Embed Size (px)
Citation preview
12/2/2020
1
WEBINAR 1MDS – VERSION 1.17.2
Demi Haffenreffer, RN
Haffenreffer and Associates, Inc
www.consultdemi.net
What we will discuss Day 1■ Using the RAI Manual
■ Chapter 2
– Types of Assessments
– Discharge / Entry / Re-entry definitions
– The OBRA and Medicare PDPM Schedules
■ Overall Steps for Conducting Assessments
■ Sections A and Z
■ Section B – Hearing, Speech and Vision
■ The Interviews:
– BIMS – Section C
– PHQ9 – Section D
– Preference – Section F
■ Section E – Behaviors
■ Section G
Assessment Types■ Two types of OBRA Assessments
– Comprehensive (MDS/CAAs/CP): Admission, Annual, SCSA, SCPA
– Non-Comprehensive: Qtr., SCQA, Entry, Discharge, Death
■ Schedules
– OBRA schedule vs. PDPM schedule
– Schedule set by ARD
– Start and stop of Hospice requires SCSA
■ Submission requirements
■ Entry – two types
– Admission (never admitted, Previous resident but d/c return not
anticipated, previous resident but d/c return anticipated and no return
within 30 days
– Reentry - Readmission of return anticipated and under 30 days
1
2
3
12/2/2020
2
Assessment Types - Sections A & Z
■ Discharge
– D/C (Planned or unplanned)
– Hospital observation stay of >24hours
– Resident is transferred from a Medicare to non-Medicare certified bed or
vice versa
■ Leave of Absence (LOA)
– Temporary home visit or therapeutic leave
– Hospital observation <24hours & NOT admitted
SECTIONS A & Z
Sections A
■ To obtain key information to uniquely identifies each resident, the home in which he/she resides, and the reasons for the
assessment
■ Sections:
– A0050
– A0100
– A0200
– A0300
– A0310 – Type; A0310 A – H
■ H=Is this a SNF Part A PPS Discharge Assessment?
4
5
6
12/2/2020
3
Section V and Z
■ Section V
– Care Area Summary page
– Signatures and dates
■ Section Z
– RUGS data
– Info relating to past Interview scores
– Signatures and dates
Section A
Sections A & Z
A0410 A1510
A0500 A1550
A0600 A1600
A0700 A1700
A0800 A1800
A0900 A1900
A1000 A2000
A1100 A2100
A1200 A2200
A1300 A2300
A1500 A2400
Changes of Condition
■ Changes as compared to two last quarter and last comprehensive
MDS
■ Declines in two or more areas as listed in RAI manual Chapter 2
■ Improvements in two or more areas as listed in RAI manual Chapter 2
■ Start of Hospice
■ End of Hospice
7
8
9
12/2/2020
4
Steps for Conducting Assessments
■ Intent of each section
■ Quality of Life and Care Planning
■ Interview & Observe the resident
■ Interview staff
■ Interview family
■ Conduct a record review
SECTION BHEARING, SPEECH & VISION
Section B
■ B0100 – Comatose
■ B0200 – Hearing
■ B0300 – Hearing Aide
■ B0600 – Speech Clarity
■ B0700 – Makes Self Understood
■ B0800 – Ability to Understand Others
■ B1000 – Vision
■ B1200 – Corrective Lenses
10
11
12
12/2/2020
5
Section B
■ If any interviews conducted this B0700 should not be coded
“rarely or never understood.”
■ Inconsistencies in coding B0700 and interviews will be
evaluated.
THE INTERVIEWS
SECTIONS C - BIMS, D – PHQ9, F – PREFERENCES
Interviews – Coding instructions
■ All interviews
– Attempt to conduct interviews on ALL residents – not contingent on
B0700.
– If interpreter needed and not available on day of interview, code
interview should not be attempted and complete staff interview.
– If interview not conducted use standard dash on resident interview items
– Do not perform staff assessment if interview should have been
conducted and was not done – with exception of PPS.
13
14
15
12/2/2020
6
Interviews – Coding instructions
■ BIMS
– Conduct on ARD or day before – however can be conducted
anytime during seven day look back
■ Preference Interview
– Use preferred language and preferred method
– Conduct during the observation period
– Ensure interpreter as needed A1100
Interviews – Coding instructions
■ BIMS, PHQ-9 and Pain
– Use preferred language and preferred method
– If coded rarely or never understood perform staff assessment
– Ensure interpreter not needed A1100
APPENDIX DInterviewing to Increase
Resident Voice in MDS
Assessments
16
17
18
12/2/2020
7
Basic Approaches
■ Introduce yourself
■ Be sure the resident can hear what you are saying
■ Ask whether the resident would like an interpreter
■ Find a quiet, private area where you are not likely to be interrupted or
overheard
■ Sit where the resident can see you clearly
■ Establish rapport and respect
■ Explain the purpose of the questions to the resident
■ Say and show item responses
Basic Approaches
■ Ask the questions as they appear in the questionnaire
■ Break the question apart if necessary
– Unfolding
– Disentangling
■ Clarify
– Echoing
■ Repeat the response options as needed
■ Move to another question
■ Break up the interview if the resident becomes tired or needs to leave
for an appointment
Basic Approaches
■ Do not try to talk a resident out of an answer
■ Record the resident’s response not what you believe they should
have said
■ If the resident becomes deeply sorrowful or agitated
– Support emotional expression
■ Resident preferences may be difficult to discern
19
20
21
12/2/2020
8
Section C - BIMS OVERVIEW■ General information
– Decreases the chance of incorrect labeling of cognitive ability
– Improves detection of delirium
– Looking for trends over time – performance on tests should
be compared
– If performance worsens consider assessment for delirium or
depression
■ 90% of the residents can accomplish the interview
■ Conduct the interview on day before or day of ARD
■ Follow interview guidelines exactly – See suggested language
C0200 Repetition of three words
■ Ask the resident to repeat three words
– Sock, blue, bed
■ Inability to repeat on first attempt may indicate:
– Hearing problem, language barrier, inattention
■ Ask the question exactly as written
■ Immediately prompt for a response
■ Resident repeats all three correctly on first attempt
– Reinforce by repeating words with category cues
– This reinforcement is essential to evaluate ability to recall later
– Code the response
– Move on to the next interview question (C0300)
C0200 Repetition of three words
■ If the resident recalls two or fewer words on first attempt make a
second attempt using a category cues to prompt memory
■ Category cues help prompt recall, stimulate learning, foster
memory
– “Sock is something to wear”; “blue is a color”; “bed is a piece
of furniture”
■ If resident does not recall all the words on second move on to next
question
■ Additional info:
– Words may be recalled in any order
– Words may be recalled in any context
– Score the maximum number of words repeated on the first
attempt only
22
23
24
12/2/2020
9
C0300 Temporal Orientation
■ Asks three questions one at a time
– The year, the month, the day of the week
■ Allow up to 30 seconds for a response
■ Do not provide clues – if resident asks for clues tell them you
need to know they can answer without any assistance.
■ Resident may use environmental clues (calendar on wall)
■ For month count current day as day 1 for code 1 and code 2
when determining accuracy within 5 days or 6 days to 1 month
C0400 Recall
■ Ask the resident to repeat the words from the earlier question –
read as it appears exactly from MDS
■ Allow up to five seconds for recall
■ Provide category cues for any word not correctly recalled after
five seconds
■ Use category cues ONLY after resident is unable to recall one or
more words
■ Allow up to five seconds for recall after cues given
■ Code per instructions
C0500 Summary Score■ Scoring intent
– Allows comparisons (past and present scores)
– Decreases the chance of incorrect labeling of cognitive ability
– Improves detection of delirium
– Provides a more reliable estimate of resident function
– Allows staff to interact based on resident ability
■ DO NOT add up while interviewing resident
■ Acknowledge the score as part of the care planning process
■ Scoring
– 13-15: Cognitively Intact
– 8-12: Moderately Impaired
– 0-7: Severe Impairment
25
26
27
12/2/2020
10
Section C – Other components
■ C0600 – Staff assessment of mental status
■ C0700 – Short-term Memory
■ C0800 – Long-term Memory
■ C0900- Memory/Recall Ability
■ C1000 – Cognitive skills for Decision Making
■ C1310 – Signs & Symptoms of Delirium (CAM) – next slide
CAM – Confusion Assessment Method
■ C1310A – Acute Mental Status Change
– Code 0, no: If no evidence of acute mental status change from
resident’s baseline.
– Code 1, yes: If resident has an alteration in mental status
observed in the past 7 days or in the BIMS that represents a
change from baseline.
■ C1310 B – D Assessment of:
– Inattention
– Disorganized Thinking
– Altered Level of Consciousness
– Fluctuation vs. continuously present
CAM – Confusion Assessment Method
■ Assessment Steps:
– Observation during BIMS interview
– Interview of staff
– Review clinical record
– Interview family members
■ Codes
– Do all sources agree or disagree?
28
29
30
12/2/2020
11
CAM Scoring Methodology
Indication of Delirium by the CAM requires the presence of:
Item A = 1 OR Item B, C or D = 2
AND
Item B = 1 or 2
AND EITHER
Item C = 1 or 2 OR Item D = 1 or 2
SECTION D - MOOD
Section D - Mood
■ Intent
– To identify signs and symptoms of mood distress which can be
treatable
■ Process
– Utilizes a validated interview for assessment – PHQ-9
– Incorporates resident voice
– Screens for symptoms of depression
■ Coding the presence of indicators does not automatically
mean a diagnosis of depression or other mood disorder
– Complete section D Staff Assessment of Resident Mood only if an
interview cannot be completed – do not complete both
31
32
33
12/2/2020
12
D0100 Should Interview be Conducted?
– Coding yes or no
– Utilize information from section B to determine interview
D0100) & needs
■ B0700 Makes Self Understood / rarely or never understood – then code “0” (No) and
skip to staff assessment of mood D0500
– Review Language item A1100 to determine if the resident
needs or wants an interpreter to communicate
■ Have interpreter assist with interview
D0200 - PHQ - 9
■ Two columns for coding responses:
– Assesses for both the presence and the frequency of each symptom
■ Provides a standardized severity score at D0300
■ Utilize same interview guidelines previously discussed
– Some specifics provided related to this interview
■ Provides for 9 questions – to first identify for presence of indicators and then
to determine the frequency
■ Read each item as it is written – do not provide definitions; must be based
on the resident’s interpretation
D0200 - PHQ - 9
■ Look back is 14 days
■ You will need cue cards to show the resident – see handouts
– Never or 1 day; 2-6 days (several days); 7-11 days (half or more of the days;
12-14 days (nearly every day).
■ Conduct interview the day before or day of ARD
■ Code one frequency per item
■ Code “9” for any nonsensical response
■ Code higher frequency if resident has difficulty selecting between two options
■ NOT scoring for etiology – just presence of symptom(s)
34
35
36
12/2/2020
13
Explaining the Interview
■ Suggested language for reason
“I am going to ask you some questions about your mood and feelings over the past 2
weeks. I will also ask about some common problems that are known to go along
with feeling down. Some of the questions might seems personal, but everyone is
asked to answer them. This will help us provide you with better care.”
■ Suggested language for using cues
“I am going to ask you how often you have been bothered by a particular problems
over the last 2 weeks. I will give you the choices that you see on this card.” Say
while pointing to cue card . . .
D0300
■ Add numbers as documented in column two
■ Do not add these while conducting the interview
■ The interview is successfully completed if the resident answered
the frequency responses of at least 7 of the 9 items
■ If the symptom frequency is blank for 3 or more items, the
interview is deemed not complete. Total severity score is “99”
and the staff assessment of mood (D0500) should be conducted
D0300
■ Enter total severity score as a two-digit number 00-27
– 1-4: Minimal depression
– 5-9: Mild depression
– 10-14: Moderate depression
– 15-19: Moderately severe depression
– 20-27: Severe depression
■ Acknowledge the score as part of care planning
37
38
39
12/2/2020
14
SECTION F – CUSTOMARY ROUTINE AND ACTIVITIES
Section F Customary Routine & Preferences
Intent
To obtain information regarding the resident’s preferences for his/her daily
routine and activities.
Process
Review “making self understood B0700 to determine if understood at least
sometimes (0, 1, or 2)
Review “language” A1100 to determine if resident wants or needs interpreter.
Determine whether to conduct interview F0300
Conduct the interview verbally or by writing
Conduct staff assessment only if interview cannot be completed with resident
or a family member / representative– do not complete both
Coding – on a laminated card
■ 1 - VERY IMPORTANT
■ 2 - SOMEWHAT IMPORTANT
■ 3 - NOT VERY IMPORTANT
■ 4 - NOT IMPORTANT AT ALL
■ 5 - IMPORTANT, BUT CAN’T DO OR NO CHOICE
■ 9 - NO RESPONSE OR NON-RESPONSIVE
40
41
42
12/2/2020
15
Explaining the Interview
■ Suggested language for reason
“I am going to ask you some questions about your preferences about personal care
and activities. Even though you may be here for a short time, knowing your
preferences will help us to provide you with better care.”
■ Suggested language for using cues
“When I ask you a question about your preferences, I am going to ask you to choose
a response from the following” – show resident your response card
“Let me explain the choice – Important, but cannot do or not available – choose this
response if that preference is important to you but due to health or availability in
this facility you cannot do it – this will help us to provide an alternative to the
activity that will align with your preference.”
F0400 Interview for Daily Preferences
Choose what clothes to wear?
Take care of your personal belongings or things?
Choose between a tub bath, shower, bed bath, or sponge bath?
Have snacks available between meals?
Choose your own bedtime?
Have your family or close friend involved in discussions?
Use a phone in private?
Have a place to lock your things?
F0500 Interview for Activity Preferences
Same codes and process/tips for interview apply
You can get more specific with each of these when a resident states something is
important. For example, music.
Activity preferences
Have books, newspapers, and magazines to read?
Listen to music you like?
Be around animals such as pets?
Keep up with the news?
Do things with groups of people?
Do your favorite activities?
Go outside?
Participate in religious services or practices?
43
44
45
12/2/2020
16
F0600 Primary Respondent
■ This item establishes the source of the information regarding the
resident’s preferences, resident or other
■ If unable to interview either – go to F0700 answer yes “1” and
continue to F0800 for staff assessment of daily and activity
preferences.
Other information - Section F Interview
■ If total number of unanswered questions in F0400 through F0500 is
equal to 3 or more, the interview is considered incomplete.
■ F0700 – F0800 – Staff interview
– Completed only if family or resident not able to complete preference
interview
SECTION E - BEHAVIOR
46
47
48
12/2/2020
17
Section E - Behavior
■ Intent
– To identify behavioral symptoms in the last seven days that cause
distress to the resident, or are distressing or disruptive to facility
residents, staff members or the care environment.
■ Process
– Does not focus on intent or etiology of behavior just symptoms
– Interview staff, family or other and conduct chart review
– Understand psychosis definitions: Hallucinations, Delusions or
none of the above
Section E – Behavior E0100
■ Hallucinations
– The perception of the presence of something that is not actually there. It may be auditory or visual or involve smells,
tastes or touch
■ Delusions
■ A fixed, false belief not shared by others that the resident holds
even in the face of evidence to the contrary
■ Coding examples Chapter 3
Section E – Behavior
■ E0200 – Behavioral symptoms – presence and frequency
■ E0300 – Overall presence and skip patterns
■ E0500 – Impact on Resident
■ E0600 – Impact on Others
■ E0800 – Rejection of Care
■ E0900 – Wandering
■ E1000 – Wandering Impact
■ E1100 – Change in Behavior or other symptoms
■ Coding examples Chapter 3
49
50
51
12/2/2020
18
SECTION G – FUNCTIONAL STATUS
Section G – Functional Status
■ Intent
– To determine the resident’s functional status and need for assistance with
ADLs, altered gait and imbalance, decreased ROM and use of mobility
devices
– In addition, documenting resident and staff assessment about potential
for functional rehabilitation
■ Process steps for entire section
– 7-day look back
– Captures staff vs. family, visitors or others providing care
– Record review, interviews and direct observations
Section G – Functional Status
■ Coding G0110
– Remember to code for entire ADL definition
– Do NOT record the type and level of assistance the resident “should”
be receiving according to the written plan of care. Code what the
resident actually did in 7-day period – each shift
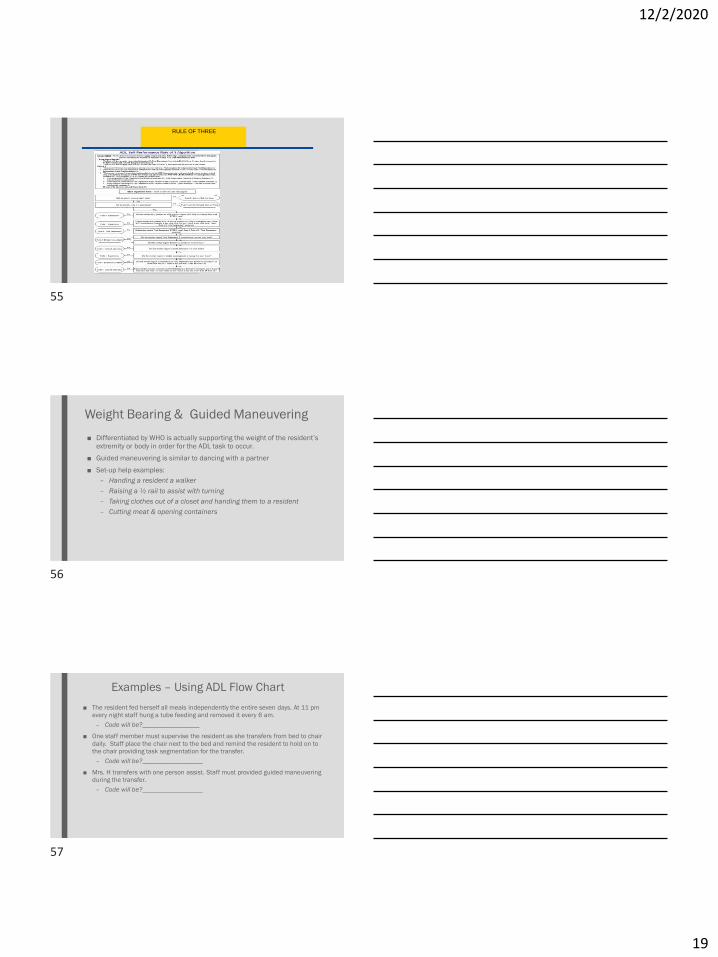
– Use the Rule of 3 – next slide
– Use the ADL Flow chart in the RAI manual to facilitate accurate coding
52
53
54
12/2/2020
19
RULE OF THREE
Weight Bearing & Guided Maneuvering
■ Differentiated by WHO is actually supporting the weight of the resident’s
extremity or body in order for the ADL task to occur.
■ Guided maneuvering is similar to dancing with a partner
■ Set-up help examples:
– Handing a resident a walker
– Raising a ½ rail to assist with turning
– Taking clothes out of a closet and handing them to a resident
– Cutting meat & opening containers
Examples – Using ADL Flow Chart
■ The resident fed herself all meals independently the entire seven days. At 11 pm
every night staff hung a tube feeding and removed it every 6 am.
– Code will be?_________________
■ One staff member must supervise the resident as she transfers from bed to chair
daily. Staff place the chair next to the bed and remind the resident to hold on to
the chair providing task segmentation for the transfer.
– Code will be?__________________
■ Mrs. H transfers with one person assist. Staff must provided guided maneuvering
during the transfer.
– Code will be?__________________
55
56
57
12/2/2020
20
G0300 Balance During Transitions & Walking
■ 7-day look back
■ Through 7-day look back staff should observe and document
■ If staff have not documented at least once during 7-day look back conduct the
assessment as follows:
– Explain the test to the resident
– Have assistive devices available
– Start with resident seated on edge of bed or chair and ask the resident to
stand and stay still for 3-5 seconds
– Ask the resident to walk 15 feet
– Ask the resident to turn around
– Ask the resident to prepare for toileting and sit on the toilet
– Ask the resident to transfer from surface to surface
G0400 Functional Limitation in ROM
■ 7-day look back
■ Functional limitation in range of motion is limited ability to move a joint that
interferes with daily functioning (particularly ADL’s) or places the resident at risk
of injury.
■ Interview staff, resident, resident family and observe
■ If there is a limitation does it interfere with function or place the resident at risk
for injury?
■ Assess range at joints indicated:
– Ask resident to follow verbal instructions
– Demonstrate each movement
– Actively assist as needed
G0400
■ Lower Extremity – includes hip, knee, ankle & foot
– While resident supine in a flat bed instruct to pull toes up towards head and push toes down away from head; lift leg one at a time
bending at the knee and then extend flat on bed.
■ Upper Extremity – includes shoulder, elbow, wrist & fingers
– While seated, open and close hand; place both hands and touch palms to back of head; touch each shoulder with opposite hand.
58
59
60
12/2/2020
21
G0600 – G0900
■ Mobility Devices
– Observe and interview
– Check all that apply
■ Functional Rehabilitative Potential
– Completed only on first OBRA or PPS assessment A0310A=1
– Interview: Find out from resident what staff do for him/her. Then ask, “Do
you think that you could get to a point where you do more or all of the
activity yourself?”
– Closely aligned with section O Rehabilitation services and also Restorative
services
Resources
■ LeadingAge.org
■ OHCA.org
■ Joy Ramsby, M.Ed. 503-407-1488 - [email protected]
■ https://www.aanac.org/Information/Government-Source-Documents
■ https://www.cms.gov/medicare/medicare-fee-for-service-
payment/snfpps/pdpm.html
■ QRP Manual
– https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment
61
62
63
12/2/2020
22
64