-
8/9/2019 Delay, Denial and Dilution
1/55
Delay, Denial and Dilu t ion
The Im pact of NH S Ra tioning on
Hear t Disease an d Cancer
-
8/9/2019 Delay, Denial and Dilution
2/55
-
8/9/2019 Delay, Denial and Dilution
3/55
IEA Hea lth a nd Welfar e Unit
Choice in Welfa re No. 55
Delay, Denia l and Dilu t ion:
The Impact of NH S Ra t ion ing onHear t Disease a nd Cancer
David G. Green
Lau ra Casper
IEA Hea lth a nd Welfar e UnitLondon
-
8/9/2019 Delay, Denial and Dilution
4/55
First published J an ua ry 2000
IEA Hea lth a nd Welfar e Unit
2 Lord N ort h StLondon SW1P 3LB
IEA Health an d Welfar e Unit 2000
All rights reserved
ISBN 0-255 36459-8ISSN 1362-9565
Typeset by the IE A Hea lth a nd Welfar e Unit
in New Century Schoolbook
Pr inted in Great Britain by
St Edmu ndsbury Press
Bury St E dmu nds, Su ffolk
-
8/9/2019 Delay, Denial and Dilution
5/55
ContentsPage
The Au thors vi
Foreword
Terence Kealey vii
Preface ix
In t roduct ion 1
Diseases of the Circula tory System 5
Cancer 21
Conclusions 33
Figures
1. Coronary Hear t Disease Dea th Ra tes for MenAged 35-74 per
100,000 Populat ion (1993 or 1994)
Selected Count r ies 6
2. Isch a em ic H ea r t Disea se,
Dea ths Per 100,000 Popula t ion , 1995 7
3. F ive-yea r Sur viva l Ra tes for Lun g Ca ncer Pa tien ts
24
4. One-yea r Surviva l Ra tes for Lung Cancer Pa t ients 24
5. F ive-yea r Surviva l for Breast Cancer Pa t ient s 266. F
ive-yea r Surviva l for Recta l Cancer Pa t ien ts 27
7. F ive-yea r Surviva l for Colon Cancer Pa t ients 27
8. F ive-yea r Surviva l for Ovar ian Cancer Pa t ient s 30
Notes 36
-
8/9/2019 Delay, Denial and Dilution
6/55
vi
The Aut hors
David G. Gree n is the Director of th e Hea lth an d Welfar e Un
it
a t the In st itu te of Economic Affa irs. His books include
Power and
Party in an English City, Allen & Unwin, 1980; Mutual Aid
orWelfare S tate, Allen & Unwin, 1984 (with L. Cromwell);
Working-
Class Patients and the Medical Establishment, Temple Smith/
Gower , 1985; T he N ew Right: The Counter R evolution in
Political,
Economic and Social Thought, Wheatsheaf, 1987; Reinventing
Civil S ociety, IEA, 1993; Com m un ity Without Politics, IEA,
1996;
Benefit Dependency, IEA, 1998; and An End to Welfare Rights,
IE A, 1999.
He wrote th e chapter on The Neo-Libera l Per spective in TheS
tu dents Com pan ion to S ocial Policy, Blackwell, 1998.
Laura Casper lives in Wisconsin a nd is cur ren tly stu dying a
t
Trin ity College, Hart ford, Conn ecticut . She worked a s a
resear ch
assistant at th e IEA Health an d Welfare Un it dur ing the summ
er
of 1999.
Terenc e Kealey lectu res in clinica l biochem istr y a t Ca
mbridgeUniversity a nd is an honora ry consu ltan t chem ical pat
hologist at
Adden brookes H ospit a l.
-
8/9/2019 Delay, Denial and Dilution
7/55
vii
Foreword
When in 1987 I toured t he un iversity teaching hospital in
Aachen,
Germa ny, th e Director boast ed of h is 80 per cent bed occupa
ncy
ra te. I wa s su rprised. But my hospita l I sa id has a 100 per
centbed occupa ncy ra te.
You do not u nder st and he sa id. We ha ve two other big
hosp-
itals in Aachen, one ha s a bed occupa ncy of 70 per cent an d t
he
other of only 60 per cen t .
In Germ an y, as in m ost coun tr ies of western E ur ope, th
ere a re
no waiting lists. Hospita ls compete for pa tien t s, the pr
ofessiona l
sta ff is cont ent , and facilities are modern . In Br ita in,
on t he oth er
ha nd, as Ca sper and Green demonstr at e in th is rema rka ble
book,th ere a re wait ing list s for th e wait ing lists. Moreover,
neither our
doctors nor our nu rses ar e cont ent , and t he facilities ar e
poor.
Brita ins health service is almost u nique. Whereas th e coun tr
ies
of western Eu rope ha ve crea ted system s of hea lth car e
based on
privat e insu ra ncebut un derpinn ed by th e stat e to ensur e
tha t
th e poor a re n ot n eglectedwe in Brita in u se a system
modelled
on Lenins dr eam of universa l free provision , an d so, in t he
midst
of an expanding and prosperous economy, we in Britain have
nu r tu red an island of Soviet socialism. How well does it
work?Not very well. For decades, the faults of the NHS have
been
obscured by the general improvements in health that our in-
crea sed prosperity, impr oved nu tr ition a nd bett er housing
have
crea ted , but n ow tha t we are prosperousnow tha t life and
dea th
depend on h ospita ls, doctors a nd n ur ses ra th er t ha n on
sewers,
agricultu re a nd accomm odat ionthe ina dequa cies of our hea
lth
delivery are increasingly being exposed. For years, people
have
been reluctan t to sha tt er our faith in t he envy of th e
world (a nenvy so envious th a t p ractically nobody has copied u
s) but in t his
courageous book Casper and Green have chronicled how poorly
the NHS does, in fact, serve the sufferers from the common
diseases of our time. Nationalisation works no better in
health
th an in telephones.
Beveridge didnt m ean it to be this way. In h is fam ous Report
,
published in December 1942, he a pplaude d t he phen omen al
growth of volunt ar y insu ra nce against sickn ess, an d
indeed, by
-
8/9/2019 Delay, Denial and Dilution
8/55
DELAY, DEN IAL AND DILUTIONviii
1938, th e 1,334 volunta ry hospita ls of Brita in r eceived 59
per cent
of their income from pa t ient s fees, pa id either directly or
via
private health insurance organised by institutions such as
the
Brit ish P roviden t Associat ion.
Beveridge wanted to foster the growth of private medical
insurance, and he wanted to restrict the state only to
under-
pinn ing pr ovision for th e poor, bu t Nye Bevan (a squa lid n
ui-
san ce as Winston Ch ur ch ill once described him) was determin
ed
on nationalisation on the Soviet modeland in a classic case
of
crowding out, his universal free provision destroyed private
hea lth car e for m ost people.
Of cour se, UK hea lth car e is cheap . We spend less on h ealth
car eth an does an y compa ra ble na tion, but th e cheapn ess of
th e NHS
is subsidised by the exhaustion and demoralisation of the
staff
and by the second-rate service it so often provides. It is
the
chea pness of th e miser who knows the price of everyth ing and
t he
value of noth ing. And it is a cheapness t ha t dem eans pat
ient s a s
supplicants and which hides the medical realities of
rationing
from th em.
Nobody wants to be told to pay more for anything, so thepolitica
l par ties now collude with th e people of Brita in in pr eten
d-
ing they ha ve crea ted a perpetua l motion ma chinea ma
gical
inst rum ent for conjur ing truly free h ealth care out of a
politician s
fiat. But th e rea lity is that , after rea ding th is book,
people will
want better t reat ment , and t hey will wan t t o find the m
oney.
Yet, and th is ha s emerged a s a n iron law of our time, people
will
not pay h igher ta xes. They will, however, pa y for pr ivat e
goods, so
we must now invent a system th at lowers the bar riers
between
the private and public sectors, to reward private payers for,
inBeveridges words , the du ty an d plea su re of th r ift .
Put simply, we should copy the German system, but if that
policy appea rs t oo eur oph iliac for some, we sh ould copy the
Swiss
system inst ead (its a lmost iden t ica l). Nobody would want to
copy
th e Amer ican s, so let u s recognise tha t h ealth is one a
rea where
th e Cont inent als do better t ha n th e Anglophones.
In rea lity, it is the Germa n h ealth care system t ha t is the
envy
of the worldor it would be, if th e world were bet ter inform
ed.Than ks t o Casper a nd Green, it now is.
Terence Kealey
-
8/9/2019 Delay, Denial and Dilution
9/55
ix
Preface
It is often s aid th at , despite the fact th at British
expenditur e on
health care is low by international standards, the British
National Health Service produces good medical outcomes. Inrecent
year s it ha s become obvious t ha t t here is r a tioning, but t
he
examples which h ave received most public a tt ent ion h ave
affected
relatively small groups, such as people suffering from
multiple
sclerosis or male impotence. The NHS could conceivably be
st ruggling to meet th e needs of such specia l groups with ou t
being
fun dam ent ally flawed, and a fa irer m easu re of its su ccess
would
be to look a t th e impa ct of th e NHS on th e killer diseases
which
affect the most people. We therefore looked at the two
maincauses of premature death: diseases of the circulatory
system
(responsible for 40 per cent of prem a tu re dea th s in men a
nd 30
per cent in women) an d cancer (the second biggest killer). J
ust
how well does t he N HS do compa red with similar coun tr
ies?
Than ks a re due to Laur a Ca sper, who worked a t t he IEA as
a
research assistan t du ring the sum mer of 1999 an d produced
such
good work th at I felt it only right to ma ke h er a co-au th
or. I h a ve
also benefited from t he resea rch a ssista nce of Selina J
ones, BenBrowning a nd Kat her ine Russell, all of whom did a fine
job. Ben
Browning deserves to be singled ou t for h is invalua ble
help.
The finished product was mu ch improved by th e comm ent s
of
Lord McColl, J im Th orn ton, Robert Whelan an d t wo an
onymous
referees. Needless to say, any remaining errors, omissions
or
oversight s a re en tirely my fau lt.
David G. Green
-
8/9/2019 Delay, Denial and Dilution
10/55
1
Introduction
T he NHS is efficient . We spend less on h ea lth a s a p roport
ionof GDP th an ma ny oth er coun tr ies, but th e results a re
justas good. Such claims a re comm on, but is it tr ue t o sa y tha
t t he
NHS produces good resu lts for pa tien ts? This st udy exam ines
the
impa ct of th e NH S on th e two ma in killer diseases. Among
both
men and women the biggest cause of death is diseases of the
circulatory system, followed by cancer. Among diseases of
the
circula tory system, we focus on corona ry hea rt disease and st
roke.
We look a t four cancers : brea st cancer, th e most common
cancer
for females; lung cancer, the most common for men;
colorectal
ca ncer, th e second most comm on fat al m aligna ncy in both
sexes
combined; and ovaria n can cer, th e four th most comm on am
ongst
women . Does t he NH S r a tion pr ovision for people su ffering
from
these conditions? And if so, does it make any difference to
the
resu lts for pa tient s?Until recently, the existence of
explicit rationing by the NHS
was consist ently den ied. All decisions were supposed to be
clinica l
ra th er t ha n fina ncial. There was priority setting but not
ra tion-
ing. Such claims h ave become increasingly implau sible,
however,
as the number of doctors complaining about rationing has
increased.
J ust as th e out right denial of ra tioning has become less
tena ble,
so defenders of the NHS have tried to offer a more
positivedefence. Instead of claiming that all decisions are
clinical, they
ar gue th at medical r at ioning is a virt ue, so long a s
decisions ar e
based on legitima te grounds. Typically they asser t, not only
th at
ra tioning exists, but also th at it is una voidable. Invar
iably th ey
object to medical paternalism and suggest one of four main
alter na tive (somet imes overlapping) ra tiona les.
One group argues that rationing should be given democratic
legitimacy, through devices such as opinion surveys and
citizen
-
8/9/2019 Delay, Denial and Dilution
11/55
DELAY, DEN IAL AND DILUTION2
juries.1 A second group dem ands evidence-based m edicine.
Only
medical procedures based on scientific evidence should be
provided by the NH S. The Na tiona l Inst itut e for Clinical E
xcel-
lence (NICE ) is a consequen ce of th is line of r easoning. A
third
group em phasises cost -effectiveness.2 In pra ctice, th ey ar e
closely
linked to enthusiasts for evidence-based medicine, but not
all
champions of scientific evidence attach the same weight to
cost
minimisation. And a fourth group has urged that treatment
should be m ade available according to the qu a lity of life
gained by
patients. The Quality Adjusted Life Year (QALY) has probably
been t he most debat ed of such a ppar ent ly technical
devices.3
These enthusiasts for openness and explicit rationing have inth
eir tu rn come u nder str ong criticism by writer s such as Da
vid
Hunter 4 and Rudolf Klein,5 who have t ended t o debun k ra
tiona l
ra tioning. The pu rpose of th e present study, however, is not
to
enter int o that debat e, but t o form a clearer view about the
extent
of ra tioning on t he t wo biggest cau ses of dea th in the UK,
diseases
of the circulat ory system an d cancer.
Before going an y fu rt her it may be advisable to clar ify wha
t we
mean by rationing. It is inevitable that words will take
onalternative meanings in different contexts, but it is rather
import an t t ha t a ny one word should mean th e sam e thing
dur ing
the course of any single argument. We follow Rudolf Klein in
distinguishing between pr iority sett ing and rat ioning.6 If a
service
is fina nced from t axes, t he government will inevita bly be gu
ided
by pr iorit ies when it a ppor tions some of th e na tional
budget to th e
NH S or elemen ts with in it. We do not call th is process r at
ioning,
but when individual doctors, working within their
assignedbudgets, make decisions about the treatment of
individual
pat ient s, th en we speak of ra tioning.
Measur es of Ra t ioning: Denia l , Dela y a nd Di lut i on
One example which has received attention in the press and
specia list jour na ls is the denial of cancer care, so much so
th a t t he
Pr ime Minister himself becam e involved. The most au th orita
tive
estimate has been made by Professor Sikora, head of the WHOcan
cer program me, who calculat ed that th ere could be as ma ny
as
-
8/9/2019 Delay, Denial and Dilution
12/55
INTRODUCTION 3
25,000 unnecessary deaths in the UK every year because of
under -provision. We can also compa re t he r at e at which ca r
e is
den ied t o people su ffering from kidney fa ilu re. A recent su
rvey of
rena l specialists in Can a da, th e US a nd t he UK found tha t
12 per
cent of UK specialists sa id th ey had refused tr eatmen t to
patient s
because of limited resources. The rate of provision between
the
three countries varied substantially. In 1992, 65 patients
per
million population (pmp) were accepted for dialysis in the
UK,
compared with 98 pmp in Canada and 212 pmp in the US.7
According to another study, by 1995 th e figur e for En glan d
was 82
pmp, significantly less than the rate in comparable European
coun t ries, where a ccepta nce rat es of over 100 pm p were
common.The authors estimated that the rate in England should
exceed
100 pmp t o meet esta blished need.8
Often tr eatm ent is n ot with held altogeth er, but it is
delayed,
somet imes with th e resu lt th at th e pat ients condition
worsens.
There ar e measu res of delay, not least th e waiting lists ,
although
th eir impact on outcomes is not a lways clear cut . The
National
S urvey of NHS Patients, published by th e Depar tm ent of Hea
lth,
is also a useful guide. It foun d th at one in t en pa tient s
were seenby a specialist on th e sa me day a s t hey were referred
by their GP.
About 50 per cent h ad to wait over a mont h a nd 20 per cent m
ore
th an th ree months. Over one in t hr ee of th ose waiting said
tha t
th eir condition had got worse while th ey were waiting an d 14
per
cent claim ed t o be in a lot of pa in. Over 50 per cent report
ed th a t
their condition limited their daily activities and ability to
work
and, not surprisingly, of the men of working age (16-64),
half
th ought th ey should ha ve been seen sooner .9
The wa iting list h as been t he focus of mu ch political a tt
ent ion
since th e Government s election pledge to cut it. It s effort s
have,
however, led to continuing claims tha t it wa s fiddling the
figur es.
One ploy used by some hospitals to avoid going over the 18-
month s th reshold is t o call in pat ient s who ha ve been wa
iting for
nearly 18 months for a check-up. If they are put back on the
wait ing list t he clock st ar ts ticking from zero, th us
concealing t he
rea l waiting time. Moreover, the Govern men t wa s forced in th
esum mer of 1999 to acknowledge tha t its r eduction in th e
waiting
list had been achieved by increasing the time it took to see
a
-
8/9/2019 Delay, Denial and Dilution
13/55
DELAY, DEN IAL AND DILUTION4
consult ant in t he first place. Ther e was now a waiting list
for t he
wa iting list .
Care may also be diluted by not providing the optimal treat-
ment. This often happens when new but expensive remedies
become a vailable. Again, demons tr a ting the impa ct of
diluted care
on out comes is not easy a nd systema tic evidence is n ot rea
dily
available. Moreover, there is invariably no clear-cut
agreement
am ong doctors a bout which tr eat men ts ar e appr opr iat e
or
opt ima l. We ar e not , however, wholly un able to judge
between
rival t rea tm ent s. A variety of organ isat ions have produced
clinical
guidelines, protocols and recommendations which enjoy wide
respect, eith er in t he U K or oversea s. If a given doctor or
h ospit alor system (such as the NHS) fa lls sh ort of a
well-respected clinical
guideline this const itut es at leastprim a facie eviden ce of
dilu t ion
and calls for further investigation. Among the official
organisa-
tions laying down benchmarks in the UK are the Clinical
Sta nda rds Advisory Group10 an d t he St an ding Medical
Advisory
Committee,11 and such work is to be stepped up through the
Commission for Health Improvement and the National Service
Frameworks.
-
8/9/2019 Delay, Denial and Dilution
14/55
5
1
Dise ase s of the Circu latory Syste m
Over 40 per cent of all deat hs ar e th e resu lt of car
diovasculardisease (CVD). The two main forms of CVD are coronaryhea
rt disease (including hear t a tt acks and an gina ) an d
cerebro-
vascu lar disea se (st roke). In 1996 just over half of all dea
ths from
CVD were from coronar y hear t disease an d a bout a quar ter
from
stroke.1
However, we must all die of somet hin g an d t he more rele-van
t figur e is for pr ema tu re dea th s, na mely th ose occur r
ing
before age 75. In 1996 ca rdiovascula r disease wa s r
esponsible for
over 40 per cent of prema tu re dea th s in men an d 30 per cent
in
women.2
The Governm ent adm its th at th e UK record is un sat
isfactory.
After allowing for the different age structure of each
country,
Saving Lives: Our Healthier Nation compa res dea th ra tes
from
circulatory disease for persons aged under 65 throughout the
European Union. Out of the 15 countries studied, the UK was
thirteenth.3
Corona ry Heart D isea se
Coronary heart disease (CHD) is the most common cause of
prem at ur e (un der t he a ge of 75) deat h in th e UK, accoun
ting for
28 per cent of prema tu re deat hs in m en a nd 17 per cent in
women
in 1996nea rly 60,000 prem at ur e deat hs in t ota l.4
For some year s now UK government s have officially sought
toreduce death s from coronar y hea rt disease,5 but CHD death r at
es
rem ain a mong the h ighest in th e world. The form er comm un
ist
countries tend to be the worst. As Figure 1 shows, the rate
for
men a ged 35-74 in La tvia in 1994 was 919 per 100,000 popu lat
ion
(age-standardised). In the Russian Federation it was 812 per
100,000; in Estonia, 744; Lithuania, 663; and Bulgaria, 352.
Compa red only with OECD count ries t he UK r ecord is also
poor
(Figure 2).
-
8/9/2019 Delay, Denial and Dilution
15/55
DELAY, DEN IAL AND DILUTION6
Figu r e 1
Corona ry Hea rt D isease Deat h Ra tes for Men Aged 35-74
p er 100,000 Pop ula t ion (1993 or 1994) Selected Count
ries
Japan
France
Australia
Germany
US
UKBulgaria
Lithuania
Estonia
Russian Federa tion
Latvia
Source: Coronary Heart Disease S tatistics, British H ear t F
oun dat ion, 1998,
p. 19.
Western coun tr ies an d J apa n t end to have lower ra tes. J
apa ns
figure is 49 per 100,000; Fra nce, 94; Canada , 212; Aus tr a
lia , 217;
German y, 237; an d th e US, 248 (in 1993). In t he U K th e r
at e of
325 per 100,000 in 1994 is closer t o the Bu lga ria n figur e.
Deat hra tes from CHD ha ve been falling in th e UK, but not as r
apidly a s
in some other countries like Australia, Sweden and the US.
Between 1983 and 1993 th e deat h r at e for m en in th e UK
fell by
30 per cent , compa red with 43 per cent in Aust ra lia , 41 per
cent
in Sweden an d 34 per cent in t he USA.6
However, the Health Survey for England and the General
Household S urvey suggest th at while deat h from CHD is
falling,
th e incidence ofill-health due t o CHD is n ot falling and ma y
in
fact be rising. Dra wing on a variety of sour ces, the British
Hea rtFounda tion (BHF ) estima tes th at appr oxima tely 300,000
people
-
8/9/2019 Delay, Denial and Dilution
16/55
DISEASES OF TH E CIRCULATORY SYSTEM 7
in the UK have a heart at tack each year and that about 1.4
million people have angina .7
Figu r e 2
Ischa emic Hear t Disease ,
Dea th s P er 100,000 Pop ula t ion, 1995
Source: OECD Health Data 1999 (CD)
Heart disease has major economic consequences as well ashu ma n
costs. CHD alone cost t he health car e system about 1.6
billion in 1996, with a bout 55 per cent going to hospita l ca
re a nd
-
8/9/2019 Delay, Denial and Dilution
17/55
DELAY, DEN IAL AND DILUTION8
32 per cent on th e cost of drugs. Only abou t one per cent of
such
costs were spent on the prevention of CHD. The British Heart
Foundation has estimated the total impact of CHD on the UK
economy t o be a bout 10 billion a year .8
The Adequa cy of CHD Treatm ent
CHD leads to the obstruction of the blood flow through the
coronary arteries to the heart muscle, due to fatty deposits
and
associated blood clots. An inadequate supply of
oxygen-enriched
blood to the h eart can dam age th e hea rt mu scle leading to
hear t
pain (angina) or to a heart attack (myocardial infarction)
that
may be fatal. CHD is influenced by several factors, not all
of
which can be altered. The genetic risk cannot be changed by
medical int ervent ion but cigar ette smoking, h igh blood
cholester ol
levels, ra ised blood pr essu re, obesity and lack of exercise
can a ll
be modified by lifestyle choices a nd /or medica l tr ea tm ent
.
The m ost comm on tr eatm ent is to take dru gs, although an
gina
can also be treated surgically, in the form of coronary
artery
bypass grafts (CABGs) or angioplasty.9 CABGs usu a lly
involve
grafting veins or ar ter ies (ta ken from th e leg) from t he a
ort a (amajor artery that takes blood from the heart to the rest of
the
body) to the corona ry a rt ery, th us bypassing th e obstructed
a rea .
Government targets have been set for CABGs. In 1986 the UK
target was 300 per million population (pmp). The number had
risen bet ween 1978 a nd 1985 from 57 pmp t o 225 pmp in
1987.
TheHealth of the N ation report of 1991 conceded t ha t th e t
ar get
of 300 pmp wa s significan tly below most ta rgets a dopted by
oth er
countries,10 and noted tha t even t his inadequate t arget had
not
been achieved. In 1990 the rate was only 278 pmp (15,967
operations) but by 1996 it had increased to 412 pmp (24,238
operations).11 At t he t ime, the British Car diac Society ta
rget was
600 per million popu lat ion.12
The UK rate compares very unfavourably with the US, where
598,000 CABGs were performed in 1996, at a rate of 2,255 per
million popu lat ion .13 The ra te for Austra lia was a bout 870
pm p;
Cana da, 582 pmp a nd Sweden, 736 pmp.14
Not only is t he overa ll ra te low, the Depa rt men t of Hea
lth alsoconcedes th at th ere ar e lar ge varia tions bet ween
differen t pa rt s
-
8/9/2019 Delay, Denial and Dilution
18/55
DISEASES OF TH E CIRCULATORY SYSTEM 9
of the country. Adjusting for age, the lowest figure was for
the
Nott ingha m H ealth Aut hority wher e only 40 bypa ss operat
ions
and angioplasties per million population were carried out.
The
highest rate was found in Brent and Harrow with 1,400 per
million.15 These local dispar ities ha d been ident ified by the
Aud it
Comm ission report of 1995, which ur ged health au th orities
with
rates below 300 pmp to give priority to increasing supply.16
Pr ogress h as been very slow.
The consequences ar e serious. A stu dy of Pa pwort h Hospita
l
found that deaths occur while patients are on waiting lists
for
CABGs. Moreover, for every one death on the waiting list
there
were between t wo an d th ree adverse car diac event s. The au
th orsconcluded th at th e high mort a lity an d complicat ion r at
es while
waiting were becau se resour ce limits mean t that pa tient s
tended
to be put on waiting lists only when th eir condition ha d
become
ur gent. They concluded t ha t ma ny UK pat ient s ar e referr
ed an d
investigated a t a critical sta ge in th eir disease a nd ar e
th erefore
at high r isk at th e time of invasive inter vention . This t
enden cy
suggested to the a ut hors t ha t t he su rgical t reat ment of
corona ry
hea rt disease in t he UK was more a form of crisis ma na
gementth an plann ed car e.17
Moreover , because of th e pr evalence of ra t ioning, doctors
ha ve
fallen into the habit of withholding treatment on
non-clinical
groun ds. In th eir 1993 report ,18 th e Clinical St an dar ds
Advisory
Group drew attention to the lack of clear criteria for
giving
priority to patient s waiting for coronar y ar ter y bypa ss su
rgery. In
response to this report, a regional workshop sponsored by
the
Northern Ireland Clinical Resource Efficiency Support Team
convened in t he spr ing of 1996 to gain a better un derst an
ding ofthe criteria used by doctors to assign priority to
particular
pat ient s. Many doctors made judgement s a bout the u rgency of
th e
pa tien ts cond ition, t ha t is th ey form ed a view about how
quickly
each pat ient should be tr eat ed in order to achieve a given m
edical
outcome. However, the study also found that demographic and
lifestyle cha ra cter isticssuch a s smoking, age, gender and
body
weightoften influenced doctors judgements on priority inde-
pendently of their beliefs about the probable effectiveness
ofsurgery.19 These findings are consistent with the
long-standing
-
8/9/2019 Delay, Denial and Dilution
19/55
DELAY, DEN IAL AND DILUTION10
practice of discrimina ting again st elder ly pa tien ts20 becau
se t hey
ha ve ha d a good inn ings, an d with th e a ckn owledged pr
actice of
discriminating against smokers, which is publicly defended
by
some doctors.21
High Blood Pr essure
The two main risk factors for CHD which are susceptible to
medical intervention are high blood pressure and the blood
cholesterol level. (Smoking is a personal choice and obesity
is
cont rollable in most cases th rough chan ges in diet a nd
exercise.)
How effectively is high blood pressure being dealt with by
the
NHS? High blood pressure or hypertension is usually a
symptomless condition which increa ses t he risk of stroke, hea
rt
failur e, hear t a tt ack and kidney failur e. It is th e most
import an t
risk factor for stroke. Because there are no symptoms in the
majorit y of cases, h igh blood pr essu re often goes u
ndetected.
When blood pr essur e is mea sur ed two figur es ar e recorded:
the
highest occur s when th e hea rt cont racts (systolic); and t he
lowest
when th e hea rt relaxes between beat s (diast olic). Blood pr
essur e
is usually written with the higher number first, for example
160/95 mmHg. The mean systolic blood pressure for men in
England is about 139 mmHg and for women 134mmHg. The
British Hear t Foundat ion defines individua ls as h yperten
sive if
th eir systolic blood pr essur e is more th an 160 mm Hg an d th
eir
diastolic blood pressure is more than 95 mmHg.22 There is no
clear m edical consen sus about t he point at which blood pr
essur e
is high enough to warrant intervention, although it is
accepted
th at th e higher t he blood pressure th e great er th e
risk.Trea tm ent involves a combina tion of lifestyle changes an d
dru g
therapies.23 Lifest yle changes genera lly come first . People
who ar e
overweight are strongly advised to lose weight and smokers
to
give up. Changes in diet, especially for those with high
blood
cholesterol levels or complications such as diabetes, are
also
str ongly recomm ended. Reducing sodium an d sa lt int ake, with
out
redu cing th e consu mpt ion of calcium, m agnesium or pot a
ssium,
and reducing alcohol int ake a re a lso highly
beneficial.Medically, a comm on first step is a th iazide diur
etic. This gr oup
-
8/9/2019 Delay, Denial and Dilution
20/55
DISEASES OF TH E CIRCULATORY SYSTEM 11
of dru gs works by helping th e kidneys to elimina te sa lt a nd
water,
which decrea ses fluid in th e body th us lowering blood pr
essur e.
Thiazide diuretics also cause blood vessels to dilate,
increasing
their capacity and lowering blood pressure.
Another appr oach is to block some of the bodys na tu ra l
defence
mecha nisms. Under str ess, or in moment s of dan ger, th e
sympa-
thetic nervous system temporarily increases blood pressure
to
cope with threats and releases hormones, such as adrenalin,
which stimu lat e t he hear t an d blood vessels. Adrenergic
blockers,
the most common of which are the beta-blockers, reduce the
effects of th e sympa th etic ner vous system .
A th ird approach is to use angioten sin conver ting enzyme
(ACE)inh ibitors, which lower blood pressu re by dilat ing the ar
ter ies.24
It is now widely acknowledged th a t ACE inhibitors ar e
effective
an d safe remedies when u sed appr opriat ely. For exam ple, it
is the
recomm endation of the North of England ACE-inhibitor
Guideline
Developmen t Group th at all patient s with symp tomat ic hea
rt
fa ilur e a nd evidence of impa ired left vent ricula r function
a s well
a s those with a r ecent myocardia l infa rct ion and evidence
of left
ventr icular dysfunct ion should be t reated with an
ACEinhibitor.25 The great majority of adults with heart failure
have
left vent ricular dysfun ction. H owever, a stu dy car ried out
by the
group foun d th at only 20-30 per cent of pat ient s with hea rt
failure
were being prescribed an ACE inh ibitor.26
This finding is similar to th ose of two Scott ish studies. The
fir st ,
by the Scotland Health Purchasing Information Centre, found
th at an ACE inhibitor wa s being pr escribed for only ar oun d
one-
th ird of pat ient s diagnosed with hear t failur e in gener al
pra ctice
in Scotland and that, even when prescribed, patients often
received su b-opt ima l doses.27 The second st udy looked a t pa
tien ts
in the Gra mpian r egion an d found tha t , under t he m ana
gement
of general practitioners, less than half the patients
diagnosed
with heart failure took ACE inhibitors. Indeed, less than
one-
third of patients with a recent myocardial infarction took
beta
blockers, despite the fact that their use has achieved
mortality
reductions of 20 per cent following hea rt a tt ack.28
These pr actices compa re ba dly with th ose pr evalent oversea
s.One st udy of US pr actice between 1986 an d 1994 exam ined th
e
-
8/9/2019 Delay, Denial and Dilution
21/55
DELAY, DEN IAL AND DILUTION12
use of ACE inhibitors in combina tion with a d iuretic and d
igitalis.
Since 1987 it had been widely accepted that ACE inhibitors
improved survival for pa tient s with hea rt failure a nd sympt
om-
at ic left ventr icular dysfun ction. Of pa tient s who were h
ospita -
lised for heart failure in 1986 and 1987, 43 per cent were
pre-
scribed a n ACE inh ibitor, wherea s of th ose h ospita lised in
1992
an d 1993, 71 per cent were pr escribed an ACE inh ibitor.29
Not on ly is t her e evidence of under -use of valua ble t her
ap ies,
there is also evidence of inadequate diagnosis. There are
some
less common cau ses of hea rt failure, such as a or tic va lve
obstr uc-
tion, where ACE inhibitors are unhelpful or harmful, and
therefore accurate diagnosis is essential. Diagnosis is
greatlyaided by the ultrasound technique known as
echocardiography,
which can produce images of the heart and show how well the
mu scle is cont ra cting. It can u sua lly esta blish th e cau
se, an d
confirm th e pr esence of hea rt failure an d t hu s a llow th e
corr ect
use of drugs.30
However, a s tu dy of th e NHS in Scotlan d showed that only
30
per cent of hea rt failur e pat ient s in general pr actice were
given
echocardiography scans despite evidence from areas whereechoca
rdiogra phy wa s freely available th at import an t cha nges in
tr eat men t were required in 69 per cent of pat ients r eferr
ed.31
Moreover, echocardiography was not expensiveabout 45 per
scan in Glasgow. The Scotland Health Purchasing Information
Cent re (SHPIC) recommen ded provision of a one-st op car
diology
service, but in deference to th e NHS tr a dition of ra tion
ing, even
th ough such a service would be cheap a nd cost -effective, the
group
recommended a second-best option of a GP echocardiography
service in the hope of reducing by about two-thirds the
casesrequiring referr al to a hospita l.32
A second stu dy by t he North of England ACE-inh ibitor
Guide-
line Development Group dr ew similar conclusions. It foun d th a
t
most pa tients who were investiga ted for h ear t failur e ha d
a chest
X-ray and electr oca rdiogra m, while on ly a t hird ha d echoca
rdio-
graph y. Diagnosis by clinical assessm ent h ad been estima ted
to
be correct in only about half of cases when confirmed by
echocardiography.33
It recommended that diagnosis should bebased on either echocar
diograph y or ra dionu clide mea sur ement.34
-
8/9/2019 Delay, Denial and Dilution
22/55
DISEASES OF TH E CIRCULATORY SYSTEM 13
To sum up: the NHS does not have a very good record of
providing these tried and tested remedies. According to the
British H ear t F oun dat ion, based on t he 1996 Hea lth Su
rvey for
En glan d, over four out of ten men an d over one in th ree
women
with hypert ension were not r eceiving tr eat men t a nd, of th
ose th at
are treated, about a third remain hypertensive.35 Even the
Government has acknowledged that fewer than half of people
with high blood pr essu re a re tr eat ed successfully. In 1997,
42 per
cent of people with hyper ten sion were being trea ted su
ccessfully,
21 per cent were being t rea ted inadequa tely and 37 per cent
were
not being treat ed at all.36
Cholesterol
A second CH D risk factor is the blood cholest erol level.
Accord ing
to the Br itish Hear t F ounda tion, lowering blood cholesterol
levels
by one per cent r educes the r isk of CHD by about two to thr ee
per
cent.37
Cholesterol is a fat ty substa nce which can be foun d in severa
l
forms in the human body. When bound to proteins it forms
lipoprotein. Cholesterol and other fatty blood components
are
often called blood lipids a nd can be d ivided in to two groups:
low-
density lipoprotein (LDL) cholesterol and high-density
lipoprotein
(HDL) cholest erol. High levels of LDL cholest erol an d low
levels
of HDL cholester ol ar e a ssociat ed with an increa sed risk of
CHD.
A new class of cholesterol-lowering drugs, the st a t ins (HMG
CoA
reducta se inhibitors), a re able to reduce LDL cholester ol
levels by
more th an 20 per cent .38 The first tr ial to show tha t CHD
patients
treated with lipid-lowering drugs gained a survival advantagewas
the Scandinavian trial, published in November 1994.39 A
Scott ish t rial confirm ed th is resu lt40 an d subsequent ly a
t ota l of
22 pu blished randomised cont rolled tr ials of cholesterol
lowering
with statins have been pooled. Overall, they show that
statins
redu ce t he risk of CHD mort ality by about 25 per cent an d th
at
sta tin tr eat men t in older people is just as effective as in
m iddle-
aged adults.41
These findings have led to increased expenditure on statindrugs.
In 1993 expenditure was over 20m and by 1997 it had
-
8/9/2019 Delay, Denial and Dilution
23/55
DELAY, DEN IAL AND DILUTION14
risen to over 113m.42 Ent hu sias ts for cost -effectiveness h
ave a lso
found in favour of st a tin s. The net cost per life-year gained
with
sta tins of ar oun d 7,000, though qu ite h igh , compa res
favoura bly
with oth er int ervent ions curr ent ly provided by th e
NHS.43
To wha t extent ha s th e NHS a cted on t he kn own evidence?
The
British Cardiac Society conducted a national sample survey
to
assess the adequacy of hear t disea se tr eat men t. It foun d
th at the
recording and management of risk factorslifestyle, blood
pressu re, cholester ol, glucosea nd th e use of prophylactic
dru g
tr eat men t were less t ha n optima l. For exam ple, according
t o th e
Brit ish Hyper lipidaem ia Associat ions (BHA) guidelines, most
of
th e pat ients in th e sur vey should ha ve been at tempt ing to
lowerth eir LDL cholesterol eith er by dieta ry cha nge or drug
trea tm ent .
Of th e m inority of pat ients on lipid lowering tr eat men t,
over ha lf
wer e not a dequ a t ely cont r olled a ccor din g to t h e
BHA
guidelines.44
Anoth er st udy of th e prescr ibing of lipid lowering dru gs in
t he
Sout h E as t Tha mes Region foun d dra ma tic var iations. With
in a
single health authority, prescribing varied by 60-fold
between
practices, and across the region the variation was 98-fold.45
AScott ish st udy concluded t ha t lipid mana gemen t was lar
gely
neglected, despite the existence of local guidelines
advocating
cholesterol lowering for pa t ient s with CHD. The blood pr
essure of
93 per cent of pat ient s in th e survey ha d been m easur ed in
t he
previous th ree year s, wherea s t heir blood cholest erol level
ha d
been checked in only 26 per cent of cases during the same
period.46
Is th e err a tic provision t he resu lt of ra tioning or is it
bad clinica lpractice? Recent discus sion in t he m edical jour na
ls provides some
insights. In August 1997, the Sta nd ing Medica l Advisory Comm
it-
tee (SMAC) issued a dvice to health au th orities a nd GP s on t
he
use of sta tins. It recomm ended tha t an yone with a th ree per
cent
an nual risk of a heart at ta ck should be trea ted.47 This
meant that
about 3.4 per cent of those aged 35-69 in England were eligible
for
sta tins in addition t o th ose who ha d alrea dy experienced a
CH D
event.
48
However, Nick Fr eema ntle, Senior Resea rch Fellow at th eCentr
e for Hea lth Economics, subsequent ly at ta cked th e modest
SMAC guidelines in a n editoria l in th eBritish Medical
Journal
-
8/9/2019 Delay, Denial and Dilution
24/55
DISEASES OF TH E CIRCULATORY SYSTEM 15
as financially unsustainable. He pointed out that the SMAC
guidelines would mea n t ha t 8.2 per cent of th e populat ion
of th ose
aged 35-69 would h ave to be tr ea ted to fu lfil a ll th e pr
ior ities. In
th e War wicksh ire Health Aut hor ity alone, adh ering to th e
SMAC
guidelines would involve tr eat ing a bout 17,000 pa tien t s.
The cost
in Warwicksh ire would be a bout 8m, representing 20 per cent
of
its drug budget.49 Such concerns have not been confined to
Warwickshire, and t he resu lt ha s been substa nt ial un
der-use of
sta tins. As th e 1999 report of th e Audit Commission r ema rk
ed,
th ere wa s evidence th at dru g thera pies for pr event ing CHD
were
not being u sed a s m uch a s t hey u sefully could be.50
Hea rt At ta cks
The Audit Commission in 1995 suggested some performance
indicators for patients arriving at a hospital with chest
pain
and/or other symptoms of a heart attack. The ideal to aim
for
would be to carry out an electrocardiogram (ECG) within 15
minut es of ar rival and, when a myocardial infar ction is
suspected,
to administer th rombolytic th era py within 30 minu tes of ar
rival
(often ca lled th e door -to-needle t ime).51 These
recommendations
are often not achieved. Moreover, one survey found that a
significant minorit y of key hospita l ma na gers did not even
kn ow
wha t t heir a chievemen ts were. A sur vey of 500 tr ust cha
irmen ,
chief execu t ives, medica l directors and chief nur ses carr
ied out by
theHealth S ervice Journal an d the Health Qua lity Service ask
ed
respondents to give a yes or no response to the following
sta tem ent : At least 80 per cent of A&E pat ient s with
chest pains
ha d a car e plan initiated with in 30 minut es of ar rival.
Only 60per cent of cha irm en a nswered Yes, compa red with 47 per
cent
of chief executives, 57 per cent of medical directors and 70
per
cent of ch ief nu rses. The rema inder typica lly answered
Dont
kn ow ra ther than No.52
Car diac reh abilitat ion a fter h ear t a tt ack can also
significan tly
improve the quality of life and reduce mortality. The most
appropriate forms of rehabilitation combine exercise with
psychologica l and educat iona l services. Evidence from th ree
meta -an alyses involving over 4,000 patient s who ha d su ffered a
hea rt
-
8/9/2019 Delay, Denial and Dilution
25/55
DELAY, DEN IAL AND DILUTION16
attack suggests that cardiac mortality can be reduced by
20-25
per cent. However, many patients who might benefit do not
receive rehabilitation under the NHS. The York Centre for
Reviews and Dissemination found that, despite increases in
reh abilita tion in recent year s, service provision in 1998 fa
iled to
meet national guidelines for cardiac rehabilitation.
Moreover,
th ere were wide var iat ions in th e sta nda rd of provision,
reflected
in staffing costs which ranged from about 10,000 per year to
62,000 per year .53
St roke
St roke is the na tions th ird biggest k iller a nd lar gest
single cause
of severe disa bility.54 TheHealth S urvey for England
1996found
that 1.8 per cent of men and 1.6 per cent of women reported
a
history of stroke an d t ha t 8.6 per cent of men over th e a ge
of 75
and 7.5 per cent of women over 75 report ed a h istory of st
roke.55
However, theHealth S urvey for En gland relies on self-report
ing,
an d a m ore reliable estimat e ha s been m ade by Geddes an d
her
colleagues based on a survey of the North Yorkshire Health
Aut hority. The t eam est ima ted th a t 4.7 per cent of people
aged 55or more ha d su rvived a str oke: 80 per cent ha d su ffered
a single
st roke, 13 per cent , two str okes an d seven per cent , three
or m ore.
Some 23 per cent reported a full recovery and the remainder
experienced subsequent impairmen ts. The m ost prevalent
were
cognit ive (33 per cent ), problems with th e right limb (33 per
cen t ),
th e left limb (27 per cent ) and speech (27 per cent ). Some 55
per
cent sa id they needed help t o fu lfil one or more of ten
activities of
daily living. Overa ll th e st udy est ima ted th e prevalence
of stroke
in th e whole popula tion to be 1.47 per cent , more th an
double th e
estima te norma lly used by health au th orities (0.6 per cent).
They
estimat ed tha t 1.13 per cent of people ha d impairm ents an d
th at
0.62 per cent were dependent as a resu lt of th eir st
roke.56
Using da ta from t he Geddes su rvey, th e Str oke Association h
as
estima ted th at 82,000 people aged 55-64 ha ve a h istory of st
roke.
Overa ll, it th ought th at 764,000 people of all ages in th e
UK h ad
a h istory of st roke, of which some 53,000 ha d severe
disabilities
as a consequence.57
Str oke car e costs ar e considera ble. At presen t, expenditu
re on
-
8/9/2019 Delay, Denial and Dilution
26/55
DISEASES OF TH E CIRCULATORY SYSTEM 17
st roke ca re is concent ra ted on th e immediat e episode of
in-pa tient
tr eat men t a nd not on long-ter m car e. Overall, th e costs
of str oke
ca re were 2.3 billion in E ngland in 1995-96. This amount s to
5.8
per cent of NHS and social services expenditure. The cost of
longer-term care for surviving stroke patients is also high
and
likely to rise fur th er a s a resu lt of demogra phic cha
nge.58
Stroke care already has a strong evidence base. Over the
last
two decades a nu mber of small, ra ndomised cont rolled t rials
of
specialised stroke units have been conducted. They found
that
stroke units reduce mortality and disability compared with
management in acute general wards. No other treatment for
str oke h as demonstr at ed such large benefits.For example, a
stu dy published in 1994 compa red a str oke un it
and a general ward. Patients within the stroke unit
recovered
more quickly as determined by their activities of daily
living
scores. Patients were also discharged more rapidly from the
str oke u nit. About ha lf were discha rged from th e str oke
unit in
about six weeks compared with over 12 weeks in the general
ward. In the stroke unit, all patients were discharged after
12
weeks, whereas it t ook 32 weeks in t he genera l war d.
59
In 1993 Peter Langhorne and his colleagues assessed the
conclusions that could be drawn from ten randomised clinical
tr ials then a vailable for st udy. They compa red a stroke un
it with
alternatives such as a general hospital ward. By a stroke
unit
th ey meant a m ult i-disciplina ry tea m of specia list s,
which could
be geogra phically based or mobile. They foun d t ha t th e ma
na ge-
ment of patients in a stroke unit was associated with lower
morta lity after 17 weeks a nd a fter 12 mont hs . After 12 mont
hs,
th e redu ction in mort ality was 21 per cent , or 25 per cent
if th etr ials based on inform al ra ndomisat ion were excluded.
The s tu dy
also found evidence that patients treated in units had an
im-
proved a bility t o fun ction .60
Special str oke u nits not only reduce morta lity but also
reduce
th e length of hospita l sta ys. The Str oke Un it Tria lists
Collabora-
tion studied 11 trials comparing a dedicated stroke unit with
a
general medical ward; six trials comparing mixed assessment/
reh abilita tion u nits with a genera l medical war d; a nd four
tr ialscomparing a mixed assessment/rehabil i tat ion unit with
a
-
8/9/2019 Delay, Denial and Dilution
27/55
DELAY, DEN IAL AND DILUTION18
dedicated unit. Dedicated units dealt with stroke cases
only.
Mixed assessment /reha bilita tion un its were eith er a ward or
a
team with an interest and expertise in the assessment and
reh abilita tion of disablin g illness but not exclusive to str
oke. The
rate of death after one year was found to be 20.9 per cent
for
str oke units an d 25.4 per cent for alter na tives. The proport
ion of
pat ient s u na ble to live at home was 40.1 per cent for str
oke un its
and 47.2 per cen t for t he a lterna tives. Benefits did not
depend on
increased hospita ls sta ys a nd ma y even h ave reduced th em.
The
team concluded that stroke unit care was unlikely to be more
expensive tha n conventiona l car e in a genera l war d a nd m
ay be
less cost ly.61
However, despite clear evidence th at str oke u nits ar e
effective,
th ey ar e un der-used. The m ost systema tic evidence comes
from
th e 1998 Stroke Association sur vey. It carr ied out two nat
iona l
surveys: one covering a ll consultant s in th e UK r esponsible
for the
care of stroke patients; and one covering all health
authorities
an d boar ds in t he U K. The findings were distu rbing. The ea
rlier
St roke Associat ion su rvey of 1992/93 had foun d th a t u nder
ha lf of
consu ltan ts h a d access to a st roke un it. Despite th e
appea l of theStr oke Associat ion for the collect ion of informa t
ion , in 1999 th ere
was still no national information about the number of stroke
units, the treatment policies they followed, or the number
of
patients treat ed by them.
Neverth eless, the 1998 sur vey foun d t hat about 75 per cent
of
consu lta nts had a ccess t o some form of specialist st roke
service,
either a defined unit with beds or an interdisciplinary
team.
However, of those with access to a specialist service, in 46 per
centof cases it was to a rehabilitation unit. Acute-only units
were
available to 17 per cent of consultants and combined acute/
reh abilita tion u nits t o 16 per cent.62
Consult ant s wer e sa id to be fairly happy with th eir a
ccess, but
a significan t minority report ed inadequat e a ccess: 18 per
cent ha d
inadequat e a ccess t o acut e str oke u nits; 20 per cent to
rehabilita-
tion units; 25 per cent to acute/rehabilitation units; and 13
per
cent to a str oke tea m.In practice, however, only one-third of
consultants said that
patients were usually managed by a stroke unit team or in a
-
8/9/2019 Delay, Denial and Dilution
28/55
DISEASES OF TH E CIRCULATORY SYSTEM 19
str oke un it. Moreover, t her e were significan t regiona l var
iations
an d, in th e worst cases of the West Midlan ds an d th e North
West,
40 per cent of consu ltan ts did not m an age their pat ient s
in str oke
units or teams.63
Despite an overall improvement in access since 1992/93, the
1998 survey foun d wide and un accepta ble variat ions a round t
he
coun tr y in t he chan ces of being ma na ged in a n organ ised
stroke
service. Consu ltan ts from England (29 per cent) a nd Wa les
(21
per cent ) had poorer a ccess to acute st roke unit car e tha n
t hose
from Scotland (41 per cent) or Northern Ireland (52 per
cent).
Patients in Northern Ireland had the best chance of being
admitted or transferred to a stroke unit, followed by
Scotland,Tren t, Wales and London. Those a dmitt ed to hospitals in
Wales,
Scotlan d or Nort her n Ir elan d were a pproxima tely twice as
likely
to be cared for in a stroke unit as those admitted to
English
hospitals.64
Of th ose consu ltan ts who trea ted st roke, only 3 per cent
were
specialists in stroke medicine. The others were specialists
in
general medicine (55 per cent), geriatric medicine (27 per
cent)
and neurology (6 per cent). Most were part of a team, but
thesurvey found that many consultants felt the time available
for
th eir st roke pa tient s wa s eith er fairly or very ina dequa
te.65
At t he t ime of th e survey it was estima ted tha t on an y
single day
th ere would be about 10,500 str oke pa tient s in U K hospita l
beds.
On t he da y of th e survey about 52 per cent were ma na ged by
an
organ ised st roke service. Tha t is, nea rly ha lf were depr
ived of th e
established a dvan ta ges of a str oke un it, nam ely a su bstan
tially
reduced risk of dea th or severe d isability. The St roke
Associationcalcula ted t ha t, of th e estim a ted 116,000 acute st
roke admissions
in a year , about 55,000 were not ma na ged in a str oke un it,
which
would ha ve reduced t he chan ces of deat h or being instit u
tiona l-
ised by 25 per cent . The Str oke Association estima ted t ha t
t his
mea nt th ere were between 4,500 an d 7,000 avoidable deat hs a
nd
institutional placements each year. Or, counting only
deaths,
between 2,000 an d 3,000 avoidable deat hs per yea r. All told,
th e
Stroke Association concluded that only about half of all
strokepa tien ts were receiving opt ima l specia list st roke car
e.66
The Stroke Association also found that other treatment tech-
-
8/9/2019 Delay, Denial and Dilution
29/55
DELAY, DEN IAL AND DILUTION20
niques of proven efficacy were not being applied. There was
evidence t ha t some consu ltan ts were not well informed about
th e
benefits of some drug treatments, including even aspirin and
hepa rin, which h ad been th e subject of two ma jor int ern at
iona l
tr ials the year before th e survey. When pa tient s were tr eat
ed in
th e comm un ity, th e Stroke Association foun d th at fewer t
han h a lf
of th e pat ient s who would benefit from t aking aspirin were
in fact
taking it. And, even following hospita l discha rge, only 80 per
cen t
were tak ing it .67
-
8/9/2019 Delay, Denial and Dilution
30/55
21
2
Cancer
I n S aving Lives: Our H ealth ier N ation th e Govern ment
report sthat overall death rates from cancer in England for
peopleun der 65 are slightly better t ha n th e EU average, but
goes on to
sa y tha t t his figure conceals some import an t differen ces.
The UK
ra te of deat h from brea st cancer is am ongst t he worst in Eu
rope,
twelfth out of 15, and for cervica l cancer t he UK is th irt
eent h out
of 15.1 The report ma kes the fur th er adm ission t ha t t he
cha nces
of sur viving ar e poorer in th e UK th an in some other coun tr
ies
and goes on to concede tha t pa rt of th e differen ce ma y
reflect the
fact that there are cancer services in other countries which
are
better th an we are in th is coun tr y at t rea ting can cer.
This
admission is then followed by a fur ther confession. People in
more
depr ived a rea s, it sa ys, ten d t o have lower su rvival ra
tes .2
The E uroca re I I st udy, based on over 3.4 million cancer r
ecordsin 17 coun tr ies, allows us t o compar e sur vival ra tes in
E ngland
an d Scotla nd with th ose for other Eu ropean coun tr ies.3 It
sh owed
that in England and Scotland the five-year survival rate
from
1985 to 1989 was below th e Eu ropean avera ge for both m en a
nd
women suffering cancer of the colon and rectum,4 lung,5 and
breast .6 The gap wa s often subst an tial. For inst an ce, five
year s
after t rea tm ent , the cha nces of sur vival for men with
colorectal
can cer were 59 per cent in t he N eth erlan ds compa red with
41 percent in En glan d a nd Scotland. In F ra nce men with lung
can cer
ha d a 40 per cent cha nce of being alive one year a fter t rea
tm ent ,
compa red with 23 per cent in En glan d.
Since the report of the Expert Advisory Group on Cancer
(Calman-Hine) in 19957 more attention has been devoted to
deficiencies in cancer care. However, despite the widespread
criticism, inadequacies remain. According to WHO cancer
progra mm e director a nd NHS consu ltan t, Professor Ka rol
Sikora ,
-
8/9/2019 Delay, Denial and Dilution
31/55
DELAY, DEN IAL AND DILUTION22
no ma jor resources ha ve been allocat ed t o sett ing up
specialist
team s, as r ecomm ended by Calma n-Hine, and th e UK h as
fewer
oncologists per pa tient th an compa ra ble Eu ropea n coun tr
ies. A
Royal College of Radiologists su rvey found t ha t the workload
of
UK oncologists was far higher than in similar European coun-
tr ies. Some U K consu ltan ts were seeing over 1,000 new pat
ient s
a year. The average was 550 a year , compa red with 250 in F ra
nce
and Germany. To match German and French figures would
require t he n um ber of UK consu ltan ts to be doubled.8
The shortage of specialists means, not only the denial of
treatment, but also delays even in emergencies. For
instance,
meta sta tic maligna nt spina l cord compression is a ma jor cau
se ofmorbidity in patients with cancer and often means that a
previous ly-fun ctioning pa tien t becomes bedr idden or
confined t o
hospita l for th e rest of his or her life.
D.J. Husband, consultant in clinical oncology in Bebington,
car ried ou t a st udy of 301 pa tient s referr ed to th e Clat
ter bridge
Cent re for Oncology for tr ea tm ent of a first episode of ma
ligna nt
spina l cord compression du ring a th ree-yea r period. It is
widely
accepted t ha t m aligna nt spina l cord compr ession is a
medical orsurgical emergency, requiring urgent diagnosis and
treatment
becau se dely can resu lt in irr eversible par a lysis or loss
of bladder
function.
However, the study found that delay in the diagnosis and
treatment of malignant spinal cord compression remained a
common problem and resulted in preventable deterioration in
neurological function before treatment in most patients. It
is
rea sona ble to expect r eferr al a nd t rea tm ent of th is
condition in
less th an 24 hour s but t he st udy foun d tha t t his tar get
was notachieved for 70 per cent of pat ient s a t gener al pr
actitioner sta ge,
79 per cent a t t he distr ict genera l hospita l sta ge, an d
33 per cent
at the treatment unit stage. Delays of more than seven days
occurred in 33 per cent of patients at the general
practitioner
sta ge, 34 per cent at th e district genera l hospital sta ge an
d six per
cent at th e tr eatm ent u nit st age. Failur e to diagnose
spina l cord
compress ion and fa ilur e to investigat e, refer, and t rea t
su fficient ly
urgently were the main causes of delay and the
consequentfunctional deterioration.9
-
8/9/2019 Delay, Denial and Dilution
32/55
CANCER 23
The Calma n-Hine report advocat ed an improved network of
care
based on some 30 specialist can cer cent res, each link ed t o
10-12
can cer u nits. In th e yea r a fter th e Calman -Hine report,
Pr ofessor
Richa rds an d colleagues10 condu cted a sur vey based on 12 tr
ust sproviding for 24 million people. The study looked at
current
activity levels, changes in activity over time, and facilities
for
can cer care. They foun d tha t t he r ecomm enda tions of the
Calman-
Hine report had not been implemented. Five out of the twelve
centres did not provide a full haemato-oncology service and
the
sam e num ber did n ot employ specialists in pa lliative
medicine.
Furthermore, considerable inequalities were evident in the
provision of h igh t echn ology equipm ent, th e referra l r a
te a nd theprovision of cancer beds between th e cent res.11 Three
year s lat er,
in 1999, Professor Kar ol Sikora described t he implemen ta tion
of
Calma n-Hine as a saga of un der-resou rcing and bu rea ucra
tic
muddle. Whole forest s had been felled, he sa id, to gener a t e
t he
paper consu med by report s, stra tegic an alyses an d focus
groups,
but progress h ad been inadequa te. A ma jor problem h ad been
th e
lack of new resour ces t o implemen t change.12
If th e UK were a s effective in tr ea ting each cancer a s t he
bes t in
Eur ope, ar gued P rofessor Sikora , it cou ld save up to 25,000
lives
a year. And if it merely hit the average, this figure would
be
10,000 lives.13 He conceded that there had been some
improve-
ments, but because the Calman-Hine report had not been
accompa nied by any promise of new fun ding, a ny impr ovemen t
s
implied a r eduction in other ser vices. He th ought t ha t th e
limited
improvemen ts following Calman-Hin e ha d been at th e expense
of
patients with cardiovascular disease, diabetes and the
chronic
problems of old a ge.14
The Main Kinds of Canc er
Lun g Can cer
Surgical resection is the recognised treatment of choice for
pat ient s with sta ge I or II non-sma ll cell lung can cer. In
t he UK
surgical resection rates have remained at about 10 per cent,
wherea s in t he USA one su rvey report ed a ra te of 28 per
cent a nd
in Europe rates have been found to be higher still. In
reality,ma ny UK pat ients with operable tumours h ave been denied
the
cha nce of cur a tive sur gery.15
-
8/9/2019 Delay, Denial and Dilution
33/55
DELAY, DEN IAL AND DILUTION24
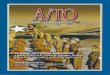
Figu r e 3
Figu r e 4
Note: All rat es ar e rela tive an d age-sta nda rdised. They
reflect findin gs from
th e Eu rocar e II st udy for 1985-1989.
-
8/9/2019 Delay, Denial and Dilution
34/55
CANCER 25
The one-year sur vival rat es in E ngland an d Scotla nd were
not
only below th e Eur opean avera ge, but th e a bsolute lowest
out of
th e 17 coun t r ieswhich included E stonia , Slovakia, Slovenia
a nd
th e oth er 14 coun tr ies in the E ur oca re II stu dy (see
Figure 4). The
five-year sur vival ra tes for En glan d a nd Scotlan d were a
lso well
below the European average but were not the absolute lowest.
Est onia ha d a five per cent sur vival ra te for m en compa red
with
Scotla nds six per cent and Englan ds seven per cent (see F igur
e
3). The Eur ocar e II au th ors believed th at th e lower su
rvival ra tes
for pa tient s with lun g can cer in E ngland an d Scotlan d
were partly
expla ined by rest ricted a ccess t o specia lised care.16
Hilary Pickles, Director of Public Health in Hillingdon, hasar
gued t ha t lung cancer is often given low pr iorit y becau se it
is
seen a s self-inflict ed. Pickles fur th er a rgued tha t on ly
so mu ch
can be done within existing resources and that the outlook
for
lung cancer compared with alternatives such as care of the
elderly, asthma, breast cancer and cardiothoracic surgery
was
bleak.17
Breast Can cerEa ch yea r a round 30,000 new cases of breast can
cer a re diagnosed
in th e UK an d ar oun d 15,000 die from th e disease. The Eu
rocar e
st udy, based on 30 can cer r egistries in 12 coun tr ies
between 1978
and 1985, foun d relat ively low survival for UK women with brea
st
cancer. England and Scotland, along with Spain, Estonia and
Poland, had the lowest rates of breast cancer survival.18
The
Eur oca re I I st udy from 1985 to 1989, based on 42 r egistr
ies in 17
countries, found that Scotland, England and Slovenia had
one-
year su rvival some 3-4 per cent below th e avera ge, and
five-year
su rvival 6-9 per cent below avera ge (see F igur e 5).19
How can th ese differences be explained? The E ur oca re a ut
hors
concluded th at low sur vival in t he UK may be a tt ribut ed t
o poor
compliance on the part of health authorities and doctors
with
consensu s t rea tm ent guidelines a s well as great er var iat
ions in
treatment .20
There is no evidence tha t brea st can cer in UK women differs
in
histology or grade from that in similar countries. Nor is
there
evidence that women in the UK who have symptomatic breast
-
8/9/2019 Delay, Denial and Dilution
35/55
DELAY, DEN IAL AND DILUTION26
disease delay any longer in seeking diagnosis.21
Consequently,
according to Professor Richa rds of Guys a nd St Thoma s, th e
chief
rea son for poor UK resu lts is th a t a significan t n um ber
of women
who ar e diagnosed with brea st cancer r eceive su b-opt ima l
ca re.22
A study of women aged under 50 in the South East Thames
Region by Pr ofessor Richa rds foun d that th e trea tment s
provided
were frequ ent ly at var ian ce with well-respected gu
idelines.23
Figu r e 5
Note: Rates a re a ge stan dar dised a nd relat ive. 1985-1989
Eu rocar e II
A study by C.J. Twelves and colleagues found that,
althoughgeographical variations in the selection of patients for
surgery
account for some of the differences in survival, the health
au th ority in which t he pa tient was first t rea ted had a n
effect on
the outcome. In fact, across health boards, estimated
five-year
survival rates ranged from 67 per cent to 84 per cent. One
possible explana tion was differen ces between health boards in
th e
proportion of patients receiving adjuvant systemic therapy
(usually tamoxifen). Analysis clearly showed that the healthboa
rd of first t rea tm ent predicted independen tly whet her or
not
pat ient s would receive adjuvan t systemic tr eat men t.24
-
8/9/2019 Delay, Denial and Dilution
36/55
CANCER 27
Figu r e 6
-
8/9/2019 Delay, Denial and Dilution
37/55
DELAY, DEN IAL AND DILUTION28
Figu r e 7
Not
e :
Ra t
e s
a r e
r e l
a t i
v e
and
a ge -
s t a
n d
a r d
ise-
d .
198
5 -
198
9 ,
Eu rocar e II
-
8/9/2019 Delay, Denial and Dilution
38/55
CANCER 29
Other studies have also found unexplained variations in
diagnosis an d tr eat men t. Chouillet a nd colleagues assessed
334
cases of breast cancer diagnosed in South East England. It
is
fundamental to effective treatment that the stage of the
cancershou ld be kn own, but it was r ecorded in only 24 per cent
of cases.
Liver and bone scan ning an d skeleta l ra diogra phy were ca rr
ied
out as frequen tly as a xillar y surgery, when the guidelines
advised
agains t t he u se of such investigations a nd st rongly
recommended
axillary sa mpling to determine t he st age of th e
disease.25
Sainsbury and colleagues investigated outcomes in 12,861
women t rea ted in Yorkshire and foun d considera ble va ria
tions in
survival between patients treated by different surgeons.
Afterallowing for case-mix and other variables, 20 per cent of
the
varia tion in su rvival was explained by chem oth era py alone a
nd
six per cent by hormone ther apy alone. If chemoth era py ha d
been
used in 40 per cent of cases (inst ead of about n ine per cent )
th ere
would h ave been a four per cent increa se in t he five-year su
rvival
rate, which would have meant that an additional 500 patients
would h ave been a live after five year s.26
Access to specialists also has a significant impa ct on su
rvival. A
study by Gillis a nd Hole measu red t he sur vival out come of
care by
specialist surgeons in breast cancer in the west of Scotland.
27
This study found that, after adjustment for prognostic
factors,
five- an d t en-year sur vival ra tes were nine per cent an d
eight per
cent higher r espectively am ong women tr eat ed by brea st can
cer
specialists as opposed to non-specialists. Out of 3,786
patients
studied, only 918 were seen by a su rgeon with a specialist
int eres t.28
Colorecta l Ca ncer
Colorecta l cancer is the second most comm on fat al ma ligna
ncy in
both sexes combined, after lung cancer.29 It was responsible
for
over 15,000 deat hs in E nglan d and Wales in 1996.30 The Eu
rocar e
II st udy of th e per iod from 1985-89 foun d t ha t five-year
su rvival
for both men an d women was below th e Eu ropean avera ge.
For
En glan d th e ra te was 41 per cent , which placed it t welfth
out of
17. Rates in the most successful countries were
substantiallyhigher. The five-year survival ra te in th e Nether
lands wa s 59 per
-
8/9/2019 Delay, Denial and Dilution
39/55
DELAY, DEN IAL AND DILUTION30
cent for m en a nd 56 per cent for women. In Fr an ce th e ra te
wa s
52 per cent for men an d 54 per cent for women .31
Ov ar i an Canc er
Ovar ian can cer is th e four th most comm on cau se of deat h
from
cancer amongst females, with an overall five-year relative
sur vival ra te of just under 30 per cent . There ar e 6,000 new
cases
an d some 4,000 death s from ovar ian cancer a year.32
One st udy audited seven district h ealth a ut horities in th e
Sout h
East Thames region covering 118 newly-diagnosed cases of
ovar ian can cer . Clinical guidelines were agreed before t he
st udy
began an d their implement at ion was t hen audited. The
guidelineswere based on consensus statements and were very similar
to
guidelines in use in the US and elsewhere in the UK. Both
investigation and management of ovarian cancer varied
signif-
icantly between hospitals. Only 53 per cent of patients
received
the recommended diagnostic procedures, and the inappropriate
investigation may explain the inadequacy of subsequent
treat-
men t. Overa ll, only 43 per cent of pa tient s were judged to
ha ve
been t he subject of appr opr iat e clin ica l investigat ion a
nd m an-agemen t. At S ta ge I, 72 per cent were judged t o have
been
inappr opriat ely ma na ged, at St age II, 47 per cent an d a t
St age
III, 54 per cent were cons idered t o ha ve been ina ppr opr iat
ely
ma na ged, when t heir tr eatment was judged a gainst intern at
ion-
a lly accepted gu idelines.33
Another ret rospective review of pat ients in Ma nchester foun
d
that fewer than half the patients underwent the generally
accepted su rgica l procedure.34 The a ctu a l conduct of consu
lta nt s
was compar ed with t he opt ima l mana gement defined in
accepted
consensus statements.35 The study found that in North West
En gland ma ny consu ltan ts were opera ting on a few patient s
each,
at th e expense of pa tient sur vival. The r ecommended pr
actice was
for pa tient s to be trea ted by specialist tea ms with th e
necessar y
combined expert ise and not by individua l consu lta n ts who
lacked
th e r equired experience an d knowledge. However, in one su
bset
of 76 patients, only 32 received the recommended treatment
of
hysterectomy, bilateral salpingo-oophorectomy and
infracolicomentectomy.36
-
8/9/2019 Delay, Denial and Dilution
40/55
CANCER 31
The CancerBACUP sur vey of ovar ian cancer tr eatment simila
rly
found that various international as well as national
guidelines
were not being followed. The use of plat inu m/pa clita xel
(Taxol)
combina tion t her apy for ovar ian can cer h ad been recomm
endedby the J oint Coun cil for Clinical Oncology (a joint body r
epr esen t-
ing the Royal College of Physicians and the Royal College of
Ra diologists) an d endorsed by the Depar tm ent of Health s
Stan ding Medica l Advisory Comm itt ee. First -line u se of
plat inum
an d Taxol had r esulted in m ore t ha n 70 per cent remission
ra tes
an d a n additiona l year of life on avera ge.37
Figu r e 8
Note: Rates a re a ge stan dar dised a nd relat ive. 1985-1989
Eu rocar e II
In th e Can cerBACUP su rvey, individua ls who were
responsible
for commissioning services for a roun d ha lf th e na t ions
popula tion
work ing in 60 NH S au th orities an d boar ds were int erviewed
in
th e sum mer of 1998. Less th an one-fifth of NH S a ut horities
a nd
boar ds were able to ensur e th at suitable ovarian can cer pa
tients
received t he r ecomm ended plat inum/paclitaxel trea tm ent .
In fact,in ma ny loca lities t here were no pa tients r eceiving th
is treat men t
from t he N HS. The cau se was almost en tirely finan cial,
becau se
-
8/9/2019 Delay, Denial and Dilution
41/55
DELAY, DEN IAL AND DILUTION32
almost all the directors of public health and consultants
approached by the su rvey team were aware of th e effectiveness
of
plat inu m/paclita xel tr eatm ent. One lead pur cha ser in
souther n
Englan d commented: we recognise tha t we ha ve got t o respond
...The advantages are too great to ignore. But at the same time
th ere ar e cost quest ions, and people ha ve got t o th ink t h
rough the
implications.38
In 1996 th e E nfield-Ha ringey Health Authority sent out a lett
er
to two tru sts with wh ich it h ad cont ra cts u rging them to
cut back
on pa tients receiving the taxanes, Taxoter e (doceta xel) for
ovarian
and brea st cancer a nd Ta xol (paclitaxel). The au th orit y,
1.7m in
debt, declared it wa s ta king the a ction becau se it ha d ru n
out ofmoney for t reat ment using the dru gs.39
Chemotherapy for cancer has been found to be effective in
clinical t rials, but n ot only is it withh eld from pa tient s,
there a re
also difficulties in fun ding fur th er vita l resea rch. R.E. H
awkins ,
Clinical E ditor of th e British Journal of Cancerand Director
of
Medical Oncology at the Christie CRC Research Centre, has
reported that some trials of potentially useful drugs have
been
delayed because of a lack of funding. The ICON3 trial, for
exa mple, was delayed beca use loca l pur cha sers r efused to
fun d
th e dru g costs.
Conclusions
Some of th e dispa rit ies described were due t o bad or incons
isten t
clinical practice, but the underlying difficulty was the lack
of
finance.
It is now accepted that adjuvant chemotherapy improves
sur vival and th at palliative chemothera py impr oves t he qua
lity
of life for sufferers of advanced cancers. However, in a lett er
t o the
British Medical Journal in September 1997 eleven doctors
representing the Association of Cancer Physicians pointed
out
th at th e rea llocation of NHS fun ding to prima ry car e ha d
been th e
cau se of ma ssive problems for can cer u nits a nd centr es an
d th at
cytotoxic therapy had often been the main target for budget
reductions. Their use had, in effect, not been funded in
many
regions. The eleven doctors compared the cost of
cytotoxicchemotherapy with other drugs. The total budget for
cytotoxic
-
8/9/2019 Delay, Denial and Dilution
42/55
CANCER 33
dru gs was about 58m compa red with th e 250m spent on th e
single ulcer-healing drug omeprazole.40 The authors quote
inform a tion from In tercont inent al Medical Stat istics, for
th e year
end ing Sept ember 1996, when about 1,038 million wa s spen t
ongastr ointest inal d ru gs, 848 million on car diovascular
medicines,
282 million on derm a tologica l tr eat ment s a nd only 167
million
on can cer dr ugs.
The situ at ion ha d become bad enough by October 1999 for th
e
Secret ar y of Sta te for H ealth , Alan Milbur n, to ann oun ce
a n ew
ten-year initiative to improve cancer care. Professor Mike
Richa rds was a ppointed th e Nat iona l Cancer Director to lead
th e
programme and Mr Milburn declared that he had asked theNa tiona
l Inst itu te for Clinica l Excellence to dr a ft ea r ly
guidance
on th e u se of th e t axan es, to end th e postcode lott ery of
ca re, as
his press release pu ts it .41 He a lso ann oun ced a n
additiona l 80
million for can cer services, but when ques tioned by journ a
list s it
tu rn ed out th at th e 80 million was coming out of a sum alrea
dy
allocated for NHS improvements and which had already been
announced.42 Such m easur es give the impression of action but ,
in
rea lity, fa ll a long way short of wha t is r equired.
-
8/9/2019 Delay, Denial and Dilution
43/55
34
3
Conclus ions
The m ain findings can be sum ma rised a s follows. The UK ha
s
a poor r ecord of preventing dea th from disea ses of the
circula -
tory system. After a llowing for th e differen t age str uctu re
of each
coun tr y in th e Eu ropean Union, t he U K death ra te from
circula-
tory diseases for per sons a ged under 65 was ranked thirteenth
outof th e 15 coun tr ies stu died.
The t wo ma in diseases of th e circula tory system ar e corona
ry
hear t disease a nd st roke. Corona ry hea rt disease is t he
biggest
single cau se of premat ur e deat h, killing 28 per cent of men
an d 17
per cent of women in 1996. High blood pr essure is one of th e
main
risk factors a nd a successfu l service would pr ide it self on
effective
tr eat men t. However, in 1997 u nder ha lf of people with high
blood
pressure were being treated successfully (42 per cent were
receiving effective treatment, 21 per cent were being
treated
inadequat ely, and 37 per cent were not being tr eat ed at
all).
Stroke is th e th ird biggest killer an d th e biggest cau se of
severe
disability. Ther e has been solid evidence for some time th at
car e
of stroke pa tient s in a specialised st roke unit r educes m
ort ality by
25 per cent. An effective health service would pride itself
on
providing for str oke pa tient s in t his ma nn er. However, in
1998
only one-th ird of NH S consu ltan ts sa id tha t t heir pa
tient s were
usu ally man aged by a str oke un it team or in a str oke un
it.
It is also difficu lt t o ta ke a ny pr ide in t he U Ks r ecord
in cancer
car e. The best evidence comes from t he 17-na tion E uroca re s
tu dy
which compares one-year and five-year su rvival rat es for t he
m ain
can cers. It foun d th at En glan d an d Scotlan d ha d th e
lowest one-
year survival rates for lung cancer. The five-year survival
rate
was little better, with England ranking 12 out of 17, above
Scotlan d, Estonia, Denm ar k, Poland a nd Slovenia.
-
8/9/2019 Delay, Denial and Dilution
44/55
CONCLUSIONS 35
For br east ca ncer (15,000 deat hs) En glan ds one-year sur
vival
was r anked tent h out of 17 a nd Scot lan ds twelfth out of 17,
above
Aus tr ia, Est onia, Poland a nd Slovakia . The five-year sur
vival ra te
in E ngland was elevent h out of 17 and in Scotlan d t welfth
out of17, above Slovenia, Aust ria , Est on ia, Poland , and Slovak
ia.
Colorecta l cancer is t he second largest k iller a ffecting
both sexes
(15,000 deaths). For cancer of the colon in men the
five-year
survival rate in Scotland an d E ngland was r an ked equa l
elevent h
out of 17. For women , Scotlan d a nd En glan d were equa l
twelfth
ou t of 17.
Ovar ian cancer is th e fourt h la rgest cancer killer. The
five-year
survival ra te for E ngland was eleventh out of 17 an d for
Scotla ndth irteen th (see Figur e 8).
There is little doubt that rationing is the root cause of
these
problems. In the early 1990s Britain had fewer
radiotherapists
per head than Poland and fewer medical oncologists than any
coun tr y in western Eu rope.1 The short age of specia list s r
eflect s
th e gener a l sca rcity of doctors. OECD figur es for 1996 show
th a t
the UK had 1.7 practising physicians per 1,000 population.
German y had 3.4 per 1,000, Fr an ce 2.9 an d Poland 2.4. The
onlycountries with a lower proportion among the 29 studied by
the
OECD wer e Korea (1.2), Mexico (1.2) and Turkey (1.1).2
However
well motivated individual doctors might be, if they are in
short
supply, the inevita ble r esult is th e dilut ion of ca re.
Tota l spending on health ca re is low by interna tiona l sta
nda rds.
In 1997 tota l expenditur e on h ealth care in t he UK was 6.9
per
cent of GDP. The German figure was 10.7 per cent and the
Fr ench, 9.6 per cent . Of th e 29 a dvanced coun tries studied
by theOECD, only Hunga ry, Ireland, Korea , Mexico, Poland and Tur
key
spent less. To ma tch Germ an levels would requ ire an increa se
of
nea r ly 30 billion per year . Even if we leave out private
expend i-
ture on health and compare only government spending, the
disparity remains. In 1997 the UK govern men t spent 5.8 per
cent
of GDP on hea lth car e, compar ed with th e Germa n figur e of
8.3
per cent . To ma tch th e Germ a n pr oport ion would require
near ly
20 billion a year extr a . Gaps of th is ma gnitu de cannot be
closed
by measu res such a s special improvemen t fun ds an d
efficiency
savings.
-
8/9/2019 Delay, Denial and Dilution
45/55
DELAY, DEN IAL AND DILUTION36
Wha t should be d one? After decades of den ial it is now
widely
accepted that NHS rationing is endemic and has harmful
consequen ces for pa tien ts . Would more money be t he
answer?
This is n ot th e place to go into the complex issues en ta iled
inan y search for a n a lterna tive to th e NH S, but st at e finan
ce has
now been test ed in a 50-year pilot schem e which a ny r
easonable
and impa rt ial observer would concede ha s been a fa ilur e. We
need
an u rgen t pu blic deba te a bout how best t o int roduce a
bigger role
for personal payment and insurance without compromising the
pr inciple of access for a ll.
There are countless alternatives available elsewhere in the
world an d a debat e ha s already begun in th e UK. For
example,Professor Chris Ham, has advocated an increased role
for
competing non-profits.3 Pr ofessor J ohn Spiers ha s advocat ed
th e
privat isat ion of hospita ls.4 J ohn Willma n, Consu mer Indust
ries
Editor of the Financial T im es, ha s a dvocat ed pat ient cha
rges.5
And Oliver Morgan of th e Observerha s put th e case for
increased
private finance.6 We hope that our findings will add a
little
ur gency to th e sear ch for a better alter na tive.
-
8/9/2019 Delay, Denial and Dilution
46/55
37
1 For instan ce, Cooper, L., Coote, A., Davies, A. and J ackson,
C.,
Voices Off: Tacklin g th e Dem ocratic Deficit in Health ,
London:
Ins tit ut e for Pu blic Policy Resear ch, 1995.
2 For example, Professor Alan Maynard at the University of
York
is a strong defender of this approach. The journal Effective
Health Care regularly publishes studies of
cost-effectiveness.
3 See for exam ple th e publicat ions of Pr ofessor Alan
Williams,
Un iversit y of York.
4 Hunter , D., Desperately Seek ing S olut ions, London:
Longman,
1997.
5 Klein, R., Day, P. and Redmayne, S.,Man aging S carcity:
Priority
Setting and Rationing in the National Health Service,
Buckingham: Open University Press, 1996.
6 Klein et al., Man aging S carcity,1996, p. 123.
7 McKenzie, J . et al., Dialysis decision ma king in Can ada ,
th e
United Kingdom a nd t he Un ited Sta tes, American Journal ofKid
ney Diseases, Vol. 31, No. 1 (Jan ua ry) 1998, pp. 12-18.
8 Roder ick, P . et al., The pr ovision of ren al r eplacemen t
th era py
for adults in England and Wales: recent trends and future
directions, Q J Med, Vol. 91, 1998, pp. 581-87.
9 Dep ar tm en t of Hea lt h , The National Survey of NHS
Patients.
10 The Clinical St an dar ds Advisory Group was esta blished in
April
1991, under Section 62 of the NHS and Community Care Act1990, as
an independent source of expert advice to UK health
ministers an d to th e NHS on st an dar ds of clinical care for,
a nd
access a nd ava ilability of services to, NHS pa tient s. The Gr
oups
members are nominated by the medical, nursing and dental
royal colleges and their faculties, the professions allied
to
medicine, and include the chairman of the Standing Medical
Advisory Committee.
11 The St an ding Medical Advisory Comm itt ee is one of
five
sta tu tory bodies which a dvise health ministers in En glan d
an dWales on t he pr ovision of medical services un der t he N HS
Acts .
Members ar e ap point ed by minist ers following nomin at ions
by
Notes
Introduction
-
8/9/2019 Delay, Denial and Dilution
47/55
DELAY, DEN IAL AND DILUTION38
professional bodies and include the presidents of all
medical
royal colleges. Nine standing advisory committees were first
esta blished in 1949, but un der t he NH S (SAC) Order 1981,
four
SACs were reta ined with u ncha nged ter ms of referen ce, to
adviseon the provision of medical, nursing & midwifery, dental,
and
pha rm aceut ical ser vices in En glan d and Wales. A fifth SAC,
now
th e Joint Comm ittee for Vaccina tion an d Imm un isat ion
Services,
was subsequently established. SACs perform their statutory
functions in three ways: developing advice (advisory role);
commenting on advice developed by others (consultative
role);
and alerting ministers an d th e depar tment to issues which a
re
likely to be import an t in t he futur e (monitoring role).
Chapter 1
1 Corona ry Heart Disease S tatist ics, British Heart
Foundation,
1998, p. 14.
2 Corona ry Heart Disease S tat istics, 1998, p. 9.
3 Saving Lives: Our Healthier Nation, Cm. 4386, London: The
Sta tioner y Office, 1999, p. 73. See also Dept of Healt h,
Coronary
Heart Disease: An Epidemiological Overview, London: HMSO,
1994.
4 Corona ry Heart Disease S tat istics, 1998, p. 14.
5 The Health of the Na tion, Cm 1523, London: HMSO, 1991, p.
59.
6 Corona ry Heart Disease S tatist ics, 1998, pp. 9-10, 19. The
figur es
ar e for m en a ged 35-74 and a re a ge-sta nda rdised, based on
t he
Eur opean St anda rd P opulation.
7 Corona ry Heart Disease S tat istics, 1998, p. 34.
8 Corona ry Heart Disease S tat istics, 1998, p. 84.
9 Coronar y angioplasty involves inserting a balloon into
the
obstructed artery and inflating it to tear the inner part of
the
ar ter ial wall in order to reduce the obstr uction. The CABG
is