Embed Size (px)
Citation preview
Dengue: The New Classification
Developed by clinicians and scientists of the DENCO study,
World Health Organization, Geneva
2
2005 to 2007
Objectives:
• Describe clinical disease in all age groups
and across a wide geographical range
• To develop a new candidate classification
3
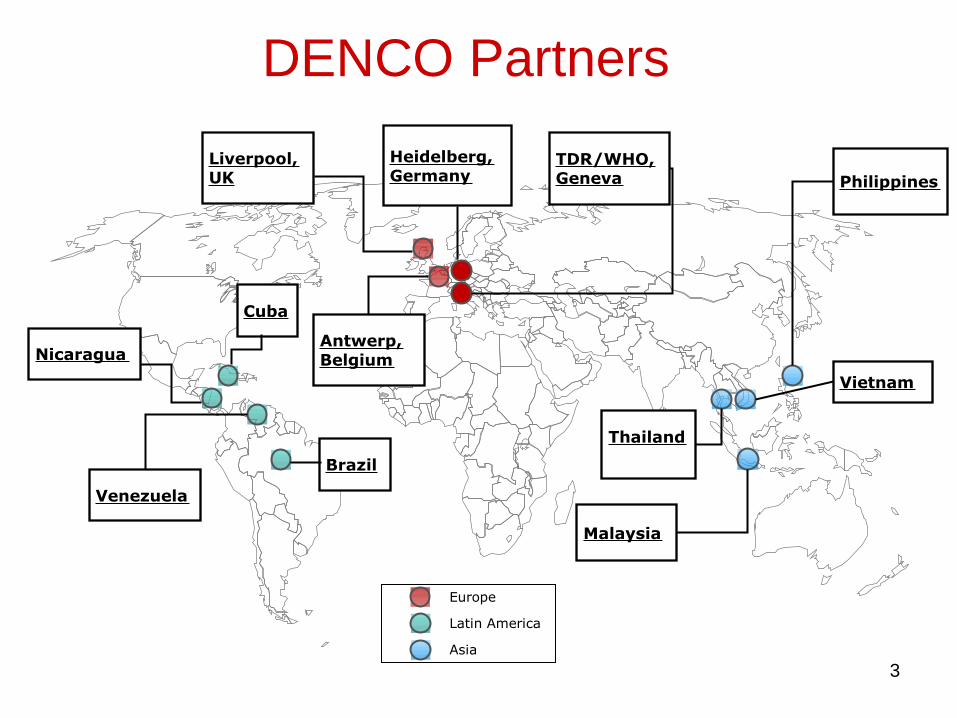
Venezuela
Antwerp,Belgium
Philippines
Heidelberg,Germany
Vietnam
Malaysia
Thailand
TDR/WHO,Geneva
Europe
Latin America
Asia
Cuba
Liverpool,UK
Nicaragua
Brazil
DENCO Partners
4
Method
• Prospective hospital based multicentre study –local centres of excellence
• Children & adults, clinically suspected dengue
• Recruited < 7 days of illness and
• Daily follow-up with a detailed CRF
– Hct and platelets done at least daily
– Other tests (liver & renal function) at least twice during acute illness
– Radiological evidence of plasma leakage within 24h of defervescence
– WHO trained monitors
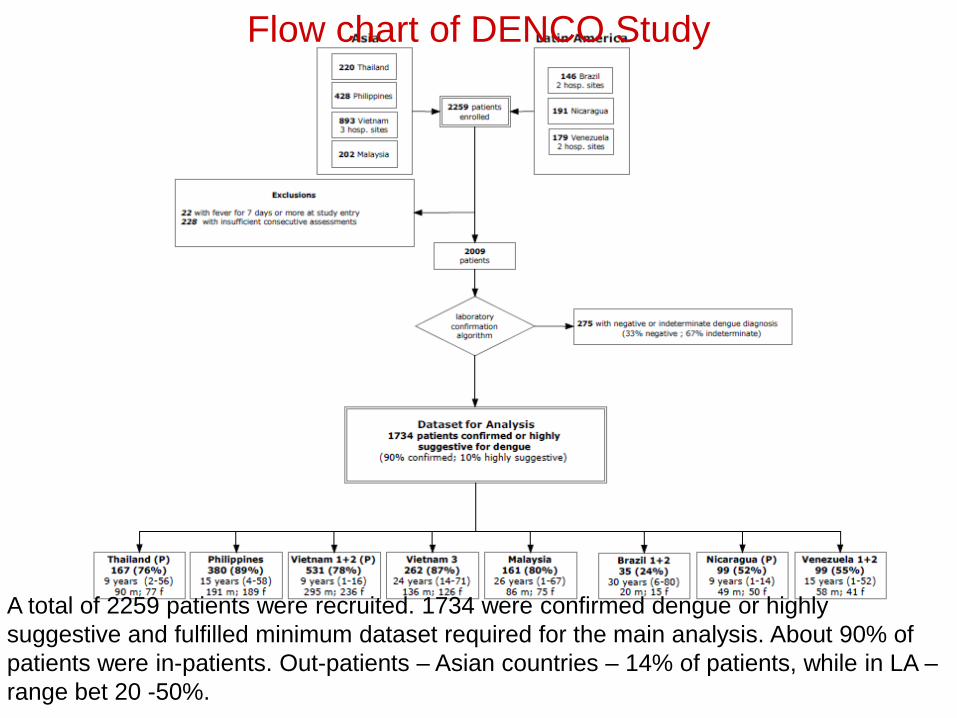
Flow chart of DENCO Study
A total of 2259 patients were recruited. 1734 were confirmed dengue or highly
suggestive and fulfilled minimum dataset required for the main analysis. About 90% of
patients were in-patients. Out-patients – Asian countries – 14% of patients, while in LA –
range bet 20 -50%.
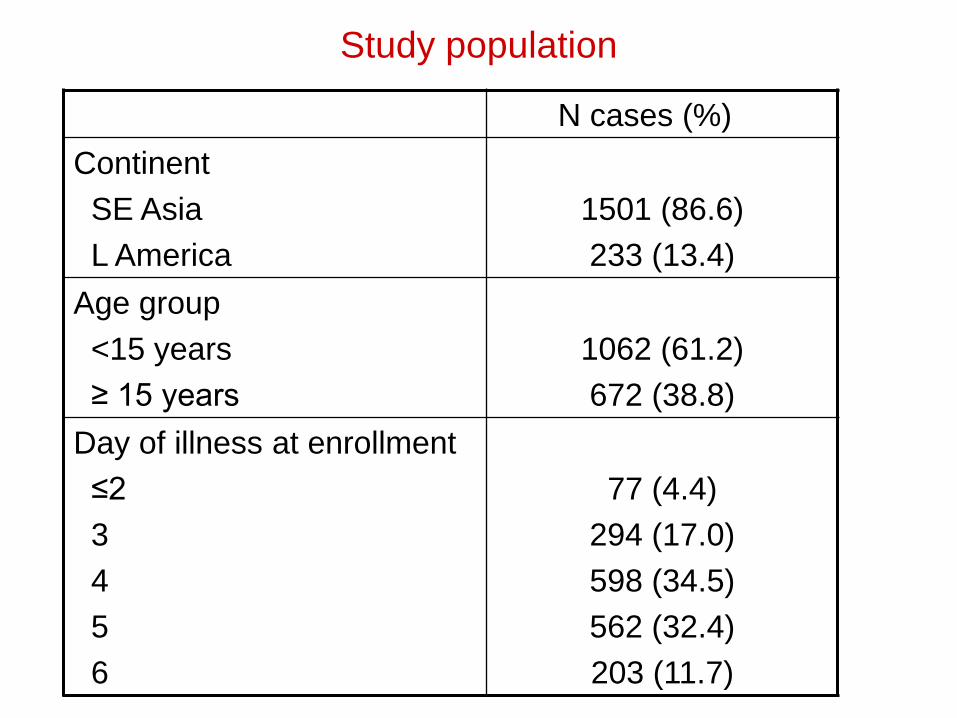
Study population
N cases (%)
Continent
SE Asia
L America
1501 (86.6)
233 (13.4)
Age group
<15 years
≥ 15 years
1062 (61.2)
672 (38.8)
Day of illness at enrollment
≤2
3
4
5
6
77 (4.4)
294 (17.0)
598 (34.5)
562 (32.4)
203 (11.7)
7
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
DSS
DHF
DF
not classifiable
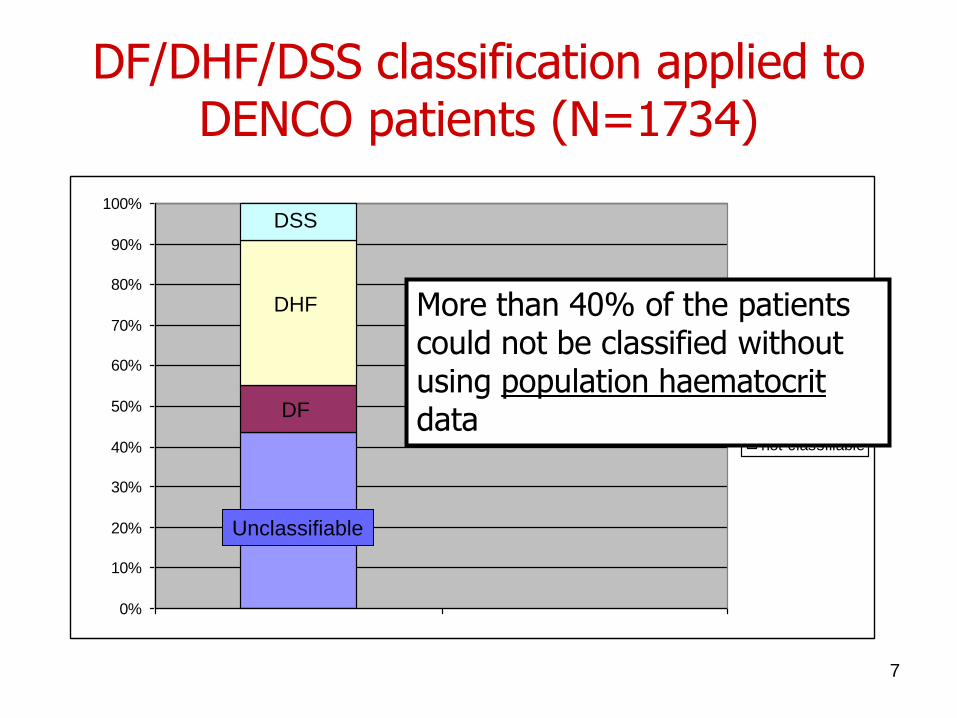
DF/DHF/DSS classification applied to DENCO patients (N=1734)
More than 40% of the patients could not be classified without using population haematocritdata
DHF
DSS
DF
Unclassifiable
8
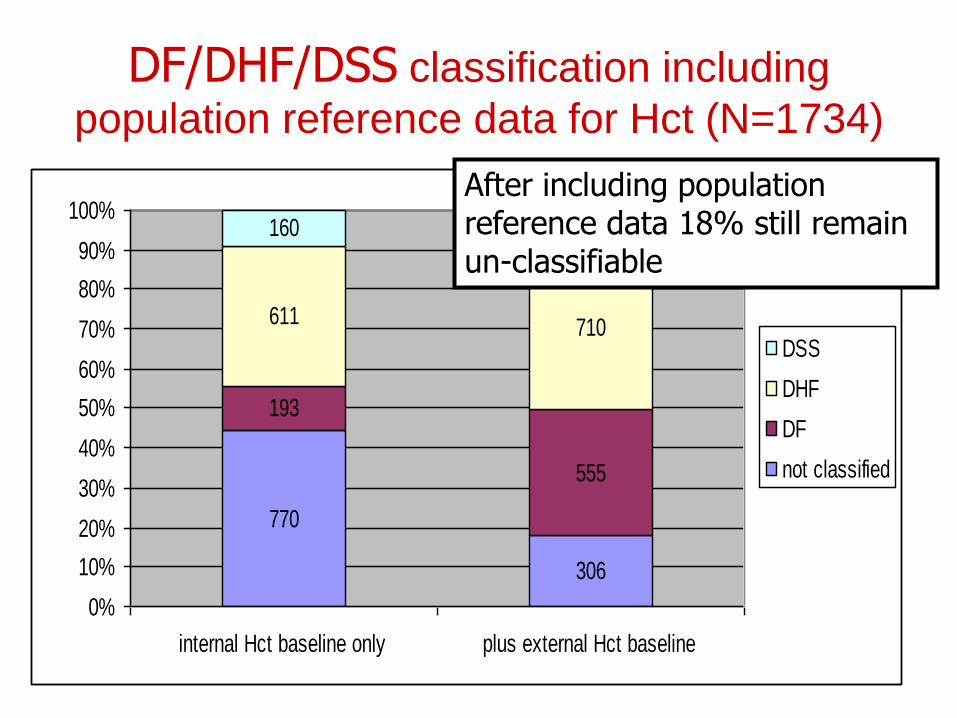
DF/DHF/DSS classification including
population reference data for Hct (N=1734)
770
306
193
555
611 710
160 163
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
internal Hct baseline only plus external Hct baseline
DSS
DHF
DF
not classified
After including population reference data 18% still remain un-classifiable
9
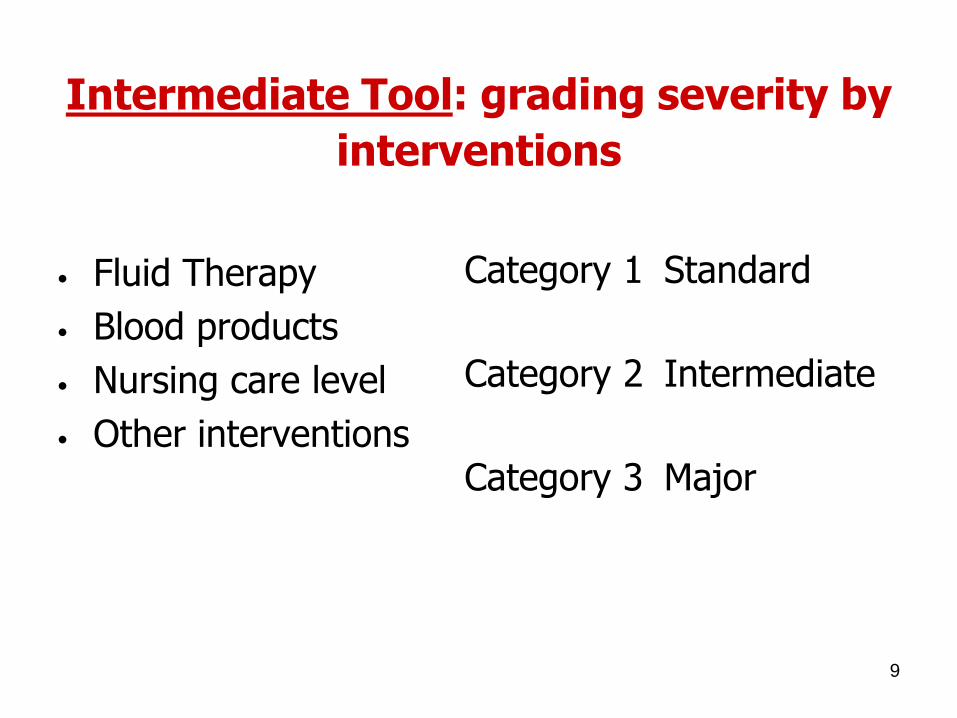
Intermediate Tool: grading severity by
interventions
• Fluid Therapy
• Blood products
• Nursing care level
• Other interventions
Category 1 Standard
Category 2 Intermediate
Category 3 Major
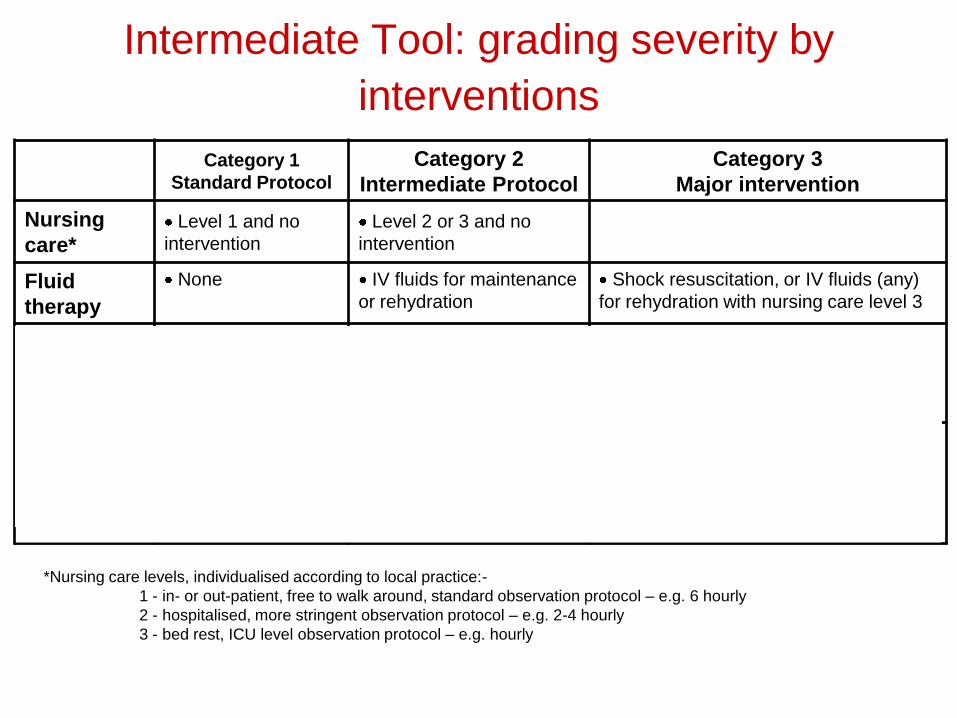
Intermediate Tool: grading severity by
interventions
*Nursing care levels, individualised according to local practice:-
1 - in- or out-patient, free to walk around, standard observation protocol – e.g. 6 hourly
2 - hospitalised, more stringent observation protocol – e.g. 2-4 hourly
3 - bed rest, ICU level observation protocol – e.g. hourly
** At some sites certain blood products were given in response to abnormal laboratory findings rather than for clinical
reasons.Such interventions were classified in the moderate category.
Category 1
Standard Protocol
Category 2
Intermediate Protocol
Category 3
Major intervention
Nursing
care*Level 1 and no
intervention
Level 2 or 3 and no
intervention
Fluid
therapy
None IV fluids for maintenance
or rehydration
Shock resuscitation, or IV fluids (any)
for rehydration with nursing care level 3
Blood
products
None Platelets, fresh frozen
plasma or
cryoprecipitate** with n.
care level 1 or 2
Platelets, fresh frozen plasma or
cryoprecipitate with nursing care level 3
Whole blood, packed red cells, or any
combination of blood products
Other
interventio
ns
None Oxygen therapy
Diuretics without other
specific intervention
Oxygen therapy with n. care level 3
Respiratory support
Inotropic support
Specific treatment for liver, renal or
other organ failure
11
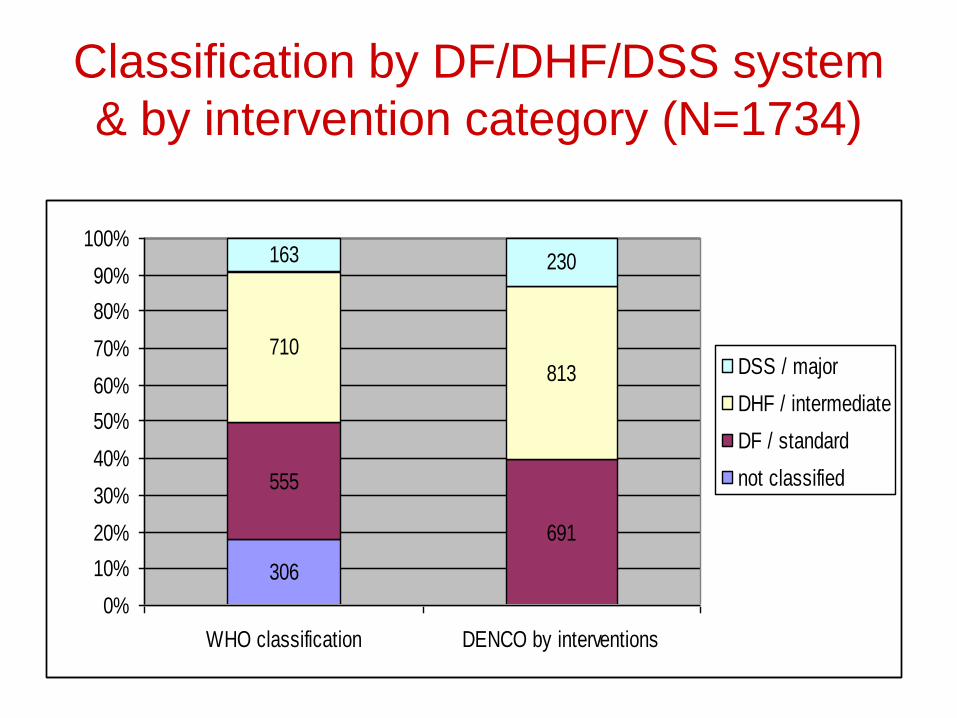
Classification by DF/DHF/DSS system
& by intervention category (N=1734)
306
555
691
710813
163 230
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
WHO classification DENCO by interventions
DSS / major
DHF / intermediate
DF / standard
not classified
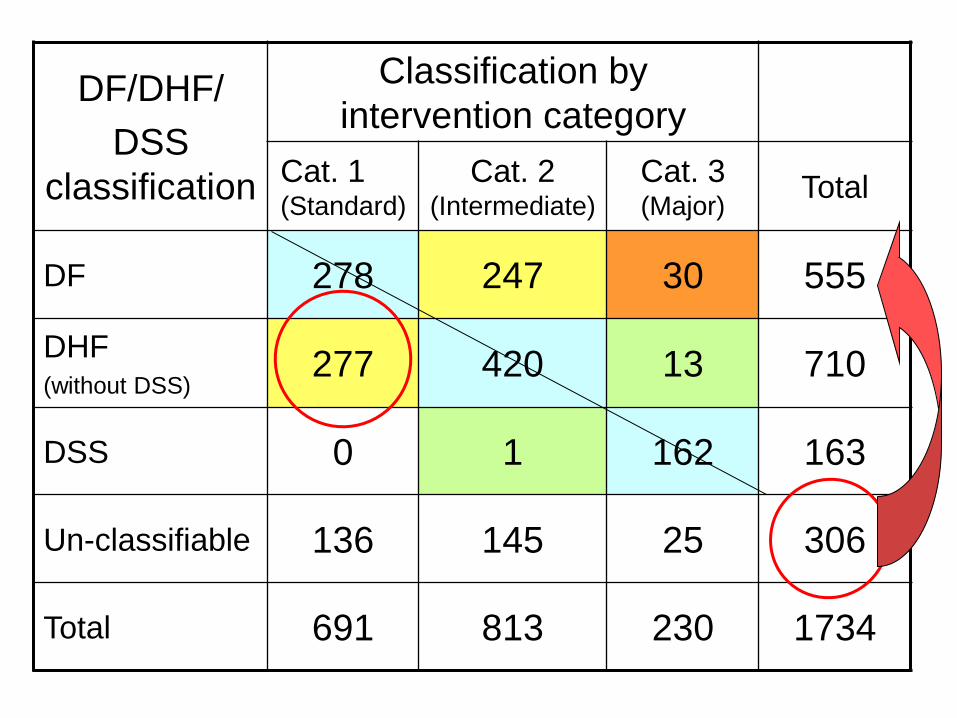
DF/DHF/
DSS
classification
Classification by
intervention category
Cat. 1 (Standard)
Cat. 2 (Intermediate)
Cat. 3 (Major)
Total
DF 278 247 30 555
DHF (without DSS)
277 420 13 710
DSS 0 1 162 163
Un-classifiable 136 145 25 306
Total 691 813 230 1734
13
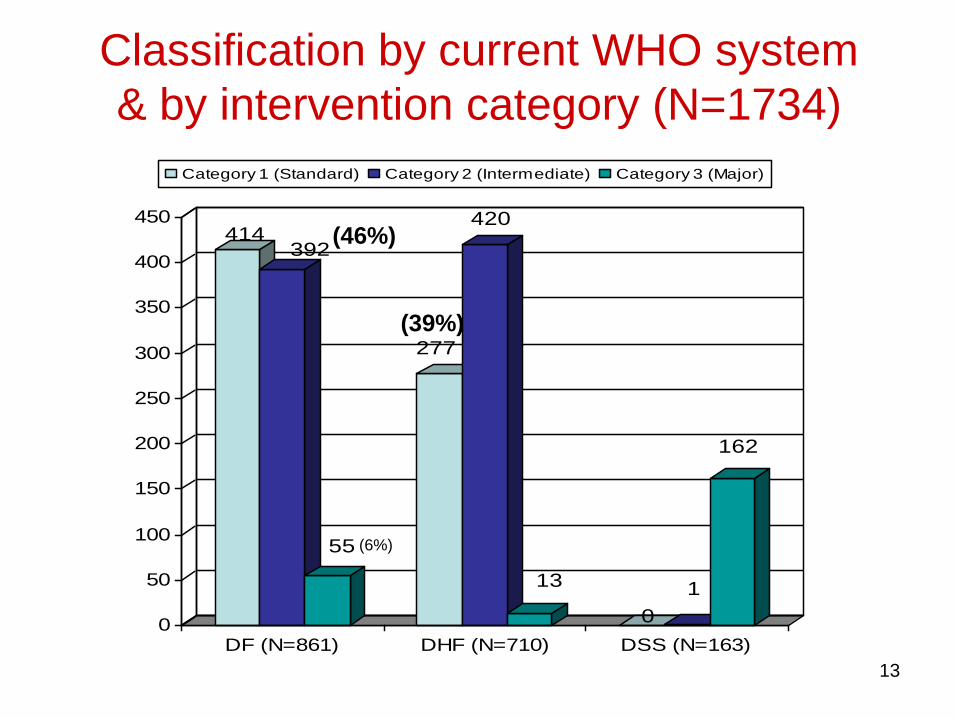
Classification by current WHO system
& by intervention category (N=1734)
414392
55
277
420
13
0
1
162
0
50
100
150
200
250
300
350
400
450
DF (N=861) DHF (N=710) DSS (N=163)
Category 1 (Standard) Category 2 (Intermediate) Category 3 (Major)
(6%)
(46%)
(39%)
14
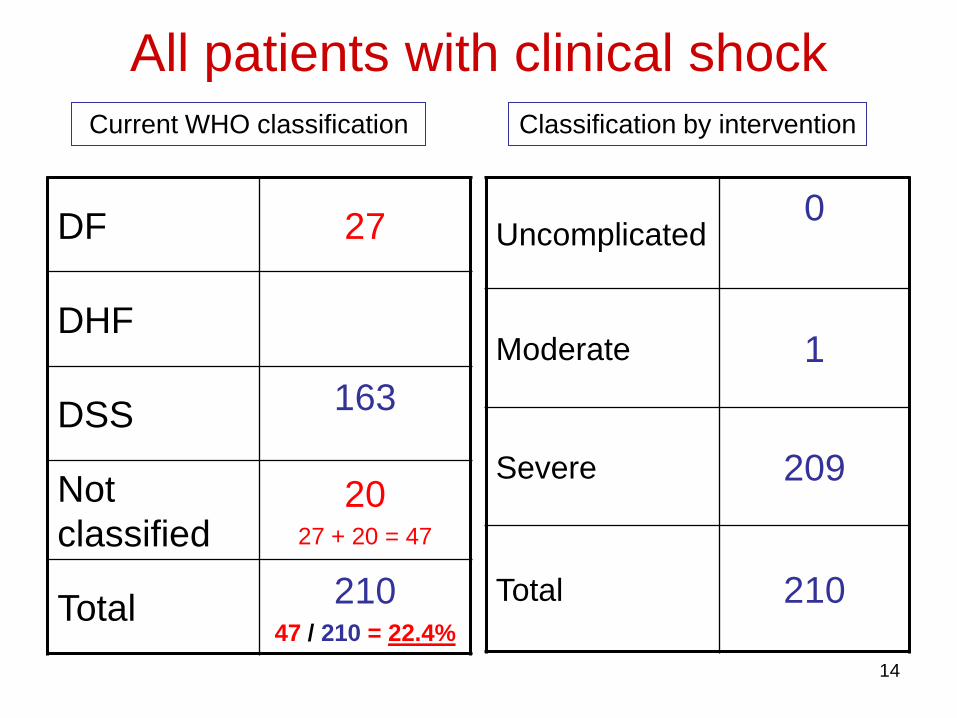
All patients with clinical shock
DF 27
DHF
DSS 163
Not
classified20
27 + 20 = 47
Total 21047 / 210 = 22.4%
Uncomplicated0
Moderate 1
Severe 209
Total 210
Current WHO classification Classification by intervention
15
What about the 277 (39%) DHF patients classified as mild (standard) by intervention?
• In addition to thrombocytopenia and skin bleeding (or nose bleeding),
• most of these patients had radiological evidence of fluid accumulation*,
• some also clinical evidence and/or Hct > 20% compared to baseline
• BUT no intravenous fluid, on a standard observation protocol.
* 151 of the 277 (~55%) only had radiological evidence of fluid accumulation
16
306
555
691
710813
163 230
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
WHO classification DENCO by interventions
DSS / major
DHF / intermediate
DF / standard
not classified
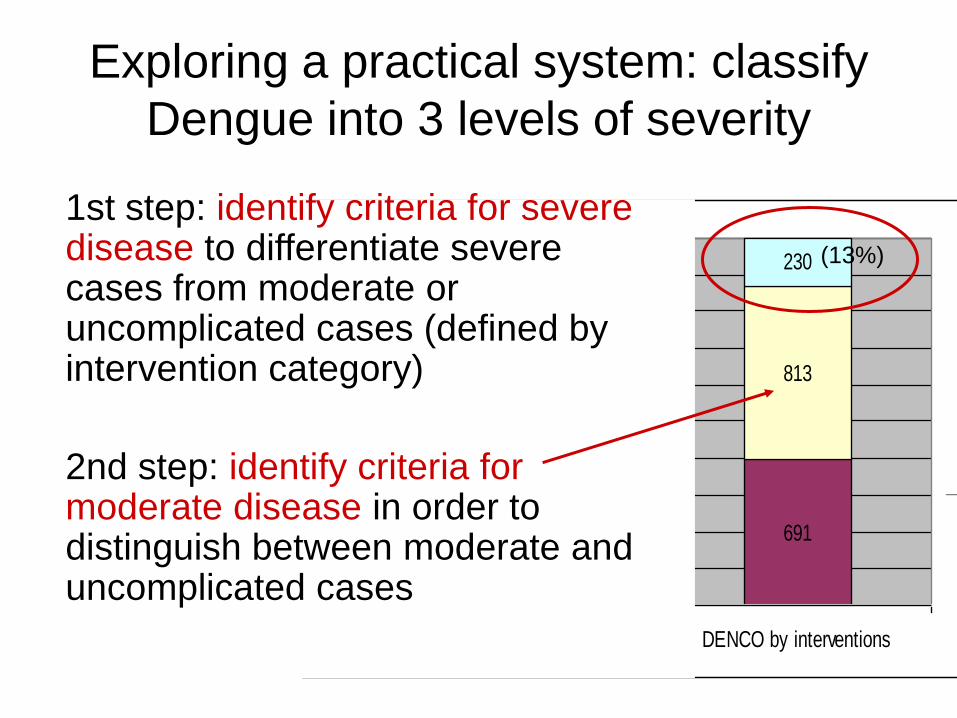
Exploring a practical system: classify
Dengue into 3 levels of severity
1st step: identify criteria for severe disease to differentiate severe cases from moderate or uncomplicated cases (defined by intervention category)
2nd step: identify criteria for moderate disease in order to distinguish between moderate and uncomplicated cases
(13%)
17
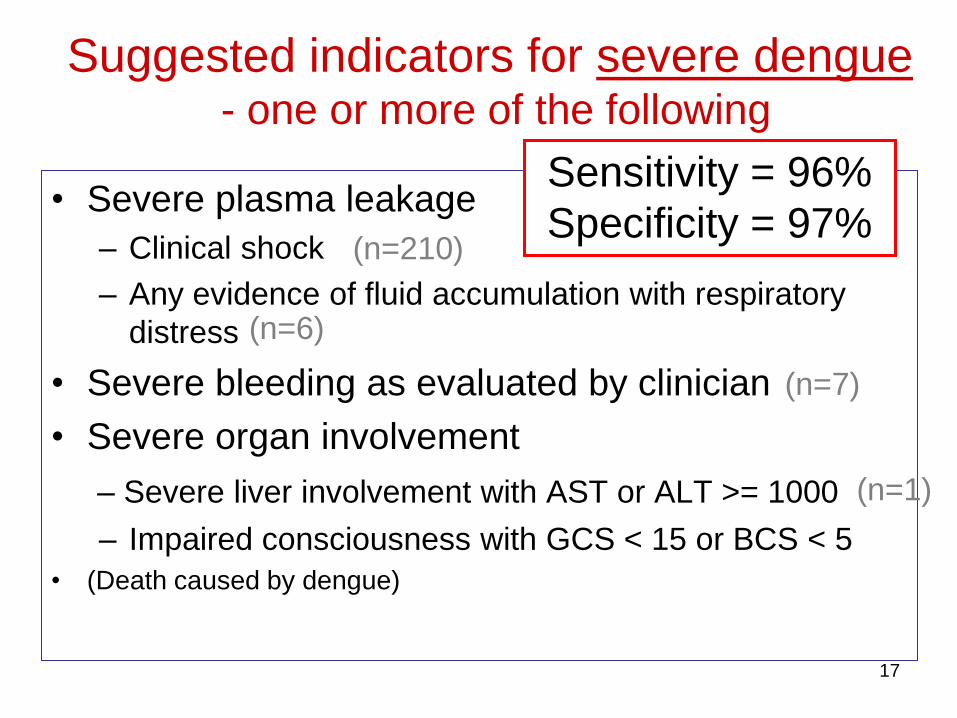
Suggested indicators for severe dengue- one or more of the following
• Severe plasma leakage
– Clinical shock
– Any evidence of fluid accumulation with respiratory
distress
• Severe bleeding as evaluated by clinician
• Severe organ involvement
– Severe liver involvement with AST or ALT >= 1000
– Impaired consciousness with GCS < 15 or BCS < 5
• (Death caused by dengue)
Sensitivity = 96%
Specificity = 97% (n=210)
(n=6)
(n=7)
(n=1)
18
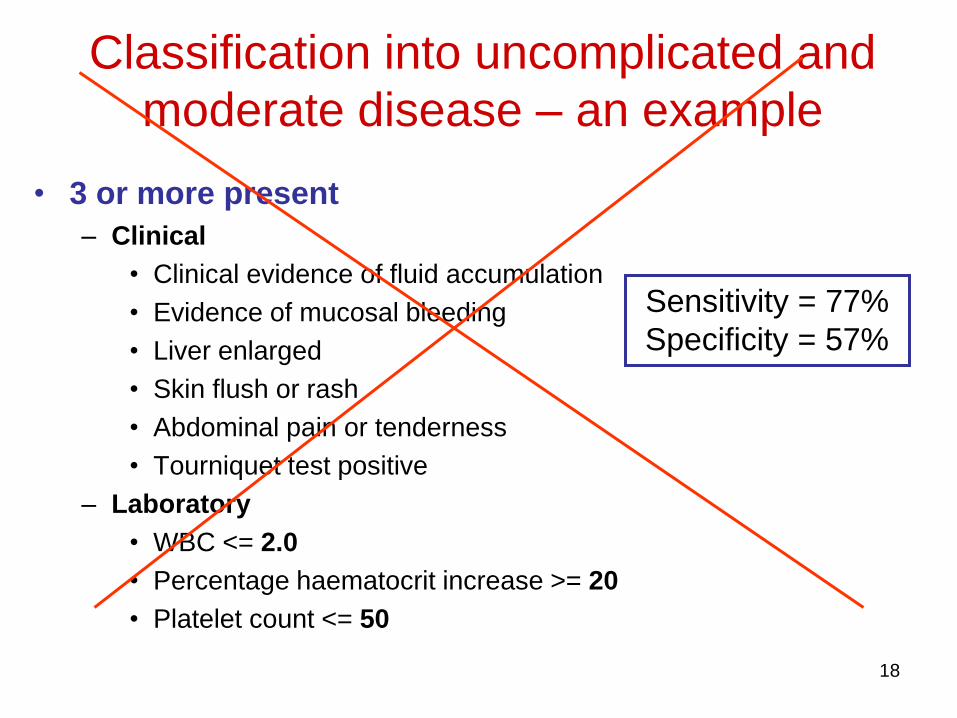
Classification into uncomplicated and
moderate disease – an example
• 3 or more present
– Clinical
• Clinical evidence of fluid accumulation
• Evidence of mucosal bleeding
• Liver enlarged
• Skin flush or rash
• Abdominal pain or tenderness
• Tourniquet test positive
– Laboratory
• WBC <= 2.0
• Percentage haematocrit increase >= 20
• Platelet count <= 50
Sensitivity = 77%
Specificity = 57%
19
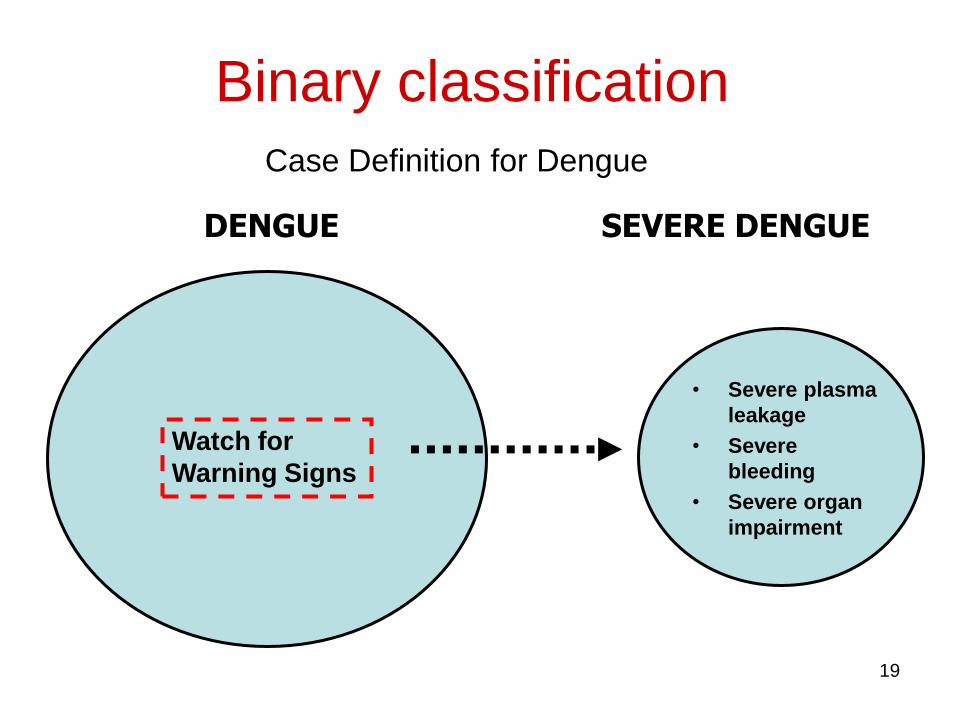
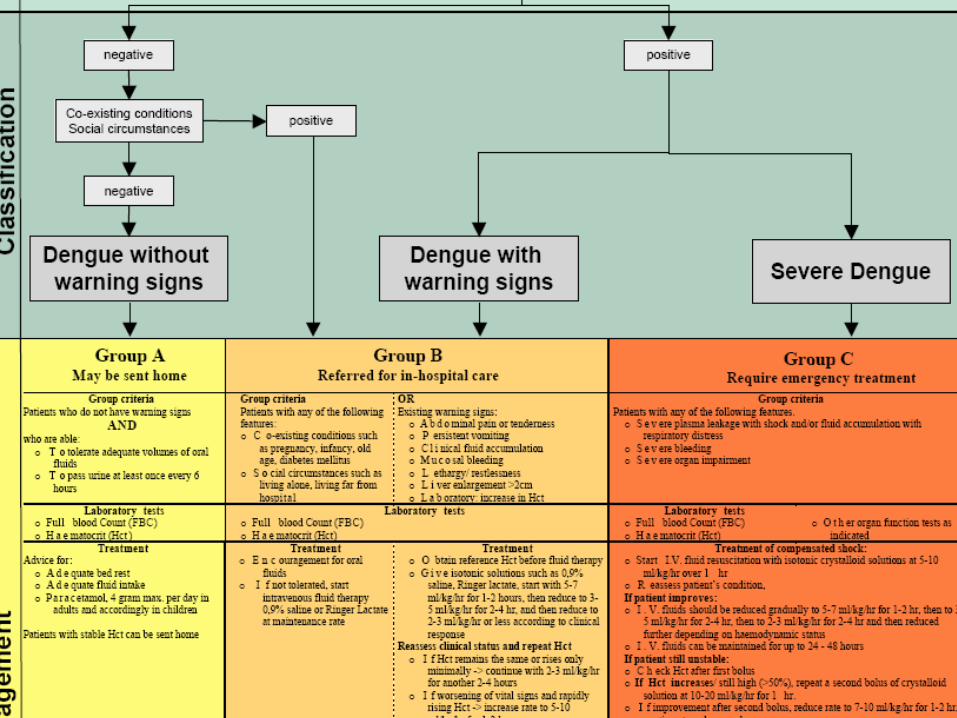
SEVERE DENGUE
Watch for
Warning Signs
DENGUE
Binary classification
• Severe plasma
leakage
• Severe
bleeding
• Severe organ
impairment
Case Definition for Dengue
20
Objective: to compare the two
classification systems
1. Applicability in the clinical practice and in
surveillance,
2. Usefulness for triage and clinical management
and
3. User-friendliness and acceptance by health
staff.
21
S. Arabia
India
Indonesia
Malaysia
Philippines
Bolivia
Colombia
Cuba
Ecuador
El Salvador
Mexico
Nicaragua
Paraguay
Peru
Puerto Rico
Venezuela
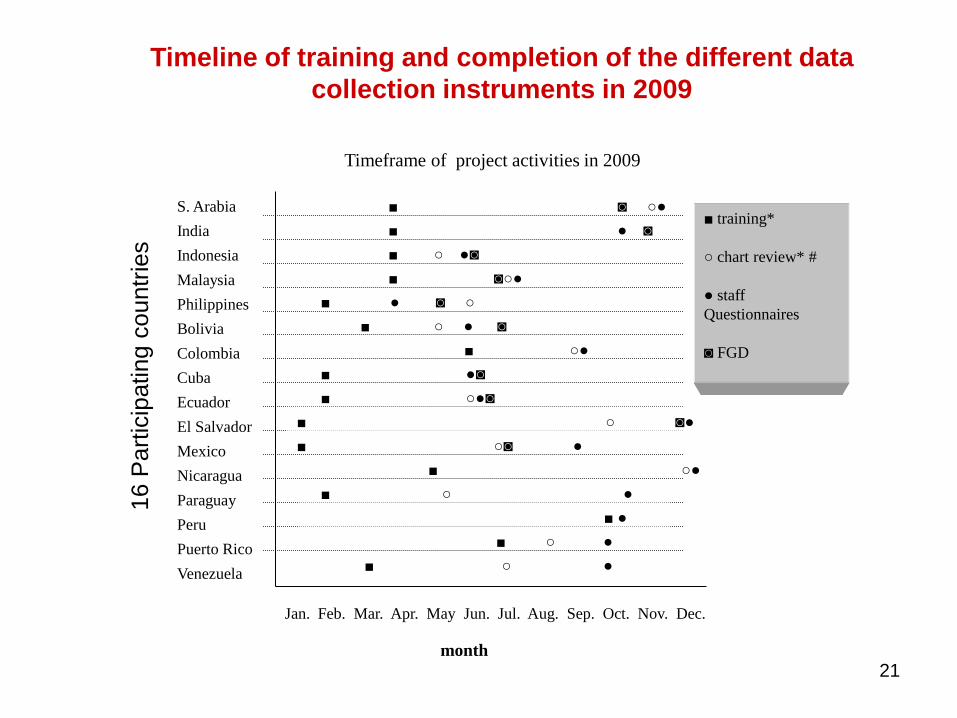
Timeline of training and completion of the different data
collection instruments in 2009
■ training*
○ chart review* #
● staff
Questionnaires
◙ FGD
Jan. Feb. Mar. Apr. May Jun. Jul. Aug. Sep. Oct. Nov. Dec.
■ ◙ ○●
■ ● ◙
■ ○ ●◙
■ ◙○●
■ ● ◙ ○
■ ○ ● ◙
■ ○●
■ ●◙
■ ○●◙
■ ○◙ ●
■ ○●
○■ ○ ●
■ ○ ●
■ ○ ●
Timeframe of project activities in 2009
month
■ ○ ◙●
■ ●
16 P
art
icip
ating c
ountr
ies
22
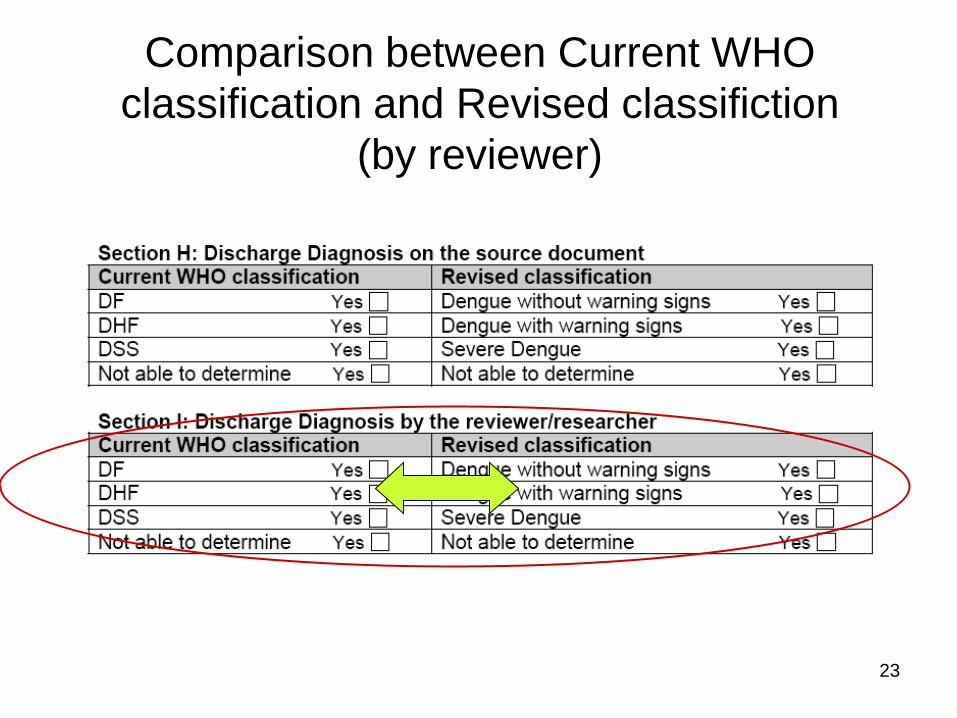
23
Comparison between Current WHO
classification and Revised classifiction
(by reviewer)
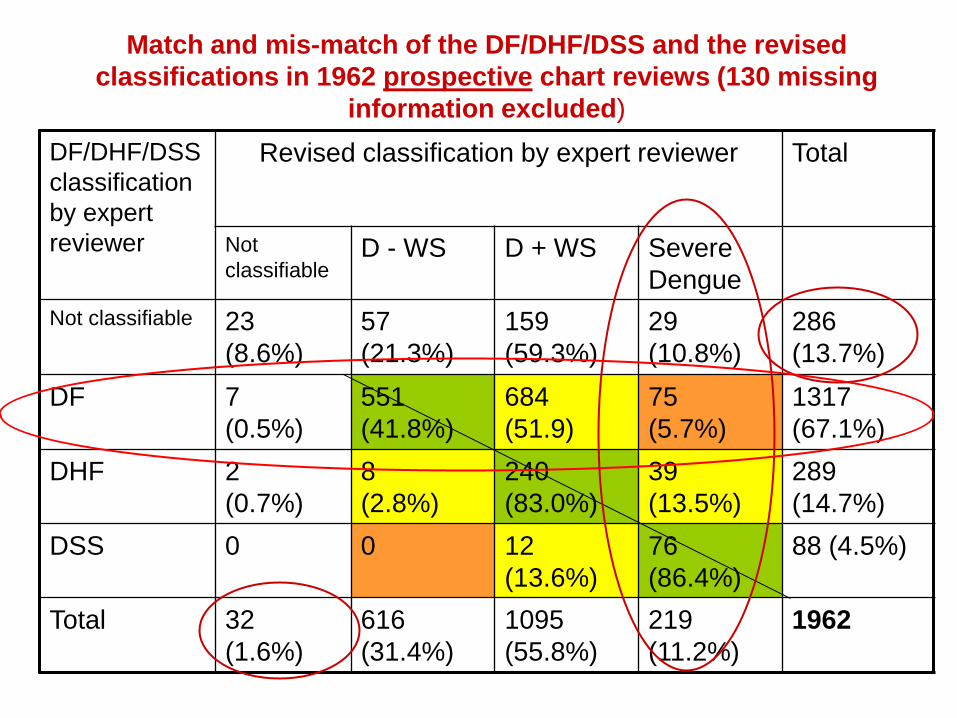
Match and mis-match of the DF/DHF/DSS and the revised
classifications in 1962 prospective chart reviews (130 missing
information excluded)
DF/DHF/DSS
classification
by expert
reviewer
Revised classification by expert reviewer Total
Not
classifiableD - WS D + WS Severe
Dengue
Not classifiable 23
(8.6%)
57
(21.3%)
159
(59.3%)
29
(10.8%)
286
(13.7%)
DF 7
(0.5%)
551
(41.8%)
684
(51.9)
75
(5.7%)
1317
(67.1%)
DHF 2
(0.7%)
8
(2.8%)
240
(83.0%)
39
(13.5%)
289
(14.7%)
DSS 0 0 12
(13.6%)
76
(86.4%)
88 (4.5%)
Total 32
(1.6%)
616
(31.4%)
1095
(55.8%)
219
(11.2%)
1962
25
Match and mis-match of the DF/DHF/DSS and the
revised classification systems
• Mismatches
• Independent of laboratory confirmation
• No significant differences in Asia with Latin
America
• Similar at all levels of the health care
system.
• More mismatches at tertiary level.
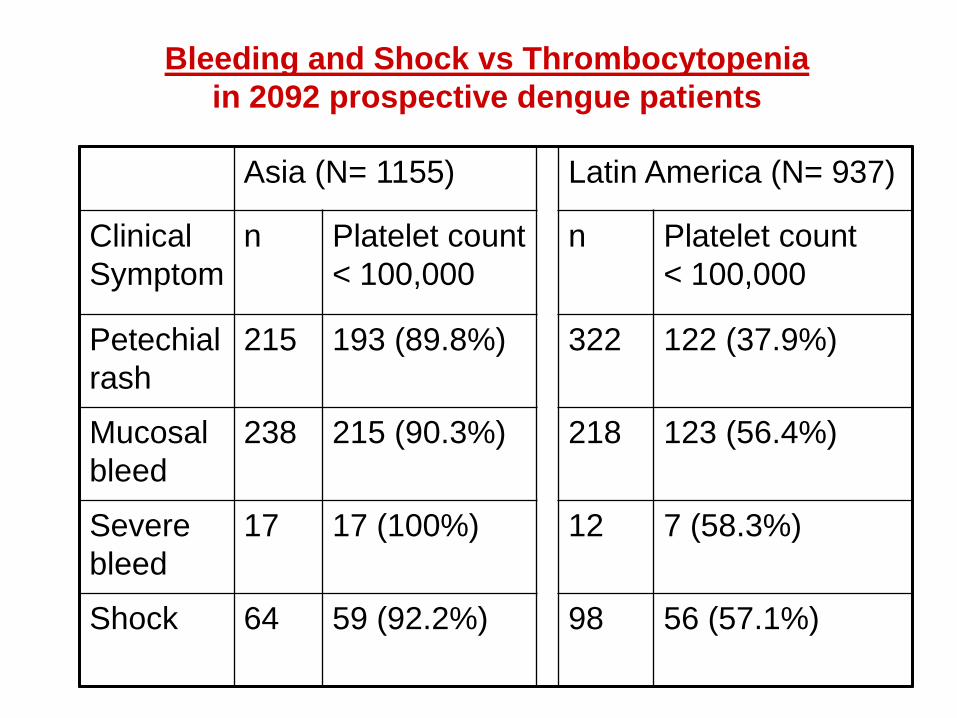
Asia (N= 1155) Latin America (N= 937)
Clinical
Symptom
n Platelet count
< 100,000
n Platelet count
< 100,000
Petechial
rash
215 193 (89.8%) 322 122 (37.9%)
Mucosal
bleed
238 215 (90.3%) 218 123 (56.4%)
Severe
bleed
17 17 (100%) 12 7 (58.3%)
Shock 64 59 (92.2%) 98 56 (57.1%)
Bleeding and Shock vs Thrombocytopenia
in 2092 prospective dengue patients
27
Conclusions
• Current classification is applied “loosely”.
A strict application leads to a substantial number
being reclassified.
• Application of the revised classification:
identified previously undetected severe cases.
• Both systems of classification: performance was
dependant on the training level of the person
classifying the case.
• A severity-based revised dengue classification
was positively validated in a large number of
countries.
28
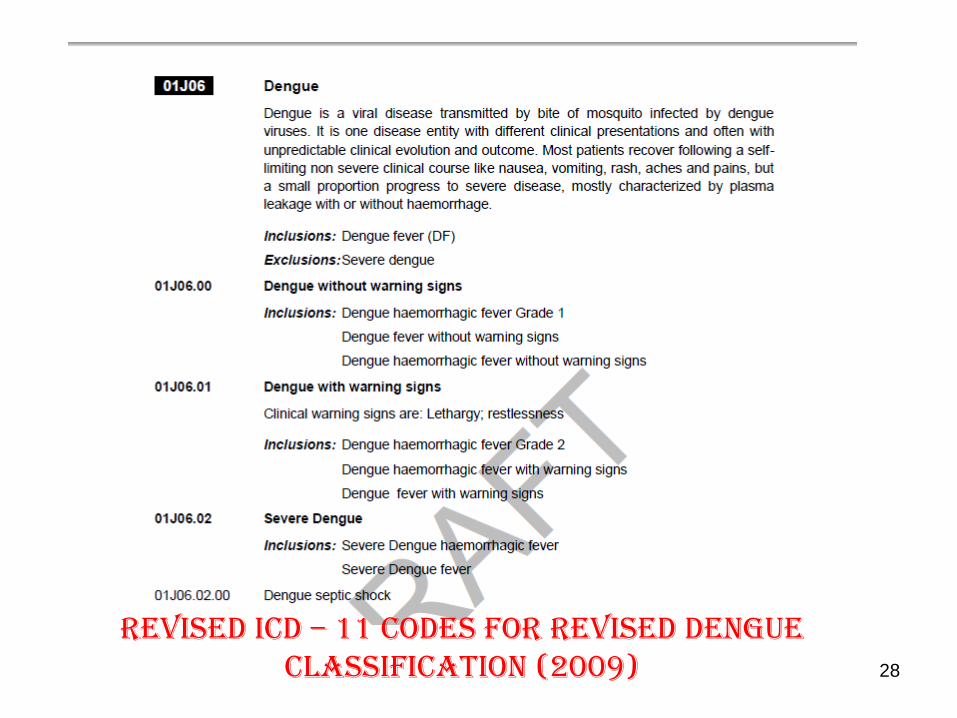
Revised ICD – 11 Codes for Revised Dengue Classification (2009)
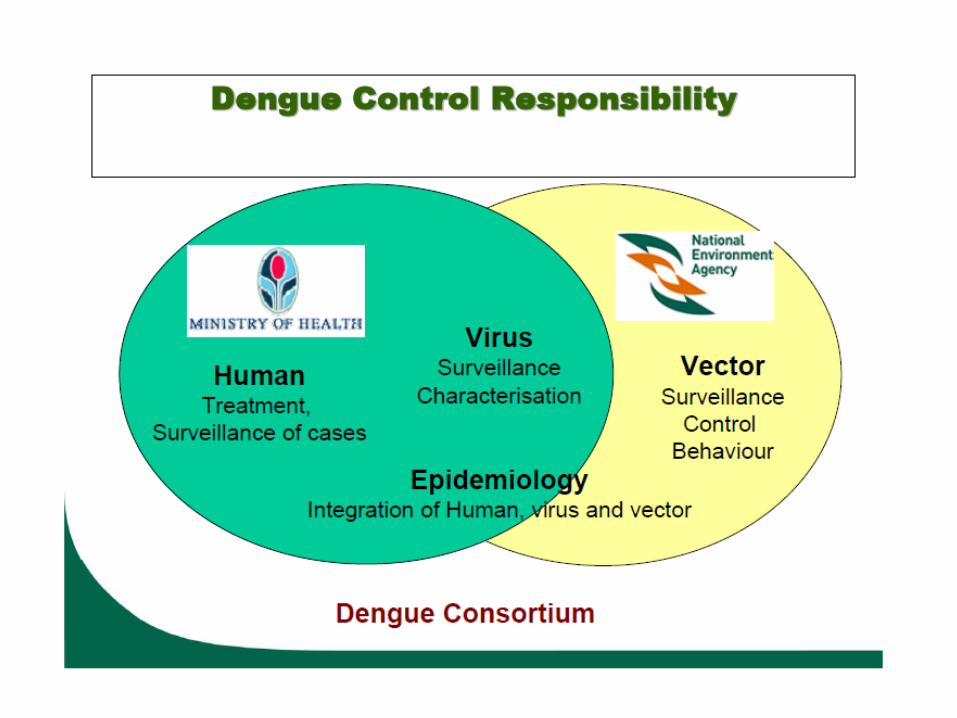

Dengue Control in Singapore
Dengue Control
Epidemiological
Surveillance of
Human Cases
Vector (Mosquito)
Surveillance &
Control
Regional Meeting-Chiang Rai
Dengue awareness – an innovative effort…
Regional Meeting-Chiang Rai
Programme Interventions
Clinical Management
National Guidelines on clinical management developed;
Diagnostic capacity enhanced and proper clinical management ensured through training of doctors and nurses;
Vector Control
Spot checking for vector density
Role of City Corporations—larvacides/fogging
Community education
Public awareness raising and campaign for reduction of breeding sources
Regional Meeting-Chiang Rai
National Guidelines for Clinical Management
of Dengue/DHF
Features of National Guidelines– Through consensus
– Uniform approach
– Simple and user friendly
– Usable in any setup of resource limitation
• Provide uniform understanding of :
– Case definition
– Structured management outline
– Communication guide
– Reporting
National Guidelines was adopted in 2000 by customizing SEARO Guidelines;
2nd edition in 2009 published
Regional Meeting-Chiang Rai
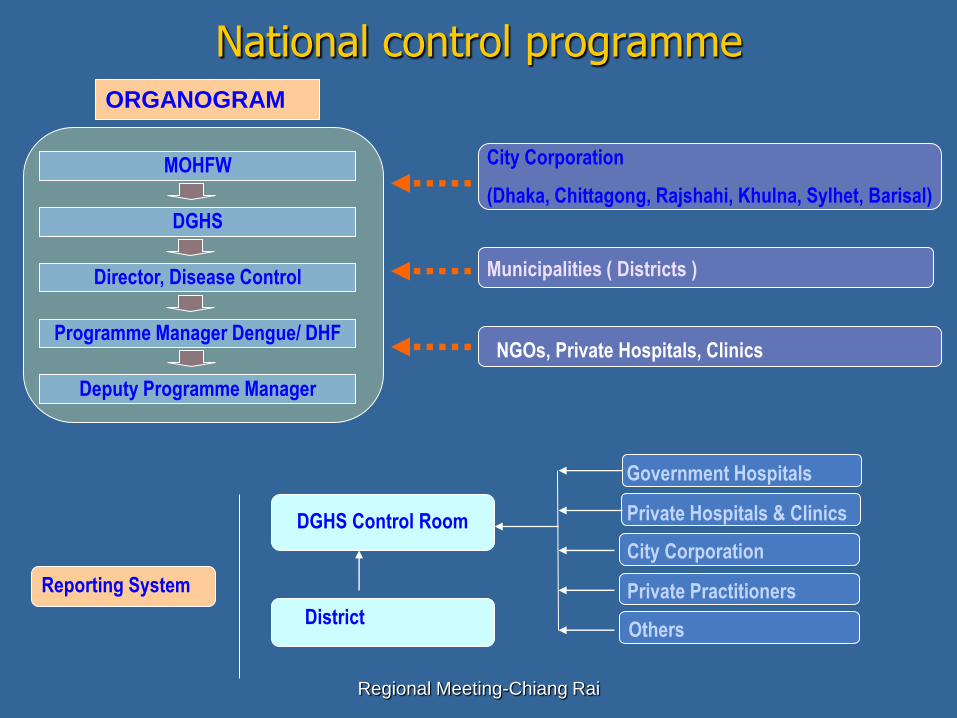
National control programmeORGANOGRAM
MOHFW
DGHS
Director, Disease Control
Programme Manager Dengue/ DHF
Deputy Programme Manager
City Corporation
(Dhaka, Chittagong, Rajshahi, Khulna, Sylhet, Barisal)
Municipalities ( Districts )
NGOs, Private Hospitals, Clinics
Reporting System
DGHS Control Room
District
Government Hospitals
Private Hospitals & Clinics
City Corporation
Private Practitioners
Others
Regional Meeting-Chiang Rai
Dengue Training for Scouts
Regional Meeting-Chiang Rai
Scouts are visiting houses …
Dengue Control
Activities in Sri Lanka
National Program Objective
Prevention and control of DF/DHF
Specific objectives
Enhance disease surveillance
Proper case management
Integrated vector management
Intersectoral coordination & social mobilization
Outbreak response
Research
1. Enhance disease surveillance
Strengthen early notification at OPD/ wards
Train doctors on standard case definition
Planning to establish 3 peripheral labs to
strengthen laboratory surveillance
Periodic district reviews (in identified high risk
areas)
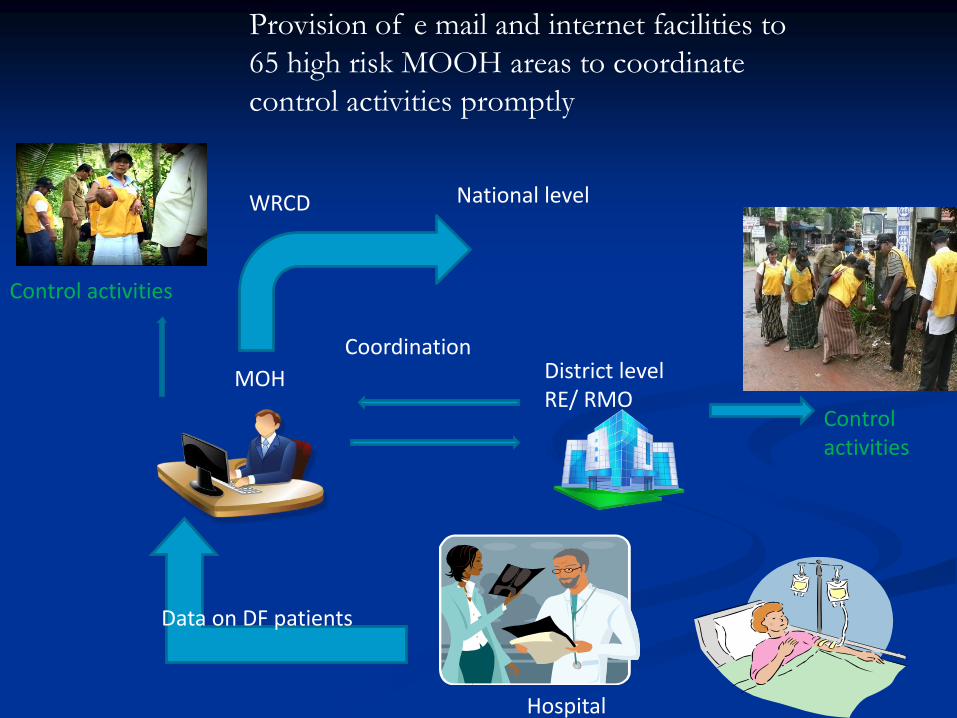
Data on DF patients
Hospital
MOH District levelRE/ RMO
Coordination
National levelWRCD
Control activities
Control activities
Provision of e mail and internet facilities to
65 high risk MOOH areas to coordinate
control activities promptly
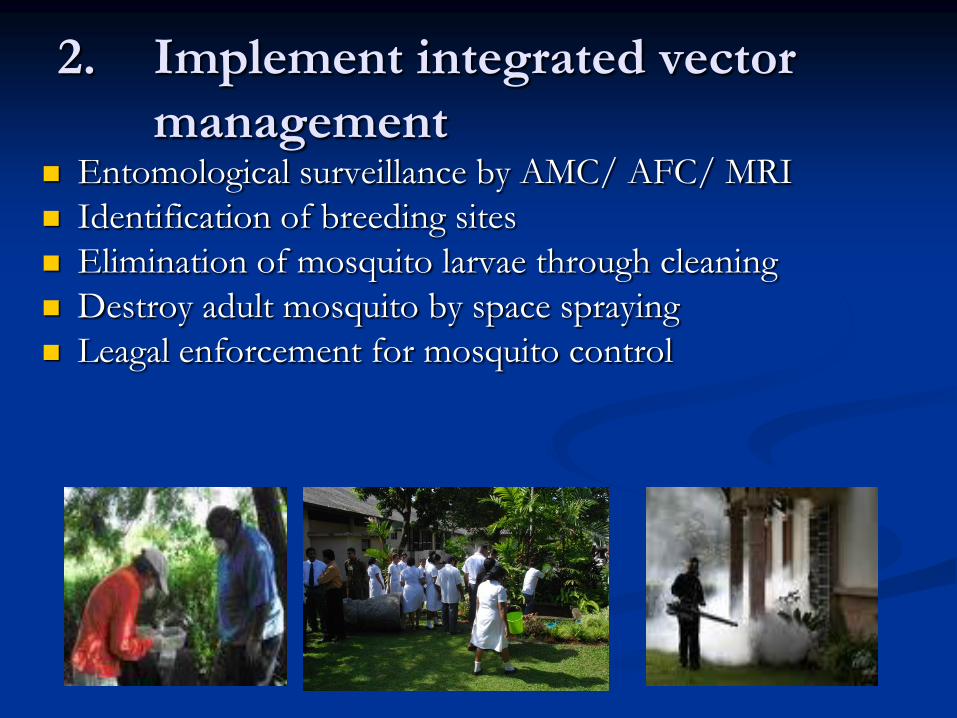
2. Implement integrated vector
management Entomological surveillance by AMC/ AFC/ MRI
Identification of breeding sites
Elimination of mosquito larvae through cleaning
Destroy adult mosquito by space spraying
Leagal enforcement for mosquito control
3. Proper case management
Guidelines and training manuals for training clinicians have been developed by Epidemiology Unit
Training of trainers
Regular training conducted in high risk areas
Conduction of death reviews in order to identify and rectify deficiencies
4. Intersectoral coordination &
social mobilization
Presidential Task Force 25.05.2010 -Members: Ministry of Health, Environment & Central Environment Authority, Local Government & Provincial Councils, Education, Defense, Media and Information, Disaster Management
COMBI training for high risk district teams
Development of district COMBI plans
Development of key messages for key target groups
Monitoring of implementation of COMBI activities

Advocacy - Highest Level
Ministries
• Health
• Local Govt.
• Environment
• Education
• Media

Mobilization of Civil Security Committees
Production of IEC materials
Specific behavioural messages are:
Inspect your premises once a week
Store tyres under cover
Scrub and clean water storage containers once a
week/ keep covered with mosquito proof
coverings
•

Mobilization of community volunteers

Mobilization of school children
5: Outbreak Response
Close monitoring of cases in geographical
regions
Early detection of outbreaks (based on
entomological data and case reporting)
Risk communication
Training of staff, building capacities of hospitals
Declaration of dengue weeks and media seminars
6: Research
Identify research priority areas( Epidemiology
Unit, Universities, RMO, PG trainees) and
mobilization of funds
Vector
Virus
Knowledge and behavior of the community
GENERAL OBJECTIVE OF DENGUE
CONTROL PROGRAM
1. Decreased of morbidity of DHF/Chikungunya cases.
2. Decreased of mortality (CFR) of DHF.
3. Prevention & control of DHF/Chikungunya outbreak.
1. Early diagnosis and prompt treatment
2. Improving epidemiological surveillance and
outbreak response
3. Integrated vector control (Risk factors prevention
and control)
4. Partnerships, capacity building, training and
survey/research
Policies and Programme
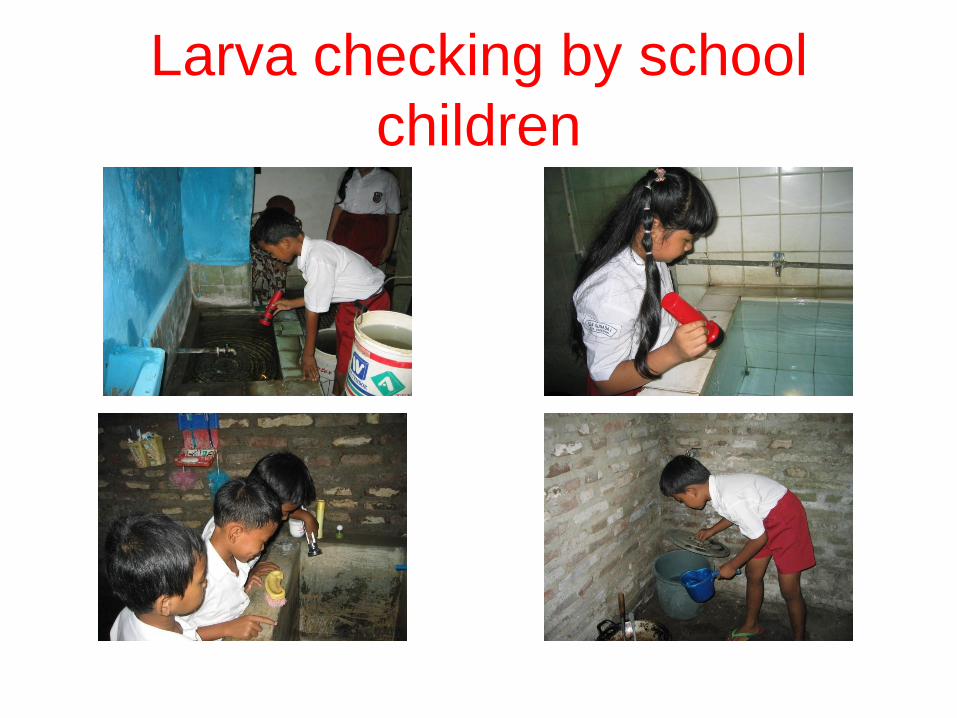
Larva checking by school
children

HOUSE VISITING
BY JUMANTIK (LARVA INSPECTOR)

LARVAE INSPECTION BY JUMANTIK

Checking of all
potential breeding
places such as
plastic barrels,
flower vase,
drinking container
for pet.
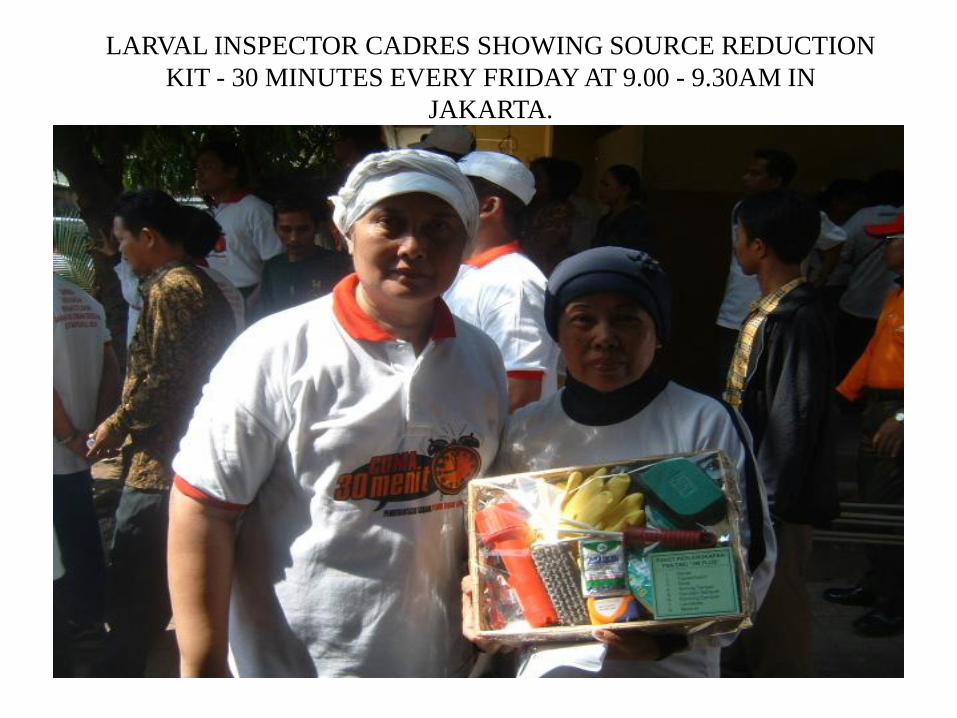
LARVAL INSPECTOR CADRES SHOWING SOURCE REDUCTION
KIT - 30 MINUTES EVERY FRIDAY AT 9.00 - 9.30AM IN
JAKARTA.
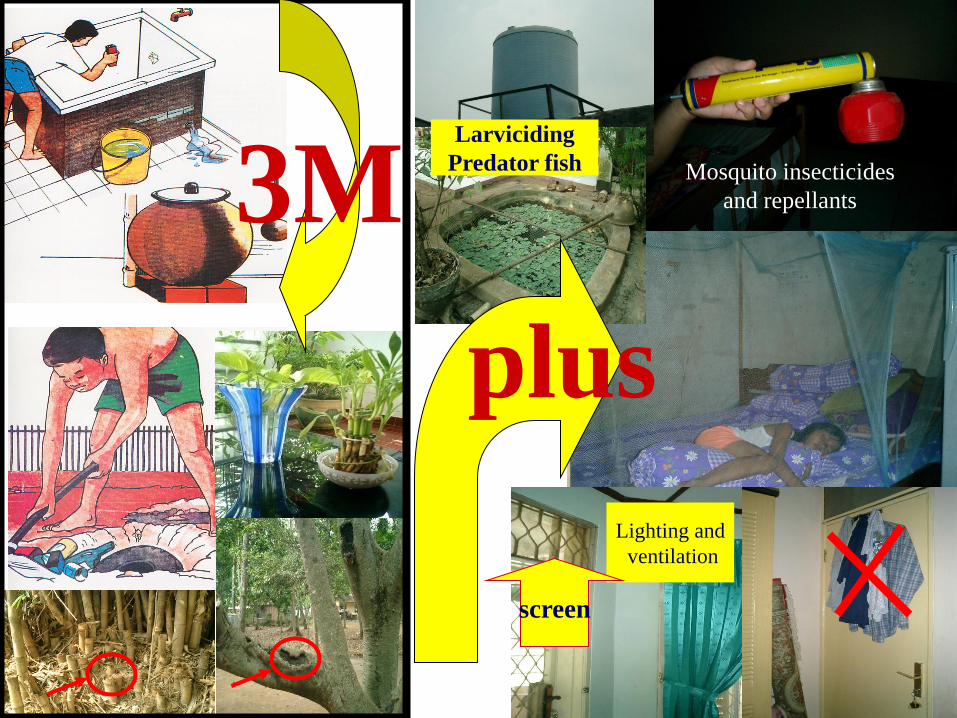
plus
3MLarviciding
Predator fish Mosquito insecticides
and repellants
Lighting and
ventilation
screen
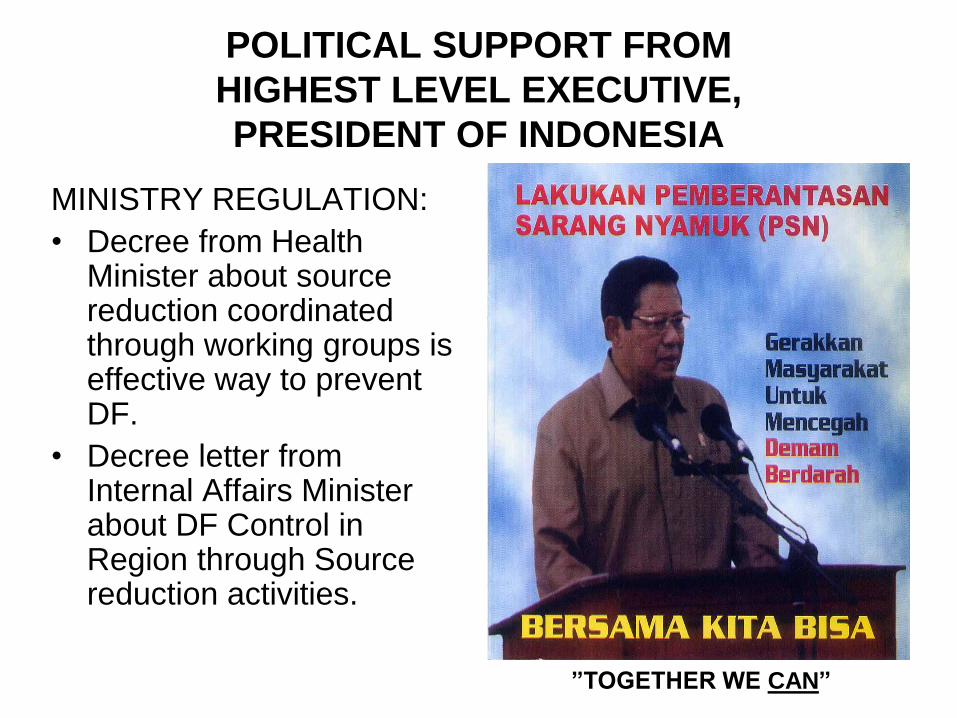
POLITICAL SUPPORT FROM
HIGHEST LEVEL EXECUTIVE,
PRESIDENT OF INDONESIA
MINISTRY REGULATION:
• Decree from Health Minister about source reduction coordinated through working groups is effective way to prevent DF.
• Decree letter from Internal Affairs Minister about DF Control in Region through Source reduction activities.
”TOGETHER WE CAN”
1. Case fatality is still high in several districts
2. Increasing trends of dengue and CHK cases
3. Inadequate of surveillance
4. Low community and inter-sectoral participation
5. Increasing risk factors
6. Inadequate funds
Problem of DHF/Chikungunya
Control Programme
Future Plan (1)
1. Legislation
Review and develop existing legislation on DHF
control.
2. Strengthening collaboration/partnerships
3. Strengthening surveillance
• Update surveillance and response guidelines
• Training for surveillance staff in PHC and
District/Prov Health services
Future Plan (2)
4. Response
• Establish and training rapid response team in
sub dustrict/district level.
• Develop the cadre to check vector breeding
places.
5. Case management
• Revise case management guidelines and its
implementation
Future Plan (3)
• Implementation of new criteria of DHF cases trial in
hospitals.
• Develop early detection with RDT for DHF.
• Training of case management of DHF for MD in
PHC.
6. Laboratory
• Develop the capacity of lab diagnostic in provinces
• Develop surveillance based lab on Chik/DHF
Future Plan (4)
7. Communication using COMBI approach