Embed Size (px)
Citation preview

FEATURE ARTICLES
3 Introduction to this issue
Bonnie Marshall (APUA News Staff)
4 Carbapenemases: a real threat
Dr. Moises Morejon Garcia, MSc (Hospital Universitario Manuel Fajardo, Havana, Cuba)
7 U.S. CDC is sounding the alarm on nightmare bacteria
Arjun Srinivasan, MD (U.S. CDC, Division of Healthcare Quality Promotion, Atlanta, GA)
10 Therapeutic approaches to carbapenem-producing Enterobacteriaceae: a brief update
Gabriel Levy Hara, MD (Hospital Durand, Buenos Aires, Argentina)
FOLLOW-UP: C. difficile
13 The epidemiology of community-acquired Clostridium difficile infection: a population-
based study
Sahil Khanna, MBBS, MS (Mayo Clinic, Rochester, MN)
APUA FIELD REPORTS & CHAPTER UPDATES
15 Impact of ESBLs and CREs—the Nigerian experience
17 ESBL-producing Enterobacteriaceae in Bulgaria
19 APUA-Kenya’s antimicrobial stewardship program
20 Acinetobacter baumannii epidemiology and
resistance in north Lebanon
18 Upcoming events
21 State & national responses to CRE & ESBL alarms
22 APUA headquarters in action: 2013 Leadership Award
and Directorship transition
23 APUA Learning Lab
24 Policy updates
25 News & publications of note
A light micrograph of the genus Klebsiella. These
non-motile, rod-shaped gram-negative bacteria live
normally in the human intestinal tract and commonly
cause opportunistic infections of the intestinal and
urinary tracts, lungs, and wounds. Highly prone to
developing antibiotic resistance, they are the most
common carriers of ESBL genes in healthcare
facilities and are the source of the KPC-type
carbapenemases that have spread globally.
Source: Med. Mic. Sciences Cardiff Uni, Wellcome Images
NEWSLETTER PUBLISHED CONTINUOUSLY SINCE 1983 BY THE ALLIANCE FOR THE PRUDENT USE OF ANTIBIOTICS
September 2013
Volume 31, No. 2
Nightmare bacteria and the worldwide threat to carbapenems
2 • The APUA Newsletter Vol. 31. No. 2 • © 2013 APUA
Chief Executives Stuart B. Levy, President
Thomas F. O’Brien, Vice President
Kathleen T. Young, Executive Director
Board of Directors Stuart B. Levy, Chairman Sherwood Gorbach
Gordon W. Grundy
Bonnie Marshall
Mark Nance
Thomas F. O’Brien
Arnold G. Reinhold
Dennis Signorovitch
Philip D. Walson
Mary Wilson
Editorial Staff Stuart B. Levy, Editor
Bonnie Marshall, Associate Editor
Michelle Haan, Assistant Editor
Thu Do, Contributor
Christopher Logan, Contributor
Advisory Board Jacques F. Acar, France
Werner Arber, Switzerland
Fernando Baquero, Spain
Michael l. Bennish, USA
Otto Cars, Sweden
Patrice Courvalin, France
Jose Ramiro Cruz, Guatemala
Julian Davies, Canada
Abdoulaye Djimde, Mali
Paul Farmer, Haiti
Walter Gilbert, USA
Herman Goossens, Belgium
Sherwood l. Gorbach, USA
Ian M. Gould, Scotland
George Jacoby, USA
Sam Kariuki, Kenya
Ellen L. Koenig, Dominican Republic
Calvin M. Kunin, USA
Jacobo Kupersztoch, USA
Advisory Board (cont.) Stephen A. Lerner, USA
Jay A. Levy, USA
Donald E. Low, Canada
Scott McEwen, Canada
Jos. W.M. van der Meer, The Netherlands
Richard P. Novick, USA
Iruka Okeke, USA & Nigeria
Maria Eugenia Pinto, Chile
Vidal Rodriguez-Lemoine, Venezuela
José Ignacio Santos, Mexico
Mervyn Shapiro, Israel
K. B. Sharma, India
Atef M. Shibl, Saudi Arabia
E. John Threlfall, United Kingdom
Alexander Tomasz, USA
Thelma e. Tupasi, Philippines
Anne K. Vidaver, USA
Fu Wang, China
Thomas E. Wellems, USA
Bernd Wiedemann, Germany
APUA Project Partnerships: The Bill and Melinda Gates Foundation
The Pew Charitable Trusts
U.S. National Institute of Health (NIH)
Pan American Health Organization
(PAHO)
U.S. Agency for International Develop-
ment (USAID)
U.S. Department of Agriculture
U.S. Office of Homeland Security
National Biodefense Analysis and Coun-
termeasures Center
The World Bank
World Health Organization (WHO)
Centers for Disease Control and Preven-
tion (CDC)
U.S. Food and Drug Administration
Ministries of Health
U.S. Defense Threat Reduction Agency
Supporting Chapters: APUA—Abu Dhabi
APUA—South Korea
Australian Society for Antimicrobials
(APUA-Australia)
British Society for Antimicrobial Chemo-
therapy (APUA-UK)
APUA gratefully acknowledges unrestrict-
ed grants from corporate sponsors:
Leadership Level ($20,000+) Clorox Healthcare
Bayer Healthcare Pharmaceuticals
Optimer Pharmaceuticals
Alere Inc.
bioMérieux
Partner Level ($10,000+) Alcon Laboratories
GlaxoSmithKline
Supporter Level ($2,500+) Cubist Pharmaceuticals
Disclaimer APUA accepts no legal responsibility for the content of any submitted articles, nor for the violation of any copyright laws by any person
contributing to this newsletter. The mention of specific companies or of certain manufacturers' products does not imply that they are endorsed
or recommended by APUA in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of
proprietary products are distinguished by initial capital letters.
The APUA Newsletter (ISSN 154-1424) © 2013 APUA Since 1983, the APUA Newsletter has been a continuous source of non-commercial information disseminated without charge to healthcare
practitioners, researchers, and policy-makers worldwide. The Newsletter carries up-to-date scientific and clinical information on prudent
antibiotic use, antibiotic access and effectiveness, and management of antibiotic resistance. The publication is translated into three languages and
distributed to over 7,000 affiliated individuals in more than 100 countries. The material provided by APUA is designed for educational purposes
only and should not be used or taken as medical advice. We encourage distribution with appropriate attribution to APUA. See previous editions
of the Newsletter on the APUA website.
*APUA welcomes letters to the Editor. Please send us your thoughts and questions. Names will be published but not
addresses. All letters may be edited for style and length.
Join the APUA corporate partnership
“Preserving the Power of Antibiotics”®
Phone: 617-636-0966 | Fax: 617-636-0458 | Email: [email protected] | Website: www.apua.org
Introduction to this issue
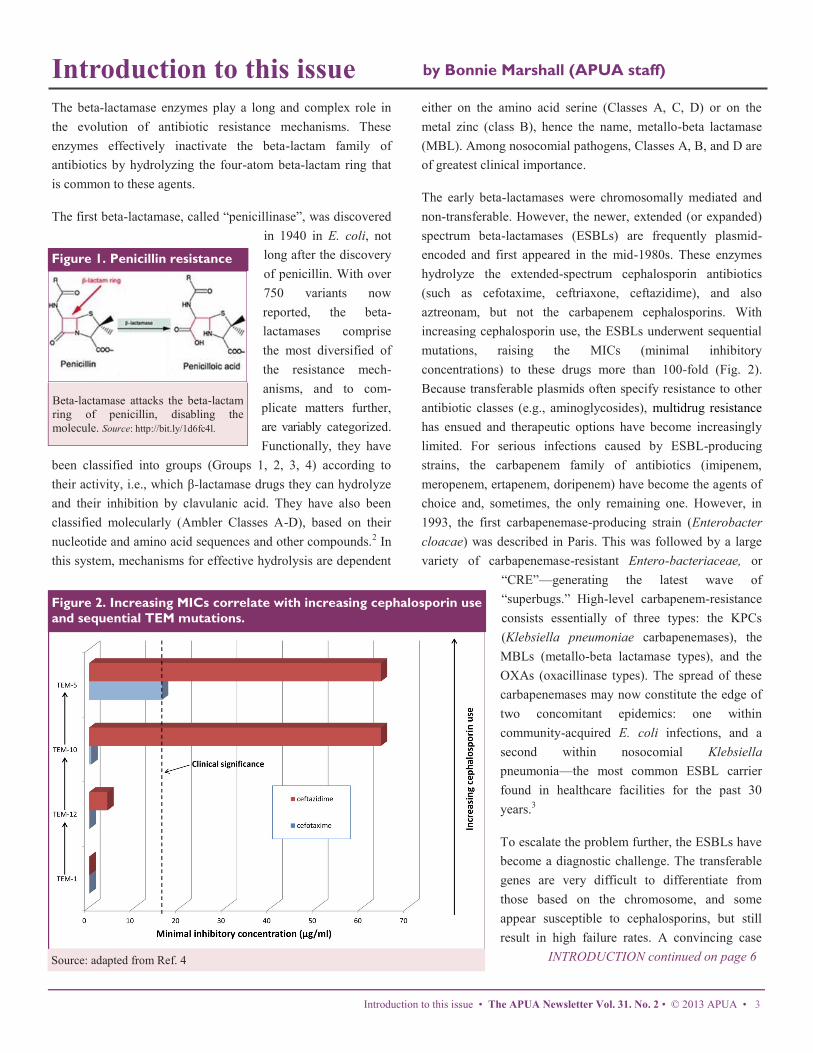
The beta-lactamase enzymes play a long and complex role in
the evolution of antibiotic resistance mechanisms. These
enzymes effectively inactivate the beta-lactam family of
antibiotics by hydrolyzing the four-atom beta-lactam ring that
is common to these agents.
The first beta-lactamase, called “penicillinase”, was discovered
in 1940 in E. coli, not
long after the discovery
of penicillin. With over
750 variants now
reported, the beta-
lactamases comprise
the most diversified of
the resistance mech-
anisms, and to com-
plicate matters further,
are variably categorized.
Functionally, they have
been classified into groups (Groups 1, 2, 3, 4) according to
their activity, i.e., which β-lactamase drugs they can hydrolyze
and their inhibition by clavulanic acid. They have also been
classified molecularly (Ambler Classes A-D), based on their
nucleotide and amino acid sequences and other compounds.2 In
this system, mechanisms for effective hydrolysis are dependent
either on the amino acid serine (Classes A, C, D) or on the
metal zinc (class B), hence the name, metallo-beta lactamase
(MBL). Among nosocomial pathogens, Classes A, B, and D are
of greatest clinical importance.
The early beta-lactamases were chromosomally mediated and
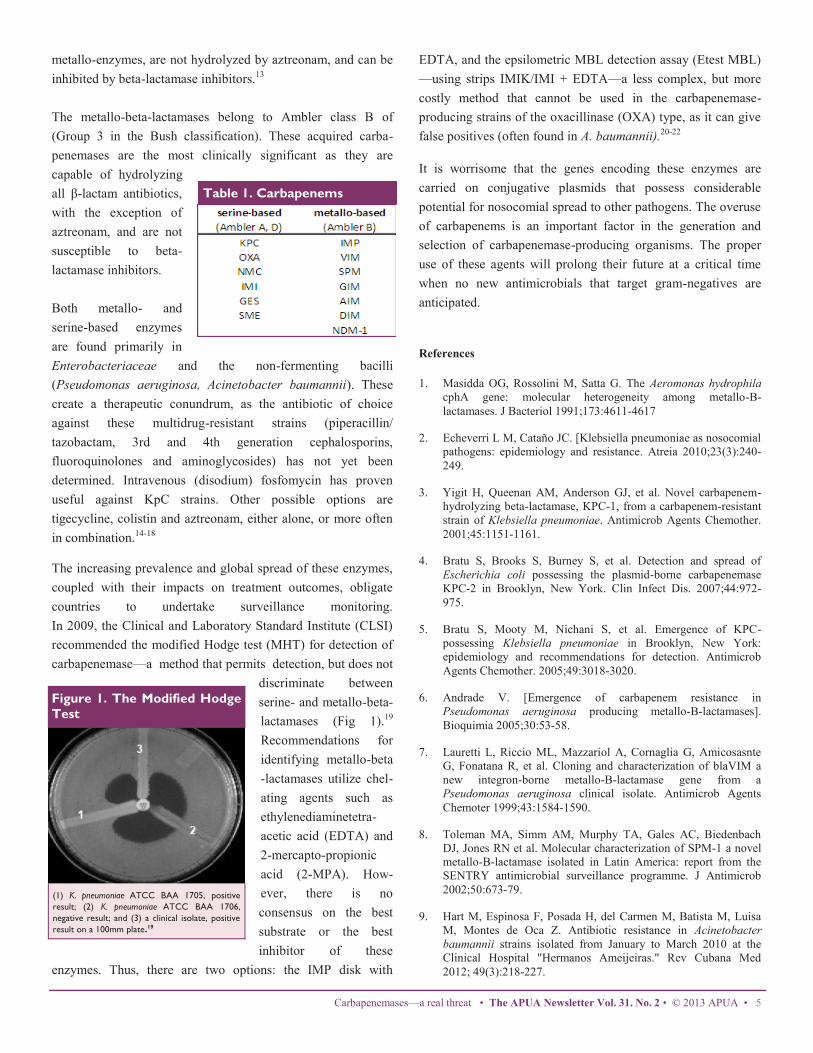
non-transferable. However, the newer, extended (or expanded)
spectrum beta-lactamases (ESBLs) are frequently plasmid-
encoded and first appeared in the mid-1980s. These enzymes
hydrolyze the extended-spectrum cephalosporin antibiotics
(such as cefotaxime, ceftriaxone, ceftazidime), and also
aztreonam, but not the carbapenem cephalosporins. With
increasing cephalosporin use, the ESBLs underwent sequential
mutations, raising the MICs (minimal inhibitory
concentrations) to these drugs more than 100-fold (Fig. 2).
Because transferable plasmids often specify resistance to other
antibiotic classes (e.g., aminoglycosides), multidrug resistance
has ensued and therapeutic options have become increasingly
limited. For serious infections caused by ESBL-producing
strains, the carbapenem family of antibiotics (imipenem,
meropenem, ertapenem, doripenem) have become the agents of
choice and, sometimes, the only remaining one. However, in
1993, the first carbapenemase-producing strain (Enterobacter
cloacae) was described in Paris. This was followed by a large
variety of carbapenemase-resistant Entero-bacteriaceae, or
“CRE”—generating the latest wave of
“superbugs.” High-level carbapenem-resistance
consists essentially of three types: the KPCs
(Klebsiella pneumoniae carbapenemases), the
MBLs (metallo-beta lactamase types), and the
OXAs (oxacillinase types). The spread of these
carbapenemases may now constitute the edge of
two concomitant epidemics: one within
community-acquired E. coli infections, and a
second within nosocomial Klebsiella
pneumonia—the most common ESBL carrier
found in healthcare facilities for the past 30
years.3
To escalate the problem further, the ESBLs have
become a diagnostic challenge. The transferable
genes are very difficult to differentiate from
those based on the chromosome, and some
appear susceptible to cephalosporins, but still
result in high failure rates. A convincing case
INTRODUCTION continued on page 6
by Bonnie Marshall (APUA staff)
Introduction to this issue • The APUA Newsletter Vol. 31. No. 2 • © 2013 APUA • 3
Figure 1. Penicillin resistance
Source: adapted from Ref. 4
Figure 2. Increasing MICs correlate with increasing cephalosporin use
and sequential TEM mutations.
Βeta-lactamase attacks the beta-lactam
ring of penicillin, disabling the
molecule. Source: http://bit.ly/1d6fc4l.

Carbapenemases: A real threat
Dr. Moises Morejon Garcia, MSc; APUA-Cuba President Hospital Universitario Manuel Fajardo, Havana, Cuba
Translated from Spanish
Although bacterial resistance is a natural evolutionary
phenomenon, the selective pressure exerted by antibiotic use in
the past 70 years has greatly accelerated this process. In their
evolution, bacteria have developed multiple mechanisms of
resistance—principally inactivating enzymes, mutations in
target sites and efflux pumps. The development and emergence
of inactivating enzymes began with the discovery and use of
the beta-lactams antibiotics—first penicillin in the 1940s and
subsequently, the cephalosporins in the 1960s. Over time, these
beta-lactam-inactivating enzymes expanded their spectrum of
activity—from penicillinases and cephalosporinases, to
extended-spectrum beta-lactamases (ESBLs) and most
recently, to the metallo-beta-lactamases (MBLs). These latter
enzymes, capable of hydrolyzing the carbapenems imipenem,
meropenem, ertapenem, and doripenem are virtually
incapacitating the last remaining treatments for multiresistant
gram-negative bacilli. The first reports of carbapenemase in the
1980s, and their subsequent spread across the globe, have
raised concern, and coincide with a decade in which no new
antimicrobial against gram-negatives is anticipated.
In the 1980s, Japan reported isolation of the first
carbapenemase from Aeromonas hydrophila.1 This was
followed by reports of the Seoul imipenemase (SME-1) from
Serratia marcescens in London (1982), and imipenemases
IMI-1 in California (1984) and NMC-A in France (1990), both
from Enterobacter cloacae.2
A report of the first Klebsiella pneumoniae carbapenemase
(KPC) in 1996 at a hospital in North Carolina raised concerns,
but outbreaks in 2001 in New York and New Jersey hospitals
created major alarm. These strains then spread across 27 U.S.
states to many Latin American countries, including Argentina,
Bolivia, Colombia, Venezuela, Uruguay, Brazil, Puerto Rico
and abroad (China, Israel, and France).3-5
In the 2000s, carbapenemase activity appeared in Southeast
Asia, Hong Kong and Singapore, while in Europe, the first
variant, IMP-2, appeared in a strain of Acinetobacter
baumannii. Meanwhile, reports of IMP increased in the U.S.,
Canada, and Brazil.6
A second family of carbapenemases, the Verona integron-
encoded metallo-lactamases (blaVIM-1), were isolated simul-
taneously in 1999 from strains of Pseudomonas aeruginosa and
Acinetobacter spp in Italy.7 Subsequently, a third metallo-
betalactamase family, SPM-1, was isolated from Pseudomonas
aeruginosa in Brazil.8 In Cuba, several reports of
carbapenemase-producing strains have sparked increased
vigilance.9,10
As the carbapenem antibiotics have been the primary therapy
against serious infections from multiresistant gram-negative
organisms, the emergence and increasing prevalence of the
carbapenemases jeopardize the effectiveness of this family of
antibiotics. According to the SENTRY global surveillance
report, rates in Latin America are higher than those in U.S. and
Europe.11
In 2008, the isolation of a new metallo-beta-lactamase, called
New Delhi metallo (NDM-1), raised global alarm due to its
isolation from Swedish and English patients who had
previously travelled to India and Pakistan. A surveillance study
between 2008 and 2010 in 29 European countries reported 77
cases of the NDM-1 enzyme in 13 of the countries,
predominantly in isolates of Klebsiella pneumoniae (54%).12
Subsequently, NDM-1 was found in Japan, Australia, Canada
and the USA.12
In November 2011, NDM-1 was first isolated in Latin
America—from a strain of Klebsiella pneumoniae. The
Guatermalan isolate prompted the Pan American Health
Organization (PAHO) to issue an alert for surveillance of these
health-care associated pathogens that seriously impact
morbidity and mortality.
The carbapenemases fall into two groups: the serine beta-
lactamases (serine-based) and the metallo-beta-lactamases
(zinc-based) (Table 1). The serine-based enzymes (enzymes of
Ambler class A or D) have less hydrolytic activity than the
4 • The APUA Newsletter Vol. 31. No. 2 • © 2013 APUA • Garcia
metallo-enzymes, are not hydrolyzed by aztreonam, and can be
inhibited by beta-lactamase inhibitors.13
The metallo-beta-lactamases belong to Ambler class B of
(Group 3 in the Bush classification). These acquired carba-
penemases are the most clinically significant as they are
capable of hydrolyzing
all β-lactam antibiotics,
with the exception of
aztreonam, and are not
susceptible to beta-
lactamase inhibitors.
Both metallo- and
serine-based enzymes
are found primarily in
Enterobacteriaceae and the non-fermenting bacilli
(Pseudomonas aeruginosa, Acinetobacter baumannii). These
create a therapeutic conundrum, as the antibiotic of choice
against these multidrug-resistant strains (piperacillin/
tazobactam, 3rd and 4th generation cephalosporins,
fluoroquinolones and aminoglycosides) has not yet been
determined. Intravenous (disodium) fosfomycin has proven
useful against KpC strains. Other possible options are
tigecycline, colistin and aztreonam, either alone, or more often
in combination.14-18
The increasing prevalence and global spread of these enzymes,
coupled with their impacts on treatment outcomes, obligate
countries to undertake surveillance monitoring.
In 2009, the Clinical and Laboratory Standard Institute (CLSI)
recommended the modified Hodge test (MHT) for detection of
carbapenemase—a method that permits detection, but does not
discriminate between
serine- and metallo-beta-
lactamases (Fig 1).19
Recommendations for
identifying metallo-beta
-lactamases utilize chel-
ating agents such as
ethylenediaminetetra-
acetic acid (EDTA) and
2-mercapto-propionic
acid (2-MPA). How-
ever, there is no
consensus on the best
substrate or the best
inhibitor of these
enzymes. Thus, there are two options: the IMP disk with
EDTA, and the epsilometric MBL detection assay (Etest MBL)
—using strips IMIK/IMI + EDTA—a less complex, but more
costly method that cannot be used in the carbapenemase-
producing strains of the oxacillinase (OXA) type, as it can give
false positives (often found in A. baumannii).20-22
It is worrisome that the genes encoding these enzymes are
carried on conjugative plasmids that possess considerable
potential for nosocomial spread to other pathogens. The overuse
of carbapenems is an important factor in the generation and
selection of carbapenemase-producing organisms. The proper
use of these agents will prolong their future at a critical time
when no new antimicrobials that target gram-negatives are
anticipated.
References
1. Masidda OG, Rossolini M, Satta G. The Aeromonas hydrophila
cphA gene: molecular heterogeneity among metallo-B-
lactamases. J Bacteriol 1991;173:4611-4617
2. Echeverri L M, Cataño JC. [Klebsiella pneumoniae as nosocomial
pathogens: epidemiology and resistance. Atreia 2010;23(3):240-
249.
3. Yigit H, Queenan AM, Anderson GJ, et al. Novel carbapenem-
hydrolyzing beta-lactamase, KPC-1, from a carbapenem-resistant
strain of Klebsiella pneumoniae. Antimicrob Agents Chemother.
2001;45:1151-1161.
4. Bratu S, Brooks S, Burney S, et al. Detection and spread of
Escherichia coli possessing the plasmid-borne carbapenemase
KPC-2 in Brooklyn, New York. Clin Infect Dis. 2007;44:972-
975.
5. Bratu S, Mooty M, Nichani S, et al. Emergence of KPC-
possessing Klebsiella pneumoniae in Brooklyn, New York:
epidemiology and recommendations for detection. Antimicrob
Agents Chemother. 2005;49:3018-3020.
6. Andrade V. [Emergence of carbapenem resistance in
Pseudomonas aeruginosa producing metallo-B-lactamases].
Bioquimia 2005;30:53-58.
7. Lauretti L, Riccio ML, Mazzariol A, Cornaglia G, Amicosasnte
G, Fonatana R, et al. Cloning and characterization of blaVIM a
new integron-borne metallo-B-lactamase gene from a
Pseudomonas aeruginosa clinical isolate. Antimicrob Agents
Chemoter 1999;43:1584-1590.
8. Toleman MA, Simm AM, Murphy TA, Gales AC, Biedenbach
DJ, Jones RN et al. Molecular characterization of SPM-1 a novel
metallo-B-lactamase isolated in Latin America: report from the
SENTRY antimicrobial surveillance programme. J Antimicrob
2002;50:673-79.
9. Hart M, Espinosa F, Posada H, del Carmen M, Batista M, Luisa
M, Montes de Oca Z. Antibiotic resistance in Acinetobacter
baumannii strains isolated from January to March 2010 at the
Clinical Hospital "Hermanos Ameijeiras." Rev Cubana Med
2012; 49(3):218-227.
Carbapenemases—a real threat • The APUA Newsletter Vol. 31. No. 2 • © 2013 APUA • 5
(1) K. pneumoniae ATCC BAA 1705, positive
result; (2) K. pneumoniae ATCC BAA 1706,
negative result; and (3) a clinical isolate, positive
result on a 100mm plate.19
Figure 1. The Modified Hodge
Test
Table 1. Carbapenems

10. Pedros W, Ramos A, Nodarse R, Padron A, De armas E.
[Bacterial resistance to extended beta-lactamase producing
bacteria) Revista Cubana de Medicina Intensiva y Emergencias
2006;5(1):294-301.
11. Suarez CJ, Kattan JN, Guzman AM, Villegas MV. [Mechanisms
of resistance to carbapenems in P. aeruginosa, Acinetobacter and
Enterobacteriaceae and strategies for its prevention and control.]
Infect. 2006;10(2):85-93.
12. Struelens MJ, Monnet DL, Magiorakos AP, Santos O’Connor F,
Giesecke J, the European NDM-1 Survey Participants. New
Delhi metallo-beta-lactamase 1–producing Enterobacteriaceae:
emergence and response in Europe. Euro Surveill. 2010;15
(46):pii=19716.
13. Tafur JD, Torres JA, Villegas MV. [Mechanisms of antibiotic
resistance in gram-negative bacteria.] CIDEIM 2008;12:217-226.
14. Oliver A. [Carbapenem Resistance and Acinetobacter
baumannii]. Enferm Infecc Microbiol Clin 2004;22(5):259-61
259.
15. Hurtado IC, Trujillo M, Restrepo A, Garcés C, Tamayo C, Mesa
JG. Experience with tigecycline compassionate use in pediatric
patients infected with carbapenem resistant Klebsiella
pneumoniae. Rev. Chil. Infectol. 2012;29(3): 317-321.
16. Jimeno A. [Epidemic outbreak of Pseudomonas aeruginosa
carbepenem-resistant producing metallo-beta-lactamase] Rev
Clin Esp.2011.doi:10.1016/j.rce.2010.12.006.
17. Cordova E, Lespada MI, Gomez N, Pasteran F, Oviedo V,
Rodriguez C. [Clinical and epidemiological description of a
nosocomial outbreak of KPC-producing Klebsiella pneumoniae
in Buenos Aires, Argentina]. 2012;30 (7):376–379.
18. Casellas JM. [Antibacterial resistance in Latin America:
Implications for infections]. Rev Panam Salud Publica 201;30
(6):519-528.
19. US Centers for Disease Control and Prevention. http://
www.ndhealth.gov/microlab/Uploads/HodgeTest.pdf.
20. Meyer G, Ulrich S. [Phenotypes of beta lactamase-producing
Klebsiella pneumoniae in the Emergency Hospital of Porto
Alegre].Bras Patol Med Lab 2011;47(1):25-31.
21. Radice M, Marin M, Giovanakis M, Bay C, Almuzara M,
Limansky A et al. [Test criteria, interpretation and reporting of
susceptibility testing to antibiotics in gram negative
nonfermenters of clinical significance: recommendations of the
Subcommittee on Antimicrobial Argentina Society of
Bacteriology, Mycology and Parasitology Clinics, Argentina
Association for Microbiology.] Revista Argentina de
Microbiología (2011) 43: 136-153.
22. Munoz JL [Problematic bacteria] Rev Esp Quimioter 2008;21:2-
6.
6 • The APUA Newsletter Vol. 31. No. 2 • © 2013 APUA • Garcia
can be made for the surveillance of ESBL activity. Many ESBL
resistances are a combination of sequential mutations. Because
the second and third mutations may result in very rapid rises in
MIC values, it is essential to detect the initial mutation early in
the process. Current clinical surveillance breakpoints are set
too high to detect these and thus will miss the first signal of an
impending resistance crisis.
The prevalence of carbapenemases is difficult to assess because
they very so widely from country to country (e.g., 3-5% in
France and >80% in India for ESBL-positive E. coli) and
because the possible “reservoir countries” have no surveillance
systems for detecting them.
This issue of the APUA Newsletter presents some of the
serious present-day challenges posed by the ESBLs and by the
newer carbapenemases in particular. The article by Garcia
overviews the emerging threat posed by the global spread of
carbapenemases, while that of CDC expert Srinivasan outlines
the seriousness of the problem in the US and government
interventions, including a “prevention toolkit” and
recommendations for providers and patients. Levy Hara
discusses the intricacies of CRE detection, as well as
antimicrobial treatment options. The articles by Ogbolu and by
Markovska/Keulyan present perspectives from sub-Saharan
Africa (Nigeria) and from Bulgaria, respectively.
References
1. Bush K, Jacoby GA, Medeiros AA (June 1995). A functional
classification scheme for beta-lactamases and its correlation with
molecular structure". Antimicrob. Agents Chemother. 39 (6):
1211–33.
2. Ambler RP (May 1980). The structure of beta-lactamases. Philos.
Trans. R. Soc. Lond., B, Biol. Sci. 289 (1036): 321–31.
3. Nordmann P, Naas T, Poirel L. (2011). Global spread of
carbapenemase-producing Enterobacteriaceae. Emerg Infect Dis
17:1791-1798.
4. Amyes S, Beta-lactamases: clinical impact and epidemiology.
2009. http://hstalks.com/main/view_talk.php?
t=1538&r=442&j=754&c=252.
Garcia references, continued INTRODUCTION, continued from page 3
“Containing healthcare associated infections through antibiotic stewardship”: webinar by Drs. Stuart Levy and
Shira Doron, http://bit.ly/18cfJCj
“Beta-lactamases: clinical impact and epidemiology”: webinar by Prof. Sebastian Amyes, http://bit.ly/14IRZVJ
Recommended Viewing
Sounding the alarm on
nightmare bacteria
The Centers for Disease Control and Prevention (CDC) and the
nation’s healthcare providers are now battling what may be one
of the most pressing patient safety threats of our time—
carbapenem-resistant Enterobacteriaceae (CRE). In its March
2013 issue of Vital Signs,1 CDC sounded the alarm on the
spread of CRE—“nightmare bacteria”—in U.S. inpatient
medical facilities, stating that action is needed now to halt the
spread of these deadly bacteria. CDC is asking for rapid action
from healthcare leaders to ensure that CRE prevention
measures are aggressively implemented in your facility and by
those around you.
Enterobacteriaceae are a family of more than 70 different
bacteria including Klebsiella pneumoniae and E. coli that
normally live in the digestive system. Over time, some of these
bacteria have become resistant to a group of antibiotics known
as carbapenems, often referred to as last-resort antibiotics.
During the last decade, CDC has tracked one type of CRE from
a single health care facility to health care facilities in at least 42
states. In some medical facilities, these bacteria already pose a
By Arjun Srinivasan, MD Associate Director for Healthcare Associated Infection Prevention Programs,
U.S. CDC, Division of Healthcare Quality Promotion
routine threat to patients.
Here are other important facts to know about CRE:
About 4% of US short-stay hospitals had at least one
patient with a serious CRE infection during the first half of
2012. About 18% of long-term acute care hospitals had
one. This totals almost 200 facilities.
The most common type of CRE is also rising rapidly –
there has been a seven-fold increase in its presence during
the last 10 years.
Up to half of patients who get CRE bloodstream infections
will die.
CRE often spread between patients on the hands of health care
personnel. In addition, CRE bacteria can transfer their
resistance to other bacteria within their family. This type of
spread can create additional untreatable infections. Currently,
almost all CRE infections occur in people receiving significant
medical care in hospitals, long-term acute care facilities, or
nursing homes.
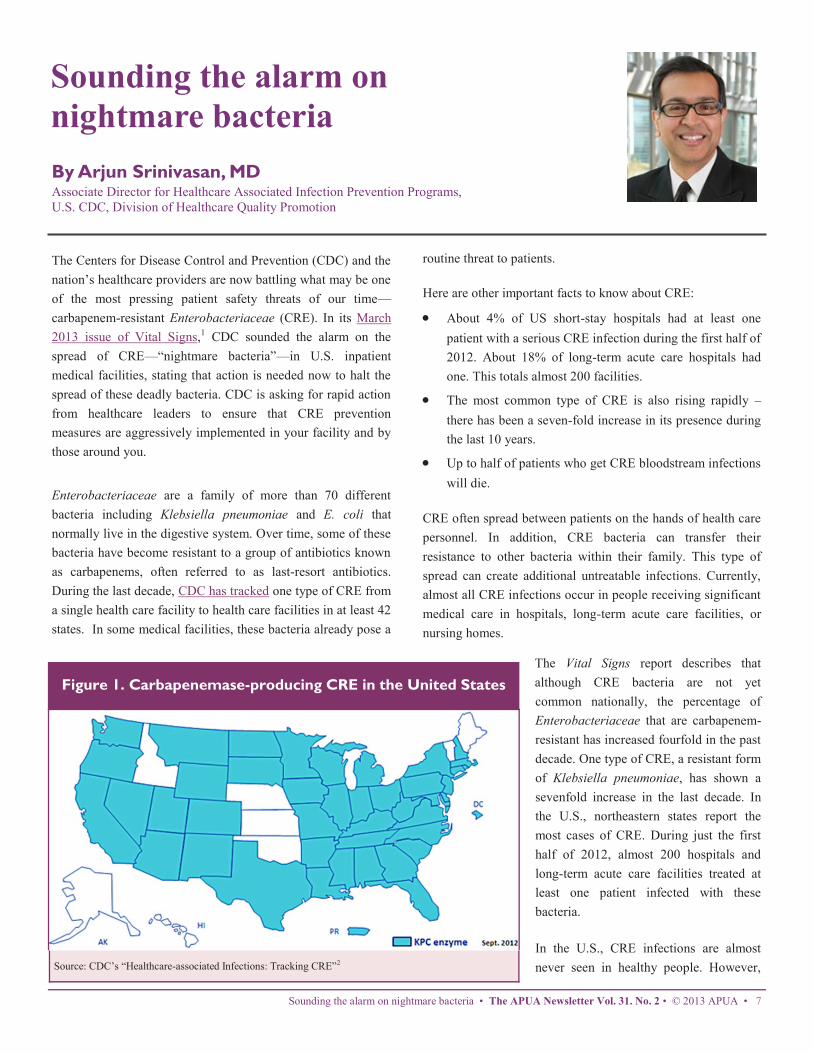
The Vital Signs report describes that
although CRE bacteria are not yet
common nationally, the percentage of
Enterobacteriaceae that are carbapenem-
resistant has increased fourfold in the past
decade. One type of CRE, a resistant form
of Klebsiella pneumoniae, has shown a
sevenfold increase in the last decade. In
the U.S., northeastern states report the
most cases of CRE. During just the first
half of 2012, almost 200 hospitals and
long-term acute care facilities treated at
least one patient infected with these
bacteria.
In the U.S., CRE infections are almost
never seen in healthy people. However,
Sounding the alarm on nightmare bacteria • The APUA Newsletter Vol. 31. No. 2 • © 2013 APUA • 7
Source: CDC’s “Healthcare-associated Infections: Tracking CRE”2
Figure 1. Carbapenemase-producing CRE in the United States

CRE’s ability to spread among people, coupled with their
ability to transfer resistance to other bacteria, raises the worry
that potentially untreatable infections could appear in otherwise
healthy people.
So how do we stop the rise of these deadly, resistant CRE
germs? Halting the rise of CRE will take a combination of
infection control measures and improved antibiotic use. CRE
have shown a propensity to spread quickly in healthcare
facilities and hence aggressive measures to find cases and apply
appropriate infection control measures are essential. But
infection control is only half the battle—we also have to focus
on antibiotic use. One study demonstrated that exposure to a
carbapenem increased a patient’s risk of developing CRE by
more than 15-fold. Reducing unnecessary use of antibiotics like
carbapenems could help slow the emergence of these deadly
bacteria. In 2012, CDC released a concise, practical CRE
prevention toolkit with recommendations for healthcare and
public health for controlling CRE transmission in hospitals,
long-term acute care facilities and nursing homes.
Key recommendations include:
enforcing use of infection control precautions (standard
and contact precautions)
grouping patients with CRE together
dedicating rooms, staff, and equipment to the care of
patients with CRE whenever possible
having facilities alert each other when patients with CRE
transfer back and forth
8 • The APUA Newsletter Vol. 31. No. 2 • © 2013 APUA • Srinivasan
Figure 2.
CDC encourages all healthcare providers to:
Know if patients with CRE are hospitalized at your
facility, and stay aware of CRE infection rates. Ask if your
patients have received medical care somewhere else,
including another country.
Follow infection control recommendations with every
patient, using contact precautions for patients with CRE.
Whenever possible, dedicate rooms, equipment, and staff
to CRE patients.
Prescribe antibiotics wisely. Use culture results to modify
prescriptions if needed.
Remove temporary medical devices as soon as possible.
CDC also encourages patients to:
Tell your doctor if you have been hospitalized in another
facility or country.
Take antibiotics only as prescribed.
Insist that everyone wash their hands before touching you.
If rapid action is not taken today, we will miss our window of
opportunity, and CRE could become widespread across the
country. Let’s act now to protect patients from healthcare-
associated infections, including CRE.
For additional information on CRE, click here.
References
1. Centers for Disease Control. “Stop
Infections from Lethal CRE Germs
Now.” CDC Vital Signs Report. 2013.
2. Centers for Disease Control.
“Healthcare-associated Infections:
Carbapenamase producing CRE in the
United States.” 2012. http://
www.cdc.gov/hai/organisms/cre/
TrackingCRE.html.
3. Centers for Disease Control. “Risk
of CRE Infections.” CDC Vital Signs
Report. 2013.
asking patients whether they have recently received care
somewhere else (including another country)
using antibiotics wisely
When implemented fully, CDC recommendations have been
proven to work. Medical facilities in several states have
reduced CRE infection rates and halted CRE outbreaks by
following CDC’s prevention guidelines.
The U.S. is at a critical point in its ability to stop the spread of
CRE. These infections can be controlled if rapid, coordinated,
and consistent facility and regional efforts are implemented by
doctors, nurses, lab staff, medical facility leadership, health
departments/states, policymakers and the federal government.
Currently, the Federal Government is:
Monitoring the presence of, and risk factors for CRE
infections through the National Healthcare Safety Network
(NHSN) and Emerging Infections Program (EIP).
Providing CRE outbreak support such as staff expertise,
prevention guidelines, tools, and lab testing to states and
facilities.
Developing detection methods and prevention programs to
control CRE. CDC's "Detect and Protect" effort supports
regional CRE programs.
Helping medical facilities improve antibiotic prescribing
practices.
Sounding the alarm on nightmare bacteria • The APUA Newsletter Vol. 31. No. 2 • © 2013 APUA • 9

Therapeutic approaches to carbapenem-
producing Enterobacteriaceae: a brief update
Gabriel Levy Hara, MD
Infectious Diseases Unit, Hospital Durand, Buenos Aires, Argentina
Carbapenems are one of few available last-resort therapeutics
for the treatment of serious infections caused by the
Enterobacteriaceae and by gram-negative non-fermenting rods
(GNB). Regrettably, in recent years, the prevalence of
carbapenemase-producing Enterobacteriaceae (CPE) has
increased rapidly in most parts of the world, leaving the
medical profession—and their patients—with limited, if any,
therapeutic options.
Classification of carbapenemases
These enzymes are encoded by bla genes carried on plasmids
and/or integrons that could easily disseminate among different
gram-negative species. Classes A, B, and D are the most
important carbapenemases.
Class A
Within the diversity of Class A enzymes, the KPC-types
(Klebsiella pneumoniae carbapenemases) are the most
frequently identified among clinical isolates. While often
present in Klebsiella pneumoniae, KPC can also be found in
other Enterobacteriaceae, as well as the non-fermenting GNB.
They are generally broadly active against all β-lactam
antibiotics, despite the fact that organisms containing them may
test susceptible to many carbapenems (with the exception of
ertapenem) by standard antimicrobial susceptibility tests
(ASTs).
Class B
Metallo-beta-lactamases (MBLs) are mostly VIM- and IMP-
types. However, the most recent to appear, the NDM-type, is
currently the most dangerous, both because of the high-level of
carbapenem resistance typically exhibited among
Enterobacteriaceae harboring this enzyme (e.g., MICs for
imipenem and meropenem are ≥32 mg/L), and because of its
rapid worldwide dissemination.
Class D
These enzymes are usually OXA-48-like producers. Their
recognition can be difficult because they exhibit no resistance
to broad-spectrum cephalosporins and only decreased
susceptibility to carbapenems. In such a case, the
microbiologist must be aware that Enterobacteriaceae (mainly
E. coli producing OXA-48-like enzymes only, and not co-
possessing ESBLs) demonstrate low MIC values for imipenem
and meropenem (e.g, 0.25-1 mg/L) and exhibit susceptibility to
the extended-spectrum cephalosporins.
Detection of carbapenemase-producers
As noted above, the detection of CPE can be difficult because
their MIC values do not always reflect resistance. This is a
concern, both in terms of early detection and adoption of
infection control measures, as well as for early prescription of
effective antibiotic therapy. CPE can be suspected based on
antimicrobial susceptibility test (AST) results obtained by
diffusion methods or by automated systems by paying close
attention to the MICs or inhibition diameters for carbapenems.
Reference methods, such as broth microdilution and agar
dilution, are preferred, since these are more sensitive than disk
diffusion, Etest, and automated methods. Susceptibility to
ertapenem can be used for the initial screening of
carbapenemase production. When possible, more appropriate
phenotypic (e.g., modified Hodge test) and molecular methods
(e.g., PCR-based or microarray) should be utilized for
confirming the presence of resistance enzymes.
Antimicrobial treatment options
Optimal treatment for CPE infections is not well established, as
most published reports have evaluated only a few patients,
retrospectively. Nonetheless, rapidly growing evidence
suggests that combined therapy can significantly reduce
mortality in severe infections. Considering the different
susceptibilities to potentially effective drugs, it is essential to
choose an antibiotic based on the AST results for each and
every specific clinical situation. Patients who are colonized
only, and who demonstrate no clinical infection, should not be
treated, and current practices for prevention of dissemination of
CPE (e.g., isolation, hand hygiene, etc) should be strictly
observed.
10 • The APUA Newsletter Vol. 31. No. 2 • © 2013 APUA • Levy Hara

The following drugs are potentially useful for CPE treatment:
Colistin
Colistin is frequently the only agent to achieve adequate serum
levels for treatment of CPE bloodstream infections (BSIs).
Globally, the sensitivity of GNB to colistin varies from 70% to
100%. Regrettably, in some countries and in certain city
hospitals, resistance is increasing due to the clonal spread of
strains. The emergence of multi drug-resistant (MDR) and
extreme drug-resistant (XDR) pathogens has led to a
significant increase in utilization of colistin—a formerly
uncommon drug. While our knowledge of the PK/PD issues of
colistin has improved, it is not yet fully established.
To avoid confusion related to different formulations, it should
be noted that 100 mg of
colistin sulfate base is
equivalent to 240 mg of
colistin methanesulfonate
(CMS) and to 3 million
units (MU) of CMS (the
non-active pro-drug of
colistin). Current dosing
schemes (commonly, 3
MU of CMS every 8h)
reach only suboptimal
concentrations—i.e., below the MIC breakpoint of 2 mg/liter—
at least during the critical first 2 to 3 days of therapy.1,2 These
levels can greatly increase mortality in critically ill patients, as
well as promote selection of resistant strains. In one study, a 20
-fold difference in the AUC0-24* between patients was
observed.2 Creatinine clearance was an important covariate in
the population PK model applied. Recent studies showed that a
loading dose of 6 to 9 MU, followed by maintenance doses of
4.5 to 6 MU every 12h—always adjusting to renal function—
could be more effective than previously prescribed regimens of
3 MU every 8h, without an increase of nephrotoxicity.2-4 In
different studies, nephrotoxicity varied from 10%-15% and, in
most cases, was transient and probably related to dosage and
duration of treatment. A recent survey of the use of colistin
showed that barely 21.2% of institutions worldwide are
currently using loading doses.
Tigecycline
The clinical use of this glycylcycline, a bacteriostatic agent, is
limited for several reasons. First, a scarcity of controlled
studies demonstrate its efficacy in the treatment of infections
due to MDR and XDR bacteria. Secondly, the PK/PD profile of
tigecycline suggests that it is not appropriate for treatment—at
least as monotherapy—of serious disease. Its protein binding
is 71 - 89%, and with a standard dosing regimen of 50 mg bid,
the peak serum concentrations range from 0.6 - 0.9 mg/l. In
contrast, the MICs for the majority of KPC-producing K.
pneumoniae isolates range between 1 to 2 mg/L. Higher doses
are badly tolerated due to gastrointestinal toxicity (e.g., nausea
and vomiting). Finally, there is a concern regarding the
development of resistance via upregulation of cellular efflux
pumps during therapy. However, as discussed below, there is
some good evidence for the efficacy of tigecycline in
combination with colistin and carbapenems in the treatment of
severely ill patients.
Aminoglycosides
Resistance to this class is increasing
among CPE. In the regrettably few
infections produced by susceptible
strains, these drugs have been
efficacious options as part of
combined therapeutic regimens.
Fosfomycin
Like colistin, this older drug has been
revitalized for the treatment of some
MDR and XDR GNB, and displays in vitro activity against
many CPE, including colistin-resistant strains. Some reports
suggest that fosfomycin should always be used in high doses
(e.g., 4 grams, 4X/day in a normal renal functioning patient)
and in combination regimens (see below).
Combination therapy
Recently published evidence supports the use of combination
therapy in patients with CPE infections. Tzouvelekis et. al.
performed a systematic search to evaluate the efficacy of
different treatment approaches.6 Among 34 small studies, a
total of 298 patients were identified: 244 with blood stream
infections (BSIs), and 32 with pneumonia. One hundred and
forty three patients received monotherapy (only one drug was
active in vitro against the infecting organism); 99 received
combination therapy (at least two drugs active in vitro), and the
remaining 56 received inappropriate therapy (no drug active in
vitro). Combination therapy was superior to monotherapy, and
those patients treated with carbapenems as part of the regimen
had the lowest failure rate (8.3%). In contrast, treatment with
tigecycline or colistin as single active agents resulted in failure
rates (35.7% and 47.2%, respectively) comparable to that
observed for patients improperly treated (45%). Combinations *Area Under the serum Concentration curve over a day
“Patients who are colonized only, and who
demonstrate no clinical infection, should
not be treated, and current practices for
prevention of dissemination of CPE
(isolation, hand hygiene, etc.) should be
strictly observed.”
Therapeutic approaches • The APUA Newsletter Vol. 31. No. 2• © 2013 • APUA • 11

12 • The APUA Newsletter Vol. 31. No. 2 • © 2013 APUA • Levy Hara
of carbapenem plus colistin (5.5% of failures) or carbapenem
plus an aminoglycoside (6.2%) exhibited better outcomes than
when these drugs were used alone or as part of other
combinations. Finally, combinations of tigecycline (24% of
failures), colistin (32%), and aminoglycosides (33.3%) in
regimens not including a carbapenem, exhibited higher failure
rates.
A recently published multicenter retrospective cohort study of
125 patients with BSIs caused by KPC-K. pneumoniae also
showed higher mortality rates in patients treated with
monotherapy (54.3% vs. 34.1% with combined drug therapy; P
= 0.02). Combination therapy with tigecycline, colistin, and
meropenem was independently associated with survival (OR:
0.11; 95% CI: .02–.69; P = 0.01). With MIC values of ≤4 mg/l
for meropenem, inclusion of this drug in a combined regimen
led to a survival rate of 86.6%, and with even higher MIC
values, the survival rate was 75%.7
Carbapenems display time-dependent bactericidal killing when
free drug concentrations remain above the MIC for 40–50% of
the time between doses. The probability of attaining 50%
T>MIC* target for an isolate with a MIC of 4 mg/l is 69% for
the traditional dosing regimen (e.g., 30 min infusion of 1g
every 8 hours for meropenem) and increases to 100% for the
high-dose/prolonged infusion regimen (e.g., 3 hour infusion of
2g every 8 hours for meropenem). Even for an MIC of 8 mg/l,
the high-dose/prolonged-infusion carries a high probability
(85%) of bactericidal activity.8
In the February 2013 issue of the Journal of Chemotherapy, an
International Working Group** published some pivotal
recommendations for the detection, treatment and prevention of
CPE.9 For all the above reasons, the recommendations of this
Working Group support the use of carbapenems, provided that:
the carbapenem MIC for the infecting organism is >4 mg/l
(and possibly up to 8 mg/l)
a high-dose, prolonged-infusion regimen is administered
(e.g. 2g meropenem every 8h, or 1g imipenem every 6-8h)
they are used in combination with another active
compound, preferably colistin or an aminoglycoside.
Considering the deficit of new drugs on the near horizon, our
most immediate option for preventing more deaths from CPE
will be the enforcement of infection control practices combined
with diligent antimicrobial stewardship.
*(Time above MIC) = the percentage of a dosage interval in which the
serum level exceeds the minimal inhibitory concentration.
**This group included representatives from the Argentinian Society of
Infectious Diseases (SADI), the International Society of
Chemotherapy (ISC), the Pan American Association of Infectious
Diseases (API), the Pan American Health Organization/World Health
Organization (PAHO/WHO), the Infection Control African Network
(ICAN), Mediterranean Society of Chemotherapy (MSC) and the
Federation of European Societies for Chemotherapy and for Infections
(FESCI). This article briefly summarizes the key points of their
recommendations.
References
1. Plachouras D, Karvanen M, Friberg L, Papadomichelakis E,
Antoniadou A, Tsangaris I et al. Population pharmacokinetic
analysis of colistin methanesulfonate and colistin after
intravenous administration in critically ill patients with infections
caused by Gram-negative bacteria. Antimicrob Agents
Chemother 2009; 53: 3430-6.
2. Garonzik SM, Li J, Thamlikitkul V, Paterson DL, Shoham S,
Jacob J, Silveira FP, et al. Population pharmacokinetics of
colistin methanesulfonate and formed colistin in critically ill
patients from a multicenter study provide dosing suggestions for
various categories of patients. Antimicrob Agents Chemother
2011; 55: 3284-94.
3. Dalfino L, Puntillo F, Mosca A, Monno R, Spada ML,
Coppolecchia S et al. High-dose, extended-interval colistin
administration in critically ill patients: is this the right dosing
strategy? A preliminary study. Clin Infect Dis. 2012; 54:1720-6.
4. Pogue JM, Lee J, Marchaim D, Yee V, Zhao JJ, Chopra T et al.
Incidence of and risk factors for colistin-associated
nephrotoxicity in a large academic health system. Clin Infect Dis
2011; 53:879-84.
5. Wertheim H, Van Nguyen K, Levy Hara G, Gelband H,
Laxminarayan R, Mouton J, Cars O. Global survey of polymyxin
use: A call for international guidelines. J Global Antimicrob
Resist (2013) in press, http://dx.doi.org/10.1016/
j.jgar.2013.03.012.
6. Tzouvelekis LS, Markogiannakis AM, Psichogiou PT, Tassios
PT, Daikos GL. Carbapenemases in Klebsiella pneumoniae and
other Enterobacteriaceae: an evolving crisis of global
dimensions. Clin Microbiol Rev; 25: 682-707.
7. Tumbarello M, Viale P, Viscoli C, Trecarichi EM, Tumietto F,
Marchese A et al. Predictors of mortality in bloodstream
infections caused by Klebsiella pneumoniae carbapenemase-
producing K. pneumoniae: Importance of combination therapy.
Clin Infect Dis 2012; 55:943-50.
8. Akova M, Daikos GL, Tzouvelekis L, Carmeli Y. Interventional
strategies and current clinical experience with carbapenemase-
producing Gram-negative bacteria. Clin Microbiol Infect 2012;
18: 439–448.
9. Levy Hara G, Gould I, Endimiani A, Ramón Pardo P, Daikos G,
Hsueh PR, et al. Detection, treatment and prevention of
carbapenemase-producing Enterobacteriaceae: Recom-
mendations from an International Working Group. J Chemother
2013; 25: 129-140.

In a population-based study from Olmsted County, Minnesota
between 1991-2005, 41% of all CDI cases were community-
acquired, 50% were hospital-acquired, and 9% were nursing
home-acquired.5 In accordance with the existing literature, the
majority of cases (53%) occurred in the elderly (age ≥65
years). The overall age- and sex-adjusted incidence of CDI was
25.2 per 100,000 person-years and there was a significant
increase in both hospital-acquired (19.3-fold) and community-
acquired (5.3-fold) cases over the study period.5
In this study, patients with community-acquired CDI were
younger, had fewer co-morbid conditions, were less likely to
have an underlying malignancy, and were less likely to develop
severe disease. Interestingly, of all CDI patients, 13% had no
documented antibiotic exposure in the preceding 90 days.
Compared to hospital-acquired CDI patients, those with
community-acquired CDI were
significantly less likely to be exposed to
antibiotics (94% vs. 78%) or gastric acid
suppression medications (47% vs. 22%).5
CDI cases were predominantly female
(75.3%); one-fifth had severe CDI; 20%
had treatment failure and a significant
proportion required hospitalization for
CDI. Community-acquired CDI patients
who required hospitalization were
significantly older (median age difference 20 years), had more
comorbid conditions and were more likely to have severe CDI.6
Within the pediatric population of Olmsted County (1991 -
2009), the majority of cases (75%) were community-acquired.
The overall age and sex-adjusted CDI incidence was 13.8 per
100,000 persons, which increased 12.5-fold over the study
period. The incidence of community-acquired CDI was 10.3
per 100,000 persons and increased 10.5-fold over the study
period.7 Of all community-acquired cases, 85.5% had an
outpatient or an emergency-department visit in the three
months prior to onset of CDI. Severe, severe-complicated, and
recurrent CDI occurred in 9%, 3%, and 20% respectively.
Community-acquired C. difficile
infection—old bug, new insights
Sahil Khanna, MBBS, MS
Mayo Clinic, Rochester, Minnesota
Clostridium difficile infection (CDI) is the most common
hospital-acquired infection and the most common cause of
infection diarrhea in the hospital—with ~500,000 - 1,000,000
infections and ~14,000 deaths annually in the United States.1, 2
While the traditional risk factors for CDI include increasing
age, antibiotic exposure and hospitalization, recent data have
shown that CDI is also present in the community—in patients
who may lack these traditional risk factors.2
According to guidelines from the Infectious Diseases Society
of America, CDI is defined as “hospital-acquired” if symptom
onset occurs more than 48 hours after admission to, or less than
4 weeks after discharge from, a
health care facility.3 CDI is
considered “community-acquired”
if symptom onset occurs in the
community or within 48 hours of
admission to a hospital, provided
that symptom onset was more
than 12 weeks after the last
discharge from a hospital. CDI is
defined as “indeterminate” if symptom onset occurs between 4
and 12 weeks following a hospital dismissal.3
Community-acquired CDI is probably an under-diagnosed and
under-recognized sub-group of patients—likely due to a lack
of awareness of the existence of CDI outside the healthcare
setting. Studies have shown that the proportion of community-
acquired CDI ranges from 27 - 41% in adults and up to 75% in
pediatric patients.2,4 CA-CDI has been described in populations
previously considered to be at low risk, including peri-partum
women, children and young adults.4 Many of these patients
lack traditional risk factors for CDI, such as antibiotic exposure
or recent hospitalization.5
Community-acquired C. difficile • The APUA Newsletter Vol. 31. No. 2 • © 2013 APUA • 13
This article is a follow-up to APUA’s April 2013
Newsletter on C. difficile infections in healthcare
institutions. For important new updates on C. difficile
management, see page 26.
“...Up to one-third of households
and half of water and swimming
pool samples may be contam-
inated with C. difficile.”

There were fewer treatment failures in those treated with
vancomycin compared to metronidazole.7
The lack of traditional risk factors in a subset of patients with
community-acquired CDI suggests alternate novel risk factors
for CDI and newer modes of transmission in the community.
Studies have suggested that up to 94% of patients may have had
health-care exposure predisposing them to CDI.8 Potential risk
factors for community-acquired CDI include contaminated food
consumption, and personal contact (person-to-person,
environment-to-person, and potentially animal-to-person. C.
difficile strains have been identified in retail meat and meat
products, including beef, chicken and pork. Similarities have
been reported in animal feed isolates with those reported to
cause CDI in
humans.9, 10
Person-to-person
spread is important
both within and
outside hospitals.
Recently published
guidelines have
suggested that
visitors to hospital
rooms harboring CDI patients should practice the same
isolation precautions as healthcare personnel.11 Additionally,
there is a potential for increased exposure to colonized or
infected persons in the community, such as health care workers,
and studies have shown that family members of patients with
recent infection have a higher risk of CDI.12 Infants and
children may be asymptomatically colonized with C. difficile,
and exposure to a colonized infant may be a risk factor for
recurrent CDI in mothers in the post-natal period.
Environmental contamination has been found in daycare
centers, and up to one-third of households and half of water and
swimming pool samples may be contaminated with C.
difficile.12 In these settings, strict hand hygiene precautions with
soap and water (not alcohol-based hand rubs) is the cornerstone
to the prevention of CDI.3, 11
As the incidence of community-acquired CDI increases, CDI
should be considered in all outpatients with acute diarrhea, even
in the absence of traditional risk factors such as hospitalization
or antibiotic exposure. A majority of patients, however, have
some form of healthcare exposure, which suggests that
outpatient and emergency room visits may also place patients at
a higher risk for CDI. Additionally, community-acquired CDI
may have serious consequences. Given the additional risks and
costs associated with hospitalization, physicians should be
aware of risk factors (increasing age, comorbid conditions and
disease severity) that predict the need for hospitalization.
Patients with community-acquired CDI should be managed
aggressively, with close clinical follow-up to prevent adverse
outcomes.6
References
1. Khanna S, Pardi DS. Clostridium difficile Infection: New Insights
Into Management. Mayo Clin Proc 2012; 87: 1106-1117.
2. Khanna S, Pardi DS. The growing incidence and severity of
Clostridium difficile infection in inpatient and outpatient settings.
Expert Rev Gastroenterol Hepatol 2010; 4: 409-416.
3. Cohen SH, Gerding DN, Johnson
S, et al. Clinical practice guidelines for
Clostridium difficile infection in adults:
2010 update by the Society for
Healthcare Epidemiology of America
(SHEA) and the Infectious Diseases
Society of America (IDSA). Infect
Control Hosp Epidemiol 2010; 31: 431-
455.
4. Centers for Disease Control and
Prevention. Severe Clostridium difficile-
associated disease in populations
previously at low risk--four states, 2005.
MMWR 2005; 54: 1201-1205.
5. Khanna S, Pardi DS, Aronson SL, et al. The Epidemiology of
Community-Acquired Clostridium difficile Infection: A
Population-Based Study. Am J Gastroenterol 2012; 107: 89-95.
6. Khanna S, Pardi DS, Aronson SL, Kammer PP, Baddour LM.
Outcomes in community-acquired Clostridium difficile infection.
Aliment Pharmacol Ther 2012; 35: 613-618.
7. Khanna S, Baddour LM, Huskins WC, et al. The Epidemiology of
Clostridium difficile Infection in Children: A Population-based
Study. Clin Infect Dis 2013; 56: 1401-1406.
8. Centers for Disease Control and Prevention. Vital signs:
preventing Clostridium difficile infections. MMWR 2012; 61: 157-
162.
9. Jhung MA, Thompson AD, Killgore GE, et al. Toxinotype V
Clostridium difficile in humans and food animals. Emerg Infect
Dis 2008; 14: 1039-1045.
10. Weese JS, Reid-Smith RJ, Avery BP, Rousseau J. Detection and
characterization of Clostridium difficile in retail chicken. Lett
Appl Microbiol 2010; 50: 362-365.
11. Surawicz CM, Brandt LJ, Binion DG, et al. Guidelines for
diagnosis, treatment, and prevention of Clostridium difficile
infections. Am J Gastroenterol 2013; 108: 478-498; quiz 499.
12. Otten AM, Reid-Smith RJ, Fazil A, Weese JS. Disease
transmission model for community-associated Clostridium
difficile infection. Epidemiol Infect 2010; 138: 907-914.
14 • The APUA Newsletter Vol. 31. No. 2 • © 2013 APUA • Khanna
“As the incidence of community-acquired CDI
increases, CDI should be considered in all out-
patients with acute diarrhea, even in the
absence of traditional risk factors such as
hospitalization or antibiotic exposure.”

Plasmids believed to be responsible for the dissemination of
ESBLs are largely members of the IncF replicon/
incompatibility group6 and parallels the pattern observed
worldwide for CTX-M-15-carrying plasmids,7-9 as well as the
spread of plasmid-mediated ampC genes (blaCMY and
blaDHA).10,11 Nigerian ampC strains demonstrate low-level re-
sistance to third-generation cephalosporins, but are associated
with high-level resistance to quinolones. The blaCTX-M genes
are associated with plasmids that also carry other resistance
genes: the tet(A) gene, aminoglycoside resistance genes (aac
(3)II and aac(6’)-Ib4),
and PMQR (plasmid-
mediated quinolone re-
sistance qnr genes, aac
(6’)-Ib-cr), and the efflux
pump gene, qepA.1
Carbapenems have re-
cently been introduced to
patient management in
Nigeria, but are rarely used by physicians, due largely to high
cost. We previously (in 2009) found extremely high levels of
resistance to all antibiotics tested and the presence of numerous
mobile genetic elements carrying resistance to ß-lactams.6
While the focus of the study was on ESBL resistance, we did
identify potential carbapenem resistance, indicating a reservoir
of carbapenem-resistant strains. Most recently, we have found
high-level carbapenemase production in gram-negative clinical
isolates, with carriage of various known carbapenemases and
potential for variants of existing carbapenemases or unknown
carbapenemase (submitted). It is surprising that such a number
of highly carbapenem-resistant isolates were observed, of
which more than half were carbapenemase-producers and pan-
drug resistant.
ESBLs have been detected not only in clinical isolates, but also
in commensal bacteria from humans and animals in Nigeria
and in isolates from products of the food chain and sewage,
demonstrating a variety of sources and reservoirs for these re-
APUA Field Report: Nigeria • The APUA Newsletter Vol. 31. No. 2 • © 2013 APUA • 15
The distribution and epidemiology of extended-spectrum beta-
lactamases (ESBLs) in various pathogens have been intensively
studied in developed countries, but data are extremely limited
from sub-Saharan Africa, including Nigeria. Antibiotic use in
Nigeria is unregulated; there are no regional or national surveil-
lance data on bacterial resistance to antibiotics, and only a few
localized institutional studies have reported the prevalence or
level of antibiotic resistance, particularly to β-lactams. In Nige-
ria, extended-spectrum cephalosporins and fluoroquinolones
are widely used as broad-spectrum antibiotics and remain the
drugs of choice to treat
infections caused by var-
ious gram-negative path-
ogens.1 Gram-negative
bacteria cause a signifi-
cant number of infections
in Nigerian hospitals and
represent the majority of
both wound and urinary
isolates, which form the
largest group of clinical specimens received in microbiology
laboratories.
A diversity of ESBL enzymes have evolved and been detected
in gram-negative pathogens over the last 30 years, with the
CTX-M group becoming the dominant ESBL identified world-
wide.2 In Nigeria, Aibinu et al.3 reported 20% carriage of
ESBLs in Enterobacter species in the capitol, Lagos—a rate
similar to that found in gram-negatives from four teaching hos-
pitals of the southwest region.1 The predominant ESBL geno-
type detected is CTX-M-15.4,5 CTX-M-3 was also reported in
2011 with TEM, SHV and OXA variants. Plasmidic or chro-
mosomal ampC genes (ACT-1, DHA-1 and CMY-2) have also
been identified, co-existing with ESBL genes such as CTX-M-
15, TEM-1, SHV-1 and OXA-1.1 Additionally, other plasmid-
mediated β-lactamases (VEB-1, OXA-10) have been found in
Providencia species, although they are believed to be less com-
mon.12 It remains to be seen whether they are of clinical signif-
icance in other genera of Enterobacteriaceae.
Impact of ESBLs and CREs—the
Nigerian Experience
David Olusoga Ogbolu, PhD, FMLSCN Ladoke Akintola University of Technology, Ogbomosho, Nigeria
“There is high-level resistance to many antimicrobials,
including cephalosporins and carbapenems, among
Enterobacteriaceae in Nigeria. This has led to
increased and widespread use of reserved antibiotics
such as carbapenems, with consequent ineffectiveness
and escalation to pan-drug resistance.”
7. Coque TM, Novias A, Carattoli A, Poirel L, Pitout J, Peixe L,
Baquero F, Canton R, Nordmann P. Dissemination of clonally
related Escherichia coli strains expressing extended-spectrum β-
lactamase CTX-M-15. Emerging Infectious Diseases 2008; 14:
195-200.
8. Marcade G, Deschamps C, Boyd A, Gautier V, Picard B, Branger
C, Denamur E, Arlet G. Replicon typing of plasmids in Esche-
richia coli producing extended-spectrum β-lactamases. J Antimi-
crob Chemother 2009; 63: 67-71.
9. Villa L, Garcia-Fernandez A, Fortini D, Carattoli A. Replicon
sequence typing of IncF plasmids carrying virulence and re-
sistance determinants. J Antimicrob Chemother 2010; 65: 2518-
2529.
10. Leflon-Guibout V, Blanco J, Amaqdouf K, Mora A, Guize L,
Nicolas-Chanoine M-H. Absence of CTX-M enzymes but a high
prevalence of clones, including clone ST131, among the faecal
Escherichia coli isolates of healthy subjects living in the Paris
area. J Clin Microbiol 2008; 46: 3900-3905.
11. Carattoli A. Resistance plasmid families in Enterobacteriaceae.
Antimicrob Agents Chemother 2009; 53: 2227-2238.
12. Aibinu I, Pfeifer Y, Ogunsola F, Odugbemi T, Koenig W, Ghe-
bremedhin B. Emergence of beta-lactamases OXA-10, VEB-1
and CMY in Providencia spp. from Nigeria. J Antimicrob
Chemother 2011; 66: 1931–1932.
13. Ogbolu D. Olusoga, Alli OA Terry, Olanipekun LB, Ojo OI,
Makinde OO. Faecal carriage of extended-spectrum beta-
lactamase (ESBL)-producing commensal Klebsiella pneumoniae
and Escherichia coli from hospital out-patients in southern Nige-
ria. Int J Med Med Sci 2013; 5(3): 97-105.
14. Fortini D, Fashae K, Garcia-Fernandez A, Villa L, Carattoli A.
Plasmid-mediated quinolone resistance and ß-lactamases in Esch-
erichia coli from healthy animals from Nigeria. J Antimicrob
Chemother 2011; 66: 1269-1272.
16 • The APUA Newsletter Vol. 31. No. 2 • © 2013 APUA • Ogbolu
sistance determinants. In humans, carriage of ESBL genes in
fecal isolates of commensal E. coli and Klebsiella species in
out-patients revealed carriage of blaCTX-M-15, blaCTX-M-2, blaOXA-
1, blaTEM-1 and bla SHV-1, including non-chromosomal AmpC
enzymes. These blaampC genes were found in isolates carrying
other ESBL genes, as commonly reported in bacterial patho-
gens.13 Similarly, ampicillin-resistant commensal E. coli iso-
lated from healthy chickens and pigs have been found to har-
bour blaTEM and blaCTX-M-15 genes.14 These ESBL-producing
bacteria can enter the human food chain through the consump-
tion of meat or by direct contact, colonizing the human gut.
In conclusion, there is a diversity of beta-lactamases and high-
level resistance to many antimicrobials, including cephalospor-
ins and carbapenems among Enterobacteriaceae in Nigeria.
This has led to increased and widespread use of reserved anti-
biotics such as carbapenems, with consequent ineffectiveness
and escalation to pan-drug resistance. The uncontrolled use of
antibiotics in Nigeria is likely to have contributed largely to
this situation. In an era of frequent global travel, the selection
of highly resistant isolates in countries such as Nigeria, where ß
-lactamases are not routinely identified, may elicit a reservoir
of resistant strains with high mobility for export to other coun-
tries.
References
1. Ogbolu DO, Daini OA, Ogunledun A, Alli AO and Webber MA.
High levels of multidrug resistance in clinical isolates of Gram-
negative pathogens from Nigeria. Int J Antimicrob Agents 2011;
37: 62-66.
2. Livermore D, Canton R, Gniadkowski M et al. CTX-M: changing
the face of ESBLs in Europe. J Antimicrob Chemother 2007; 59:
165–174.
3. Aibinu IE, Ohaegbulam VC, Adenipekun EA, Ogunsola FT,
Odugbemi TO, Mee BJ. Extended-spectrum beta-lactamase en-
zymes in clinical isolates of Enterobacter species from Lagos,
Nigeria. J Clin Microbiol 2003; 41: 2197-2200.
4. Soge OO, Queenan AM, Ojo KK, Adeniyi BA, Roberts MC.
CTX-M-15 extended-spectrum beta-lactamase from Nigerian
Klebsiella pneumoniae. J Antimicrob Chemother 2006; 57: 24-
30.
5. Olowe OA, Grobbel M, Buchter B, Lubke-Becker A, fruth A,
Wieler LU. Detection of bla CTX-M-15 extended-spectrum β-
lactamase genes in Escherichia coli from hospital patients in
Nigeria. Int J Antimicrob Agents 2010; 35: 200–209.
6. Ogbolu DO, Daini OA, Ogunledun A et al. Dissemination of
IncF plasmids carrying beta-lactamase genes in Gram-negative
bacteria from Nigerian hospitals. J Infect Dev Ctries 2013; 7(5):
382-390.

ESBL-producing Enterobacteriaceae
in Bulgaria – a short overview
Rumyana Markovska, APUA-Bulgaria Medical University—Sofia, Bulgaria
Emma Keuleyan, APUA-Bulgaria Medical Institute—Ministry of the Interior
Since the first report of an ESBL-producing microorganism in
Bulgaria in 1992,1 the national data tracking system
(BulSTAR) has recorded increases from 1 - 5.7% for ESBL-
producing Escherichia coli and from 5 - 22.5% for ESBL-
producing Klebsiella pneumoniae (2001-2010).2 These rates
are lower than those for Bulgaria in the European
Antimicrobial Resistance Surveillance System (EARSS) which
reported increases from 7 - 22.9% in E. coli (mostly from
bacteremia resistant to oxyimino-cephalosporins; 2001-2011)
and from 50 - 81% (also invasive isolates; 2005-2011) in K.
pneumoniae.3, 4 Early studies among different enterobacteria
between 1994 and 1999 at the National Cancer Centre reported
ESBL production at 4.4% and detected enzymes of the SHV
and TEM families.5
The APUA-funded small grants program project on
Antimicrobial Resistance Surveillance (1999–2000) confirmed
an emerging problem.6 Beta-lactamases TEM-3, SHV-5, SHV-
12 were detected among nosocomial strains of K. pneumoniae
isolated in 1999 in Military Medical Academy.7 The wide
investigation of 451 different enterobacteria (K. pneumoniae,
E. coli, Enterobacter spp., Serratia marcescens, Citrobacter
freundii, K. oxytoca, Salmonella enterica serotype Corvallis 1)
conducted between 1997 and 2003 has shown a similar
distribution.8 Until 2000, only SHV- and TEM- ESBLs were
detected, with TEM-139 being reported for the first time
globally. It was limited mainly to one city (Pleven) and one
species (K. pneumoniae).8,9 SHV enzymes detected included
SHV-2, -5, and -12. They were found in all centers through the
entire investigation period.8 The first CTX-M enzyme found in
Bulgaria was CTX-M-15, isolated in 2001 (shortly after its first
report in India).10 CTX-M-3 was also detected for the first time
in Bulgaria in 2002.11 CTX-M frequency subsequently
increased to 65% by the end of the investigation period.8 A
novel CTX-M enzyme, CTX-M-71, was first detected in
Bulgaria in 2003.12
The increased rates of ESBL-producing isolates in Bulgaria are
most probably due to the distribution of a few specific clones
or plasmids. Various studies have found a few primary clones:
K. pneumoniae with SHV-12 or CTX-M-3; E.coli with CTX-M
-15; and S. marcescens with CTX-M-3.13-15 Further
investigation demonstrated country-wide dissemination of a
highly resistant B2 O25b-ST131 CTX-M-1- producing E. coli
clone in Bulgaria, representing 68% of all ESBL-producing E.
coli isolates. Almost all O25b-ST131 E. coli produced CTX-M
-15 (96%).13 The important role of horizontal transfer of
plasmids, carrying blaESBL, predominantly blaCTX-M-3, has been
shown as well.8, 16
In conclusion, the wide spread of ESBLs in Bulgaria is
extremely worrying and suggests a need for more prudent
antibiotic prescription, (e.g. limitation of 3rd generation
cephalosporins) and stricter infection control. It is becoming
obvious that the problem of ESBL-producing
Enterobacteriaceae cannot be resolved without the intervention
of strict government controls and the external assistance of
international societies/communities.
References:
1. Keuleyan E, Kaludova V, Marinova R. Comparative
susceptibility to β-lactams and spectra of β-lactamases in clinical
Enterobacteriaceae strains. 4th Biennial Conference on
Chemotherapy of Infectious Diseases and Malignancies, Prague,
Czechoslovakia. 1992. Program and Abstracts, Abstr 217.
2. Velinov Tz, Todorova B, Kantardjiev T. Surveillance of
antimicrobial resistance in infections of hospitalized patients in
Bulgaria: Bulgarian Surveillance Tracking Antimicrobial
Resistance (BulSTAR) 2010. Nosocomial infections. 2011, 1-2:
50-57 (in Bulgarian)
3. EARSS-Net Annual Reports 2008. ECDC /www.ecdc.europa.eu/
en/activities/surveillance/EARS-et/
Documents/2008_EARSS_Annual_Report.pdf/
APUA Field Report: Bulgaria • The APUA Newsletter Vol. 31. No. 2 • © 2013 APUA • 17
R. Markovska E. Keuleyan
4. EARSS-Net Annual Reports 2009-2011. ECDC (http://
www.ecdc.europa.eu/en/healthtopics/antimicrobial
epidemiological_data/Pages/ears-net_annual_reports.aspx).
5. Sabtcheva S. Phenotypic and genotypic characterization of
extended spectrum beta-lactamases with extended spectrum
among Enterobacteriaceae, isolated from cancer patients. PhD
thesis - Sofia, 2003.
6. Keuleyan E, Sredkova M, Ivanova D, Haydoushka I, Markovska
R, Hadjieva N, Strateva T, Mitov I. ESBLs producing
Enterobacteriaceae from APUA Bulgaria Chapter survey. 11th
ECCMID (European Congress of Clinical Microbiology and
Infectious Diseases), Istanbul, Turkey. Clin Microbiol Infect, 7,
2001.Suppl 1, Astr P1343/ p 286.
7. Jacoby G, Vacheva-Dobrevsky R. Epidemiology of Extended
Spectrum Beta-Lactamases in Sofia, Bulgaria. Eur J Clin
Microbiol Infect Dis 2003; 22: 385-388.
8. Markovska R, Schneider I, Keuleyan E, Sredkova M, Ivanova D,
Markova B, Lazarova G, Dragigeva E, Savov E, Haydouchka I,
Hadjieva N, Setchanova L, Mitov I, Bauernfeind A. Extended-
spectrum beta-lactamase-producing Enterobacteriaceae in
Bulgarian hospitals. Microbiol Drug Resist. 2008. 14, 2: 119-28.
9. Schneider I, Markovska R, Keuleyan E, Sredkova M, Rachkova
K, Mitov I, Bauernfeind A. Dissemination and persistence of a
plasmid-mediated TEM-3-like beta-lactamase, TEM-139, among
Enterobacteriaceae in Bulgaria. Int J Antimicrob Agents. 2007;
29 (6): 710-714.
10. Markovska, R., Schneider, I., Keuleyan, E., and Bauernfeind, A.
Extended spectrum beta-lactamase( ESBL) CTX-M-15 producing
E. coli and K. pneumoniae in Sofia, Bulgaria , Clinical
Microbiolody Infection. 2004. 8, 752- 755.
11. Markovska R, Keuleyan E, Schneider I, Markova B, Rachkova
K, Sredkova M, and Bauernfeind A. CTX-M-3 Extended
Spectrum Beta-Lactamase producing K. pneumoniae and
dissemination of the plasmidic blaCTX-M-3 in Bulgaria. Eur. J. Clin.
Microbiol. Infect. Dis. 2006. 25; 123-125.
12. Schneider I, Qeenan AM, Markovska R, Markova B, Keuleyan
E, Bauernfeind A. New Variant of CTX-M-Type Extended-
Spectrum β-Lactamases, CTX-M-71, with Gly238Cys
Substitution in a Klebsiella pneumoniae Isolate from Bulgaria.
Antimicrob Agents Chemother. 2009, 53,10:4518-4521.
13. Markovska R, I Schneider, D Ivanova, E Keuleyan, T Stoeva, M
Sredkova, B Markova, K Bojkova, R Gergova, A Bauernfeind, I
Mitov. High prevalence of CTX-M-15-producing O25b-ST131
Escherichia coli clone in Bulgarian hospitals. Microb Drug
Resist; 2012. 18 (4):390-5.
14. Ivanova D, Markovska R, Hadjieva N, Schneider I, Mitov I ,
Bauernfeind A.Extended-spectrum b-lactamase-producing
Serratia marcescens outbreak in a Bulgarian hospital. J Hosp.
Infect. 2008; 70: 60-65.
15. Ivanova D., R. Markovska, B. Markova, M. Leseva, N. Hadjieva,
E. Zamfirova, Y. Marteva-Proevska, I. Mitov . Complex
molecular epidemiology of ESBL-producing Klebsiella
pneumoniae: long-term persistence and spread of epidemic
clones among Bulgarian hospitals. 22th European Congress of
Clinical Microbiology and Infectious Diseases London UK.
31.03 – 3.04.2012. P 1872.
16. Sabtcheva S, Saga T, Kantardjiev T, Ivanova M, Ishii Y, Kaku
M. Nosocomial spread of armA-mediated high-level
aminoglycoside resistance in Enterobacteriaceae isolates
producing CTX-M-3 beta-lactamase in a cancer hospital in
Bulgaria. J Chemother. 2008. 20 (5):593-9.
18 • The APUA Newsletter Vol. 31. No. 2 • © 2013 APUA • Markovska & Keuleyan
September 10-13, 2013: Interscience Conf. on
Antimicrobial Agents and Chemotherapy (ICAAC
2013), Denver, CO, USA.
September 28, 2013: MRSA Survivors' Network
hosts (5th Annual World MRSA Day Kickoff Event and
the Global MRSA & C. diff Summit), Chjcago, IL, USA.
October 2-6, 2013: Infectious Diseases Society of
America (IDSA), the Society for Healthcare Epi-
demiology of America (SHEA), the HIV Medicine
Association (HIVMA), and the Pediatric Infectious
Diseases Society (PIDS)'s IDWeek 2013, San Francisco,
CA.
November 18-24, 2013: CDC Hosts Get Smart
About Antibiotics Week, Online.
November 19-22, 2013: International Conference on
Infectious Disease Dynamics (EPIDEMICS 2013),
Amsterdam, Netherlands.
December 9-13: RIPAQS-INPIQS hosts its 1st
International Congress.
APUA will host a Learning Lab on Thursday, October 3rd
from 12:15pm to 1pm at ID Week, entitled, “Antibiotic
stewardship and the role of diagnostics: barriers and
opportunities.”
Upcoming Events

For instance, a surgical site infection study in one of the local
district hospitals was successfully completed recently.
Interventions done through continuous medical education on
rational use of antibiotics for surgical prophylaxis showed a
decrease in antibiotic consumption and eventual rational use of
antibiotics through the development of an antibiotic use policy
within the hospital. Currently, this study is being replicated in
two other hospitals by members of the working group, with the
aim of rationalizing antibiotic use in surgical procedures. In
addition, the working group is in the process of developing an
exciting 5-day training course on AMR and rational antibiotic
use targeting both human and veterinary medicine practitioners
from different regions in the country who will then serve as
“AMR champions” countrywide.
In the course of its activities, the working group has learned a
number of lessons, including the following:
Global problems are best tackled through national action
Both underuse and overuse of antibiotics co-exist.
Underuse of antibiotics leads to childhood deaths from
common infectious diseases, while overuse is propagated
mostly by hospitals and through self-treatment.
The need for antibiotics can be reduced through coverage
by childhood immunization programs (e.g. Hib and the
newly introduced pneumococcal vaccines) and improved
hospital infection control.
Inappropriate antibiotic use can be reduced through the
following three ways: reducing provider and self-
prescribing for coughs and colds; reducing use for watery
diarrhea; and reducing use in food animals.
APUA-Kenya’s antimicrobial
stewardship program
Sam Kariuki, PhD, APUA-Kenya Chapter Leader Kenya Medical Research Institute, Nairobi, Kenya
Kenya is challenged with increasing rates of antimicrobial
resistance (AMR), which can be attributed to a multiplicity of
factors, including a high infectious disease burden. Acute
respiratory infections, diarrheal diseases and HIV/AIDS are
among the leading causes of mortality. HIV/AIDS has
predisposed infected individuals to an undue increase in the
utilization of antibiotics in order to prevent and treat
opportunistic infections—raising concerns over the looming
emergence and spread of resistance to commonly available
antibiotics. Other factors include inadequate diagnostic capacity
and a large rural dwelling population (70%) with limited access
to formal healthcare services. The latter is demonstrated by the
prevalence of self-medication and inadequate knowledge of
appropriate antibiotic use in both healthcare providers and the
general population.
A recent situation analysis cites 2002, 2008 and 2009 reports
that most pharmacies dispensed antibiotics without
prescriptions. It also documents that most doctors and other
healthcare professionals wrote prescriptions for antibiotics
inappropriately—for common coughs, colds and diarrhea.
Many, perhaps most, of those who self-prescribe would have
been prescribed antibiotics officially if they had visited a
doctor or clinic. There is good evidence that many patients
simply have no option but self-medication as they may have no
access to healthcare for financial reasons or because an
appropriate health facility is physically inaccessible, or
antibiotic supplies are depleted. Another challenge for Kenya
is posed by the widespread use of antibiotics in animals for
prophylaxis and treatment, especially in poultry farming in the
neighborhoods of big cities.
It is a complex situation, but the Antimicrobial Resistance
Working Group established in 2011—with a membership of 20
and with representation from different stakeholders in the
Ministry of Health, non-governmental organizations, and
private sector healthcare providers—is volunteering its time to
mobilize resources to fight AMR. One of its objectives is to fill
information gaps with regard to the rational use of antibiotics.
APUA Field report: Kenya • The APUA Newsletter Vol. 31. No. 2 • © 2013 APUA • 19

susceptibility (98.57%), followed by imipenem (85.94%).
PFGE and Quantitative Antibiotic Testing both revealed the
presence of 2 clusters. Phenotypic tests for MBL and AmpC
production were negative. The 4 strains of A. baumannii (2
each from 2011 and 2012) selected for SDS-PAGE analysis
revealed no difference in the OMP profile. An efflux pump for
imipenem was not detected in any isolate (all CCCP negative);
however, all 8 strains isolated in 2011 and 2012 revealed
positive results for the oxacillinase phenotype test. The PCR
performed for blaOXA-23-like and blaOXA-24-like genes gave
negative results, while all 8 strains gave positive results for
blaOXA-51 and blaOXA-58 genes.
Conclusion
Determining the mechanism of resistance to imipenem in A.
baumannii and the number of circulating epidemic strains helps
to understand how the resistance is spreading and emphasizes
the need for having infection control and antimicrobial
stewardship programs in hospitals.
Objective
This study aimed to determine the relatedness of Acinetobacter
baumannii strains collected from the north of Lebanon and to
identify their mechanism(s) of resistance to imipenem.
Acinetobacter baumannii causes opportunistic nosocomial
infections, mainly in intensive care units. In addition to its
natural resistance, acquired resistance to many antibiotics can
occur. As a result, carbapenems have become the drug of
choice in treating such resistant strains. Unfortunately,
resistance to imipenem has been reported in several countries
since 1990.
Methods
A total of 149 non-duplicate strains of A. baumannii (identified
by API 20NE) were isolated and analyzed between 2006 and
2012 from different types of infections in hospitalized patients.
Their profile of resistance was determined using the Kirby-
Bauer disk diffusion method, in which the diameters of
inhibition were measured and used for Quantitative
Antibiogram Typing. Typing was also performed using ST
typing by multiplex PCR and PFGE.
For the detection of the mechanisms
of resistance, phenotypic methods
were used: DDST IMP-EDTA for
MBL detection, 200mM NaCl for
OXA detection, 200mg/l cloxacillin
and PBA for AmpC detection, and
noital carbonyl-cyanide m-chloro
phenylhydrazone as efflux inhibitor.
In addition, PCR was used to detect
the genes of resistance and SDS-
PAGE was performed to study the
protein profiles of resistant versus
susceptible strains.
Results
Forty-five percent of the isolates
were collected from the Intensive
Care Unit and 58% of the specimens
were from the sputum. Colistin was
associated with the highest
20 • The APUA Newsletter Vol. 31. No. 2 • © 2013 APUA • APUA Field report: Lebanon
Acinetobacter baumannii epidemiology
and resistance in north Lebanon Ziad Daoud, PhD, APUA-Lebanon Chapter Leader University of Balamand; CHN Hospital, Deir El-Balamand, Al-Kurah, North Lebanon
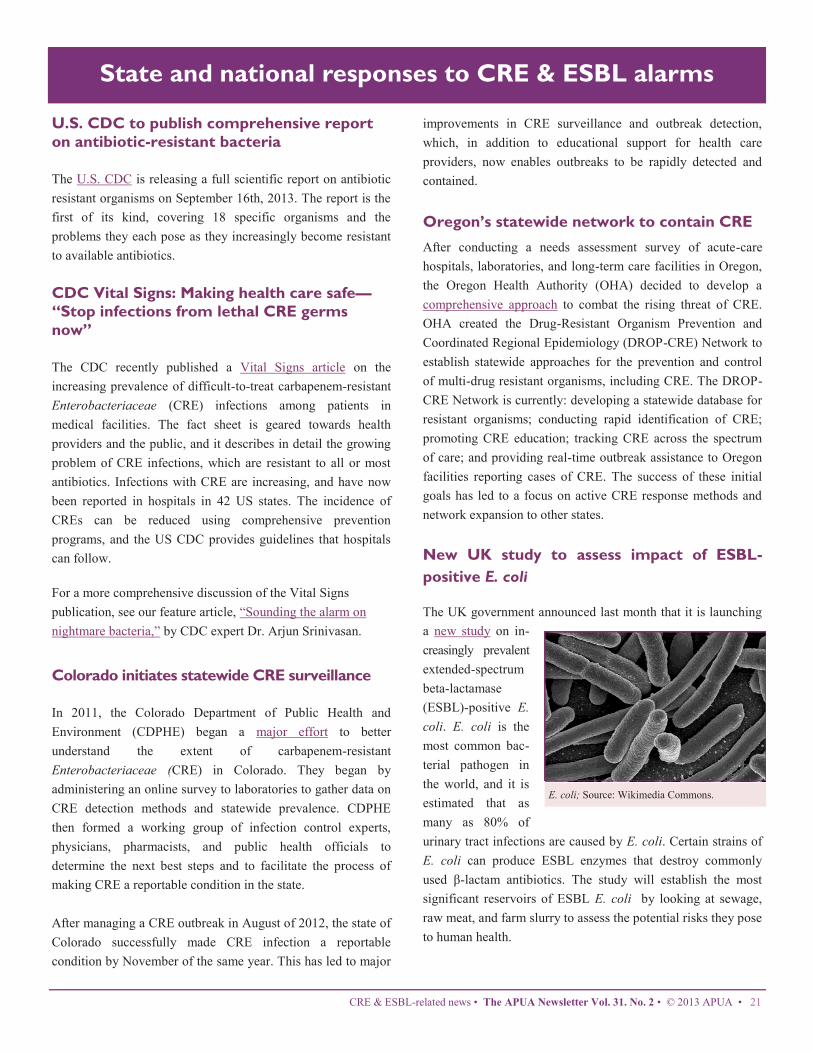
State and national responses to CRE & ESBL alarms
U.S. CDC to publish comprehensive report
on antibiotic-resistant bacteria
The U.S. CDC is releasing a full scientific report on antibiotic
resistant organisms on September 16th, 2013. The report is the
first of its kind, covering 18 specific organisms and the
problems they each pose as they increasingly become resistant
to available antibiotics.
CDC Vital Signs: Making health care safe—
“Stop infections from lethal CRE germs
now”
The CDC recently published a Vital Signs article on the
increasing prevalence of difficult-to-treat carbapenem-resistant
Enterobacteriaceae (CRE) infections among patients in
medical facilities. The fact sheet is geared towards health
providers and the public, and it describes in detail the growing
problem of CRE infections, which are resistant to all or most
antibiotics. Infections with CRE are increasing, and have now
been reported in hospitals in 42 US states. The incidence of
CREs can be reduced using comprehensive prevention
programs, and the US CDC provides guidelines that hospitals
can follow.
For a more comprehensive discussion of the Vital Signs
publication, see our feature article, “Sounding the alarm on
nightmare bacteria,” by CDC expert Dr. Arjun Srinivasan.
Colorado initiates statewide CRE surveillance
In 2011, the Colorado Department of Public Health and
Environment (CDPHE) began a major effort to better
understand the extent of carbapenem-resistant
Enterobacteriaceae (CRE) in Colorado. They began by
administering an online survey to laboratories to gather data on
CRE detection methods and statewide prevalence. CDPHE
then formed a working group of infection control experts,
physicians, pharmacists, and public health officials to
determine the next best steps and to facilitate the process of
making CRE a reportable condition in the state.
After managing a CRE outbreak in August of 2012, the state of
Colorado successfully made CRE infection a reportable
condition by November of the same year. This has led to major
improvements in CRE surveillance and outbreak detection,
which, in addition to educational support for health care
providers, now enables outbreaks to be rapidly detected and
contained.
Oregon’s statewide network to contain CRE
After conducting a needs assessment survey of acute-care
hospitals, laboratories, and long-term care facilities in Oregon,
the Oregon Health Authority (OHA) decided to develop a
comprehensive approach to combat the rising threat of CRE.
OHA created the Drug-Resistant Organism Prevention and
Coordinated Regional Epidemiology (DROP-CRE) Network to
establish statewide approaches for the prevention and control
of multi-drug resistant organisms, including CRE. The DROP-
CRE Network is currently: developing a statewide database for
resistant organisms; conducting rapid identification of CRE;
promoting CRE education; tracking CRE across the spectrum
of care; and providing real-time outbreak assistance to Oregon
facilities reporting cases of CRE. The success of these initial
goals has led to a focus on active CRE response methods and
network expansion to other states.
New UK study to assess impact of ESBL-
positive E. coli
The UK government announced last month that it is launching
a new study on in-
creasingly prevalent
extended-spectrum
beta-lactamase
(ESBL)-positive E.
coli. E. coli is the
most common bac-
terial pathogen in
the world, and it is
estimated that as
many as 80% of
urinary tract infections are caused by E. coli. Certain strains of
E. coli can produce ESBL enzymes that destroy commonly
used β-lactam antibiotics. The study will establish the most
significant reservoirs of ESBL E. coli by looking at sewage,
raw meat, and farm slurry to assess the potential risks they pose
to human health.
CRE & ESBL-related news • The APUA Newsletter Vol. 31. No. 2 • © 2013 APUA • 21
E. coli; Source: Wikimedia Commons.

APUA headquarters in action
APUA 2013 Leadership and Chapter Award
Recipients
APUA is pleased to award Dr. Keith
Klugman, Director for Pneumonia at the
Gates Foundation, the 2013 Leadership
Award. Keith has served on numerous
committees as an expert in antimicrobial
resistance, including those for the World
Health Organization (WHO) and the
Centers for Disease Control and Prevention
(CDC). He has published more than 450
scientific papers on the subjects of
pneumonia, meningitis, antimicrobial resistance, and vaccines
for bacterial pathogens.
The annual APUA Leadership Award recognizes an individual or
organization demonstrating extraordinary leadership in promoting the
prudent use of antibiotics in order to contain antibiotic resistance.
APUA is also pleased to announce APUA-Cuba as the winner
of the 2013 Chapter Award. APUA-Cuba has over 1,000
members in 60 different
medical specialties. Chapter
leader Dr. Moisés Morejón
(Manual Fajardo Hospital)
and his colleagues have held
multiple symposia on
antimicrobial resistance and
the need for new antibiotics.
The annual APUA Chapter Award recognizes one of 66 international
chapters affiliated with the organization for its members’ dedication
to the APUA mission of ensuring access to effective treatment and
promoting appropriate antibiotic use to contain drug resistance.
The 2013 winners will be celebrated a special event at ID
Week, October 2—6 in San Francisco, CA.
Directorship Transition at APUA
Effective October 15, Ms. Kathleen Young will be
transitioning from her position as APUA Executive Director to
a role as program consultant. According to Dr. Stuart B. Levy,
APUA President, “Through Kathy’s commitment and
initiative, APUA has played a major role in driving the drug
resistance issue to the top of the national and international
health agenda.” During her 15 year tenure, APUA expanded its
affiliated international chapter network to over 66 countries
and extended its mission to increase access to effective
antibiotics in resource-poor countries.
Ms. Young introduced important research projects to document
antibiotic resistance problems and then forged public and
private partnerships to build consensus on interventions.
Among the projects she initiated were:
the first international antibiotic resistance surveillance
meeting involving over fifteen major surveillance systems
(1997)
the first peer-reviewed study providing evidence and
detailed recommendations to limit antibiotics in food
animal production (FAAIR report 2002)
the first multi-university network investigating resistance
in commensal organisms for early warning signs for
resistance in pathogens (2002-2007)
the first report to document global antimicrobial resistance
trends in the major pathogens (GAARD report 2005)
the first detailed African country situation analysis of
antibiotic use and resistance (2008), and
an updated peer-reviewed estimate of the U.S. cost of
antibiotic resistance in over ten years, now widely cited in
policy debates (2009)
Ms. Young notes: “Fortunately, we are now seeing active
investments in antibiotic stewardship and infection control and
new treatment and diagnostics coming online. With the
continued commitment of APUA’s board and advisors and
dedicated staff in place, APUA will continue to play a
leadership role in ensuring access to effective antimicrobials
for generations to come.” With a background in biochemistry
and corporate organizational development, Dr. Barbara
Lapinskas, PhD ([email protected]), will continue
as APUA’s Administrative Director. Jane Kramer, JD, is
serving as APUA’s Program Development Director with
experience as Director of Communications for several global
pharmaceutical companies supporting programs to increase
access to medicines.
APUA cautions against use of antibiotics to
treat malnutrition
On June 20, a letter crafted by the APUA Nutrition Group was
22 • The APUA Newsletter Vol. 31. No. 2 • © 2013 APUA • APUA headquarters
Keith Klugman,
MD, PhD

APUA invites its chapter organizations and any
interested readers to submit commentary on their
opinions and observations regarding the use of
antibiotics to treat malnourished children in their
countries.
APUA headquarters in action
APUA headquarters • The APUA Newsletter Vol. 31. No. 2 • © 2013 APUA • 23
APUA’s ID Week Learning Lab Antibiotic Stewardship and the Role of Diagnostics: Barriers and Opportunities
Thursday, October 3, 2013; 12:15 pm – 1:00 pm; Booth 1501
Agenda (12:15-12:45pm)
1. The mandate for stewardship: antibiotic resistance trends and costs
2. Benefits of hospital antibiotic resistance susceptibility testing in targeting therapy
3. Diagnostics and their role in antibiotic stewardship
Group Discussion: (12:45-1:00pm)
What are the barriers to greater use of susceptibility testing?
What would increase the value of diagnostics for clinicians? (sensitivity? specificity?)
What incentives would promote use of diagnostics and stewardship programs?
Presenters:
Stuart B. Levy, M.D. Co-founder and President of the Alliance for the Prudent Use of Antibiotics (APUA). Distinguished Professor of Molecular
Biology and Microbiology, and of Medicine, Director of the Center for Adaptation Genetics and Drug Resistance, Tufts
University School of Medicine; Staff Physician, Tufts Medical Center, Boston, MA
Kavita K. Trivedi, M.D. Public Health Medical Officer of Healthcare Associated Infections Program at the Center for Health Care Quality, California
Department of Public Health. Dr. Trivedi leads the California Antimicrobial Stewardship Initiative and is a former Epidemic
Intelligence Service Officer with the CDC.
Learning Lab Summary:
Antibiotic stewardship experts, Levy and Trivedi will review and lead an open discussion on current drug resistance trends, antibiotic
stewardship practices, and new resources available to control antibiotic resistance. APUA is an international public health organization
conducting research and education in conjunction with affiliated chapters in 66 countries (www.apua.org).
published in the New England Journal of Medicine. The letter,
which cautioned against the use of antibiotics to treat
malnutrition in resource-limited settings, was a response to an
earlier article by researchers at the University of Washington in
St. Louis who tested antibiotic treatment of severely
malnourished Malawi children in a clinical trial. The authors
claim that recovery rates were higher and mortality rates were
lower among children who received antibiotics than among
those who received placebo as part of their outpatient treatment
with ready-to-use therapeutic foods (RUTFs).
APUA compiled expert opinion from its Scientific Advisory
Board, including co-authors Iruka Okeke, Jose Ramiro Cruz,
and Gerald Keusch, in order to formulate an editorial in
response to the suggested implementation of routine antibiotics
for severe malnutrition. APUA supports further research
because the potential broad-scale expansion of antibiotic use
could prompt widespread antibiotic misuse and resistance in
the community. Instead, researchers should focus on immediate
expansion of validated interventions, including breast-feeding,
the use of probiotics, and increased access to traditional RUTFs
and clean water. These strategies will be more effective in
reducing malnutrition in the long run.
APUA collaborates with Alere to produce
webinar
As part of an ongoing partnership, APUA and Alere
Diagnostics held the first of three live webinars on July 2nd.
Dr. Philip Carling, Professor of Clinical Medicine at Boston
University School of Medicine, hosted the webinar on the
impact of antimicrobial stewardship in healthcare settings.
With over 500 attendees, the webinar discussed the elements of
successful antimicrobial stewardship, how to analyze and
measure antibacterial use in hospitals, and the importance of
rapid diagnostics to ensure appropriate antimicrobial use.
The full webinar recording and slides can be accessed here.

German parliament proposes strict
measures to cut antibiotic use
Germany’s Parliament, The Bundestag, has made major
revisions to its policies on the use of medications for livestock.
The Ministry for Food, Agriculture and Consumer Protection
announced in March that the use of antibiotics in food animal
production needs to be significantly reduced, and ideally,
strictly limited to therapeutic purposes. The policy will give
regional authorities greater power over the exchange of
information between regions thanks to a new national database
of antibiotic use on farms. Authorities, as well as farmers, will
be able to compare the frequency of antibiotic therapy between
farms across the country. Farmers and veterinarians will bear
the responsibility of monitoring the frequency of medication
and enacting measures to reduce antibiotic use if appropriate.
FY14 Global Health Appropriations
In the last week of July, the House Appropriations Committee
approved its FY 2014 State/Foreign Operations spending bill,
allocating $40.6 billion in discretionary funding—a 19%
decrease from FY 2013. While eliminating spending for certain
international organizations, the House bill does provide
generous funding to various key global health programs,
including $6 billion to the President’s Emergency Plan For
AIDS Relief, and hundreds of millions of dollars each to
tuberculosis, malaria, maternal and child health, and nutrition
programs. Meanwhile, the Senate Appropriations Committee
passed its FY 2014 bill which sets overall spending at $50.5
billion and provides much more for foreign assistance than the
House. It appears most likely that committee staff on both
sides of the Capitol will have to work to bridge the major gaps
between the two bills.
India poised for National Antibiotics Policy
The Union Health Ministry of India is considering a new
National Antibiotics Policy to restrain the overuse of
antibiotics and reduce an already alarming rate of resistance. A
policy was drawn up in 2011 following the release of Timothy
Walsh’s article in The Lancet which detailed the emergence of
a new enzyme—named New Delhi Metallo-1 (NDM-1) after
the city it was discovered in—that made bacteria resistant to all
antibiotics. The policy was ultimately scrapped, but as
antibiotic resistance has only increased, policy makers are re-
examining options to limit antibiotic use. The Chennai
Declaration, an August 2012 event that convened specialists to
form a plan for tackling antimicrobial resistance in India, is
believed to have reignited Indian stakeholders’ calls for
change.
FDA requires veterinary oversight for
livestock antibiotics
The U.S. Food and Drug Administration (FDA) is
implementing a new strategy to encourage more appropriate
and prudent use of antibiotics in food animal production. The
strategy intends to curb antibiotic overuse and misuse by
identifying certain antibiotics that will now require veterinary
oversight via the Veterinary Feed Directive (VFD). The FDA
will also help drug companies voluntarily re-label antibiotic
products to remove feed efficiency and growth promotion
claims. Labels will instead emphasize antibiotic use for the
prevention, control, and treatment of bacterial diseases.
Michelle Arnold, a veterinarian from the University of
Kentucky College of Agriculture, Food, and Environment,
approved of the FDA’s program, stating that “veterinarians are
uniquely qualified to determine which specific disease-causing
organisms are likely to be present and to determine
appropriately timed administration of medication relative to the
disease.”
In July, APUA, along with multiple other national health
organizations, signed a letter submitted to the FDA and the US
Department of Agriculture (USDA) commenting on their
proposed changes to the VFD. While the changes would keep
certain over-the-counter drugs under closer supervision by
veterinarians, they would alter the definition of the veterinary
client patient relationship (VCPR) in a way that allows a
veterinarian’s practice to issue a VFD without requiring a visit
to each facility. The letter states support for the FDA and
USDA to retain the current, stricter VCPR definition. The letter
also recommends that language be included to define a limit of
21 days for the duration of use of an antibiotic in a herd, pen or
barn.
Policy updates
24 • The APUA Newsletter Vol. 31. No. 2 • © 2013 APUA • Policy updates
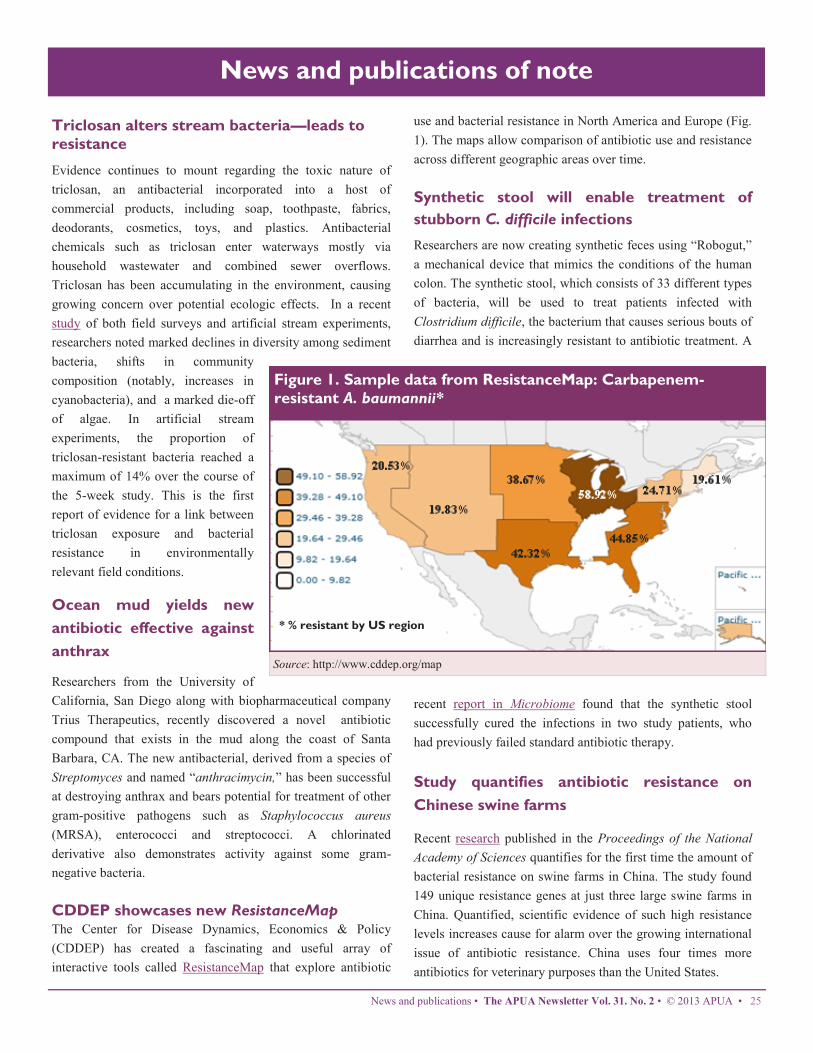
Triclosan alters stream bacteria—leads to
resistance
Evidence continues to mount regarding the toxic nature of
triclosan, an antibacterial incorporated into a host of
commercial products, including soap, toothpaste, fabrics,
deodorants, cosmetics, toys, and plastics. Antibacterial
chemicals such as triclosan enter waterways mostly via
household wastewater and combined sewer overflows.
Triclosan has been accumulating in the environment, causing
growing concern over potential ecologic effects. In a recent
study of both field surveys and artificial stream experiments,
researchers noted marked declines in diversity among sediment
bacteria, shifts in community
composition (notably, increases in
cyanobacteria), and a marked die-off
of algae. In artificial stream
experiments, the proportion of
triclosan-resistant bacteria reached a
maximum of 14% over the course of
the 5-week study. This is the first
report of evidence for a link between
triclosan exposure and bacterial
resistance in environmentally
relevant field conditions.
Ocean mud yields new
antibiotic effective against
anthrax
Researchers from the University of
California, San Diego along with biopharmaceutical company
Trius Therapeutics, recently discovered a novel antibiotic
compound that exists in the mud along the coast of Santa
Barbara, CA. The new antibacterial, derived from a species of
Streptomyces and named “anthracimycin,” has been successful
at destroying anthrax and bears potential for treatment of other
gram-positive pathogens such as Staphylococcus aureus
(MRSA), enterococci and streptococci. A chlorinated
derivative also demonstrates activity against some gram-
negative bacteria.
CDDEP showcases new ResistanceMap The Center for Disease Dynamics, Economics & Policy
(CDDEP) has created a fascinating and useful array of
interactive tools called ResistanceMap that explore antibiotic
use and bacterial resistance in North America and Europe (Fig.
1). The maps allow comparison of antibiotic use and resistance
across different geographic areas over time.
Synthetic stool will enable treatment of
stubborn C. difficile infections
Researchers are now creating synthetic feces using “Robogut,”
a mechanical device that mimics the conditions of the human
colon. The synthetic stool, which consists of 33 different types
of bacteria, will be used to treat patients infected with
Clostridium difficile, the bacterium that causes serious bouts of
diarrhea and is increasingly resistant to antibiotic treatment. A
recent report in Microbiome found that the synthetic stool
successfully cured the infections in two study patients, who
had previously failed standard antibiotic therapy.
Study quantifies antibiotic resistance on
Chinese swine farms
Recent research published in the Proceedings of the National
Academy of Sciences quantifies for the first time the amount of
bacterial resistance on swine farms in China. The study found
149 unique resistance genes at just three large swine farms in
China. Quantified, scientific evidence of such high resistance
levels increases cause for alarm over the growing international
issue of antibiotic resistance. China uses four times more
antibiotics for veterinary purposes than the United States.
News and publications of note
News and publications • The APUA Newsletter Vol. 31. No. 2 • © 2013 APUA • 25
Figure 1. Sample data from ResistanceMap: Carbapenem-
resistant A. baumannii*
* % resistant by US region
Source: http://www.cddep.org/map
News and publications of note
Within the scope of the natural environment is antibiotic
resistance, an area the Institute refers to as the “invisible”
environment and believes is of critical importance to human
interaction and health. To inform Harmony residents of the
impending crisis of antibiotic resistance and the overuse of
antibacterial products, the Institute included language in the
Residential Properties document and regularly educates
residents through science advisories in its quarterly newsletter.
The Institute also presents a youth education program entitled
“Good Germ, Bad Germ” in an effort to instill in children the
reality that bacteria are alive and the vast majority of them are
their friends.
A major Florida university has recently committed to pursuing
longitudinal studies within the town of Harmony and the
Institute is proposing that antibacterial resistance be one of two
initiating studies.
Updates in C. difficile management
In a recent Medscape article, Dr. John G. Bartlett discussed
five important developments on the topic of preventing and
treating C. difficile infections (CDI):
1. A new U.S. CDC study found that 75% of patients
admitted to a hospital or nursing home were already
colonized with C. difficile at the time of admission. This
knowledge has important ramifications for infection
control practices.
2. Fidaxomicin is now the second drug approved by the U.S.
FDA for the treatment of CDI. While relatively costly, it
has global cure rates superior to those of vancomycin.
3. Doctors in the Netherlands have trained a beagle to detect
CDI based on the odor of p-cresol, the phenolic compound
that is thought to be associated with C. difficile. The
beagle’s performance in the trial was near perfect.
4. Surgeons at the University of Pittsburgh have reported a
new surgical approach, called “diverting loop ileostomy
with colonic vancomycin lavage,” which has lower
mortality rates than the standard colectomy procedure.
5. Stool transplants for patients with multiple relapses of CDI
are becoming more widely accepted, thanks to more
research and relaxed FDA requirements.
A novel community addresses antibiotic
resistance
Martha E. Lentz
Founder and President of The Harmony Institute
In 1996 the Harmony Institute was created with a unique
mission that proposes that people who have routine interactions
with animals and the natural environment experience the
benefits of a healthier lifestyle. Based upon existing science
that demonstrates the health benefits of human-animal-nature
interactions, and with the knowledge of the concept and
capacity of longitudinal studies to affect human health choices
and community environments such as the Framingham Heart
Study, the Institute believed a similar study might drive better
health and smarter, more sustainable, living.
The Institute formed a science advisory board of renowned
researchers in disciplines including environmental psychology,
human-animal relations, public health, energy, education,
urban design, veterinary medicine and wildlife management to
work with the community development team in designing the
community of Harmony, Florida to specifically accommodate,
encourage and maximize these interactions and to serve as a
living laboratory for longitudinal study. To direct the
education and management of the community, the Institute’s
advisory board authored the document “Harmony Residential
Properties Restrictions, Guidelines and Goals Concerning
Companion Animals, Habitat and Wildlife©.”
26 • The APUA Newsletter Vol. 31. No. 2 • © 2013 APUA • The Harmony Institute
was founded in 1996
with the mission of
promoting “human
health and well-being through the interaction
of people, animals and the environment.” The
vision and goals of the Institute led to the
formation of Birchwood Acres L.L.L.P., the
purchase of an 11,000+ acre property in
1998, and the development of the Town of
Harmony. Harmony, Florida is a town
specially formed with the Institute’s mission
in mind, and it serves as a “living laboratory”
for the study of green living.

About us
Antibiotics are humanity's key defense against disease-causing microbes. The growing prevalence of antibiotic resistance
threatens a future where these drugs can no longer cure infections and killer epidemics run rampant. The Alliance for
the Prudent Use of Antibiotics (APUA) has been the leading global non-governmental organization fighting to preserve
the effectiveness of antimicrobial drugs since 1981. With affiliated chapters in more than 66 countries, including 33 in
the developing world, we conduct research, education and advocacy programs to control antibiotic resistance and en-
sure access to effective antibiotics for current and future generations.
Our global network of infectious disease experts supports country-based activities to control and monitor antibiotic
resistance tailored to local needs and customs. The APUA network facilitates the exchange of objective, up-to-date
scientific and clinical information among scientists, health care providers, consumers and policy makers worldwide.
The APUA Clinical Newsletter has been published continuously three times per year since 1983.
Tel: 617-636-0966 • Email: [email protected] • Web: www.apua.org
APUA global chapter network
of local resources & expertise
200 Harrison Ave, Posner Building (Business) Level 3, Boston, MA 02111
Phone: 617-636-0966 | Fax: 617-636-0458 | E-mail: [email protected]
www.apua.org
“Preserving the Power of Antibiotics”®
About us • The APUA Newsletter Vol. 31. No. 2 • © 2013 APUA • 27
28 • The APUA Newsletter Vol. 31. No. 2 • © 2013 APUA • Upcoming events
“Preserving the Power of Antibiotics”®
200 Harrison Ave, Posner Building
(Business) Level 3, Boston, MA 02111
Phone: 617-636-0966 | Fax: 617-636-0458 |
E-mail: [email protected]
www.apua.org





























