Embed Size (px)
Citation preview

www.europcronline.com/
Decision making for Pulmonary
Embolism
Michał Chyrchel MDUniversity Hospital , Krakow, Poland

Risk stratification according to expected PE –related early mortality rate
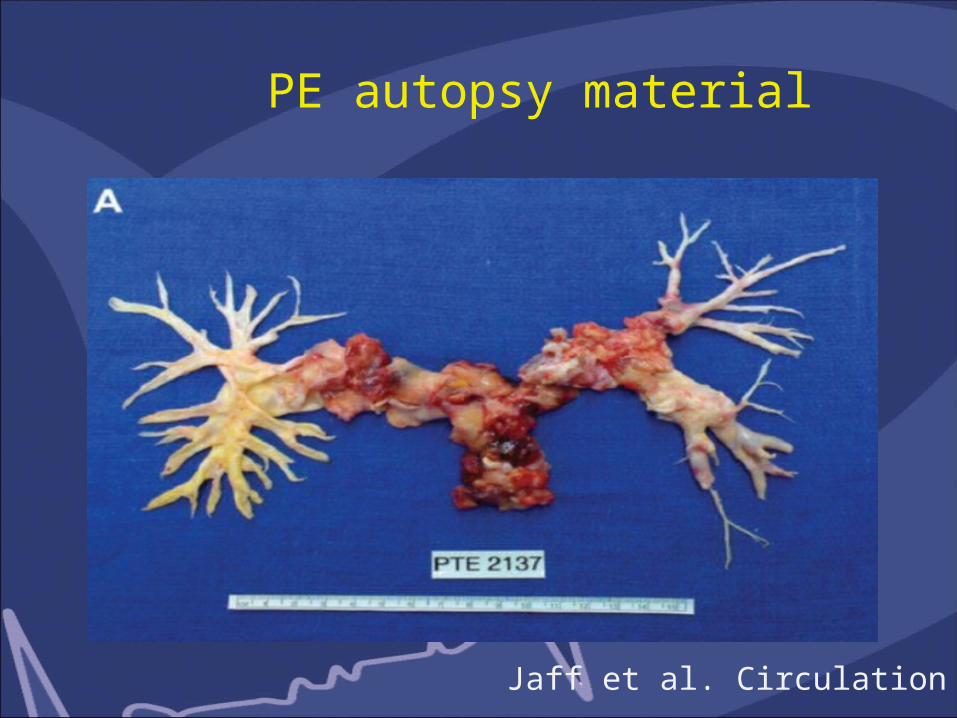
PE autopsy material
Jaff et al. Circulation 2011

PE treatment (including high risk PE)
• Respiratory and hemodynamic support
• Anticoagulation
• Trombolytic treatment
• Percutaneous intervention
• Surgical trombectomy

Anticoagulation
• Anticoagulation treatment plays a pivotal role in the management of patients with PE
• Initial anticoagulation should be introduce immediately • Potential options:
- UFH
- LMWH (dalteparin, enoxaparin, nodraparin)
- Fondaparynuks
- Riwaroksaban
- other

Anticoagulation options for Venous Thromboembolism
JAMA 2014;311(7): 717-728 Wells PS et al.

Anticoagulation
• In massive PE with hemodynamic consequences or a
shock - anticoagulation with UFH
• LMWH should be given in care in pts with renal failure
• Due to high mortality rate in untreated pts anticoagulation
should be considered when PE is strongly suspected:
awaiting for definite dgn confirmation
• Duration depends on many factors (PE etiology, transient
risk factors, cancer coexistence,etc.) BLEEDING RISK

Thrombolyitic regimens for PE• rtPA- standard: 100 mg i.v. (2 h)- fast regimen: 0,6 mg/kg (max. 50 mg) during 15 min• Streptokinase- fast regimen: 1,5 mln j.m. units i.v. (2h)- standard: 250 000 j.m. within 30 min, followed by 100 000
jm/h within 12-24 h • Urokinase- fast regimen: 3 mln j.m. i.v. within 2 h- standard: 4400 j.m./kg within 10 min, followed by 4400
j.m./h within 12-24 h
Specifity of lungs circulation
• Exquisitely sensitive to lysis
• Point of convergence of venous circulation
• Pulmonary blood flow = entire CO (Cardiac Output)
• In comparison: brain 15 % of CO, heart 5 % of CO
• Repeated „hits” of tPA by recirculation

Combined pharmacological approach
• Safe dose thrombolysis• Modified and short dose of heparin• New oral anticoagulants• 98 pts with moderate and severe PE• O mortality rate in hospital, bleeding 0 in hospital• Low adverse events in follow-up
Sharifi et al. Clin Card 10/2013

Other therapautic options for PE
• Surgical pulmonary embolectomy
• Percutaneous catheter embolectomy and fragmentation
- When contraindications for fibrynolytic therapy- Fibrynolytic therapy failed
! Only if: • applicable technical condition available • experienced interventional team
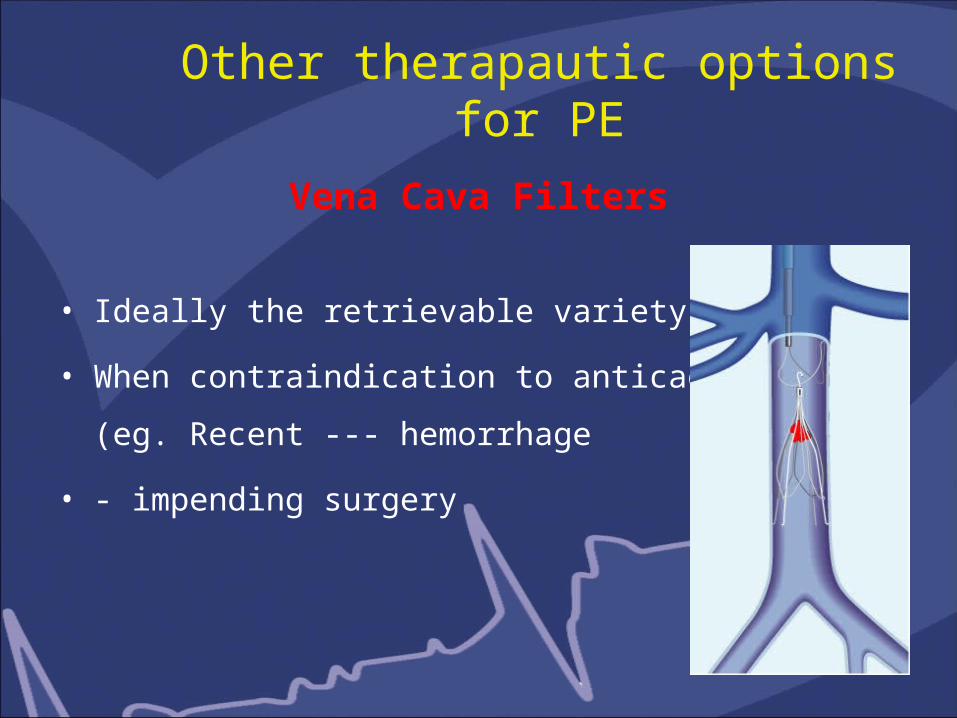
Other therapautic options for PE
Vena Cava Filters
• Ideally the retrievable variety of device
• When contraindication to anticaogaulation (eg. Recent
--- hemorrhage
• - impending surgery

Mortality spectrum in PE patients
W Kasper JACC 1997;30:1165-1171

Conclusions
• PE is common, potential live threatening condition
• In hospital mortality rate up to 12 % (US)
• Aggressive pharmacological - interventional treatment
is effective in majority of cases
• Farther diagnosis of possible PE causes is mandatory
(deep vein thrombosis, cancer, other)
• Is one of more frequent comorbiditie in patients
hospitalized from other reason.