Embed Size (px)
Citation preview
David Biko, MD, MAJ, USAF
Assistant Professor of Radiology
Uniformed Services University of the Health Sciences
Thank you to Monica Epelman, MD for her
contribution to this presentation
Disclaimer
The views expressed in this presentation are those of the authors
and do not necessarily reflect the official policy or position of the
Department of the Navy, Army, Air Force, Department of Defense,
nor the U.S. Government.
We certify that all individuals who qualify as authors have been
listed; each has participated in the conception and design of this
work, the writing of this presentation, and the approval of the
submission of this version; that this presentation represents valid
work; that if we used information derived from another course, we
obtained all necessary approvals to use it and made appropriate
acknowledgements; and that each takes public responsibility for it.
Background
Traumatic injury is the leading cause of death
in children older than 1 year
Vascular injury well studied in adult population,
but not in children
Uncommon (0.6% all pediatric trauma patients)
Management of most pediatric injuries
often similar to adult strategies

Background
Differences between adults and children
Children less severely injured than adults
Significant injuries more difficult to detect
○ Asymptomatic
○ Associated with spasm
○ Other more severe injuries take priority
Small vessel size
○ Technical challenges in diagnosis and treatment

Imaging Evaluation
Clinical presentation varies depending
anatomic location and type of injury
Hard Signs
Soft Signs
Imaging Evaluation
Prompt diagnosis important
Good outcome
○ *64/66 (97%) with initial correct diagnosis
○ *19/23 (83%) with delayed diagnosis
Poor results most likely in arteries adjacent to
elbow and knee
*Evans WE, King DR, Hayes JP. Ann Vasc Surg 1988;3:268-2270.
Consider liberal use of angiography in
child with involvement of elbow or knee
Imaging Evaluation –
Which Modality?
Duplex Ultrasound
Noninvasive, no radiation burden, portable
Limited evaluation of many structures
CT angiography (CTA) or Conventional
Angiography (CA)
Both have potential risks of radiation exposure
and contrast reactions
Although CA still the gold standard, CTA is
largely replacing it for vascular injuries

CT Angiogram vs. Conventional
Angiography in Pediatric Population
• Noninvasive, widely available, rapidly obtained
• Limited studies diagnostic in pediatric population
• Neck and Extremity -95% sensitive; 97% specific*
CTA
• Gold standard
• Invasive but safe
• Low complication rate in pediatric population**
• May perform thrombolysis or embolization
CA
*Hogan et al. J Ped Surg 2009;44:1236-1241.
**Puapong et al. J Ped Surg 2006; 41: 1859-1863
Vascular Injuries in Children
Iatrogenic Vascular Injuries
Most etiologies of pediatric vascular injury
Extremity Vascular Injuries
High incidence of isolated upper extremity
injuries
Truncal Vascular Injuries
Additional major injuries common
○ Most commonly with abdominal trauma
Iatrogenic Vascular Injuries
Significant proportion of pediatric vascular
trauma (33-100%)
Diagnostic catheterization
Cannulation for ECMO or cardiopulmonary
bypass
Placement of Arterial Lines
Arterial puncture/Venopuncture
Postoperative
Extremity Vascular Injuries
Non-iatrogenic injury increases with age
½ - ¾ penetrating injury
Children more likely to develop collaterals
Amputation rate still up to 50% after major vascular
compromise

Extremity Vascular Injuries-
Management
Soft Signs Arterial Pressure Index (API) with
Doppler
API > 0.90
99% NPV*
API < 0.90
95% Sensitivity for Major Arterial Injury*
Hard Signs
(absence of distal pulses, active external hemorrhage, signs of ischemia, pulsatile
bruit or thrill)
Intervention
*Johansen K, Lynch K. J Trauma 1991;31:515-522.
Angiographic Signs of Extremity
Trauma
Active contrast extravasation
Loss of opacification or occlusion of an
arterial segment
Intraluminal filling defect
Early venous opacification
Abnormal change in vessel caliber,
course, or contour
Truncal Vascular Injuries
Includes thoracic, abdominal, and cervical
vascular injuries
Outcomes/intervention based on hemodynamic
stability of patient
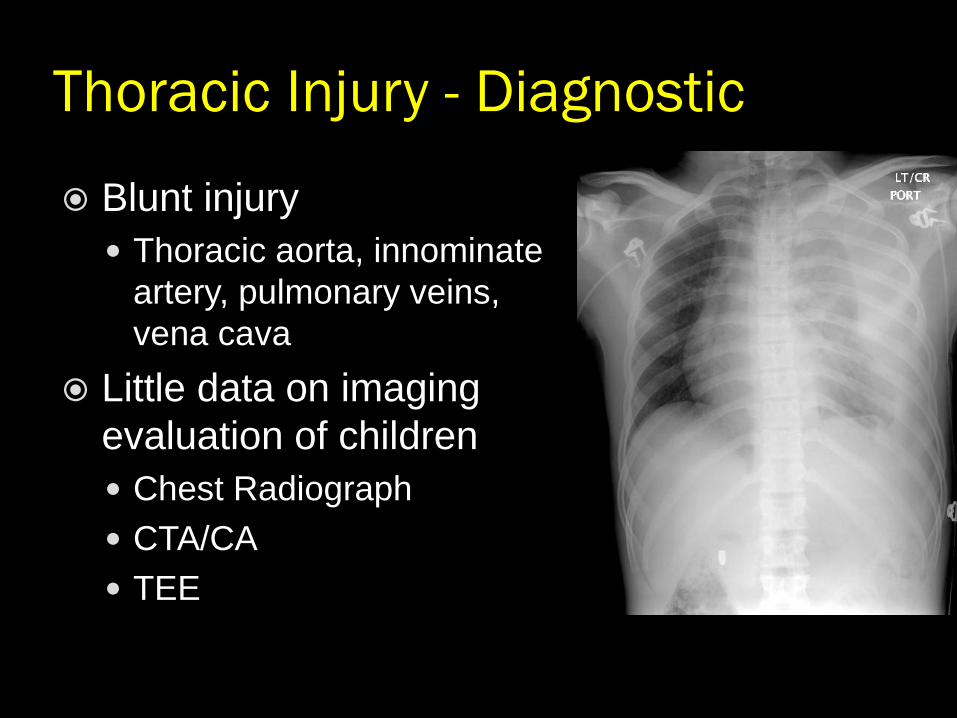
Thoracic Injury - Diagnostic
Blunt injury
Thoracic aorta, innominate
artery, pulmonary veins,
vena cava
Little data on imaging
evaluation of children
Chest Radiograph
CTA/CA
TEE

Thoracic Injury
OPEN repair standard of care
Endovascular interventions common in
adults, but limited in children
Existing stent grafts too large for children
Delivery systems too large or too short
Vessel growth lead to migration
Abdominal Injury
Renal, mesenteric, iliac, aorta
Management driven by
hemodynamic stability
Penetrating trauma (90-95%
vascular injury)
Blunt trauma- more likely solid
organ injury

Abdominal Injury: Children vs. Adults
Children more prone to abdominal
solid organ injury
Abdominal organs relatively larger
Abdominal musculature less mature
Abdominal organs and wall have less fat
Compliant ribcage
Cervical Vascular Injury
Penetrating injuries less frequent than blunt
trauma
Arterial injury 25x higher with penetrating injury
Morbidity mostly related to stroke
Mechanisms of Injury
Penetrating vascular trauma
Along the injury tract
○ Direct contact with vessel wall
○ Energy imparted to the vessel by projectile
Blunt vascular trauma (carotid artery)
Direct blow to the anterior neck
Blow to the side of the head with stretching of vessel
Fracture of the skull base
Intra-oral
○ Falling on toothbrush or lollipop in mouth

Management of Cervical
Vascular Injury
Immediate exploration
Hemodynamically unstable
Hard Signs
○ Rapidly expanding hematoma
○ Pulsatile bleeding
○ Air bubbles in the wound
Imaging for all others
Most often CT angiography
Conclusion
Pediatric vascular trauma is rare
Most injuries iatrogenic or isolated extremity
Diagnostic evaluation and management
based on adult strategies
But remember that children have unique
anatomic and physiologic consideration so
adult management should be approached
with caution
Conclusion
Conventional angiography remains the gold
standard to evaluate vascular trauma, but
CT angiography is often replacing it
Noninvasive, widely available, rapidly
obtained
Although studies limited, CTA has been
successful in the evaluation of pediatric
vascular injury
References 1. Corneille MG et al. Pediatric Vascular Injuries: Acute Management
and Early Outcomes. J Trauma 2011;70: 823-828.
2. Barmpras G et al. Pediatric vs adult vascular trauma: a National Trauma Databank review. J Ped Surg 2010;45:1404-1412.
3. Cannon JW, Peck MA. Vascular Injuries in the Young. Perspect Vasc Surg Endovasc Ther 2011 doi: 10.1177/1531003511408439.
4. Evans WE, King DR, Hayes JP. Arterial Trauma in Children: Diagnosis and Management. Ann Vasc Surg 1988;3:268-2270.
5. Lineen EB et al. Computed tomographic angiography in pediatric blunt vascular injury, J Ped Surg 2008; 43:549-554.
6. Hogan AR et al. Value of computed angiography in neck and extremity pediatric vascular trauma. J Ped Surg 2009; 44:1236-1241.
7. Wallin D et al. Computed Tomographic Angiography as the Primary Diagnostic Modality in Penetrating Lower Extremity Vascular Injuries: A Level I Trauma Experience. Ann Vasc Surg 2011;25:620-623.
References
8. Puapong D et al. Angiography and the pediatric trauma patient: 10- year review. J Ped Surg 2006; 41:1859-1863.
9. Johansen K, Lynch K. Non-invasive vascular tests reliably exclude occult arterial trauma in injured extremities J Trauma 1991;31:515-522.
10. Gakhal MS, Sartip KA. CT Angiography Signs of Lower Extremity Vascular Trauma. AJR 2009;193:W49-W57.
11. Allison ND et al. Outcomes of truncal vascular injuries in children. J Ped Surg 2009; 44: 1957-1964
12. Wang NE, Blankenburg RL. Pediatric Abdominal Trauma. Trauma Reports 2007;.8:1-12.
13. Schroeder JW, Baskaran V, Aygun N. Imaging of traumatic arterial injuries in the neck with an emophasis on CTA. Emerg Radiol





























