Embed Size (px)
Citation preview
DCC-2618,apan-KITandPDGFRAswitchcontrolinhibitor,achievesproof-of-concept
inafirst-in-humanstudy
FilipJanku,SuzanneGeorge,AlbiRazak,MichaelGordon,DavidBrooks,DanielFlynn,MichaelKaufman,JamaPitman,BryanSmith,Neeta
Somaiah,EricGerstenberger,DebWestwood,OliverRosen
2016 EORTC-NCI-AACRDecember 1, 2016
DISCLOSURES
• F.Janku:ResearchfundingfromDeciphera,SABDeciphera• S.George:ResearchfundingfromDeciphera,Blueprint
Medicine,Pfizer,Bayer,Novartis• A.Razak:ResearchfundingfromDeciphera• M.Gordon:ResearchfundingfromDeciphera• D.G.Brooks,D.Flynn,M.Kaufman,J.Pitman,O.Rosen,B.
Smith,D.Westwood:Deciphera employees
• Ongoingstudy:Presentationcontainspreliminarydatathatarepartiallymonitoredandvalidated
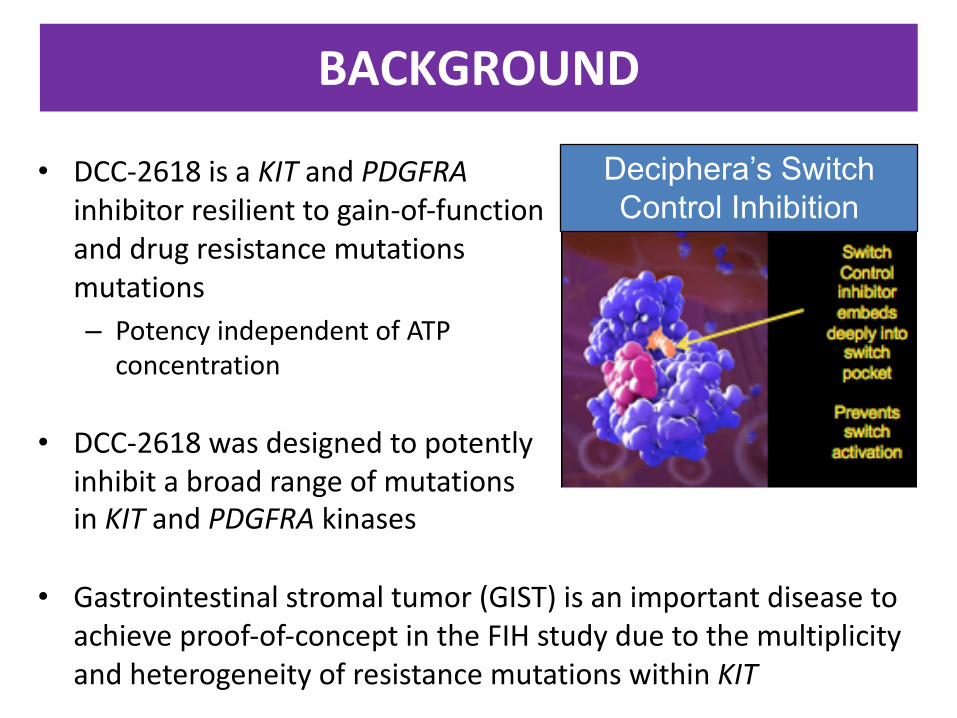
BACKGROUND
• DCC-2618isaKIT andPDGFRAinhibitorresilienttogain-of-functionanddrugresistancemutationsmutations– PotencyindependentofATP
concentration
• DCC-2618wasdesignedtopotentlyinhibitabroadrangeofmutationsinKIT andPDGFRA kinases
• Gastrointestinalstromaltumor(GIST)isanimportantdiseasetoachieveproof-of-conceptintheFIHstudyduetothemultiplicityandheterogeneityofresistancemutationswithinKIT
Deciphera’s Switch Control Inhibition

RATIONALEFORDCC-2618STUDY• ActivityregardlesswhetherprimarymutationisinKIT Exon9,Exon11,orExon17
– IC50 forKIT Exon11deletion3nM,IC50PDGFRA D842V60nM• BroadactivityinsecondaryKITmutationsacrossExons13,14,17,and18
– ActivemetaboliteDP-5439possessescomparableactivityacrossallmutations• KIT T670IandV654AsecondarymutationsaretheleastsensitivetoDCC-2618
– IC50 forKIT T670I221nM ,IC50 for189nM forKITV654A
D81
6VD
820A
DV
559-
V56
0/D
816V
AY
du
p/N
655S
AY
du
p/N
680K
AY
du
p/D
816G
AY
du
p/D
820G
AY
du
p/D
820E
AY
du
p/N
822K
AY
du
p/N
822Y
AY
du
p/N
822H
WK
V55
7C/T
670I
WK
V55
7C/D
820Y
WK
V55
7CD
820A
V56
0D/V
654A
V56
0D/T
670I
V56
0D/N
822K
V56
0D/Y
823D
D81
6VD
820A
DV
559-
V56
0/D
816V
AY
du
p/N
655S
AY
du
p/N
680K
AY
du
p/D
816G
AY
du
p/D
820G
AY
du
p/D
820E
AY
du
p/N
822K
AY
du
p/N
822Y
AY
du
p/N
822H
WK
V55
7C/T
670I
WK
V55
7C/D
820Y
WK
V55
7CD
820A
V56
0D/V
654A
V56
0D/T
670I
V56
0D/N
822K
V56
0D/Y
823D
D81
6VD
820A
DV
559-
V56
0/D
816V
AY
du
p/N
655S
AY
du
p/N
680K
AY
du
p/D
816G
AY
du
p/D
820G
AY
du
p/D
820E
AY
du
p/N
822K
AY
du
p/N
822Y
AY
du
p/N
822H
WK
V55
7C/T
670I
WK
V55
7C/D
820Y
WK
V55
7CD
820A
V56
0D/V
654A
V56
0D/T
670I
V56
0D/N
822K
V56
0D/Y
823D
D81
6VD
820A
DV
559-
V56
0/D
816V
AY
du
p/N
655S
AY
du
p/N
680K
AY
du
p/D
816G
AY
du
p/D
820G
AY
du
p/D
820E
AY
du
p/N
822K
AY
du
p/N
822Y
AY
du
p/N
822H
WK
V55
7C/T
670I
WK
V55
7C/D
820Y
WK
V55
7CD
820A
V56
0D/V
654A
V56
0D/T
670I
V56
0D/N
822K
V56
0D/Y
823D
0
5 0 0
1 0 0 0
1 5 0 0
2 0 0 0
C H O K IT M u ta n t A s s a y s
IC5
0 (
nM
)
ND
ND
D C C -2 6 1 8 Im a tin ib S u n it in ib R e g o ra fe n ib
DCC-2618-01-001:DESIGNANDOBJECTIVES• Design(NCT02571036)
– Pharmacologically-guided3+3escalationphaseIstudyoforalDCC-2618administeredBIDevery28days
• Objectives– Primary:Safety,tolerability,maximumtolerateddose(MTD),dose-
limitingtoxicities(DLT)– Secondary:Pharmacokineticprofile,antitumorefficacy– Exploratory:DeterminationofKIT and/orPDGFRAmutationsinplasma
cell-freeDNA(NGS)andserumtryptase
• Majoreligibilitycriteria– Patientswithadvancedrefractorycancersandmolecularrationalefor
activity– ECOG0-1– Adequateorganfunction– PriorKIT/PDGFRAinhibitorswereallowed

DCC-2618:DOSELEVELS&PATIENTSCHARACTERISTICS
DoseLevel(mg)(TimeonStudy)
NumberofPatients TumorTypes: Tissueand/orPlasma cfDNA Mutations
20BID(1x> 1year) 4 GIST:KIT Exon11(1x),KIT Exon17(1x),PDGFRA (1x)
GBM:PDGFRA/KIT/KDR co-amplified(1x)
30BID(1x6 months*) 4
GIST:KIT Exon11(1x),KITExon11 &17(1x)Thymic Carcinoma:KIT Exon11(1x)Desmoid tumor(1x)
50BID(2x> 6 months) 4 GIST:KIT Exon9(1x),KITExon11(3x)
100BID 6 GIST: KIT Exon9(x3),KITExon11(1x),PDGFRA Exon18(1x),SDHA(1x)
150BID 6 GIST: KIT Exon9(x2),KITExon11(x3),KITExon17(1x)
200BID Enrolling
Enrolled: 24 patients with mean of 4.7 prior therapies
*Patient stayed on study following PD due to clinical benefit
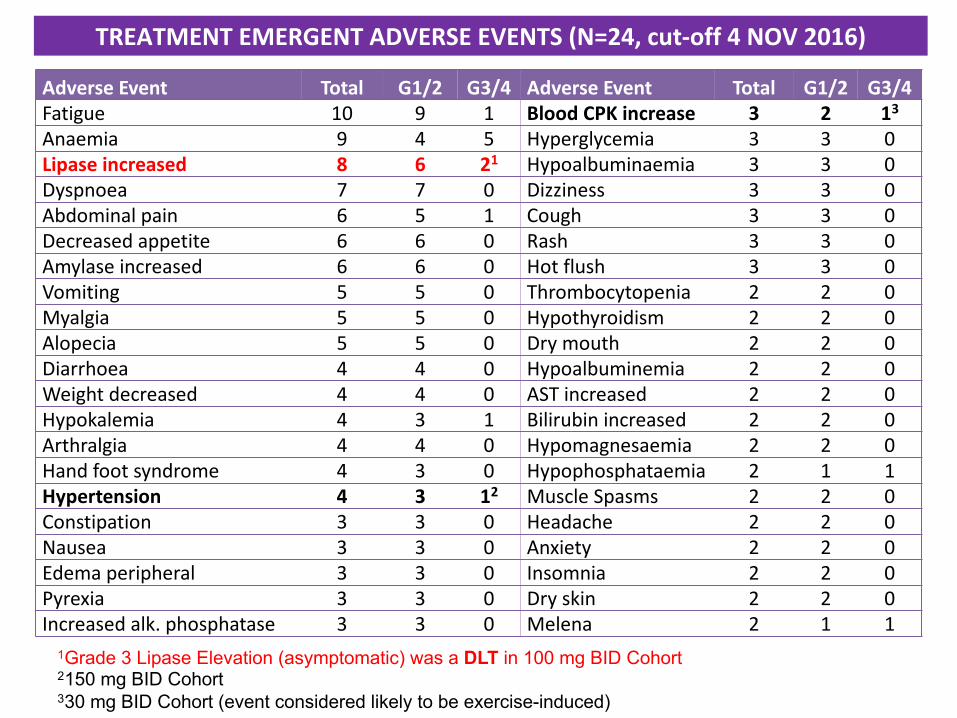
1Grade 3 Lipase Elevation (asymptomatic) was a DLT in 100 mg BID Cohort2150 mg BID Cohort330 mg BID Cohort (event considered likely to be exercise-induced)
AdverseEvent Total G1/2 G3/4 AdverseEvent Total G1/2 G3/4Fatigue 10 9 1 BloodCPKincrease 3 2 13Anaemia 9 4 5 Hyperglycemia 3 3 0Lipaseincreased 8 6 21 Hypoalbuminaemia 3 3 0Dyspnoea 7 7 0 Dizziness 3 3 0Abdominalpain 6 5 1 Cough 3 3 0Decreasedappetite 6 6 0 Rash 3 3 0Amylaseincreased 6 6 0 Hotflush 3 3 0Vomiting 5 5 0 Thrombocytopenia 2 2 0Myalgia 5 5 0 Hypothyroidism 2 2 0Alopecia 5 5 0 Drymouth 2 2 0Diarrhoea 4 4 0 Hypoalbuminemia 2 2 0Weightdecreased 4 4 0 ASTincreased 2 2 0Hypokalemia 4 3 1 Bilirubinincreased 2 2 0Arthralgia 4 4 0 Hypomagnesaemia 2 2 0Handfootsyndrome 4 3 0 Hypophosphataemia 2 1 1Hypertension 4 3 12 MuscleSpasms 2 2 0Constipation 3 3 0 Headache 2 2 0Nausea 3 3 0 Anxiety 2 2 0Edemaperipheral 3 3 0 Insomnia 2 2 0Pyrexia 3 3 0 Dryskin 2 2 0Increased alk.phosphatase 3 3 0 Melena 2 1 1
TREATMENTEMERGENTADVERSEEVENTS(N=24,cut-off4NOV2016)

DCC-2618* Cycle1Pharmacokinetics:150mgBIDCohortandAcrossAllDosingCohorts
*combined plasma concentration of DCC-2618 and its active metabolite DP-5439
T670I IC90 level: 1016 ng/ml (1989 nM ) achieved at Cmin of 50 mg BID
DAY 15
DAY -7, DAY 1, DAY 15

DCC-2618:CYCLE1PETINGISTPATIENTSDoseLevelmgBID
MutantGene
PatientID
InvestigatorReview
CTScanC3D1
30 KIT 01.001 PMR SD50 KIT 01.003 PMR PD50 KIT 03.003 PMR SD50 KIT 03.004 PMR SD50 KIT 04.008 PMR SD100 KIT 04.009 PMR PR100 KIT 01.004 PMR SD100 KIT 04.010 PMR SD100 KIT 01.005 PMR SD150 KIT 01.007 PMR SD150 KIT 02.002 PMR SD150 KIT 03.005 PMR SD150 KIT 01.006 PMR PD150 KIT 04.012 PMR Tooearly150 KIT 03.007 PMD SD100 PDGFRA 04.011 SMD SD100 SDHA 03.006 SMD PD
Baseline Cycle1
• 14 of 15 patients with KIT-mutant GIST had PMR
• 13 of 15 patients with KIT-mutant GIST had PMRconfirmed by central review, using EORTC PET response criteria

DCC-2618:RECISTRESPONSES
MRIaftercycle12
CTaftercycle2BaselineCT
BaselineMRI
§ Widely metastatic GIST with KIT Exon 11 deletion, who received 6 different prior KIT inhibitors
§ RECIST: partial response (-37%) maintained for 5+ cycles on DL4 100mg BID
§ Glioblastoma multiformewith PDGFRA / KIT / KDR co-amplification, who received prior XRT and temozolomide and progressed after 3 months
§ RECIST: partial response (-49%), on study for 12+ cycles on DL1 20mg BID
§ RANO: PR after cycle 12
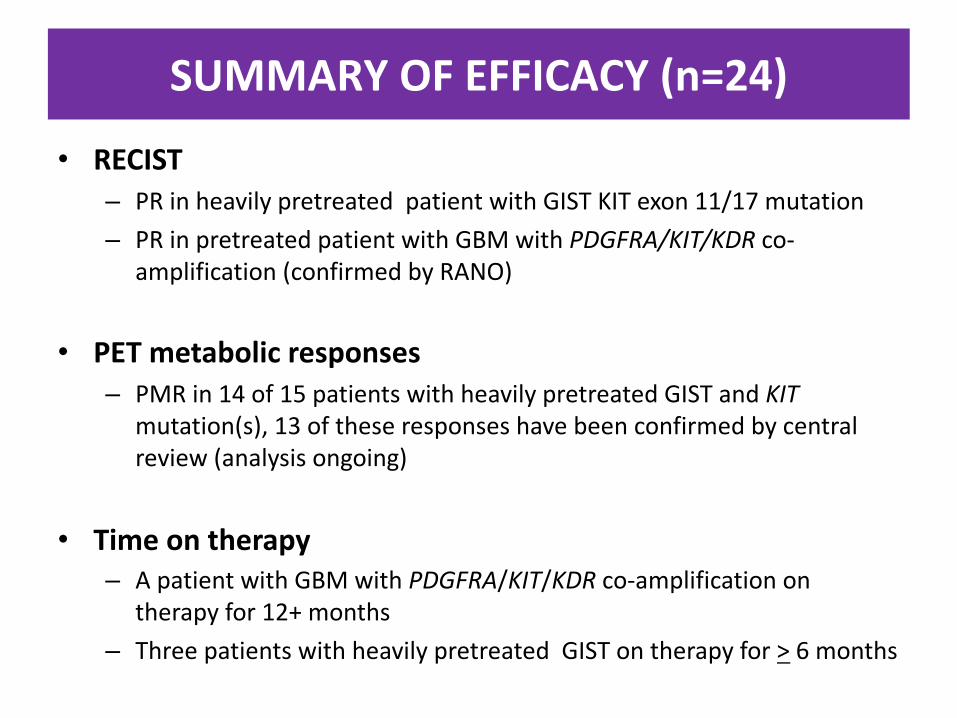
SUMMARYOFEFFICACY(n=24)
• RECIST– PRinheavilypretreatedpatientwithGISTKITexon11/17mutation– PRinpretreatedpatientwithGBMwithPDGFRA/KIT/KDR co-
amplification(confirmedbyRANO)
• PETmetabolicresponses– PMRin14of15patientswithheavilypretreatedGISTandKIT
mutation(s),13oftheseresponseshavebeenconfirmedbycentralreview(analysisongoing)
• Timeontherapy– ApatientwithGBMwithPDGFRA/KIT/KDR co-amplificationon
therapyfor12+months– ThreepatientswithheavilypretreatedGISTontherapyfor> 6months
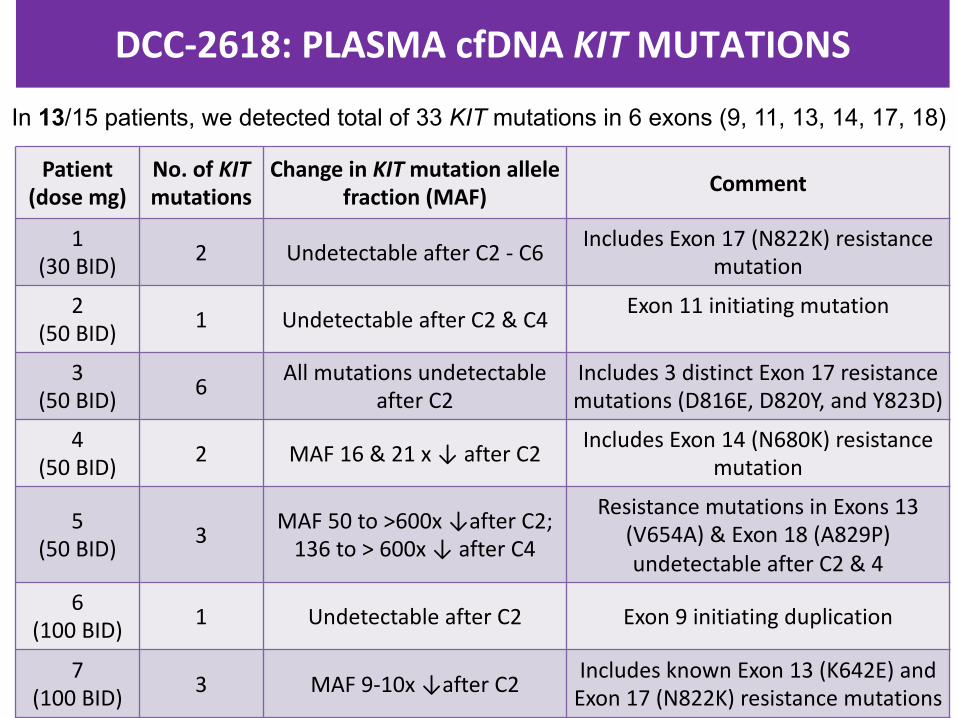
DCC-2618:PLASMAcfDNA KITMUTATIONS
Patient(dosemg)
No.ofKITmutations
ChangeinKITmutationallelefraction(MAF) Comment
1(30BID) 2 UndetectableafterC2- C6 IncludesExon17(N822K)resistance
mutation
2(50BID) 1 UndetectableafterC2&C4 Exon11initiating mutation
3(50 BID) 6 Allmutations undetectable
afterC2Includes 3distinctExon17resistancemutations(D816E,D820Y,andY823D)
4(50BID) 2 MAF16 &21x↓afterC2 IncludesExon14(N680K)resistance
mutation
5(50BID) 3 MAF50to >600x↓afterC2;
136to>600x↓afterC4
Resistance mutationsinExons13(V654A)&Exon18(A829P)undetectableafterC2&4
6(100BID) 1 UndetectableafterC2 Exon9initiating duplication
7(100BID) 3 MAF9-10x↓afterC2 Includes knownExon13(K642E)and
Exon17(N822K)resistancemutations
In 13/15 patients, we detected total of 33 KIT mutations in 6 exons (9, 11, 13, 14, 17, 18)

DCC-2618:DOSERESPONSERELATIONSHIPWITHSERUMTRYPTASELEVELS
Limit of detection(LabCorp)
Cohort (mg BID) Pre-treatmentMean± SD OntreatmentMean± SD P-value
20 3.57± 1.05 2.55± 1.04 0.073
30 3.08± 0.97 1.82± 0.95 0.011
50 2.48± 0.35 1.15± 0.33 <.001
100 2.27± 0.47 0.76± 0.44 <.001
150 3.24± 0.49 0.72± 0.47 <.001
P < 0.05 for tryptase decline as a function of dose
• DCC-2618iswelltoleratedtodatewithanencouragingsafetyprofileandrobustexposurefollowingoraldosesfrom20to150mgBID−Startingat50mgBID,meantroughlevelsofcombinedplasmaconcentrationexceedIC90 ofleastsensitivemutations T670IandV654A
−MTDhasnotbeenreachedyetanddoseescalationisongoing−Asymptomaticgrade3lipaseelevationhasbeentheonlyDLTtodate
• PreliminarysignalsofactivityperRECISTandPEThavebeenobservedinpretreatedpatientGBMwithco-amplificationofPDGFRA/KIT/KDRandGIST(s)with KITmutations
• DCC-2618leadstorapidclearanceofbroadspectrumofKITmutationsfromplasmacfDNA inpatientswithheavilypretreatedGIST
• Dose-dependentrapidreductionofserumtryptase warrantstestingofDCC-2618insystemicmastocytosis
CONCLUSIONS
ACKNOWLEDGEMENTSMDAndersonCancerCenter• NeetaSomaiah,MD• Vivek Subbiah,MD• SarinaPiha-Paul,MD• Funda Meric-Bernstam,MD• AungNaing,MD• Shubham Pant,MD• ChenGuo,PhD• JohndeGroot,MD• Nishma M.Ramzanali• Divya Sakamuri,MD• VandaStepanek,MD,PhD
DanaFarberCancerInstitute• SuzanneGeorge,MD• MicheleDorio,RN• MelissaHohos,RN• JuliaJ.Jennings• SarahSolomon• StephanieN.Vangellow
PrincessMargaretCancerCenter• Albiruni Razak,MD• Samer Salah• PenelopeBradbury• MaraKolodziejczyk,RN,MScN• MaryamMasood
HonorHealthResearchInstitute• MichaelGordon,MD• KristinHendrickson,BA,RN• AgnieszkaJezierska-Drutel• LeticiaLebron,RN,BSN
GuardantHealth• ElenaHelman
Nuventra• GrantHogeland,PharmD• DavidMitchell,PhD
Deciphera• Dennise Greensmith• DanLarson• LindaMartin• NicoleTurcuotte
OUR PATIENTS AND THEIR FAMILIES





























