-
7/29/2019 Deep Lamellar Keratoplasty
1/5
Deep Lamellar KeratoplastyUsing Viscoelastic Dissection
Edward E. Manche, MD; Gary N. Holland, MD; Robert K. Maloney,
MD, MA
We describe a technique for performing deep lamellar
keratoplasty using viscoelas-
tic dissection. Deep lamellar dissections of the cornea using
viscoelastic sub-
stances (sodium hyaluronate) were performed on 4 eyes of 4
patients. One pa-
tient with keratoconus and another with corneal scarring
underwent lamellar
keratoplasty using the technique as the sole procedure for
visual rehabilitation. Two patients (2 eyes)
with opaque corneas underwent deep lamellar dissection with
removal of stromal tissue to allow vi-
sualization of the anterior segment structures prior to
penetrating keratoplasty, thereby facilitating
separation of iridocorneal adhesions as the Descemet membrane
was incised. Deep lamellar dissec-tion was performed without
complications related to the procedure in all 4 eyes. The 2
lamellar grafts
cleared completely, and both eyes achieved excellent visual
acuity with spectacle correction. In the
other 2 eyes, deep lamellar dissection provided clear
visualization of anterior segment structures dur-
ing incision of the Descemet membrane. Deep lamellar dissection
using viscoelastic substances is a
useful technique during lamellar keratoplasty. Arch Ophthalmol.
1999;117:1561-1565
Lamellar keratoplasty is a procedure inwhich a donor graft is
placed within a par-tial depth recipient corneal bed after a
la-mellar resection has removed abnormalstromal tissue from the
host. The proce-
dure can be used to restore the optical orstructural integrity
of the globe; cur-rently,it is used most commonly
duringtheplacement of tectonic grafts to restore nor-mal thickness
to globes after loss of tissuefrom thinning disorders of the
cornea.
Today, the procedure is used infre-quently for restoration of
vision because itis technically more difficultto perform andhas
traditionally yieldedinferior optical re-sultswhen compared
withpenetrating kera-toplasty. Nevertheless, lamellar kerato-plasty
has a number of advantages overpenetrating keratoplasty. With
lamellar
keratoplasty, the patients endothelium re-mains intact,
eliminating the risk of endo-thelial rejection, which is the most
com-mon cause of graft failure followingpenetrating keratoplasty.
Another advan-tage of lamellar keratoplasty is that the
structural integrity of the globe is bettermaintained than with
penetrating kerato-plasty.
There are a variety of techniques forperforming lamellar
keratoplasty.1-17 Tra-
ditionally, the lamellar resection has
beenperformedmanually,using sharp andbluntdissection.2-6,14,15
Others have tried usingair dissection,1,9 microkeratome
dissec-tion,10,11 dissection using the excimer la-ser,12 and
hydrodelamination using sa-line dissection,16 all with varying
degreesof success. Sun and coauthors17 de-scribeda similar
technique they termed vis-codelamination for the treatment of
bul-lous keratopathy.We describe a techniquefor performing deep
lamellar dissection ofthe cornea that uses a viscoelastic agentto
dissect all of the stromal tissue from the
underlying Descemet membrane and en-dothelium.
SURGICAL TECHNIQUE
Based on our experiences with these cases,we have found the
following procedures tobeeffective(Figure). After determining
theappropriate diameter of the tissue to be re-moved from the
patient, a trephine, or a
From the Department of Ophthalmology, Stanford University School
of Medicine,Stanford, Calif (Dr Manche); Department of
Ophthalmology, Jules Stein Eye Institute,University of California
at Los Angeles (Dr Holland); and the Maloney Vision Institute,Los
Angeles (Dr Maloney).
SURGICAL TECHNIQUE
ARCH OPHTHALMOL/ VOL 117, NOV 1999
WWW.ARCHOPHTHALMOL.COM1561
1999 American Medical Association. All rights reserved.on April
4, 2008www.archophthalmol.comDownloaded from
http://www.archophthalmol.com/http://www.archophthalmol.com/http://www.archophthalmol.com/http://www.archophthalmol.com/http://www.archophthalmol.com/
-
7/29/2019 Deep Lamellar Keratoplasty
2/5
combination of a trephine and arounded blade, is used to create
anincision of 80%to 90% thicknessintothe patients cornea (Figure,
A). APaufique blade is then used to makea deep incision that runs
parallel tothe stromal lamellae. This incisionshould start at the
bottom of the
trephine incision, moving radiallytoward the central cornea,
creatinga 1- to 2-mmpocket. The blade is re-moved, and a 25-gauge
cannula at-tached to a syringe containing vis-coelastic material is
introduced intothepocket(Figure, B).Theviscoelas-ticmaterial is
slowly injected into thispocket. It is forced through the
pos-terior stromal lamellae along thepathof least resistance,
causing the Des-
cemet membrane to separate from theposterior stromal tissue
(Figure, C).Once the Descemet membrane hasbegun to detach,
thecannulaisslowlyadvanced into the space being cre-ated, thereby
completing the dissec-tion(Figure, D). Corneal scissorsareused to
remove the diseased patient
tissueby cutting along thegroovecre-ated by the trephine. A
modificationof this technique can also be used incorneas with
severe opacification. Astab incision can be made into thecornea and
viscoelastic material in-fused through a cannula placed intothe
incision to separate the Desce-met membrane from the
overlyingstromaltissue. After separation of theDescemet membrane, a
trephine can
be used to cut a central groove intotherecipient corneal bed
until a gushof viscoelastic material is seen. Theoverlying tissue
can then be excisedusing corneal scissors withoutcausing damage to
the Descemetmembrane.
Forlamellar keratoplastiesa full-
thickness button from a donor ca-daver is then cutwith a
trephine, andthe endothelium is removed with amethylcellulose
sponge. The donorbutton is then sutured to the recipi-ent corneal
bed (Figure, E).After thedonor button has been sutured intoplace,
the remaining viscoelastic ma-terial is irrigated out of the
interfacewith a balanced salt solution in-fused through a 25-gauge
cannula.
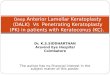
A
B
C
E
D
A, A trephine is used to make an 80%- to 90%-thick incision into
the hosts cornea. B, A sharp, rounded blade is used carefully at
the base of the groove to dissectthe deep stromal tissue parallel
to the Descemet membrane. A 25-gauge cannula is inserted into this
groove, and viscoelastic material (sodium hyaluronate[Healon]) is
slowly injected. C, The viscoelastic material is forced between the
corneal lamellae in a central direction, dissecting the Descemet
membrane from theoverlying stroma. D, The cannula is advanced into
the space between the stroma and detached Descemet membrane as
viscoelastic material is injected tocomplete the dissection. E, The
donor graft is sewn into the recipient corneal bed and the
viscoelastic material irrigated from the interface between the
donortissue and the patients Descemet membrane.
ARCH OPHTHALMOL/ VOL 117, NOV 1999
WWW.ARCHOPHTHALMOL.COM1562
1999 American Medical Association. All rights reserved.on April
4, 2008www.archophthalmol.comDownloaded from
http://www.archophthalmol.com/http://www.archophthalmol.com/http://www.archophthalmol.com/http://www.archophthalmol.com/http://www.archophthalmol.com/
-
7/29/2019 Deep Lamellar Keratoplasty
3/5
For penetrating keratoplastiesthe same techniques are used.
Fol-lowing resection of the diseasedstro-mal tissue from the
Descemet mem-brane,iris-endothelial adhesions andother anterior
segment abnormali-ties can be seen through the trans-parent
Descemet membrane. Thesurgeon then carefully incises the
Descemet membrane and separatesadhesions from the underlying
tis-sue, with direct visualization pre-venting the inadvertent
incision ofunderlying anterior segment struc-tures. The Descemet
membrane canthen be incised along the trephineincision, and a
full-thickness do-nor button can be sutured to the re-cipient
corneal bed.
REPORT OF CASES
CASE 1
A 48-year-old man with keratoco-nus had a best-corrected visual
acu-ity of 20/30 OS because of keratoco-nus; a visual acuity of
countingfingers at 2 ft OD was uncorrectablebecause of previous
trauma. He wasunable to tolerate spectacle correc-tion because of
distortion. His best-corrected visual acuity was 20/25OSwith a
rigid, gas permeable contactlens, but he was intolerant ofthe
lens.Deep lamellar keratoplasty as a tech-nique for optical
restoration wasper-
formed to minimize the risk of graftrejection. Using an 8-mm
suction tre-phine, a partial-thickness groove wasmade in the
recipient corneal bed.The wound was separated in the 10-oclock
position using Colibri for-ceps, and a rounded blade was thenused
to make a deep incision that ranparallel to the stromal lamellae.
Theincision began at the bottom of thetrephine incision, moving
radially to-ward thecentral cornea, creating a 1-to 2-mm pocket.
Theviscoelasticma-terial, sodium hyaluronate (Healon),
was slowly injected into this pocket.It was forced through the
posteriorstromal lamellae along the path ofleast resistance,
causing the Desce-met membrane to separate from theposterior
stromal tissue. Corneal scis-sors were then used to separate
thepatients corneal stromal tissue fromthe underlying Descemet
mem-brane by cutting along the groovewith one blade between the
stroma
and Descemet membrane. Centralstromaltissuewasliftedfrom
theeye.The Descemet membrane remainedintact. An
8.25-mmfull-thicknessdo-nor button was cut with a trephine,and the
endothelium was removedwith a methylcellulose sponge. Thedonor
button was sutured to the re-cipient corneal bed. The remaining
viscoelastic material was then irri-gated from the interface
with a bal-anced salt solution using a 25-gaugecannula. The
postoperative coursewasuneventful, with complete clear-ing of the
graft occurring within 2weeks. The interface between thegraft and
Descemet membrane re-mained clear. The patient under-went selective
suture removal 3months postoperatively. Uncor-rected visual acuity
was 20/70 OS,and best spectacle-corrected visualacuity was 20/25 OS
with 3.5 diop-
ters (D) of residual astigmatism.
CASE 2
A 63-year-old man had a best-corrected visualacuity of
20/400OD,attributable to corneal thinning andscarring from a
previously treatedbacterial ulcer that extended ap-proximately 60%
to 70% into theanterior corneal stroma withoutinvolvement of the
Descemet mem-brane. Deep lamellar keratoplastywas performed for
visual rehabili-
tation. Using a 7.5-mm suction tre-phine, the same technique
used incase 1 was then employed to suc-cessfully dissect down to an
intactDescemet membrane. A 7.75-mmfull-thickness donor button was
su-tured to the recipient corneal bed.The postoperative course was
un-eventful, with complete clearing ofthe graft occurring within 3
weeks.The junction between the graft andDescemet membrane remained
clear.The patient underwent selective su-ture removal 3 months
postopera-
tively and had an uncorrected vi-sual acuity of 20/70 OD and a
bestspectacle-corrected visual acuity of20/30 OD with 2.5 D of
residualastigmatism.
CASE 3
An 8-year-old boy sustained a force-ful blowto the right eye
with a bluntobject 9 months prior to our exami-
nation. The trauma was compli-cated by total hyphema,
glaucoma,and subsequent dense blood stain-ing of the entire cornea.
Intraocularpressure could not be controlledwith topical
medications, and heunderwent cyclocryotherapy on 2occasions. He was
referred to us foradditional care that included pen-
etrating keratoplasty and surgery forglaucoma. Visual acuity was
lightperception OD with good color dis-crimination and entopic
phenom-enon.Findingsfrom ultrasound bio-microscopy indicated
extensivedisruption of the anterior segmentwith anterior synechiae
anddisplace-ment of the lens into the anteriorchamber.Because
evidence of iris ad-herence to the endothelial surfacecould not be
seen directly, deep la-mellar dissection was performed toremove
blood-stained stroma,
thereby allowing visualization of theiris through the Descemet
mem-brane prior to entering the anteriorchamber during penetrating
kera-toplasty. Using an 8-mm trephine,a partial-thickness groove
was madein the recipient corneal bed. Thewound was separated in the
10-oclock position using Colibri for-ceps, and a rounded blade was
thenused to make a deep incision that ranparallel to the stromal
lamellae. So-dium hyaluronate was slowly in-jected into this
pocket. It was forced
through the posterior stromal lamel-lae along the path of least
resis-tance, causing the Descemet mem-brane to separate from the
posteriorstromal tissue. Corneal scissorswereused to separate
blood-stained stro-mal tissue of the host by cuttingalong the
groove with one blade be-tween the stroma and Descemetmembrane.
Central stromal tissuewas lifted from the eye. The Desce-met
membrane remained intact. Aretrocorneal inflammatory mem-brane
could be seen clearly through
the Descemet membrane. The iristissue was adherent to the
endothe-lial surface, and a preexisting rent inthe anterior lens
capsule, attribut-ableto the patients previoustrauma,with release
of cortical material intothe anterior chamber, could be seen.The
Descemet membrane was care-fully incised in the 9-oclock posi-tion,
and a potential space wasidentified between the Descemet
ARCH OPHTHALMOL/ VOL 117, NOV 1999
WWW.ARCHOPHTHALMOL.COM1563
1999 American Medical Association. All rights reserved.on April
4, 2008www.archophthalmol.comDownloaded from
http://www.archophthalmol.com/http://www.archophthalmol.com/http://www.archophthalmol.com/http://www.archophthalmol.com/http://www.archophthalmol.com/
-
7/29/2019 Deep Lamellar Keratoplasty
4/5
membrane and underlying tissues.The Descemet membrane was
gen-tly separated from these underly-ing tissues as it was incised
along thetrephination wound. Using thesemaneuvers, no inadvertent
inci-sions were made in the iris tissue asit was dissected from the
endothe-lial surface. Cataract removal, pen-
etrating keratoplasty, and Ahmedvalve placement were
completedwithout difficulty.
CASE 4
A 79-year-old man had previouslyundergone repair of a
complicatedretinal detachment in the right eyeusing vitrectomy and
silicone oiltamponade. He was left aphakic andeventually developed
corneal de-compensation, attributable to sili-cone oil toxicity. He
was referred to
us for penetrating keratoplasty alongwith silicone oil removal
from thevitreous cavity to provide better vi-sualization of the
posterior seg-ment and for possible visual reha-bilitation. Prior
to surgery, it wasknown that the iris was adherent tothe posterior
surface of the corneain several areas, although anteriorsegment
structures could not be seenat the time of surgery because of
cor-neal clouding. A stab incision wasmade into the cornea at the
limbusin the 9-oclock position, and vis-
coelastic material (Healon) wasinstilled through deep corneal
la-mellae to separate the Descemetmembrane from overlying
stromaltissue over theentire area of thecor-nea. An 8-mm trephine
was thenused to cut a central groove into therecipient corneal bed.
A gush of vis-coelastic material (Healon) indi-cated that the
lamellar dissectionplane had been reached. The stro-m al t i ssue w
as ex ci sed usi ngcorneal scissors along the trephina-tion groove.
The Descemet mem-
brane remained intact. It was thenpossible to see anterior
segmentstructures through the Descemetmembrane. Several areas of
ante-rior synechiae were present. TheDescemet membrane was
incisedwith a supersharp blade in an areawithout iris adhesions,
and the in-cision was continued along thetrephination wound using
cornealscissors. During this process the iris
was separated from the Descemetmembrane ahead of the scissors
byblunt dissection using a cyclodialy-sis spatula. Following these
maneu-vers the anterior chamber was re-formed. Silicone oil removal
andpenetrating keratoplasty were com-pleted without
complications.
COMMENT
Detachment of the Descemet mem-brane following inadvertent
injec-tion of viscoelastic material ante-rior to the membrane has
beendescribed during intraocular sur-gery.18-21 These detachments
havebeen successfully repaired using avariety of techniques
includingplacementof sulfur hexafluoride gas(SF6), 22 air,23
viscoelastic sub-stances,24 and perfluoropropane gas(C3F8)25 into
the anterior cham-
ber. Spontaneous reattachment canalso occur.23 Based on these
obser-vations, we postulated that we couldcreate a controlled
separation of theDescemet membrane from overly-ing stromal tissue
using viscoelas-tic material to facilitate deep lamel-lar
dissection.
One of the reasons why tradi-tional lamellar keratoplasty
mayyield a suboptimal visual result isthat withcurrent
technologies, someof the stroma left behind during thelamellar
dissection becomes opaque
or contains residual diseased tis-sue. A variety of surgical
tech-niqueshave been developedover theyears to facilitatedeep
lamellar kera-toplasty and improve optical out-comes. Deep lamellar
dissectionwithintrastromal air was originally de-scribed by
Archila.1 Using this tech-nique, he was able to perform
deeplamellar dissectionsuccessfullyin 10eyes with no inadvertent
entry intothe anterior chamber. In anotherstudy,9 deeplamellar
dissection withintrastromal air was attempted in 10
eyes. Air dissection was performedsuccessfully in 6 of 10 eyes
in thatstudy. Conversion to full-thicknesspenetrating keratoplasty
was re-quired in4 of10 eyes because ofin-advertent perforation into
the Des-cemet membrane at the time ofsurgery. In only 1 of 6 eyes
that un-derwent successful air dissectionwasthe separation at the
Descemet mem-brane.
Deeplamellar keratoplasties us-ing Barraquer microkeratomes
havealso been attempted by several au-thors, with mixed
results.10,11 Thereare a number of technical difficul-ties in
performing microkeratome-assisted lamellar keratoplasty. In
ad-dition, the procedure results in onlya partial-thickness
dissection, leav-
ing residual corneal stroma downto the Descemet membrane;
thisresidual stromal tissue may opacify,necessitating eventual
performanceof a full-thickness penetrating kera-toplasty.
Deeplamellar keratoplasties us-ing hydrodelineation have also
beenattempted with some success.16 Us-ing this technique, saline
solution isinjected through a partial-thick-ness lamellar incision
using a blunt27-gauge cannula. The saline pen-etrates the stromal
collagen fibers,
causing them to whiten and swell.This in turn makes tissue
removalusing blunt dissection easier to per-form. Using this
technique, Sugitaand Kondo16 performed deeplamel-lar keratoplasty
on 120 eyes withcorneal stromal opacification. Theywere able to
successfully dissectdown to the Descemet membrane in75% of eyes
using this technique.However, they also reported a 39.2%rate of
puncture of the Descemetmembrane in this series of eyes. Theauthors
stated that none of the eyes
with punctures in the Descemetmembrane required conversion
topenetrating keratoplasty, and allhad similar outcomes to
eyeswithout puncture 6 months post-operatively.
Full-thickness keratoplasty us-ing viscodelamination has been
pre-viously described in the treatment ofpainful bullous
keratopathy.17 Sunand coauthors17 used this tech-nique to
facilitate dissection of cor-neal tissuein 21 eyes in
patientswithpainful bullous keratopathy. Using
this technique, Sun et al success-fully dissected the diseased
edema-tous corneal tissue in all of the eyeswith no cases of
inadvertent pen-etration of the Descemet mem-brane. They did not
dissect all theway down to the Descemet mem-brane but attempted to
remove asmuch of the edematous corneal tis-sue as possible. Six
months postop-eratively, the painfulsymptoms were
ARCH OPHTHALMOL/ VOL 117, NOV 1999
WWW.ARCHOPHTHALMOL.COM1564
1999 American Medical Association. All rights reserved.on April
4, 2008www.archophthalmol.comDownloaded from
http://www.archophthalmol.com/http://www.archophthalmol.com/http://www.archophthalmol.com/http://www.archophthalmol.com/http://www.archophthalmol.com/
-
7/29/2019 Deep Lamellar Keratoplasty
5/5
relieved in all of the cases, and amodest improvement in vision
wasachieved in 73% of the eyes. How-ever, since the underlying
cause ofthe bullous keratopathy is pre-sumed to be a poorly or
nonfunc-tioning endothelial pumpingmecha-nism, one would assume
that thedonor lamellar graft would eventu-
ally become edematous as well.All 4 patients in our study
hadsuccessful surgical outcomes; spe-cifically, there were no cases
of in-advertent puncture of the Descemetmembrane during
theviscoelasticdis-section. In the2 patients whounder-went lamellar
keratoplasty, thedonor grafts remained clear postop-eratively with
no evidence of inter-face opacification, host
endothelialdecompensation, pseudoanteriorchamber formation, or
complica-tions from retained viscoelastic sub-
stance. In the 2 patients who under-went penetrating
keratoplasty, theiris-endothelial adhesions, inflam-matory
membranes, and disruptedanterior segment
structuresweresuc-cessfully visualized prior to incisionof the
Descemet membrane, allow-ing us to avoid inadvertent surgicaltrauma
to normal tissues.
Thesurgical techniquewe havedescribed offers all of the
advan-tages of traditional lamellar kerato-plasty with the added
advantage ofleaving a clear interface. It shoulden-
able surgeons to remove all of thestroma from the underlying
Desce-met membrane safely and reliably,therebyeliminating the
potential dis-advantage of leaving residual tissuethat could
compromise vision. Thistechnique has the advantage over theother
full-thickness techniques, in-cluding air dissection and
hydrode-lamination, in that there is a low riskof inadvertent
puncture of the Des-cemet membrane, and it is techni-cally easy to
perform. The simplifi-cationof the techniqueshouldallow
surgeons to offer lamellar kerato-plasty to those patients who
havetheir disease process confined to thestroma with normal
endothelium.The technique is also a useful meansfor seeing anterior
segment struc-tures prior to incising the Desce-met membrane in
patients with sus-pected iridocorneal adhesions or
other disruption of normal ante-rior segment architecture. By
visu-alizing the tissue, inadvertent inci-sion of the iris can be
avoided.
Accepted for publication July16, 1999.This study was supported
in part
by Research to Prevent Blindness, Inc,New York, NY. Dr Maloney
is the re-cipient of a Research to PreventBlind-ness, Inc, Career
Development Award,and Dr Holland is the recipient of aResearch to
Prevent Blindness, Inc,Lew R. Wasserman Merit Award.
Corresponding author: EdwardE. Manche, MD, Stanford
UniversitySchool of Medicine, Department ofOphthalmology,
300PasteurDr, RoomA157, Stanford, CA 94305-5308(e-mail:
[email protected]).
REFERENCES
1. Archila EA. Deep lamellar keratoplasty dissec-
tion of host tissue with intrastromal air injection.
Cornea. 1985;3:217-218.
2. Morrison JC, Swan KC. Full thickness lamellar
keratoplasty: a histologic study in human eyes.Ophthalmology.
1982;89:715-719.
3. Gasset AR. Lamellar keratoplasty in the treat-
ment of keratoconus: conectomy. Ophthalmic
Surg. 1979;10:26-33.
4. Richard JM, Paton D, Gasset AR. A comparison
of penetrating keratoplasty and lamellar kerato-
plasty in the surgical management of keratoco-
nus. Am J Ophthalmol. 1978;86:807-811.
5. McDonald MB, Koenig SB, Safir A, Kaufman HE.
On-lay lamellar keratoplasty for the treatment of
keratoconus. Br J Ophthalmol. 1983;67:615-618.
6. Polack FM. Lamellar keratoplasty: Malbranss
peeling-off technique. Arch Ophthalmol. 1971;
86:293-295.
7. Wood TO. Lamellar transplants and keratoco-
nus. Am J Ophthalmol. 1977;83:543-545.
8. Ehrlich ML, Phinney RB, Mondino BH, Petitt TH.
Techniquesof lamellar keratoplasty. Int Ophthal-
mol Clin. 1988;28:24-29.
9. Price FWJr. Airlamellar keratoplasty. RefractCor-
neal Surg. 1989;5:240-243.
10. Hanna DK, David T, Besson J, Pouliquen Y. La-
mellar keratoplastywith theBarraquer microkera-
tome. Refract Corneal Surg. 1991;7:177-181.
11. Haimovici R, Culbertson WW. Optical lamellar
keratoplasty using the Barraquer microkera-
tome. Refract Corneal Surg. 1991;7:42-45.
12. Gabay S, Slomovic A, Jares T. Excimer laser-
processed donor corneal lenticules for lamellar
keratoplasty. Am J Ophthalmol. 1989;107:47-
51.
13. Yee RD, Pettit TH. Corneal intrastromal cyst fol-
lowing lamellar keratoplasty. Ann Ophthalmol.
1975;7:644-646.
14. Pettit TH. Corneoscleral freehand lamellar kera-
toplasty in Terriensmarginaldegenerationof the
cornea: long term results. Refract Corneal Surg.
1991;7:28-32.
15. Tsubota K, Kaido M, Yu M, et al. A new surgical
techniquefor deeplamellarkeratoplastywith single
running suture adjustment. Am J Ophthalmol.
1998;126:1-8.
16. Sugita J, Kondo J. Deeplamellarkeratoplasty with
complete removal of pathological stroma for vi-
sion improvement. Br J Ophthalmol. 1997;81:
184-188.
17. SunB, HeY, Ding X. Full thicknesslamellarkera-
toplasty withviscodelamination of corneafor treat-
ment of bullous keratopathy. Chung Hua Yen Ko
Tsa Chih. 1995;31:142-144.
18. Hoover DL, Giangiacomo J, Benson RL. Desce-
metsmembrane detachment by sodium hyaluro-
nate. Arch Ophthalmol. 1985;103:805-808.
19. Ostberg A, Tornqvist G. Management of detach-
ment of Descemets membrane caused by injec-
tion of hyaluronic acid. Ophthalmic Surg. 1989;
20:886-896.
20. Pieramici D, Green WR, Stark WJ. Stripping of
Descemets membrane: a clinicopathologic cor-
relation. Ophthalmic Surg. 1994;25:226-231.
21. MascaiMS. Totaldetachment of Descemetsmem-
braneafter smallincision cataract extraction. AmJ Ophthalmol.
1992;114:365-366.
22. Zusman NB,WaringGO, Narjarian LV,WilsonLA.
Sulfur hexafluoride gas in the repair of intrac-
table Descemets membrane detachment. Am J
Ophthalmol. 1987;104:660-662.
23. Walland MJ,Stevens JD,Steele AD.Repair ofDes-
cemets membrane detachment after intraocular
surgery. J Cataract Refract Surg. 1995;21:250-
253.
24. Donzis PB, Karcioglu AZ, Insler MS. Sodium hy-
aluronate (Healon) in the surgical repair of Des-
cemetsmembranedetachment.OphthalmicSurg.
1986;17:735-737.
25. MacsaiMS, GainerKM,ChisholmL. Repairof Des-
cemets membrane detachment with perfluoro-
propane (C3F8). Cornea. 1998;17:129-134.
ARCH OPHTHALMOL/ VOL 117, NOV 1999
WWW.ARCHOPHTHALMOL.COM1565
1999 American Medical Association. All rights reserved.on April
4, 2008www.archophthalmol.comDownloaded from
http://www.archophthalmol.com/http://www.archophthalmol.com/http://www.archophthalmol.com/http://www.archophthalmol.com/http://www.archophthalmol.com/