Embed Size (px)
Citation preview

Defining and applying a functionality approach tointellectual disabilityjir_1575 1..12
R. Luckasson1 & R. L. Schalock2
1 Department of Educational Specialties, Special Education Program, University of New Mexico, Albuquerque, NM, USA2 Hastings College, Hastings, NE, USA
Abstract
Background The current functional models of dis-ability do not adequately incorporate significantchanges of the last three decades in our under-standing of human functioning, and how thehuman functioning construct can be applied toclinical functions, professional practices and out-comes evaluation.Methods The authors synthesise current literatureon human functioning dimensions, systems of sup-ports and approaches to outcomes evaluation forpersons with intellectual disability (ID), andpropose a functionality approach that encompassesa systems perspective towards understandinghuman functioning in ID. The approach includeshuman functioning dimensions, interactive systemsof supports and human functioning outcomes.Results Based on this functionality approach theauthors: (1) describe how such an approach can beapplied to clinical functions related to defining ID,assessment, classification, supports planning andoutcomes evaluation; and (2) discuss the impact ofa functionality approach on professional practices inthe field of ID.Conclusions A functionality approach can increasefocus on the integrative nature of human function-ing, provide unified language, align clinical func-
tions and encourage evidence-based practices. Theapproach incorporates a holistic view of humanbeings and their lives, and can positively affect sup-ports provision and evaluation.
Keywords assessment, classification, functionalityapproach, human functioning outcomes, intellectualdisability, systems of supports
Introduction and overview
The functionality approach to intellectual disability(ID) described in this article is a logical extensionof the functional approach to reasoning and deci-sion making. As in other fields, this logical exten-sion of reasoning emerged when the field of IDsought to ‘discover the significance of a fact througha determination of its implications or consequencesin . . . context’ (Cohen 1935, p. 829). A functionalapproach is generally seen as a way to go beyondclassical theory, dogma or vague notions as explana-tions of phenomena to a recognition of the ecologi-cal factors effecting the individual. Furthermore, afunctional approach is not merely more practical,but can also help move a field forward by taking amore holistic approach. In that regard, Cohenasserted that a functional redefinition of scientificconcepts has been a keynote of most significanttheoretical advances in the sciences (p. 824).
In this article we define a functionality approach tointellectual disability and propose that a functionalityapproach in the field of ID can be used to integrate
Correspondence: Prof. Ruth Luckasson, Department of Educa-tional Specialties, Special Education Program, University of NewMexico, MSC05 3040, Albuquerque, NM 87131-0001, USA(e-mail: [email protected]).
Journal of Intellectual Disability Research doi: 10.1111/j.1365-2788.2012.01575.x1
bs_bs_banner
© 2012 The Authors. Journal of Intellectual Disability Research © 2012 Blackwell Publishing Ltd

a functional and social–ecological approach to dis-ability, but also to provide the basis for rethinkingand updating policies and professional practices indefining, assessment, classification, the planningand implementation of individualised supports, andevaluating human functioning outcomes. We definethe functionality approach in intellectual disability as:
a systems perspective towards understandinghuman functioning in intellectual disability thatincludes human functioning dimensions, interac-tive systems of supports and human functioningoutcomes.
The proposed functionality approach expands thefunctional approach envisioned by both the WorldHealth Organization (WHO) and the AmericanAssociation on Intellectual and Developmental Dis-abilities [AAIDD; formerly American Associationon Mental Retardation (AAMR)]. The approachincorporates the significant changes of the lastthree decades in our understanding of human func-tioning, and describes how the human functioningconstruct can be applied to clinical functions, pro-fessional practices and outcomes evaluation. Inreference to expanding the earlier framework pro-posed by WHO and AAIDD, it is important tounderstand that these earlier frameworks concep-tualised functioning as: (1) an umbrella term refer-ring to the life activities of an individual; (2) amultidimensional phenomenon composed of bodystructures and functions, personal abilities and par-ticipation [in regard to the International Classifica-tion of Functioning, Disability and Health (ICF)]or dimensions related to intellectual abilities, adap-tive behaviour, health, participation and context (inregard to AAIDD); and (3) influenced by contex-tual factors (i.e. personal, environmental and cul-tural factors) and the provision of individualisedsupports (World Health Organization 2001, 2007;Buntinx 2006; Luckasson et al. 2002; Schalocket al. 2010).
In reference to incorporating contextual under-standing, it is important to remember that both theICF (World Health Organization 2001) andAAIDD (Luckasson et al. 1992) models of humanfunctioning and disability were initially developed10–20 years ago when the ecological model of dis-ability was just emerging and when there was lessknown about multidimensional assessment and
classification systems, the supports paradigm andoutcomes evaluation. We now know much moreabout the multidimensionality of human function-ing, the role that environments and individualisedsupports play in impacting human functioning andpersonal outcomes, and the interactive and dynamicnature of clinical functions related to assessment,classification, systems of supports and outcomesevaluation. As a field we are also aware of theincreased emphasis in public policies throughoutthe world regarding ways to meaningfully accountfor resources and evaluate the outcomes of servicesand supports, and to recognise and act on the inter-dependence and functional relatedness of humanfunctioning dimensions, socio-ecological factors andresultant effects on the person. Because of thisbetter understanding of contextual factors, the pro-posed functionality model incorporates a socio-ecological view of disability and emphasises thathuman functioning results from an interactionbetween an individual and his or her environment.
The article is divided into four sections. First, wediscuss how three factors are impacting how weview disability, and creating the need to integratehuman functioning dimensions, systems of supportsand human functioning outcomes. Second, weoutline and describe the parameters of a functional-ity approach to human functioning. Third, wedescribe how the approach can be applied to clini-cal functions related to defining ID, assessingpotential members of the class, using a multidimen-sional classification system, planning and imple-menting individualised supports and evaluatingoutcomes. Finally, we discuss the impact on profes-sional practices of using a functionality approach inthe field of ID.
Factors impacting the field
The relevance of the proposed functionalityapproach is embedded within three significantfactors impacting the field of ID. The first is ourmore in-depth understanding of the role that envi-ronments and individualised systems of supportsplay in the manifestation of human functioning. Thesecond is our better integration of the critical com-ponents of human functioning dimensions, systemsof supports and personal outcomes. The third is
2Journal of Intellectual Disability Research
R. Luckasson & R. L. Schalock • A functionality approach
© 2012 The Authors. Journal of Intellectual Disability Research © 2012 Blackwell Publishing Ltd

the public policy changes regarding the rights ofpersons with ID to be included in one’s society, andthe resultant need to develop meaningful indices ofhuman functioning to meet the increasing expecta-tion for outcomes evaluation.
Role of environments
The concept of disability has changed from focus-ing solely on pathology or a defect within theperson to a socio-ecological conceptualisation thatfocuses on understanding human functioning anddisability based on the interactions among personaland environmental characteristics (Luckasson et al.1992; Mercer 1992; Rioux 1997; World HealthOrganization 2001; Wehmeyer et al. 2008). Con-ceiving disability in the context of person–environmental interactions not only enhances theunderstanding of the person’s disability, but alsochanges the approach to classification and supportsplanning, provision and evaluation.
An ecological model of disability also focuses onthe multiple interrelated factors impacting humanfunctioning. As conceptualised by Bronfenbrenner(1977, 1999) and applied specifically in ID in Scha-lock et al. (2010) and Shogren & Turnbull (2010),these three systems are the micro-, meso- andmacrosystems.• The microsystem includes the immediate socialsetting including the person, family, friends,colleagues and close support staff.• The mesosystem includes the neighbourhood, com-munity and organisations providing services andsupports to persons with ID.• The macrosystem includes the overarching patternsof culture, society, larger populations, country orsocio-political influences.
Critical components of human functioning
Over the last decade we have come to understandbetter the multidimensionality of human function-ing. Significant progress has also been made indeveloping systems of supports and specific supportstrategies applicable to persons with ID. Finally, weunderstand better the evaluation of human func-tioning outcomes. Each of these three advance-ments is discussed next.
Multidimensionality of human functioning
A multidimensional model of human functioningwas first proposed by AAIDD (formerly AAMR)in the 1992 Manual (Luckasson et al. 1992) andfurther refined in the 2002 and 2010 Manuals(Luckasson et al. 2002; Schalock et al. 2010). Thefive dimensions of the AAIDD model, which areconsistent with the International Classification ofDisease (ICD) model (Buntinx 2006), are:• Intelligence: a general mental ability. It includesreasoning, planning, solving problems, thinkingabstractly, comprehending complex ideas, learningquickly and learning from experience.• Adaptive behaviour: the collection of conceptual,social and practical skills that have been learnedand are performed by people in their everyday lives.• Health: a state of complete physical, mental andsocial well-being.• Participation: the performance of people in actualactivities in social life domains.• Context: the interrelated conditions within whichpeople live their everyday lives. Context representsan ecological perspective that involves the micro-,meso- and macrosystems described above.
Systems of supports
Beginning in the 1980s, individuals with ID, fami-lies, advocates and professionals began to systemati-cally seek ways to manipulate the interactionsbetween a person and his or her environment toimprove human functioning. The notion of usingsupports to enhance the interactions of people withID within their environments and thus enhancehuman functioning took root, emphasising that IDwas no longer regarded solely as a static deficiency,but conceptualised as at least partly a manifestationof an interactive phenomenon. The supports para-digm has made several significant impacts on pro-fessional practices in the field of ID. First, thepattern of assessed needed supports has become thebasis of individualised education and habilitationplanning (Thompson et al. 2009). Second, the levelor intensity of a person’s support needs is beingused as the basis for agency and systems-level plan-ning and resource allocation (Fortune et al. 2009).Third, the supports orientation has broughttogether the related practices of person-centredplanning, personal growth and development oppor-
3Journal of Intellectual Disability Research
R. Luckasson & R. L. Schalock • A functionality approach
© 2012 The Authors. Journal of Intellectual Disability Research © 2012 Blackwell Publishing Ltd

tunities, community inclusion and empowerment(Claes et al. 2010). Thus, the supports paradigmthat incorporates systems of supports has provideda useful and robust framework for the provision ofindividualised supports that focus on improvinghuman functioning.
Supports are resources and strategies that aimto promote the development, education, interestsand personal well-being of an individual and thatenhance human functioning (Schalock et al. 2010,p. 175). Over the last decade, our understanding ofsupports has evolved to include the concept of‘systems of supports’ that involve the planned andintegrated use of individualised support strategiesand resources that encompass the multiple aspectsof human performance in multiple settings andprovide a structure for the organisation andenhancement of human performance elements thatare interdependent and cumulative. Components ofsystems of supports will be described later in refer-ence to Fig. 1.
Human functioning outcomes
Vague, conclusory statements no longer sufficefor the evaluation of the impact of services andsupports. Policy makers and service/support provid-
ers are held accountable for demonstrating proofof value in exchange for expenditure of resourcesand the participation of individuals with ID. Anadditional expectation in human services is thatoutcome data will be regularly reported. In orderfor assessed outcome data to be meaningful, impor-tant conceptualisations and measures of value mustbe selected. What do we value as the justification forthe expenditure of resources? What do individualswith ID value for their lives? Our contention is thatwhat is valued in both cases is improved humanfunctioning. Thus, we need a model that shows howhuman functioning outcomes can be operationalisedwithin a systems perspective. We discuss threeproposed outcome categories later in reference tothe parameters of a functionality model.
Public policy changes
Societal views of persons with disabilities have alsochanged significantly over the last few decades duein large part to the concept of egalitarianism, which isthe belief in human equality, especially with respectto social, political, economic and human rights.Since the 1960s, throughout much of the world wehave seen the emergence of the egalitarian move-
SYSTEMS OF
SUPPORTS
Throughput Output
Human Functioning Outcomes
SOCIO–ECONOMIC •
•
•
STATUS
HEALTH STATUS
SUBJECTIVE WELL-BEING
Input
ADAPTIVE SKILLS
PARTICIPATION
CONTEXTPersonal Factors •
• Environmental Factors
Human Functioning Dimensions
HEALTH
INTELLECTUAL •
•
•
•
•
FUNCTIONING
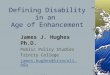
Figure 1 Functionality model.
4Journal of Intellectual Disability Research
R. Luckasson & R. L. Schalock • A functionality approach
© 2012 The Authors. Journal of Intellectual Disability Research © 2012 Blackwell Publishing Ltd

ment from both a legal and service delivery per-spective. Legally, we have seen that people with IDhave a right to a free and appropriate public educa-tion, community-based services and freedom fromoverly restrictive environments (Stowe et al. 2006).Programmatically, we have seen the egalitarianmovement reflected in services and supports basedon the concept of person-centred planning, self-advocacy and empowerment, and the enhancementof personal, quality of life-related outcomes(Shogren et al. 2009).
This changed view of persons with disabilities isreflected in the development of progressive interna-tional conventions such as the Universal Declarationof Human Rights (1948) and the Declaration on theRights of Mentally Retarded Persons (1971) that wereintended to guide the policy of governments andpublic authorities. Rights, however, are not suffi-cient if they are not accompanied by opportunitiesto exercise those rights. Therefore, The StandardRules on the Equalisation of Opportunities for Personswith Disabilities (1993) was an important additionalinternational document defining the societal pre-requisites of equality. In 2006, the Standard Ruleswere replaced by the United Nation’s Conventionon the Rights of Persons with Disabilities (UnitedNations 2006). The rules state the socio-politicalconditions for achieving equality, autonomy, non-discrimination, participation and inclusion insociety. The Convention stresses that persons withdisabilities should be able to participate fully in allaspects of life and specifies necessary social andlegal conditions for achieving such participation.As summarised by Buntinx & Schalock (2010) andVerdugo et al. (in press) the Convention Articlesaddress the following aspects of human function-ing: rights (access and privacy); participation;autonomy, independence and choice (i.e. self-determination); physical well-being; materialwell-being (work/employment); social inclusion,accessibility and participation; emotional well-being(freedom from exploitation, violence and abuse);and personal development (education andrehabilitation).
In summary, these three factors have moved thefield of ID to a recognition of the multiple inter-related factors impacting human functioning, thedevelopment of a multidimensional conceptualisa-tion of human functioning, a recognition of the
significant role that systems of supports play inenhancing human functioning and a framework toevaluate human functioning outcomes. What is stillneeded, however, is a synthesis or integration ofthese factors into a heuristic functionality modelthat can guide the field in the future. Such a modelis described next.
Parameters of a functionality model
Models are developed to aid people’s thinking andfacilitate dialogue and problem solving. The ratio-nale for the model presented in this section of thearticle is that the contextual factors previouslydiscussed (role of environments, components ofhuman functioning and policy changes) have movedthe field away from a primarily descriptive model ofdisability to a functionality model that can be usedfor multiple purposes.
The model presented in Fig. 1 incorporates thethree contextual factors just discussed into asystems approach to conceptualising human func-tioning as an integrated system, with input andthroughput factors whose impact can be evaluatedon the basis of three human functioning outcomes:social–economic status, health status and subjectivewell-being. In addition, the proposed model inte-grates current best practices in the field of ID inreference to: using programme logic models toarticulate the operative relationships among thecritical factors impacting human functioning (Millaret al. 2001; Donaldson 2007), providing systems ofsupports to enhance human functioning (Thomp-son et al. 2009; Schalock et al. 2010) and operation-ally defining human functioning outcomes on thebasis of valued indicators of life events and circum-stances (World Health Organization Quality of LifeWork Group 1995; World Health Organization1997; Cummins 2005; Emerson et al. 2006; UnitedNations 2006; Schalock et al. 2010; Shogren &Turnbull 2010; Walsh et al. 2010).
The functionality model shown in Fig. 1 reflectsthe three 21st century thinking styles of systemsthinking, synthesis and alignment (Schalock &Verdugo 2012). Systems thinking focuses on themultiple factors that affect human functioning andreflects the critical roles played by the micro-,meso- and macrosystems. Synthesis involves theintegration of information from multiple sources to
5Journal of Intellectual Disability Research
R. Luckasson & R. L. Schalock • A functionality approach
© 2012 The Authors. Journal of Intellectual Disability Research © 2012 Blackwell Publishing Ltd

improve the precision, accuracy and validity of adecision or practice. Alignment means to place criti-cal organisation and system functions into a logicalsequence. Alignment, which is typically depictedand implemented through a programme logicmodel, positions the input, throughput and output/outcome components of planning or implementa-tion into a logical sequence for the purposes ofreporting, monitoring, evaluation and continuousquality improvement.
These three thinking styles are reflected in thefunctionality model that integrates a socio-ecological model of disability with the changingsocietal views of persons with disabilities, and alignsthe supports paradigm with enhanced human func-tioning and desired personal outcomes. Systemsthinking is incorporated into each of the three com-ponents (i.e. input, throughput and output). Syn-thesis is reflected in the integration of the humanfunctioning dimensions (input component), systemsof supports (throughput component) and humanfunctioning outcomes (output component). Align-ment is reflected in the logical sequence of thesethree components.
Input component
The input component is composed of the slightlyrevised human functioning dimensions containedin the current ICF and AAIDD models. The corecomponents of the ICF model are incorporated intothe input component shown in Fig. 1 as follows: the‘health condition’ is incorporated into the healthdimension; ‘body functions’ are incorporated intothe intellectual functioning dimension; ‘activities’are incorporated into the adaptive skills dimension;and ‘personal and environmental factors’ are incor-porated into the context dimension.
Throughput component
The throughput component is composed of systemsof supports. Such systems include technology (e.g.assistive, information and prosthetic devices), skillsand knowledge, environmental accommodation,incentives, befriending, personal characteristics,natural supports, professional services, and policiesand practices (Wile 1996; Thompson et al. 2009;Schalock & Verdugo 2012).
Output component
The output component is composed of three humanfunctioning outcome categories and associated indi-cators that represent valued life events and circum-stances. The three outcome categories, whichoperationally define human functioning outcomes,are used frequently to analyse and evaluate publicpolicy outcomes (Cummins 1998, 2005; Emersonet al. 2006; Emerson & Hatton 2008; Mackenbachet al. 2008; Shogren & Turnbull 2010). Specificoutcome measures are:• education status, employment status and income(socio-economic status);• longevity, wellness and access to health care(health status); and• life satisfaction, positive affect such as happinessand contentment, quality of life domains andabsence of negative affect such as sadness, worry orhelplessness (subjective well-being).
Application of the model
From our perspective, not every aspect of thefunctionality approach will be apparent in everyclinical practice or activity. However, we feelstrongly that the functionality approach sets thestage for a better understanding of ID, and certainaspects of the model will be applied in reference toclinical functions related to defining ID, assessment,classification, planning supports and evaluatingoutcomes.
Better understanding
Terminology and concepts used in one field or pro-fession (such as ID) are frequently not understoodclearly by members of another field or profession.As a result, confusion and misunderstanding canoccur about ‘what is ID?’ Based on the functionalitymodel presented in Fig. 1, a better understanding ofID is based on the fact that: (1) ID is characterisedby significant limitations in both intellectual func-tioning and adaptive behaviour; (2) limitations inthe individual’s present functioning must be consid-ered within the context of the other dimensions ofhuman functioning that involve health, participationand context; (3) within an individual, limitationsoften coexist with strengths; (4) adaptive behaviour
6Journal of Intellectual Disability Research
R. Luckasson & R. L. Schalock • A functionality approach
© 2012 The Authors. Journal of Intellectual Disability Research © 2012 Blackwell Publishing Ltd

is conceptually different from maladaptive orproblem behaviour; (5) limitations in present func-tioning must be considered within the context ofcommunity environments typical of the individual’sage peers and culture; (6) an important purposeof describing limitations is to develop a profile ofneeded supports; and (7) with appropriate person-alised supports over a sustained period, the lifefunctioning of the person with ID generally willimprove (Luckasson et al. 1992, 2002; Schalocket al. 2007, 2010, 2012).
Defining
A functionality approach will impact defining a par-ticular condition and the assumptions underlying itsapplication. This application is exemplified currentlyin four of the five assumptions related to the currentAAIDD operational definition of ID which is that:
Intellectual disability is characterised by signifi-cant limitations both in intellectual functioningand in adaptive behavior as expressed in concep-tual, social, and practical adaptive skills. This dis-ability originates before age 18. (Schalock et al.2010, p. 1)
Specifically, and in reference to the input compo-nent of the functionality model presented in Fig. 1,the human functioning dimensions of context andparticipation are incorporated in the first assump-tion, ‘limitations in present functioning must beconsidered within the context of community envi-ronments typical of the individual’s age peers andculture’. Health is incorporated in the secondassumption, ‘valued assessment considers culturaland linguistic diversity and differences in communi-cation, sensory, motor, and behavioural factors’.The role of supports is incorporated in the fourthassumption, ‘an important purpose of describinglimitations is to develop a profile of needed sup-ports’. Human functioning outcomes are incorpo-rated in the fifth assumption, ‘with appropriatepersonalised supports over a sustained period, thelife functioning of persons with ID generally willimprove’ (Schalock et al. 2010, p. 1).
Assessment
Typically, assessment in the field of ID hasinvolved systematically collecting information for
decision making and communication related tothree assessment functions: diagnosing, classifyingand planning individualised supports. Within eachof these functions, professionals conduct assess-ments for a variety of specific purposes. Forexample, a diagnosis might determine an individu-al’s eligibility for services or legal protections,or it might establish whether a person could beincluded in a research study. Based on the avail-able assessment information and purpose, classifi-cation activities could focus on classifying forintensity of needed supports, research purposesand/or reimbursement/funding. Support intensitymeasures, such as the Supports Intensity Scale(Thompson et al. 2004) have been developedto determine the pattern and intensity of theindividual’s needed supports.
A functionality approach facilitates a multidimen-sional approach to assessment that is a prerequisiteto the development and implementation of a multi-dimensional classification system. As shown inTable 1 (middle column), there are numerous mea-sures to assess each of the six input dimensions ofthe proposed functionality model (see Fig. 1). Alisting of specific assessment instruments withineach of the exemplary categories can be found inSchalock et al. (2010, pp. 78–9).
A multidimensional approach to assessmentwithin a functionality approach to ID will allowprofessionals to integrate an operational and aconstitutive definition into an integrative diagnosticand classification system. An operational definitionis a more practical and applied definition thatmakes it possible to precisely define the class andidentify individuals with ID. In distinction, a con-stitutive definition is a more theoretical definitionthat is used to define the theoretical constructbehind ID in relation to related theoretical con-structs such as a multidimensional model of humanfunctioning, an ecological model of disability andthe supports paradigm (Wehmeyer et al. 2008;Schalock et al. 2010). Collectively, these two defini-tional approaches facilitate a better understandingof ID and its construct, and allow professionals tobetter align the multidimensionality of human func-tioning with clinical activities related to assessment,diagnosis, classification, planning and implementingindividualised supports, and evaluating personaloutcomes.
7Journal of Intellectual Disability Research
R. Luckasson & R. L. Schalock • A functionality approach
© 2012 The Authors. Journal of Intellectual Disability Research © 2012 Blackwell Publishing Ltd

Classification
Classifying refers to breaking the large group ofpeople diagnosed with ID into smaller segmentsbased on criteria selected for a specific purpose.The major impact of a functionality approach onclassification activities is to take a broader approachto classification than the IQ referenced system(mild, moderate, severe, profound) that has typicallybeen used historically. As discussed in Schalocket al. (2010, 2012), a classification system has toserve a purpose, be based on a coherent theoreticalframework, contribute to the efficient organisationof knowledge for application to practice and beused to better understand the person.
As the field of ID moves increasingly to an eco-logical focus and a supports paradigm, a number ofcurrent policies and practices have emerged thatrequire a broader, multidimensional approach toclassification. These changes relate to: (1) groupingfor reimbursement/funding on the basis of somecombination and weighting of levels of assessedsupport needs, level of adaptive behaviour, healthstatus and/or contextual factors such as residentialplatform and geographical location; (2) researchmethods that focus not just on the assessed level ofintellectual function or adaptive behaviour, but alsoon the multidimensional predictors of human func-tioning outcomes; and (3) individualised services
and supports based on the pattern and intensity ofassessed support needs across dimensions of humanfunctioning and life activities. Within this context,and based on the input, throughput and outputcomponents shown in Fig. 1, the parameters of amultidimensional classification system based on afunctionality approach could include classificationbased on the five human functioning dimensions,the intensity of assessed support needs and/or thelevel of one or more human functioning outcomes.
As a result of these changes in policies and prac-tices, multidimensional classification frameworks areemerging that reflect the multidimensionality ofhuman functioning. One such framework, which isconsistent with both the ICF and the AAIDDmodels, is shown in Table 1 (right column). Thematerial in the table lists exemplary measures andclassification schemes for each of the five humanfunctioning dimensions plus a ‘supports’ dimension.The authors recognise that considerable work is yetto be done in this area – work that is currentlybeing engaged in by one or more ICD-11 andAAIDD work groups.
Planning supports
A functionality approach will impact supports plan-ning in three significant ways. First, the focus ofassessment will expand to include assessing the
Table 1 Exemplary components of a multidimensional assessment and classification system within a functionality approach to intellectualdisability
Dimension Exemplary measures Classification scheme
Intellectual functioning Individually administered IQ tests IQ ranges or levelsAdaptive behaviour Adaptive behaviour scales Adaptive behaviour levelsHealth Health and wellness inventories Health status
Mental health measures Mental health statusEtiological assessment Risk factors
Etiological groupingsParticipation Community integration scales Degree of community integration
Community involvement scales Degree of community involvementMeasures of social relationships Level of social interactionsMeasures of home life Level of in-home activities
Context Environmental assessments (physical, social, attitudinal) Environmental statusPersonal assessments (motivation, coping styles,
learning styles, lifestyles)Personal status
Supports Support need scales Level of needed supportFunctional behavioural assessment Pattern of needed supports
8Journal of Intellectual Disability Research
R. Luckasson & R. L. Schalock • A functionality approach
© 2012 The Authors. Journal of Intellectual Disability Research © 2012 Blackwell Publishing Ltd

pattern and intensity of the individual’s supportneeds. This assessment will centre on what specificsupports the person needs to be more successful inlife activities rather than solely a description of theperson’s level of intellectual functioning or adaptivebehaviour. Second, clinicians and other profession-als will become more proficient in understandingand implementing systems of supports that: (1)organise potential support categories into a systemthrough which individualised supports can beimplemented to enhance intellectual functioning,adaptive skills, health, participation, and contextand/or human functioning outcomes; (2) provide aframework for coordinating the procurement ofindividual support strategies across the sources ofsupport that include natural supports, technology,environmental accommodation, support staff-directed activities, professional services, and organi-sation and system-level policies and practices; and(3) provide a framework for evaluating the impactof individualised supports on human functioningoutcomes (Schalock & Verdugo 2012).
The third impact of a functionality approach onsupports planning is that clinicians and other profes-sionals will increasingly incorporate evidence-basedpractices in making clinical decisions about the sup-ports individuals receive in specific situations.Thedetermination of evidence-based practices necessi-tates clearly operationalised support strategies that areused as independent variables, and clearly opera-tionalised and measured human functioning outcomesthat are used as dependent variables in evidence-based research studies (Schalock et al. 2011).
Outcomes evaluation
The functionality model shown in Fig. 1 provides aconceptual and measurement framework for assess-ing human functioning outcomes related to a per-son’s socio-economic status, health status andsubjective well-being. These outcome measuresreflect the intended impact of public policiestowards people with ID. The focus of these mea-sures also reflects the movement within the ID fieldaway from a primary focus on diagnosis and classi-fication to an emphasis on the planning and provi-sion of individualised supports that enhance humanfunctioning. Furthermore, outcome measures resultin information that is responsive to the quality revo-
lution, with its emphasis on valued outcomes, thereform movement, with its focus on outcomesrather than inputs and throughputs, the movementtowards evidence-based practices, and the qualitymanagement movement, with its emphasis on usingpersonal outcomes for continuous quality improve-ment. These outcomes can be used for multiplepurposes including analysing the impact of specificpublic policies, monitoring the effectiveness andefficiency of services and supports, providing a basisfor continuous quality improvement and perfor-mance enhancement, meeting the increasing needfor accountability and helping establish the param-eters of best practices (Shogren et al. 2009; Scha-lock et al. 2010; Shogren & Turnbull 2010; Schalock& Verdugo 2012).
Potential impacts of a functionalityapproach on professional practices
We envision at least four significant impacts of thefunctionality approach on professional practices inthe field of ID. These are to: (1) focus on the inte-grative nature of human functioning; (2) provide aunified language; (3) align clinical functions; and(4) encourage evidence-based practices.
Integrative nature of human functioning
A functionality approach will sensitise professionalsto the interactive nature of human functioningdimensions, systems of supports and human func-tioning outcomes. Understanding this interactivenature is maximised when one uses a systems per-spective in which human functioning dimensionsare viewed as significant input variables that deter-mine both the pattern and intensity of an individu-al’s supports needs and the selection of specificsupport strategies. The support strategies that areprovided, in turn, interact with relative levels ofthe human functioning dimension(s) and relevantcomponents of the meso- and macrosystems toproduce differential levels of human functioningoutcomes.
Unified language
A functionality model that integrates the multidi-mensionality of human functioning, the role that
9Journal of Intellectual Disability Research
R. Luckasson & R. L. Schalock • A functionality approach
© 2012 The Authors. Journal of Intellectual Disability Research © 2012 Blackwell Publishing Ltd

systems of supports play in enhancing human func-tioning and the evaluation of human functioningoutcomes provides a unified language that can beused across disciplines, organisations and systems topromote public policies, professional standards andorganisation practices that enhance the functioningof an individual with ID. In addition, an integrativeconceptual and measurement framework such asdescribed in this article can reduce the discrepancybetween contemporary thinking and how variousorganisations define and operationalise disability.Reducing this discrepancy will require a betteralignment of operational frameworks and a shift inevaluation, intervention and outcomes evaluationprocesses to reflect current best practices (Bruyereet al. 2005; Brandt et al. 2011; Salvador-Carulla &Gasca 2011).
Align clinical functions
A functionality approach will cause clinicians torealise that they should do more than just diagnoseand/or classify individuals with ID; rather, bestpractices dictate that they align their professionalcontributions with the contributions of collaborat-ing team members to diagnose and assess function-ing, determine support needs, plan and implementindividualised supports, and assess personal out-comes. This alignment requires that cliniciansaddress four basic questions (Buntinx & Schalock2010): (1) what are the limitations of the personin terms of diagnosis and present functioning? (2)what are the supports needed by the person toenhance human functioning? (3) what actionsshould be planned and implemented in order torespond to the person’s support needs? and (4) didthe person benefit from the support interventions?The alignment of these four professional activitiesrepresents a logical sequence of actions that guideand support best professional practices.
Encourage evidence-based practices
The concept and application of evidence-based prac-tices originally started in medicine in the 1990s andhas spread rapidly to many social and behaviouraldisciplines including ID. Across these broad areas,evidence-based practices generally refer to the use ofcurrent best evidence in making clinical decisions
about the interventions and/or supports that servicerecipients receive in specific situations. Despite theirwidespread advocacy and use, there are at leastthree perspectives on evidence and evidence-basedpractices (Schalock et al. 2011; Schalock &Verdugo 2012): the empirical–analytical, thephenomenological–existential and the post-structural.These three perspectives relate to differentapproaches to intervention and the conceptualisa-tion, measurement and application of evidence-based practices.The empirical–analytical perspectiveplaces a premium on experimental or scientificevidence as the basis for evidence-based practices.The phenomenological–existential perspectiveapproaches treatment or intervention success basedon the reported experiences of well-being concern-ing the intervention. From the post-structural per-spective, treatment or intervention decisions andintervention success is based on an understandingof public policy principles such as inclusion, self-determination, participation and empowerment.
At the individual level – and from the perspectiveof a functionality approach to ID – the practices inquestion typically relate to assessment, diagnosis,classification, the provision of systems of supportsand the evaluation of human functioning outcomessuch as those listed in Fig. 1. Over time, as ourunderstanding of disability and human functioninghas deepened, and as outcomes evaluation hasbecome a part of professional best practices, we arenow in a better position to evaluate the specificeffects of specific policies and practices.This abilitywill lead increasingly to a better understanding ofthe characteristics and components of evidence-based practices, and to a policy-relevant, multidi-mensional framework for data collection (Zola 1993;Walkup 2000; Duchan 2004).
Conclusion
As discussed throughout the article there are anumber of advantages to a functionality approach. Inaddition to those advantages and impacts discussed,we also point out that such an approach incorporatesa holistic view of human beings and their lives,provides a new common language among disparateprofessionals and the individual and his or herfamily, creates the opportunity for a more compre-
10Journal of Intellectual Disability Research
R. Luckasson & R. L. Schalock • A functionality approach
© 2012 The Authors. Journal of Intellectual Disability Research © 2012 Blackwell Publishing Ltd

hensive and flexible approach to supports provisionand allows for a more effective and comprehensiveevaluation of meaningful personal outcomes.
The authors also recognise potential challengesposed by the functionality approach. Chief amongthese are: it is a relatively new paradigm and willrequire new thinking styles, mental models and timeto implement; the data obtained from the approachmay be difficult to integrate into existing national orinternational data collection surveys; the approach ismore complex than one that focuses solely on staticlabelling – and hence, diagnostic reliability may becompromised initially; and the proposed approachmay be incompatible with historical language andparadigms in a particular profession or jurisdiction.
Approaches such as those discussed in this articleare developed to aid people’s thinking and facilitatedialogue and problem solving. Today, the field of IDis in an enviable position to better integrate currentthinking and align itself with desired future policiesand practices regarding persons with ID. This effortwill require rethinking the role that human func-tioning plays in defining a condition, diagnosingindividuals who meet the operational criteria, classi-fying on the basis of a multidimensional classifica-tion system, planning supports and evaluatinghuman functioning outcomes. Integrating thesefunctions into a coherent model, which positivelyaffects clinical functions, professional practices andthe life functioning of individuals with ID, will bechallenging. Our primary purpose in writing thisarticle is to define and describe a functionalityapproach to ID that facilitates this integration andthus begin a dialogue and discussion around theapplications of such an approach in the field of ID.
References
Brandt D. E., Houtenville A. J., Huynh L. C. & RaschE. K. (2011) Connecting contemporary paradigms tothe Social Security Administration’s disability evaluationprocess. Journal of Disability Policy Studies 22, 116–28.
Bronfenbrenner U. (1977) Toward an experimentalecology of human development. American Psychologist32, 513–31.
Bronfenbrenner U. (1999) Environments in developmentalperspective: theoretical and operational models. In:Measuring Environments Across the Life Span: EmergingMethods and Concepts (eds S. L. Friedman & T. D.Wachs), pp. 3–28. American Psychological Association,Washington, DC.
Bruyere S. M., Van Looy S. A. & Peterson D. B. (2005)The International Classification of Functioning, Disabil-ity and Health (ICF): contemporary literature review.Rehabilitation Psychology 50, 113–21.
Buntinx W. H. E. (2006) The relationship between theWHO-ICF and the AAMR-2002 system. In: What IsMental Retardation? Ideas for an Evolving Disability inthe 21st Century (eds H. Switzky & S. Greenspan), pp.303–23. American Association on Mental Retardation,Washington, DC.
Buntinx W. H. E. & Schalock R. L. (2010) Models ofdisability, quality of life, and individual supports: impli-cations for professional practice in intellectual disability.Journal of Policy and Practice in Intellectual Disabilities 7,283–94.
Claes C., vanHove G., Vandevelde S., van Loon J. &Schalock R. L. (2010) Person-centered planning:analysis of research and effectiveness. Intellectual andDevelopmental Disabilities 48, 432–53.
Cohen F. S. (1935) Transcendental nonsense and thefunctional approach. Columbia Law Review 35, 809–49.
Cummins R. A. (1998) The second approximation to anindividual standard for life satisfaction. Social IndicatorsResearch 43, 307–34.
Cummins R. A. (2005) Moving from the concept ofquality of life to a theory. Journal of Policy and Practicesin Intellectual Disabilities 49, 699–706.
Donaldson S. I. (2007) Program Theory-Driven EvaluationScience. Lawrence Erlbaum Associates, New York.
Duchan J. F. (2004) Where is the person in the ICF?Advances in Speech-Language Pathology 6, 63–5.
Emerson E. & Hatton C. (2008) Self-reported well-beingof women and men with intellectual disabilities inEngland. American Journal on Mental Retardation 113,143–55.
Emerson E., Graham H. & Hatton C. (2006) The mea-surement of poverty and socio-economic positioninvolving people with intellectual disability. In: Interna-tional Review of Research in Mental Retardation (ed.L. M. Glidden), pp. 77–108. Academic Press, New York.
Fortune J., Agosta J., Auerbach K., Kimmich M., MeldaK., Smith D. et al. (2009) Developing ReimbursementLevels Using the Supports Intensity Scale (SIS) in Louisi-ana. Human Services Research Institute, Portland, OR.
Luckasson R., Coulter D., Polloway E., Reiss S., SchalockR. L., Snell M. et al. (1992) Mental Retardation: Defini-tion, Classification, and Systems of Supports. AmericanAssociation on Mental Retardation, Washington, DC.
Luckasson R., Borthwick-Duffy S., Buntinx W., CoulterD., Craig P., Reeve A. et al. (2002) Mental Retardation:Definition, Classification, and Systems of Support. Ameri-can Association on Mental Retardation, Washington,DC.
Mackenbach J. P., Stirbu I., Roskan A. R., Schapp M. M.,Menvielle G. & Kunst A. E. (2008) Socioeconomic
11Journal of Intellectual Disability Research
R. Luckasson & R. L. Schalock • A functionality approach
© 2012 The Authors. Journal of Intellectual Disability Research © 2012 Blackwell Publishing Ltd

inequalities in health in 22 European countries. TheNew England Journal of Medicine 358, 2468–81.
Mercer J. R. (1992) The impact of changing paradigmsof disability on mental retardation in the year 2000.In: Mental Retardation in theYear 2000 (ed. L. Rowitz),pp. 15–38. Springer-Verlag, New York.
Millar A., Simeone R. S. & Carvevale J. T. (2001) Logicmodels: a systems tool for performance management.Evaluation and Program Planning 24, 73–81.
Rioux M. H. (1997) Disability: the place of judgment in aworld of fact. Journal of Intellectual Disability Research41, 102–11.
Salvador-Carulla L. & Gasca V. I. (2011) The role offunctional disability in psychiatric classification. LifeSpan and Disability 13, 7–27.
Schalock R. L. & Verdugo M. A. (2012) A LeadershipGuide for Today’s Disabilities Organizations: OvercomingChallenges and Making Change Happen. Paul H. Brookes,Baltimore, MD.
Schalock R. L., Buntinx W., Borthwick-Duffy S., Luckas-son R., Snell M., Tasse M. J. et al. (2007) User’s Guide:Mental Retardation: Definition, Classification, and Systemsof Supports. American Association on Intellectual andDevelopmental Disabilities, Washington, DC.
Schalock R. L., Borthwick-Duffy S. A., Bradley V. J.,Buntinx W. H. E., Coulter D. L., Craig E. M. et al.(2010) Intellectual Disability: Definition, Classification, andSystems of Supports. American Association on Intellectualand Developmental Disabilities, Washington, DC.
Schalock R. L., Verdugo M. A. & Gomez L. E. (2011)Evidence-based practices in the field of intellectual anddevelopmental disabilities. Evaluation and Program Plan-ning 34, 79–89.
Schalock R. L., Luckasson R., Bradley V., BuntinxW. H. E., Lachapelle Y., Shogren K. et al. (2012) User’sGuide to Accompany the 11th Edition of Intellectual Disabil-ity: Definition, Classification, and Systems of Support:Appli-cations for Clinicians, Educators, Organizations ProvidingSupports, Policy Makers, Family Members and Advocates,and Health Care Providers. American Association on Intel-lectual and Developmental Disabilities, Washington, DC.
Shogren K. A. & Turnbull H. R. (2010) Public policy andoutcomes for persons with intellectual disability: extend-ing and expanding the public policy framework of the11th edition of Intellectual Disability: Definition, Classifica-tion, and Systems of Supports. Intellectual and Developmen-tal Disabilities 48, 375–86.
Shogren K. A., Bradley V. J., Gomez S., Yeager M. H.,Schalock R. L., Borthwick-Duffy S. et al. (2009) Publicpolicy and the enhancement of desired outcomes forpersons with intellectual disability. Intellectual andDevelopmental Disabilities 47, 307–19.
Stowe M. J., Turnbull H. R. & Sublet C. (2006) TheSupreme Court, ‘our town’, and disability policy:boardrooms and bedrooms, courtrooms and cloak-rooms. Mental Retardation 44, 83–99.
Thompson J. R., Bryant B., Campbell E., Craig E. M.,Hughes C., Rotholz D. A. et al. (2004) The SupportsIntensity Scale (SIS): User’s Manual. American Associa-tion on Mental Retardation, Washington, DC.
Thompson J. R., Bradley V., Buntinx W. H. E., SchalockR. L., Shogren K. A., Snell M. A. et al. (2009) Concep-tualizing supports and the support needs of people withintellectual disability. Intellectual and DevelopmentalDisabilities 47, 135–46.
United Nations (2006) Convention on the Rights of Personswith Disabilities. Available at: http://www.un.org/disabilities/default.asp?navid=14&pid=150 (retrieved 25
April 2011).
Verdugo M. A., Navas P., Gomez L. E. & Schalock R. L.(in press) The concept of quality of life and its role inenhancing human rights in the field of intellectual dis-ability. Journal of Intellectual Disability Research.
Walkup J. (2000) Disability, health care, and public policy.Rehabilitation Psychology 45, 409–22.
Walsh P. N., Emerson E., Lobb C., Hatton C., Bradley V.,Schalock R. L. et al. (2010) Supported accommodationfor people with intellectual disabilities and quality oflife: an overview. Journal of Policy and Practice in Intellec-tual Disabilities 7, 137–42.
Wehmeyer M. L., Buntinx W. H. E., Lachapelle Y., Luck-asson R., Schalock R. L., Verdugo M. A. et al. (2008)The intellectual disability construct and its relationto human functioning. Intellectual and DevelopmentalDisabilities 46, 311–18.
Wile D. (1996) Why doers do. Performance and Instruction35, 30–5.
World Health Organization (1997) Measuring Quality ofLife. World Health Organization, Geneva.
World Health Organization (2001) International Classifica-tion of Functioning, Disability, and Health. World HealthOrganization, Geneva.
World Health Organization (2007) International Classifica-tion of Functioning, Disability, and Health: Children andYouthVersion. World Health Organization, Geneva.
World Health Organization Quality of Life Work Group(1995) The World Health Organization Quality of LifeAssessment (WHOQOL). Position paper from the WorldHealth Organization. Social Science Medicine 41, 1403–9.
Zola I. K. (1993) Disability statistics, what we count andwhat it tells us: a personal and political analysis. Journalof Disability Policy Studies 4, 9–39.
Accepted 17 April 2012
12Journal of Intellectual Disability Research
R. Luckasson & R. L. Schalock • A functionality approach
© 2012 The Authors. Journal of Intellectual Disability Research © 2012 Blackwell Publishing Ltd