Embed Size (px)
Citation preview

www.escardio.org
Device therapy in heartfailure
Update of the ESC guidelines
Professor of Medicine
Department of emergency and cardiovascular medicine
Sahlgrenska Academy
University of Gothenburg, Sweden
Karl Swedberg
Disclosure
No conflicts in relation to this presentation
www.escardio.org
2010 Focused Update of ESC Guidelines on
Device Therapy in Heart Failure
An Update of the 2008 ESC guidelines for the Diagnosis and Treatment of Acute and Chronic
Heart Failure and the 2007 ESC guidelines for Cardiac and Resynchronization Therapy,
developed in collaboration with the HFA and EHRA
Authors/Task Force Members: Kenneth Dickstein* (Chairperson) (Norway), Panos E. Vardas** (Chairperson) (Greece),
Angelo Auricchio (Switzerland), Jean-Claude Daubert (France), Cecilia Linde (Sweden), John McMurray (UK), Piotr
Ponikowski (Poland), Silvia Giuliana Priori (Italy), Richard Sutton (UK), Dirk van Veldhuisen (Netherlands)
ESC Committee for Practice Guidelines (CPG): Alec Vahanian (Chairperson) (France), Angelo Auricchio (Switzerland),
Jeroen Bax (The Netherlands), Claudio Ceconi (Italy), Veronica Dean (France), Gerasimos Filippatos (Greece), Christian
Funck-Brentano (France), Richard Hobbs (UK), Peter Kearney (Ireland), Theresa McDonagh (UK), Bogdan A. Popescu
(Romania), Zeljko Reiner (Croatia), Udo Sechtem (Germany), Per Anton Sirnes (Norway), Michal Tendera (Poland), Panos
Vardas (Greece), Petr Widimsky (Czech Republic)
Document Reviewers, Michal Tendera (CPG Review Coordinator) (Poland), Stefan D. Anker (Germany), Jean-Jacques
Blanc (France), Maurizio Gasparini (Italy), Arno W. Hoes (Netherlands), Carsten W. Israel (Germany), Zbigniew Kalarus
(Poland), Bela Merkely (Hungary), Karl Swedberg (Sweden), A. John Camm (UK)
European Heart Journal
doi:10.1093/eurheartj/ehq337
www.escardio.org
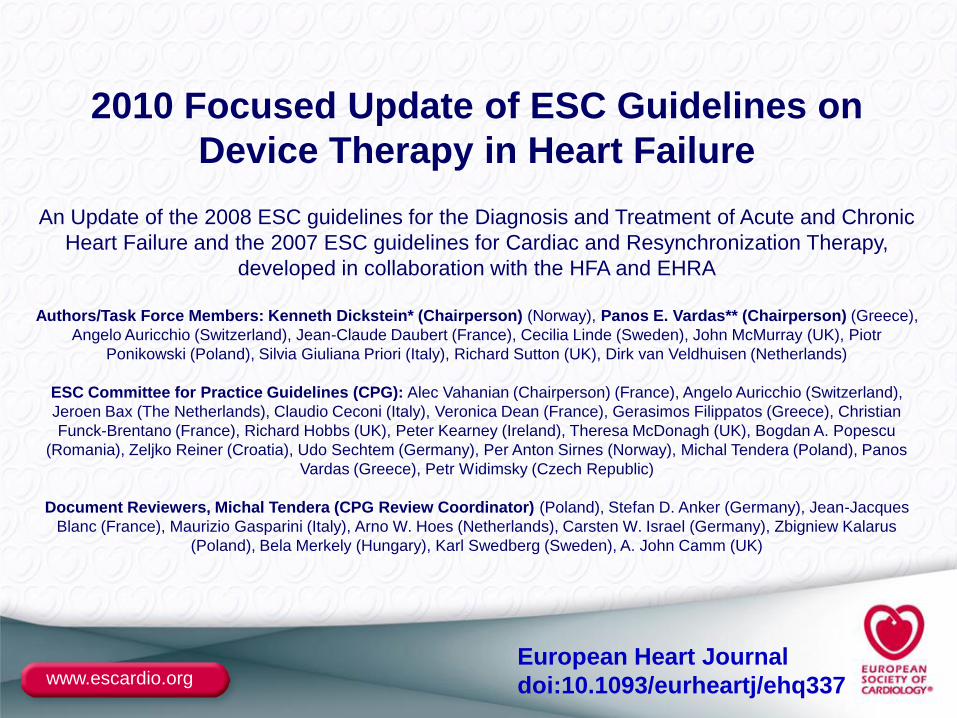
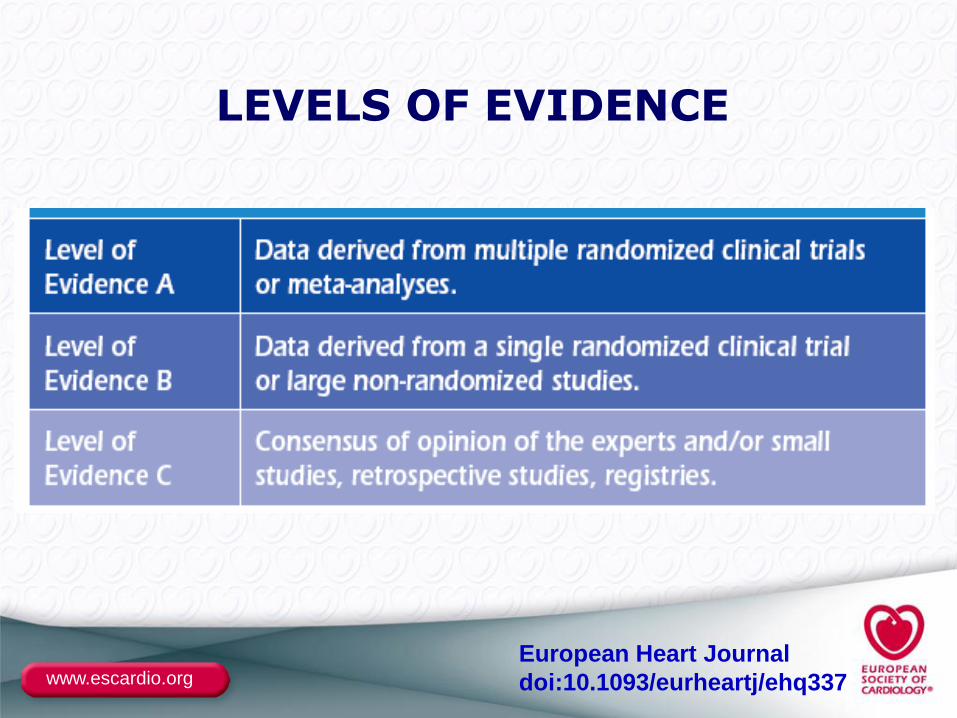
Classes of Recommendations
DefinitionSuggested wording
to useClass I Evidence and/or general
agreement that a given treatment or procedure is beneficial, useful, effective.
Is recommended/is indicated
Class II Conflicting evidence and/or a divergence of opinion about the usefulness/efficacy of the given treatment or procedure.
Class IIa Weight of evidence/opinion is in favour of usefulness/efficacy.
Should be considered
Class IIb Usefulness/efficacy is less well established by evidence/opinion.
May be considered
Class III Evidence or general agreement that the given treatment or procedure is not useful/effective, and in some cases may be harmful.
Is not recommended
European Heart Journal
doi:10.1093/eurheartj/ehq337
www.escardio.org
LEVELS OF EVIDENCE
European Heart Journal
doi:10.1093/eurheartj/ehq337
www.escardio.org
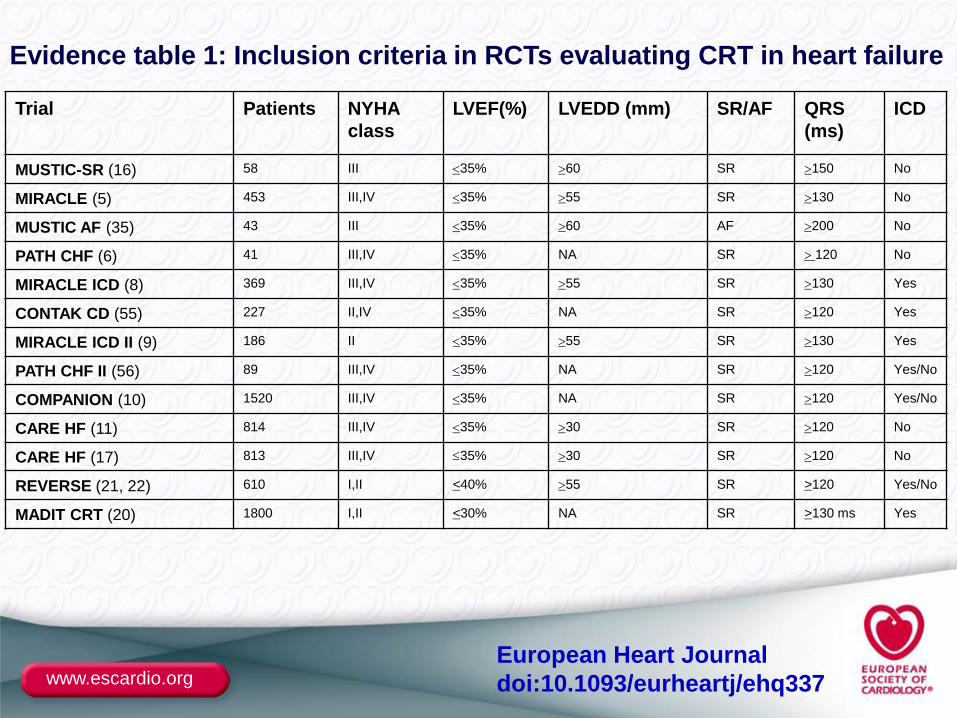
Evidence table 1: Inclusion criteria in RCTs evaluating CRT in heart failure
Trial Patients NYHA
class
LVEF(%) LVEDD (mm) SR/AF QRS
(ms)
ICD
MUSTIC-SR (16) 58 III 35% 60 SR 150 No
MIRACLE (5) 453 III,IV 35% 55 SR 130 No
MUSTIC AF (35) 43 III 35% 60 AF 200 No
PATH CHF (6) 41 III,IV 35% NA SR 120 No
MIRACLE ICD (8) 369 III,IV 35% 55 SR 130 Yes
CONTAK CD (55) 227 II,IV 35% NA SR 120 Yes
MIRACLE ICD II (9) 186 II 35% 55 SR 130 Yes
PATH CHF II (56) 89 III,IV 35% NA SR 120 Yes/No
COMPANION (10) 1520 III,IV 35% NA SR 120 Yes/No
CARE HF (11) 814 III,IV 35% 30 SR 120 No
CARE HF (17) 813 III,IV 35% 30 SR 120 No
REVERSE (21, 22) 610 I,II <40% 55 SR >120 Yes/No
MADIT CRT (20) 1800 I,II <30% NA SR >130 ms Yes
European Heart Journal
doi:10.1093/eurheartj/ehq337
www.escardio.org
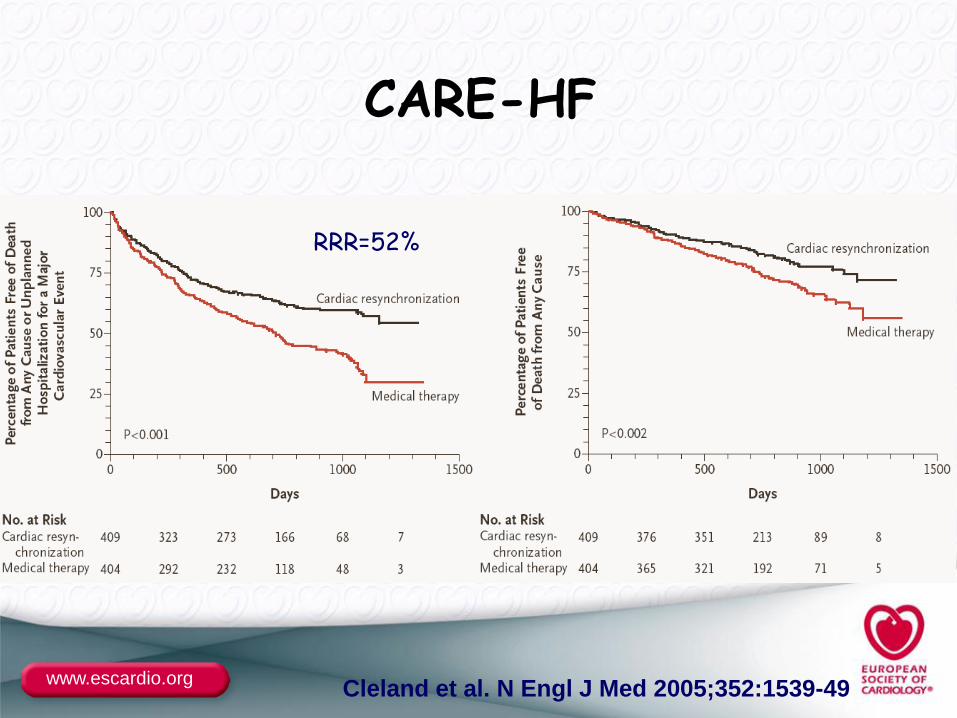
CARE-HF
Mortality or CV hospitalisation
Cleland et al. N Engl J Med 2005;352:1539-49
RRR=52%
www.escardio.org
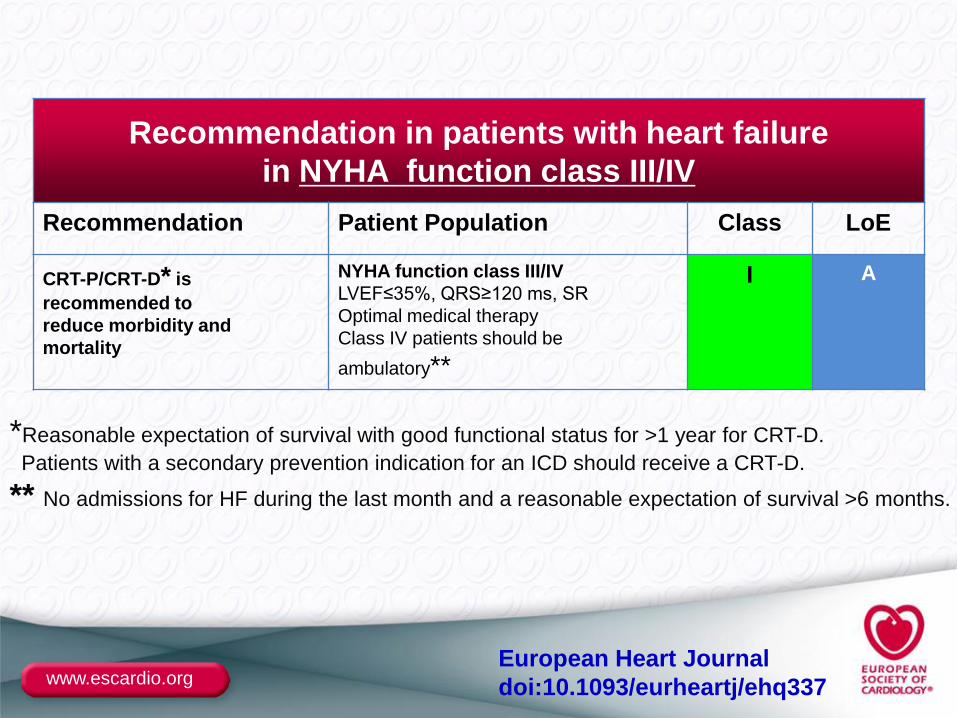
Recommendation in patients with heart failure
in NYHA function class III/IV
Recommendation Patient Population Class LoE
CRT-P/CRT-D* is
recommended to
reduce morbidity and
mortality
NYHA function class III/IV
LVEF≤35%, QRS≥120 ms, SR
Optimal medical therapy
Class IV patients should be
ambulatory**
I A
*Reasonable expectation of survival with good functional status for >1 year for CRT-D.
Patients with a secondary prevention indication for an ICD should receive a CRT-D.
** No admissions for HF during the last month and a reasonable expectation of survival >6 months.
European Heart Journal
doi:10.1093/eurheartj/ehq337
www.escardio.org
Key points:
• New: LV dilatation no longer required
• New: Class IV patients should be ambulatory
• New: Reasonable expectation of survival with good
functional status for >1 year for CRT-D
• Evidence is strongest for patients with typical LBBB
• Similar level of evidence for CRT-P and CRT-D
CRT-P/CRT-D in patients with heart failure
in NYHA function class III/IV
European Heart Journal
doi:10.1093/eurheartj/ehq337
www.escardio.org
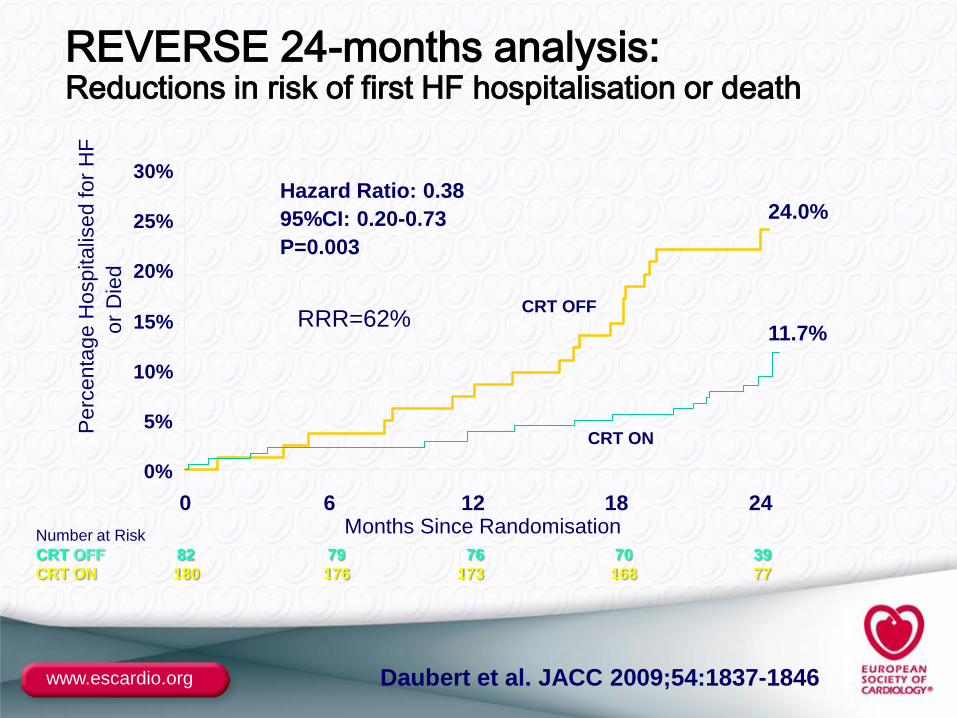
Number at Risk
CRT OFF 82 79 76 70 39
CRT ON 180 176 173 168 77
Daubert et al. JACC 2009;54:1837-1846
REVERSE 24-months analysis:Reductions in risk of first HF hospitalisation or death
0%
5%
10%
15%
20%
25%
30%
0 6 12 18 24Months Since Randomisation
Perc
enta
ge H
ospitalis
ed for
HF
or
Die
d
CRT ON
CRT OFF
24.0%
11.7%
Hazard Ratio: 0.38
95%CI: 0.20-0.73
P=0.003
RRR=62%
www.escardio.org N Engl J Med 2009;361
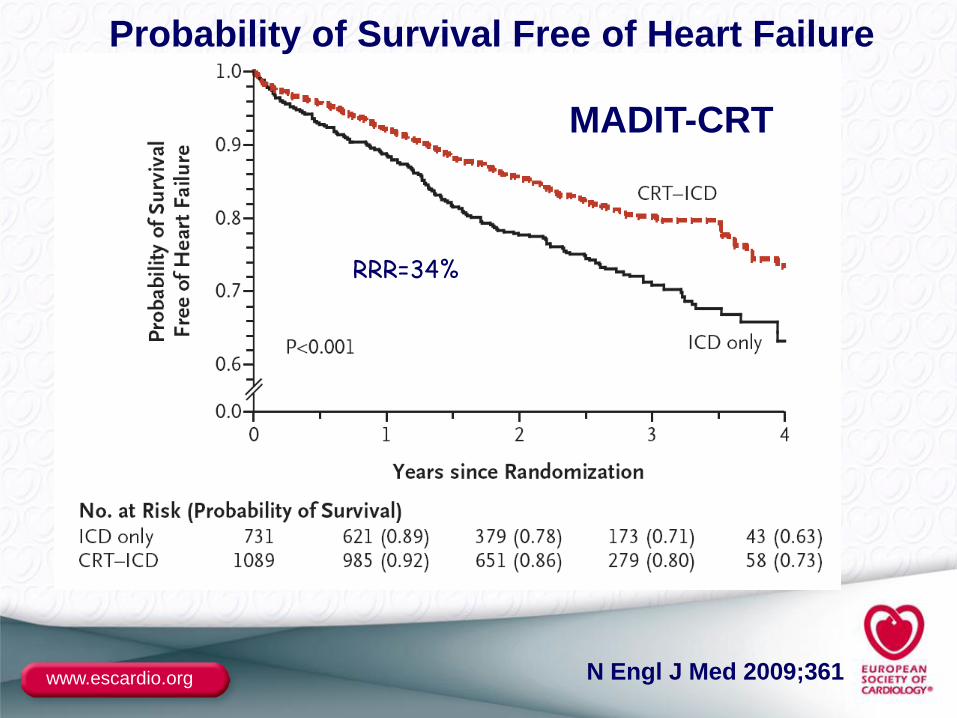
Probability of Survival Free of Heart Failure
MADIT-CRT
RRR=34%
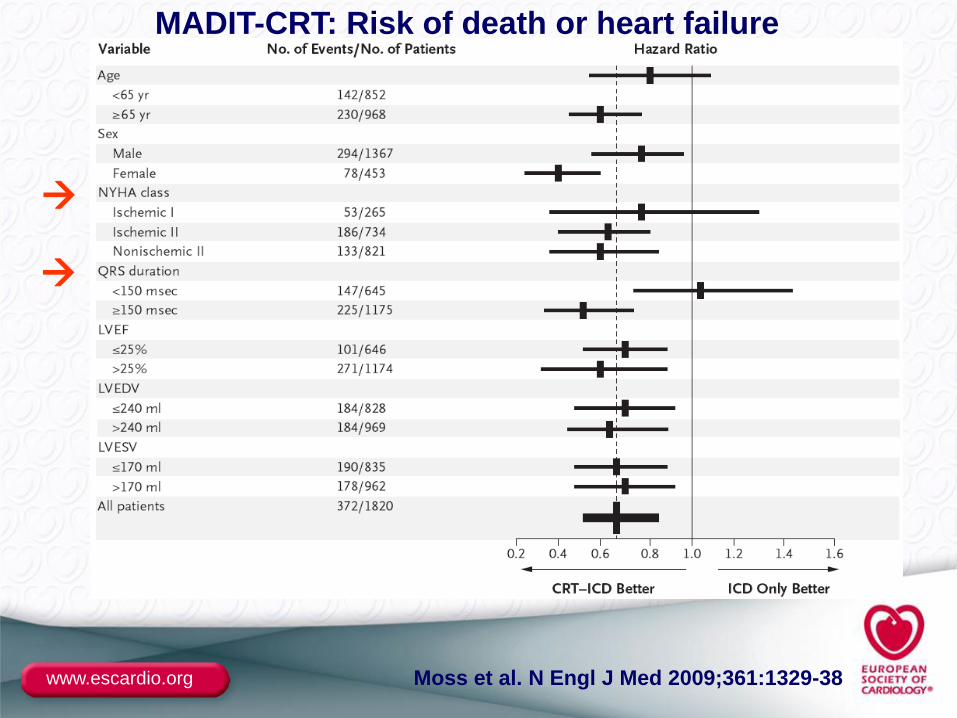
www.escardio.org Moss et al. N Engl J Med 2009;361:1329-38
MADIT-CRT: Risk of death or heart failure
www.escardio.org
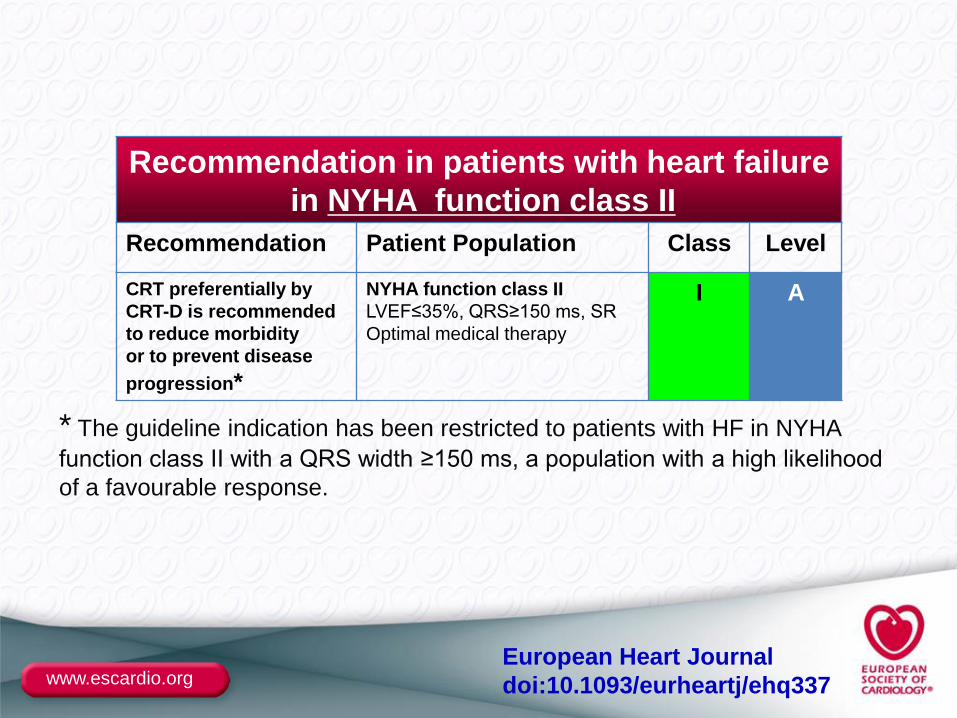
Recommendation in patients with heart failure
in NYHA function class II
Recommendation Patient Population Class Level
CRT preferentially by
CRT-D is recommended
to reduce morbidity
or to prevent disease
progression*
NYHA function class II
LVEF≤35%, QRS≥150 ms, SR
Optimal medical therapy
I A
* The guideline indication has been restricted to patients with HF in NYHA
function class II with a QRS width ≥150 ms, a population with a high likelihood
of a favourable response.
European Heart Journal
doi:10.1093/eurheartj/ehq337
www.escardio.org
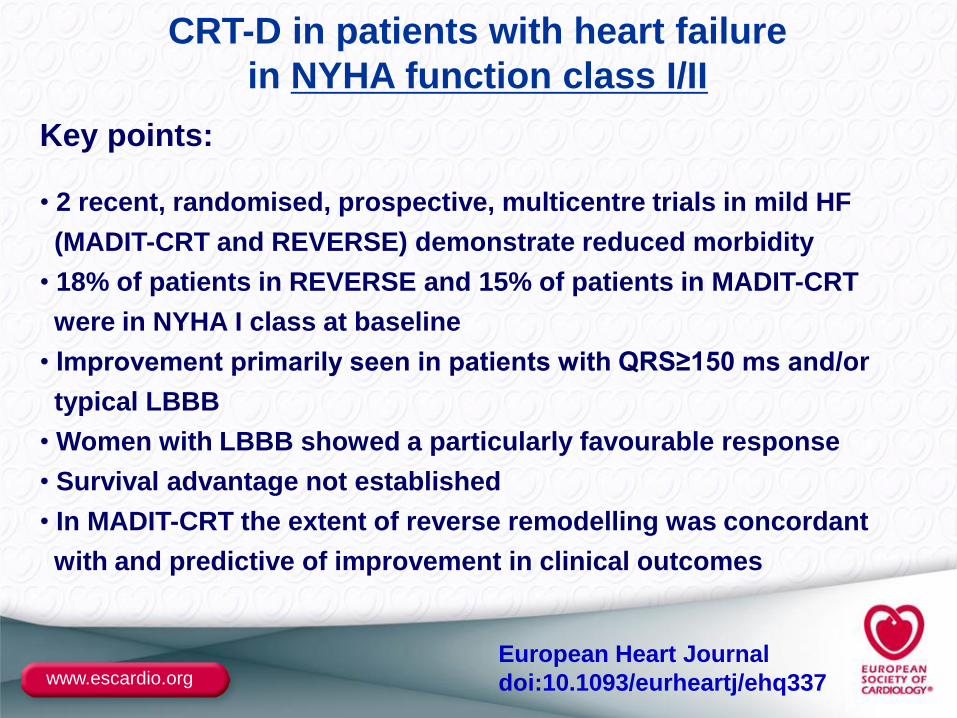
CRT-D in patients with heart failure
in NYHA function class I/II
Key points:
• 2 recent, randomised, prospective, multicentre trials in mild HF
(MADIT-CRT and REVERSE) demonstrate reduced morbidity
• 18% of patients in REVERSE and 15% of patients in MADIT-CRT
were in NYHA I class at baseline
• Improvement primarily seen in patients with QRS≥150 ms and/or
typical LBBB
• Women with LBBB showed a particularly favourable response
• Survival advantage not established
• In MADIT-CRT the extent of reverse remodelling was concordant
with and predictive of improvement in clinical outcomes
European Heart Journal
doi:10.1093/eurheartj/ehq337
RAFT
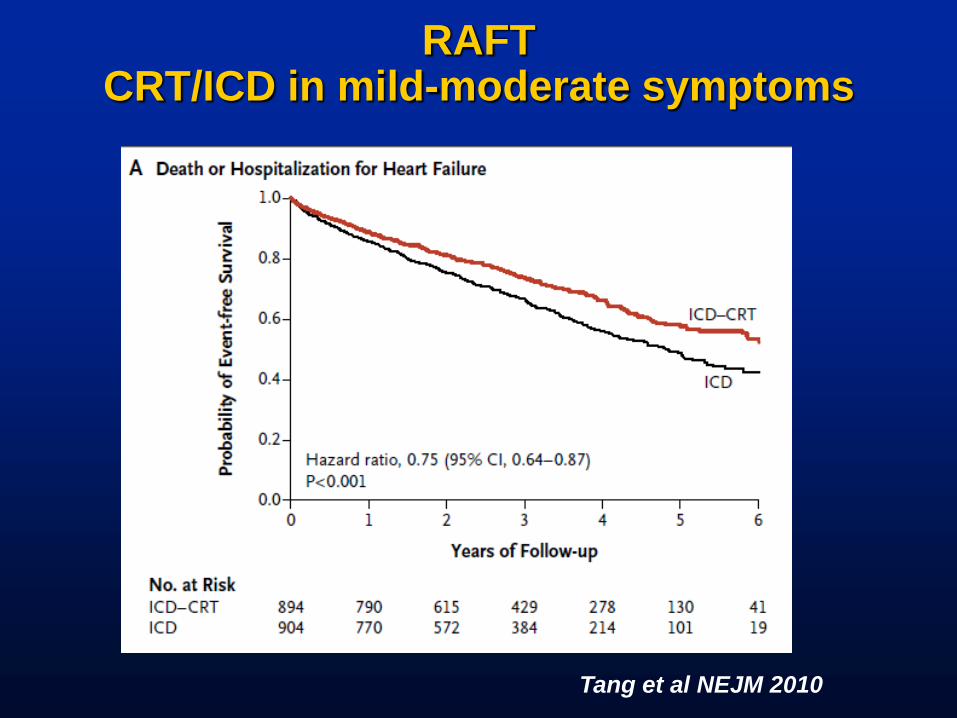
RAFTCRT/ICD in mild-moderate symptoms
Tang et al NEJM 2010
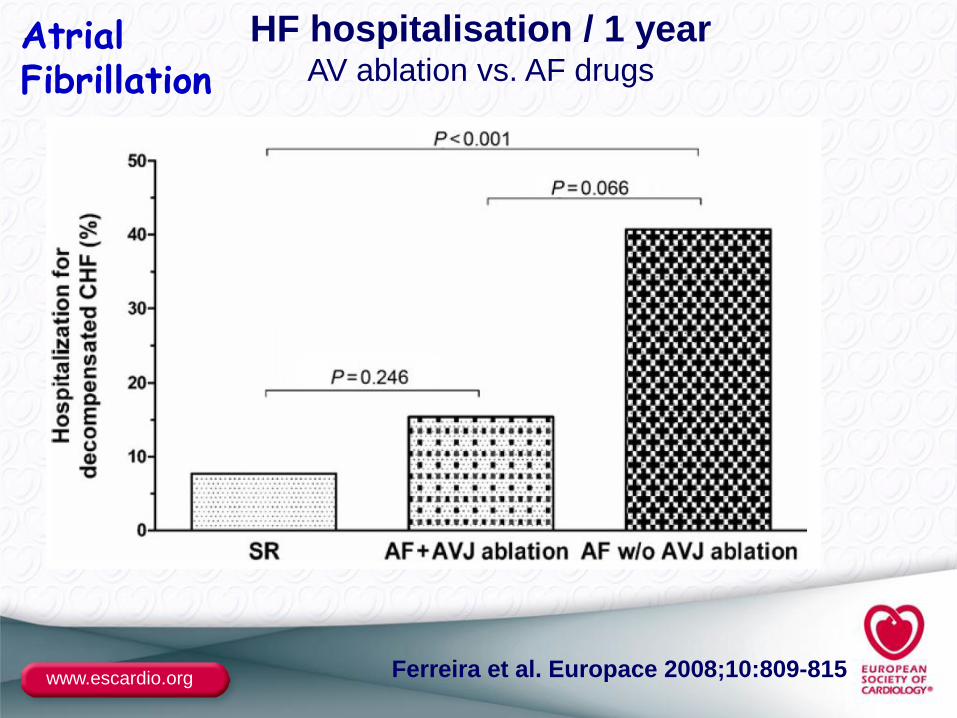
www.escardio.org Ferreira et al. Europace 2008;10:809-815
HF hospitalisation / 1 yearAV ablation vs. AF drugs
AtrialFibrillation
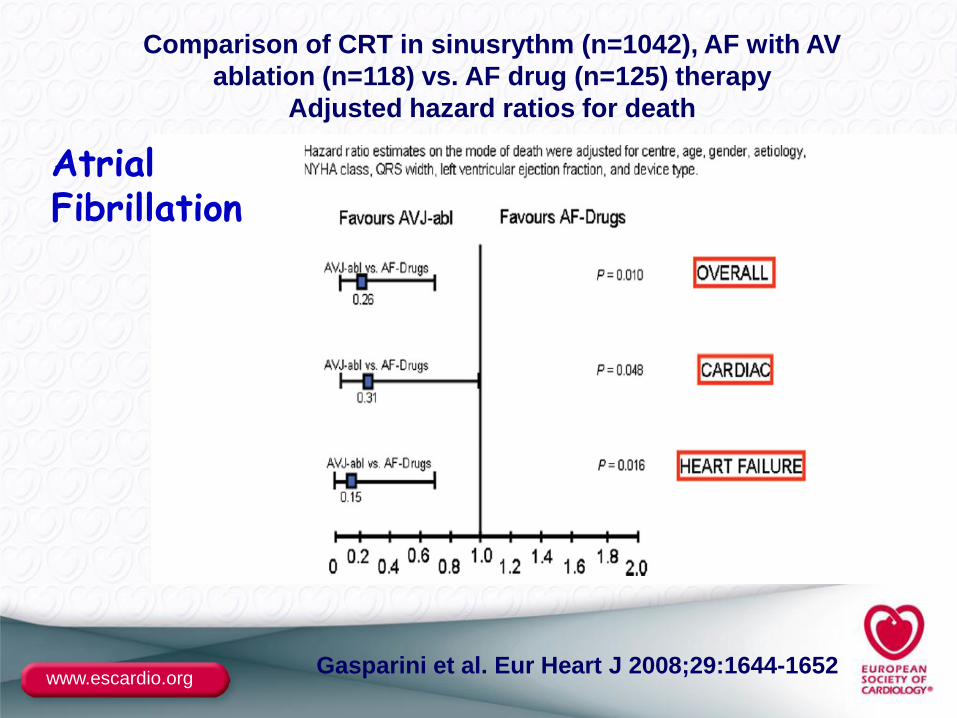
www.escardio.orgGasparini et al. Eur Heart J 2008;29:1644-1652
Comparison of CRT in sinusrythm (n=1042), AF with AV
ablation (n=118) vs. AF drug (n=125) therapy
Adjusted hazard ratios for death
AtrialFibrillation
www.escardio.org
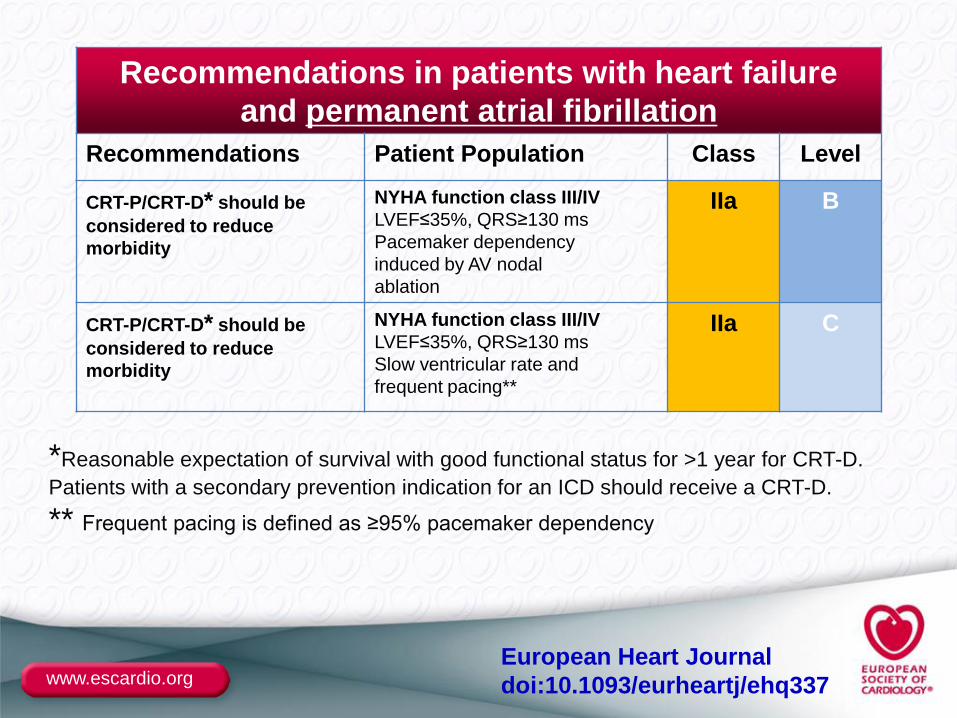
Recommendations in patients with heart failure
and permanent atrial fibrillation
Recommendations Patient Population Class Level
CRT-P/CRT-D* should be
considered to reduce
morbidity
NYHA function class III/IV
LVEF≤35%, QRS≥130 ms
Pacemaker dependency
induced by AV nodal
ablation
IIa B
CRT-P/CRT-D* should be
considered to reduce
morbidity
NYHA function class III/IV
LVEF≤35%, QRS≥130 ms
Slow ventricular rate and
frequent pacing**
IIa C
*Reasonable expectation of survival with good functional status for >1 year for CRT-D.
Patients with a secondary prevention indication for an ICD should receive a CRT-D.
** Frequent pacing is defined as ≥95% pacemaker dependency
European Heart Journal
doi:10.1093/eurheartj/ehq337
www.escardio.org
CRT-P/CRT-D in patients with heart failure
and permanent atrial fibrillation
Key points:
• Approximately 1/5 of CRT implantations in Europe are in
patients with permanent AF
• NYHA class III/IV symptoms and an LVEF ≤35% are
well-established indications for ICD
• Frequent pacing is defined as ≥95% pacemaker dependency
• AV nodal ablation may be required to assure adequate pacing
• Evidence strongest for patients with an LBBB pattern
• Insufficient evidence for mortality recommendation
European Heart Journal
doi:10.1093/eurheartj/ehq337
www.escardio.org
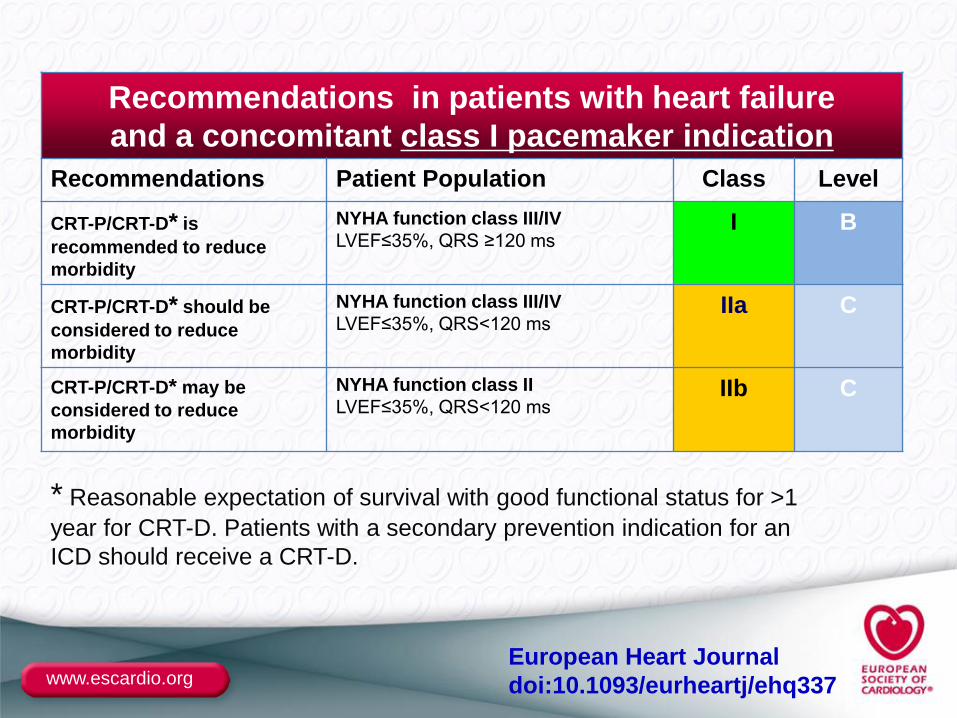
Recommendations in patients with heart failure
and a concomitant class I pacemaker indication
Recommendations Patient Population Class Level
CRT-P/CRT-D* is
recommended to reduce
morbidity
NYHA function class III/IV
LVEF≤35%, QRS ≥120 msI B
CRT-P/CRT-D* should be
considered to reduce
morbidity
NYHA function class III/IV
LVEF≤35%, QRS<120 msIIa C
CRT-P/CRT-D* may be
considered to reduce
morbidity
NYHA function class II
LVEF≤35%, QRS<120 msIIb C
* Reasonable expectation of survival with good functional status for >1
year for CRT-D. Patients with a secondary prevention indication for an
ICD should receive a CRT-D.
European Heart Journal
doi:10.1093/eurheartj/ehq337
www.escardio.org
CRT-P/CRT-D in patients with heart failure
and a conventional pacemaker indication
Key points:
•In patients with a conventional indication for pacing, NYHA III/IV
symptoms, LVEF ≤35%, QRS width ≥120 ms, a CRT-P/CRT-D is indicated
•RV pacing will induce dyssynchrony
•Chronic RV pacing in patients with LV dysfunction should be avoided
•CRT may permit adequate uptitration of beta-blocker treatment
European Heart Journal
doi:10.1093/eurheartj/ehq337
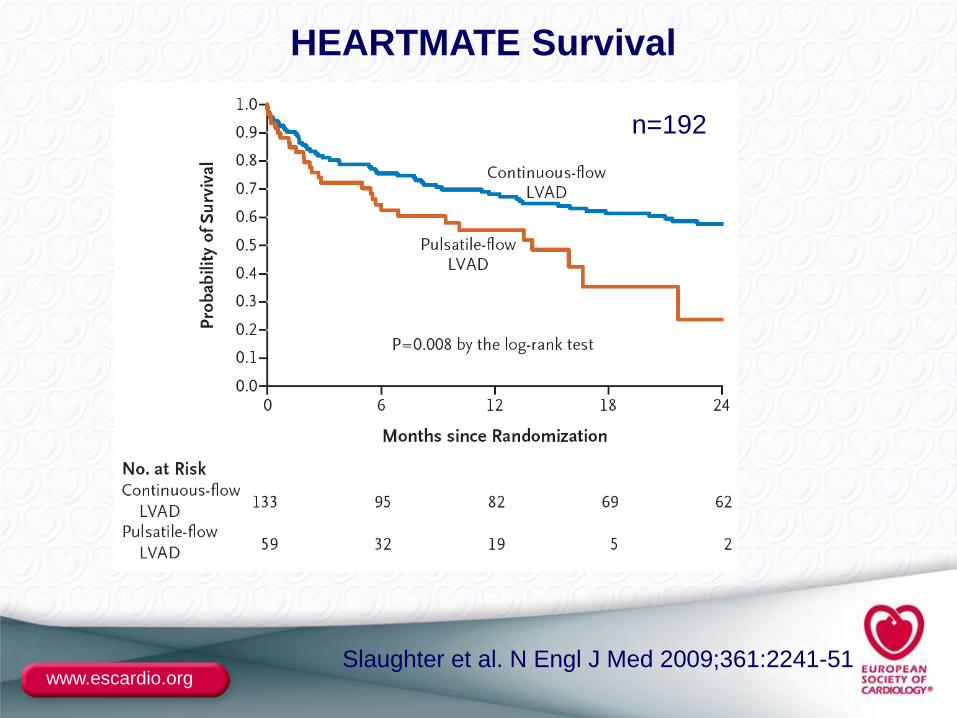
www.escardio.orgSlaughter et al. N Engl J Med 2009;361:2241-51
HEARTMATE Survival
n=192
www.escardio.org
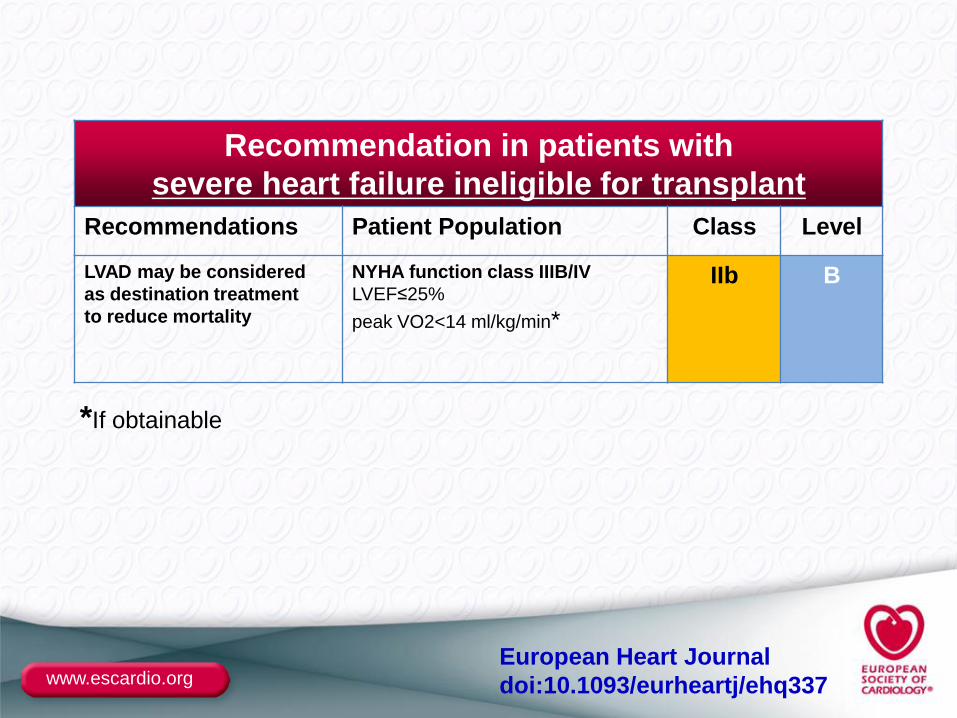
Recommendation in patients with
severe heart failure ineligible for transplant
Recommendations Patient Population Class Level
LVAD may be considered
as destination treatment
to reduce mortality
NYHA function class IIIB/IV
LVEF≤25%
peak VO2<14 ml/kg/min*
IIb B
*If obtainable
European Heart Journal
doi:10.1093/eurheartj/ehq337
www.escardio.org
Left Ventricular Assist Device as destination therapy for
patients with severe HF ineligible for cardiac transplantation
Key points:
• The NIH INTERMACS registry indicates that ~10% of
patients in clinical practice receive an LVAD as destination therapy
• Patient population mainly consists of patients on inotropic (and/or
mechanical) support prior to LVAD implantation
• Patient selection is crucial and candidates should not have significant
renal, pulmonary or hepatic dysfunction or infection
• The available evidence suggests that a continuous flow device is
superior to a pulsatile flow device
• No controlled data available as bridge to heart transplantation
European Heart Journal
doi:10.1093/eurheartj/ehq337
www.escardio.org
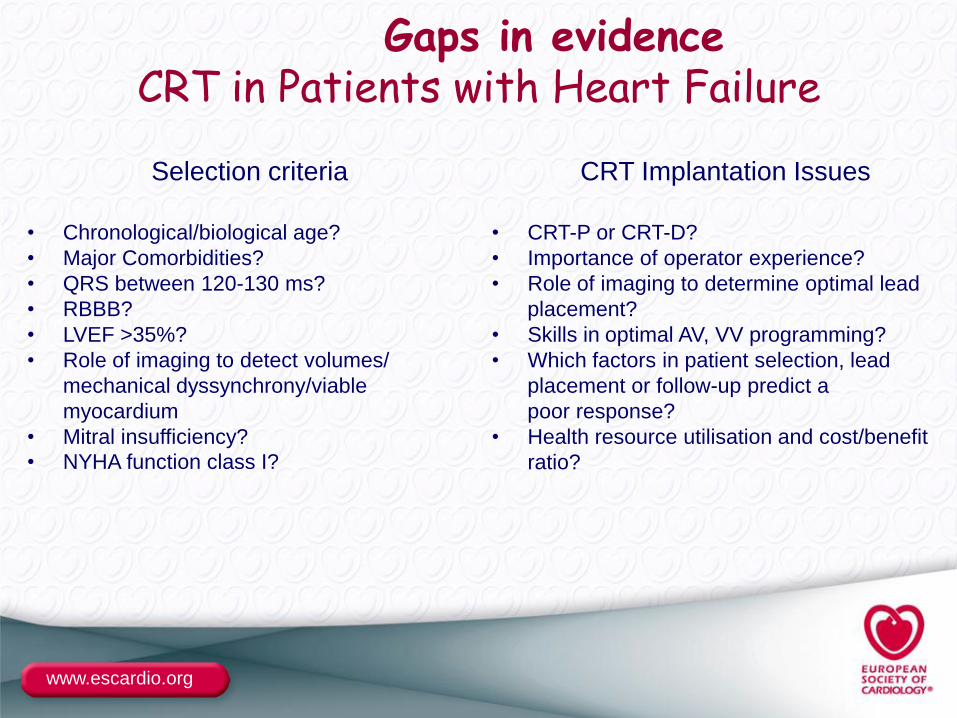
Gaps in evidenceCRT in Patients with Heart Failure
Selection criteria CRT Implantation Issues
• Chronological/biological age?
• Major Comorbidities?
• QRS between 120-130 ms?
• RBBB?
• LVEF >35%?
• Role of imaging to detect volumes/
mechanical dyssynchrony/viable
myocardium
• Mitral insufficiency?
• NYHA function class I?
• CRT-P or CRT-D?
• Importance of operator experience?
• Role of imaging to determine optimal lead
placement?
• Skills in optimal AV, VV programming?
• Which factors in patient selection, lead
placement or follow-up predict a
poor response?
• Health resource utilisation and cost/benefit
ratio?
www.escardio.org
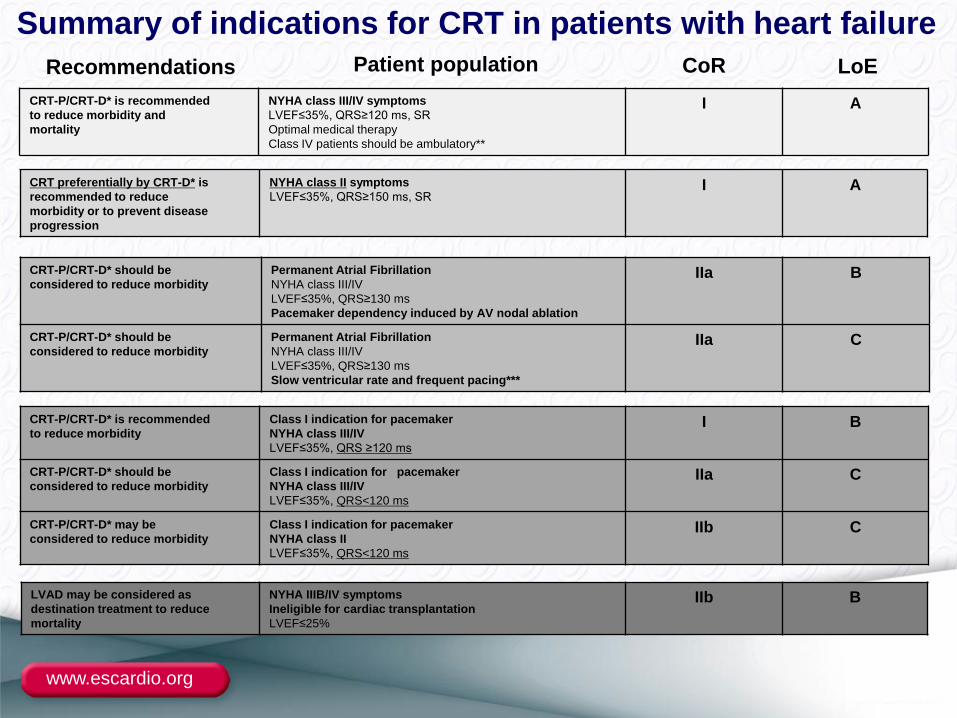
CRT-P/CRT-D* is recommended
to reduce morbidity and
mortality
NYHA class III/IV symptoms
LVEF≤35%, QRS≥120 ms, SR
Optimal medical therapy
Class IV patients should be ambulatory**
I A
CRT preferentially by CRT-D* is
recommended to reduce
morbidity or to prevent disease
progression
NYHA class II symptoms
LVEF≤35%, QRS≥150 ms, SRI A
CRT-P/CRT-D* should be
considered to reduce morbidity
Permanent Atrial Fibrillation
NYHA class III/IV
LVEF≤35%, QRS≥130 ms
Pacemaker dependency induced by AV nodal ablation
IIa B
CRT-P/CRT-D* should be
considered to reduce morbidity
Permanent Atrial Fibrillation
NYHA class III/IV
LVEF≤35%, QRS≥130 ms
Slow ventricular rate and frequent pacing***
IIa C
Summary of indications for CRT in patients with heart failure
CRT-P/CRT-D* is recommended
to reduce morbidity
Class I indication for pacemaker
NYHA class III/IV
LVEF≤35%, QRS ≥120 ms
I B
CRT-P/CRT-D* should be
considered to reduce morbidity
Class I indication for pacemaker
NYHA class III/IV
LVEF≤35%, QRS<120 ms
IIa C
CRT-P/CRT-D* may be
considered to reduce morbidity
Class I indication for pacemaker
NYHA class II
LVEF≤35%, QRS<120 ms
IIb C
Patient populationRecommendations CoR LoE
LVAD may be considered as
destination treatment to reduce
mortality
NYHA IIIB/IV symptoms
Ineligible for cardiac transplantation
LVEF≤25%
IIb B
www.escardio.org
●BACKUP
www.escardio.org
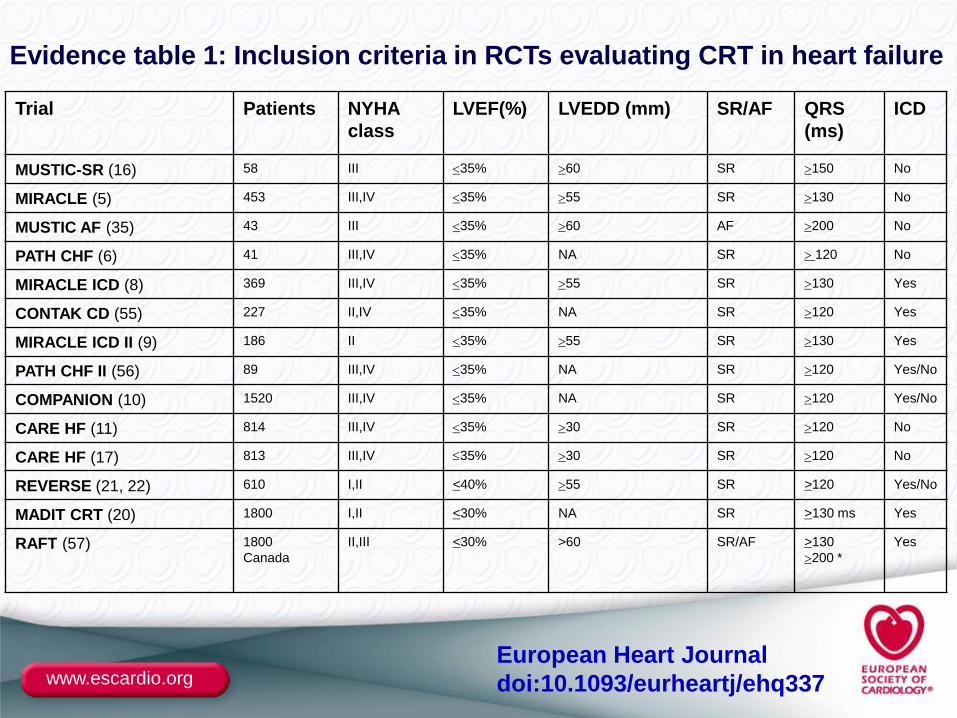
Evidence table 1: Inclusion criteria in RCTs evaluating CRT in heart failure
Trial Patients NYHA
class
LVEF(%) LVEDD (mm) SR/AF QRS
(ms)
ICD
MUSTIC-SR (16) 58 III 35% 60 SR 150 No
MIRACLE (5) 453 III,IV 35% 55 SR 130 No
MUSTIC AF (35) 43 III 35% 60 AF 200 No
PATH CHF (6) 41 III,IV 35% NA SR 120 No
MIRACLE ICD (8) 369 III,IV 35% 55 SR 130 Yes
CONTAK CD (55) 227 II,IV 35% NA SR 120 Yes
MIRACLE ICD II (9) 186 II 35% 55 SR 130 Yes
PATH CHF II (56) 89 III,IV 35% NA SR 120 Yes/No
COMPANION (10) 1520 III,IV 35% NA SR 120 Yes/No
CARE HF (11) 814 III,IV 35% 30 SR 120 No
CARE HF (17) 813 III,IV 35% 30 SR 120 No
REVERSE (21, 22) 610 I,II <40% 55 SR >120 Yes/No
MADIT CRT (20) 1800 I,II <30% NA SR >130 ms Yes
RAFT (57) 1800
Canada
II,III <30% >60 SR/AF >130
200 *
Yes
European Heart Journal
doi:10.1093/eurheartj/ehq337
www.escardio.org
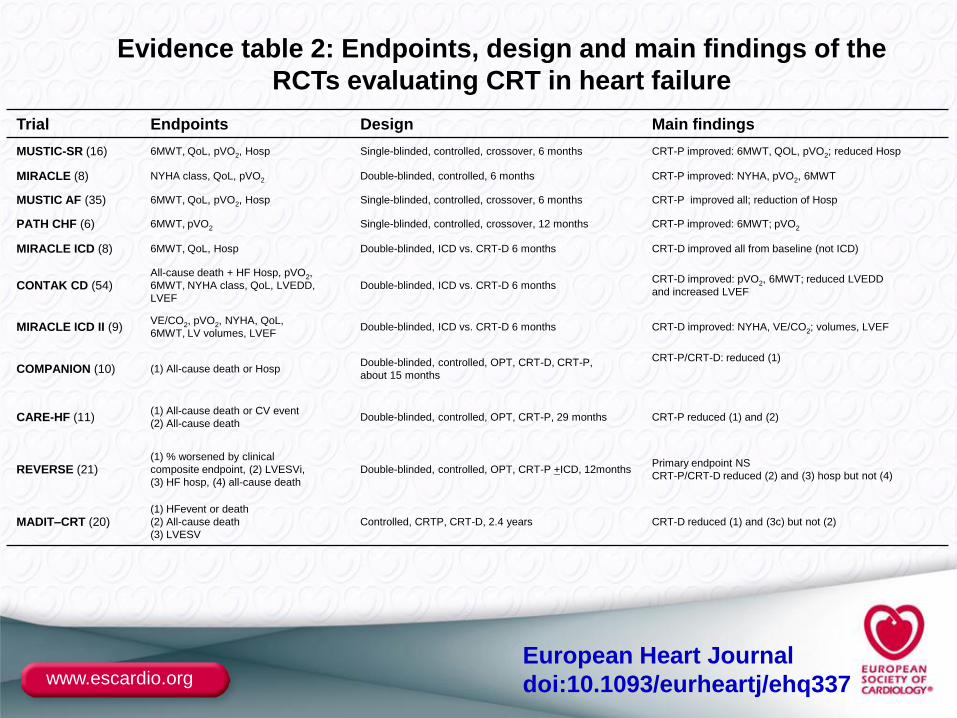
Trial Endpoints Design Main findings
MUSTIC-SR (16) 6MWT, QoL, pVO2, Hosp Single-blinded, controlled, crossover, 6 months CRT-P improved: 6MWT, QOL, pVO2; reduced Hosp
MIRACLE (8) NYHA class, QoL, pVO2 Double-blinded, controlled, 6 months CRT-P improved: NYHA, pVO2, 6MWT
MUSTIC AF (35) 6MWT, QoL, pVO2, Hosp Single-blinded, controlled, crossover, 6 months CRT-P improved all; reduction of Hosp
PATH CHF (6) 6MWT, pVO2 Single-blinded, controlled, crossover, 12 months CRT-P improved: 6MWT; pVO2
MIRACLE ICD (8) 6MWT, QoL, Hosp Double-blinded, ICD vs. CRT-D 6 months CRT-D improved all from baseline (not ICD)
CONTAK CD (54)All-cause death + HF Hosp, pVO2,
6MWT, NYHA class, QoL, LVEDD,
LVEF
Double-blinded, ICD vs. CRT-D 6 monthsCRT-D improved: pVO2, 6MWT; reduced LVEDD
and increased LVEF
MIRACLE ICD II (9)VE/CO2, pVO2, NYHA, QoL,
6MWT, LV volumes, LVEF Double-blinded, ICD vs. CRT-D 6 months CRT-D improved: NYHA, VE/CO2; volumes, LVEF
COMPANION (10) (1) All-cause death or HospDouble-blinded, controlled, OPT, CRT-D, CRT-P,
about 15 months
CRT-P/CRT-D: reduced (1)
CARE-HF (11)(1) All-cause death or CV event
(2) All-cause death Double-blinded, controlled, OPT, CRT-P, 29 months CRT-P reduced (1) and (2)
REVERSE (21)(1) % worsened by clinical
composite endpoint, (2) LVESVi,
(3) HF hosp, (4) all-cause death
Double-blinded, controlled, OPT, CRT-P +ICD, 12months Primary endpoint NS
CRT-P/CRT-D reduced (2) and (3) hosp but not (4)
MADIT–CRT (20)(1) HFevent or death
(2) All-cause death
(3) LVESV
Controlled, CRTP, CRT-D, 2.4 years CRT-D reduced (1) and (3c) but not (2)
Evidence table 2: Endpoints, design and main findings of the
RCTs evaluating CRT in heart failure
European Heart Journal
doi:10.1093/eurheartj/ehq337
www.escardio.org
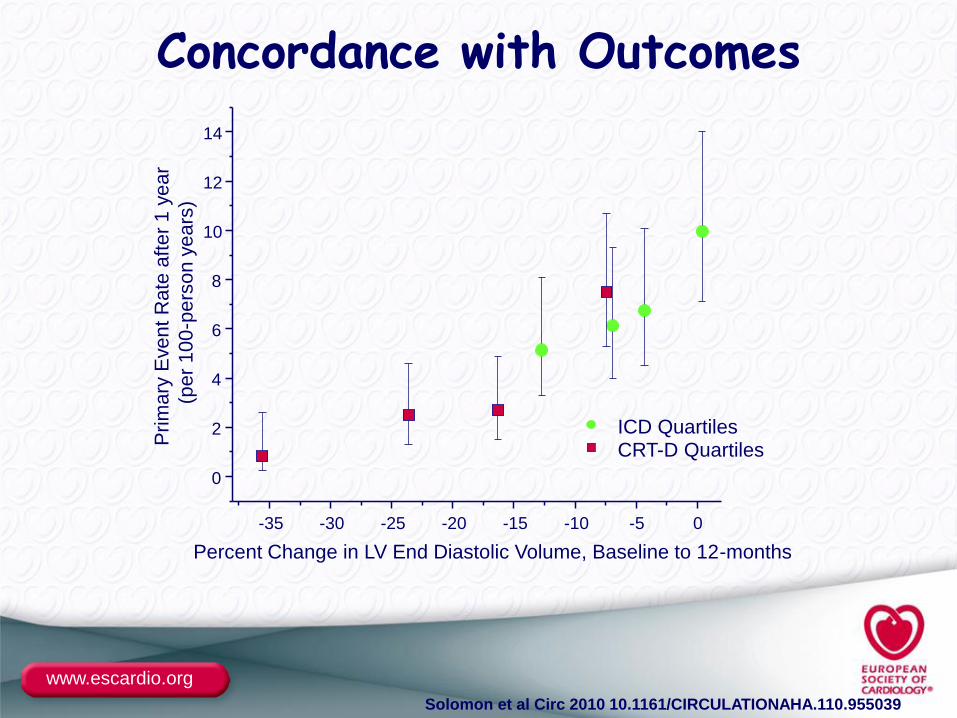
-35 -30 -25 -20 -15 -10 -5 0
0
2
4
6
8
10
12
14
ICD QuartilesCRT-D Quartiles
Pri
ma
ry E
ve
nt
Ra
te a
fte
r 1
ye
ar
(pe
r 1
00
-pe
rso
n y
ea
rs)
Percent Change in LV End Diastolic Volume, Baseline to 12-months
Concordance with Outcomes
Solomon et al Circ 2010 10.1161/CIRCULATIONAHA.110.955039
www.escardio.org
Traditionally, guideline recommendations are based on the
outcomes in the cohort of patients described by the inclusion
criteria in the protocols of Randomised Clinical Trials.
In contrast to previous guidelines, this focused update considers
the characteristics of the patients included in the trials and
contains several examples.
The text accompanying these recommendations explains and
justifies the decisions to diverge from a traditional
recommendation based strictly on the protocol inclusion criteria.
The task force hopes that the users of the Guidelines will
appreciate that this adjustment provides a more realistic
application of the trial evidence to daily clinical practice.
www.escardio.org
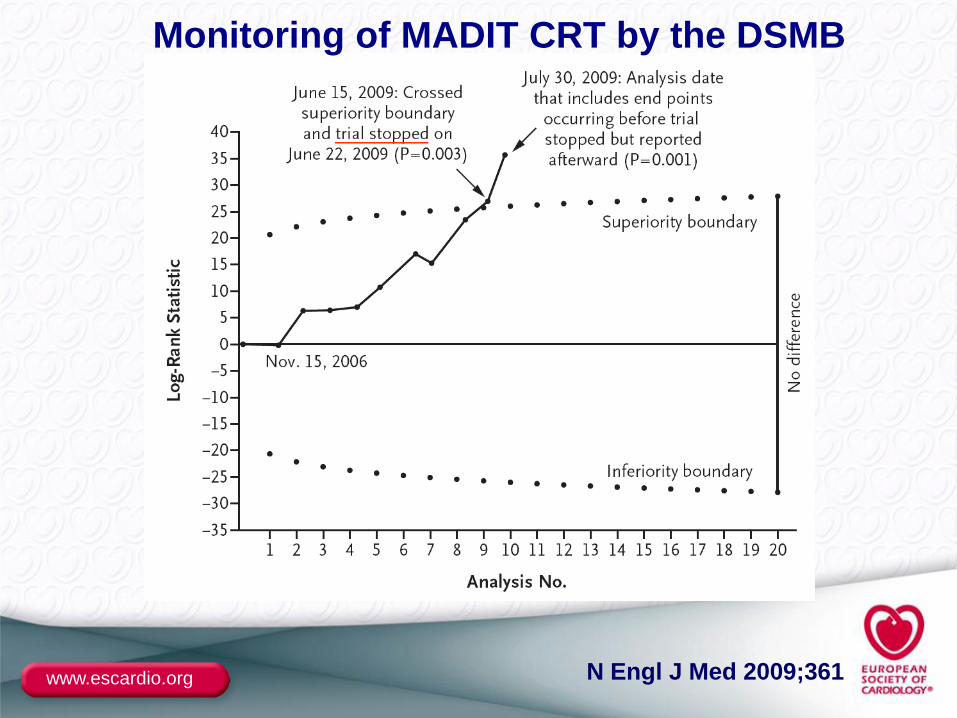
Monitoring of MADIT CRT by the DSMB
N Engl J Med 2009;361
_______
www.escardio.org
In MADIT-CRT, although the protocol permitted inclusion
of patients in both NYHA I and II function class, only 15%
of the patients included in this trial were classified as
NYHA I, many of whom had been previously symptomatic.
Similarly, although the inclusion criteria permitted
randomisation of patients with a QRS width ≥130 m, the
favourable effect on the primary endpoint was limited to
patients with a QRS width ≥150 ms, a prospective, pre-
specified cut-off.
www.escardio.org
In patients with mild symptoms and a QRS width of 120-150 ms, clinicians may wish to assess other criteria associated with a favourable outcome such as:
•dyssynchrony by echocardiography•LV dilatation•LBBB•non-ischaemic cardiomyopathy•recent NYHA class III symptoms
www.escardio.org
ESC CRT SURVEY
NYHA I 2%
NYHA II 20%
Age ≥ 75 (%) 31%
Atrial fibrillation 23%
QRS duration < 120 ms 9%
QRS duration 120 – 129 ms 10%
Eur Heart J 2009;30:2450–2460

www.escardio.org
Parachutes appear to reduce the risk of injury, but their effectiveness has not been proved with randomised controlled trials