchi et al. 1998). A recent test on the
inhibitory effect of platelet-derived growth factor antagonist on intimal hyperplasia in a rat
carotid artery injury model found that the beneficial effect was lost after 2 weeks of treatment
(Leppänen et al. 2000).
When microvascular anastomosis was performed in the presence of bacterial infection, the
intima remained unaffected, but the media and adventitia became oedematous and, in
thrombosed arteries, highly fibrotic, causing constriction of the vessel ( Luk et al. 1987).
Histopathology of human microvascular anastomoses
Two large-scale histopathological studies of human microvascular anastomoses were
conducted in the 1980s and 1990s. The first, by Lidman and Daniel, consisted of 45 vessel
biopsies, both arterial and venous, taken during free flap transfers and 32 taken during
replantations. In addition, 10 anastomoses were harvested during free flap transfers, mostly at
the time of reoperation, and 14 during replantations (Lidman and Daniel 1981). The vessel
biopsies showed intact endothelium and internal elastic lamina in most of the free flap
transfers during primary operations, but only in less than half of the cases during secondary
operations. Moreover, inflammation and thrombosis were found in about half of the cases
during the secondary operation. Enhanced intimal proliferation on the recipient vessels was
observed in more than half of the cases during both primary and secondary operations. When
the biopsies were taken from replantations, thrombi and inflammation and also damaged
endothelium and internal elastic lamina, were found in most of the replantation cases during
secondary operations, but in many during primary operations, too. Bleeding into the media
was also evident in some cases, as were old intimal proliferations on the distal vessels in some
of the primary replantations. Evaluation of the failed anastomoses from both the free flap
transfers and the replantations showed thrombi, inflammation, endothelial damage, and
intimal proliferations present in most of the anastomoses, the technical quality was in general
good.
The other study of vessel pathology examined a series of 100 toe transplantations; the
samples were obtained from uncomplicated anastomoses, vasospastic areas or sites of thrombi
(Gu et al. 1992). In over half of the cases, primary histology was normal, and only a few of

32
them had postoperative circulatory crisis. Thickness of the intima was seen in 21 cases, but
none of these had circulatory problems. However, a circulatory crisis occurred in 10 out of 14
cases with acute or chronic inflammation of the vascular wall; most of these had a history of
veinpuncture and some had previous surgical trauma as well. Only five transplantations
failed, and in all but one of these, the primary histopathology revealed inflammation of the
vascular wall.
33
3. AIMS OF THE STUDY
The general aim of our studies was to evaluate the occurrence of acute arterial thrombosis in
association with microsurgery, a field in which anastomotic failures are still a problem. As
new sensitive, coagulation markers have already been tested in other thrombotic
manifestations, the focus of our interest was on assessing their capacity to detect procoagulant
states and local thrombosis developing intra- or postoperatively. By using specific,
immunohistochemical staining we hoped to gain further insight into the local pathogenesis of
the thrombi formed in the failed anastomoses. Also, as HEP-PG have recently shown in vitro
to have promise in blocking thrombus growth, we wanted to test their antithrombotic effect in
vivo in microvascular anastomoses.
The specific aims of these studies were as follows:
1. To investigate the activation of coagulation and fibrinolysis during microsurgery, and
the association of plasma markers with clinical thrombotic manifestations.
2. To evaluate the locally formed thrombi by immunohistochemical methods;
specifically accumulation of platelets and fibrin on the damaged vascular tissue.
3. To conduct experimental studies on the inhibitory effect of HEP-PG on platelet-
collagen interaction in a high shear rate microvascular anastomosis model in rat
common femoral arteries.
34
4. MATERIALS AND METHODS
4.1. PATIENTS AND METHODS; CLINICAL PART - Studies I,
II and III
4.1. Patients and microsurgical procedures (Studies I, II and III)
These studies were carried out during a period of 4 months in 1998 at the Department of
Plastic Surgery (studies I, II and III), and at the Fourth Department of Surgery (study I),
Helsinki University Central Hospital. The coagulation and fibrinolytic assays were performed
in consecutive patients in the three following groups: patients requiring late breast
reconstructions, patients with trauma or chronic ulcer in the lower extremities and patients
with cancer in the oral cavity or the extremities [study I (including four patients with
previously unpublished data), studies II and III]. After permission the blood samples for
coagulation and fibrinolytic parameters were collected from a total of 24 informed patients
with the approval of the local Ethical Committee. A vessel sample was taken from six of these
patients for study I and additionally from seven patients with a non-functioning anastomosis
that was resected during primary surgery or reoperation (study I). All patients had been given
thrombosis prophylaxis according to the protocol below, except one patient in study I from
whom only a vessel sample was taken. The patients were interviewed about their smoking
habits, chronic diseases, medication and previous history of thromboembolism, i.e. deep
venous thrombosis (DVT) or pulmonary embolism (PE). Information was also collected from
medical records. The characteristics of the patients from whom the coagulation and
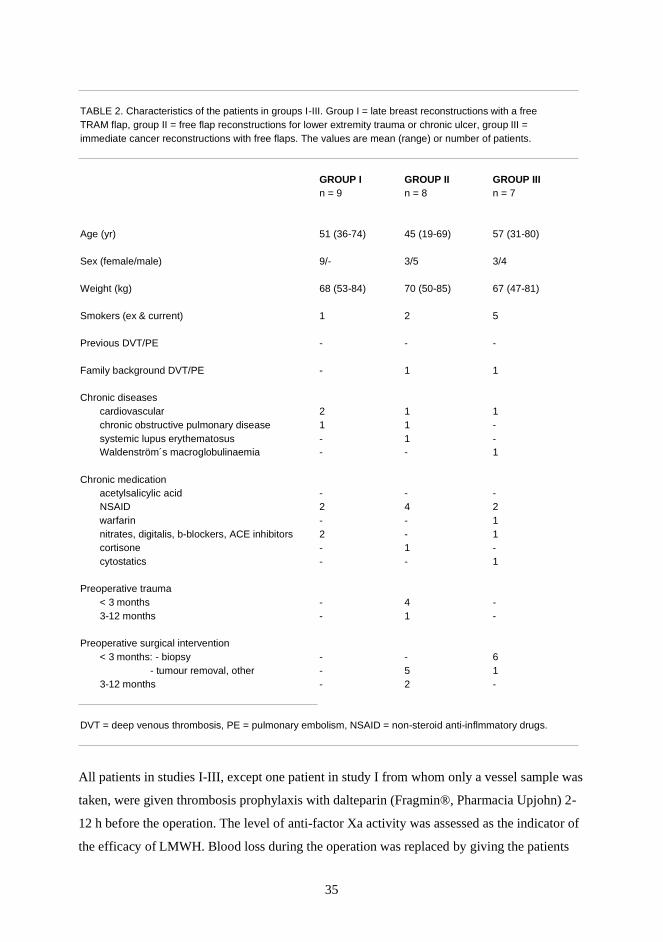
fibrinolytic markers were analysed are listed in Table 2.
35
TABLE 2. Characteristics of the patients in groups I-III. Group I = late breast reconstructions with a free TRAM flap, group II = free flap reconstructions for lower extremity trauma or chronic ulcer, group III = immediate cancer reconstructions with free flaps. The values are mean (range) or number of patients.
GROUP I GROUP II GROUP III n = 9 n = 8 n = 7
Age (yr) 51 (36-74) 45 (19-69) 57 (31-80)
Sex (female/male) 9/- 3/5 3/4
Weight (kg) 68 (53-84) 70 (50-85) 67 (47-81)
Smokers (ex & current) 1 2 5
Previous DVT/PE - - -
Family background DVT/PE - 1 1
Chronic diseases cardiovascular 2 1 1 chronic obstructive pulmonary disease 1 1 - systemic lupus erythematosus - 1 - Waldenström´s macroglobulinaemia - - 1
Chronic medication acetylsalicylic acid - - - NSAID 2 4 2 warfarin - - 1 nitrates, digitalis, b-blockers, ACE inhibitors 2 - 1 cortisone - 1 - cytostatics - - 1
Preoperative trauma < 3 months - 4 - 3-12 months - 1 -
Preoperative surgical intervention < 3 months: - biopsy - - 6 - tumour removal, other - 5 1 3-12 months - 2 -
DVT = deep venous thrombosis, PE = pulmonary embolism, NSAID = non-steroid anti-inflmmatory drugs.
All patients in studies I-III, except one patient in study I from whom only a vessel sample was
taken, were given thrombosis prophylaxis with dalteparin (Fragmin®, Pharmacia Upjohn) 2-
12 h before the operation. The level of anti-factor Xa activity was assessed as the indicator of
the efficacy of LMWH. Blood loss during the operation was replaced by giving the patients
36
crystalloids and 6% hydroxyethylstarch ad 20 ml/kg (HES, Plasmafusin®, Pharmacia
Upjohn) and, when appropriate, blood and albumin 4%. Our protocol does not include
intraoperative use of Dextran. In all patients, the anastomosis region was irrigated with
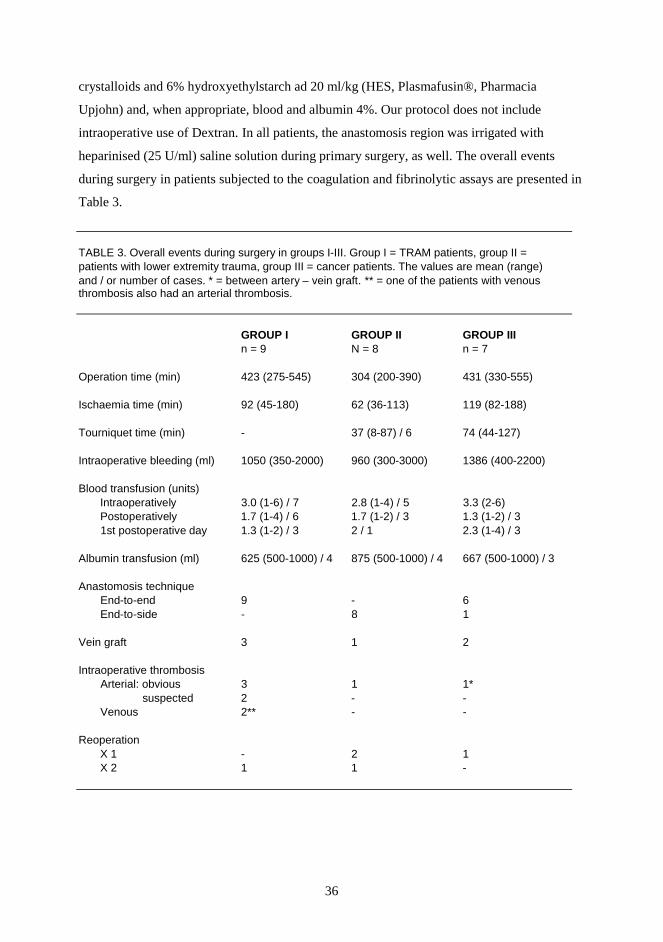
heparinised (25 U/ml) saline solution during primary surgery, as well. The overall events
during surgery in patients subjected to the coagulation and fibrinolytic assays are presented in
Table 3.
TABLE 3. Overall events during surgery in groups I-III. Group I = TRAM patients, group II = patients with lower extremity trauma, group III = cancer patients. The values are mean (range) and / or number of cases. * = between artery – vein graft. ** = one of the patients with venous thrombosis also had an arterial thrombosis.
GROUP I GROUP II GROUP III n = 9 N = 8 n = 7
Operation time (min) 423 (275-545) 304 (200-390) 431 (330-555)
Ischaemia time (min) 92 (45-180) 62 (36-113) 119 (82-188)
Tourniquet time (min) - 37 (8-87) / 6 74 (44-127)
Intraoperative bleeding (ml) 1050 (350-2000) 960 (300-3000) 1386 (400-2200)
Blood transfusion (units) Intraoperatively 3.0 (1-6) / 7 2.8 (1-4) / 5 3.3 (2-6) Postoperatively 1.7 (1-4) / 6 1.7 (1-2) / 3 1.3 (1-2) / 3 1st postoperative day 1.3 (1-2) / 3 2 / 1 2.3 (1-4) / 3
Albumin transfusion (ml) 625 (500-1000) / 4 875 (500-1000) / 4 667 (500-1000) / 3
Anastomosis technique End-to-end 9 - 6 End-to-side - 8 1
Vein graft 3 1 2
Intraoperative thrombosis Arterial: obvious 3 1 1* suspected 2 - - Venous 2** - -
Reoperation X 1 - 2 1 X 2 1 1 -
37
The TRAM group (study I)
The TRAM group consisted of nine patients who underwent delayed breast reconstruction
with a transversus rectus abdominis musculocutaneous (TRAM) flap (five of the patients in
study I, the other patients’ unpublished data). The breast reconstruction was made 3-6 yr after
mastectomy with the exception of one, which was made 21 yr afterwards. Eight of the
patients had received postoperative irradiation, and one had had a liver metastasis removed 2
yr earlier; follow-up was uneventful. The TRAM reconstruction was made, as described
earlier (Asko-Seljavaara 1998, Nieminen et al. 1999), bilaterally in one of the patients and
unilaterally in all the others. Three patients needed vein grafts due to resection of
intraoperatively non-functioning or thrombosed anastomoses, with subsequent loss of the
vessel required for anastomosis. The first two patients (arterial anastomoses) were given
Heparin® 5000 IU iv (Leiras, Helsinki, Finland) after vein grafting; the third patient (venous
anastomosis) received an extra dose of dalteparin 2500 IU sc. One other patient was given
heparin after the artery had been reanastomosed due to intraoperative thrombosis. Two
patients with intraoperative thrombosis were treated only surgically by resecting and redoing
the anastomosis. The patients with intraoperative thrombosis were divided into two subgroups
for the statistical analysis: 1) those with arterial and venous thrombosis, both obvious and
suspected; and 2) those with obvious arterial thrombosis only.
The lower extremity trauma group (study II)
This group consisted of eight patients receiving different types of free flaps in the lower
extremities due to trauma or chronic ulcer (study II). The defects of the lower extremities
were due to recent (within 3 months) complicated fracture of the leg in three patients and
open calcaneal fracture in one patient; an old (10 months) complicated tibial fracture with
osteitis and pseudoarthrosis in one; an ulcer in the foot after metatarsal amputation because of
arteriosclerosis obliterans (ASO) in one; and other previous injuries in two patients. Four
patients were treated with antibiotics before surgery, and preoperative infection parameters
(CRP, leukocytes) were within normal limits or just slightly above normal in all eight
patients. The donor sites for reconstructions were as follows: gracilis in four patients, and
latissimus dorsi (LD) in one, LD with scapular rim in one, radial forearm in one, and tensor
fasciae latae (TFL) in one patient. Three patients received heparin intraoperatively: one
38
because of femorodorsal bypass with an autologous vein to enhance blood circulation to the
flap, another because blood appeared to clot in the operation area, and the third after removal
of an intraoperative arterial thrombus with a fogarty catheter. For the statistical analysis, this
group was divided into two according to previous trauma: 1) patients with recent trauma (< 3
months; four patients), and 2) patients with older trauma (> 3 months) or chronic ulcer (four
patients).
The cancer group (study III)
The cancer group consisted of seven patients undergoing elective reconstructive
microsurgery. Five of them had oral or pharyngeal cancers: one of them had a recurrent
cancer in the tongue (the first tumour had been removed 5 yr earlier), one in the tonsillae, and
one in the floor of the mouth; two had a cancer in the larynx, one of them with metastases in
the neck. The remaining two had sarcoma in the extremity: one a synovial sarcoma in the
elbow, and the other a malignant fibrous histiocytoma (MFH) in the lower leg. One patient
with larynx cancer had received preoperative irradiation within the previous 12 months and
had undergone two operations for lung cancer, 4 and 1 yr earlier. The other patient with
larynx cancer had been operated on for stomach cancer 8 yr earlier. Microsurgical
reconstruction in all the head and neck cancer patients was performed with a radial forearm
flap. The patient with a synovial sarcoma in the elbow was treated, at his own request to
retain his hand, by amputation of the humerus and replantation of the remnant forearm to the
stump of the arm. The patient with MFH in the lower leg received a latissimus dorsi flap to
cover the defect. Vein grafts were used in two patients to reconstruct the radial artery; in one
of these patients a thrombus formed intraoperatively at the proximal arteriovenous
anastomosis and required resection and reanastomosing.
The vessel sample group (study I)
The failed vessel samples for immunohistochemical study were gathered from 12 patients
undergoing elective free flap surgery: nine for late breast reconstruction with a TRAM flap,
two for immediate reconstruction due to oropharyngeal cancer with a radial forearm flap, and
one for reconstruction due to a 2-week-old instabile lower leg fracture with a LD flap
combined with scapular bone. One sample was also obtained from a digital artery of a patient
39
whose thumb and three other fingers were primarily replanted by the hand surgeons, but who
developed thrombosis on the 1st postoperative day and was reoperated on by the plastic
surgery team.
All of the patients except one were female, with a mean age of 51 (range 34 - 75) yr. Three
patients received medication for hypertension. One patient, who had been operated on for
breast cancer with axillar metastases 3 yr earlier, was treated with tamoxifen. The patient with
cancer of the larynx had been surgically treated for stomach cancer 8 yr earlier. Four of the
patients were current smokers. During the primary operations, vein grafts were used in four
patients: in two of the TRAM patients and in both cancer patients.
4.1.2. Blood sampling and analysis (Studies I, II and III)
Four blood samples for plasma markers were routinely taken from each patient at the
beginning of the operation before the induction of anaesthesia (B), at 2 h (± 30 min) after the
start of the operation (2h), at the end (± 1h) (E), and at 24 h (± 6h) after completion of the
operation (24h). Additional samples were taken, if needed, in the event of intraoperative
thrombosis (T) or postoperative thrombosis requiring reoperation (R). Free flowing blood was
collected via a clean venipuncture or through an arterial cannula (Viggo® AB, Helsingborg,
Sweden). The first 3 ml or 6 ml, respectively, were discarded. The blood was collected in
plastic tubes containing 3.8% sodium citrate (9:1); approtinin (0.2 TIU/ml) was added for D-
dimer, and prostaglandin E1 (0.9 µM) and theophylline (10 mM) for PAI-1 (Kluft and
Verheijen 1990). Within 1 h of the collection, samples were centrifuged at 1800 G (+22° C)
for 10 min, except for the PAI-1 samples, which were centrifuged for 30 min (+4° C). The
plasma was then separated, divided into aliquots, and stored at -70° C until analysed. Routine
blood cell counts and C-reactive protein (CRP) determinations to detect
infection/inflammation were conducted before and after surgery (CRP, immunochemical
method; Orion Diagnostica, Espoo, Finland).
The plasma markers were analysed within 6 months. Fibrinogen (reference value < 4 g/l) was
determined by the functional method of Clauss. Enzyme-linked immunosorbent assays were
used to determine TAT (< 4.1 µg/l), F1+2 (< 1.1 nmol/l), D-dimer (< 400 ng/ml), tPA (< 20
ng/ml), and PAI-1 (< 43 ng/ml) (Enzygnost TAT micro and Enzygnost F1+2 micro,
40
Behringwerke AG, Marburg, Germany; Asserachrom D-di, Diagnostica Stago, Asnieres-sur-
Seine, France; TintElize tPA and TintElize PAI-1, Biopool, Umeå, Sweden, respectively).
F1+2 and PAI activities (< 40 U/ml) [Spectrolyse (pL) PAI, Biopool] were measured only in
patients with intra- or postoperative thrombosis. The functional concentration of dalteparin
was determined by photometric anti-factor Xa assay (Coatest LMW Heparin/Heparin; Kabi
Diagnostica, Mölndal, Sweden).
4.1.3. Vessel samples and their histopathological and
immunohistochemical analysis (Study I)
Vessel samples and associated clinical manifestations
A total of 17 vessel samples were obtained from 13 patients. The majority (14/17) of the
samples were taken during primary surgery, and in half of them the clinical manifestation at
operation was obvious thrombosis. In the other cases the anastomoses were defined as non-
functioning, or as having poor flow or too sharp a pulse during primary surgery. Three of the
vessel samples were resected at reoperations when an obvious occlusion was present. The
samples consisted mainly of the arterial anastomosis region, and in some cases the adjacent
piece of vessel was also resected. Since, however, two samples were obtained from
thrombosed arterialised vein grafts, one sample of a venous thrombus was included for
comparison.
Sample preparation
After resection, the anastomosis or adjacent piece of vessel was fixed in formalin. Later, the
stitches were removed from the formalin-fixed anastomoses under light microscope. If the
samples were long, they were transversely cut into 2-8 mm slices and then embedded in
paraffin. During the stitch removing procedure the overall morphology and histopathology of
the vessels and adjacent thrombi were primarily evaluated.
41
Immunohistochemistry
Immunohistochemical markers
The immunohistochemical markers used were: CD31 (PECAM-1, platelet-endothelial cell
adhesion molecule; DAKO A/S, Glostrup, Denmark), CD42b (glycoprotein=GP 1b α;
Novocastra Laboratories Ltd., Newcastle upon Tyne, UK) and fibrin (fibrin II, T2G1;
Accurate Chemical & Scientific Corp., Westbury, NY, USA) (Bini et al. 1989).
Staining procedure
In the prepared transverse sections immunohistochemical staining was carried out by standard
methods (Hsu et al. 1981). The paraffin-embedded sections were deparaffinised and then the
slides used for the CD42b and fibrin stainings were pretreated with citric acid solution in a
microwave oven to enhance the staining intensity (von Boguslawski 1994). To enhance the
staining intensity with the CD31 antibodies, the deparaffinised sections were treated with
0.4% pepsin solution in 1 M HCl (Sigma No P-7000) for 1 h at 37 ºC before the H2O
2
blocking. After rinsing in PBS, the deparaffinised sections were incubated with blocking
serum (10% horse serum in PBS) for 15 min. Thereafter, the sections were incubated
overnight with primary monoclonal antibodies at optimal dilution (CD31 1:100, CD42b 1:500
and Fibrin 1 1:500) in humid atmosphere at room temperature. After the sections had been
rinsed in PBS, the avidin-biotin complex (ABC) detection method was used (Vectastain Elite
ABC- Kit, Vector Laboratories Inc., Burlingame, CA). Finally, the sections were developed in
3-amino-9-ethylcarbazole (Sigma No A-5754) solution (0.2 mg/ml in 0.05 M acetate buffer
containing 0.03% H2O
2) and counterstained with Mayer´s haematoxylin.
Evaluation of immunoreactivities
Immunoreactivities were visually assessed by two experienced observers, who evaluated the
vessel structures and amount of stained cells in the studied areas. The immunoreaction was
scored: negative (-), or slightly (+), moderately (++) or strongly (+++) positive.

42
4.1.4. Statistics (Studies I, II and III)
The statistical analysis in the studies on activation of blood coagulation and fibrinolysis
during microsurgical reconstructions was made by using SigmaStat®, version 2.0 for
Windows® 95, Jandel statistical software. The Spearman Rank Order Correlation test was
used when both variables were continuous. In comparisons of two groups, the Fisher Exact
Test, paired t-test or Mann-Whitney Rank Sum Test was used, as appropriate. The Friedman
Repeated Measures Analysis of Variance on Ranks was applied to compare coagulation and
fibrinolysis parameters at different time intervals within groups. The values are expressed as
mean ± standard error of mean (SE) or as mean (range), unless otherwise indicated.
43
4.2. ANIMALS AND METHODS; EXPERIMENTAL PART -
Study IV
4.2.1. Animals and thrombosis models in experiments I-III
Experiments I-III
We studied the capacity of heparin proteoglycans (HEP-PG) to inhibit both early and late
thrombus formation in rat common femoral arteries, and we measured it semiquantitatively
with scanning electron microscopy (SEM) and quatitatively with Indium 111-labelled
platelets. We thus set up three different experiments in a total number of 87 rats as follows:
Experiment I: Study of early (10 min) thrombus formation in three thrombosis models
analysed by SEM. A total of 45 samples, 15 in each thrombosis model, five in each irrigation
solution group, were analysed. This procedure was a pilot study to find the thrombosis model
best reproduceable and most suitable for quantification.
Experiment II: Assessment of early (10 min) thrombus formation on an anastomosis with
Indium 111-labelled platelets. The platelet specific radioactivity was measured and translated
into the number of attached platelets per vessel in 21 samples in the different irrigation
solution groups.
Experiment III: A 3-day follow-up study in the anastomosis model. The study comprised 21
samples, of which 12, four in each of the irrigation solution groups, were analysed by SEM.
Animals and operation technique
Our animal models were male Brown Norwegian (BN/R1) rats (210-490 g) in all three
experiments and, in addition, male rats of an inbred strain of WAG/RijHsd (270-390g) in
experiment II. The animals were fed a regular rat chow diet, with water provided ad libitum.
In experiment III the rats were individually caged during the follow-up period. Animal care,
anaesthesia and the experimental protocol complied with the guidelines of the Helsinki
University Central Hospital animal care committee. The rats were anaesthetised i.p. 0.10-0.15
ml/kg with a mixed solution of fentanyl-fluanisone (Hypnorm
, Jansen-Cielag,

44
Buckinghamshire, UK), midazolam (Dormicum
, Roche, Basel, Switzerland) and sterile aqua
(10 ml, 3 ml and 10 ml, respectively) according to approximated weight. After anaesthesia,
the rats were weighed before the operation. During the operation additional doses of
anaesthetic were given if required. The operations were performed with a clean, but not
sterile, technique under an operating microscope (Wild M 651, Heerbrugg, Switzerland).
Before the operation, the rats´ groins were shaved and thereafter a linear incision was made
overlying the femoral vessels. The common femoral artery (diameter 0.7-1.0 mm) was
dissected free and smaller branches were electrocauterised. A plastic sheet was placed under
the artery to isolate it from surrounding structures. A standardised number of stitches was
used in the different thrombosis models, the suture material being 10-0 nylon (non sterile
microsutures for experimental surgery, B. Braun-SSC AG, Neuhausen, Switzerland). In
experiment II, the contralateral femoral artery was dissected as on the other side but not
opened. After completion of the dissection, the distal part was ligated with 9-0 Nylon
(B.Braun-SSC AG, Emmenbruck, Switzerland), the vessel was then cut, and a 24-G
intravascular neonatal Neoflon cannula (BOC Ohmeda AB, Helsingborg, Sweden) was
inserted proximally for blood sampling and injection of Indium 111-labelled platelets. In all
experiments, the vascular clamps were released and bleeding time was recorded. Bleeding
time was measured as the time elapsing between release of the microvascular double clamp
(restoration of blood flow) and cessation of bleeding from the sutured
arteriotomy/anastomosis. Patency was tested at 10 min in all experiments, and in experiment
III repeatedly up to 3 days postoperatively. In experiment III, the skin incision was sutured
after a patency test performed at 60 min. At 24 h the animals were again anaesthetised, the
wound was opened and a patency test was performed and the wound closed. After the final
patency test (10 min in experiments I and II, and 3 days postoperatively in experiment III)
vascular clamps were again inserted on each side of the injured area and a piece (3-5 mm) of
the vessel was dissected, either for SEM or measurement of radioactivity, and flushed gently
with normal saline to release the remaining blood from the lumen. At the end of the
procedure, while the animals were still anaesthetised, a blood sample was taken by cardiac
puncture for measurement of thrombin time (experiment I). A lethal dose of barbiturate (1 ml,
Mebunat
, Orion, Espoo, Finland) was then given by cardiac puncture (experiments I and III)
or via intra-arterial cannula (experiment II). All surgical procedures were performed by the
same microsurgeon.
45
Thrombosis models
We started the pilot studies in the first experiment by using the model of Davidson et al.
(thrombosis model 1, TM 1; Davidson et al. 1990), which we modified by not applying stasis.
The thrombogenic injury was made as follows: the loose adventitia on the left common
femoral artery was removed from the area of intended injury and a bulldog clamp was placed
on the vessel for 2 min to create a crush injury. Next, a microvascular double clamp was
placed on the vessel, and a transverse arteriotomy involving approximately one-half of the
circumference was made between the two clamps. The intima proximal to the arteriotomy on
the anterior side (=arteriotomy side) of the vessel was then scratched with a 5-mm tapered
microsurgical needle (B. Braun-SSC AG, Emmenbruck, Switzerland) through the arteriotomy
site to create a subendothelial injury (approximately 20 scratches). The arteriotomy was
closed with 3-5 stitches.
The second model (thrombosis model 2, TM 2) in the pilot studies was that described by
Barker et al. consisting of arteriotomy and inversion of the full thickness of the vessel wall
into the lumen (Barker et al. 1992). We modified this model by enlargening the flap from one-
third to one-half and by reversing the inverted flap site. The thrombogenic injury was made as
follows: a microvascular double clamp was placed on the vessel and a transverse arteriotomy
involving approximately one half of the circumference was made on the anterior side. Three
to five stitches were placed in a manner that inverted a full thickness of the distal vessel wall
into the lumen and thus enabled all layers of the cut vessel end to confront circulating blood.
The third model used in the first experiment was an ordinary end-to-end anastomosis (study
IV). This model was chosen as the basic, physiological model for the second and third
experiments. The thrombogenic injury was made as follows: a microvascular double clamp
was placed on the artery, which was then transversely cut with microscissors. No adventitial
circumcision was made at the vessel ends and only some of the excess loose hanging
periadventitial tissue was removed. A regular anastomosis was performed with 8-10 stitches.
46
Irrigation solutions and thrombin time
Three different irrigation solutions in a volume of 0.2 ml were used in all experiments in a n
open manner. The solutions included normal saline (saline group, controls), heparinised
normal saline (unfractionated heparin, Heparin
Lövens, Ballerup, Denmark, MW 15 kD, 1
mg/ml) (HEP group) (Cox et al. 1992) and heparin-proteoglycans (HEP-PG, MW 750 kD, 10
ug/ml) (HEP-PG group). The remaining blood was flushed away from the vessel lumen with
normal saline. Any exess saline remaining around and inside the vessel was dried before
either HEP-PG, UFH or saline was applied into the lumen at the site of arteriotomy; half of
the solution was given at the beginning of suturing and the other half before the last two
stiches were tied. HEP-PG was obtained as a soluble fraction of stimulated (compound 48/80)
rat serosal mast cells, as previously described (Lassila et al. 1997). To evaluate the systemic
effect of the irrigation solutions, thrombin time was measured in the anastomosis model at 10
min in experiment I. 100 µl of citrated plasma was incubated with 0.7 U of Test Thrombin
Reagent (Behring Diagnostics GmbH, Marburg, Germany) according to the manufacturer´s
instructions.
4.2.2. Methods for thrombosis evaluation
Patency testing (experiments I, II and III)
To evaluate the occurrence of occlusive thrombi, patency was tested at 10 min in all
experiments (I-III), and in experiment III repeatedly at 30 min, 60 min, 24 h and 3 days
postoperatively. The patency test (distal milking test) was performed using two pairs of
microforceps, the first clamping and occluding the vessel just distal to the sutured
arteriotomy/anastomosis and the other emptying the blood more distally over a short distance.
The first pair of forceps was then opened and patency assessed (Wieslander et al. 1990). The
criterion of patency (P) was rapid or good refilling and that of absent patency (T, thrombosis)
no refilling. An additional definition, between P and T, was markedly reduced flow (Rf).
Vessels with markedly reduced flow or no refilling, but which were still distally dilated with
pulsewave (thought to represent distal perfusion via collaterals), were separately defined by *
(Rf*, and T*, respectively).
47
Scanning electron micrographs (SEM) (experiments I and III)
For the semiquantitative analysis by SEM, the dissected piece of vessel was carefully opened
longitudinally with microscissors, placed on a plastic sheet and sutured with 2-4 stitches to
keep the tissue piece flat for fixation. The vessel-on-plastic was put into a polypropylene tube
containing 2.5% glutaraldehyde for 2 h for fixation at 22 °C. After fixation the sample was
rinsed with and placed in PBS to be processed routinely for SEM (Lassila et al. 1997). The
2.5% glutaraldehyde-fixed samples were dehydrated, critical-point dried with CO2, sputter-
coated with platinum, and viewed by SEM (Jeol JSEM-820 scanning electron microscope,
Tokyo, Japan) at the Institute of Biotechnology, Electron Microscopy, University of Helsinki.
The electronmicroscopist did not know what irrigation solution had been used. In experiment
I, two scanning electron micrographs were obtained of each sample at standard
magnifications of x 45 and x 300 and preanalysed for severity of thrombotic response. The
pictures were later grouped and re-examined by two independent observers, and the
intraluminal thrombotic material was quantified as -/+ (clean or minimal amounts), + (small
amounts), ++ (moderate amounts) or +++ (large amounts). In experiment III, one picture was
taken of each sample at a magnification of x 60 to optimally cover the whole anastomotic
area.
Measurement of Indium 111-labelled platelets (experiment II)
Platelet preparation and labelling
In experiment II, the thrombotic response was quantified by using Indium 111-labelled
platelets. The labelled platelets were prepared by collecting samples from anaesthetised rats
of the same strain as those on which the experiment was performed (either BN/R1 or
WAG/RijHsd). The blood was collected into polypropylene tubes containing 1/10 volume of
acidic citrated dextrose (ACD) anticoagulant and repeatedly centrifuged (1900 rpm, at 22 °C)
for 15-30 s four times. Between each spin the platelet-rich plasma (PRP) layer was collected
and anticoagulant was added as described by Catalfamo and Dodds (Catalfamo adn Dodds
1989). 10 vol of the pooled PRP was added in 1 vol of ACD; the platelets were washed twice
and resuspended in MTS buffer (NaCl 8 mg, KCl 0.2mg, MgCl2
x 6 H2O 0.43 mg, glucose
1.1 mg, acidic citrate x H2O 1.34 mg, Na OH 0.36 mg, per 1 ml H
2O) at normal pH. Indium
48
111-label (100 µCi) was added to the platelet suspension and incubated for 5 min. To capture
unbound Indium 111-label, platelet-poor plasma (PPP) was added, and the suspension was
centrifuged at 2000 rpm for 5 min. Finally, the platelet pellet was resuspended in 0.9% NaCl
to obtain a platelet number between 400 and 600 x 106/ml for injection.
Blood sampling and injection of Indium 111-labelled platelets
Blood samples for platelet count and thrombin time were collected via the inserted cannula on
the arteria femoralis into plastic syringes containing EDTA and 110 mM sodium citrate,
respectively. The vessel surface on the opposite femoral artery was treated with the irrigation
solution, and the anastomosis was completed. Thereafter the double clamp was released, and
after 15 s Indium 111-labelled platelets (200-300 x 106 in 0.5 ml) were infused slowly (within
40-55 s) via the cannula. After 10 min patency was tested, the anastomosis was resected, and
two blood samples (0.5 ml and 1.0 ml) were taken for platelet count and for measurement of
radioactivity in the blood.
Vessel samples and measurement of radioactivity
The anastomosed tissue sample was kept unopened and put into a polypropylene tube
containing 2.5% glutaraldehyde. The retained radioactivity was measured (LKP, Wallac 1272
clinigamma, Turku, Finland) together with the blood samples to assess platelet-related Indium
111 activity. The number of platelets deposited on the vessel was calculated from the activity
of the blood and its platelet number.
4.2.3. Statistics
The variability of the results between the three different groups was statistically tested with
ANOVA using Fisher’s exact t-test.
49
5. RESULTS
5.1. Activation of coagulation and fibrinolysis in free flap surgery
- association with flap failure (Studies I, II and III)
Outcome of the patients and intra- and postoperative thrombotic events
The TRAM group (n=9) consisted of six patients with obvious or suspected intraoperative
thrombosis, and of three patients without thrombosis, see Table 3. Five of the patients with
thrombotic events are discussed in study I; the data on the other patients in the TRAM group
are unpublished. One of the patients with intraoperative thrombosis requiring resection of the
vessel and replacement by vein graft, the oldest patient in the TRAM group (age 74),
underwent two reoperations, on the 3rd and 7th postoperative days, because the graft
occluded. The final outcome was good. The outcome was also uneventful for all the other
patients except one in whom a thrombus formed during primary surgery and small edge
necrosis developed some months later.
In the lower extremity trauma group (n=8), comprising patients with both recent and old
trauma in the lower extremities, only one of the patients with old trauma had an event of
intraoperative thrombosis (Table 3). Hovever, three patients had an event of postoperative
thrombosis requiring reoperation on the same day as primary surgery; the outcome was good
in two of them, both with recent trauma. The third patient, the one with ASO and LED, had a
flap failure on the 8th postoperative day, and her lower leg had to be amputated. All the other
patients in this group had a good outcome. The patient data are published in study II.
In the cancer group, two thrombotic events (one intraoperative and one postoperative)
occurred (Table 3), but no flaps were lost. In the patient with metastatic larynx cancer, in
whom an autogenous vein graft was used to reconstruct the radial artery, an intraoperative
thrombus formed at the proximal arteriovenous anastomosis in the forearm, making resection
and reanastomosis necessary. The other patient, who was operated on for an epidermoid
cancer in the floor of the mouth, had to undergo reoperation on the 8th postoperative day
because of necrosis in the tongue due to thrombosis in the arteria lingualis, and the tongue had
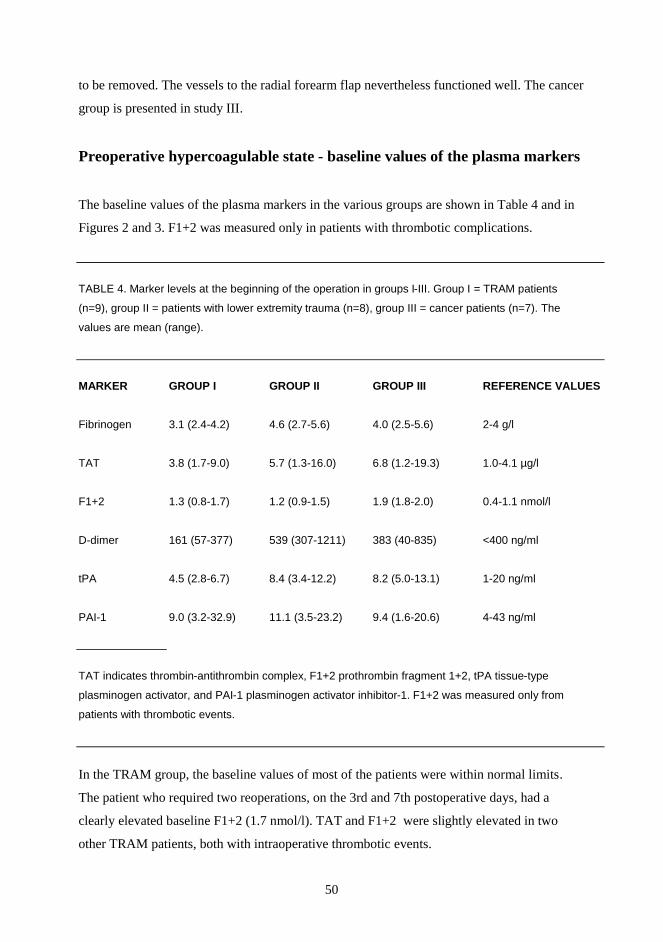
50
to be removed. The vessels to the radial forearm flap nevertheless functioned well. The cancer
group is presented in study III.
Preoperative hypercoagulable state - baseline values of the plasma markers
The baseline values of the plasma markers in the various groups are shown in Table 4 and in
Figures 2 and 3. F1+2 was measured only in patients with thrombotic complications.
TABLE 4. Marker levels at the beginning of the operation in groups I-III. Group I = TRAM patients
(n=9), group II = patients with lower extremity trauma (n=8), group III = cancer patients (n=7). The
values are mean (range).
MARKER GROUP I GROUP II GROUP III REFERENCE VALUES
Fibrinogen 3.1 (2.4-4.2) 4.6 (2.7-5.6) 4.0 (2.5-5.6) 2-4 g/l
TAT 3.8 (1.7-9.0) 5.7 (1.3-16.0) 6.8 (1.2-19.3) 1.0-4.1 µg/l
F1+2 1.3 (0.8-1.7) 1.2 (0.9-1.5) 1.9 (1.8-2.0) 0.4-1.1 nmol/l
D-dimer 161 (57-377) 539 (307-1211) 383 (40-835) <400 ng/ml
tPA 4.5 (2.8-6.7) 8.4 (3.4-12.2) 8.2 (5.0-13.1) 1-20 ng/ml
PAI-1 9.0 (3.2-32.9) 11.1 (3.5-23.2) 9.4 (1.6-20.6) 4-43 ng/ml
TAT indicates thrombin-antithrombin complex, F1+2 prothrombin fragment 1+2, tPA tissue-type
plasminogen activator, and PAI-1 plasminogen activator inhibitor-1. F1+2 was measured only from
patients with thrombotic events.
In the TRAM group, the baseline values of most of the patients were within normal limits.
The patient who required two reoperations, on the 3rd and 7th postoperative days, had a
clearly elevated baseline F1+2 (1.7 nmol/l). TAT and F1+2 were slightly elevated in two
other TRAM patients, both with intraoperative thrombotic events.
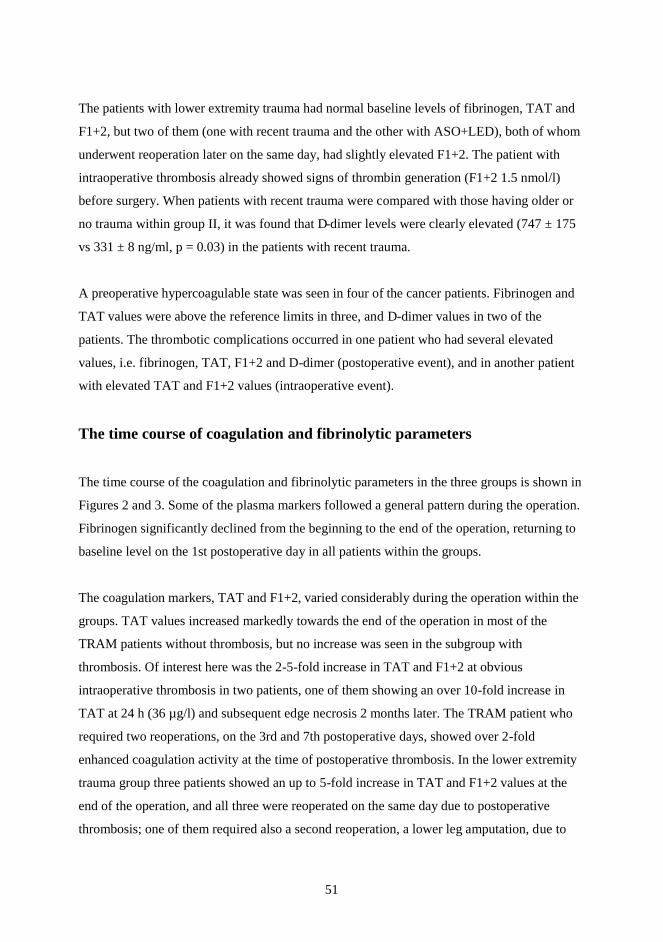
51
The patients with lower extremity trauma had normal baseline levels of fibrinogen, TAT and
F1+2, but two of them (one with recent trauma and the other with ASO+LED), both of whom
underwent reoperation later on the same day, had slightly elevated F1+2. The patient with
intraoperative thrombosis already showed signs of thrombin generation (F1+2 1.5 nmol/l)
before surgery. When patients with recent trauma were compared with those having older or
no trauma within group II, it was found that D-dimer levels were clearly elevated (747 ± 175
vs 331 ± 8 ng/ml, p = 0.03) in the patients with recent trauma.
A preoperative hypercoagulable state was seen in four of the cancer patients. Fibrinogen and
TAT values were above the reference limits in three, and D-dimer values in two of the
patients. The thrombotic complications occurred in one patient who had several elevated
values, i.e. fibrinogen, TAT, F1+2 and D-dimer (postoperative event), and in another patient
with elevated TAT and F1+2 values (intraoperative event).
The time course of coagulation and fibrinolytic parameters
The time course of the coagulation and fibrinolytic parameters in the three groups is shown in
Figures 2 and 3. Some of the plasma markers followed a general pattern during the operation.
Fibrinogen significantly declined from the beginning to the end of the operation, returning to
baseline level on the 1st postoperative day in all patients within the groups.
The coagulation markers, TAT and F1+2, varied considerably during the operation within the
groups. TAT values increased markedly towards the end of the operation in most of the
TRAM patients without thrombosis, but no increase was seen in the subgroup with
thrombosis. Of interest here was the 2-5-fold increase in TAT and F1+2 at obvious
intraoperative thrombosis in two patients, one of them showing an over 10-fold increase in
TAT at 24 h (36 µg/l) and subsequent edge necrosis 2 months later. The TRAM patient who
required two reoperations, on the 3rd and 7th postoperative days, showed over 2-fold
enhanced coagulation activity at the time of postoperative thrombosis. In the lower extremity
trauma group three patients showed an up to 5-fold increase in TAT and F1+2 values at the
end of the operation, and all three were reoperated on the same day due to postoperative
thrombosis; one of them required also a second reoperation, a lower leg amputation, due to

52
necrotic flap on the 8th postoperative day (the data on the first reoperation of the patient with
two reoperations are not shown in Figures 2 and 3). In the lower extremity trauma patient
with intraoperative thrombosis, thrombin generation persisted at 24 h (F1+2 2.6 nmol/l). In
the cancer group, TAT values consistently increased by as much as 6-fold at the end of the
operation, returning to normal at 24 h in all patients, except the one with postoperative
thrombosis.
53
Figure 2. Time course of fibrinogen (FG), thrombin-antithrombin III complex (TAT) and
prothrombin fragment 1+2 (F1+2) during free flap transfers in groups I-III. Group I = patients
undergoing late breast reconstruction with a transversus rectus abdominis musculocutaneous
(TRAM) flap (black triangles indicate patients with thrombotic complications, and open
triangles patients with uncomplicated operations), Group II = patients with lower extremity
trauma or chronic ulcer in lower extremitites ( black circles indicate patients with recent
trauma, and open circles patients with older trauma or chronic ulcer), Group III = patients
with oropharyngeal cancer or cancer in the extremitites (black rhomboids indicate the patient
with postoperative thrombosis, and open rhomboids the patient with intraoperative
thrombosis). B = at the beginning of the operation, 2h = at 2 h from the beginning, T1 = at
first intraoperative thrombosis, T2 = at second intraoperative thrombosis, E = at the end of the
operation, 24h = at 24 h after completion of the operation, R1 = at first reoperation, R2 = at
second reoperation.
D-dimer showed a general decrease during the operation in the TRAM patients with
intraoperative thrombosis and in all patients in the lower extremity trauma group except two
with recent trauma, whose levels remained elevated during primary surgery and at
postoperative thrombosis and who required reoperation on the same day. Activation of
fibrinolysis with increased D-dimer values at 24 h occurred in all the TRAM patients without
54
thrombosis, but in only one patient with intraoperative thrombosis. Also, the TRAM patient
who was reoperated on twice showed activation of fibrinolysis at the time of reoperations.
Only one patient with lower extremity trauma showed a clear increase in the values at 24 h
and at the time of the second reoperation. Interestingly, in the cancer group, following
activation of coagulation, fibrinolysis was clearly stimulated at 24 h, as shown by the 2-3-
fold, maximally even 10-fold, increase in D-dimer values.
The fibrinolytic markers tPA and PAI-1 ag were within normal limits at all times in most of
the patients. In two TRAM patients, PAI-1 antigen values increased 2-6-fold at the time of the
second intraoperative obvious thrombosis; one of them also had a 2-fold increase in PAI-1
activity (data not shown). One patient with lower extremity trauma showed a clear increase in
tPA values at the time of the second reoperation due to a necrotic flap. Two other trauma
patients with postoperative thrombosis had a 2-2.5-fold increase in PAI-1 antigen levels at the
time of reoperation, one of them having a 5-fold increase in PAI-1 activity as well. Of special
interest in the cancer group was the increase in tPA and PAI-1 in the two patients who
developed thrombosis, whereas in the patients without thrombotic complications the
fibrinolytic enzymes remained quite stable.
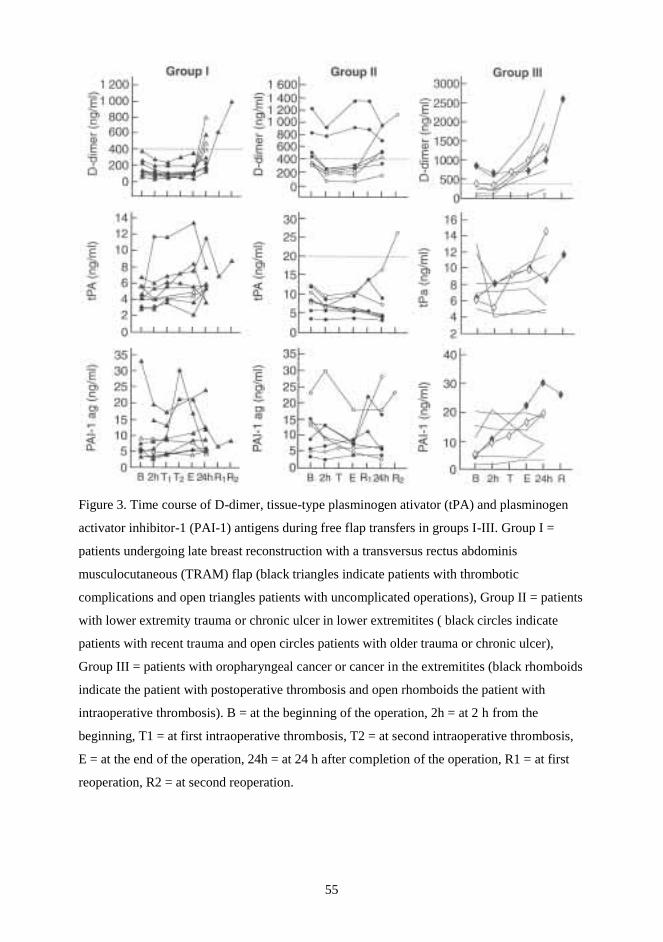
55
Figure 3. Time course of D-dimer, tissue-type plasminogen ativator (tPA) and plasminogen
activator inhibitor-1 (PAI-1) antigens during free flap transfers in groups I-III. Group I =
patients undergoing late breast reconstruction with a transversus rectus abdominis
musculocutaneous (TRAM) flap (black triangles indicate patients with thrombotic
complications and open triangles patients with uncomplicated operations), Group II = patients
with lower extremity trauma or chronic ulcer in lower extremitites ( black circles indicate
patients with recent trauma and open circles patients with older trauma or chronic ulcer),
Group III = patients with oropharyngeal cancer or cancer in the extremitites (black rhomboids
indicate the patient with postoperative thrombosis and open rhomboids the patient with
intraoperative thrombosis). B = at the beginning of the operation, 2h = at 2 h from the
beginning, T1 = at first intraoperative thrombosis, T2 = at second intraoperative thrombosis,
E = at the end of the operation, 24h = at 24 h after completion of the operation, R1 = at first
reoperation, R2 = at second reoperation.
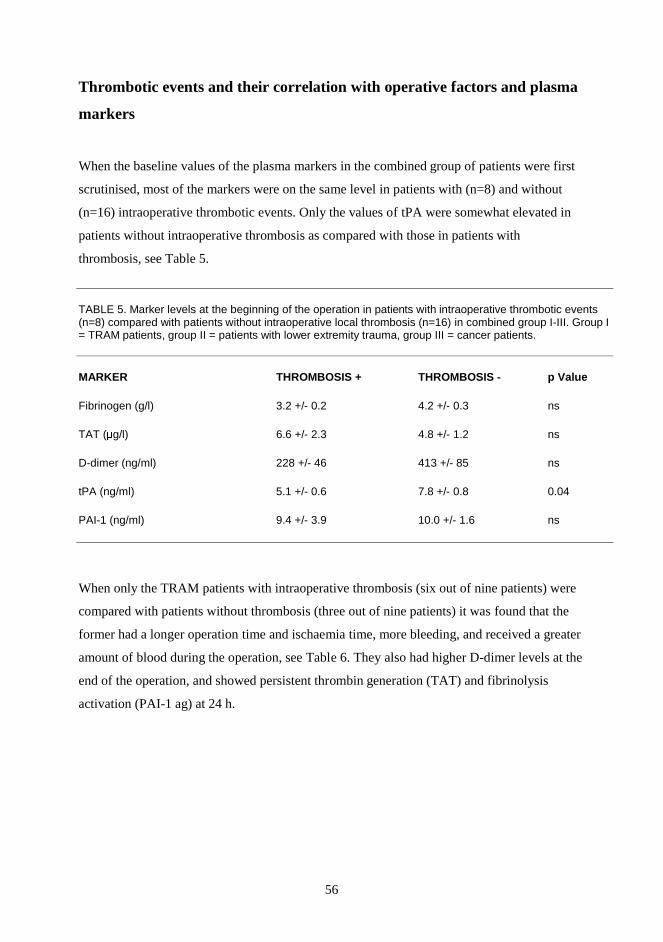
56
Thrombotic events and their correlation with operative factors and plasma
markers
When the baseline values of the plasma markers in the combined group of patients were first
scrutinised, most of the markers were on the same level in patients with (n=8) and without
(n=16) intraoperative thrombotic events. Only the values of tPA were somewhat elevated in
patients without intraoperative thrombosis as compared with those in patients with
thrombosis, see Table 5.
TABLE 5. Marker levels at the beginning of the operation in patients with intraoperative thrombotic events (n=8) compared with patients without intraoperative local thrombosis (n=16) in combined group I-III. Group I = TRAM patients, group II = patients with lower extremity trauma, group III = cancer patients.
MARKER THROMBOSIS + THROMBOSIS - p Value
Fibrinogen (g/l) 3.2 +/- 0.2 4.2 +/- 0.3 ns
TAT (µg/l) 6.6 +/- 2.3 4.8 +/- 1.2 ns
D-dimer (ng/ml) 228 +/- 46 413 +/- 85 ns
tPA (ng/ml) 5.1 +/- 0.6 7.8 +/- 0.8 0.04
PAI-1 (ng/ml) 9.4 +/- 3.9 10.0 +/- 1.6 ns
When only the TRAM patients with intraoperative thrombosis (six out of nine patients) were
compared with patients without thrombosis (three out of nine patients) it was found that the
former had a longer operation time and ischaemia time, more bleeding, and received a greater
amount of blood during the operation, see Table 6. They also had higher D-dimer levels at the
end of the operation, and showed persistent thrombin generation (TAT) and fibrinolysis
activation (PAI-1 ag) at 24 h.
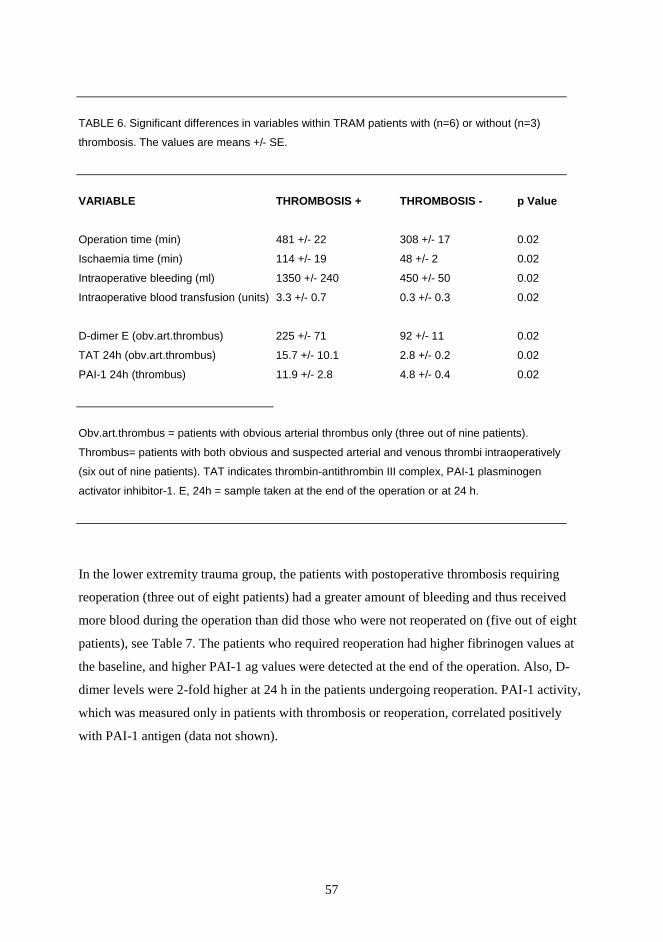
57
TABLE 6. Significant differences in variables within TRAM patients with (n=6) or without (n=3)
thrombosis. The values are means +/- SE.
VARIABLE THROMBOSIS + THROMBOSIS - p Value
Operation time (min) 481 +/- 22 308 +/- 17 0.02
Ischaemia time (min) 114 +/- 19 48 +/- 2 0.02
Intraoperative bleeding (ml) 1350 +/- 240 450 +/- 50 0.02
Intraoperative blood transfusion (units) 3.3 +/- 0.7 0.3 +/- 0.3 0.02
D-dimer E (obv.art.thrombus) 225 +/- 71 92 +/- 11 0.02
TAT 24h (obv.art.thrombus) 15.7 +/- 10.1 2.8 +/- 0.2 0.02
PAI-1 24h (thrombus) 11.9 +/- 2.8 4.8 +/- 0.4 0.02
Obv.art.thrombus = patients with obvious arterial thrombus only (three out of nine patients).
Thrombus= patients with both obvious and suspected arterial and venous thrombi intraoperatively
(six out of nine patients). TAT indicates thrombin-antithrombin III complex, PAI-1 plasminogen
activator inhibitor-1. E, 24h = sample taken at the end of the operation or at 24 h.
In the lower extremity trauma group, the patients with postoperative thrombosis requiring
reoperation (three out of eight patients) had a greater amount of bleeding and thus received
more blood during the operation than did those who were not reoperated on (five out of eight
patients), see Table 7. The patients who required reoperation had higher fibrinogen values at
the baseline, and higher PAI-1 ag values were detected at the end of the operation. Also, D-
dimer levels were 2-fold higher at 24 h in the patients undergoing reoperation. PAI-1 activity,
which was measured only in patients with thrombosis or reoperation, correlated positively
with PAI-1 antigen (data not shown).
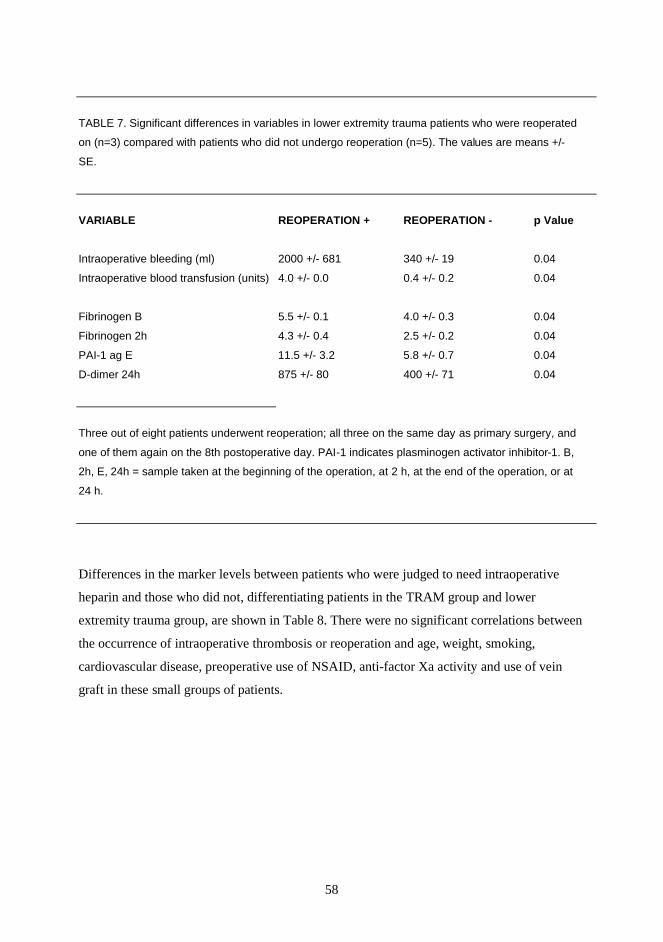
58
TABLE 7. Significant differences in variables in lower extremity trauma patients who were reoperated
on (n=3) compared with patients who did not undergo reoperation (n=5). The values are means +/-
SE.
VARIABLE REOPERATION + REOPERATION - p Value
Intraoperative bleeding (ml) 2000 +/- 681 340 +/- 19 0.04
Intraoperative blood transfusion (units) 4.0 +/- 0.0 0.4 +/- 0.2 0.04
Fibrinogen B 5.5 +/- 0.1 4.0 +/- 0.3 0.04
Fibrinogen 2h 4.3 +/- 0.4 2.5 +/- 0.2 0.04
PAI-1 ag E 11.5 +/- 3.2 5.8 +/- 0.7 0.04
D-dimer 24h 875 +/- 80 400 +/- 71 0.04
Three out of eight patients underwent reoperation; all three on the same day as primary surgery, and
one of them again on the 8th postoperative day. PAI-1 indicates plasminogen activator inhibitor-1. B,
2h, E, 24h = sample taken at the beginning of the operation, at 2 h, at the end of the operation, or at
24 h.
Differences in the marker levels between patients who were judged to need intraoperative
heparin and those who did not, differentiating patients in the TRAM group and lower
extremity trauma group, are shown in Table 8. There were no significant correlations between
the occurrence of intraoperative thrombosis or reoperation and age, weight, smoking,
cardiovascular disease, preoperative use of NSAID, anti-factor Xa activity and use of vein
graft in these small groups of patients.
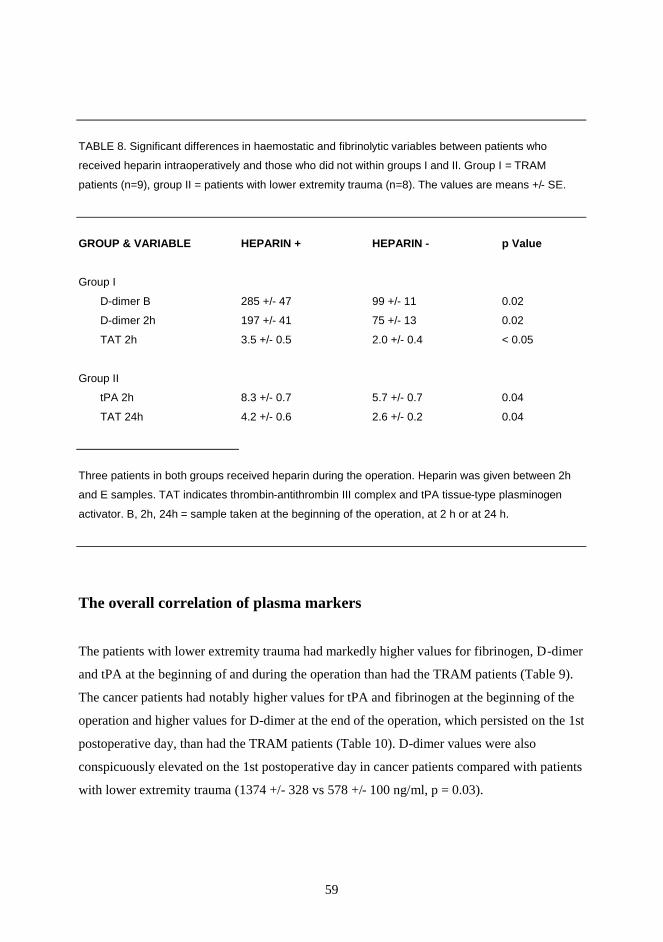
59
TABLE 8. Significant differences in haemostatic and fibrinolytic variables between patients who
received heparin intraoperatively and those who did not within groups I and II. Group I = TRAM
patients (n=9), group II = patients with lower extremity trauma (n=8). The values are means +/- SE.
GROUP & VARIABLE HEPARIN + HEPARIN - p Value
Group I
D-dimer B 285 +/- 47 99 +/- 11 0.02
D-dimer 2h 197 +/- 41 75 +/- 13 0.02
TAT 2h 3.5 +/- 0.5 2.0 +/- 0.4 < 0.05
Group II
tPA 2h 8.3 +/- 0.7 5.7 +/- 0.7 0.04
TAT 24h 4.2 +/- 0.6 2.6 +/- 0.2 0.04
Three patients in both groups received heparin during the operation. Heparin was given between 2h
and E samples. TAT indicates thrombin-antithrombin III complex and tPA tissue-type plasminogen
activator. B, 2h, 24h = sample taken at the beginning of the operation, at 2 h or at 24 h.
The overall correlation of plasma markers
The patients with lower extremity trauma had markedly higher values for fibrinogen, D-dimer
and tPA at the beginning of and during the operation than had the TRAM patients (Table 9).
The cancer patients had notably higher values for tPA and fibrinogen at the beginning of the
operation and higher values for D-dimer at the end of the operation, which persisted on the 1st
postoperative day, than had the TRAM patients (Table 10). D-dimer values were also
conspicuously elevated on the 1st postoperative day in cancer patients compared with patients
with lower extremity trauma (1374 +/- 328 vs 578 +/- 100 ng/ml, p = 0.03).
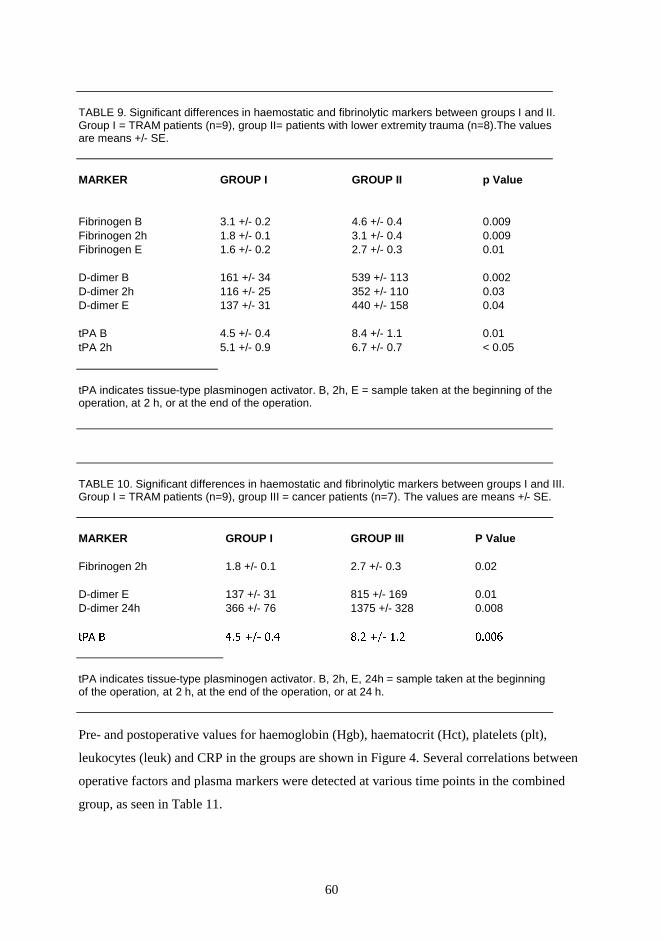
60
TABLE 9. Significant differences in haemostatic and fibrinolytic markers between groups I and II. Group I = TRAM patients (n=9), group II= patients with lower extremity trauma (n=8).The values are means +/- SE.
MARKER GROUP I GROUP II p Value
Fibrinogen B 3.1 +/- 0.2 4.6 +/- 0.4 0.009 Fibrinogen 2h 1.8 +/- 0.1 3.1 +/- 0.4 0.009 Fibrinogen E 1.6 +/- 0.2 2.7 +/- 0.3 0.01
D-dimer B 161 +/- 34 539 +/- 113 0.002 D-dimer 2h 116 +/- 25 352 +/- 110 0.03 D-dimer E 137 +/- 31 440 +/- 158 0.04
tPA B 4.5 +/- 0.4 8.4 +/- 1.1 0.01 tPA 2h 5.1 +/- 0.9 6.7 +/- 0.7 < 0.05
tPA indicates tissue-type plasminogen activator. B, 2h, E = sample taken at the beginning of the operation, at 2 h, or at the end of the operation.
TABLE 10. Significant differences in haemostatic and fibrinolytic markers between groups I and III. Group I = TRAM patients (n=9), group III = cancer patients (n=7). The values are means +/- SE.
MARKER GROUP I GROUP III P Value
Fibrinogen 2h 1.8 +/- 0.1 2.7 +/- 0.3 0.02
D-dimer E 137 +/- 31 815 +/- 169 0.01 D-dimer 24h 366 +/- 76 1375 +/- 328 0.008
��� � ��� � ��� �� � ��� �����
tPA indicates tissue-type plasminogen activator. B, 2h, E, 24h = sample taken at the beginning of the operation, at 2 h, at the end of the operation, or at 24 h.
Pre- and postoperative values for haemoglobin (Hgb), haematocrit (Hct), platelets (plt),
leukocytes (leuk) and CRP in the groups are shown in Figure 4. Several correlations between
operative factors and plasma markers were detected at various time points in the combined
group, as seen in Table 11.
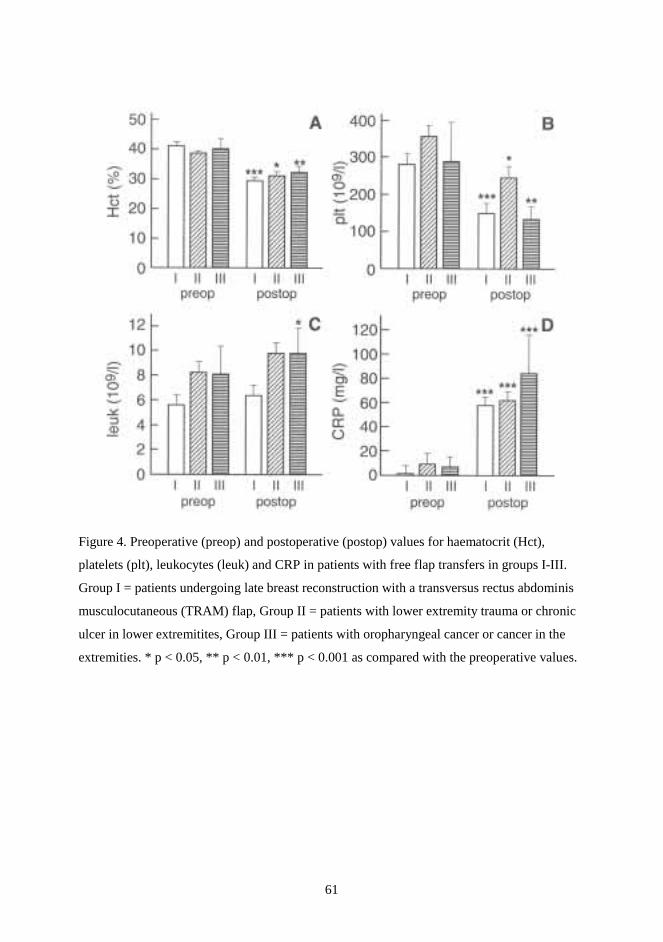
61
Figure 4. Preoperative (preop) and postoperative (postop) values for haematocrit (Hct),
platelets (plt), leukocytes (leuk) and CRP in patients with free flap transfers in groups I-III.
Group I = patients undergoing late breast reconstruction with a transversus rectus abdominis
musculocutaneous (TRAM) flap, Group II = patients with lower extremity trauma or chronic
ulcer in lower extremitites, Group III = patients with oropharyngeal cancer or cancer in the
extremities. * p < 0.05, ** p < 0.01, *** p < 0.001 as compared with the preoperative values.

62
TABLE 11. Correlations between plasma markers and operative factors in combined group I-III. Group I = TRAM patients (n=9), group II = lower extremity trauma patients (n=8), group III = cancer patients (n=7).
R p
Haemoglobin and haematocrit vs fibrinogen B -0.44- -0.46 0.02-0.03 Haematocrit vs TAT 24h 0.41 <0.05 Haemoglobin and haematocrit vs tPA 24h 0.55-0.59 0.002-0.005 Haemoglobin and haematocrit vs PAI-1 24h 0.55-0.64 0.006-0.0001
Leukocytes vs tPA B and 24h 0.46-0.47 both 0.02 Leukocytes vs PAI-1 B and 24h 0.52-0.58 <0.01-0.004 Leukocytes vs D-dimer 24h 0.45 0.03
Platelets vs TAT B 0.43 0.04
CRP vs fibrinogen B and 24h 0.50-0.52 both 0.01 CRP vs D-dimer 24h 0.47 0.02 CRP vs PAI-1 24h 0.54 0.006
Operation time vs TAT 24h 0.48 0.02 Operation time vs tPA 24h 0.46 0.02 Operation time vs PAI-1 E and 24h 0.43-0.54 0.03-0.008
Tourniquet time vs TAT 24h 0.59 0.04
Intraoperative bleeding vs TAT 24h 0.46 0.02 Intraoperative bleeding vs tPA 24h 0.52 0.009 Intraoperative bleeding vs PAI-1 E 0.64 <0.0001
Postoperative blood transfusion vs tPA 24h 0.68 0.01
The effect of LMWH (dalteparin)
The level for systemic anticoagulation with dalteparin was assessed by anti -factor Xa activity
before induction of anaesthesia. No significant correlations were found either in plasma
markers at baseline when the patients who had received LMWH the previous evening were
compared with those who had received it in the morning or in the patients with or without
intraoperative thrombosis. In the TRAM group, anti-factor Xa activity ranged from 0.14 to
0.55 U/ml in the patients who had received dalteparin 2500-5000 IU in the morning 2-3 h
before induction of anaesthesia. In addition, anti-factor Xa activity was measured during the

63
operation in one patient who developed intraoperative venous thrombosis. The activity was
lowest one, 0.14 U/ml, at the beginning of the operation; 8 h later, at the time of
intraoperative thrombosis, it was undetectable (unpublished data). In the TRAM group,
positive correlations existed between anti-factor Xa and tPA as well as PAI-1 levels at 2 h (r
0.77-0.80).
In patients with lower extremity trauma, anti-factor Xa activity ranged from 0.21 to 0.36 U/ml
in the four patients who had received dalteparin 2500 IU in the morning 2-3 hours before
induction of anaesthesia, one of them twice daily since the previous day. The remaining four
patients, who had received dalteparin 2500 IU the previous evening, had anti-factor Xa
activity levels of under 0.3 U/ml. One of these patients with non-valid anticoagulation levels
received unfractionated heparin intraoperatively, since blood appeared to clot in the operation
area and the anastomosis did not function optimally; another patient, the one with ASO and
LED who received a vein graft, was also heparinised, but even so she developed a
postoperative thrombosis and had to undergo reoperation some hours later.
In the cancer group, the level of systemic anticoagulation ranged from < 0.04 (= undetectable)
to 0.07 U/ml in the patients given dalteparin 2500-5000 IU the previous evening, and from
0.26 to 0.38 U/ml in those given 2500 IU in the morning, 2-3 h earlier. The patient who
developed intraoperative thrombosis had anti-factor Xa < 0.04, and the patient with
postoperative thrombosis requiring reoperation 0.26 U/ml.
5.2. Histopathology and immunohistochemistry of failed human
anastomoses (Study I)
Overall vessel morphology
Evaluation of the overall morphology of the failed human anastomoses revealed technical
problems in two of the anastomoses collected at TRAM reconstructions, a thrombus having
formed adjacent to a constricting suture. An occlusive thrombus was present in 6/17 samples,
and a smaller, non-occlusive thrombus in 4/17 samples. The other samples showed limited
mural thrombosis only.

64
Immunohistochemistry
The immunohistochemical analysis was targeted at the three main factors underlying
thrombus formation: damaged endothelial cells, accumulation of platelets and accumulation
of fibrin. We found colocalised loss of endothelial cells (CD 31) and accumulation of platelets
(CD 42b) and mature fibrin at the failed anastomosis sites, see Table 12. Overall, the staining
for platelets and fibrin correlated, the staining intensity for plateles being highest in the totally
occluded samples. CD 31 (PECAM-1) was mainly used to verify the presence of endothelial
cells, but since it is also expressed in platelets, it could recognise the adhered platelets as well
(DeLisser et al 1993). A typical feature was the lack of PECAM-1-positive endothelial cells
in the anastomosis area. These endothelium-deficient sites were mainly covered with
moderate to large thrombi in which both platelets and fibrin were present. Of interest was the
finding that, at the anastomoses with loss of endothelial cells, platelet-related PECAM-1
staining, too, was lacking in the single layers of GP 1b α - positive platelets. However, mural
and larger thrombi were positive for both PECAM-1 and CD 42b, detecting GP 1b α.
Adjacent sections further from the anastomoses (2 mm - 3 cm), when available, revealed
intact endothelial cells and only limited platelet and fibrin-associated staining.
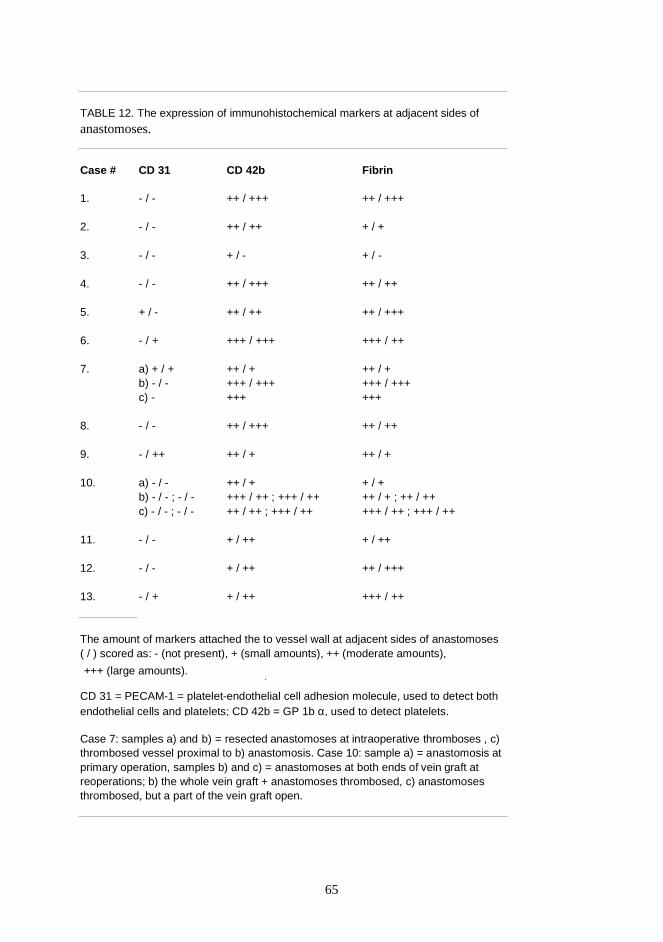
65
TABLE 12. The expression of immunohistochemical markers at adjacent sides of
anastomoses.
Case # CD 31 CD 42b Fibrin
1. - / - ++ / +++ ++ / +++
2. - / - ++ / ++ + / +
3. - / - + / - + / -
4. - / - ++ / +++ ++ / ++
5. + / - ++ / ++ ++ / +++
6. - / + +++ / +++ +++ / ++
7. a) + / + ++ / + ++ / + b) - / - +++ / +++ +++ / +++ c) - +++ +++
8. - / - ++ / +++ ++ / ++
9. - / ++ ++ / + ++ / +
10. a) - / - ++ / + + / + b) - / - ; - / - +++ / ++ ; +++ / ++ ++ / + ; ++ / ++ c) - / - ; - / - ++ / ++ ; +++ / ++ +++ / ++ ; +++ / ++
11. - / - + / ++ + / ++
12. - / - + / ++ ++ / +++
13. - / + + / ++ +++ / ++
The amount of markers attached the to vessel wall at adjacent sides of anastomoses ( / ) scored as: - (not present), + (small amounts), ++ (moderate amounts),
+++ (large amounts). )
CD 31 = PECAM-1 = platelet-endothelial cell adhesion molecule, used to detect both endothelial cells and platelets; CD 42b = GP 1b α, used to detect platelets.
Case 7: samples a) and b) = resected anastomoses at intraoperative thromboses , c) thrombosed vessel proximal to b) anastomosis. Case 10: sample a) = anastomosis at primary operation, samples b) and c) = anastomoses at both ends of vein graft at reoperations; b) the whole vein graft + anastomoses thrombosed, c) anastomoses thrombosed, but a part of the vein graft open.
66
Histopathology
Histopathological analysis of the failed anastomoses showed that inflammation of the vessel
was a prominent feature at reoperations when the anastomosis was occluded. Inflammation
was found in the two thrombosed vein grafts of the TRAM patient who underwent
reoperations on the 3rd and 7th postoperative days, in the thrombosed venous anastomosis of
the patient with tonsillar cancer at reoperation on the 3rd postoperative day and in the arterial
sample from the patient with failed replantation of the mid-hand on the 1st postoperative day.
In some of these vessels, the internal elastic lamina was discontinuous and fibrin was found,
even in the smooth muscle cell layer extending into the media. In one of the TRAM patients,
inflammatory cells had already been found at primary operation at the second thrombotic
event (unpublished data).
5.3. Local anti-thrombotic effect of HEP-PG (Study IV)
Thrombin times and bleeding times
In this experimental study we tested the local effect of HEP-PG in early (10 min) and late (3-
day) thrombus formation in rat common femoral arteries. We started the experiments with
three different thrombosis models (TM), using SEM to evaluate early thrombus formation
(experiment I). These models included scratching of the vessel wall (TM 1), arterial wall
inversion (TM 2) and an ordinary microvascular anastomosis (TM 1 and TM 2 unpublished
data). The anastomosis model was also used to quantify early thrombus formation with
Indium 111-labelled platelets (experiment II) and to analyse late thrombus formation
(experiment III). Three different irrigation solutions were employed locally at the site of
vessel injury: saline (saline group, controls), unfractionated heparin (HEP group) and heparin-
proteoglycans (HEP-PG group). To exlude a systemic effect of the irrigation solutions we
demonstrated that thrombin times were equal in each treatment group in the anastomosis
model at 10 min (mean, range): saline group 30.0 (27.8-31.0), HEP group 30.6 (27.6-35.3)
and HEP-PG group 29.6 (28.2-31.3). In no experiment did bleeding from the sutured vessels
differ significantly between the treatments. Bleeding times tended to be prolonged in the HEP
group but did not markedly differ in the saline or HEP-PG groups, see Table 13 (TM 1 and
TM 2 unpublished data).

67
TABLE 13. Bleeding times at 10 min in the thrombosis models.
Experiment & Model Saline group HEP group HEP-PG group
Experiment I TM1 52 (35-90) 72 (25-180) 35 (15-65) TM2 15 (0-30) 42 (10-75) 41 (5-150) Anastomosis 30 (10-60) 66 (20-100) 42 (15-80)
Experiment II (anastomosis) 34 (20-45) 45 (35-90) 49 (15-110)
Experiment III (anastomosis) 46 (15-120) 86 (30-225) 47 (15-100)
The values are means (ranges) in seconds. TM = thrombosis model.
Patency rates
To test for the occurrence of occlusive thrombi, we tested patency in experiments I and II at
10 min, and in experiment III repeatedly during a follow-up period of 3 days. Details of
patency and blood flow characteristics in the three thrombosis models at the 10 min follow-up
in experiment I are presented together with the results of the SEM analysis in Table 13 (TM 1
and TM 2 unpublished data). In general, thrombotic occlusion and flow problems tended to
occur in the saline group in TM 2 and anastomosis. The HEP and HEP-PG groups generally
remained patent but two animals in TM 1 showed somewhat compromised flow in the HEP-
PG group. The anastomosis model provided fairly uniform patency data in the HEP and HEP-
PG groups. In experiment II (Indium 111-labelling) patency at 10 min was 6/7 in the saline
group, 6/6 in the HEP group and 6/7 in the HEP-PG group. In experiment III (3-day follow-
up) patency varied somewhat during the follow-up period (see Table 14), and on the 3rd
postoperative day was as follows: 5/7 in the saline group, 6/7 in the HEP group and 7/7 in the
HEP-PG group.
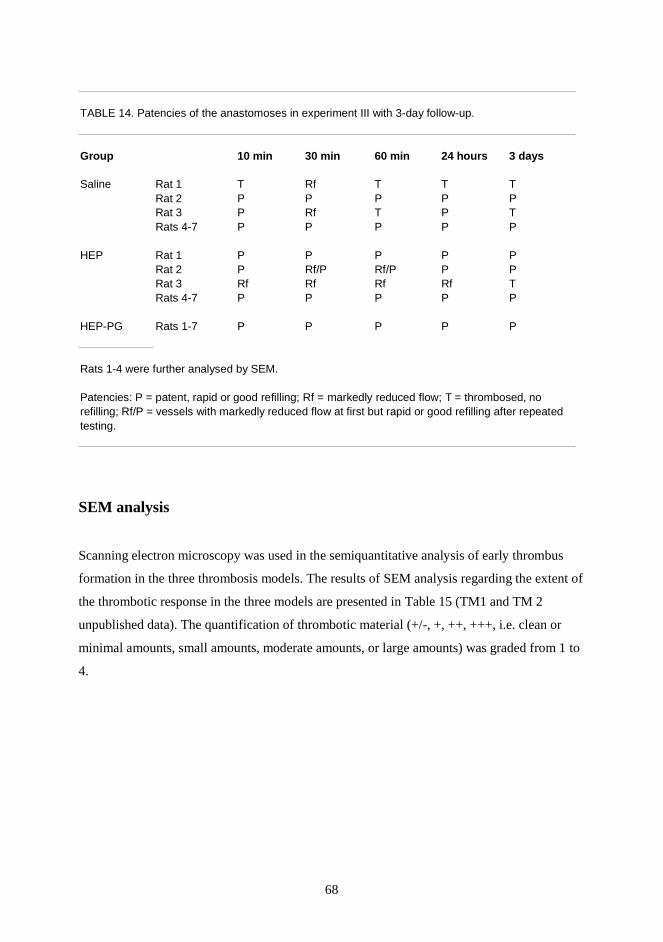
68
TABLE 14. Patencies of the anastomoses in experiment III with 3-day follow-up.
Group 10 min 30 min 60 min 24 hours 3 days
Saline Rat 1 T Rf T T TRat 2 P P P P PRat 3 P Rf T P TRats 4-7 P P P P P
HEP Rat 1 P P P P PRat 2 P Rf/P Rf/P P PRat 3 Rf Rf Rf Rf TRats 4-7 P P P P P
HEP-PG Rats 1-7 P P P P P
Rats 1-4 were further analysed by SEM.
Patencies: P = patent, rapid or good refilling; Rf = markedly reduced flow; T = thrombosed, norefilling; Rf/P = vessels with markedly reduced flow at first but rapid or good refilling after repeatedtesting.
SEM analysis
Scanning electron microscopy was used in the semiquantitative analysis of early thrombus
formation in the three thrombosis models. The results of SEM analysis regarding the extent of
the thrombotic response in the three models are presented in Table 15 (TM1 and TM 2
unpublished data). The quantification of thrombotic material (+/-, +, ++, +++, i.e. clean or
minimal amounts, small amounts, moderate amounts, or large amounts) was graded from 1 to
4.
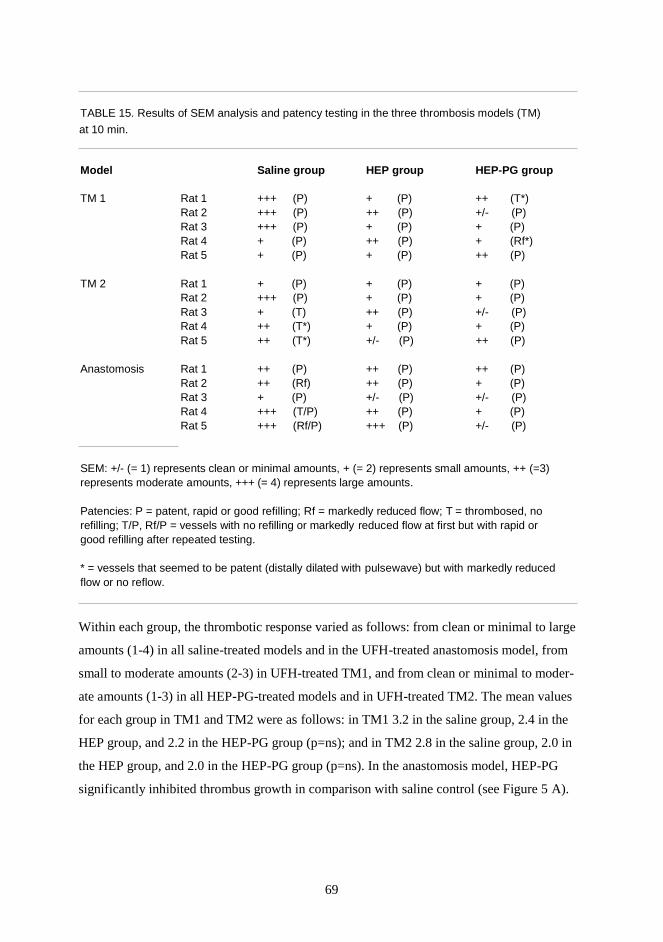
69
TABLE 15. Results of SEM analysis and patency testing in the three thrombosis models (TM)
at 10 min.
Model Saline group HEP group HEP-PG group
TM 1 Rat 1 +++ (P) + (P) ++ (T*)Rat 2 +++ (P) ++ (P) +/- (P)Rat 3 +++ (P) + (P) + (P)Rat 4 + (P) ++ (P) + (Rf*)Rat 5 + (P) + (P) ++ (P)
TM 2 Rat 1 + (P) + (P) + (P)Rat 2 +++ (P) + (P) + (P)Rat 3 + (T) ++ (P) +/- (P)Rat 4 ++ (T*) + (P) + (P)Rat 5 ++ (T*) +/- (P) ++ (P)
Anastomosis Rat 1 ++ (P) ++ (P) ++ (P)Rat 2 ++ (Rf) ++ (P) + (P)Rat 3 + (P) +/- (P) +/- (P)Rat 4 +++ (T/P) ++ (P) + (P)Rat 5 +++ (Rf/P) +++ (P) +/- (P)
SEM: +/- (= 1) represents clean or minimal amounts, + (= 2) represents small amounts, ++ (=3)represents moderate amounts, +++ (= 4) represents large amounts.
Patencies: P = patent, rapid or good refilling; Rf = markedly reduced flow; T = thrombosed, norefilling; T/P, Rf/P = vessels with no refilling or markedly reduced flow at first but with rapid orgood refilling after repeated testing.
* = vessels that seemed to be patent (distally dilated with pulsewave) but with markedly reducedflow or no reflow.
Within each group, the thrombotic response varied as follows: from clean or minimal to large
amounts (1-4) in all saline-treated models and in the UFH-treated anastomosis model, from
small to moderate amounts (2-3) in UFH-treated TM1, and from clean or minimal to moder-
ate amounts (1-3) in all HEP-PG-treated models and in UFH-treated TM2. The mean values
for each group in TM1 and TM2 were as follows: in TM1 3.2 in the saline group, 2.4 in the
HEP group, and 2.2 in the HEP-PG group (p=ns); and in TM2 2.8 in the saline group, 2.0 in
the HEP group, and 2.0 in the HEP-PG group (p=ns). In the anastomosis model, HEP-PG
significantly inhibited thrombus growth in comparison with saline control (see Figure 5 A).
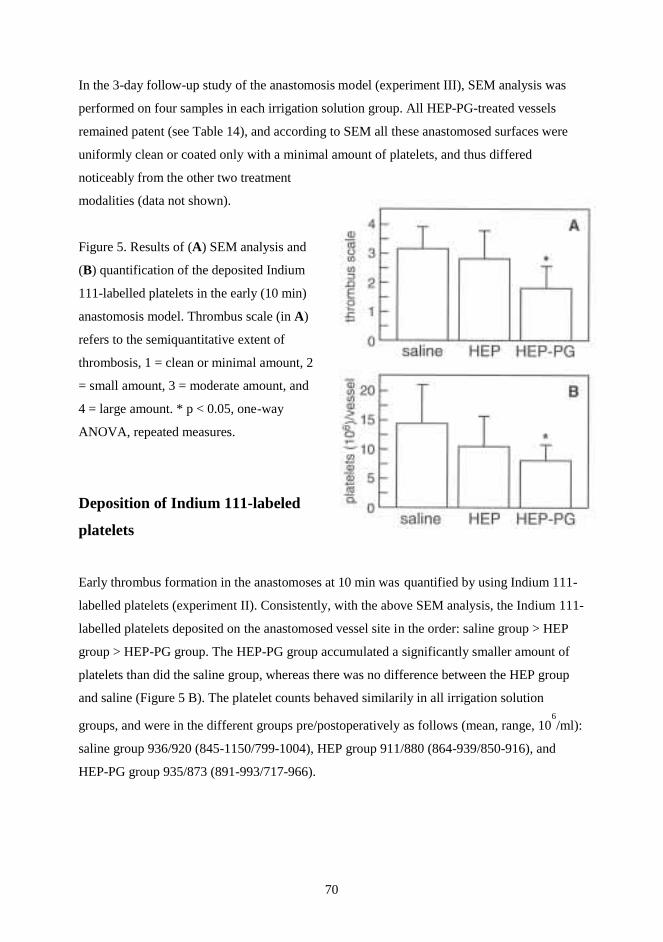
70
In the 3-day follow-up study of the anastomosis model (experiment III), SEM analysis was
performed on four samples in each irrigation solution group. All HEP-PG-treated vessels
remained patent (see Table 14), and according to SEM all these anastomosed surfaces were
uniformly clean or coated only with a minimal amount of platelets, and thus differed
noticeably from the other two treatment
modalities (data not shown).
Figure 5. Results of (A) SEM analysis and
(B) quantification of the deposited Indium
111-labelled platelets in the early (10 min)
anastomosis model. Thrombus scale (in A)
refers to the semiquantitative extent of
thrombosis, 1 = clean or minimal amount, 2
= small amount, 3 = moderate amount, and
4 = large amount. * p < 0.05, one-way
ANOVA, repeated measures.
Deposition of Indium 111-labeled
platelets
Early thrombus formation in the anastomoses at 10 min was quantified by using Indium 111-
labelled platelets (experiment II). Consistently, with the above SEM analysis, the Indium 111-
labelled platelets deposited on the anastomosed vessel site in the order: saline group > HEP
group > HEP-PG group. The HEP-PG group accumulated a significantly smaller amount of
platelets than did the saline group, whereas there was no difference between the HEP group
and saline (Figure 5 B). The platelet counts behaved similarily in all irrigation solution
groups, and were in the different groups pre/postoperatively as follows (mean, range, 106/ml):
saline group 936/920 (845-1150/799-1004), HEP group 911/880 (864-939/850-916), and
HEP-PG group 935/873 (891-993/717-966).

71
6. DISCUSSION
Local thrombi at microanastomoses threaten the outcome of tissue transplantations (Khouri
1992). An occlusion formed intraoperatively is easier to detect in time to salvage the
transplanted tissue, whereas thrombi formed during the postoperative period may be observed
too late, and part of, or even the whole, flap may develop necrosis. Recent studies have
described sensitive, new markers for coagulation and fibrinolysis that have been found
promising in detecting threatening or obvious thrombosis during heterogeneous microsurgical
reconstructions in various diseases (Komuro et al. 1998).
Our studies show that the problem of thrombosis still exists in microsurgery. Two thirds of
the TRAM patients had an event of intraoperative local thrombosis, one third of the patients
with lower extremity trauma required reoperation, and two out of seven cancer patients had
thrombotic events either during or after surgery. However, only one of the flaps was lost. The
greater amount of thrombotic events in the TRAM group could be due to the fact that the
vessels are smaller and often located in scarry tissue whereas those in the two other groups are
larger, and in the head and neck area the flow is higher (Lorenzetti et al. 2001).
The plasma markers used in this study are very specific and sensitive in measuring the
activation of thrombin and plasmin. Their capacity to predict or diagnose local thrombosis is,
however, a different matter. Through careful sample handling special attention was paid to
preventing artificial activation of blood coagulation and fibrinolysis (Hafner et al. 1993,
Iversen 1997). Since the ELISA assays used are quantitative, the results may not be applicable
to semiquantitative latex and haemagglutination tests (Meissner et al. 2000).
Preoperative assessment of hypercoagulability showed that half of the TRAM patients with an
intraoperative thrombotic event had enhanced thrombin generation, revealed by TAT and/or
F1+2, before primary surgery. Patients with lower extremity trauma had higher levels of
fibrinogen, D-dimer and tPA than did TRAM patients, reflecting long-lasting activation of the
coagulation system (Brozovic 1977, Bennet and Towler 1985). Within the lower extremity
trauma group, the patients with surgically treated recent trauma had clearly higher D-dimer
levels than did patients with old trauma. In the cancer group assessment of preoperative
hypercoagulability with fibrinogen and/or D-dimer revealed that half of the patients were
72
hypercoagulable, a finding that is consistent with reports published elsewhere (Yoda and
Tsukasa 1981, Falanga et al. 1993, Falanga and Rickles 1999). The same was true when more
sensitive markers, TAT and F1+2, were used, likewise in conformity with other reports
(Falanga et al. 1993, Falanga and Rickles 1999, Gouin-Thibault and Samama 1999).
However, no significant differences were noted in the plasma markers at baseline between
patients with and patients without intraoperative local thrombosis, except for slightly
enhanced fibrinolysis, with elevated levels of tPA, in the patients without thrombosis.
The thrombin markers TAT and F1+2 were found to have potential in predicting thrombotic
risk in the context of both intraoperative thrombosis and reoperation within all groups. In half
of the TRAM patients with intraoperative thrombosis, the markers of thrombin generation
increased at the time of obvious thrombosis or reoperation. Of interest was the finding of a 9-
fold increase in TAT on the 1st postoperative day in the patient who went on to develop edge
necrosis some months later. In the lower extremity trauma group, one third of the patients, all
with excessive bleeding, showed distinct thrombin generation at the end of primary surgery,
and later on the same day all underwent reoperation. One of them also generated excessive
thrombin on the 8th postoperative day upon the removal of a necrotic flap. In the cancer
group, the patients with thrombotic events, and who were in a clear hypercoagulable state
before surgery, showed increased thrombin generation at the time of thrombosis, as well.
We also investigated how surgery itself with the associated bleeding would affect the plasma
markers. An earlier study on coagulation activation during microsurgery showed that, the
thrombin markers gradually increased during the operation in some of the patients (Komuro et
al. 1998). In the present study, TAT values increased markedly towards the end of the
operation in half of the lower extremity trauma patients and in all, but one, of the patients
with cancer and likewise in all, but one, of the TRAM patients without thrombosis, indicating
distinct thrombin generation in response to surgical trauma and possibly ischaemia and
reperfusion (Holmberg et al. 1999). The values returned to normal the next day in all patients
except for the two with lower extremity trauma who underwent reoperation. Interestingly, this
phenomenon was not found in the TRAM patients with intraoperative thrombosis, suggesting
consumption of antithrombin III, a hypothesis that needs to be tested in a further study. A
general decrease in fibrinogen levels, due to haemodilution and bleeding, followed by an
increase on the 1st postoperative day, has been reported elsewhere (Brozovic 1977, Bennett
and Towler 1985, Murray et al. 1988, Fujii et al. 1994, Peltonen et al. 1997). Increased fibrin
73
turnover has previously been shown in the context of surgery and bleeding as well (Fujii et al.
1994, Peltonen et al. 1997). In the present study, the cancer patients showed markedly
elevated D-dimer levels on the 1st postoperative day, as did the TRAM patients, only to a
lesser extent. Activation of the fibrinolytic system, as measured by tPA and PAI-1 levels, was
seen only in some of the vascular compromised patients. Also, ischaemia and tourniquet
application have been found to promote fibrinolysis (Brozovic 1977, Petäjä et al. 1987, Niemi
et al. 1996), although this was not found in our combined group of patients. The interactive
complexity of the activation of the coagulation and fibrinolytic systems with the changes in
haemorheology during surgery is reflected in the vast number of other significant correlations
between the operative events and plasma markers.
The intraoperative use of unfractionated heparin in six patients was necessitated mainly by
manifest local thrombosis, and half of these patients required reoperation as well. During
active inflammation caused by increased concentrations of several acute phase proteins, the
specifity of heparin binding to antithrombin III diminishes. Even before the operation, the D-
dimer level in the heparinised group was almost 3-fold that in the other patients, which is
compatible with the finding that pre-existing enhancement of fibrin generation complicates
the operative outcome. No difference in plasma markers between heparinised and non-
heparinised patients was observed at the end of the operation, suggesting that heparin did
neutralise some, but only some, of the excessive thrombin generation in the complicated
cases, since persistent thrombin formation was measured on the 1st postoperative day in the
group receiving heparin (Amelsberg et al. 1992).
Preoperative anticoagulation therapy with LMWH, dalteparin, was given routinely for
prophylaxis of deep vein thrombosis and pulmonary embolism (Weitz 1997, Prandoni 2001).
As recently suggested, the efficacy of LMWH might be improved by monitoring anti-factor
Xa levels (Hirsh et al. 2001). In our studies, the anti-thrombotic effect of dalteparin turned out
to be incomplete in the patients who had received it the previous evening, as measured by
anti-factor Xa levels. This is not surprising since the doses used were low and the half-lives of
LMWH range from 2 to 4 h for anti-factor Xa activity (Bergqvist et al 19983, Nader et al.
1999). However, even in some patients who had received dalteparin a few hours before
surgery, the dose did not cover the whole operation. No significant associations could,
however, be seen between the timing of LMWH or level of anti-factor Xa and the baseline
levels of plasma markers or occurrence of thrombosis in this small number of patients.
74
Enhanced anticoagulation therapy is recommended in oncological surgery since cancer
patients undergoing extensive surgery are considered to be at particularly high risk of
developing thromboembolic complications (Gouin-Thibault and Samama 1999, Prandoni
2001). The risk of haemorrhagic complications has, however, discouraged some
microsurgeons from the systemic use of anticoagulants during extensive reconstructive
operations. Yet, previous studies have shown that the use of LMWH, even in high dosages,
does not lead to enhanced bleeding in cancer patients (Bergqvist et al. 1995, Gondret et al.
1995, Enoxan Study group 1997). In these patients, as well as in those with recent trauma,
recognition of the procoagulant state could help us to target meticulous antithrombotic
protection during and after surgery. Further studies will show how enhanced anticoagulation
therapy influences coagulation activation and perioperative bleeding during microsurgical
reconstructions.
Since local thrombotic problems were encountered during many of the reconstructive
procedures, we were also interested in evaluating the failed vessel anastomoses. The novelty
of these studies was that they focused mainly on arterial anastomoses that failed during
primary microsurgery; previously, failed human anastomoses have mostly been harvested at
reoperations (Lidman and Daniel 1981, Gu et al. 1992). As the majority of the anastomoses in
our study were done by experienced microsurgeons, the technical quality was good - only in
two cases had a thrombus formed adjacent to a constricting suture. The thrombus size varied
in the samples from a clear, either occlusive or partial, clot to a mural thrombus with an open
lumen. In at least one of these samples, during vessel harvesting, a loose red thrombus had
dropped out at the time of resection.
The immunohistochemichal analysis sought to reveal the three main factors underlying
thrombus formation: endothelial cell damage, and the accumulation of platelets and of fibrin.
These markers have not been used previously in this context. Our finding of loss of
endothelial cells around the anastomoses is consistent with earlier studies, both experimental
and clinical, and is considered normal (Acland and Tranchtenberg 1977, Lidman and Daniel
1981). However, the use of clamps or heparinised saline irrigation instead of lactated Ringer’s
solution may have contributed to this injury (Acland et al. 1980, Thomson et al. 1998). When
vein graft was used, the endothelium in the middle of the graft was intact and the lumen open,
as the thrombus had formed adjacent to both anastomoses. We found that the de-

75
endothelialised anastomoses were covered with platelets and fibrin. The staining pattern for
platelets and fibrin correlated, suggesting that the platelet thrombi had proceeded to a stage of
stabilisation by mature fibrin strands (Bennett and Towler 1985). Earlier, experimental studies
on anastomotic healing have shown that a monolayer of platelets normally exists at the site of
endothelial damage (Nightingale et al. 1980, Sigurbjörnsson et al. 1994). Of interest would
have been to study the amount of platelets and fibrin needed for anastomotic sealing in a well-
functioning anastomosis, but this information was not available for comparison. A novel
finding was the absence of PECAM-1 staining in the single adherent layers of platelets,
whereas PECAM-1 was found positive in micro and larger thrombi. As PECAM-1 is
currently throught to represent an inhibitory signalling molecule involved in platelet adhesion,
our finding is important and calls for further studies (DeLisser et al. 1993, Newman 1999).
Experimental studies have shown that leukocytes appear at anastomoses from 1 h onwards
(Nightingale et al. 1980). It has been found that endothelial cells and platelets via their surface
protein, P-selectin, may localise leukocytes to the region (Ruggeri and Ware 1993, Ware and
Coller 1995, Downing et al. 1997). The release of vasoactive and mitogenic agents from
platelets can also contribute to the inflammatory response (Ware and Coller 1995). In our
study, inflammatory cells had accumulated in one of the samples harvested at the second
intraoperative thrombotic event. At reoperations, however, all the thrombosed vessels showed
distinct inflammation, consistent with previous findings (Lidman and Daniel 1981, Gu et al.
1992). Even the internal elastic lamina were disrupted in some of the inflamed vessels, as
reported earlier (Lidman and Daniel 1981), indicating proteolytic remodelling in the vessel.
Also, fibrin associated with these deeper structures of the vessel are indicative of local
activation of coagulation.
The ideal antithrombotic agent is still lacking (Cooley and Gould 1991). Even at an optimal
plasma anticoagulation level, the antithrombotic effect of systemic heparin has proved to be
inadequate to address the mechanisms of arterial thrombosis (Johnson and Barker 1992,
Maraganore 1993, Arnljots and Bergqvist 1995, Arnljots et al. 1997). Recently, HEP-PG have
shown promise in blocking thrombus growth, in contrast to standard heparins, in an arterial
thrombosis model in vitro (Lassila et al. 1997). The inhibitory effect of HEP-PG on platelet-
collagen interaction was observed at both low and high shear rates, the shear-induced
enhancement of platelet deposition being fully eliminated. The efficacy of soluble HEP-PG
depended both on the inhibition of GPIa/IIa-mediated platelet recruitment and on tight
76
binding to von Willebrand factor. More recently, similar results have been obtained by
immobilising HEP-PG together with collagen (Kauhanen et al. 2000).
New antithrombotic agents can be studied in vivo in a multitude of more or less artificial
models of vascular trauma. In our pilot studies we first used two models in which the
subendothelial collagen was exposed to circulating platelets to varying extents. The first
model, that of Davidsson et al., was chosen to create a severe lesion on the endothelium,
intima and media by scratching the vessel, but was modified by omitting stasis (Davidson et
al. 1990). In a related model, Rooks et al. have shown that patency was directly related to the
length of stasis after vessel repair; when no distal clamping occurred, the patency was 100%,
whereas with 90 s clamping the patency rate fell to 20% (Rooks et al. 1993). We confirmed
this finding in our experiments - except for some reflow problems all the vessels were patent.
The overall suitability of this thrombosis model was compromised by the large variability
caused by the difficulty of standardising the scratching procedure. The second model was
intended to simulate an injury revealing all layers of the vessel wall including the adventitia,
especially the most thrombogenic collagen types I and III encountered in the media and
adventitia (Kehrel 1995). Scanning electron micrographic analysis of this model was not
feasible, since only the superficial thrombus attached to the flap surface could be observed
and we could not quantify the extent of thrombotic response underneath the flap.
Quantification would, however, have been possible with Indium 111-labelled platelets.
The anastomosis model was technically feasible, reproduceable and amenable to
semiquantification in SEM. Since it is clinically most relevant in microvascular surgery and
arteriovenous (a-v) shunts, it was chosen for quantitative analysis with Indium 111-labelled
platelets and long-term follow-up. Thrombogenicity was enhanced by leaving the adventitia at
vessel ends, thus allowing adventitial collagen and tissue factor to enter the lumen at needle
holes and eventually between the sutures (Kehrel 1995).
The effect of repeated patency testing in producing emboli and eventually maintaining
patency was seen in both the acute and the long-term follow-up groups. In the first series of
acute thrombosis assessments the repeated patency test revealed possible embolisation in
some of the control vessels and, moreover, SEM analysis showed the largest number of
platelets on these vessels. In the 3-day follow-up, one vessel in the HEP group had to struggle
for patency during the first hour, and two anastomoses in the control group became
77
thrombosed during the same time. In both of these vessels a struggle for patency with
repetitive occlusion and recanalisation occurred during the first hour to first day after the
operation. As previous studies have shown, thrombosis is not an all-or-none phenomenon but
a continuous struggle between coagulation and fibrinolytic systems, from the first minutes to
hours or even days after surgery (Tangelder 1989, Salemark et al. 1995, Weinzweig and
Gonzalez 1995, Chen et al. 1996, Arnljots et al. 1997).
In the labelling experiment, two strains of rats were used after a red blood cell-rollage had
formed on the intraluminal surface in BN/R1 rats. An immunological reaction was suspected
since the Indium 111-labelled platelets were obtained from animals with an unknown blood
group, and this could be especially undesirable in the HEP-PG group, which had a double
load of antigens (Indium 111-labelled platelets and HEP-PG itself). However, the amount of
platelet accumulation per vessel was on the same level in both rat species, and the results of
the two strains were combined.
Both the semiquantitative SEM analysis and quantification with Indium 111-labelled platelets
showed that the thrombotic response was lowest in the HEP-PG group, thus markedly
differing from the control group. As previously stated, the initial monolayer of platelets on
endothelial defects is essential in vascular repair as it forms a non-thrombogenic pseudo-
intima that is less attractive to additional platelet accumulation (Nightingale et al. 1980, Yo-
dong et al. 1989, Johnson 1990). Consistent with this finding, most of the HEP-PG-treated
vessels studied by SEM, revealed only a thin seal of platelets on the injured area.
Unfractionated heparin in a concentration of 100 U/ml, as used in the present study, has
previously had some local efficacy experimentally, but higher concentrations have led to
systemic effects and bleeding (Cox et al. 1992). In our experimental study, no increase in
anastomotic bleeding was noted with HEP-PG, in contrast to the result with recently
described locally used agent, FFR-rFVIIa (Sørensen et al. 1999). Even in a concentration 100
times smaller than that of unfractionated heparin HEP-PG were found to be very effective at
hindering the growth of thrombi and keeping them mural. HEP-PG, by having a strongly
retaining bond to extracellular matrix, seem to have potential as a locally active
antithrombotic agent in arterial circulation. However, further studies are needed to establish
whether HEP-PG can be used to prevent thombotic events in human circulation as well.
78
7. CONCLUSIONS
1. In clinical microsurgery, a preoperative hypercoagulable state was found by using markers
of coagulation activation (TAT, F1+2 and D-dimer) in half of the patients in each of the
following study groups: TRAM patients with an intraoperative thrombotic event, patients with
lower extremity trauma and patients with active cancer. The specific markers of thrombin
generation, TAT and F1+2, also associated with threatening flap failure, and they could
possibly be used for the perioperative evaluation of patients needing more intense
antithrombotic therapy in order to avoid reoperations when more rapid analyses become
available.
2. The effect of systemic anticoagulation with LMWH, dalteparin, as measured by anti-factor
Xa levels, turned out to be incomplete in all patients who had received it the previous
evening. Anticoagulation therapy must be enhanced in patients in a preoperative
hypercoagulable state, especially in those with recent trauma or active cancer. Further studies
will show the advantages and disadvantages of higher doses of LWMH, where possible
hemorrhagic complications can be reduced by assessing the systemic bleeding risk
preoperatively.
3. Immunohistochemical analysis of failed human anastomoses showed a lack of endothelial
cells with colocalised recruitment of platelets and fibrin. Of interest was the new finding that
PECAM-1 staining was absent in the single adherent layers of platelets, but that staining was
positive in micro and larger thrombi. Inflammation was prominent in vessels collected at
reoperations. Although technical failures were rare, refined microsurgical techniques remain
essential in order to diminish thrombotic stimuli.
4. The newly applied, locally active antithrombotic agent, macromolecular HEP-PG, was
effective in hindering thrombus growth in the anastomoses of common femoral arteries in rats
acutely (10 min) and in the long-term (3 days) as compared with saline, whereas
unfractionated heparin in a 100-fold higher concentration failed to markedly reduce the
thrombotic response. This was evidenced by SEM analysis and quantified with Indium 111-
labelled platelets. The feasibility of applying HEP-PG to inhibit thrombosis under high shear
rate conditions prevailing during microsurgery and at a-v shunts warrants further studies.

79
8. ACKNOWLEDGEMENTS
These studies were carried out at the Department of Plastic Surgery, the IV Department of
Surgery and the Wihuri Research Institute. Professor Sirpa Asko-seljavaara, Chief of Plastic
Surgery, with her committed staff has created an outstanding microsurgical clinic that is
unique in Scandinavia. Thanks to her I had no difficulty collecting the blood and vessel
samples needed for the clinical part of this study. Professor Vesa Manninen and Professor
Petri Kovanen, the former and present heads of the Wihuri Research Institute, put excellent
research facilities at my disposal.
I owe my deepest gratitude to my supervisor, Docent Riitta Lassila, Head of the Thrombosis
Group at the Wihuri Research Institute, for her enthusiasm, knowledge, and research skills,
and for creating such an encouraging working atmosphere. During my short visits to Finland
she always made time for discussions despite her busy schedule at Meilahti Hospital or even
in the evenings at her home.
My warmest thanks go to Dr. Nils Svartling for his help in collecting the blood samples
during the microsurgical operations, which made it possible for me to participate more
intensively in the operations. Eeva-Liisa Miettinen kindly allowed us to use the laboratory
facilities during the pretreatment of the blood samples at Töölö Hospital. The technical
assistance of Ruusa Hälvä, Marja Lemponen, Tuula Järvenpää and Jaana Tuomikangas in
analysing the blood samples in both the clinical and experimental parts of these studies is
gratefully acknowledged. It was a priviledge to work with the plastic surgery team in the
operation theatre at Töölö Hospital. I am sincerely grateful to Docent Erkki Tukiainen as I
learned a lot from him during my stay in Finland and later when working together with him in
Sweden. I also want to thank Sorella, Petteri, Markus and Laura for their advise and help at
Wihuri Research Institute.
Dr. Maarit Sarlomo-Rikala and Assistant Professor Tom Böhling from the Department of
Pathology, Haartman Institute, deserve special thanks for their inspiring collaboration during
the immunohistochemical analysis of the vessel samples. The technical assistance of Leena
80
Vantunen and Tuula Nousiainen in performing the immunohistochemical staining is
greatfully appreciated.
I am grateful for the constructive criticism and advice of Docent Disa Lidman and Docent Jari
Petäjä during the review of the manuscript. My sincere thanks are also due to Gillian Häkli
for revising the English of this thesis.
My dear friends Virpi and Anne were always there if I needed to sleep over a night or two in
Helsinki or in Turku during my visits to Finland. Mikko and Jyrki kindly helped me to solve
mathematical and information technological problems.
I express my deepest thanks to my family: to my husband, Jan Arne, whose invaluable
expertise in information technology made this thesis possible, to my daughter, Annnika,
whose love enlightened my heart even during the darkest days, and to my parents and parents-
in-law, without whose help with baby-sitting, house-keeping and animal care this work would
have been unthinkable.
These studies were financially supported by the Aarne Koskelo Foundation, the
Instrumentarium Foundation, Helsinki University Central Hospital, Finland, and FoU-Forum,
Landstinget Gävleborg, Sweden. My chance to work at Kosmetisk Kirurgi AB, Sweden, made
it possible for me to dedicate weeks and months solely to the writing of this thesis.
Helsinki, October 2001
Eija Olsson
81
9. REFERENCES
Acland R. Thrombus formation in microvascular surgery: an experimental study of the effects of surgical trauma. Surgery 1973; 73: 766-771. Acland RD, Trachtenberg L. The histopathology of small arteries following experimental microvascular anastomosis. Plast Reconstr Surg 1977; 60: 868-875. Acland RD, Lubbers LL, Grafton RB, Bensimon R. Irrigating solutions for small blood vessel surgery - a histologic comparison. Plast Reconstr Surg 1980; 65: 460-465. Adams JG, Dhar A, Shukla SD, Silver D. Effect of pentoxifylline on tissue injury and platelet-activating factor production during ischemia-reperfusion injury. J Vasc Surg 1995; 21: 742-749. Antithrombotic Trialists’ (ATT) Collaboration. Prevention of death, myocardial infarction and stroke by antiplatelet therapy: collaborative meta-analysis of 266 trials involving 200,000 patients at high risk of occlusive vascular events. BMJ 2001 (in press). Atchabahian A, Masquelet AC. Experimental prevention of free flap thrombosis. I: a model of free flap failure. Microsurgery 1996; 17: 710-713. Amelsberg A, Zurborn K-H, Gärtner U, Kiehne KH, Preusse A-K, Bruhn HD. Influence of heparin treatment on biochemical markers of an activation of the coagulation system. Thromb Res 1992; 66: 121-131. Andresen DM, O´Shaughnessy M, Ackland RD, Anderson GL, Schuscke D, Banis J Jr, Barker JH. Direct visualization and measurement of microsurgically induced thromboembolism. Microsurgery 1994; 15: 413-420. Arfors K-E, Dhall DP, Engeset J, Hint H, Matheson NA, Tangen O. Biolaser endothelial trauma as a means of quantifying platelet activity in vivo. Nature 1968; 218: 887-888. Arnljots B, Dougan P, Salemark L, Bergqvist D. Effects of streptokinase and urokinase on microarterial thrombosis and haemostasis. Scand J Plast Reconstr Hand Surg 1994; 28: 9-13. Arnljots B, Bergqvist D. Inhibition of heparin-resistant microarterial thrombosis by recombinant hirudun: a spacific thrombin inhibitor. Plast Reconstr Surg 1995; 95: 894-900. Arnljots B, Ezban M, Hedner U. Prevention of experimental arterial thrombosis by topical administration of active site-inactivated factor VIIa. J Vasc Surg 1997; 25: 341-346. Arnljots B, Dougan P, Bergqvist D. Antithrombotic and platelet activating effects of heparin in prevention of microarterial thrombosis. Plast Reconstr Surg 1997; 99: 1122-1128. Asko-Seljavaara S. Delayed breast reconstruction. Clin Plast Surg 1998; 25:157-166. Bajzar L, Manuel R, Nesheim ME. Purification and characterization of TAFI, a thrombin-
82
activable fibrinolysis inhibitor. J Biol Chem 1995; 270: 14477-14484. Barker JH, Acland RD, Anderson GL, Patel J. Microcirculatory disturbances following the passage of emboli in an experimental free-flap model. Plast Reconstr Surg 1992; 90: 95-102. Barker JH, Andresen DM, Anderson GL, Schuschke D, Gu J-M, Gupta S, Hjortdal VE, Derr JW Jr, Banis JC Jr, Acland RD. Can varying flow velocity across an arterial anastomosis prevent thromboembolic injury? Microsurgery 1995; 16: 349-356. Bassiouny HS, Song RH, Kocharyan H, Kins E, Glagov S. Low flow enhances platelet activation after acute experimental arterial imjury. J Vasc Surg 1998; 27: 910-918. Batlle J, del Rio F, López Fernández MF, Martin R, López Borrasca A. Effect of dextran on factor VIII/von Willebrand factor structure and function. Thromb Haemost 1985; 54: 697-699. Baxter TJ, O’Brien BMcC, Henderson PN, Bennett RC. The histopathology of small vessels following microvascular repair. Br J Surg 1972; 59: 617-622. Bennett B, Towler HMA. Haemostatic responce to trauma. Br Med Bull 1985; 41: 274-280. Bergqvist D, Hedner U, Sjörin E, Holmer E. Anticoagulant effects of two types of low molecular weight heparin administered subcutaneously. Tromb Res 1983; 32: 381-391. Bergqvist D, Burmark US, Flordal PA, Frisell J, Hallböök T, Hedberg M, Horn A, Kelty E, Kvitting P, Lindhagen A, Ljungström KG, Mätzsch T, Risberg B, Syk I, Törngren S, Wellander E, Örtenwall P. Low molecular weight heparin started before surgery as prophylaxis against deep vein thrombosis: 2500 versus 5000 XaI units in 2700 patients. Br J Surg 1995; 82: 496-501. Bergqvit D. Low molecular weight heparins. J Intern Med 1996; 240: 63-72. Bini A, Fenoglio JJ Jr, Mesa-Tejada R, Kudryk B, Kaplan KL. Identification and distribution of fibrinogen, fibrin, and fibrin(ogen) degradation products in atherosclerosis. Use of monoclonal antibodies. Arteriosclerosis 1989; 9: 109-121. Boeckx WD, Vijay Haribhakti VV, Bosmans L. Scanning electron microscopic study of thrombus formation in an end-to-side anastomosis of the rat carotid artery. J Reconstr Microsurg 1994; 10: 35-38. von Boguslawsky K. Immunohistochemical detection of progesterone receptors in paraffin sections. APMIS 1994, 102: 641-646. Bona RD. Thrombotic complications of central venous catheters in cancer patients. Semin Thromb Hemost 1999; 25: 147-155. Boneu B, Bes G, Pelzer H, Sié P, Boccalon H. D-dimers, thrombin antithrombin III complexes and prothrombin fragments 1+2: diagnostic value in clinically suspected deep vein thrombosis. Thromb Haemost 1991; 65: 28-32.
83
Brophy CM, Woodrum D, Dickinson M, Beall A. Thrombin activates MAPKAP2 kinase in vascular smooth muscle. J Vasc Surg 1998; 27: 963-969. Brown DM, Kania N, Lantieri LA, Pasia EN, Khouri RK. Effect of phosphate concentration in buffered irrigating solutions on arterial thrombosis. Microsurgery 1995; 16: 757-759. Broze GJ Jr. Tissue factor pathway inhibitor. Thromb Haemost 1995; 74: 90-93. Brozovic M. Physiological mechanisms in coagulation and fibrinolysis. Br Med Bull 1977; 33: 231-238. Buckley RC, Davidson SF, Das SK. The role of various antithrombotic agents in microvascular surgery. Br J Plast Surg 1994; 47: 20-23. Carroll VA, Binder BR. The role of the plasminogen activation system in cancer. Semin Thromb Hemost 1999; 25: 183-197. Catalfamo JL, Dodds WJ. Isolation of platelets from laboratory animals. In: Hawiger J ed. Methods in Enzymology. San Diego, Academic Press, Inc., 1989. Pp. 27-34. ten Cate JW, van der Poll T, Levi M, ten Cate H, van Deventer SJH. Cytokines: triggers of clinical thrombotic disease. Thromb Haemost 1997; 78: 415-419. Chen L-E, Seaber AV, Korompiliasis AV, Urbaniak JR. Effects of enoxaparin, standard heparin, and streptokinase on the patency of anastomoses in severely crushed arteries. Microsurgery 1995; 16: 661-665. Chen L-E, Seaber AV, Urbaniak JR. Thrombosis and thrombolysis in crushed arteries with or without anastomosis: a new microvascular thrombosis model. J Reconstr Microsurg 1996; 12: 31-38. Chen JP, Rowe DW, Enderson BL. Contrasting post-traumatic serial changes for D-dimer and PAI-1 in critically injured patients. Thromb Res 1999; 94: 175-185. Colman RW, Marder VJ, Salzman EW, Hirsh J. Overview of hemostasis. In: Colman RW, Hirsh J, Marder VJ, Salzman EW eds. Hemostasis and thrombosis: basic principles and clinical practice, 3rd ed. Philadelphia, JB Lippincott Company, 1994. Pp. 3-18. Cooley B, Gould J. Topically applied antithrombotic agents offer a new therapeutic approach to the prevention of microvascular thrombosis. Microsurgery 1991; 12: 281-287. Cooley BC, Ruas EJ, Shaw Wilgis EF. Scanning electron microscopy of crush/avulsion arterial trauma: effect of heparin and aspirin administration. Microsurgery 1987; 8: 11-16. Cox GW, Runnels S, Hsu HS-H, Das SK. A comparison of heparinised saline irrigation solutions in a model of microvascular thrombosis. Br J Plast Surg 1992; 45: 345-348. Dahlbäck B. Blood coagulation. Lancet 2000; 355: 1627-1632. D’Angelo A, Kluft C, Verheijen JH, Rijken DC, Mozzi E, Mannucci PM. Fibrinolytic shut-
84
down after surgery: impairment of the balance between tissue-type plasminogen activator and its spesific inhibitor. Eur J Clin Invest 1985; 15: 308-312. Das S, Miller J. Current status of topical antithrombotic agents in microvascular surgery. Microsurgery 1994; 15: 630-632. Dawes J. Interactions of heparins in the vascular environment. Haemostasis 1993; 23(suppl 1): 212-219. Davidson SF, Brantley SK, Talbot PJ, Das SK. A functional model of microvascular thrombosis. Plast Reconstr Surg 1990; 86: 579-581. Davies D. A world survey of anticoagulation practice in clinical microvascular surgery. Br J Plast Surg 1982; 35: 96-99. Derlerck PJ, Mombaerts B, Holvoet P, De Mol M, Collen D. Fibrinolytic response and fibrin fragment D-dimer levels in patients with deep vein thrombosis. Thromb Haemost 1987 58: 1024-1029. Deutinger M, Rath T, Constantinou E, Schneider B. The influence of postoperative medical treatment and type of microvascular anastomosis on free tissue transfer. Eur J Plast Surg 1998; 21: 273-276. Donati MB. Cancer and thrombosis: from phlegmasia albo dolens to transgenic mice. Thromb Haemost 1995; 74: 278-281. Donati MB. Pathogenesis of thrombosis in cancer. Vessels 1996; 2: 4-8. Downing LJ, Wakefield TW, Strieter RM, Prince MR, Londy FJ, Fowlkes JB, Hulin MS, Kadell AM, Wilke CA, Brown SL, Wrobleski SK, Burdick MD, Anderson DC, Greenfield LJ. Anti-P-selectin antibody decreases inflammation and thrombus formation in venous thrombosis. J Vasc Surg 1997; 25: 816-828. Downing LJ, Strieter RM, Kadell AM, Wilke CA, Greenfield LJ, Wakefield TW. Low-dose low-molecular-weight heparin is anti-inflammatory during venous thrombosis. J Vasc Surg 1998; 28: 848-854. Dujovny M, Wakenhut N, Kossovsky N, Gomes CW, Laha RK, Leff L, Nelson D. Minimum vascular occlusive force. J Neurosurg 1979; 51: 662-668. Eagle H, Harris TN. Studies on blood coagulation: V. The coagulation of blood by proteolytic enzymes (trypsin, papain). J Gen Physiol 1937; 20: 543-560. Egli GA, Zollinger A, Seifert B, Popovic D, Pasch T, Spahn DR. Effect of progressive haemodilution with hydroxyethyl starch, gelatin and albumin on blood coagulation. Br J Anaesth 1997; 78: 684-689. Ehrlich J, Stivala SS. Chemistry and pharmacology of heparin. J Pharm Sci 1973; 62: 517-544.

85
Engelberg H. Actions of heparin in the atherosclerotic process. Pharm Rev 1996; 48: 327-352. Enoxan Study group. Efficacy and safety of enoxaparin versus unfractionated heparin for prevention of deep vein thrombosis in elective cancer surgery: a double-blind randomised multicentre trial with venographic assessment. Br J Surg 1997; 84: 1099-1103. Ernofsson M, Strekerud F, Toss H, Abildgaard U, Wallentin L, Siegbahn A. Low-molecular weight heparin reduces the generation and activity of thrombin in unstable coronary artery disease. Thromb Haemost 1998; 79: 491-494. Falanga A, Barbui T, Rickles FR, Levine MN. Guidelines for clotting studies in cancer patients. Thromb Haemost 1993; 70: 540-542. Falanga A, Ofosu FA, Cortelazzo S, Delaini F, Consonni R, Caccia R, Longatti S, Maran D, Rodeghiero F, Pogliani E, Marassi A, D’Angelo A, Barbui T. Preliminary study to identify cancer patients at high risk of venous thrombosis following major surgery. Br J Haematol 1993; 85: 745-750. Falanga A, Rickles FR. Pathophysiology of the thrombophilic state in the cancer patient. Semin Thromb Hemost 1999; 25: 173-182. Fernández JA, Petäjä J, Gruber A, Griffin JH. Activated protein C correlates inversely with thrombin levels in resting healthy individuals. Am J Hematol 1997; 56: 29-31. Folts JD, Crowell EB, Rowe GG. Platelet aggregation in partially obstructed vessels and its elimination with aspirin. Circulation 1976; 54: 365-370. Friedman M, Byers SO. Employment of polyethylene tubing for production of intra-arterial thrombi in rabbits and rats. Proc Soc Exp Biol Med 1961; 106: 796-799. Fujii Y, Tanaka R, Takeuchi S, Koike T, Minakawa T, Sasaki O. Serial changes in hemostasis after intracranial surgery. Neurosurgery 1994; 35: 26-33. Fu K, Izquierdo R, Hubbard T, Fareed J. Modified crush-avulsion anastomosis model on the rat femoral vein. Microsurgery 1995; 16: 536-541. Fukui A, Maeda M, Sempuku T, Tamai S, Mizumoto S, Inada Y. Continuous local intraarterial infusion of anticoagulants for digit replantation and treatment of damaged arteries. J Rec Microsurg 1989; 5: 127-136. Gachet C. Platelet activation by ADP: the role of ADP antagonists. Ann Med 2000; 32 Suppl 1: 15-20. Garcia-Avello A, Lorente JA, Cesar-Perez J, Garcia-Frade LJ, Alvarado R, Arévalo JM, Navarro JL, Esteban A. Degree of hypercoagulability and hyperfibrinolysis is related to organ failure and prognosis after burn trauma. Thromb Res 1998; 89: 59-64. Goldberg JA, Pederson WC, Barwick WJ. Salvage of free tissue transfers using thrombolytic agents. J Rec Microsurg 1989; 5: 351-356.
86
Gondret R, Dominici L, Angelard B, Dubos S, Al-Rawi S, Huet Y, Clerque F, Saint-Guily JL. Safety of preoperative enoxaparin in head and neck cancer surgery. Head&Neck Surgery 1995; 17: 1-6. Gouin-Thibault I, Samama MM. Laboratory diagnosis of the thrombophilic state in cancer patients. Semin Thromb Hemost 1999; 25:167-172. Gu Y-d, Zhang L-y, Zhang L, Sung Q-l, Sun L-x. Vessel pathology and its clinical significance in toe transfer. J Reconstr Microsurg 1992; 8: 363-370. Hafner G, Schinzel H, Ehrenthal W, Wagner C, Konheiser U, Zotz R, Lotz J, Blank R, Weilemann LS, Prellwitz W. Influence of blood sampling from venipunctures and catheter systems on serial determinations of prothrombin activation fragment 1+2 and thrombin-antithrombin III complex. Ann Hematol 1993; 67: 121-125. Hansen J-B, Sandset PM. Differential effects of low molecular weight heparin and unfractionated heparin on circulating levels of antithrombin and tissue factor pathway inhibitor (TFPI): a possible mechanism for difference in therapeutic efficacy. Thromb Res 1998; 91: 177-181. Harashina T. Analysis of 200 free flaps. Br J Plast Surg 1988; 41: 33-36. Hashim HA, Atiyeh BS, Hamdan AM, Musharrafieh RS. Local intravenous thrombolysis with recombinant tissue plasminogen activator for salvage of forearm replantation. J Rec Microsurg 1996; 12: 543-546. Hiebert LM, Jaques LB. The observation of heparin on endothelium. Thromb Res 1976; 8: 195-204. Hirsh J, Warkentin TE, Raschke R, Granger C, Ohman EM, Dalen JE. Heparin and low-molecular-weight heparin. Mechanisms of action, pharmacokinetics, dosing considerations, monitoring, and safety. Chest 1998; 114: 489S-510S. Hirsh J, Weitz JI. New antithrombotic agents. Lancet 1999; 353: 1431-36. Hirsh J, Anand SS, Halperin JL, Fuster V. Guide to anticoagulant therapy: heparin. Circulation 2001; 103: 2994-3018. Hoffman R. The thrombo-embolic risk in surgery. Hepatogastroenterology 1991; 38: 272-279. Holmberg A, Bergqvist D, Siegbahn A. Coagulation and fibrinolysis after open infrarenal abdominal aortic aneurysm repair in a long-term perspective. Thromb Res 1999; 96: 99-105. Holmberg A, Siegbahn A, Westman B, Bergqvist D. Ischaemia and reperfusion during open abdominal aortic aneurysm surgery induce extensive thrombin generation and activity. Eur J Vasc Endovasc Surg 1999; 18: 11-16. Hsu S-M, Raine L, Fanger H: Use of avidin-biotin-peroxidase complex (ABC) in immunoperoxidase techniques: a comparison between ABC and unlabeled antibody (PAP)
87
procedures. J Histochem Cytochem 1981, 29: 577-580. Illig KA, Green RM, Ouriel K, Riggs, PN, Bartos S, Whorf R, DeWeese JA, Chhibber A, Marder VJ, Francis CW. Primary fibrinolysis during supraceliac aortic clamping. J Vasc Surg 1997; 25: 244-254. Iversen LH. Pre-analytical variation in the measurements of sensitive markers of coagulation and fibrinolysis: the influence of venipuncture and mixing of blood. Haemostasis 1997; 27: 119-124. Jackiewicz TA, McGeachie JK, Tennant M. Structural recovery of small arteries following clamp injury: a light and electron microscopic investigation in the rat. Microsurgery 1996; 17: 674-680. Jeske W, Fareed J. Antithrombin III- and heparin cofactor II-mediated anticoagulant and antiprotease actions of heparin and its synthetic analogues. Semin Thromb Hemost 1993; 19: 241-247. Johnson PC. Platelet-mediated thrombosis in microvascular surgery: New knowledge and strategies. Plast Reconstr Surg 1990; 86: 359-367. Johnson PC, Barker JH. Thrombosis and antithrombotic therapy in microvascular surgery. Clin Plast Surg 1992; 19: 799-807. Johnson PC, Dickson CS, Garrett KO, Sheppeck RA, Bentz ML. The effect of microvascular anastomosis configuration on initial platelet deposition. Plast Reconstr Surg 1993; 91:522-527. Johnson AJ, Tillett WS. The lysis in rabbits of intravascular blood clots by the streptococcal fibrinolytic system (streptokinase). J Exp Med 1952; 95: 449-463. Kalweit GA, Feindt P, Micek M, Gams E, Hellstern P. Markers of activated hemostasis and fibrinolysis in patients with pulmonary malignancies: comparison of plasma levels in central venous and pulmonary venous blood. Thromb Res 2000; 97: 105-111. Karpatkin S; Nierodzik ML, Klepfish A. Role of platelets and thrombin in cancer. Vessels 1996; 2: 17-30. Kashyap MVS, Reil TD, Moore WS, Hoang TX, Gelabert HA, Byrns RE, Ignarro LJ, Freischlag JA. Acute arterial thrombosis causes endothelial dysfunction: a new paradigm for thrombolytic therapy. J Vasc Surg 2001; 34: 323-329. Kauhanen P, Kovanen PT, Reunala T, Lassila R. Effects of skin mast cells on bleeding time and coagulation activation at the site of platelet plug formation. Thromb Haemost 1998; 79: 843-847. Kauhanen P, Kovanen PT, Lassila R. Coimmobilised native macromolecular heparin proteoglycans strongly inhibit platelet-collagen interactions in flowing blood. Arterioscler Thromb Vasc Biol 2000; 20: e113-e119.
88
Kaviani A, Organ CH Jr. Clotting and cancer: Trousseau´s warning. J Am Coll Surg 1999; 189: 504-507. Kehrel B. Platelet-collagen interactions. Semin Thromb Hemost 1995; 21: 123-129. Kersch RA, Handren J, Hergrueter C, May JW Jr. Microvascular surgical experimental thrombosis model: rationale and design. Plast Reconstr Surg 1989; 83: 866-872. Khouri RK, Cooley BC, Kenna DM, Edstrom LE. Thrombosis of microvascular anastomoses in traumatized vessels: fibrin versus platelets. Plast Reconstr Surg 1990; 86: 110-117. Khouri RK. Avoiding free flap failure. Clin Plast Surg 1992; 19: 773-781. Khouri RK, Sherman R, Buncke HJ Jr, Feller A-M, Hovius S, Benes CO, Ingram DM, Natarajan NN, Sherman JW, Yeramian PD, Cooley BC. A phase II trial of intraluminal irrigation with recombinant human tissue factor pathway inhibitor to prevent thrombosis in free flap surgery. Plast Reconstr Surg 2001; 107: 408-415. Kikuchi S, Umemura K, Kondo K, Saniabadi AR, Nakashima M. Photochemically induced endothelial injury in the mouse as a screening model for inhibitors of vascular intimal thickening. Arterioscler Thromb Vasc Biol 1998; 18: 1069-1078. Kluft C, Verheijen JH, Jie AFH, Rijken DC, Preston FE, Sue-Ling HM, Jespersen J, Aasen AO. The post-operative fibrinolytic shutdown: a rapidly reverting acute phase pattern for the fast acting inhibitor of tissue-type plasminogen activator after trauma. Scand J Clin Lab Invest 1985; 45: 605-610. Kluft C, Verheijen JH. Leiden fibrinolysis working party: blood collection and handling procedures for assessment of tissue-type plasminogen activator (t-PA) and plasminogen activator inhibitor-1 (PAI-1). Fibrinolysis 1990; 4 (suppl 2): 155-161. Komuro Y, Sekiguchi J, Nomura S, Ohmori K, Takasugi Y, Arai C. Blood coagulation activity during microsurgery. Ann Plast Surg 1998; 40: 53-58. Kroll SS, Miller MJ, Reece GP, Baldwin BJ, Robb GL, Bengtson BP, Phillips MD, Kim D, Schusterman MA. Anticoagulants and hematomas in free flap surgery. Plast Reconstr Surg 1995; 96: 643-647. Kronen G, Ferder M, Hunzicker K, Strauch B. The use of pentoxifylline in microvascular surgery. J Rec Microsurg 1994; 10: 17-20. Kudrjashov B, Kalishevskaya T, Kolomina S. Blood anticoagulating system and malignant tumours. Nature 1969; 222: 548-550. Kwaan HC, Barlow GH. Nature and biological activities of degradation products of fibrinogen and fibrin. Ann Rev Med 1973; 24: 335-344. Lan M, lu Li X, Cooley BC, Gould JS. Microvascular Salvage procedures with adjuvant antithrombotic therapy for restitution of patency in a rat model. J Reconstr Microsurg 1992; 8: 201-205.
89
Lanzetta M, Owen ER. Scanning electron microscopy evaluation of endothelial regeneration in 1-mm PTFE prostheses. J Reconstr Microsurg 1996; 2: 47-53. Lassila R, Badimon JJ, Vallabhajosula S, Badimon L. Dynamic monitoring of platelet deposition on severely damaged vessel wall in flowing blood. Arteriosclerosis 1990; 10: 306-315. Lassila R, Lindstedt K, Kovanen PT. Native macromolecular heparin proteoglycans exocytosed from stimulated rat serosal mast cells strongly inhibit platelet-collagen interactions. Arterioscler Thromb Vasc Biol 1997; 17: 3578-3587. Lee AYY, Levine MN. The thrombophilic state induced by therapeutic agents in the cancer patient. Semin Thromb Hemost 1999; 25: 137-145. Leppänen O, Janjic N, Carlsson M-A, Pietras K, Levin M, Vargeese C, Green LS, Bergqvist D, Östman A, Heldin C-H. Intimal hyperplasia recurs after removal of PDGF-AB and –BB inhibition in the rat carotid artery injury model. Thromb Vasc Biol 2000; 20: e89-e95. Levy EA, Sadove AM, Eppley BL, Evan AP. A comparison of human recombinant tissue-type plasminogen activator and urokinase in microsurgical thrombolysis in the rat. J Reconstr Microsurg 1991; 7: 209-216. Lidman D, Daniel RK. Evaluation of clinical microvascular anastomoses - reasons for failure. Ann Plast Surg 1981; 6: 215-223. Lidman D, Daniel RK. The normal healing process of microvascular anastomoses. Scand J Plast Reconstr Surg 1981; 15: 103-110. Lidman D, Lyczakowski T, Daniel RK. The morphology and patency of arterial and venous microvascular anastomoses throughout the first post-operative year. Scand J Plast Reconstr Surg 1984; 18: 187-192. Lijnen HR, Collen D. Mechanisms of physiological fibrinolysis. Baillieres Clin Haematol 1995; 8:277-290. Lindstedt KA, Kokkonen JO, Kovanen PT. Soluble heparin proteoglycans released from stimulated mast cells induce uptake of low density lipoproteins by macrophages via scavanger receptor-mediated phagocytosis. J Lipid Res 1992; 33: 65-75. De Lisser HM, Yan HC, Newman PJ, Muller WA, Buck CA, Albelda SM. Platelet/endothelial cell adhesion molecule-1 (CD 31) – mediated cellular aggregation involves cell surface glycosaminoglycans. J Biol Chem 1993; 268: 16037-16046. Ljungström K-G. The anti-thrombotic efficacy of dextran. Acta Chir Scand Suppl 1988, 543: 26-30. López Y, Paloma MJ, Rifón J, Cuesta B, Páramo JA. Measurement of prethrombotic markers in the assessment of acquired hypercoagulable states. Thromb Res 1999; 93: 71-78.
90
Lorenzetti F, Suominen S, Tukiainen E, Kuokkanen H, Suominen E, Vuola J, Asko-Seljavaara S. Evaluation of blood flow in free microvascular flaps. J Reconstr Microsurg 2001; 17: 163-167. Luk KDK, Zhou LR, Chow SP. The effect of established infection on microvascular surgery. Plast Reconstr Surg 1987; 80: 423-427. Lykoudis EG, Panayotou PN, Stamatopoulos CN, Frangia KB, Papalois AE, Ioannovich JD. Microvascular repair following a modified crush-avulsion injury in a rat model: effect of recombinant human tissue-type plasminogen activator on the patency rate. Microsurgery 2000; 20: 52-58. Maeda M, Fukui A, Inada Y, Tamai S, Mizumoto S. Continuous local intraarterial infusion of antithrombotic agents for epigastric flap transfer in rabbit. J Rec Microsurg 1990; 6: 261-266. Makhoul RG, Fields CE, Cassano AD. Nitric oxide and the vascular surgeon. J Vasc Surg 1999; 30: 569-572. Maraganore JM. Thrombin, thrombin inhibitors, and the arterial thrombotic process. Thromb Haemost 1993; 70: 208-211. May JW Jr, Rothkopf DM. Salvage of a failing microvascular free muscle flap by direct continuous intravascular infusion of heparin: a case report. Plast Reconstr Surg 1989; 83: 1045-1048. Meissner MH, Zierler BK, Bergelin RO, Chandler WC, Manzo RA, Strandness DE Jr. Markers of plasma coagulation and fibrinolysis after acute deep venous thrombosis. J Vasc Surg 2000; 32: 870-880.
Merlini PA, Bauer KA, Oltrona L, Ardissino D, Cattaneo M, Belli C, Mannucci PM, Rosenberg RD. Persistent activation of coagulation mechanism in unstable angina and myocardial infarction. Circulation 1994; 90: 61-68. Merlini PA, Bauer KA, Mannucci PM. Laboratory detection of the prethrombotic state. In: Verstraete, V Fuster, Topol EJ eds. Cardiovascular thrombosis: thrombocardiology and thromboneurology, 2nd ed. Philadelphia, Lippincott-Raven Publishers, 1998. Pp. 103-118. Moor E, Blombäck M, Silveira A, Wiman B, Cederlund K, Bergstrand L, Ivert T, Rýden L, Hamsten A. Haemostatic function in patients undergoing coronary artery bypass grafting: peroperative perturbations and relations to saphenous vein graft closure. Thromb Res 2000; 98: 39-49. Murray DWG, Jaques LB, Perret TS, Best CH. Heparin and vascular occlusion. Can Med Assoc J 1936; 621-622. Murray DJ, Olson J, Strauss R, Tinker JH. Coagulation changes during packed red cell replacement of major blood loss. Anesthesiology 1988; 69: 839-845. Nader HB, Walenga JM, Berkowitz SD, Ofosu F, Hoppensteadt DA, Cella G. Preclinical differentiation of low molecular weight heparins. Semin Thromb Hemost 1999; 25: 63-72.
91
Nichter LS, Bindiger A. Improving micrograft patency. Microsurgery 1988; 9: 235-241. Niemi TT, Kuitunen AH, Vahtera EM, Rosenberg PH. Haemostatic changes caused by i.v. regional anesthesia with lignocaine. Br J Anaesth 1996; 76: 822-828. Niemi T, Svartling N, Syrjälä M, Asko-Seljavaara S, Rosenberg P. Haemostatic disturbances in burned patients during early excision and skin grafting. Blood Coagul Fibrinol 1998; 9: 19-28. Nieminen T, Asko-Seljavaara, Suominen E, Kuokkanen H, von Smitten K. Free microvascular TRAM flaps: report of 185 breast reconstructions. Scand J Plast Reconstr Hand Surg 1999; 33: 295-300. Nievelstein P, de Groot PH: Interaction of blood platelets with the vessel wall. Haemostasis 1988; 18: 342-359. Nightingale G, Fogdestam I, O´Brien BMcC. Scanning electron microscope study of experimental microvascular anastomoses in the rabbit. Br J Plast Surg 1980; 33: 283-298. Ozbek MR, Deune EG, Cooley BC, Khouri RK. Experimental reproduction of free flap errors: a new model of thrombosis. Ann Plast Surg 1994; 32: 474-477. Ozbek MR, Brown DM, Deune EG, Lantieri LA, Kania NM, Pasia EN, Cooley BC, Wun T-C, Khouri RK. Topical tissue factor pathway inhibitor improves free-flap survival in a model simulating free-flap errors. J Reconstr Microsurg 1995; 11: 185-188. Peetz D, Hafner G, Hansen M, Mayer A, Rippin G, Rommens PM, Prellwitz W. Dose-adjusted thrombosis prophylaxis in trauma surgery according to levels of D-dimer. Thromb Res 2000; 98: 473-483. Peltonen S, Lassila R, Rossi P, Salenius J-P, Lepäntalo M. Blood coagulation and fibrinolysis activation during sudden arterial occlusion of lower extremities - an association with ischemia and patient outcome. Thromb Haemost 1995; 74: 1442-1446. Peltonen S, Lassila R, Lepäntalo M. Increased circulating plasminogen activator inhibitor-1 in patients with patent femorodistal venous bypass. Thromb Res 1996; 82: 369-377. Peltonen S, Lassila R, Heikkilä J. Activation of coagulation and fibrinolysis despite heparinization during successful elective coronary angioplasty. Thromb Res 1996; 82: 459-468. Peltonen S, Juvela S, Kaste M, Lassila R. Hemostasis and fibrinolysis activation after subarachnoid hemorrhage. J Neurosurg 1997; 87: 207-214. Pelzer H, Schwarz A, Heimburger N. Determination of human thrombin-antithrombin III complex in plasma with an enzyme-linked immunosorbent assay. Thromb Haemost 1988; 59: 101-106. Pelzer H, Schwarz A, Stüber W. Determination of human prothrombin activation fragment
92
1+2 in plasma with an antibody against the synthetic peptide. Thromb Haemost 1991; 65: 153-159. Percival NJ, Sykes PJ, Earley MJ. Free flap surgery: the Welsh regional unit experience. Br J Plast Surg 1989; 42: 435-440. Petäjä J, Myllynen P, Myllylä G, Vahtera E. Fibrinolysis after application of a pneumatic tourniquet. Acta Chir Scand 1987; 153: 647-651. Petäjä J, Peltola K, Sairanen H, Leijala M, Kekomäki R, Vahtera E, Siimes MA. Fibrinolysis, antithrombin III, and protein C in neonates during cardiac operations. J Thorac Cardiovasc Surg 1996; 112: 665-671. Prandoni P. Heparins and venous thromboembolism: current practice and future directions. Thromb Haemost 2001; 86: 488-498. Rahr HB, Fabrin K, Larsen JF, Throlacius-Ussing O. Coagulation and fibrinolysis during laparoscopic cholecystectomy. Thromb Res 1999; 93: 121-127. Reber K. A device for the production of well-defined lesions of mesenteric blood vessels with resulting platelet thrombi. Thromb Diath Haemorrh 1966; 15: 471-475. Reichel CA, Croll GH, Puckett CL. A comparison of irrigation solutions for microanastomoses. Am J Handsurg 1988; 13: 33-36. Reidy MA. Neointimal proliferation: the role of basic FGF on vascular smooth muscle cell proliferation. Thromb Haemost 1993; 70: 172-176. Rickles FR, Levine M, Edwards RL. Hemostatic alterations in cancer patients. Cancer and Metastasis Reviews. 1992; 11:237-248. Rieck B, Mailänder P, Machens HG. Vascular complications after free tissue transfer. Microsurgery 1995; 16: 400-403. Rooks MD, Rodriquez J, McNaughton M, Turnidge K, Zusmanis K, Hutton W. Refinement of the rat crush-avulsion femoral artery injury model. Microsurgery 1993; 14: 130-134. Rooks MD, Rodriguetz J Jr, Blechner M, Zusmanis K, Hutton W. Comparative study of intraarterial and intravenous anticoagulants in microvascular anastomoses. Microsurgery 1994; 15:123-129. Rosenbaum TJ, Sundt TM. Thrombus formation and endothelial alterations in microarterial anastomoses. J Neurosurg 1977; 47: 430-441. Ruggeri ZM, Ware J. von Willebrand factor. FASEB J 1993; 7: 308-316. Ruggeri ZM. Mechanisms initiating platelet thrombus formation. Thromb Haemost 1997; 78: 611-616. Rånby M, Bergsdorf N, Nilsson T, Mellbring G, Winblad B, Bucht G. Age dependence of
93
tissue plasminogen activator concentrations in plasma, as studied by an improved enzyme-linked immunosorbent assay. Clin Chem 1986; 32: 2160-2165. Salemark L, Wieslander JB, Dougan P, Arnljots B. Adverse effects of topical prostacyclin application in microvascular surgery: an experimental study. J Reconstr Microsurg 1991; 7: 27-30. Salemark L. International survey of current microvascular practices in free tissue transfer and replantation surgery. Microsurgery 1991; 12: 308-311. Salemark L, Knudsen F, Dougan P. Effects of the prostacyclin analogue iloprost on patency in small arteries and veins: an experimental study in the rabbit. Microsurgery 1995; 16: 94-97. Salzman EW, Rosenberg RD, Smith MH, Lindon JN, Favreau L. Effect of heparin and heparin fractions on platelet aggregation. J Clin Invest 1980; 65: 64-73. Savoie FH, Cooley BC, Gould JS. Evaluation of the effect of pharmacologic agents on crush-avulsion arterial injuries: a scanning electron microscopy study. Microsurgery 1991; 12: 292-300. Schafer AI. The primary and secondary hypercoagulable states. In: Schafer I ed. Molecular mechanisms of hypercoagulable states. Georgetown, Landes Bioscience, 1997. Pp 1-47. Schmitt M, Harbeck N, Thomssen C, Wilhelm O, Magdolen V, Reuning U, Ulm K, Höfler H, Jänicke F, Graeff H. Clinical impact of the plasminogen activation system in tumor invasion and metastasis: prognostic relevance and target for therapy. Thromb Haemost 1997; 78: 285-296. Serra A, Esteve J, Reverter JC, Lozano M, Escolar G, Ordinas A. Differential effect of a low-molecular-weight heparin (dalteparin) and unfractionated heparin on platelet interaction with the subendothelium under flow conditions. Thromb Res 1997; 87: 405-410. O´Shaugnessy M, Gu J-M, Wyllie F, Ackland RD, Anderson GL, Banis JC Jr, Barker JH. Microcirculatory consequences of microvascular surgery. Microsurgery 1994; 15: 405-412. Shireman PK, Mc Carthy WJ, Pearce WH, Shively VP, Cipollone M, Kwaan HC. Elevations of tissue-type plasminogen activator and differential expression of urokinase-type plasminogen activator in diseased aorta. J Vasc Surg 1997; 25: 157-164. Siegel D. Use of anticoagulants in replantation and elective microsurgery. Microsurgery 1991; 12: 277-280. Sigurbjörnsson BTh, Hallberg E, Andrén-Sandberg Å, Ribbe E. Endothelialization of anastomoses in the aorta and inferior vena cava of the rat. Microsurgery 1994; 15: 787-794. Sinclair S. The importance of topical heparin in microvascular anastomoses: a study in the rat. Br J Plast Surg 1980; 33: 422-426. Solandt DY, Best CH. Heparin and coronary thrombosis in experimental animals. Lancet 1938; July 16: 130-132.
94
Stockmans F, Deckmyn H, Gruwez J, Vermylen J, Acland R. Continuous quantitative monitoring of mural, platelet-dependent, thrombus kinetics in the crushed rat femoral vein. Thromb Haemost 1991; 65: 425-431. Stone P. Lord JW Jr. An experimental study of the thrombogenic properties of magnesium and magnesium-aluminium wire in the dog´s aorta. Surgery 1951; 30: 987-993. Strauss RG, Stansfield C, Henriksen RA, Villhauer PJ. Pentastarch may cause fewer effects on coagulation than hetastarch. Transfusion 1988; 28: 257-260. Suominen S, Asko-Seljavaara S. Free flap failures. Microsurgery 1995; 16: 396-399. Syrjälä MT, Krusius T, Petäjä J, Vehtera E, Rasi V. Venous occlusion test: assessment of fibrinolytic capacity by D-dimer latex agglutination test. Fibrinolysis 1993; 7: 41-45. Szczeklik A, Dropinski J, Radwan J, Krzanowski M. Persistent generation of thrombin after acute myocardial infarction. Arterioscler Thromb 1992; 12: 548-553. Söderström T, Hedner U, Arnljots B. Active site-inactivated factor VIIa prevents thrombosis without increased surgical bleeding: topical and intravenous administration in a rat model of deep arterial injury. J Vasc Surg 2001; 33: 1072-1079. Sørensen HB, Kristensen AT, Ravn HB, Fuglsang J, Hjortdal VE. Local application of FFR-rFVIIa reduces thrombus formation at arterial anastomosis in rats. Microsurgery 1999; 19: 369-373. Takano K, Yamaguchi T, Uchida K. Markers of a hypercoagulable state following acute ischemic stroke. Stroke 1992; 23: 194-198. Tangelder GJ, oude Egbrink MGA, Slaaf DW, Reneman RS. Blood platelets: an overview. J Reconstr Microsurg 1989; 5: 167-171. von Tempelhoff G-F, Dietrich M, Niemann F, Schneider D, Hommel G, Heilman L. Blood coagulation and thrombosis in patients with ovarian malignancy. Thromb Haemost 1997; 77: 456-461. Theile RJW, Coombs CJ. Microvascular and thrombolytic revascularization of an arm in a 32-week-gestation neonate: case report and review of the literature. J Rec Microsurg 1996; 12: 539-542. Thomson JG, Kim JH, Seyd SA, Reid MA, Madsen J, Restifo RJ. The effect of prolonged clamping and vascular stasis on the patency of arterial and venous microanastomoses. Ann Plast Surg 1998; 40: 436-441. Tonken HP, Zhang F, Yim KK, Gencosmanoglu R, Sudekum AE, Campagna-Pinto D, Newlin L, Buncke HJ, Lineaweaver WC. Experimental microvenous thrombosis following anastomosis with a knotted suture. Microsurgery 1995; 16: 98-102. Turpie AGG. Clinical trials of low molecular weight heparins. Eur Heart J Supplements 1999;
95
1 (Suppl R: R18-R27). Wang Y, Kovanen P. Heparin proteoglycans released from rat serosal mast cells inhibit proliferation of rat aortic smooth muscle cells in culture. Circ Res 1999; 84: 74-83. Ware JA, Coller BS. Platelet morphology, biochemistry, and function. In: Beutler E, Lichtman MA, Coller BS, Kipps TJ eds. Williams Hematology, 5th ed. New York, McGraw-Hill, Inc., 1995. Pp 1161-1201. Warner ED, Brinkhous KM, Seegers WH, Smith HP. Further experience with the use of thrombin as a hemostatic agent. Proc Soc Exp Biol Med 1939; 41: 655-657. Weinzweig N, Gonzalez M. Free tissue failure is not an all-or-none phenomenon. Plast Reconstr Surg 1995; 96: 648-659. Weitz J. Low-molecular-weight heparins. N Engl J Med 1997; 337: 688-698. van Wersch JWJ, van Mourik-Alderliesten, Coremans A. Comparison of markers of coagulation activation under oral anticoagulation at different levels. Eur J Clin Chem Clin Biochem 1992; 30: 461-466. Wieslander JB, Åberg M, Dougan P. Accumulation of isotope labeled platelets in small arteries after end-to-end and end-in-end anastomoses in the rabbit. Br J Plast Surg 1982; 35: 158-162. Wieslander JB, Dougan P, Stjernquist U, Åberg M, Bergentz S-E. The influence of dextran and saline solution upon platelet behaviour after microarterial anastomosis. Surg Gyn Obstr 1986; 163: 256-262. Wieslander JB, Dougan P. Washout of vessels with heparin does not improve patency following severe microarterial trauma: an experimental study. Ann Plast Surg 1990; 24: 216-222. Wieslander JB, Salemark L, Dougan P. Hydroxyethyl starch increases patency and reduces thrombus formation following arteriotomy/intimectomy in small arteries: an experimental study in the rabbit. J Reconstr Microsurg 1990; 6: 357-361. Wolfort SF, Angel MF, Knight KR, Amiss LR, Morgan RF. The beneficial effect of dextran on anastomotic patency and flap survival in a strongly thrombogenic model. J Reconstr Microsurg 1992; 8: 375-378. Yang J-P, Glickman AM, Edwards V, Boyer MI, Vaughan C, Bowen A. An ultrastructural study of the intimal hyperplasia in healing microarterial anastomoses. Microsurgery 1998; 18: 391-396. Yoda Y, Abe T. Fibrinopeptide A (FPA) level and fibrinogen kinetics in patients with malignant disease. Thromb Haemost 1981; 46: 706-709. Yu-dong G, Ji-feng L, Ji-fu J, Ci-sheng Z, Pei-zhu T. Scanning electron microscopic observations on the endothelial healing mechanism of vessels. J Reconstr Microsurg 1989; 5:
96
327-330. Yurt RW, Leid RW Jr, Austen KF. Native heparin from rat peritoneal mast cells. J Biol Chem 1977; 252: 518-521. Zacharski LR, Wojtukiewicz MZ, Costantini V, Ornstein DL, Memoli VA. Pathways of coagulation/fibrinolysis activation in malignancy. Semin Thromb Hemost 1992; 18: 104-116. Zacharski LR, Ornstein DL. Heparin and cancer. Thromb Haemost 1998; 80: 10-23. Zhang B, Wieslander JB. Low-molecular-weight heparin exerts an early antithrombotic effect in small arteries and veins following severe trauma. Microsurgery 1992; 13: 295-298. Zhang B, Dougan P, Wieslander JB. A comparison of the early antithrombotic effects between low molecular weight heparin and heparin in small arteries following a severe trauma: an experimental study. Ann Plast Surg 1993; 31: 255-261. Zhang B, Wieslander JB. Dextran´s antithrombotic properties in small arteries are not altered by low-molecular-weight heparin or the fibrinolytic inhibitor tranexamic acid: an experimental study. Microsurgery 1993; 14: 289-295. Zhang B, Wieslandr JB. Comparison of the antithrombotic effect of the new recombinant hirudin HBW 023 and heparin in small arteries and veins. Microsurgery 1996; 17: 89-96. Zhang B, Wieslander JB. Influence of early fibrinolysis inhibition on thrombus formation following microvascular trauma. Microsurgery 1996; 17: 278-285. Zinberg EM, Choo DI, Zotter LA. Effect of heparinized irrigating solutions on patency of experimental microvascular anastomoses. Microsurgery 1989; 10: 103-107.





























