Embed Size (px)
Citation preview

FEATURE ARTICLES
3 Introduction to this issue
Bonnie Marshall and Rebecca Crowder (APUA News Staff)
4 The cost of methicillin-resistant Staphylococcus aureus in pediatric neck and pharyngeal
infections
Michael E. McCormick, MD (Medical College of Wisconsin, Milwaukee, WI)
6 MIC creep
Ian M. Gould, MD (Aberdeen Royal Infirmary, Aberdeen, UK)
9 Swine livestock production as a risk factor for community-associated MRSA in
Pennsylvania
Joan A. Casey, MA and Brian S. Schwartz, MD, MS (Johns Hopkins Bloomberg School of Public Health, Baltimore, MD)
13 Diagnostics for invasive infection: Biomarkers and antibiotic utilization
Devandra N. Amin, MD, FCCM, FCCP (Morton Plant Hospital, Clearwater, Florida, Univ. of South Florida School of
Medicine) and Philipp P. Schuetz, MD, MPH (Univ. Hospital Basel, Basel Switzerland)
MRSA FIELD REPORTS & RELATED NEWS
17 Characterization of methicillin-resistant Staphylococcus aureus isolated in Bulgarian
hospitals, 2005-2011
Dimitar Nashev (National Center of Infectious and Parasitic Diseases, Sofia, Bulgaria)
20 Methicillin-resistant Staphylococcus aureus in Cuba
Gilda Toraño Peraza, PhD and Alexis Monzote López, MD (Pedro Kouri Institute, Havana, Cuba)
22 MRSA News
23 APUA Headquarters and Chapters in Action
24 Obituaries; Upcoming Events
25 APUA Leadership and Chapter Awards
26 Policy Updates
27 News and Publications of Note
NEWSLETTER PUBLISHED CONTINUOUSLY SINCE 1983 BY THE ALLIANCE FOR THE PRUDENT USE OF ANTIBIOTICS
December 2013
Volume 31, No. 3
Healthcare- and Community-Associated MRSA
Clumps of MRSA bacteria, magnified 2390x Source: CDC
Visit our website Support our work
2 • The APUA Newsletter Vol. 31. No. 3 • © 2013 APUA
Chief Executives Stuart B. Levy, President
Thomas F. O’Brien, Vice President
Board of Directors Stuart B. Levy, Chairman
Sherwood Gorbach
Gordon W. Grundy
Bonnie Marshall
Thomas F. O’Brien
Arnold G. Reinhold
Dennis Signorovitch
Philip D. Walson
Mary Wilson
APUA Staff Barbara Lapinskas, Administrative Director
Jane Kramer, Program Director
Kathleen Young, Projects Consultant
Stuart B. Levy, Newsletter Editor Bonnie Marshall, Associate Editor
Rebecca Crowder, Assistant Editor
Michelle Haan, Contributor
Advisory Board Jacques F. Acar, France
Werner Arber, Switzerland
Fernando Baquero, Spain
Michael l. Bennish, USA
Otto Cars, Sweden
Patrice Courvalin, France
Jose Ramiro Cruz, Guatemala
Julian Davies, Canada
Abdoulaye Djimde, Mali
Paul Farmer, Haiti
Walter Gilbert, USA
Herman Goossens, Belgium
Sherwood l. Gorbach, USA
Ian M. Gould, Scotland
George Jacoby, USA
Sam Kariuki, Kenya
Ellen L. Koenig, Dominican Republic
Advisory Board (cont.) Calvin M. Kunin, USA
Jacobo Kupersztoch, USA
Jay A. Levy, USA
Scott McEwen, Canada
Jos. W.M. van der Meer, The Netherlands
Richard P. Novick, USA
Iruka Okeke, USA & Nigeria
Maria Eugenia Pinto, Chile
Vidal Rodriguez-Lemoine, Venezuela
José Ignacio Santos, Mexico
Mervyn Shapiro, Israel
K. B. Sharma, India
Atef M. Shibl, Saudi Arabia
E. John Threlfall, United Kingdom
Alexander Tomasz, USA
Thelma e. Tupasi, Philippines
Anne K. Vidaver, USA
Fu Wang, China
Thomas E. Wellems, USA
Bernd Wiedemann, Germany
APUA Project Partnerships: The Bill and Melinda Gates Foundation
The Pew Charitable Trusts
U.S. National Institute of Health (NIH)
Pan American Health Organization
(PAHO)
U.S. Agency for International Develop-
ment (USAID)
U.S. Department of Agriculture
U.S. Office of Homeland Security
National Biodefense Analysis and Coun-
termeasures Center
The World Bank
World Health Organization (WHO)
Centers for Disease Control and Preven-
tion (CDC)
U.S. Food and Drug Administration
Ministries of Health
U.S. Defense Threat Reduction Agency
Supporting Chapters: APUA—Abu Dhabi
APUA—South Korea
Australian Society for Antimicrobials
(APUA-Australia)
British Society for Antimicrobial Chemo-
therapy (APUA-UK)
APUA gratefully acknowledges unrestrict-
ed grants from corporate sponsors:
Leadership Level ($20,000+) Clorox Healthcare
Bayer Healthcare Pharmaceuticals
Optimer Pharmaceuticals
Alere Inc.
bioMérieux
Partner Level ($10,000+) Alcon Laboratories
GlaxoSmithKline
Supporter Level ($2,500+) Cubist Pharmaceuticals
Disclaimer APUA accepts no legal responsibility for the content of any submitted articles, nor for the violation of any copyright laws by any person
contributing to this newsletter. The mention of specific companies or of certain manufacturers' products does not imply that they are endorsed
or recommended by APUA in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of
proprietary products are distinguished by initial capital letters.
The APUA Newsletter (ISSN 154-1424) © 2013 APUA Since 1983, the APUA Newsletter has been a continuous source of non-commercial information disseminated without charge to healthcare
practitioners, researchers, and policy-makers worldwide. The Newsletter carries up-to-date scientific and clinical information on prudent
antibiotic use, antibiotic access and effectiveness, and management of antibiotic resistance. The publication is translated into three languages and
distributed to over 7,000 affiliated individuals in more than 100 countries. The material provided by APUA is designed for educational purposes
only and should not be used or taken as medical advice. We encourage distribution with appropriate attribution to APUA. See previous editions
of the Newsletter on the APUA website.
*APUA welcomes letters to the Editor. Please send us your thoughts and questions. Names will be published but not
addresses. All letters may be edited for style and length.
Join the APUA corporate partnership
“Preserving the Power of Antibiotics”®
Phone: 617-636-0966 | Email: [email protected] | Website: www.apua.org

Introduction to this issue
Staphylococcus aureus has proved to be as an extremely
versatile pathogen—having emerged with penicillin resistance
in 1942, erythromycin, streptomycin and tetracyline resistances
in the 1950s, followed by resistance to methicillin in 1961. By
the early 2000s, it manifested as a multidrug-resistant super
pathogen exceeding 50% of all S. aureus in US intensive care
units, Latin America and the Asia-Pacific. The responsible
culprit was a mobile genomic element—the staphylococcal
cassette chromosome (SCC), carrying mecA and a PBP2a
transpeptidase gene with reduced affinity for beta-lactam
antibiotics.
The appearance of VISA (vancomycin-intermediate S. aureus)
in 1996 was also of growing concern and ultimately heralded
the onset of full-blown resistance to vancomycin—a drug of
last resort for multi-resistant staph. Currently still rare (13
cases of VRSA reported in the US since 2002), its occurrence
appears predisposed by chronic underlying
conditions such as skin ulcers and diabetes,
prior infections, colonization by MRSA or
Enterococcus and previous treatment with
vancomycin. Appearing some 40 years after
the advent of vancomycin, this resistance was
mediated by the vanA gene, acquired from
Enterococcus.
Concurrently, a new pandemic was spread-
ing outside the hospital, starting with the
appearance in the 1990’s of distinct strains
that caused purulent skin infections or
pneumonia within Australian youth having
no health-care contact. While generally
more susceptible to antibiotics, community-
associated S. aureus (CA-MRSA) commonly
carried the highly virulent Panton-Valentine
leukocidin gene (PVL gene). With their
considerable propensity for evolution, these
strains soon entered hospitals and began
causing invasive infections, thus blurring the
“community” distinction.
Currently MRSA clones are identified by
pulsed-field gel electrophoresis (PFGE)
patterns (e.g., USA 100), by multilocus
sequence typing and by spa typing, which
indicates variants of the polymorphic X
region of the protein A gene (spa). Five major pandemic clones
account for ~70% of hospital MRSA: Iberian, Brazilian,
Hungarian, New York/Japan (or USA100) and Pediatric. The
major MRSA clones are believed to have arisen from
successful epidemic methicillin-sensitive S. aureus (MSSA).
Strain USA 300, which spread rapidly across the US, is now
the predominant cause of skin and soft tissue infections in the
community setting. With the identification of a distinguishable
cluster of genes known as ACME (arginine catabolic mobile
element), it is now postulated that these genes were assembled
in the commensal skin bacterium Staphylococcus epidermidis
and only recently transferred horizontally into the ancestor of
the current USA 300 strain. The speG gene of this cluster
reportedly confers a set of multiple selective advantages over
other clones, including enhanced adhesion and biofilm
properties, resistance to antibiotics and also to polyamines,
by Bonnie Marshall and Rebecca Crowder (APUA staff)
Introduction • The APUA Newsletter Vol. 31. No. 3 • © 2013 APUA • 3
Introduction continued on Page 5
The Cost of Methicillin-resistant Staphylococcus aureus
in Pediatric Neck and Pharyngeal Infections
Michael E McCormick, MD
Assistant Professor, Division of Pediatric Otolaryngology, Medical College of Wisconsin and Children's
Hospital of Wisconsin
The incidence of methicillin-resistant Staphylococcus aureus
(MRSA), especially community-acquired-MRSA (CA-MRSA),
infections has been increasing over the last decade.1,2 Not
confined to adults, the troubling trend of increased MRSA in
the pediatric population is the focus of a great deal of research.3
While MRSA obviously presents treatment challenges with
regard to antimicrobial resistance, there exists another growing
problem associated with the rise of MRSA: the socioeconomic
implications. Studies have demonstrated an overall increase in
resource utilization associated with MRSA.4 Most of this
increased burden comes from longer hospital stays, inadequate
or delayed antibiotic use, and the use of newer, more expensive
antimicrobial agents needed to treat patients with MRSA
appropriately.
The overall increased incidence of
MRSA in children has been
paralleled by a rise in the incidence
of MRSA in head and neck
infections, including cellulitis and
deep neck abscesses.5-7 We re-
cently published our database
analysis of more than 3500 children
treated across the United States for
MRSA cervical infections.8 The average cost of each child’s
hospitalization was more than $20,000, and almost twenty
percent of children had hospitalization charges in excess of
$25,000. Most stayed in the hospital more than 4 days,
especially younger ones. Sixty percent of children required at
least one surgical procedure during their hospitalization, most
commonly incision and drainage of an abscess.
One of the keys to combating rising costs when fighting a
particular disease or illness is being able to identify patients
who may require additional resources to treat that disease.
There exists a known increase in the prevalence of MRSA in
non-white communities in the United States.9,10 It has been
proposed that this difference may be confounded by factors
such as socioeconomic status or the increased prevalence of
comorbid conditions in certain populations. For instance,
diabetes mellitus and HIV infection are more prevalent in
blacks in the United States. These illnesses are known to be
associated with compromise of the patient’s native immune
functions.
Issues with access to care have also been described for lower
socioeconomic groups, and it is plausible that this discrepancy
in access to care can explain the increased severity and
mortality associated with MRSA infections in some of these
populations. Our study found longer hospitalizations and an
increased need for surgical drainage in non-white children. In
addition, children from lower socioeconomic backgrounds also
required surgical drainage more frequently than other children.
We can potentially explain this finding
by suggesting that children from lower
socioeconomic groups who might have
issues with access to care are
presenting to the hospital with more
advanced MRSA infections. Therefore,
they are potentially undergoing surgical
drainage procedures at an earlier point
in their hospitalizations.
Healthcare in the United States will be
undergoing major changes in 2013 and 2014 (and beyond),
primarily as a result of the Affordable Care Act and budget
sequestration.11 More than ever, the “cost” of the care we
provide will be scrutinized and analyzed. The growing
incidence and associated cost of MRSA in today’s medical
environment will remain a microbiological and socioeconomic
challenge in both adult and pediatric medicine. Understanding
the socioeconomic aspects of a disease like MRSA can allow
researchers and healthcare providers to quickly identify and
treat patients infected with, carrying, or at risk for MRSA.
References
1. Johnigan RH, Pereira KD, Poole MD. Community-acquired
methicillin-resistant Staphylococcus aureus in children and
adolescents: changing trends. Archives of otolaryngology--head &
neck surgery. 2003;129(10):1049-52.
References Continued on Page 8
4 • The APUA Newsletter Vol. 31. No. 3 • © 2013 APUA • McCormick
“Most of this increased burden comes from longer hospital stays, inadequate or delayed antibiotic use, and the use of newer, more expensive antimicrobial agents needed to treat patients with MRSA appropriately.”

Introduction, continued from Page 3
which are native skin compounds that confer a natural tolerance
to other MRSA clones.
In the landscape of life-threatening “superbugs,” only MRSA
infection trends have demonstrated some reason for
encouragement: recent surveillance reports suggest an actual
decline in the national rate of invasive MRSA (31.2% between
2005-2011). For the first time, the incidence of invasive
hospital-onset MRSA has fallen below that among community
residents who lack significant health-care contact. In contrast,
community-associated MRSA (CA-MRSA) infections remain
stable or have declined only slightly (5%).
Nonetheless, MRSA remains a challenging pathogen and a
major cause of morbidity and mortality worldwide, with
significant economic consequences. In the US alone, >80,000
invasive MRSA infections still occur each year, the majority of
which have community or outpatient onset. In-hospital
mortality of MRSA bloodstream infections is ~30%, and in
some centers, as high as 65%, resulting in >11,000 deaths
annually.
This issue of the APUA Newsletter features several diverse
examinations of the S. aureus resistance problem. McCormick
presents a perspective on the escalating costs of community-
based infections localized to the head and neck. The article by
Gould looks at the phenomenon of “MIC creep” and the
problems it poses in treatment of MRSA with vancomycin—
one of few remaining drugs for the most resistant MRSA
strains. Casey and Schwartz examine the impacts of antibiotic
use in high-density livestock farming on the incidence of
MRSA infections in the farming community. The articles by
Nashev and by Peraza and Lopez present international
perspectives of the MRSA problem from Bulgaria and Cuba,
respectively. These studies examine more closely the specific
strains that are circulating in non-industrialized countries on
two different continents. Lastly, this issue takes an in-depth
look at the tracking of procalcitonin levels as a new diagnostic
tool for the recognition and management of bacterial sepsis.
Procalcitonin testing is one approach to addressing the nagging
problem of discerning between bacterial- and viral-mediated
illnesses. Reliable differentiation of these two is crucial to
antimicrobial stewardship decision-making and can be highly
instrumental in reducing the unnecessary use of antibiotics for
infections by viruses and other non-bacterial agents.
Sources
Stryjewski ME and Corey GR. ( 2014) Methicillin-resistant Staphylococcus
aureus: an evolving pathogen. Clin Infect Dis 58: (Supple1) S10-S18.
Dantes R, Mu Y, Belflower
R et al (2013) National
Burden of invasive meth-
icillin-resistant Staphylo-
coccus aureus infections,
United states, 2011. JAMA
Intern Med 173:1970-78.
Lowy D. (2013) Methicillin-
resistant Staphylococcus
aureus Where is it coming
from and where is it going?
JAMA Intern Med 173:1978
-9.
Planet PJ, LaRussa SJ, Dana
A et al. (2013) Emergence
of the epidemic methicillin-
resistant Staphylococcus
aureus strain US300 co-
incides with horizontal
transfer of the arginine
catabolic mobile element
and SpeG-mediated adapt-
ations for survival on skin.
mBio online. 4(6)
Introduction, cont. • The APUA Newsletter Vol. 31. No. 3 • © 2013 APUA • 5

MIC Creep
Ian M. Gould, MD
Department of Medical Microbiology, Aberdeen Royal Infirmary, Aberdeen, UK
The term “MIC creep” has come to be associated with the
complicated issues around the dose response to vancomycin
when used in the treatment of staphylococcal infection, most
usually due to methicillin-resistant Staphylococcus aureus.1
The MIC (minimum inhibitory concentration) is a standard
measurement for assessing bacterial susceptibility to an
antibiotic and indicates the likely clinical response if the
antibiotic is used to treat infection. While it is a well-
established measurement, the MIC has its limitations,
particularly in the limits of reproducibility. An additional
problem when considering vancomycin MIC creep is the
breakpoint (BP), which is currently 2mg/L vancomycin for
both CLSI and EUCAST.*
“Creep” has come to mean elevated MICs within the
breakpoint—so technically still susceptible. The question
arises: elevated from what? Here is the first difficulty, as there
is no clear evidence of what the vancomycin MIC should be for
a wild-type strain of staphylococcus—that is, one that has
never been exposed to vancomycin (or another glycopeptide).2
As vancomycin has been in use since 1955, it is not even
certain that such strains exist anywhere and so one must
assume that such a figure would be the lowest that is currently
measured in community isolates (with presumably only a small
potential for exposure to glycopeptides), which would be an
MIC of 0.25/0.5mg/L. Unfortunately, as the reproducibility of
standard doubling dilution MIC tests is + 1 dilution, it is
difficult to identify MIC creep with confidence. An MIC of 1
mg/L one day may be as low as 0.5mg/L on another day or as
high as 2mg/L i.e. exactly on the BP.3 With the understanding
that different, commonly used, MIC tests all have bias up or
down from the reference micro-dilution test, and that storage of
organisms (as often happens prior to testing in surveys) can
affect the MIC, one can see nothing but increasing confusion!4-
5 But it is important that we try to resolve these issues, as the
response of serious staphylococcal infections seems quite
critically dependent upon the MIC. Perhaps the problem is the
actual MIC, rather than MIC creep; however understanding
whether creep actually exists will help us understand the
dynamics of the organism’s response to antibiotics, the ways in
which resistance can develop and the likely future utility of
vancomycin.6 The latter is immediately important as that utility
seems to be balanced on a knife’s edge at the moment. With a
BP of 2mg/L and most series showing modal MICs of 1, 1.5 or
2mg/L, we can see immediately that there is little room for
maneuver. Indeed many experts now hold that it is already too
late for vancomycin as the BP should really be reclassified to
1.0 or 1.5mg/L, depending on the method used to measure the
MIC. I would certainly concur with this position for treatment
of life-threatening infection. The evidence here is uniformly
consistent and weighty that organisms with such an MIC
respond poorly to vancomycin (or teicoplanin). However, this
also may be partly explained by the other changes (e.g. in
autolysis, accessory gene regulation and biofilm formation)
that occur simultaneously in such organisms with an elevated
MIC.
6 • The APUA Newsletter Vol. 31. No. 3 • © 2013 APUA • Gould
Figure 1. E test MIC of S. aureus on Mueller Hinton
agar
The antibiotic test strips above are vancomycin (VA)
and teicoplanin (TP). The MIC is read from the gradient scale at the
point of complete inhibition of bacterial growth; thus the MIC
of VA is 1.5mg/L and TP is 1.0mg/L.
*CLSI: Clinical Laboratory Standards Institute (U.S); EUCAST:
European Committee of Antimicrobial Susceptibility Testing

Some authors have maintained that the observed elevated MICs
are actually a demonstration of MIC leap—i.e., a strain
change—but the evidence for this is weak. On the other hand
there is mounting evidence that creep is an ongoing process
over years of persistent vancomycin exposure in hospital
strains, and represents sequential acquisitions of multiple
mutations in several areas of cell wall manufacture that
ultimately lead to intermediate or full GISA status.7 Such
strains can accumulate up to 20 or 30 mutations through several
different pathways, which has prevented the development of
any single molecular detection tests so far. There is mounting
evidence that storage of such organisms, even just for a few
months, leads to either loss of expression of the mutations or
loss of the mutations themselves.4,5
So what can we do to clarify the situation and ensure the best
treatment for our patients? A few suggestions for further
research are included in Table 1. One interesting debate centers
on the quest for accuracy versus reproducibility or precision.
Traditionally, the latter has been the gold standard in
susceptibility testing, particularly in surveillance surveys of
MICs and resistance where isolates are often stored for up to
several years, before testing in a central laboratory under
strictly controlled conditions. With recent observations of MIC
regression following storage, a debate has arisen on whether
striving for reproducibility produces unacceptable loss of
accuracy and rather does not reflect the actual MIC at time of
isolation.8 This is, presumably, the MIC we strive to measure,
as it will best reflect what is happening in the patient and what
the likely clinical response will be to treatment. Unfortunately,
most studies of MIC creep poorly define whether and how
isolates are stored. This, we now understand, may well affect
the results obtained from such studies and have important
implications for many future surveillance studies, even for other
classes of antibiotics.4,5
In conclusion, much work is required before we achieve clarity
on these issues. In the meantime, I recommend use of the E test
gradient MIC measurement in serious staphylococcal infection
and a BP of 1mg/L for conventional dosing schedules and 1.5
mg/L for high-dose schedules. A loading dose of either
vancomycin or teicoplanin is also necessary to rapidly achieve
therapeutic levels, as well as trough serum monitoring for
teicoplanin. New agents such as daptomycin9-10 and linezolid
are costly, but these and other drugs will almost certainly
provide benefits to critically ill patients, providing they too are
dosed properly. Lastly, if it is not possible to measure an E test
MIC, then a risk factor analysis can be performed on the
patient.11
References
1. Gould IM. 2008. Clinical relevance of increasing glycopeptide MICs
against Staphylococcus aureus. Internat J Antimicrob Agents. 31
Suppl 2:1-9.
2. Gould IM, Cauda R, Esposito S et al. 2011 Management of serious
methicillin-resistant Staphylococcus aureus infections: what are the
limits? Internat J Antimicrob Agents 37(3):202-9.
3. Lawes T, Edwards B, Gould IM. 2013. Comment on: Lack of
upward creep of glycopeptide MICs for methicillin-resistant
Staphylococcus aureus (MRSA) isolated in the UK and Ireland 2001-
07. J Antimicrob Chemother 68(7):1691-2.
4. Ludwig F, Edwards B, Lawes T, et al. 2012. J Clin Microbiol.
Effects of storage on vancomycin and daptomycin MIC in susceptible
blood isolates of methicillin-resistant Staphylococcus aureus. J Clin
Microbiol Oct;50(10):3383-7.
5. Edwards B, Milne K, Lawes T et al. 2012. Is vancomycin
MIC “creep” method dependent? Analysis of methicillin-resistant
Staphylococcus aureus susceptibility trends in blood isolates from
North East Scotland from 2006 to 2010. J Clin Microbiol 50(2);318-
25.
6. Gould IM. 2010. International Journal of Antimicrobial Agents. Is
vancomycin redundant for serious staphylococcal infection? Internat J
Antimicrob Agents 36 (Suppl 2):S55-7.
MIC creep • The APUA Newsletter Vol. 31. No. 3 • © 2013 APUA • 7
Relationships between different MIC testing methods and
clinical outcome
Storage of organisms before testing versus testing at time
of isolation
Strain types versus MIC
Should the break point be reduced?
Can increased vancomycin dosing compensate for MIC
creep?
Do new antibiotics give better outcomes?; are they cost
effective?
Better define the PK/PD target for glycopeptides
MICs/resistance mechanisms versus different glycol/lipo
peptide
Does MIC creep occur with other antibiotic groups?
Better define mutations/expression/stability; develop
molecular tests
Compare E test with other gradient methods
Table 1. Research Issues in MIC Creep
7. Hafer C, Lin Y, Kornblum J et al. 2012. Contribution of selected
gene mutations to resistance in clinical isolates of vancomycin-
intermediate Staphylococcus aureus. Antimicrob Agents Chemother
56;11:5845-51.
8. Reynolds R, Hope R, Warner M et al. 2012. Lack of upward creep
of glycopeptide MICs for methicillin-resistant Staphylococcus aureus
(MRSA) isolated in the UK and Ireland 2001-07. J Antimicrob
Chemother 67 (12):2919-26.
9. Ammerlaan H, Seifert H, Harbarth S et al. 2009. Adequacy of
antimicrobial treatment and outcome of Staphylococcus aureus
bacteremia in 9 Western European countries. Clin Infect Dis 49
(7):997-1005.
10. Dong H, Wang X, Dong Y et al. 2011. Clinical pharmacokinetic/
pharmacodynamic profile of linezolid in severely ill Intensive Care
Unit patients. Internat J Antimicrob Agents.38:296-300.
11. Lubin AS, Snydman DR, Ruthazer R et al. 2011. Predicting high
vancomycin minimum inhibitory concentration in methicillin
resistant staphylococcus aureus bloodstream infections. Clin Infect
Dis 52 (8):997-1002.
McCormick references, continued from Page 4
2. Klevens RM, Morrison MA, Nadle J, et al. Invasive methicillin-
resistant Staphylococcus aureus infections in the United States.
JAMA. 2007;298(15):1763-71.
3. Brook I. The increased risk of community-acquired methicillin-
resistant Staphylococcus aureus in neck infections in young children.
Curr Infect Dis Rep. 2012;14(2):119-120.
4. Schorr AF LT. Burden of methicillin-resistant Staphylococcus aureus
8 • The APUA Newsletter Vol. 31. No. 3 • © 2013 APUA • Gould; McCormick cont.
on healthcare cost and resource utilization. ISMR Update. 2006;1(2).
5. Brook I. Role of methicillin-resistant Staphylococcus aureus in head
and neck infections. J Laryngol Otol. 2009;123(12):1301-7.
6. Naseri I, Jerris RC, Sobol SE. Nationwide trends in pediatric
Staphylococcus aureus head and neck infections. Otolaryngol Head
Neck Surg. 2009;135(1):14-16.
7. Thomason TS, Brenski A, McClay J, Ehmer D. The rising incidence
of methicillin-resistant Staphylococcus aureus in pediatric neck
abscesses. Otolaryngol Head Neck Surg. 2007;137(3):459-64.
8. McCormick ME, Chun RH, Lander L, Shah RK. Socioeconomic
implications of pediatric cervical methicillin-resistant
Staphylococcus aureus infections. JAMA Otolaryngol Head Neck
Surg. 2013;139(2):124-28.
9. Fridkin SK, Hageman JC, Morrison M, et al. Methicillin-resistant
Staphylococcus aureus disease in three communities. New Eng J
Med. 2005;352(14):1436-44.
10. Laupland KB, Church DL, Mucenski M, Sutherland LR, Davies HD.
Population-based study of the epidemiology of and the risk factors
for invasive Staphylococcus aureus infections. J Infect Dis.
2003;187(9):1452-59.
11. CCH Incorporated. Patient Protection and Affordable Care Act;
Health Care and Education Reconciliation Act of 2010 : text of P.L.
111-148, as signed by the President on March 23, 2010; text of P.L.
111-152, as signed by the President on March 30, 2010 : JCT
technical explanation of P.L. 111-148 and P.L. 111-152. Chicago,
IL: CCH; 2010.

Swine livestock production as a risk factor for
community-associated MRSA in Pennsylvania
Joan A. Casey, MA and Brian S. Schwartz, MD, MS
Johns Hopkins Bloomberg School of Public Health, Baltimore, MD
Over 80% of antibiotics in the United States are sold for use in
livestock feeds,1 most commonly in very large, industrial
operations with a high density of animals, but with insufficient
land acreage on which to spread, and thus dispose of, the
produced manure (Fig. 1). Because of this antibiotic use, the
manure produced at these operations contains antibiotics,
antibiotic-resistant bacteria, and resistance genes.2 This
manure, spread on crop fields, sometimes near human
dwellings, may put people at
risk for antibiotic-resistant
infections; however, no prior
studies have formally evaluated
this question.
Methicillin-resistant Staphylo-
coccus aureus (MRSA) colon-
ization was first linked to high-
density livestock operations in
studies from Europe.3-5 A
landmark 2005 study3 reported
that the pre-valence of MRSA
colonization in Dutch farmers
was 760 times that of the
general population. In Europe,
a strain of MRSA called
sequence type 398 (ST398) has been the most common
colonizer of swine and their owners.4,6 In the United States, the
incidence of community-associated MRSA (CA-MRSA)
infection appeared to increase throughout the early 2000s,
without good explanation or understanding of the drivers of the
epidemic.7,8 Genetics has proven useful to the epidemiologic
investigation of MRSA, and shown that nearly all CA-MRSA
in the US carries the Panton-Valentine leukocidin (PVL)
genes.9 We hypothesized that high-density livestock operations
could play a role in the CA-MRSA epidemic.
Methods
To evaluate this, we first used electronic health records (EHR)
from 2001 to 2010 from the Geisinger Health System (GHS) in
Pennsylvania to characterize MRSA infection in a large,
geographically diverse population with urban and rural areas
and many animal feeding operations. The EHR dataset
included over 150 million records on 450,000 patients. Incident
MRSA cases were identified using EHR data, classified as CA-
MRSA or healthcare-associated (HA-MRSA) and frequency-
matched to randomly selected controls and patients with skin
and soft tissue infection (SSTI) but without a history of MRSA.
We then estimated the incidence of CA-MRSA, HA-MRSA,
and SSTIs.
To assess high-density live-
stock production as a risk
factor for MRSA infection and
SSTIs, we conducted a nested
case-control study. Using
nutrient management plans,
two individual-level exposure
variables were created, based
on the distance between
patients’ home addresses and:
(1) the location and number of
animals (livestock model); and
(2) the location of crop fields,
their acreage, and the volume
of manure applied (crop field
model). We used multilevel logistic regression to assess the
association between exposure and case status, while adjusting
for potential confounding variables: age, sex, race/ethnicity,
smoking status, antibiotic order in the two years preceding
diagnosis, Medical Assistance for health insurance as a
surrogate for low family socioeconomic status, residential
community (city, borough, or township), and community-level
socioeconomic deprivation.
We also prospectively collected MRSA isolates from a
subsample of GHS patients with MRSA infections throughout
2012 and collaborated with New York University to
characterize them molecularly. Here, the goal was to identify
particular strains of MRSA infection associated with high-
density livestock production in Pennsylvania.
Swine livestock production as a risk factor • The APUA Newsletter Vol. 31. No. 3 • © 2013 • APUA • 9
Figure 1. A swine concentrated animal feeding
operation (CAFO)
Source: USDA.gov
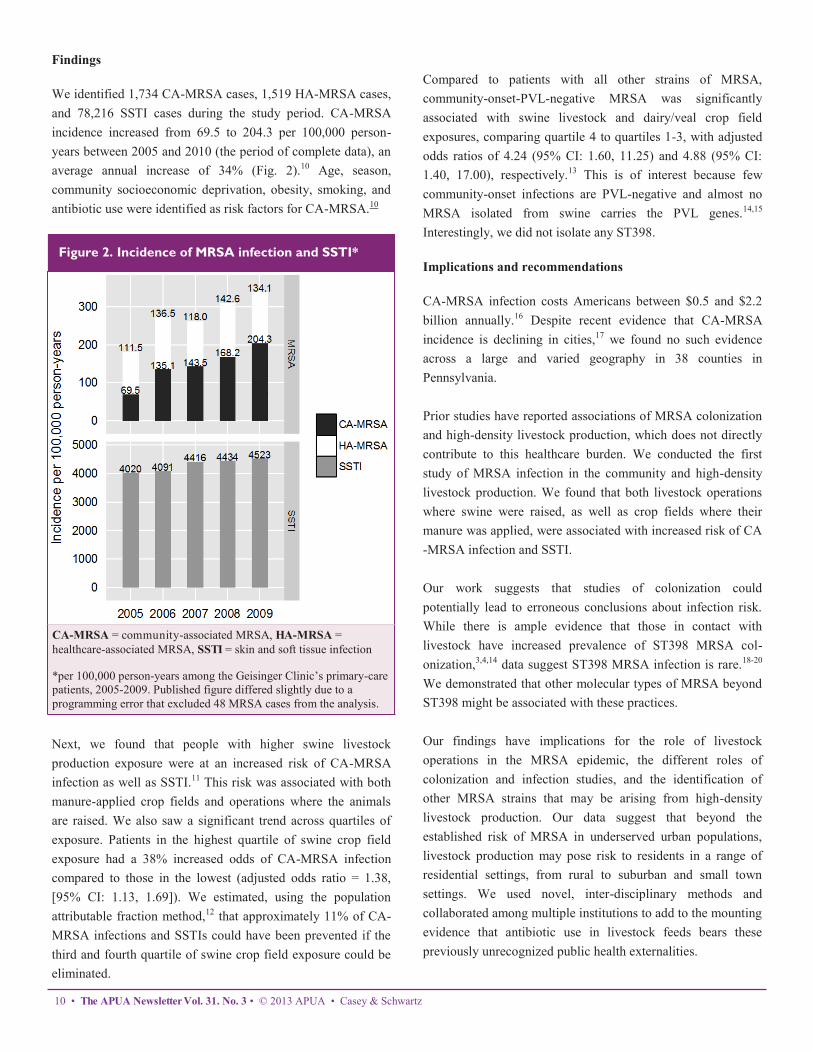
Findings
We identified 1,734 CA-MRSA cases, 1,519 HA-MRSA cases,
and 78,216 SSTI cases during the study period. CA-MRSA
incidence increased from 69.5 to 204.3 per 100,000 person-
years between 2005 and 2010 (the period of complete data), an
average annual increase of 34% (Fig. 2).10 Age, season,
community socioeconomic deprivation, obesity, smoking, and
antibiotic use were identified as risk factors for CA-MRSA.10
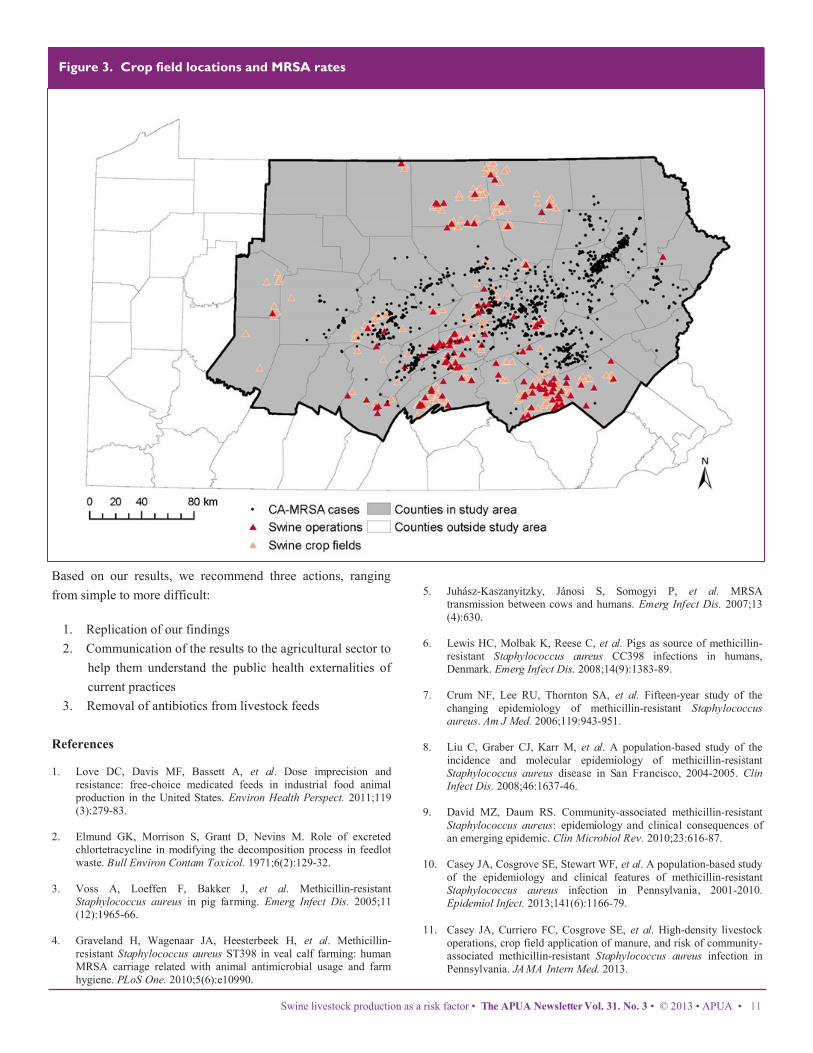
Next, we found that people with higher swine livestock
production exposure were at an increased risk of CA-MRSA
infection as well as SSTI.11 This risk was associated with both
manure-applied crop fields and operations where the animals
are raised. We also saw a significant trend across quartiles of
exposure. Patients in the highest quartile of swine crop field
exposure had a 38% increased odds of CA-MRSA infection
compared to those in the lowest (adjusted odds ratio = 1.38,
[95% CI: 1.13, 1.69]). We estimated, using the population
attributable fraction method,12 that approximately 11% of CA-
MRSA infections and SSTIs could have been prevented if the
third and fourth quartile of swine crop field exposure could be
eliminated.
Compared to patients with all other strains of MRSA,
community-onset-PVL-negative MRSA was significantly
associated with swine livestock and dairy/veal crop field
exposures, comparing quartile 4 to quartiles 1-3, with adjusted
odds ratios of 4.24 (95% CI: 1.60, 11.25) and 4.88 (95% CI:
1.40, 17.00), respectively.13 This is of interest because few
community-onset infections are PVL-negative and almost no
MRSA isolated from swine carries the PVL genes.14,15
Interestingly, we did not isolate any ST398.
Implications and recommendations
CA-MRSA infection costs Americans between $0.5 and $2.2
billion annually.16 Despite recent evidence that CA-MRSA
incidence is declining in cities,17 we found no such evidence
across a large and varied geography in 38 counties in
Pennsylvania.
Prior studies have reported associations of MRSA colonization
and high-density livestock production, which does not directly
contribute to this healthcare burden. We conducted the first
study of MRSA infection in the community and high-density
livestock production. We found that both livestock operations
where swine were raised, as well as crop fields where their
manure was applied, were associated with increased risk of CA
-MRSA infection and SSTI.
Our work suggests that studies of colonization could
potentially lead to erroneous conclusions about infection risk.
While there is ample evidence that those in contact with
livestock have increased prevalence of ST398 MRSA col-
onization,3,4,14 data suggest ST398 MRSA infection is rare.18-20
We demonstrated that other molecular types of MRSA beyond
ST398 might be associated with these practices.
Our findings have implications for the role of livestock
operations in the MRSA epidemic, the different roles of
colonization and infection studies, and the identification of
other MRSA strains that may be arising from high-density
livestock production. Our data suggest that beyond the
established risk of MRSA in underserved urban populations,
livestock production may pose risk to residents in a range of
residential settings, from rural to suburban and small town
settings. We used novel, inter-disciplinary methods and
collaborated among multiple institutions to add to the mounting
evidence that antibiotic use in livestock feeds bears these
previously unrecognized public health externalities.
10 • The APUA Newsletter Vol. 31. No. 3 • © 2013 APUA • Casey & Schwartz
Figure 2. Incidence of MRSA infection and SSTI*
CA-MRSA = community-associated MRSA, HA-MRSA =
healthcare-associated MRSA, SSTI = skin and soft tissue infection
*per 100,000 person-years among the Geisinger Clinic’s primary-care
patients, 2005-2009. Published figure differed slightly due to a
programming error that excluded 48 MRSA cases from the analysis.
Swine livestock production as a risk factor • The APUA Newsletter Vol. 31. No. 3 • © 2013 • APUA • 11
Based on our results, we recommend three actions, ranging
from simple to more difficult:
1. Replication of our findings
2. Communication of the results to the agricultural sector to
help them understand the public health externalities of
current practices
3. Removal of antibiotics from livestock feeds
References 1. Love DC, Davis MF, Bassett A, et al. Dose imprecision and
resistance: free-choice medicated feeds in industrial food animal
production in the United States. Environ Health Perspect. 2011;119
(3):279-83.
2. Elmund GK, Morrison S, Grant D, Nevins M. Role of excreted
chlortetracycline in modifying the decomposition process in feedlot
waste. Bull Environ Contam Toxicol. 1971;6(2):129-32.
3. Voss A, Loeffen F, Bakker J, et al. Methicillin-resistant
Staphylococcus aureus in pig farming. Emerg Infect Dis. 2005;11
(12):1965-66.
4. Graveland H, Wagenaar JA, Heesterbeek H, et al. Methicillin-
resistant Staphylococcus aureus ST398 in veal calf farming: human
MRSA carriage related with animal antimicrobial usage and farm
hygiene. PLoS One. 2010;5(6):e10990.
5. Juhász-Kaszanyitzky, Jánosi S, Somogyi P, et al. MRSA
transmission between cows and humans. Emerg Infect Dis. 2007;13
(4):630.
6. Lewis HC, Molbak K, Reese C, et al. Pigs as source of methicillin-
resistant Staphylococcus aureus CC398 infections in humans,
Denmark. Emerg Infect Dis. 2008;14(9):1383-89.
7. Crum NF, Lee RU, Thornton SA, et al. Fifteen-year study of the
changing epidemiology of methicillin-resistant Staphylococcus
aureus. Am J Med. 2006;119:943-951.
8. Liu C, Graber CJ, Karr M, et al. A population-based study of the
incidence and molecular epidemiology of methicillin-resistant
Staphylococcus aureus disease in San Francisco, 2004-2005. Clin
Infect Dis. 2008;46:1637-46.
9. David MZ, Daum RS. Community-associated methicillin-resistant
Staphylococcus aureus: epidemiology and clinical consequences of
an emerging epidemic. Clin Microbiol Rev. 2010;23:616-87.
10. Casey JA, Cosgrove SE, Stewart WF, et al. A population-based study
of the epidemiology and clinical features of methicillin-resistant
Staphylococcus aureus infection in Pennsylvania, 2001-2010.
Epidemiol Infect. 2013;141(6):1166-79.
11. Casey JA, Curriero FC, Cosgrove SE, et al. High-density livestock
operations, crop field application of manure, and risk of community-
associated methicillin-resistant Staphylococcus aureus infection in
Pennsylvania. JAMA Intern Med. 2013.
Figure 3. Crop field locations and MRSA rates

12 • The APUA Newsletter Vol. 31. No. 3 • © 2013 APUA • Casey & Schwartz
12. Rockhill B, Newman B, Weinberg C. Use and misuse of population
attributable fractions. Am J Public Health. 1998;88(1):15-19.
13. Casey JA, Shopsin B, Cosgrove SE, et al. Molecular characterization
of MRSA infection and association with high-density livestock
production in Pennsylvania (in press). Environ Health Perspect.
2013.
14. Smith TC, Male MJ, Harper AL, et al. Methicillin-resistant
Staphylococcus aureus (MRSA) strain ST398 is present in
midwestern U.S. swine and swine workers. PLoS One. 2009;4
(1):e4258.
15. Sunde M, Tharaldsen H, Marstein L, et al. Detection of methicillin-
resistant Staphylococcus aureus sequence type 8 in pigs, production
environment, and human beings. J Vet Diagn Invest. Mar 2011;23
(2):348-50.
16. Lee BY, Singh A, David MZ, et al. The economic burden of
community-associated methicillin-resistant Staphylococcus aureus
(CA-MRSA). Clin Microbiol Infect. 2013;19(6):528-36.
17. Dantes R, Mu Y, Belflower R, et al. National burden of invasive
methicillin-resistant Staphylococcus aureus infections, United States,
2011. JAMA Intern Med. 2013.
18. Golding GR, Bryden L, Levett PN, et al. Livestock-associated
methicillin-resistant Staphylococcus aureus sequence type 398 in
humans, Canada. Emerg Infect Dis. 2010;16(4):587-94.
19. Salmenlinna S, Lyytikainen O, Vainio A, et al. Human cases of
methicillin-resistant Staphylococcus aureus CC398, Finland. Emerg
Infect Dis. 2010;16(10):1626-29.
20. Wulf MW, Verduin CM, van Nes A, et al. Infection and colonization
with methicillin-resistant Staphylococcus aureus ST398 versus other
MRSA in an area with a high density of pig farms. Eur J Clin
Microbiol Infect Dis. 2012;31(1):61-65.
APUA’s Antibiotic Stewardship Webinar Series
Past webinar available for viewing:
Containing Healthcare Associated Infections Through
Antibiotic Stewardship
This webinar:
Describes trends of major HAIs including MRSA, ESBLs
and C. difficile Reviews the causes and mechanisms driving antibiotic
resistance problems Explains the link between antibiotic overuse and the
emergence of resistant infections Reviews effective ASP practices and the importance of
diagnostics in improving antibiotic treatment and
minimizing resistance Illustrates specific examples to enhance hospital-based
antimicrobial stewardship
Presenters:
Stuart Levy, MD and Shira Doron, MD, MS
Tufts University School of Medicine
VIEW HERE
Biomarkers and antibiotic
utilization
Procalcitonin and Antibiotic management
Respiratory tract infections (RTI) remain the most common
illness in humans, responsible for the most physician or
emergency room visits and the most frequent cause of sepsis.
While mortality is primarily associated with bacterial
pneumonia or severe influenza, most patients have a mild viral
illness.1 Interestingly, 75% of all antibiotic doses are prescribed
for acute RTI, the majority of which are viral and not bacterial
in etiology.2 Early differentiation between viral and bacterial,
as well as severity of infection, are key to managing acute RTI,
especially given evidence from studies that demonstrate that
early and appropriate antibiotic use improves survival.3
Concurrently, the need for prudent antibiotic utilization
avoiding overuse and prolonged use—is important for
minimizing antibiotic-related complications, including side
effects, drug interactions, development of resistance, and
secondary infection such as Clostridium difficile colitis. Initial
history, physical signs, imaging studies and current laboratory
data do not reliably differentiate viral from bacterial infection.4
Blood cultures have a low sensitivity, and sputum cultures, if
available, have a low specificity due to quality, contamination
and colonization issues.5
An innovative approach to assessing the likelihood and
severity of a bacterial infection is the use of blood biomarkers
that reflect the host response to infection. Although there are
many markers of an acute inflammatory response, only a few
have undergone rigorous, randomized clinical trials that
evaluate the clinical outcome associated with antibiotic
management strategies. Procalcitonin (PCT) has been
evaluated in numerous such studies and has been shown
to be more specific for bacterial infection than traditional
white cell count and C-reactive protein.5 In response to a
bacterial infection, PCT is released from multiple tissues
via direct stimulation of cytokines, including interleukin-
1β, interleukin-6, and tumor necrosis factor 1α (TNF1α).
The degree of up-regulation of PCT correlates with the
severity of bacterial infection.6-8 Conversely, interferon g
is the cytokine released in response to a viral infection.
This blocks up-regulation of PCT, resulting in a higher
specificity of PCT for bacterial infections.9,10
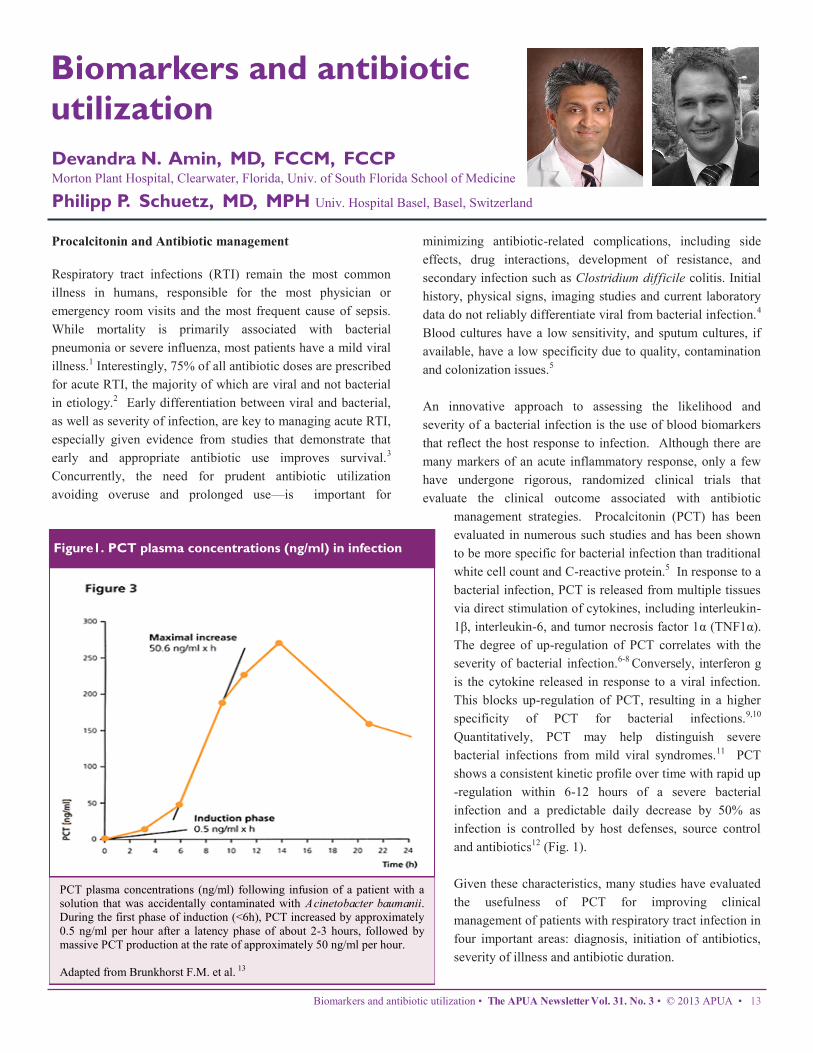
Quantitatively, PCT may help distinguish severe
bacterial infections from mild viral syndromes.11 PCT
shows a consistent kinetic profile over time with rapid up
-regulation within 6-12 hours of a severe bacterial
infection and a predictable daily decrease by 50% as
infection is controlled by host defenses, source control
and antibiotics12 (Fig. 1).
Given these characteristics, many studies have evaluated
the usefulness of PCT for improving clinical
management of patients with respiratory tract infection in
four important areas: diagnosis, initiation of antibiotics,
severity of illness and antibiotic duration.
Biomarkers and antibiotic utilization • The APUA Newsletter Vol. 31. No. 3 • © 2013 APUA • 13
Devandra N. Amin, MD, FCCM, FCCP Morton Plant Hospital, Clearwater, Florida, Univ. of South Florida School of Medicine
Philipp P. Schuetz, MD, MPH Univ. Hospital Basel, Basel, Switzerland
Figure1. PCT plasma concentrations (ng/ml) in infection
PCT plasma concentrations (ng/ml) following infusion of a patient with a
solution that was accidentally contaminated with Acinetobacter baumanii.
During the first phase of induction (<6h), PCT increased by approximately
0.5 ng/ml per hour after a latency phase of about 2-3 hours, followed by
massive PCT production at the rate of approximately 50 ng/ml per hour.
Adapted from Brunkhorst F.M. et al. 13

PCT for diagnosis of significant bacterial respiratory tract
infection
Numerous studies have investigated the PCT for initial
diagnosis of a bacterial infection and differentiation from viral
infection. In one study of 925 patients with community-
acquired pneumonia (CAP), 7.9% of patients were bacteremic.
PCT was significantly increased in bacteremic patients
compared to non-bacteremic patients. Less than 1% of patients
had a positive blood culture if the initial PCT level was
<0.25mg/L, which increased to greater than 20% in patients
with initial PCT >2.5mg/L.5 Another study investigated 103
patients with confirmed influenza A (H1N1). PCT had an area
under the curve (AUC) of 0.90, differentiating the 48 patients
with bacterial super-infection from patients with viral
pneumonia only (PCT cut off of 0.8 mg/L). The negative
predictive value was 91% for excluding bacterial co-infection.11
Prognostic value for prediction of adverse outcomes
Clinical risk scores, such as APACHE or SAPS II, are
somewhat limited in assessing disease severity and these scores
are only validated when admission values are available.14,15
Indeed, the utility of monitoring these scores over the course of
sepsis is not well-established. Thus, there is interest in
predictive use of biomarkers that: 1) are objectively and rapidly
measurable; 2) respond to clinical recovery and 3) add relevant,
reliable, real-time information.16 A recent derivation-validation
cohort study using retrospective data from two independent
U.S. critical care institutions found a high prognostic value
when considering the 72-hour PCT kinetic for sepsis
mortality.17 A PCT decrease of >80% over 72 hours had a
negative predictive value of 90% (and 91% to exclude ICU
mortality) which may aid in identifying individuals at reduced
risk—thus good early ICU discharge candidates. Conversely,
no decrease, or an increased PCT, had a positive predictive
value of 35-50%, helping to flag patients who were at high
mortality risk and likely to require treatment escalation.
PCT and antibiotic management
To date, a total of 14 randomized controlled trials with over
4,000 patients have assessed the efficacy and safety of using
PCT for antibiotic initiation, duration and cessation in a range
of respiratory illnesses—including acute exacerbation of
COPD, bronchitis, asthma, community acquired pneumonia,
sepsis, ventilator associated pneumonia and postoperative
pneumonia. All studies used somewhat similar protocols,
which recommended initiation or discontinuation of antibiotics
based on PCT levels. Several cutoff ranges were used reflecting
the increase in likelihood of bacterial infection with higher PCT
levels. Cutoff levels were adapted to the clinical setting or
acuity of the patient.18
In low-acuity settings (primary care) and low-acuity conditions
(bronchitis), PCT levels were used to withhold or prescribe
antibiotics. In higher acuity patients with more severe findings
(patients with pneumonia requiring hospitalization and ICU
patients with sepsis), PCT was used not for initiation of
antibiotics, but rather for discontinuation when a predetermined
drop in PCT levels was achieved with concordant clinical
improvement.
In all 14 studies this strategy proved to be highly effective in
reducing antibiotic exposure. In patients with a lower risk of
recurrent infection, PCT guidance reduced antibiotic
prescription rates by 40-75% in primary care patients with
upper and lower respiratory symptoms; by 60-75% in patients
with bronchitis; and by 30-45% in patients with an acute
exacerbation of COPD. In higher acuity patients with
community-acquired pneumonia, PCT guidance reduced
antibiotic duration by 35-55% and by about 35% in patients
with ventilator-associated pneumonia. Crucially, there was no
increase in mortality or other adverse events during the course
of the various studies.18 In addition, a prospective real-life
multicenter, multinational evaluation of a PCT guidance
algorithm study also found significant reduction in antibiotic
usage, without increase in adverse outcomes.19
Utilization of PCT in the antibiotic management of patients
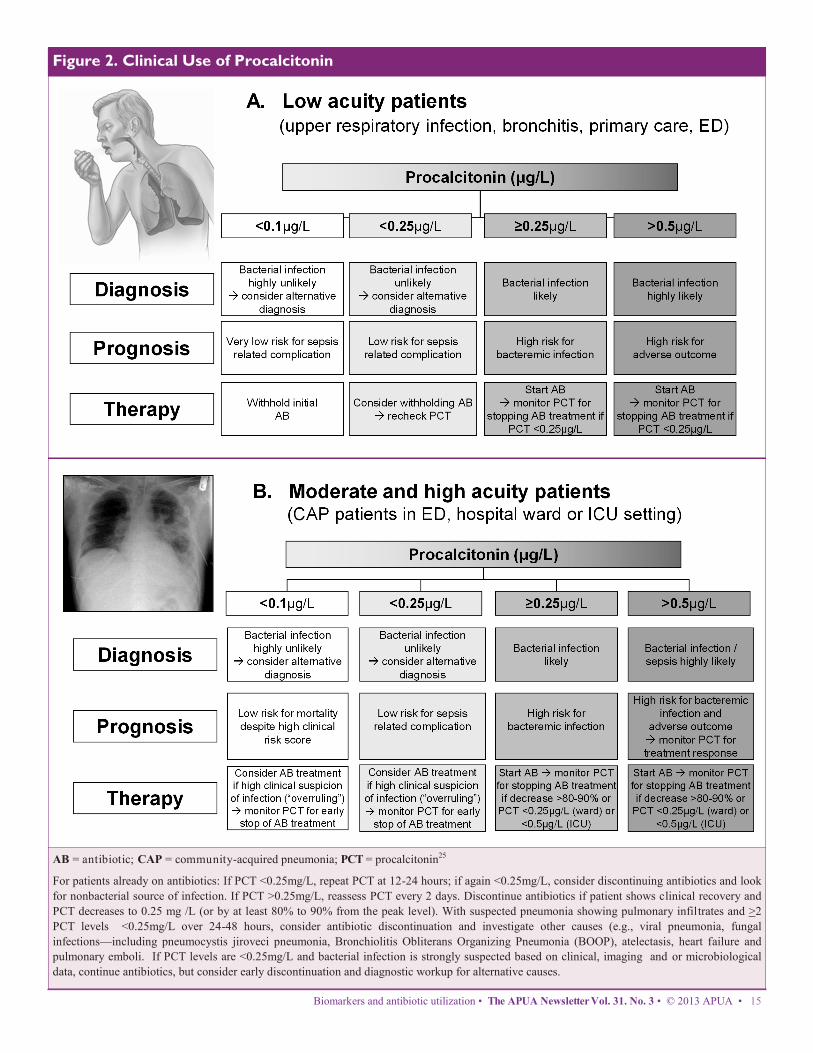
with respiratory infection
Algorithms for the diagnosis, prognosis and therapy of both
low-acuity and high-acuity patients are presented in Figure 2.
In general, for the low-acuity patient with a PCT <0.25mg/L,
antibiotics can be withheld—or withdrawn, if the PCT remains
stable (Fig. 2A). For high-risk patients with severe respiratory
infection, empiric antibiotic therapy should not be delayed,
even with a low initial PCT (0.25mg/L). The progression and
response to effective treatment of severe infection is dynamic,
and serial PCT measurements at 0, 12, 24 and 48 hours help
with assessing severity of infection. PCT usually peaks within
12-48 hrs.—as the patient responds to treatment, the levels
drop by 50% per day. Catching the peak level is important for 3
reasons:
1. Prognostication—the higher the peak level, the higher the
morbidity;
2. Treatment duration can be optimized (see Fig. 2B therapy);
3. Failure to drop by 50% every 1-2 days suggests treatment
failure. Reassessment of infection source and treatment are
strongly recommended. 19
14 • The APUA Newsletter Vol. 31. No. 3 • © 2013 APUA • Amin & Schuetz
Biomarkers and antibiotic utilization • The APUA Newsletter Vol. 31. No. 3 • © 2013 APUA • 15
AB = antibiotic; CAP = community-acquired pneumonia; PCT = procalcitonin25
For patients already on antibiotics: If PCT <0.25mg/L, repeat PCT at 12-24 hours; if again <0.25mg/L, consider discontinuing antibiotics and look
for nonbacterial source of infection. If PCT >0.25mg/L, reassess PCT every 2 days. Discontinue antibiotics if patient shows clinical recovery and
PCT decreases to 0.25 mg /L (or by at least 80% to 90% from the peak level). With suspected pneumonia showing pulmonary infiltrates and >2
PCT levels <0.25mg/L over 24-48 hours, consider antibiotic discontinuation and investigate other causes (e.g., viral pneumonia, fungal
infections—including pneumocystis jiroveci pneumonia, Bronchiolitis Obliterans Organizing Pneumonia (BOOP), atelectasis, heart failure and
pulmonary emboli. If PCT levels are <0.25mg/L and bacterial infection is strongly suspected based on clinical, imaging and or microbiological
data, continue antibiotics, but consider early discontinuation and diagnostic workup for alternative causes.
Figure 2. Clinical Use of Procalcitonin
9. Christ-Crain M, Müller B. Biomarkers in respiratory tract infections:
diagnostic guides to antibiotic prescription, prognostic markers and
mediators. Eur Respir J . 2007; 30(3): 556-573.
10. Linscheid P, Seboek D, Zulewski H , et al. Autocrine/paracrine role of
inflammation-mediated calcitonin gene-related peptide and
adrenomedullin expression in human adipose tissue. Endocrinology.
2005; 146(6): 2699-2708.
11. Cuquemelle E, Soulis F, Villers D, et al. A/H1N1 REVASRLF Study
Group. Can procalcitonin help identify associated bacterial infection in
patients with severe influenza pneumonia? A multicentre study.
Intensive Care Med. 2011; 37 (5): 796-800.
12. Becker KL , Nylén ES , White JC , et al . Clinical review 167:
Procalcitonin and the calcitonin gene family of peptides in
inflammation, infection, and sepsis: a journey from calcitonin back to
its precursors. J Clin Endocrinol Metab. 2004; 89 (4): 1512-25.
13. Brunkhorst FM, Heinz U, Forycki F. et al., Kinetics of procalcitonin in
iatrogenic sepsis. Intensive Care Med 1998, 24: 888-89.
14. Dellinger RP, Carlet JM, Masur H, Gerlach H, Calandra T, Cohen J, et
al. Surviving Sepsis Campaign guidelines for management of severe
sepsis and septic shock. Critical care medicine. 2004;32(3):858-73.
15. Dellinger RP, Levy MM, Carlet JM, et al. Surviving Sepsis Campaign:
international guidelines for management of severe sepsis and septic
shock: 2008. Critical care medicine. 2008; 36(1):296-327.
16. Schuetz P, Wolbers M, Christ-Crain M, et al. Prohormones for
prediction of adverse medical outcome in community-acquired
pneumonia and lower respiratory tract infections. Crit Care. 2010;14
(3):R106.
17. Schuetz P, Maurer P, Punjabi V, et al. Procalcitonin decrease over 72
hours in US critical care units predicts fatal outcome in sepsis patients.
Crit Care. 2013;17(3):R115.
18. Schuetz P , Chiappa V, Briel M , Greenwald JL . Procalcitonin
algorithms for antibiotic therapy decisions: a systematic review of
randomized controlled trials and recommendations for clinical
algorithms. Arch Intern Med. 2011; 171 (15): 1322-31
19. Schuetz P, Amin DN, Greenwald JL. Role of procalcitonin in
managing adult patients with Respiratory Tract Infections. Chest
2012;141(4):1063-73.
20. Sponholz C, Sakr Y, Reinhart K , Brunkhorst F. Diagnostic value and
prognostic implications of serum procalcitonin after cardiac surgery: a
systematic review of the literature. Crit Care. 2006; 10 (5): R145.
21. Schuetz P, Affolter B, Hunziker S, et al . Serum procalcitonin, C-
reactive protein and white blood cell levels following hypothermia
after cardiac arrest: a retrospective cohort study. Eur J Clin Invest.
2010; 40 (4): 376-81.
In patients suspected of respiratory infection complicating
major surgery, trauma or cardiogenic shock, PCT levels may
reflect the underlying cytokine response to major tissue injury,
and not necessarily reflect an infectious process alone. Serial
procalcitonin levels may be suggestive of infection when a
secondary elevation is seen if the underlying condition is stable
or improving.20,21
These recommendations and guidelines are valid only with
highly sensitive PCT assays and should not be applied to
patient populations that have not been studied, e.g., immune-
compromised patients, neonates and pregnant females.
Importantly, no diagnostic test should be used in isolation, out
of clinical context, for decision-making. PCT does not replace
good clinical evaluation and judgment. The correct
understanding of PCT levels is predicated on the physician’s
pretest probability for the test. Given the appropriate clinical
situation, the addition of the highly sensitive PCT biomarker
appears to help in the diagnosis of upper and lower respiratory
tract bacterial infection and more importantly, aids in guiding
antibiotic duration, based on its strong negative predictive
value.
References
1. Macfarlane JT , Colville A, Guion A, Macfarlane RM, Rose DH.
Prospective study of etiology and outcome of adult lower-respiratory-
tract infections in the community. Lancet. 1993; 341 (8844): 511-14.
2. Carlet J. Rapid diagnostic methods in the detection of sepsis. Infect Dis
Clin North Am. 1999; 13 (2): 483-94.
3. Kumar A, Roberts D, Wood KE, et al . Duration of hypotension before
initiation of effective antimicrobial therapy is the critical determinant
of survival in human septic shock. Crit Care Med. 2006; 34 (6): 1589-
96
4. Müller B, Harbarth S, Stolz D, et al. Diagnostic and prognostic
accuracy of clinical and laboratory parameters in community-acquired
pneumonia. BMC Infect Dis. 2007; 7: 1.
5. Müller F, Christ-Crain M, Bregenzer T, et al ProHOSP Study Group .
Procalcitonin levels predict bacteremia in patients with community-
acquired pneumonia: a prospective cohort trial. Chest 2010; 138 (1):
121-29.
6. Schuetz P, Christ-Crain M, Albrich W, et al. ProHOSP Study Group.
Guidance of antibiotic therapy with procalcitonin in lower respiratory
tract infections: insights into the ProHOSP study. Virulence. 2010;1
(2):88-92.
7. Christ-Crain M, Stolz D, Bingisser R , et al. Procalcitonin guidance of
antibiotic therapy in community-acquired pneumonia: a randomized
trial. A m J Respir Crit Care Med. 2006; 174 (1): 84-93.
8. Gogos CA, Drosou E, Bassaris HP, Skoutelis A. Pro- versus anti-
inflammatory cytokine profile in patients with severe sepsis: a marker
for prognosis and future therapeutic options. J Infect Dis. 2000; 181
(1): 176-80.
16 • The APUA Newsletter Vol. 31. No. 3 • © 2013 APUA • Amin & Schuetz

distribution. These two spa types comprised the majority
(43.2%) of MRSA isolates in the present study. This lineage
has been reported in many European countries, including those
neighboring to Bulgaria. ST239 is widely distributed in Greece
and is the predominant endemic clone in the University
hospital in Patras.5 Spa type t030 has been described as the
prevalent MRSA spa type in Turkey6 and Romania.1 Therefore,
the prevalence of ST239 related spa types in Bulgaria is not
surprising. The majority of Bulgarian t030/t037 MRSA strains
reflected the ST239 multi-resistance pattern (Table 1).
Spa types t010 and t002, (SCCmec IV and negative for PVL-
genes) were frequently associated with ST5-IV, known as
Pediatric clone (http://spa.ridom.de/mlst.shtml). According to
spa-server, t010 was detected in Austria, Belgium, Czech
Republic, Denmark, France, Germany, Island, Ireland,
Netherlands, Poland, Spain, Sweden, Switzerland and UK, but
not reported in Bulgaria’s neighbors, Greece, Turkey and
Romania (http://spa.ridom.de/frequencies.shtml). In the present
study, most of the ST5-IV related isolates were resistant only to
beta-lactams. Sporadic t010 isolates showed resistance to
kanamycin, gentamicin or tetracycline.
As reported previously, spa type t300 and t1143 were
associated with ST30.7,8 PVL-positive ST30-IV is an important
pandemic community-associated clone known as Southwest
Pacific Clone, USA1100 or West Samoan Phage Pattern
(WSPP) clone. Interestingly, in the present study, t1143
isolates were found to be hospital-associated. However, CA-
MRSA has been increasingly associated with nosocomial
infections with various reports of CA-MRSA isolation in
European hospitals.9,10
As shown above, ST239 associated spa-types t030/t037 and
ST30 related t1143 and t300 were clustered together in spa CC
1143. The wrong clustering of spa types of ST239 with those
found in CC30 has been reported previously and could be
explained by recombinative replacement of a large stretch of
Characterization of methicillin-resistant Staphylococcus
aureus isolated in Bulgarian hospitals, 2005-2011
Dimitar Nashev, MD, PhD
Staphylococcal Reference Lab at the National Center for Infectious and Parasitic Diseases, Sofia, Bulgaria
In collaboration with: L. Bizeva1, D. Merdzhanov1, E. Keuleyan2, T. Kantardjiev1 1Microbiology Dept., National Center of Infectious and Parasitic Diseases, Sofia, Bulgaria 2Microbiology Dept., Medical Institute of Ministry of Interior, Sofia, Bulgaria
Reports documenting the clonal spread of MRSA in Bulgaria
are still limited in number and focused mainly on single
hospital outbreaks, isolates collected in a short period of time
or sporadic cases of community-associated MRSA infections.1,2
We aimed to define the most prevalent spa types of MRSA
found in Bulgarian hospitals in the period 2005-2011 and to
associate them with the corresponding sequence types (ST),
SCCmec type, PVL (Panton-Valentine leukocidin) production
and phenotype of antibiotic resistance.
A total of 293 MRSA isolated between 2005 and 2011 from 31
hospitals in 20 cities were studied. The isolates were grouped
according to their antibiotic resistance phenotypes and 104
representative isolates were selected for further genotyping,
including spa sequence typing, SCCmec typing3 and PCR
detection of the genes encoding PVL.4 The existing sequence
database for spa types (http://spa.ridom.de) and literature data
were used to associate spa types with a particular MLST
sequence type (ST).
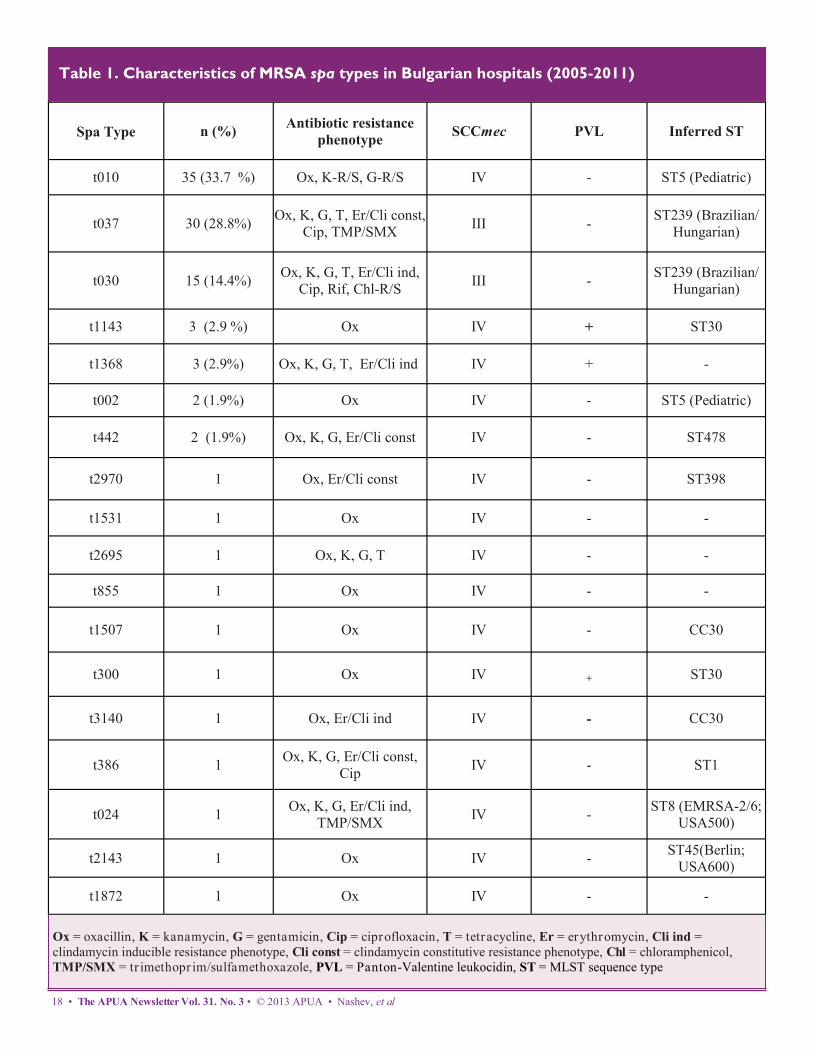
Among 18 spa types defined, the most prevalent was t010
(33.7%), followed by t037 (28.8%), t030 (14.4%), t1143 and
t1368 (2.9%). The remaining spa types were sporadically
isolated. The isolates belonging to spa types t030 and t037
possessed SCCmec type III, whereas all other isolates were
found to carry SCCmec type IV. Only isolates with spa types
t1143, t300 and t1368 were positive for PVL genes. (Table 1)
Using the BURP (Based Upon Repeat Pattern) algorithm
integrated in Staphtype software v.2.2.1, two spa-clusters were
defined: spa–clonal complex (CC) 1143 (t030, t037, t300,
t1143, t1507, t3140) and spa CC 010 (t002, t010, t442, t855,
t2695) (Table 1). Eight isolates were defined as singletons
(t024, t056, t731, t1368, t1531, t1872, t2143, t2970) and one
spa type was excluded (t386).
Spa types t030 and t037 are associated with ST239, a
pandemic MRSA lineage characterized by worldwide
Field report—Bulgaria • The APUA Newsletter Vol. 31. No. 3 • © 2013 APUA • 17
18 • The APUA Newsletter Vol. 31. No. 3 • © 2013 APUA • Nashev, et al
Table 1. Characteristics of MRSA spa types in Bulgarian hospitals (2005-2011)
Spa Type n (%) Antibiotic resistance
phenotype SCCmec PVL Inferred ST
t010 35 (33.7 %) Ox, K-R/S, G-R/S IV - ST5 (Pediatric)
t037 30 (28.8%) Ox, K, G, T, Er/Cli const,
Cip, TMP/SMX III -
ST239 (Brazilian/
Hungarian)
t030 15 (14.4%) Ox, K, G, T, Er/Cli ind,
Cip, Rif, Chl-R/S III -
ST239 (Brazilian/
Hungarian)
t1143 3 (2.9 %) Oх IV + ST30
t1368 3 (2.9%) Ox, K, G, T, Er/Cli ind IV + -
t002 2 (1.9%) Ox IV - ST5 (Pediatric)
t442 2 (1.9%) Ox, K, G, Er/Cli const IV - ST478
t2970 1 Ox, Er/Cli const IV - ST398
t1531 1 Ox IV - -
t2695 1 Ox, K, G, T IV - -
t855 1 Ox IV - -
t1507 1 Ox IV - CC30
t300 1 Ox IV + ST30
t3140 1 Ox, Er/Cli ind IV - CC30
t386 1 Ox, K, G, Er/Cli const,
Cip IV - ST1
t024 1 Ox, K, G, Er/Cli ind,
TMP/SMX IV -
ST8 (EMRSA-2/6;
USA500)
t2143 1 Ox IV - ST45(Berlin;
USA600)
t1872 1 Ox IV - -
Ox = oxacillin, K = kanamycin, G = gentamicin, Cip = ciprofloxacin, T = tetracycline, Er = erythromycin, Cli ind =
clindamycin inducible resistance phenotype, Cli const = clindamycin constitutive resistance phenotype, Chl = chloramphenicol,
TMP/SMX = tr imethopr im/sulfamethoxazole, PVL = Panton-Valentine leukocidin, ST = MLST sequence type
chromosomal DNA in MRSA isolates of CC8 by a stretch
originating from CC30 and including the spa gene.11
The PVL-negative spa types t3140 and t1507 were also
grouped in the spa CC-1143 clonal complex. Data on their
corresponding ST were not found in the spa-server, but
according to BURP-clustering they could probably belong to
CC30.
A PVL-positive spa type, t1368, defined as singleton by BURP,
was detected in three isolates (Table 1). We have not found data
on the ST association of this spa-type on the spa server or in the
literature, but the closely related spa-type t9381 was associated
with CC8; ST-72. However, for the exact ST identification,
MLST analysis should be performed.
Along with the prevalent spa types and their relatives, several
minor spa types, classified by BURP as singletons were found.
Their characteristics and ST association are shown in Table 1.
In conclusion, spa types associated with ST239 and ST5-IV
clones were largely predominant among MRSA isolates in 20
Bulgarian hospitals. Sporadic strains belonging to different
MRSA lineages, including PVL-positive CA-MRSA showed
potential for further spread of new clones in Bulgaria, although
in relatively small proportions.
References
1. Grundmann, H., et al., Geographic distribution of Staphylococcus
aureus causing invasive infections in Europe: a molecular-
epidemiological analysis. PLOS Med, 2010. 7(1): e1000215.
2. Nashev, D., L. Bizeva, and K. Toshkova, First cases of infections
caused by Panton-Valentine leukocidin positive community-acquired
methicillin-resistant Staphylococcus aureus in Bulgaria. Euro
Surveill, 2007. 12: 26.
3. Oliveira, D.C. and H. de Lencastre, Multiplex PCR strategy for rapid
identification of structural types and variants of the mec element in
methicillin-resistant Staphylococcus aureus. Antimicrob Agents
Chemother, 2002. 46(7): 2155-2161.
4. Lina, G., et al., Involvement of Panton-Valentine leukocidin—
producing Staphylococcus aureus in primary skin infections and
pneumonia. Clin Infect Dis, 1999. 29(5): 1128-1132.
5. de Sousa, M.A., et al., Two international methicillin-resistant
Staphylococcus aureus clones endemic in a university hospital in
Patras, Greece. J Clin Microb, 2003. 41(5): 2027-32.
6. Alp, E., et al., MRSA genotypes in Turkey: persistence over 10 years
of a single clone of ST239. J Infect, 2009. 58(6): 433.
7. Monecke, S., et al., A field guide to pandemic, epidemic and sporadic
clones of methicillin-resistant Staphylococcus aureus. PLoS One,
2011. 6(4): e17936.
8. Ionescu, R., et al., Molecular characterization and antibiotic
susceptibility of Staphylococcus aureus from a multidisciplinary
hospital in Romania. Microb Drug Resist, 2010. 16(4): 263-72.
9. Otter, J. and G. French, The emergence of community-associated
methicillin-resistant Staphylococcus aureus at a London teaching
hospital, 2000–2006. Clin Microb and Infect, 2008. 14(7): 670-76.
10. Köck, R., et al., The epidemiology of methicillin-resistant
Staphylococcus aureus (MRSA) in Germany. Deutsches Ärzteblatt
International, 2011. 108(45): 761.
11. Strommenger, B., et al., Assignment of Staphylococcus isolates to
groups by spa typing, SmaI macrorestriction analysis, and multilocus
sequence typing. J Clin Microb, 2006. 44(7): 2533-40.
Field report—Bulgaria • The APUA Newsletter Vol. 31. No. 3 • © 2013 APUA • 19
APUA’s Antibiotic Stewardship
Webinar Series
Past webinar available for viewing:
The Clinical Impact of Antimicrobial Stewardship and
Rapid Diagnostic Tests: From Bench to Bedside PACE® credit available until June 11, 2014
This webinar:
Reviews trends in antimicrobial resistance and C. difficile
infections Discusses strategies for implementing antimicrobial
stewardship in acute care hospitals Analyzes various ways in which rapid diagnostics
information can be brought from bench to bedside
Presenter:
Lilian Abbo, MD
Associate Professor of Clinical Medicine
Division of Infectious Diseases, University of
Miami Miller School of Medicine
Dr. Abbo's clinical and research areas of interest are in
antimicrobial stewardship and transplant associated
infections. Dr. Abbo has been an active member of the
Infectious Diseases Society of America Standard and Practice
Guidelines Committee and a committee member of the
International Society of Chemotherapy, Antimicrobial
Stewardship Working Group. She has published numerous
original research and review articles in antimicrobial
stewardship and immune-compromised host-associated
infections.
VIEW HERE

This is the first report of molecular typing of MRSA isolates
from Cuba and shows that the predominant clone is spa-type
149, followed by CA-MRSA USA300. This clone was first
described in the United States, where it has now become en-
demic; it’s finding in Cuba highlights the wide spread of this
strain over Latin America.9
Another study in a Havana paediatric institution between 2010
-2012 confirmed 333 MRSA isolates and revealed that 65.9%
of MRSA isolates caused severe skin and soft tissue infections
requiring hospitalization. Genes encoding PVL were detected
both in community-acquired isolates (86%) and hospital-
associated strains (54.5%), pointing to the possible movement
of MRSA clones to the hospital environment, but also suggest-
ing that hospital isolates could be producing the toxin, thus
reducing PVL as a valuable epidemiological marker.
In conclusion, MRSA is both a hospital and community prob-
lem for Cuba and demands local surveillance on prevalence
and transmission dynamics. Surveillance studies that utilize
molecular typing will lead to a better understanding of its epi-
demiology and permit the design of more assertive control
strategies. However, faced with the inability to conduct com-
prehensive studies of molecular characterization, we must
ensure that the microbiology laboratory can accurately identify
MRSA infections. Physicians must be alerted to control its
spread through prudent use of antibiotics, with an emphasis on
limiting the use of glycopeptides and prolonged therapy. Hos-
pitals must also define appropriate protocols for the manage-
ment or treatment of individuals colonized or infected with
CA-MRSA.
References
1. Holden MTG, Hsu L, Kurt K, et al. A genomic portrait of the
emergence, evolution, and global spread of a methicillin-resistant
Staphylococcus aureus pandemic. Genome Res. 2013;23:653–64.
2. Guzman-Blanco M, Mejia C, Isturiz R, et al. Epidemiology of
methicillin-resistant Staphylococcus aureus (MRSA) in Latin Amer-
ica. Int J Antimicrob Agents 2009;34:304-308.
20 • The APUA Newsletter Vol. 31. No. 3 • © 2013 APUA • Peraza & Lopez
Staphylococcus aureus is responsible for a wide variety of
clinical problems, ranging from skin and soft tissue infections,
to severe systemic and life threatening diseases. The organism
is relevant in the community and is commonly associated with
nosocomial infections. S. aureus possesses a large capacity to
acquire antimicrobial resistance genes, with strains currently
resistant to the majority of available antibiotics—particularly
to methicillin, a resistance reported initially in the hospital
environment (hospital-associated methicillin resistant S. aure-
us, HA-MRSA) and subsequently in the community
(community-associated methicillin resistant S. aureus, CA-
MRSA), has complicated the worldwide control of infection
by this microorganism.1
MRSA is an increasing problem in the Americas and the Car-
ibbean, but in Cuba very little is known about its epidemiolo-
gy and even less about its behavior in the community.2 Some
epidemiological data are available from independent studies of
different hospital institutions and nasal carriage surveys, but
the reports are infrequent and insufficient to estimate the
change in the morbidity and mortality of annual national fig-
ures.3-6 However, the available evidence suggests a MRSA
incidence greater than 50% in Cuban hospitals. 7
A collaborative study between Hospital Canisius-Wilhelmina
in Nijmegen, Netherlands, and Pedro Kourí Institute (IPK) in
Havana, Cuba investigated the molecular epidemiology of 68
MRSA clinical strains (isolated from wounds, bronchial/
tracheal aspirations, blood, skin, abdominal drainage and chest
tissue biopsy), prospectively collected from three major hospi-
tals in Cuba during three months in 2008. Molecular testing
was performed for detection of Panton-Valentine leukocidin
(PVL), mecA , the Sa442 element and spa typing. Forty iso-
lates were mecA positive and confirmed to be MRSA. Spa
typing identified five different spa types: t149 (n = 24), t008
(n = 8), t037 (n = 6), and one each of t4088 (closely related to
t149) and t2029 (closely related to t037). All eight t008 iso-
lates (but none of the other spa types) were PVL-positive.
Multi locus sequence typing (MLST) was performed on t008
isolates and all proved to be CC8 positive.8
Methicillin-resistant Staphylococcus
aureus in Cuba
Gilda Toraño Peraza, PhD and Alexis Monzote López, MD
Bacteriology-Mycology Department, Pedro Kourí Institute, Havana, Cuba; APUA-Cuba Members

Clínico-Quirúrgico Hermanos Ameijeiras de La Habana, Cuba. La
Gaceta de Infectología y Microbiología Latinoamericana. 2012;2
(2):47-54.
7. Latin American Resistance Surveillance Network. Annual report on
the antibiotic resistance monitoring/surveillance network, 2008. ©
PAHO HSD/CD 2011.
8. Hopman J, Toraño G, Espinosa F, et al. USA300 Methicillin-
resistant Staphylococcus aureus in Cuba. Antimicrob Resist Infect
Control. 2012;1:2.
9. Reyes J, Rincon S, Diaz L, et al. Dissemination of methicillin-
resistant Staphylococcus aureus USA300 sequence type 8 lineage in
Latin America. Clin Infect Dis 2009,49:1861-1867.
Upcoming webinar:
Antibiotics: Managing a Medical Treasure
Live Event: Friday, January 31, 2014 1:00 PM EST
PACE® credit available
Antimicrobial agents are a remarkable class of drugs that are
responsible for some of the most dramatic improvements in
medical therapy in history. However, these medicines are
also the only class of drugs whose efficacy diminishes as we
use them. The link between antibiotic use and the
development of resistance has been repeatedly made since the 1950s, yet clinicians have not learned from mistakes that have
occurred with the introduction of new antibiotics. The development of resistance to carbapenems is now one of the greatest
challenges to medicine since there is little on the horizon for patients suffering from carbapenem-resistant, gram-negative
infections. Clinicians must realize how perilously close we are to a ’post-antibiotic’ era.
While no one doubts the importance of infection control practices in limiting the spread of antibiotic-resistant organisms,
optimizing antibiotic use, also known as antibiotic stewardship, remains essential for successful control of the antibiotic
resistance. Approaches to optimize antibiotic use vary in their effectiveness; some interventions are restrictive while others are
persuasive. The overriding premise that antimicrobials are medical treasures, should guide all prescribers whenever these drugs
are used. Once begun, their continued use must be scrutinized. Antibiotic de-escalation is a complex concept comprised of three
questions: Is the patient actually infected at all? Is the patient actually infected with bacteria? How long do you need to treat with
antimicrobials?
This webinar will:
Analyze the relationship between antibiotic use and antibiotic resistance
Review the reasons for the dearth of new antibacterial antibiotics
Discuss the need for antibiotic stewardship
Describe the methods for optimizing antibiotic use including the use of biomarkers, newer diagnostic tools and approaches to
de-escalate antibiotics
Field report—Cuba • The APUA Newsletter Vol. 31. No. 3 • © 2013 APUA • 21
3. Nodarse R. Detection of methicillin-resistant Staphylococcus aureus
by cefoxitin sodium disc. Rev Cub Med Mil 2009;38:3-4 http://
scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0138-
65572009000300004&lng=es.
4. Toraño G, Quiñones D, Hernández I, et al. Portadores nasales de
Staphylococcus aureus resistente a la meticilina entre niños
cubanos que asisten a círculos infantiles. Enferm Infecc Microbiol
Clin. 2001;19(8):367-70.
5. Hernández IT, Toraño GT, González M, González I. Staphylococcus
aureus resistente a la meticilina: detección de portadores entre
niños hospitalizados y niños sanos de la comunidad. Rev Cubana
Med Trop 2003; 55(3):153-61.
6. Espinosa F, López AL, Hart M, Toraño G. Susceptibilidad antibac-
teriana de cepas de Staphylococcus aureus aisladas en el hospital
Presenter: Robert Gaynes, MD
Professor of Medicine
Emory University School of Medicine
Dr. Gaynes is Chair of the Antimicrobial
Stewardship Committee and Infection Control
Committee at Emory University School of Medicine and the
Atlanta VA Hospital. Dr. Gaynes has authored and/or coauthored
over 145 papers/book chapters on infectious disease topics and in
2011 published a book entitled, Germ Theory: Medical Pioneers in
Infectious Diseases.
APUA’s Antibiotic Stewardship Webinar Series
REGISTER HERE

MRSA News
New compounds may boost antibiotic
efficacy for MRSA, anthrax
Thomas Poulos of University of California - Irvine and Richard
Silverman of Northwestern University have demonstrated an
approach for treating neurodegenerative diseases that may be
applicable to combating bacterial diseases. By using inhibitor
compounds to block neuronal nitric oxide synthase (NOS—an
enzyme that appears to help bacteria resist antibiotics), the
researchers believe they may be able to increase antibiotic
effectiveness. By coupling antibiotics with NOS-inhibitor
compounds, bacteria were killed off more effectively than they
were using antibiotics alone. Testing suggests that combining
the compounds with antibiotics creates a special bond that
increases the efficacy of the drug. The studies, which will be
extended to animal models, have implications for treatment of
severe bacterial pathogens, such as MRSA and anthrax.
MRSA survivors unite for World MRSA Day
Kickoff Event
On September 28, the Chicago-based non-profit MRSA
Survivors Network held its 5th Annual World MRSA Day
Kickoff Event & Global C. difficile Summit. The Chicago,
Illinois gathering brought together MRSA survivors,
physicians and lawmakers at an event designed to raise
awareness in the fight against MRSA and other healthcare-
acquired infections. The Network’s founder, Jeanine Thomas,
declared that the U.S. CDC has underreported MRSA infection
and death rates in its recent studies. Thomas also called upon
Congress to “declare MRSA and C. difficile epidemics and
appropriate funds for prevention and public awareness
campaigns.” The MRSA Survivors Network calls for a
comprehensive approach to MRSA detection and control,
including patient isolation and decolonization, strict adherence
to hand hygiene guidelines, vigilant decontamination of
surfaces, and more prudent usage of antibiotics. The kickoff
event was a precursor to World MRSA Day, (October 2), and
World MRSA Awareness Month (October).
CDC: Community-associated MRSA not
declining
A CDC study published in The Journal of the American
Medical Association (JAMA) in September sought to estimate
the burden of methicillin-resistant Staphylococcus aureus
(MRSA) among US adults. The study, titled “National Burden
of Invasive Methicillin-Resistant Staphylococcus aureus
Infections, United States, 2011,” used laboratory-based
findings to identify MRSA cultures in nine different US cities
between the years 2005 and 2011. In 2011, there were 80,461
total cases of MRSA infections across the nation. Of these,
48,353 were classified as healthcare-associated community-
onset (HACO), 14,156 as hospital-onset infections, and 16,560
as community-associated infections. Between 2005 and 2011,
national incidence rates for HACO infections and for hospital-
onset infections decreased markedly (by 27.7% and 54.2%,
respectively). Community-associated infections, however, only
decreased by 5% across the same six years. Overall, the
decreases in MRSA infection rates are encouraging signs, but
this study makes it clear that increased emphasis must be
placed on decreasing the spread of MRSA outside of the
healthcare setting.
CDC reports on pediatric MRSA
In September, the U.S. CDC published a new study in
Pediatrics that found unexpected results regarding the
incidence and prevalence of invasive MRSA infections in
children. The study, titled, “Trends in Invasive Methicillin-
Resistant Staphylococcus aureus Infections,” found that rates
of invasive pediatric MRSA between 2005-2010 were much
lower than those reported among adults. However, while
national trends in invasive adult healthcare-associated MRSA
have shown dramatic declines, no significant changes were
found among children aged three months to 17 years. Most
alarming is the CDC’s finding that community-associated
MRSA infections are actually increasing among children—
signaling the need for more prevention of MRSA infections
outside of the hospital. Lastly, it appears that both young
infants and black children are disproportionately affected by
serious MRSA infections.
22 • The APUA Newsletter Vol. 31. No. 3 • © 2013 APUA • MRSA news

APUA headquarters and chapters in action
APUA headquarters and chapters in action • The APUA Newsletter Vol. 31. No. 3 • © 2013 APUA • 23
APUA partners with Alere Inc. to build “Test
Target Treat” educational platform
Through an unrestricted educational grant from Alere, APUA
has brought together multiple experts from around the world to
contribute to a diverse collection of educational materials dedi-
cated to antimicrobial stewardship. The materials will include
clinical monographs, case studies addressing six different dis-
ease states, personal perspectives from stake holders within the
healthcare system, recorded interviews, and three educational
webinars. APUA looks forward to the roll-out process, which
will follow in the coming months. Please check here for more
details and updates as new educational pieces are added.
APUA attends ID week – presents “Learning
Lounge”
APUA president, Dr. Stuart Levy, and Executive Director,
Kathleen Young, hosted a booth at this year’s ID Week, which
took place from October 2-6 in San Francisco, CA. ID Week is
an annual collaboration between the Infectious Diseases Socie-
ty of America (IDSA), the Society for Healthcare Epidemiolo-
gy of America (SHEA), the HIV Medicine Association
(HIVMA), and the Pediatric Infectious Diseases Society
(PIDS). Every year, more than 5,500 professionals from 80
different countries attend the five-day meeting, which serves as
an educational and networking event for those with an interest
in infectious diseases.
In addition to hosting a booth that shared APUA’s mission
and recent work, Drs. Stuart Levy and Kavita Trivedi (CA
Department of Public Health) held a “Learning Lounge”
presentation and discussion titled, “Antibiotic Stewardship and
the Role of Diagnostics: Barriers and Opportunities,” which
drew over one hundred participants.
APUA participates in CDC’s Get Smart About
Antibiotics Week 2013
APUA was a proud participant in the U.S. Centers for Disease
Control and Prevention’s (CDC) annual Get Smart About Anti-
biotics Week (November 18-24). The CDC’s campaign com-
bines non-profit partners, for-profit partners, and state-based
campaigns supporting appropriate antibiotic use. The collabo-
ration sets the stage for a week-long observance of antibiotic
resistance and the need for proper usage of antibiotics. APUA
contributed throughout the week with extensive social media
communications, which culminated in a live Twitter chat host-
ed by the CDC.
Boston-area Antimicrobial Research
Network (BAARN) Meeting
Posing the question ‘What does it take to succeed in antibiotic
R&D?’ a group of like-minded stakeholders gathered for a day
-long symposium this fall as the Boston-area Antimicrobial
Research Network or BAARN. The 110 individual partici-
pants, coming from industry, academia, medical centers, and
NGOs, examined the emerging regulatory landscape and avail-
able resources to develop and utilize novel approaches to target
pathogen-directed therapies. APUA and the ~30 other organi-
zations that comprise the network pledged to meet annually
and maintain a website to share information towards their com-
mon goal.
Chapter update: APUA-Ecuador
APUA-Ecuador reports several significant accomplishments in
its recent history. This 180-member chapter has enacted con-
trol over antibiotics and established resistance surveillance
programs in five different specialty hospitals in the capital city
of Quito. In a joint effort with other Ecuadorian scientific soci-
eties, the Chapter has also submitted a letter to the Presidency
and National Assembly, alerting them to the growing issue of
bacterial resistance. The letter serves as a call-to-action and
asks for the government’s support with bacterial resistance
prevention programs. In order to better educate healthcare pro-
viders and patients on the issue of antimicrobial resistance,
APUA-Ecuador has developed a monthly publication that is
delivered to all Specialization Public Hospitals across the
country.
The Chapter also reports the hosting of two upcoming confer-
ences in Ecuador: the Pan American Congress of Infectious
Diseases, and the Pan American Association for Infectious
Diseases, which will be chaired by its leader, Dr. Ana Celi de
la Torre.
Chapter update: APUA-Nepal
Access the tenth annual APUA -Nepal Newsletter, here.
24 • The APUA Newsletter Vol. 31. No. 3 • © 2013 APUA • Obituaries; upcoming events
January 27-29, 2014: American Society for
Microbiology (ASM) BioDefense & Emerging Diseases
Research Meeting, Washington, DC, USA.
March 20, 2014: British Society for Antimicrobial
Chemotherapy’s Spring Meeting 2014, London, UK.
May 10-13, 2014: European Congress on Clinical
Microbiology and Infectious Diseases (ECCMID 2014),
Barcelona, Spain.
May 17-20, 2014: American Society for Microbiology’s
Annual Meeting (ASM 2014), Boston, MA, USA.
June 7-9, 2014: Association for Professionals in
Infection Control and Epidemiology’s Annual Conference
(APIC 2014), Anaheim, CA.
June 23-24, 2014: Annual Global Healthcare Conference
(GHC 2014), Singapore.
July 6-9, 2014: The Australasian Society for Infectious
Diseases (ASID) Annual Scientific Meeting, Melbourne,
Australia.
July 27- August 1, 2014: International Union of
Microbiological Societies’ 2014 Congresses, Montreal,
Canada.
XIVth International Congress of Mycology
XIVth International Congress of Bacteriology and Applied
Microbiology
XVIth International Congress of Virology
September 5-9, 2014: Interscience Conference on
Antimicrobial Agents and Chemotherapy (ICAAC 2014),
Washington, DC, USA.
October 8-12, 2014: Infectious Diseases Society of
America (IDSA), the HIV Medicine Association (HIVMA),
and the Pediatric Infectious Diseases Society (PIDS)’s ID
Week 2014, Philadelphia, PA, USA.
October 31- November 3, 2014 : 5th International
Meeting on Emerging Diseases and Surveillance - “IMED
2014,” Vienna Austria.
Upcoming Events Obituaries
Both of these APUA Scientific Advisory Board members were
instrumental in initiating and supporting the Reservoirs of
Antibiotic Resistance project.
Dr. Donald Low, an internationally
recognized Canadian microbiologist and
member of APUA’s Scientific Advisory
Board, passed away on September 18,
2013 at the age of 68. Low led an active
and meaningful career as microbiologist-
in-chief at Mount Sinai Hospital in
Toronto. He was diagnosed with a brain
tumor earlier this year. Low was most known for his tireless
efforts responding to the 2003 Toronto outbreak of severe
acute respiratory syndrome (SARS), during which he became
a public figure for the city’s response to the outbreak that
claimed 44 lives in Toronto. Over his lifespan, he co-authored
over 400 peer-reviewed articles for scientific journals and
made a name for himself as an expert in necrotizing fasciitis
(flesh-eating disease) caused by Group A Streptococcus. As
evidenced by his role at APUA, Low dedicated himself to
combating the rise of antimicrobial resistance by championing
the appropriate use of antibiotics.
Dr. Abigail Salyers, a wor ld re-
nowned research scientist, author and
professor at the University of Illinois at
Urbana-Champaign, passed away at the
age of 70 on November 6, 2013. In
1983, Salyers became the first female
tenured professor in microbiology at
Illinois. She quickly went on to become
a full professor, and received a multitude of awards in the
three decades she taught and researched there. Dr. Salyers
wrote five books and published over 200 peer-reviewed
research articles, book chapters, and reviews that were widely
read and cited. From 2001 to 2002, Abigail was president of
the American Society for Microbiology, where she shone as a
leader and championed her interest in the diversity of
microorganisms on the planet. She was also one of the original
members of APUA's Reservoirs of Antibiotic Resistance
project.

Leadership Award: Dr. Keith Klugman
The distinguished recipient of this year’s 2013 APUA
Leadership Award is Dr. Keith Klugman, who was honored at
a dinner held in San Francisco, CA during ID Week 2013.
Chosen from a pool of highly qualified individuals nominated
for this year’s award, Dr. Klugman received the award for his
work on the pneumococcal vaccine. His research has focused
on the emergence of antibiotic-resistant pneumococci and
factors that spread this resistance. He has published more than
450 scientific papers on pneumonia, meningitis, antimicrobial
resistance, and vaccines for bacterial pathogens and served as
an expert on antimicrobial resistance for numerous committees,
including at the WHO and the CDC. APUA also commends
him for his recent appointment as the Director of Pneumonia
Studies at the Bill and Melinda Gates Foundation.
APUA 2013 Leadership & Chapter Awards
APUA headquarters and chapters in action • The APUA Newsletter Vol. 31. No. 3 • © 2013 APUA • 25
of Microbiological Societies)-sponsored international
conference on antibiotic resistance in Havana, Cuba where
he had the honor of personally presenting APUA’s 2013
Chapter Award. The conference on resistant bacteria and
fungi addressed pressing problems related to antibiotic use in
Cuba. The visit provided an opportunity to share per-
spectives on important global issues and congratulate Cuban
colleagues on their impressive multi-faceted approach to
fighting antimicrobial resistance.
As part of these efforts, APUA-Cuba has hosted multiple
symposia on antimicrobial resistance and the need for new
antibiotics. The chapter’s electronic database allows for daily
communication and serves as an important venue for
discussion of scientific issues. APUA-Cuba has also utilized
four television appearances to educate the public on the
importance of proper use of antibiotics and the consequences
of inappropriate use.
Recently APUA-Cuba unveiled its new San Cristobal sub-
chapter, with an enrollment of 150 members. Before an
audience of almost 200 medical professionals, five
specialists from APUA-Cuba presented updated information
and led discussions on antibiotic stewardship, childhood
pneumonia, the human microbiome, treatment of multi-
resistant infections, and surgical prophylaxis.
Chapter Award: APUA-Cuba
The Alliance for the Prudent Use of Antibiotics was pleased to
bestow its 2013 APUA Chapter Award on APUA-Cuba, in
recognition of the chapter’s exemplary efforts to improve
antibiotic stewardship and awareness in Cuba and throughout
Latin America. In just six years of existence, APUA-Cuba has
enrolled over 2,000 members from 63 medical specialties and
has established 9 provincial chapters nationwide, including a
newly established sub-chapter in San Cristobal.
November 14-16, APUA President Dr. Stuart B. Levy
attended and presented at the 2nd IUMS (International Union
Dr. Keith Klugman (center), recipient of the APUA
Leadership Award, with Dr. Jay Levy (left) and
APUA President Dr. Stuart Levy (right).
APUA President Dr. Stuart Levy (right) with chapter
leader, Dr. Moises Morejon, who received the 2013
Chapter Award on behalf of APUA-Cuba
New Chinese policies promote rational use
of antibiotics
A PLOS Medicine study titled, “Changes in Chinese Policies
to Promote the Rational Use of Antibiotics” evaluates the
success of a recent antimicrobial stewardship program in
China. The Chinese campaign, motivated by the high rates of
morbidity and mortality due to antimicrobial resistance in
China, was designed to promote more rational use of
antimicrobials in healthcare settings. The campaign,
implemented by the Chinese Ministry of Health in 2011, was
coupled with new healthcare reforms and established new
mandatory management approaches, such as the development
of audit and inspection systems, target-setting, and task force
organization. According to the study, the campaign
successfully decreased antibiotic sales by eight percentage
points in one year and reduced prescriptions for
antimicrobials for both outpatients and hospitalized patients.
Despite promising results, the study highlights the need to
improve antimicrobial use in other settings, including over-the-
counter sales and animal husbandry.
Netherlands and Russia to collaborate on
antibiotic resistance effort
In a recently announced partnership, the Netherlands and
Russia are joining forces to combat antibiotic resistance. A
Dutch-Russian commission will be established to examine the
issue of antimicrobial resistance and the best policies for
reducing its impact. The agreement between these two
countries signifies that both governments acknowledge the
serious nature of this growing problem and the potential public
health consequences it may hold for each.
FDA releases guidelines to limit use of
antibiotics in meat production
On Wednesday, December 11 the FDA released the final FDA
Guidance for Industry 213 and the draft Veterinary Feed
Directive (VFD). This is the first time since 1977 the FDA has
taken broad action against the use of antibiotics in livestock.
The two sets of guidelines are designed to encourage
agriculture to voluntarily stop using sub-therapeutic growth-
promoting dosing, and to involve veterinarians in the
administration of antibiotics to farm animals. Although only
voluntary, the FDA guidelines do demonstrate progress
towards the goal of eliminating sub-therapeutic antibiotic use
in food animal production. This positive step will help the
US catch up with EU regulations on agriculture.
APUA played a major role in promoting this policy change
by documenting the science as evidence and publishing in
journals such as Clinical Microbiology Reviews. APUA’s
comprehensive FAAIR (Facts About Antibiotics in Animals
and their Impact on Resistance) report, published in Clinical
Infectious Diseases (CID) was used as evidence and expert
opinion in testimony by advocacy groups. Current legislation
in Congress, the Preservation of Antibiotics for Medical
Treatment Act, would go much further towards eliminating
the use of medically important antibiotics for growth
promotion.
Antibacterials questioned by the FDA
In the face of mounting evidence that questions the safety of
antibacterials in soaps, toothpastes and a multitude of other
household products, the U.S. FDA has moved to require
manufacturers to demonstrate the safety and efficacy of such
chemicals. The antibacterials of concern, triclosan and
triclocarban, are accumulating in groundwater and soils and
have been found in 75% of US urine samples and 97% of
breast milk samples. Following proliferation of these agents
in non-hospital-based products over previous decades,
evidence has accumulated showing hormone disturbances in
children (e.g., decreasing thryroid function). Furthermore,
worries over escalating antibiotic resistance have fueled
concerns over the possible promotion of cross-resistance to
antibiotics. The proposed FDA rule will provide a 1-year
period for manufacturers to demonstrate product safety and
efficacy before requiring removal of the antibacterial
components.
Policy Updates
26 • The APUA Newsletter Vol. 31. No. 3 • © 2013 APUA • Policy updates

Salmonella outbreak exposes weaknesses in
monitoring of US food chain
A recent news article highlights the weaknesses in the U.S.
Food and Drug Administration (FDA) and U.S. Department of
Agriculture (USDA)’s methods for ensuring the safety of the
food supply. Beginning in October, a virulent, antibiotic-
resistant Salmonella outbreak, traced to three poultry plants in
California, sickened over 300 people across the U.S.
Surprisingly, none of the plants in question failed salmonella
testing in October because inspectors do not test chicken after
processing into parts, such as drumsticks, thighs, and breasts. It
is believed that the Salmonella contamination spread during
this secondary processing step. Under current federal rules, no
more than 7.5 percent of broilers should test positive for the
bacteria, but no rules govern the quantities of salmonella that
are acceptable in chicken parts. The government estimates that
24% of chicken parts are positive.
Even if inspectors had detected an alarming amount of the
bacteria before the outbreak, USDA authority could only have
pressured the plants to improve the processes—not force plant
closure. Such federal policies are just some of many that
expose Americans to the risks of food-borne illnesses that are
becoming increasingly resistant to antibiotics.
Taiwan reports successes of antimicrobial
stewardship program
An antimicrobial stewardship program in a Taiwan
community public teaching hospital has demonstrated marked
success in reducing unnecessary antibiotic use and costs. In a
study published in the American Journal of Infection Control,
researchers examined the effects of a three-year stewardship
program on antibiotic consumption, costs, and quality of
patient care in a 415-bed hospital. The three primary strategies
implemented were: clinical pharmacist-based intervention,
education of prudent antimicrobial use, and regular
announcements of outcomes. The program lowered
consumption of aminoglycosides, first-generation
cephalosporins, and aminopenicillins and successfully
reduced hospital antibiotic costs by 43.4% over the three-year
period—from $21,464 to $12,146 per 1,000 patient-days.
$2.5 million was saved in total hospital costs despite an
estimated labor cost of $3,935 per month. Lastly, patients’
quality of care did not decline, as measured by length of stay,
incidence of healthcare-associated infections, and mortality.
Harmony Institute endows antibiotic
resistance research
In a recent press release The Univ-
ersity of Central Florida College of
Medicine and the Harmony
Institute announced a partnership with the goal of creating an
endowed “Harmony Scholars” chair to embark upon
longitudinal studies in Harmony, Florida, a planned community
specifically designed to accommodate such studies. Because
of the critical nature of antibiotic resistance and the opportunity
for a population study, the Harmony Institute and UCF College
of Medicine are investigating antibacterial resistance as one of
several beginning studies.
This project was first reported in the APUA Newsletter, Volume
31. For further information contact Martha E. Lentz, President
and Founder, The Harmony Institute at
CDDEP researches free antibiotics programs
Are “free antibiotic programs” doing more harm than good?
Health Economics recently published a new study from the
Center for Disease Dynamics, Economics and Policy (CDDEP)
that gives evidence to the concerns that free antibiotic programs
are contributing to unnecessary drug prescriptions and possibly
to the problem of antibiotic resistance. The study, co-authored
by CDDEP Director Ramanan Laxminarayan, looked at the
consequences of the first free antibiotic program in the U.S.,
started in 2006 as an effort by the Meijer supermarket chain to
improve access to valuable drugs. Researchers found that across
four states, zip codes in which the program operated had 5%
higher rates of antibiotic prescription than those without the
program. Low-income areas, which the program would
ostensibly aid the most, showed a 12% increase in antibiotic
prescriptions. This study shows that such well-intentioned
programs may be inadvertently contributing to over prescription
and overconsumption of antibiotics in the U.S.
News and publications of note
News and Publications of Note • The APUA Newsletter Vol. 31. No. 3 • © 2013 APUA • 27
About us
Antibiotics are humanity's key defense against disease-causing microbes. The growing prevalence of antibiotic resistance
threatens a future where these drugs can no longer cure infections and killer epidemics run rampant. The Alliance for
the Prudent Use of Antibiotics (APUA) has been the leading global non-governmental organization fighting to preserve
the effectiveness of antimicrobial drugs since 1981. With affiliated chapters in more than 65 countries, including 33 in
the developing world, we conduct research, education and advocacy programs to control antibiotic resistance and en-
sure access to effective antibiotics for current and future generations.
Our global network of infectious disease experts supports country-based activities to control and monitor antibiotic
resistance tailored to local needs and customs. The APUA network facilitates the exchange of objective, up-to-date
scientific and clinical information among scientists, health care providers, consumers and policy makers worldwide.
The APUA Clinical Newsletter has been published continuously three times per year since 1983.
Tel: 617-636-0966 • Email: [email protected] • Web: www.apua.org
APUA global chapter network
of local resources & expertise
200 Harrison Ave, Posner Building (Business) Level 3, Boston, MA 02111
Phone: 617-636-0966 | Fax: 617-636-0458 | E-mail: [email protected]
www.apua.org
“Preserving the Power of Antibiotics”®
About us • The APUA Newsletter Vol. 31. No. 3 • © 2013 APUA • 28