Embed Size (px)
Citation preview

Delayed dental development in a patient with Gorlinsyndrome: case reportScott H. Rosenblum DDS, MPH
G orlin syndrome is a relatively uncommon en-¯ tity which was first reported by Ancell in 1841in a patient with multiple benign cysts of the
jaws.~ In 196’5, this condition took on its current namewhen Gorlin catalogued the related findings of 150 pa-tients, 2 the most common of which were multiplenevoid basal cell carcinomas of the neck and face, riband spine abnormalities, multiple cysts of the jaws, andlemellar calcifications of the falx cerebri.3 Since thattime, the condition has been variously known asGorlin-Goltz syndrome, Nevoid Basal Cell Carcinomasyndrome, and Basal Cell Nevus syndrome) Thiscase presents an additional previously unreported find-ing of delayed dental development in a patient withGorlin syndrome.
Literature reviewGorlin syndrome is inherited as an autosomal domi-
nant trait with a high degree ofpenetrance and variableexpressivity.5 The disorder has a population prevalenceof 1 per 57,000 people, with a 3:1 male sex predilec-tion. 6 There are more than 40 different diagnosticfindings associated with Gorlin syndrome. The bestknown feature is the presence of multiple basal cellcarcinomas, which typically appear between pubertyand 35 years of age,7 covering the trunk, neck, cheeks,nose, and eyelids of affected individuals.3 The numberof these lesions can vary from a few to several thou-sand, varying in size from 1 to 10 mm in diameter.7
The second most common diagnostic finding inGorlin syndrome is the presence of multiple odonto-genic keratocysts (OKCs), which occur in up to 75%of all cases. These cysts have a peak occurrence in thesecond and third decade of life and are more commonin the body and ramus of the mandible (80%) than the maxilla. The OKCs may vary in size, be found sin-gularly or in groups, and be unilateral or bilateral.5 Inyoung patients, the OKCs can cause displacement ofdeveloping permanent teeth, expansion of the bone, beassociated with an unerupted tooth, and occasionallycause root resorption.6
Radiographically, the OKC appears as a well-cir-cumscribed radiolucency with smooth or scalloped
margins and a thin opaque border. They may be ei-ther unilocular or multilocular in appearance.5
The OKCs have been reported to have a recurrencerate of between 20 and 60%, with a peak recurrencerate within the first 5 postoperative years.8 Treatmentof odontogenic keratocysts usually includes completeenucleation with aggressive curettage to ensure removalof accessory daughter cysts that can be found in andadjacent to the walls of the parent cyst.9
The skeletal components of patients with Gorlinsyndrome include a characteristic marfanoid appear-ance as well as frontoparietal bossing, a low occiput,and mild hypertelorism. More than 85% of patient’swith Gorlin syndrome exhibit lamellar calcification ofthe falx cerebri. Additional skeletal defects may includeanteriorly splayed, fused, partially missing, hypoplas-tic, or bifid ribs.1°
The neurologic anomalies associated with Gorlin syn-drome are agenesis of the corpus callosum, congenitalhydrocephalus, bridged sella turcica, medulloblastoma,seizure activity, and mental retardation.~°
The dental components of Gorlin syndrome includethe odontogenic keratocysts of the jaws, mandibularprognathism, and/or cleft lip and palate.6 While manyof these findings will be found in conjunction withdelayed dental development, to date there have beenno reports of patients with Gorlin syndrome who havesignificantly delayed dental exfoliation, eruption, anddevelopment as a component.
Case reportA 14-year, 9-month-old Caucasian male presented
to the University of Maryland Pediatric DentistryEmergency Clinic complaining of increasing difficultywith chewing. A review of the patient’s past medicalhistory was unremarkable.
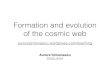
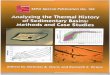
On physical examination, the patient was found tohave an asymptomatic expansile swelling of unknownduration in the left anterior maxilla (Figs 1, 2), whichwas causing an extraoral obliteration of the patient’sleft nasal cheek fold. No signs of trigeminal or facialparasthesia were observed.
The patient exhibited significantly delayed dental ex-
Pediatric Dentistry-20:5, 1998 American Academy of Pediatric Dentistry 355

Figure 1: Preoperative clinical photograph of maxillary anteriorcyst—occlusal view.
Figure 2: Preoperative clinical photograph of maxillary anteriorcyst—lateral view.
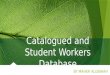
Figure 3: Preoperative panorex radiograph showing maxillary anteriorradiolucency, maxillary left and right posterior expansion between thesecond and third permanent molars, delayed dental development anddilacerated root on the mandibular right lateral incisor.
foliation, eruption, and development for a 14-year, 9-month-old Caucasian male. The maxillary right firstand second primary molars, mandibular left first andsecond primary molars, and mandibular right secondprimary molar were all over-retained and nonmobile.There was no clinical evidence of the permanent leftmaxillary lateral incisor, cuspid, or second premolar.The patient's maxillary left permanent first premolarwas found to be partially erupted and exhibited ClassII mobility. The patient's permanent second and thirdmolars were not clinically visable, nor was there anyevidence of the patient's mandibular right lateral inci-sor or cuspid.
Additionally, on physical examination, the patientwas found to have several palmar and plantar pitsas well as mild frontoparietal bossing. The patient'smother exhibited multiple basal cell carcinomasabout the head and neck, although none were foundon the patient.
On radiographic examination Fig 3, a 3.0 x 2.5-cmradiolucency with poorly defined borders was seen inthe left anterior maxilla, which was causing significantdisplacement of the adjacent permanent left lateral in-cisor and cuspid, without evidence of obvious rootresorption. In addition, there was superior and lateraldisplacement of the floor of the maxillary sinus in theanterior region. The posterior wall of the maxillaryanterior cyst was shown to have displaced the root ofthe maxillary left first premolar distally and laterallyover the developing second premolar, preventing thesecond premolar from erupting.
The Panorex® also revealed a bilateral expansionbetween the impacted maxillary second and third mo-lars, with a poorly defined radiolucency surroundingthe maxillary left third molar. In addition, there ap-peared to be a pericoronal radiolucency associated withthe unerupted mandibular permanent right canine.The mandibular permanent right lateral incisor wasimpacted and found to have a dilacerated root, whichwas preventing its eruption.
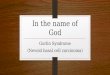
Based on these previously undiagnosed findings, thepatient was referred to the Oral-Maxillofacial Surgeryservice at the University of Maryland Hospital. As partof the patient's surgical work-up a head and neckCT scan was ordered, which revealed three separate,well-defined cystic areas of bone expansion in theleft posterior, left anterior, and right posterior max-
illa (Fig 4).The patient's lateral skull film showed a calcified falx
cerebri and his chest film revealed evidence of a bifur-cation in the right seventh rib. Vertebral examinationrevealed no spinal deformities or abnormalities.
In addition to the patient's generalized delayed erup-tion of permanent teeth and delayed exfoliation ofprimary teeth, the unerupted permanent teeth appearfully developed on radiographs without any subsequent
356 American Academy ofPediatric Dentistry Pediatric Dentistry - 20:5, 1998

primary tooth root resorption. A differential diagnosisfor these dental findings may include systemic diseasessuch as hypothyroidism, hypoparathyroidism, hypopi-tuitarism, or Albright's hereditary osteodystrophy(pseudohypoparathyroidism). The patient's baselinelaboratory studies were all within normal limits; how-ever, the patient needs to be referred for a morethorough endocrine work-up before these systemic dis-eases can be eliminated as possible etiologies for thedental presentation.
The patient's left maxillary anterior lesion was sub-sequently biopsied and sent for histologic evaluation.A differential diagnosis was developed including pri-mordial cyst, dentigerous cyst, ameloblastoma,adenomatoid odontogenic tumor (AOT), odontogenicmyxoma, calcified odontogenic cyst, and calcifying epi-thelial odontogenic (Pindborg) tumor as well as OKC.9
Figure 4: Computed tomography (CT) image revealing three separate,well-defined areas of bone expansion in the left posterior, left anterior,and right posterior maxilla. The left anterior cyst contains the left lateralincisor and canine.
Figure 5: Maxillary anterior cyst with accessory daughter cysts afterremoval.
The results of the biopsy confirmed that the specimenwas an odontogenic keratocyst.
This patient's history and physical examination re-vealed three major (multiple OKCs, palmar/plantarpits, and calcified falx cerebri) as well as two minor(bifid rib and frontoparietal bossing) diagnostic crite-ria to satisfy the diagnosis of Gorlin syndrome."
The patient was admitted to the hospital for totalcyst enucleation with aggressive currettage which wasperformed under general anesthesia. The surgical pro-cedure included removal of the patient's maxillary leftand right posterior cysts along with the impacted sec-ond and third molars associated with them. Themaxillary left anterior cyst was removed along with thelateral incisor and cuspid that were contained withinthe cyst cavity. Several accessory daughter cysts wereremoved adjacent to the wall of the maxillary anteriorparent cyst Fig 5.
The five over-retained primary molars were re-moved, as well as the dilacerated mandibularlateral incisor. The pericoronal radiolucency associatedwith the unerupted mandibular permanent right caninewas believed to be a hyperplastic dental follicle, notan early OKC, and the decision was made to followit on recall. The patient was discharged thefollowing day having tolerated all procedures well with-out complications.
The patient was seen in the Pediatric Dental Clinicat the University of Maryland Dental School for anevaluation 1 week postoperatively and found to behealing well. There was significant mobility associatedwith the maxillary left first premolar, however, splinttherapy was not recommended due to the patient'spostoperative level of discomfort as well as the longspan needed between abutment teeth in order toachieve proper immobilization. The patient was givenhome care instructions and was to be seen in the clinic3 months postoperatively for prosthetic and orthodon-tic evaluations.
The patient did not present to the clinic for his 3-month recall appointment and all attempts to locateand contact the patient have been unsuccessful. At thispoint, the patient is currently lost to any follow-up.
DiscussionGorlin syndrome is a rare but significant entity that
affects the cranial, maxillofacial, cutaneous, and mus-culoskeletal systems of the body. The management ofpatients with Gorlin syndrome depends on the specificdefects, anomalies, and pathologic findings which aremanifested and to what extent they are expressed.
The dental findings of patients with Gorlin syn-drome include odontogenic keratocysts, mandibularprognathism, and/or cleft lip and palate.4 While manyof these dental conditions may be associated withdelayed dental and oral development, there has not pre-
Pediatric Dentistry -20:5, 1998 American Academy of Pediatric Dentistry 357

viously been a report of a patient with Gorlin syndromewith delayed primary tooth exfoliation and permanenttooth eruption as a significant dental finding.
This patient’s dental findings may be a manifesta-tion of a systemic disease, and not at all related toGorlin syndrome. Additional endocrine studies arenecessary in order to completely eliminate the possi-bility of hypothyroidism, hypoparathyroidism,hypopituitarism, or Albright’s hereditary osteodystro-phy as possible etiologies. Additionally, the patient’sunusual dental presentation may merely be a coinci-dental finding, and not at all associated with thepresence of Gorlin syndrome. More patients withGorlin syndrome will have to be evaluated by pediat-ric dentists and endocrinologists in order to confirmthis finding.
While this patient has currently been lost to follow-up, it is anticipated that the dentition will continue todevelop. The maxillary left first and second premolars,which were found outside the wall of the anterior cyst,were retained in the hope that the cavity would fill inwith bone. The first premolar would then continue toerupt and could be orthodontically repositioned. Thiswould allow for the normal eruption of the patient’smaxillary second premolar and a more stable arch formwith less severe prosthetic consequences. Eventually,the patient’s posterior occlusion and anterior segmentcan be properly restored using an implant retainedprosthesis or a removable partial denture. As this pa-tient is currently lost to follow-up, I can’t state whatdental events actually occurred.
A patient with Gorlin syndrome should be moni-tored annually by a dental and medical team to evaluatefor potential cyst recurrences, new cyst formations,and/or the development of basal cell carcinomas thatmay require additional treatment.12
Because of the multisystem involvement and vari-able expressivity of Gorlin syndrome, these patientsmust be evaluated by many medical and dental special-ists in order to properly sequence their treatment. Asmany of these patients will be seen and subsequently
diagnosed by pediatric dentists, a thorough understand-ing of the various components of the syndrome isessential. Delayed dental development in a patient withGorlin syndrome is a new finding that requires atten-tion and appropriate management in order to providethe patient with comprehensive treatment.
Dr. Rosenblum was previously a resident in pediatric dentistryat the University of Maryland at Baltimore, School of Dentistry,Baltimore, Maryland and is currently in private practicewith "Children’s Dentistry and Orthodontics" in ViriginaBeach, Virginia.
References1. Ruprecht A, Austermann KH, Umstadt H: Cleft lip and pal-
ate, seldom seen features of the Gorlin-Goltz syndrome.Dentomaxillofac Radiol 116:99-103, 1987.
2. Gorlin RJ, Vickers RA, Kelln E, Williamson JJ: The mul-tiple basal-cell nevi syndrome. Cancer 18:89-104, 1965.
3. Goodman RM, Gorlin RJ : Atlas of the Face in Genetic Dis-orders. CV Mosby Co, St. Louis, 166-67, 1977.
4. Gorlin RJ: Nevoid basal cell carcinoma syndrome. DermatolClin 13:113-24, 1995.
5. Lovin JD, Talarico CL, Wegert SL, Gaynor LF, Sutley SS:Gorlin’s syndrome with associated odontogenic cysts. Pedi-atr Radiol 21:584-87, 1991.
6. Gorlin RJ: Nevoid basal-cell carcinoma syndrome. Medicine66:98-113, 1987.
7. Crean SJ, Cunningham SJ: Gorlin’s syndrome: main featuresand recent advances. Br J Hosp Med 56:392-97, 1996.
8. Mustaciuolo VW, Brahney CP, Aria AA: Recurrentkeratocysts in basal cell nevus syndrome: review of the lit-erature and report of a case. J Oral Maxillofac Surg 47:870-73, 1989.
9. Regezi JA, Sciubba JJ: Oral pathology. WB Saunders, Phila-delphia, 313-17, 1989.
10. Esposito SJ, Kast G, BradrickJP: Basal cell nevus syndrome:a clinical report. J Prosthet Dent 73:405-410, 1995.
11. Evans DGR, Ladusans EJ, Rimmer S, Burnell LD, ThakkerN, Farndon PA: Complications of the naevoid basal cell car-cinoma syndrome. J Med Genet 30:460-64, 1993.
12. Frledlander AH, Herbosa EG, Peoples JR 3d: Ocularhypertelorism, facial basal cell carcinomas, and multipleodontogenic keratocysts of the jaws. J Am Dent Assoc116:887-89, 1988.
358 American Academy of Pediatric Dentistry Pediatric Dentistry - 20:5, 1998