Embed Size (px)
Citation preview

David S. George, MD
The Eye MDs

63 y/o female referred from OD for cataract evaluation
C/O gradual decrease vision over 12 months
Glare form headlights when driving
Episodes of temporal flashes on occasion

Trauma OS as child
OS always “weaker” than OD
Arthritis

BCVA 20/30 OD, 20/60 OS
SLE – NSC OS > OD
BAT 20/60 OD, 20/400 OS
Amsler grid wnl OD, temporal grid blurred OS
No APD

RBAs of CE discussed
During discussion, patient mentioned she had had a blind post on visual field testing for years
I discussed a scotoma is not necessarily consistent with a cataract
Patient was very reluctant to have another VF as these have been done yearly by OD “without change” per patient


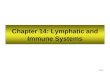
MRI :
Tumor in Sella measuring 2.5 X 3.2 cm is displacing optic chiasm


Compression of crossing fibers leads to classic bitemporal hemianopsia
Disc edema due to increased intracranial pressure uncommon (papilledema not seen)
Disc pallor sometimes seen and later increased cupping

“Bow Tie” atrophy possible but not always present early in course

Chiasmal Syndrome (compression)
Pituitary Adenoma (most common)
Craniopharyngioma
Parasellar Internal Carotid Artery Aneurysm
Chiasmal Glioma


Bitemporal Hemianopsia Tumors can reach relatively large size without
symptoms unless hormonally active Prolactin production decreases male libido May enlarge during pregnancy Diplopia possible if involvement of cavernous
sinus due to involvement of other cranial nerves (CN III most common).
Occasional hemorrhage into tumor produces sudden enlargement, headache, and sudden vision loss (Pituitary Apoplexy). Diplopia may be present.

Goals of treatment Control of tumor growth
Normalization of pituitary function
Restoration of vision
Treatment Trans-sphenoidal removal
Pre-op acuity correlates with results
BVA < 20/100 only 62% improved
BVA > 20/100 , 89% showed improvement

Non-surgical Treatment
Bromocriptine for prolactin-secreting tumors
Irradiation as primary therapy or adjunctive therapy for incompletely resectable tumors

Patient returned 6 weeks later, after trans-sphenoidal resection of tumor
“Everything is so much brighter”
BVA now 20/25 OU
(pre-op BVA was 20/30 OD and 20/60 OS)
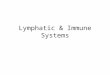
VF – bitemporal hemianopsia now resolved


20/30
20/25
20/60
20/25

79 yo diabetic male presents with 3 week history of a red, painful left eye
Current treatment is Tobradex drops hourly provided by referring OD
No improvement of symptoms despite use of Tobradex drops

BVA 20/20 OD 20/25 OS
IOP 12 OD 14 OS
SLE Conj 2+ Injection
Mild, Diffuse Corneal Edema
Sub-epi haze /No corneal staining
Rare Cell in A/C / Fine KP
Sectoral Iris Atrophy (9 to 10:00)
Posterior synechia
Mild NSC / No vit cell

Unilateral iritis with mild cells, KP and posterior synechia
Corneal edema and folds with mild sub-epi haze suggests corneal involvement in the dz process
Iris atrophy was sectoral, suggesting viral etiology such as HSV or HZV
Iritis not responding well to Tobradex

No vit cell or pigment
C/D 0.4 OU
No DR
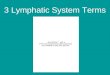
Inferior RD OS!
No break seen in retina
Amelanotic mass under the retina detachment noted from 5 to 7:00 !!!




Incidence 6 cases per million population
Mean age at diagnosis 50 y/o
Choroidal Melanomas rare among non-white individuals
Occurrance is sporadic, not genetic
Role of sunlight and environmental factors remains unknown

Large Tumors (>8mm thick or 16mm longest base diameter)
Enucleation or
External-beam Irradiation then Enucleation
Medium Sized Tumors (3.1 to 8mm thick and < 16 mm)
Enucleation
Brachytherapy with Iodine-125 (local irradiation)
Small Tumors (1 to 3 mm apical thickness, < 5mm dia)
Followed clinically

Large tumors
Pre-op irradiation did not improve survival
5 yr survival 40% (27% mortality due to melanoma)
Medium tumors (N=1317, 12 yrs of data)
Mortality rates same for enucleation or brachytherapy (5yr rate 28% vs 27% respectively)
Small tumors
Tumor related deaths 1% at 5 yrs and 3.7% at 8 yrs

Represent only 1/10th of all ocular melanomas
Overall mortality at 10 years 30-50%, often due to distant metastasis of tumor
Ciliary body and anterior choroidal melanomas carry higher mortality rates than posterior melanomas (likely related to delayed diagnosis)
Can cause local problems as it infiltrates and takes up space

CB melanomas can grow like a ring around the circumference of the ciliary body (up to 360 degrees) – transillumiantion may reveal tumor but ultrasound best (B scan and Ultrasound biomicroscopy)
Hypotension if tumor disrupts overlying ciliary epithelium (often 5 mm Hg lower than other eye)
Angle closure and vascularization of iris possible May find large “sentinel vessel” in conjunctiva (one or
more large episcleral vessels feeding the metabolically active tumor)
Trabecular meshwork can be blocked by melanin laden macrophages or secondary Pigment dispersion syndrome
Lens dislocation and cataract Hyphema or vitreous hemorrhage due to infiltration
into vessels

Metastatic potential depends on the phenotype
of the cells No lymphatic system in the eye thus the only
route of dissemination is hematological Tendency to metastasize to liver Other locations for metastasis include lung,
bone, skin and CNS Check Liver Enzymes and if abnormal then
obtain ultrasound and/or CT studies of the liver (still can miss micrometastasis)