Embed Size (px)
Citation preview
David Publishing Company
www.davidpublishing.com
PublishingDavid
Volume 7, Number 4, April 2010 (Serial Number 65)
Journal of US-China
Medical Science

Publication Information: Journal of US-China Medical Science (ISSN1548-6648) is published monthly in hard copy and online by David Publishing Company located at 1840 Industrial Drive, Suite 160, Libertyville, Illinois 60048, USA. Aims and Scope: Journal of US-China Medical Science, a monthly professional academic journal, covers all sorts of researches on Original Articles, Review Articles, Medical Progress, Brief Reports, Case Reports and Conference Proceedings. We welcome current original articles and rapid communications on all aspects of the medical sciences and related areas, both experimental and clinical, from any part of the world. Editors: Cecily Z., Lily L., Jim Q., Jimmy W., Hiller H., Jane C., Betty Z., Gloria G., Stella H., Clio Y., Grace P., Caroline L., Alina Y., Sharry L. Manuscripts and correspondence are invited for publication. You can submit your papers via Web Submission, or E-mail to [email protected]. Submission guidelines and Web Submission system are available at http://www.davidpublishing.com. Editorial Office: 1840 Industrial Drive, Suite 160 Libertyville, Illinois 60048 Tel: 1-847-281-9826 Fax: 1-847-281-9855 E-mail: [email protected] Copyright©2010 by David Publishing Company and individual contributors. All rights reserved. David Publishing Company holds the exclusive copyright of all the contents of this journal. In accordance with the international convention, no part of this journal may be reproduced or transmitted by any media or publishing organs (including various websites) without the written permission of the copyright holder. Otherwise, any conduct would be considered as the violation of the copyright. The contents of this journal are available for any citation; however, all the citations should be clearly indicated with the title of this journal, serial number and the name of the author. Abstracted / Indexed in: Database of EBSCO, Massachusetts, USA Chinese Database of CEPS, Airiti Inc. & OCLC Chinese Scientific Journals Database, VIP Corporation, Chongqing, P. R. China Ulrich’s Periodicals Directory Subscription Information: Price: $360 David Publishing Company 1840 Industrial Drive, Suite 160, Libertyville, Illinois 60048 Tel: 1-847-281-9826. Fax: 1-847-281-9855 E-mail: [email protected]

Journal of US-China Medical Science
Volume 7, Number 4, April 2010 (Serial Number 65)
Contents Basic Research
1 An in Vitro Tissue-Culture Evaluation of the Cell Toxicity of Platelet-Rich Plasma and Silver Dressings Donald. F. Du Toit and Benedict. J. Page
9 Effect of Dietary Oleic Acid and Palmitic Acid on Cerebellum Histological Changes and Sensorimotor Coordination in Rat H. Morovvati, Z. Hosseinzadeh, A. A. Moazedi and H. Najafzadeh
Clinical Study 14 Pro-apoptotic Effect of Recombinant Anti-HER2 Fusion Protein Scfv/Tbid on Osteosarcoma E10 Cells
Xiuchun Qiu, Lequn Shan, Sai Ma, Zhengang JI, Tongtao Yang, Hua Long, Yanming Xu, Yong Zhou, Baoan Ma, Angang Yang and Qingyu Fan
20 The Aged Organism as a Model of Successful Copping with Tumor Progression—Implications for Therapy Judith Leibovici, Tatiana Kaptzan, Orit Itzhaki, Ehud Skutelsky, Judith Sinai, Moshe Michowitz, Ginnette Schiby, Annette Siegal and Monica Huszar
29 Diagnosis and Management of Intractable Hemoptysis by Bronchoscopic Intervention Faguang Jin, Deguang Mu, Dongling Chu, Enqing Fu, Yonghong Xie and Tonggang Liu
31 VEGF and Angiogenesis in Renal Cell Carcinoma: A Minireview Ketao Jin, Ling Zheng, Kaiyan Fu, Yefei Zhang, Tieming Zhu and Zhigang Jin
34 The Influence of Hyperoxygenated Solution for High Altitude Hemorrhagic Shock Rabbits’ Resuscitational Effects and Plasma Endothelin and Nitric Oxide Release Qiquan Zhou, Dongxue Zhi, Liju Gao and Bo Zhou
Case Report 40 Discussion about the Prognoses of Wilson's Disease with Severe Cortex Structure Impairment—A Case
Report of Wilson’s Disease (WD) Treated by the Traditional Chinese Medicine and Western Medicine Songlin Chen, Yingyin Liang, Xiangxue Zhou and Xunhua Li
45 Case Report: Treatment of Canary Pox with Orally Administration of Acyclovir Mansour Mayahi and Forogh Talazade
47 A Deformity Fetus Delivered by a Hepatitis B Woman Treated with Lamivudine during Pregnancy Qing He, Liansan Zhao, Qiyuan Tang and Zhou Zhou
50 Hyperglycemia and Lactic Acidosis after Ingestion of a Lethal Dose of Slow-Release Nidedipine––Case Report Cristina Bologa, Adorata Coman, Catalina Lionte, Ovidiu Petris and Laurentiu Sorodoc
Medical Management Study 54 The Effect of Official Automation on Performance Improvement Based on Balanced Scorecard Model
(BSC) Nour Mohammad Yaghoubi and Sadegh Khazaee Asl
Apr.2010, Volume7, No.4 (Serial No.65) Journal of US-China Medical Science, ISSN 1548-6648, USA
An in Vitro Tissue-Culture Evaluation of the Cell Toxicity
of Platelet-Rich Plasma and Silver Dressings
Donald. F. Du Toit and Benedict. J. Page
Division of Anatomy and Histology, Academic Department of Biomedical Sciences, Faculty of Health Sciences, Medical School,
University of Stellenbosch, Tygerberg Campus, Parow, South Africa Abstract: Objective: To establish whether platelet–rich plasma (PRP) and silver–impregnated dressings, used individually are cytotoxic to human-skin keratinocytes, dermal-fibroblasts and adipose derived stem cells (ADSC) cultured in vitro. Method: Cultures of human keratinocytes, fibroblasts and ADSC were established in vitro. All test-cells were raised initially on RegenPRP®-Kit coated, testing petri-dishes. Group-I served as cultures without PRP or silver-stimulation. Group-II consisted of continuous culture of the 3-cell lines on the PRP-base without any further additives. Group-III cells initially raised on PRP were now exposed to and co-cultured with small nanocrystalline silver implants placed on the established cell monolayers (Acticoat®). Diagnostic inverted-microscopy, trypan–blue staining, cell-testing and the Rosdy and Clauss cell-toxicity scoring system were used to identify cell-toxicity. Results: Cultures consisting of keratinocytes, dermal fibroblasts and ADSC (group-II) were established in 95% of all explants on platelet-rich plasma coated test-wells. In group-III or cell-recipients treated with silver implants, marked cell toxicity developed within days, with high non-viability staining and cell-scoring counts compared to Group-II (p< 0.05). Diluted PRP has a strong proliferative effect on keratinocytes, dermal fibroblasts and adipose derived stem cells (ADSC). While silver impregnated implants interferes with newly cultured cells, epidermal cell proliferation and migration, and has notable cytotoxic properties in vitro. Conclusion: Diluted Regen-PRP shows good cytocompatibility with tissue-culture including keratinocytes, dermal fibroblasts and ADSC and favours cell proliferation of skin epidermal and mesodermal components ex vivo. Silver dressing explants placed on established cell-lines ex vivo, induce consistent cell-toxicity in the same cell lines when cultured under controlled conditions. Key words: Platelet-rich plasma, silver, tissue-culture, RegenPRP®-Kit, Adipose Derived Stem Cells, keratinocyte, fibroblast, Acticoat®.
1. Introduction
There exists scanty evidenced-based tissue-culture data and comparisons of autologous or allogeneic-PRP and silver-impregnated dressings on integument- derived cell-lines relevant to wound-healing. Silver- dressings and topicals, by nature of the potential anti-microbial effect, have been used for decades as wound-healing devices, but are associated with negative cell-cytopathic properties, varying from mild to severe [1-3]. Recently, topical biologicals, showing trophic effects on cell growth, such as platelet-rich plasma (PRP) have been advocated for chronic
Corresponding author: Donald. F. Du Toit, PhD., professor,
research fields: Cell biology, platelet-rich plasma and cell transplantation. Email: [email protected].
wound-healing treatment and care as alternatives to chemicals and heavy-elements, because of the potential natural release of alpha-granule platelet-derived growth-factors(GF), such as platelet-derived growth factor, (PDGF-AA,PDGF-BB and PDGF-AB), transforming growth-factors (TGFbeta-1,TGFbeta-2 and consisting of a further 47 ill-defined factors and cytokines), vascular endothelial growth-factor (VEGF), and epidermal growth-factor (EGF) [4-14]. Here the proposed wound-healing cells and cascade is stimulated by platelet-gel derived growth-factors and details can be reviewed elsewhere [13, 14].
For the tissue-culture (TC), cell-toxicity study, we selected RegenPRP®-Kit and a nanocrystalline silver impregnated dressing (Acticoat®, Smith and Nephew™). These are considered to represent PRP and

An in Vitro Tissue-Culture Evaluation of the Cell Toxicity of Platelet-Rich Plasma and Silver Dressings
2
silver-preparations used frequently by practitioners and wound-care specialists in hospitals and ulcer clinics. The silver dressing served as a culture-control for the platelet-rich plasma product.
Study outcomes were to compare the biological effects of PRP-gel or lysate and silver impregnated dressings on epidermal, dermal and mesodermal cell proliferation, and to record any negative growth effects(that is, if one or both compounds had a negative effect on cell growth) and local cell-toxicity under standard tissue-culture and cell-testing conditions. Cell-proliferation was studied within an ethical authorised tissue-culture research-protocol for utilizing keratinocytes, fibroblasts and adipose derived stem cells.
2. Material and Methods
2.1 Tissue Culture and Platelet–Rich Plasma Preparation
Small tissue-explants consisting of epidermis, dermis and subcutaneous fat within protocol (measuring 0.5 × 0.5 mm) were used to generate monolayers of keratinocytes, dermal fibroblasts and adipose derived stem-cells (ADSC), by the air-lifting technique, without collagenase digestion, in PRP- coated petri-dishes (20% dilution of RegenPRP®-Kit). One millilitre of activate-PRP was instilled into each testing dish, allowed to incubate over-night at 37-degrees and form a platelet-gel after activation with calcium-chloride, but not thrombin. The sticky coated-dishes were seeded with the explants, without need for heat-fixation, and then subjected to conventional tissue-culture (TC) without addition of fetal calf serum (FCS). Well formed monolayers, after dynamic culture, in all 3-lines were present at about 30-days, at which stage half the cells in culture ( the rest remaining as controls) were challenged with small round silver-dressing implants of Acticoat® (0.5 × 0.5 cm). Cell-morphology changes focusing on cytopathic changes, was studied thereafter on a daily-basis by inverted-microscopy in Groups II and III.
RegenPRP-Kit® (Regen Lab®-Lausanne, Switzer- land) was generated by a two-spin method, from centrifuged peripheral venous-blood harvested in Regen-THT® tubes containing sodium-citrate, separating off the platelet-poor plasma (PPP). Activated platelet-rich plasma (PRP) was used to coat the test TC-plates. The RegenPRP-Kit® outcome- based profile is as follows: PRP-volume per tube 5±0.5ml, platelet-recovery 90±5%, Pl concentration 962±437 (106/ml), PDGF-AB 140±14 (ng/ml), EGF 650±120 (pg/ ml), and VEGF 80±22 (pg/ml).
2.2 Tissue Culture: Methodology, Cytological Cell-testing and Cell-statistics
Primary and secondary cultures were instituted and culture-mediums were exchanged three times a week, under controlled anti-septic conditions in an academic, clean-room TC-facility. Cell-proliferation and cell-morphology criteria assessed and audited in TC-format, included locomotion (crawling), filopodia formation, branching, network-formation, cell-death, monolayer dysfunction, daily by inverted light- microscopy/photography with varying magnification over a 4-month period. For cell-testing, cell-viability was determined by microscopic changes on captured images, and the trypan-blue method. Cell-audits, record-keeping and cell-tracking were carefully assessed. Tissue-processing and culturing technology was as follows: Dissecting Olympus® Microscope SZ61 for tissue-trimming; laminar flow-hood (Lab Air™, Midrand, 1200 H) for plating and medium exchanges, CO2-incubator (ShelLab®) for tissue- expansion, inverted dissecting-microscope (Olympus® CKX31) and Sony® Digital-Camera/ Carl Zeiss®, Japan, for cell-morphology studies; cell-plating (CellStar-Greiner Bio-One®). Basic culture-medium without FCS (Dulbecco’s Modified Eagle’s Medium-Highveld Biologicals®, RSA), and antibiotic enrichment (penicillin, streptomycin, fungizone: Highveld Biologicals®, Midrand, RSA), was used in the study; exchange mediums contained no FCS
An in Vitro Tissue-Culture Evaluation of the Cell Toxicity of Platelet-Rich Plasma and Silver Dressings
3
(Highveld Biologicals®, Midrand, in DMEM). For diagnostic cytological cell-testing statistics, parametric and non-parametric statistical analysis to assess cell-proliferation, included Student’s T-test or Mann-Whitney U-Test for small numbers. Visual images of individual cells or cell groups were captured on a Sony® Digital-Camera (Carl Zeiss, Vario–Tessa®).
Groups studied: (1) Group-I, Control TC with cellular-explants
without any product on uncoated–dishes, indefinitely. (2) Group-II, PRP-coating and three cell lines, TC
study-group, indefinitely. (3) Group-III, Silver implants (Acticoat®): TC
study-group, three-cell lines on PRP coated plates, challenged with silver-implants indefinitely.
2.3 Cell Biology Assessment Post-product Stimulation: Cell Morphology, Cytological-testing and Viability-scoring
Cell-morphology was assessed daily under an inverted-microscope, to study general, nuclear and gross cyto-cavitary morphology. • Cell-proliferation (growth) and migration, • Cell-toxicity, • Killing or inhibitory effects of the silver test-product, • Cyto-compatibility or cytopathic effects [15].
Cellular viability was performed by the trypan-blue exclusion, cytological test. Cytokine, dressing absorbency tests, cell-extractions, flow-cytometry and MTT (yellow-dye test) assay’s were not performed, and were beyond the scope of the study. For each experiment, tests were performed in duplicate if necessary.
Cell-shape and configuration of keratinocytes, fibroblasts and ADSC were cytologically evaluated by inverted-microscopy using the morphology assessment-technique of Rosdy-and-Clauss scoring system (1990) for comparison of the effects of the two products on cells in the test-wells [15]. This permitted
appropriate diagnostic cytological cell-testing, measurement and scoring of cell-proliferation and morphological changes affecting cell-shape as follows:
0 = No change noted. 1 = Slight, but clear change in shape without
decrease of cell-density. 2 = Considerable alterations in cell-shape. Slight
decrease of cell-density. 3 = Loss of cell-shape. More than 50% of cells
detached. 4 = All the cells are dead, lysed or detached.
3. Results
3.1 Group I: Control Untreated TC-Studies without Product Stimulation Ex Vivo
Cell-growth and proliferation from tissue-explants resulting in monolayers could not be established on uncoated Petri-dishes.
3.2 Group II: Cell Proliferation TC Studies Ex Vivo with Well-Exposure to RegenPRP-Kit®-Platelet Rich Plasma
Cell-proliferation and expansion of all three lines, in terms of keratinocyte, fibroblast and ADSC cell-counts per millimetre, increased uniformly and rapidly in almost all wells containing diluted PRP (RegenPRP®-Kit), according to assessed criteria compared to the untreated-controls (Group-I, p < 0.05) and silver-group (Group-III). Within 4-days of cell-seeding with explants, cell-proliferation was evident and faster than Group-1(p < 0.05). Dermal-fibroblasts seem to proliferate the fastest, followed by ADSC and keratinocytes. Keratinocytes and fibroblasts developed monolayers quickly, but not ADSC. Nuclear and cyto-cavitary networks appeared normal, suggesting no local-toxicity. These changes were observed with the use of serum-free medium and without further addition or spiking of the dishes and cells with PRP-gel. PRP (RegenPRP-Kit®), stimulated
An in Vitro Tissue-Culture Evaluation of the Cell Toxicity of Platelet-Rich Plasma and Silver Dressings
4
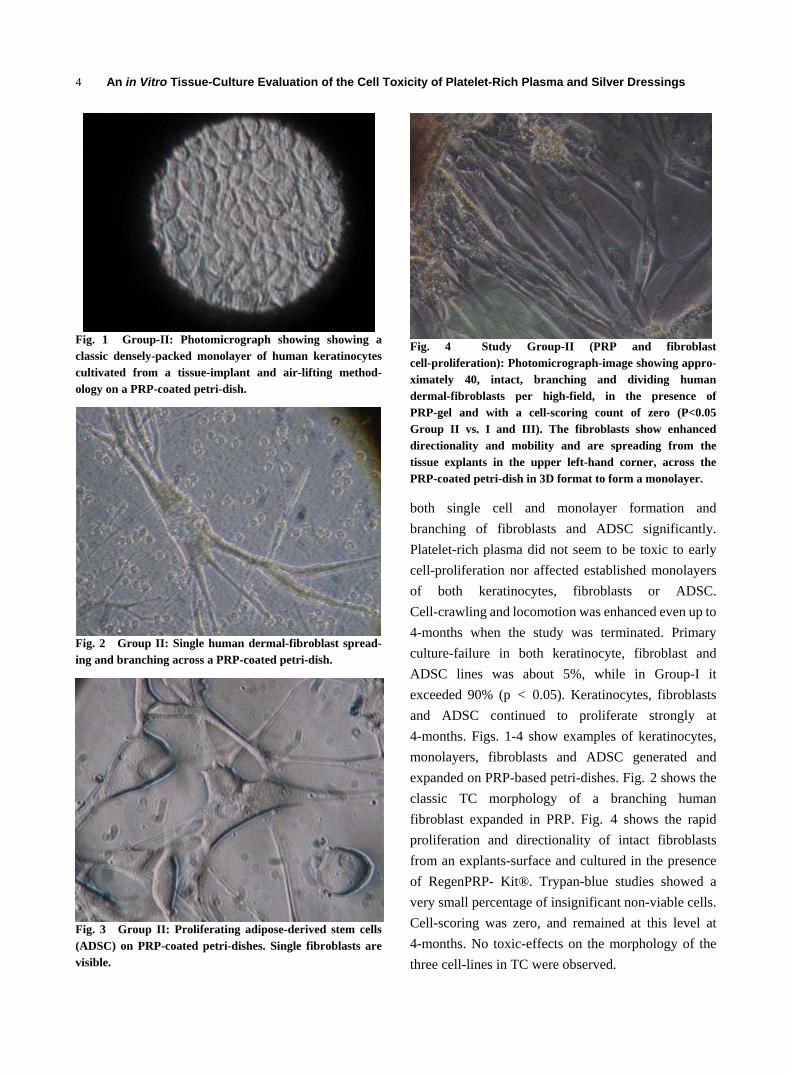
Fig. 1 Group-II: Photomicrograph showing showing a classic densely-packed monolayer of human keratinocytes cultivated from a tissue-implant and air-lifting method- ology on a PRP-coated petri-dish.
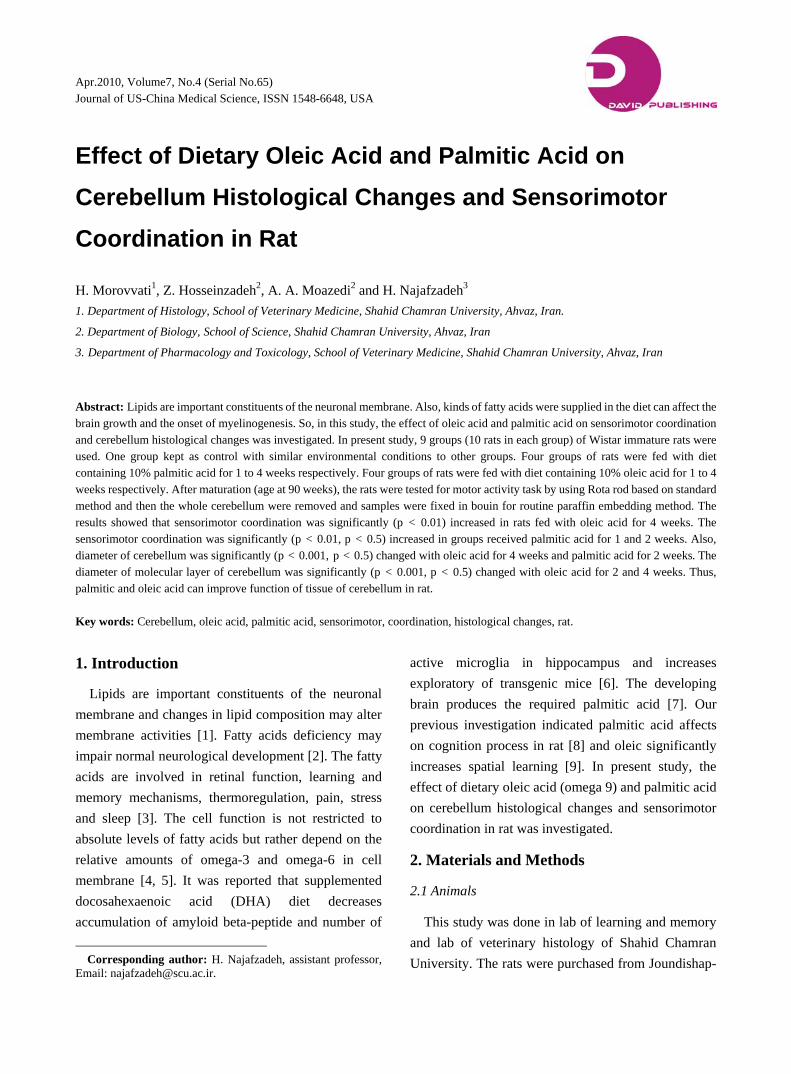
Fig. 2 Group II: Single human dermal-fibroblast spread- ing and branching across a PRP-coated petri-dish.
Fig. 3 Group II: Proliferating adipose-derived stem cells (ADSC) on PRP-coated petri-dishes. Single fibroblasts are visible.
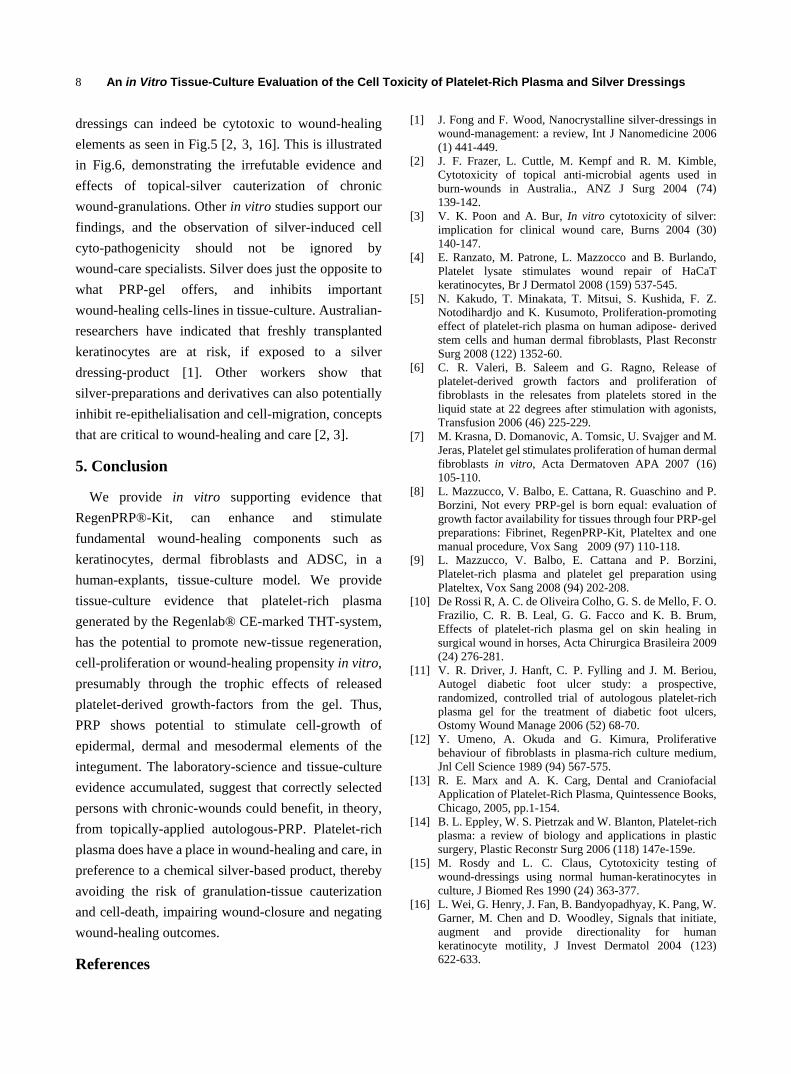
Fig. 4 Study Group-II (PRP and fibroblast cell-proliferation): Photomicrograph-image showing appro- ximately 40, intact, branching and dividing human dermal-fibroblasts per high-field, in the presence of PRP-gel and with a cell-scoring count of zero (P<0.05 Group II vs. I and III). The fibroblasts show enhanced directionality and mobility and are spreading from the tissue explants in the upper left-hand corner, across the PRP-coated petri-dish in 3D format to form a monolayer.
both single cell and monolayer formation and branching of fibroblasts and ADSC significantly. Platelet-rich plasma did not seem to be toxic to early cell-proliferation nor affected established monolayers of both keratinocytes, fibroblasts or ADSC. Cell-crawling and locomotion was enhanced even up to 4-months when the study was terminated. Primary culture-failure in both keratinocyte, fibroblast and ADSC lines was about 5%, while in Group-I it exceeded 90% (p < 0.05). Keratinocytes, fibroblasts and ADSC continued to proliferate strongly at 4-months. Figs. 1-4 show examples of keratinocytes, monolayers, fibroblasts and ADSC generated and expanded on PRP-based petri-dishes. Fig. 2 shows the classic TC morphology of a branching human fibroblast expanded in PRP. Fig. 4 shows the rapid proliferation and directionality of intact fibroblasts from an explants-surface and cultured in the presence of RegenPRP- Kit®. Trypan-blue studies showed a very small percentage of insignificant non-viable cells. Cell-scoring was zero, and remained at this level at 4-months. No toxic-effects on the morphology of the three cell-lines in TC were observed.

An in Vitro Tissue-Culture Evaluation of the Cell Toxicity of Platelet-Rich Plasma and Silver Dressings
5
3.3 Group III: Cell Proliferation TC Studies Ex Vivo with Cell Exposure to Silver (Acticoat®)
Small round discs containing crystalline silver were inserted into established and healthy, three-cell line culture monolayers generated over weeks in platelet-gel (RegenPRP-Kit®). A rapid and steady deterioration and degradation of cell-proliferation and cell-monolayer formation regarding all 3-cell lines, compared to unstimulated PRP (RegenPRP-Kit®) (GroupII) on the other-hand, was detected uniformly in silver-treated wells (Acticoat®, Group-III). Killing and inhibitory effects of silver on cell-growth of keratinocytes, fibroblasts, and ADSC throughout the wells was rapidly evident. With time, most cells became non-viable in the absence of infection. Enhanced cell-proliferation was not detectable, and monolayers and cell-migration became inhibited by the silver, compared to PRP (RegenPRP-Kit®) (Group-II, p < 0.05), cells that were run in parallel under the same laboratory conditions, including use of the same media (DMEM). Disturbed fibroblast and ADSC morphology (i.e., crawling, filopodia, branching etc.) was graded II-III (on a scale of I-III; I = good, II= intermediate, III= very poor). Cell-survival, migration and shapes were negatively affected. General single-cell proliferation and monolayers were inhibited in the silver-based group wells, compared to PRP (RegenPRP-Kit®, Group-II), and cell-numbers declined with time indicating continuous and ongoing cell-toxicity (Group III, p < 0.05, vs. Group-II). In some wells, enhanced cell-failure was prominent and monolayers fragmented. Despite the sample size being small, striking negative morphological changes including cell-proliferation and monolayer inhibition was detectable in the silver-study group. Silver-treated cells, and tissue explants-cultures faired poorly in culture, and showed poor proliferation potential compared to control PRP (RegenPRP-Kit®). Trypan- blue staining showed a high percentage of non-viable cells. Fig. 5 shows poor cell-proliferation in the presence of silver, and is representative of ongoing
Fig. 5 Study Group-III (cytological-testing in vitro): Photomicrograph-image showing silver-induced inhibition of cell-expansion and cell-death (Acticoat®) with a cell-scoring-count of 3-4 (p < 0.05, Group III vs. Group-II). A few fibroblasts are still visible in the presence of wide-spread monolayer degeneration and fragmentation due to the cytopathic effects of topical silver.
cell-inhibition as seen in this group. There were no surviving keratinocytes, fibroblast cultures, ADSC or monolayers at 4-weeks compared to cells cultured on PRP-gel (P < 0.05, Group III vs. Group-II). Trypan-blue staining confirmed high-counts, indicating non-viable cells and cells-scores (cell-shape changes) ranged from 3-4 (80% > 3: P < 0.05, Group III compared to Group-II).Very poor cell-counts, of both cell-lines, were recorded eventually.
4. Discussion
4.1 Platelet–rich Plasma TC Study
These findings demonstrate that platelet-rich plasma (PRP) or PRP-gel is a biological stimulator of wound-healing, cell-proliferation lines, such as keratinocytes, dermal-fibroblasts and adipose-derived stem cells (ADSC) in vitro. These results confirm the findings of other workers (4-7). The study also confirms that PRP, also referred to by some as platelet-gel or platelet-lysate, can facilitate wound- healing components by stimulating keratinocyte- migration [4]. Clinical applicability of autologous-PRP, including safety and efficacy has appeared in the medical literature [11, 13-14]. In vitro testing in an

An in Vitro Tissue-Culture Evaluation of the Cell Toxicity of Platelet-Rich Plasma and Silver Dressings
6
animal model with HaCat keratinocytes shows that cell stimulation can be accomplished now by the application of non-toxic, 20% platelet-lysate, through a calcium- and p38-dependent mechanism [4]. This study and others suggest the proliferation potential of activated-PRP, in tissue-culture (TC), more specifically the cell biology effect on ADSC and dermal-fibroblasts [5-7]. The Japanese-group, have confirmed that enriched-PRP can contain up to 7.9 times as many platelets as peripheral whole-blood, as delivered by the Japanese’s Paramedeic® platelet-rich plasma kit [5]. Mazzucco et al, have published evidence regarding the efficacy and quantification of various PRP-kits, and indicated that the RegenPRP-Kit® is capable of generating the highest platelet-recovery [9]. Activation of PRP in the Paramedeic-Kit®, results in release of favourable amounts of PDGF-AB and TGF-beta1 [5]. An interesting finding in their study is the documentation that both activated-PRP and platelet-poor plasma (PPP), are strong promoters of ADSC and human-dermal fibroblast cell-proliferation in vitro [5]. This is not an unexpected finding as PPP still does contain substantial amounts of PDGF, TGF-beta1 and osteocalcin [6]. They also clearly demonstrate that a dilution of 5%-PRP and medium is far more effective than 20% in the promotion of cell-proliferation ex vivo. Others, in contrast, report good proliferative results using 20%-PRP or lysate [4].This important cell-culture work strongly suggests that the cell-growth induction, proliferation and differentiation for tissue-regeneration, is orchestrated at least by two growth-factors, PDGF-AA and TGF-beta1, that are released from the platelet alpha-granules [5]. But these two GF may not be the only optimal stimulants of cell-proliferation, within the 37 cytokine-cascade secreted by platelets [4]. Currently, there is insufficient evidence for researchers to completely accept that PDGF and TGF are the only relevant stimulants of cell-proliferation in the wound-healing process or cascade. Mazzucco and co-workers have pointed out that the bioavailability of
GF in the tissue-healing arena, depends on the amount of GF stored in platelets [8, 9]. Also it is important to remember that many GF supposedly get lost or degrade in the manipulation of platelet-gel generation [8]. This may also impact negatively on the wound-healing process if inferior quality PRP is applied to a wound. Also lacking in the cytokine-literature, is convincing evidence regarding the kinetics of GF-release from PRP-gels [8]. The Italian group, have recently pointed out huge differences in GF-release depending upon the separation-technology used to generate PRP-gel, and this needs to be taken into account [8]. This may well influence GF-performance and kinetics at cellular-level, thereby potentially affecting wound-healing capacity [8]. The Japanese-group, indeed, did show important proliferation-potential of activated PRP-gel on ADSC and dermal fibroblasts, the former being an important source of multi-potent stem cells in man for potential engineering application in plastic surgery, and the latter for wound-healing [5]. Of note is that these researchers were able to induce cell-stimulation with activated-PPP, which one normally discards with the upper supernatant, because this stratum is devoid of the buffy-coat and has a low platelet-concentration therein [5]. Our study-design differs from the Japanese one, in that we exclusively used traditional enriched, quantified and activated-PRP. We accept that GF release varies from kit to kit as reported in the literature [9]. However, in a recent publication showing comparison of numerous other PRP-generation kits (including Plateltex®, Fibrinet®, Harvest®, PCC® and PRGF kit®), the RegenPRP-Kit® (THT-tube) compared favourably and was able to generate the most PDGF-AB (140±14 ng/ml) after activation with thrombin [8]. Biological data is outstanding on PRP-generation regarding home-developed devices and MyCells®. We concur with Kakudo et al, that enhanced proliferation of ADSC’s and dermal-fibroblasts induced by activated-PRP or PRP-gel is driven to a large extent by platelet-release of PDGF-AB and TGF-beta1, and that

An in Vitro Tissue-Culture Evaluation of the Cell Toxicity of Platelet-Rich Plasma and Silver Dressings
7
our observations are evidenced-based [5]. Kakudo’s cell-biology experience and observations were observed over a 7-day period and culture-cells were released by collagenase-digestion, and so differ from our study where a dynamic TC-system was instituted without static–growth TC methodology [2]. We selected a TC-explants methodology with tissue- explants air-lifting (exposure of a part of the explants above the medium fluid-line, DMEM culture-medium) over a 4-month period. Apart from the two GF’s released by the platelets and reported in the cell-biology media, we speculate that our interim-study proliferation study results over 4-months may also well be explained by subtle release of plasma-fibronectin, and development of a cell-friendly fibrin-lattice or network in the platelet-gel. Previous observations in our laboratory point out that it is possible to sustain human-fibroblast and ADSC proliferation on human fibronectin-based plates (BD Biocoat™) or petri-plates coated with Tisseel™( without platelets), that contains clottable human-protein(unspecified), bovine aprotinin and bovine thrombin.
Our proliferation results with human-fibroblasts stimulated with 20%-PRP are also supported by other researchers from The Blood Transfusion Service in Slovenia and researchers from Kyushu University [6, 7]. Furthermore, the wound-healing properties of autologous-PRP in horses, and patient’s presenting with diabetic-foot ulceration have been demonstrated, emphasizing the relevance of platelet-gel or lysate and growth-factor integration in wound-care management [10, 11]. Of importance is that GF’s and extracellular matrix (ECM) work together synergistically and as promotion-stimuli, thereby providing directionality for human-keratinocyte motility [16]. More evidence- based research is clearly needed to clarify release- mechanisms, signalling-systems and kinetics of GF from PRP-gels or lysates. Clinical-studies using autologous-PRP to enhance wound-healing are in progress in various institutions, based on wound- healing enhancement by release of GF from platelets,
gels and lysates [11]. However comparisons of autologous-PRP versus conventional dressings for chronic-wound management in trials do not exist. Benefits to wound-healing in diabetic-patient’s with distal lower-extremity ulceration has been documented [11]. Honey and silver surgical dressings are chiefly directed at wound-exudates removal and combined local anti-microbial effect. Wound-healing by biologicals differ, as the PRP-gel is applied to the wound-surface in order to intentionally facilitate release of platelet-derived growth-factors at the point-of-care from the gel, and to induce wound-closure by stimulation of host or recipient keratinocyte, dermal fibroblast and ADSC regeneration, together with extracellular matrix (ECM).
4.2 Silver–impregnated Surgical Dressing TC Study
It is clear from this in vitro tissue-culture and cell-biology based study, that a randomly selected silver-implant had a direct and consistently inhibitory effect on established, fragile monolayers of keratinocytes, dermal fibroblasts and ADSC. Although silver-impregnated dressings are affordable, and portray useful antimicrobial-properties relevant to chronic wound-care, there is evidence now that silver-
Fig. 6 “Silver-eschar”: Anterior view of the lower shin, showing large, non-cancerous ulcer and granulation staining following the application of silver.
An in Vitro Tissue-Culture Evaluation of the Cell Toxicity of Platelet-Rich Plasma and Silver Dressings
8
dressings can indeed be cytotoxic to wound-healing elements as seen in Fig.5 [2, 3, 16]. This is illustrated in Fig.6, demonstrating the irrefutable evidence and effects of topical-silver cauterization of chronic wound-granulations. Other in vitro studies support our findings, and the observation of silver-induced cell cyto-pathogenicity should not be ignored by wound-care specialists. Silver does just the opposite to what PRP-gel offers, and inhibits important wound-healing cells-lines in tissue-culture. Australian- researchers have indicated that freshly transplanted keratinocytes are at risk, if exposed to a silver dressing-product [1]. Other workers show that silver-preparations and derivatives can also potentially inhibit re-epithelialisation and cell-migration, concepts that are critical to wound-healing and care [2, 3].
5. Conclusion
We provide in vitro supporting evidence that RegenPRP®-Kit, can enhance and stimulate fundamental wound-healing components such as keratinocytes, dermal fibroblasts and ADSC, in a human-explants, tissue-culture model. We provide tissue-culture evidence that platelet-rich plasma generated by the Regenlab® CE-marked THT-system, has the potential to promote new-tissue regeneration, cell-proliferation or wound-healing propensity in vitro, presumably through the trophic effects of released platelet-derived growth-factors from the gel. Thus, PRP shows potential to stimulate cell-growth of epidermal, dermal and mesodermal elements of the integument. The laboratory-science and tissue-culture evidence accumulated, suggest that correctly selected persons with chronic-wounds could benefit, in theory, from topically-applied autologous-PRP. Platelet-rich plasma does have a place in wound-healing and care, in preference to a chemical silver-based product, thereby avoiding the risk of granulation-tissue cauterization and cell-death, impairing wound-closure and negating wound-healing outcomes.
References
[1] J. Fong and F. Wood, Nanocrystalline silver-dressings in wound-management: a review, Int J Nanomedicine 2006 (1) 441-449.
[2] J. F. Frazer, L. Cuttle, M. Kempf and R. M. Kimble, Cytotoxicity of topical anti-microbial agents used in burn-wounds in Australia., ANZ J Surg 2004 (74) 139-142.
[3] V. K. Poon and A. Bur, In vitro cytotoxicity of silver: implication for clinical wound care, Burns 2004 (30) 140-147.
[4] E. Ranzato, M. Patrone, L. Mazzocco and B. Burlando, Platelet lysate stimulates wound repair of HaCaT keratinocytes, Br J Dermatol 2008 (159) 537-545.
[5] N. Kakudo, T. Minakata, T. Mitsui, S. Kushida, F. Z. Notodihardjo and K. Kusumoto, Proliferation-promoting effect of platelet-rich plasma on human adipose- derived stem cells and human dermal fibroblasts, Plast Reconstr Surg 2008 (122) 1352-60.
[6] C. R. Valeri, B. Saleem and G. Ragno, Release of platelet-derived growth factors and proliferation of fibroblasts in the relesates from platelets stored in the liquid state at 22 degrees after stimulation with agonists, Transfusion 2006 (46) 225-229.
[7] M. Krasna, D. Domanovic, A. Tomsic, U. Svajger and M. Jeras, Platelet gel stimulates proliferation of human dermal fibroblasts in vitro, Acta Dermatoven APA 2007 (16) 105-110.
[8] L. Mazzucco, V. Balbo, E. Cattana, R. Guaschino and P. Borzini, Not every PRP-gel is born equal: evaluation of growth factor availability for tissues through four PRP-gel preparations: Fibrinet, RegenPRP-Kit, Plateltex and one manual procedure, Vox Sang 2009 (97) 110-118.
[9] L. Mazzucco, V. Balbo, E. Cattana and P. Borzini, Platelet-rich plasma and platelet gel preparation using Plateltex, Vox Sang 2008 (94) 202-208.
[10] De Rossi R, A. C. de Oliveira Colho, G. S. de Mello, F. O. Frazilio, C. R. B. Leal, G. G. Facco and K. B. Brum, Effects of platelet-rich plasma gel on skin healing in surgical wound in horses, Acta Chirurgica Brasileira 2009 (24) 276-281.
[11] V. R. Driver, J. Hanft, C. P. Fylling and J. M. Beriou, Autogel diabetic foot ulcer study: a prospective, randomized, controlled trial of autologous platelet-rich plasma gel for the treatment of diabetic foot ulcers, Ostomy Wound Manage 2006 (52) 68-70.
[12] Y. Umeno, A. Okuda and G. Kimura, Proliferative behaviour of fibroblasts in plasma-rich culture medium, Jnl Cell Science 1989 (94) 567-575.
[13] R. E. Marx and A. K. Carg, Dental and Craniofacial Application of Platelet-Rich Plasma, Quintessence Books, Chicago, 2005, pp.1-154.
[14] B. L. Eppley, W. S. Pietrzak and W. Blanton, Platelet-rich plasma: a review of biology and applications in plastic surgery, Plastic Reconstr Surg 2006 (118) 147e-159e.
[15] M. Rosdy and L. C. Claus, Cytotoxicity testing of wound-dressings using normal human-keratinocytes in culture, J Biomed Res 1990 (24) 363-377.
[16] L. Wei, G. Henry, J. Fan, B. Bandyopadhyay, K. Pang, W. Garner, M. Chen and D. Woodley, Signals that initiate, augment and provide directionality for human keratinocyte motility, J Invest Dermatol 2004 (123) 622-633.
Apr.2010, Volume7, No.4 (Serial No.65) Journal of US-China Medical Science, ISSN 1548-6648, USA
Effect of Dietary Oleic Acid and Palmitic Acid on
Cerebellum Histological Changes and Sensorimotor
Coordination in Rat
H. Morovvati1, Z. Hosseinzadeh2, A. A. Moazedi2 and H. Najafzadeh3 1. Department of Histology, School of Veterinary Medicine, Shahid Chamran University, Ahvaz, Iran.
2. Department of Biology, School of Science, Shahid Chamran University, Ahvaz, Iran
3. Department of Pharmacology and Toxicology, School of Veterinary Medicine, Shahid Chamran University, Ahvaz, Iran
Abstract: Lipids are important constituents of the neuronal membrane. Also, kinds of fatty acids were supplied in the diet can affect the brain growth and the onset of myelinogenesis. So, in this study, the effect of oleic acid and palmitic acid on sensorimotor coordination and cerebellum histological changes was investigated. In present study, 9 groups (10 rats in each group) of Wistar immature rats were used. One group kept as control with similar environmental conditions to other groups. Four groups of rats were fed with diet containing 10% palmitic acid for 1 to 4 weeks respectively. Four groups of rats were fed with diet containing 10% oleic acid for 1 to 4 weeks respectively. After maturation (age at 90 weeks), the rats were tested for motor activity task by using Rota rod based on standard method and then the whole cerebellum were removed and samples were fixed in bouin for routine paraffin embedding method. The results showed that sensorimotor coordination was significantly (p < 0.01) increased in rats fed with oleic acid for 4 weeks. The sensorimotor coordination was significantly (p < 0.01, p < 0.5) increased in groups received palmitic acid for 1 and 2 weeks. Also, diameter of cerebellum was significantly (p < 0.001, p < 0.5) changed with oleic acid for 4 weeks and palmitic acid for 2 weeks. The diameter of molecular layer of cerebellum was significantly (p < 0.001, p < 0.5) changed with oleic acid for 2 and 4 weeks. Thus, palmitic and oleic acid can improve function of tissue of cerebellum in rat. Key words: Cerebellum, oleic acid, palmitic acid, sensorimotor, coordination, histological changes, rat.
1. Introduction
Lipids are important constituents of the neuronal membrane and changes in lipid composition may alter membrane activities [1]. Fatty acids deficiency may impair normal neurological development [2]. The fatty acids are involved in retinal function, learning and memory mechanisms, thermoregulation, pain, stress and sleep [3]. The cell function is not restricted to absolute levels of fatty acids but rather depend on the relative amounts of omega-3 and omega-6 in cell membrane [4, 5]. It was reported that supplemented docosahexaenoic acid (DHA) diet decreases accumulation of amyloid beta-peptide and number of
Corresponding author: H. Najafzadeh, assistant professor, Email: [email protected].
active microglia in hippocampus and increases exploratory of transgenic mice [6]. The developing brain produces the required palmitic acid [7]. Our previous investigation indicated palmitic acid affects on cognition process in rat [8] and oleic significantly increases spatial learning [9]. In present study, the effect of dietary oleic acid (omega 9) and palmitic acid on cerebellum histological changes and sensorimotor coordination in rat was investigated.
2. Materials and Methods
2.1 Animals
This study was done in lab of learning and memory and lab of veterinary histology of Shahid Chamran University. The rats were purchased from Joundishap-
Effect of Dietary Oleic Acid and Palmitic Acid on Cerebellum Histological Changes and Sensorimotor Coordination in Rat
10
our laboratory animal center (Ahvaz- Iran). Rats were fed diet that contained oleic acid or palmitic acid for 8 weeks before their adult age (i.e., from 4th to 8th week of age) and they were tested in adulthood. The rats were housed in individual cages with free access to water and Pellets food daily. So, 90 adult male Wistar rats (at 175+25g weight) were used and their age was 1.5-2 month at the training test. The study was done with permission based on ethical committee of laboratory sciences.
2.2 Group Treatment
Palmitic acid (10 g) or oleic acid (10 g) and standard food (90 g) were mixed. Palmitic acid (C16H32O2) and oleic acid (C18H3602) were obtained from Merck chemical company. At analysis, the diets contained the following matters: 5% soybean protein isolate, o.3% DL-methioninm, 32.7% corn starch, 25% sucrose, 2% cellulose powder, 5% mineral mixture, 1% vitamin. Rats were divided 9 groups: Group 1 to 4 was fed diet with 10% palmitic acid for 1 to 4 weeks respectively. Group 5 to 8 was fed diet with 10% palmitic acid for 1 to 4 weeks respectively (this protocol was obtained from pilot study and previous motor activity research). Group 9 was kept as control group and fed standard diet.
2.3 Behavioral Testing
In the Rotarod test, a rat was placed on a rotating rod apparatus (COSLAB Model PI –72- India). The speed of rotation was gradually increased and the rat’s ability to remain on the rotating rod or balances was recorded. The animals were placed on textured drums to avoid slipping. The Rotation was done at a constant speed for 10 rpm (RUN Mode), in a choice of 3 selected times: maximum 60 sec. Then average of three times was measured [10]. This model shows sensorimotor coordination.
2.4 Histological Evaluation
The rats were euthanized and their brain were removed and fixed by bouin for light microscopic
studies. Respect sections for light microscopic study were prepared by routine paraffin embedding method and were stained with haematoxylin-eosin [11]. Then, the cerebellum tissue studied by using routine histological protocols and the graticale lens and calibrated slide which were used for the estimation of diameter of granular and molecular layers.
2.5 Statistical Analysis
The student t-test and two ways ANOVA and post hot the tukey test (P < 0.05) were used for data analysis. The statistical analysis was performed using Minitab R13 software.
3. Results
3.1 Behavioral Results
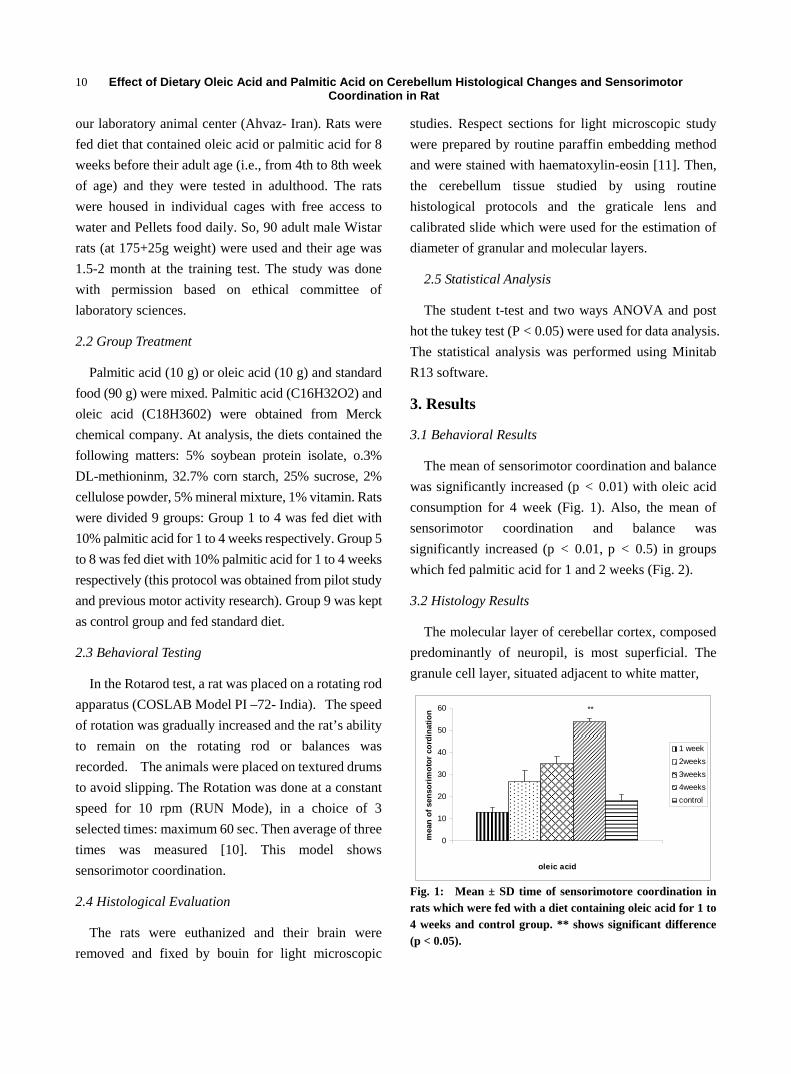
The mean of sensorimotor coordination and balance was significantly increased (p < 0.01) with oleic acid consumption for 4 week (Fig. 1). Also, the mean of sensorimotor coordination and balance was significantly increased (p < 0.01, p < 0.5) in groups which fed palmitic acid for 1 and 2 weeks (Fig. 2).
3.2 Histology Results
The molecular layer of cerebellar cortex, composed predominantly of neuropil, is most superficial. The granule cell layer, situated adjacent to white matter,
0
10
20
30
40
50
60
1
oleic acid
mea
n of
sen
sorim
otor
cor
dina
tion
1 week2weeks3weeks4weekscontrol
**
Fig. 1: Mean ± SD time of sensorimotore coordination in rats which were fed with a diet containing oleic acid for 1 to 4 weeks and control group. ** shows significant difference (p < 0.05).
Effect of Dietary Oleic Acid and Palmitic Acid on Cerebellum Histological Changes and Sensorimotor Coordination in Rat
11
0
10
20
30
40
50
60
1
palmitic acid
mea
n of
sen
sorim
otor
of
cord
inat
ion
1 week2weeks3weeks4weekscontrol
**
*
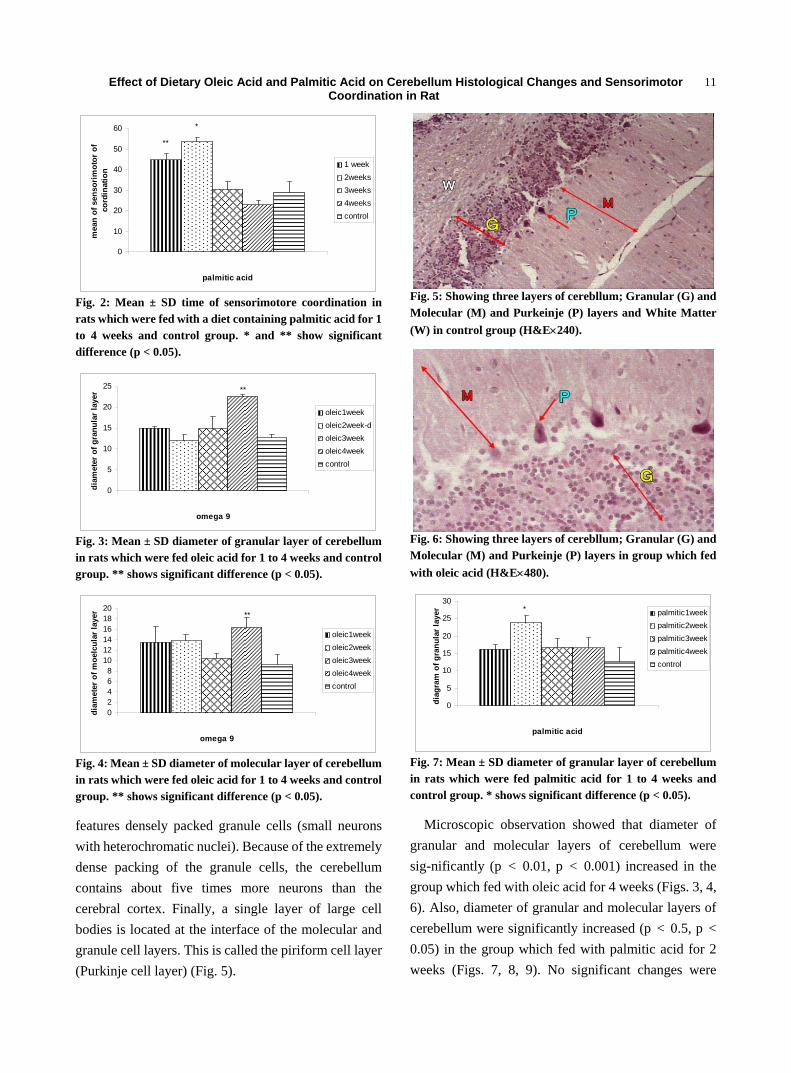
Fig. 2: Mean ± SD time of sensorimotore coordination in rats which were fed with a diet containing palmitic acid for 1 to 4 weeks and control group. * and ** show significant difference (p < 0.05).
0
5
10
15
20
25
1
omega 9
diam
eter
of g
ranu
lar
laye
r
oleic1weekoleic2week-doleic3weekoleic4weekcontrol
**
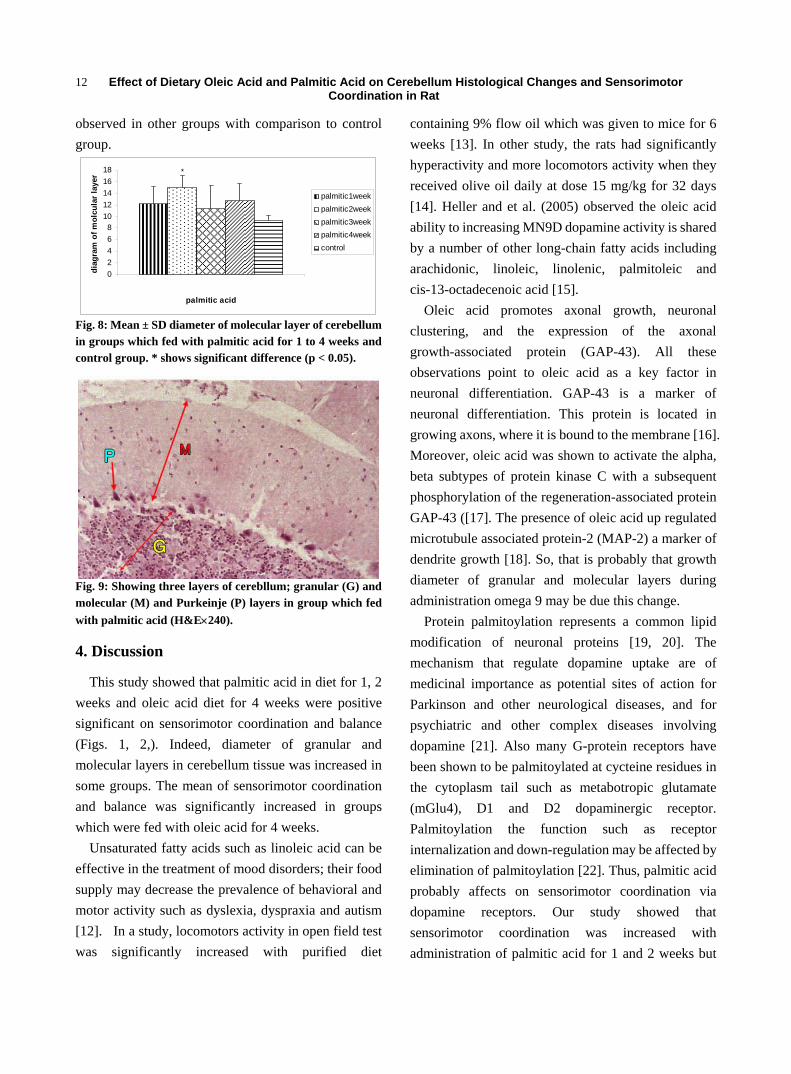
Fig. 3: Mean ± SD diameter of granular layer of cerebellum in rats which were fed oleic acid for 1 to 4 weeks and control group. ** shows significant difference (p < 0.05).
02468
101214161820
1
omega 9
diam
eter
of m
oelc
ular
laye
r
oleic1weekoleic2weekoleic3weekoleic4weekcontrol
**
Fig. 4: Mean ± SD diameter of molecular layer of cerebellum in rats which were fed oleic acid for 1 to 4 weeks and control group. ** shows significant difference (p < 0.05).
features densely packed granule cells (small neurons with heterochromatic nuclei). Because of the extremely dense packing of the granule cells, the cerebellum contains about five times more neurons than the cerebral cortex. Finally, a single layer of large cell bodies is located at the interface of the molecular and granule cell layers. This is called the piriform cell layer (Purkinje cell layer) (Fig. 5).
Fig. 5: Showing three layers of cerebllum; Granular (G) and Molecular (M) and Purkeinje (P) layers and White Matter (W) in control group (H&E×240).
Fig. 6: Showing three layers of cerebllum; Granular (G) and Molecular (M) and Purkeinje (P) layers in group which fed with oleic acid (H&E×480).
0
5
10
15
20
25
30
1
palmitic acid
diag
ram
of g
ranu
lar l
ayer palmitic1week
palmitic2weekpalmitic3weekpalmitic4weekcontrol
*
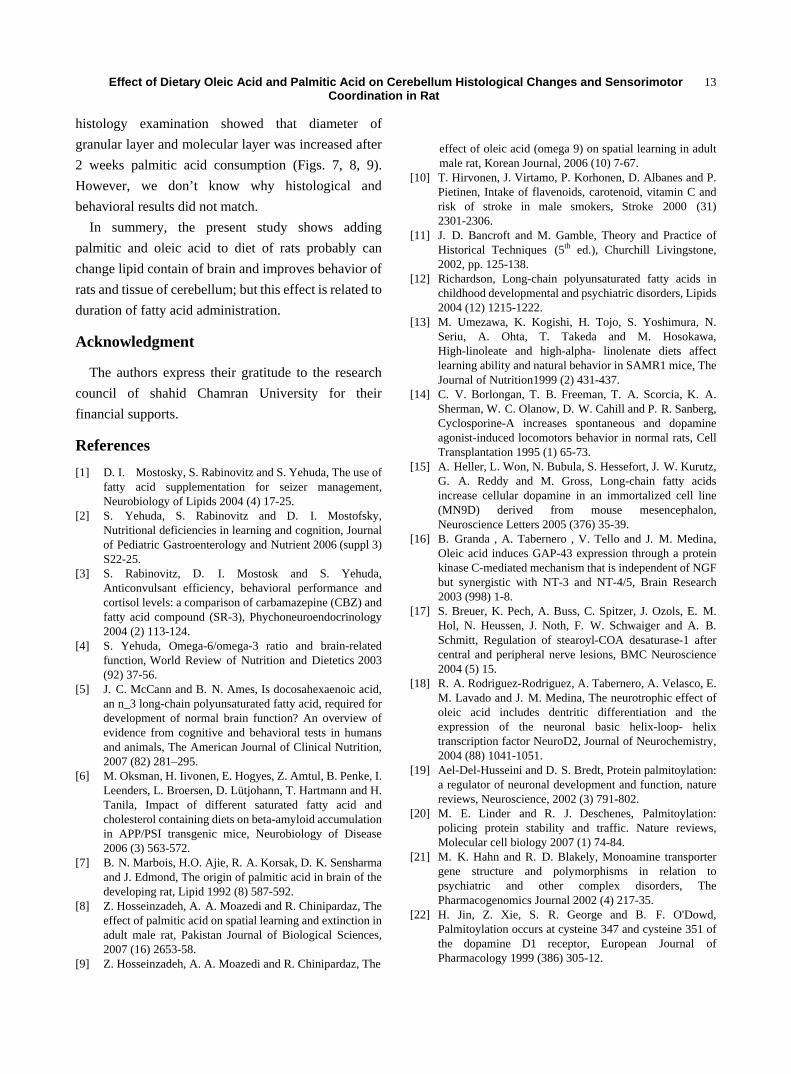
Fig. 7: Mean ± SD diameter of granular layer of cerebellum in rats which were fed palmitic acid for 1 to 4 weeks and control group. * shows significant difference (p < 0.05).
Microscopic observation showed that diameter of granular and molecular layers of cerebellum were sig-nificantly (p < 0.01, p < 0.001) increased in the group which fed with oleic acid for 4 weeks (Figs. 3, 4, 6). Also, diameter of granular and molecular layers of cerebellum were significantly increased (p < 0.5, p < 0.05) in the group which fed with palmitic acid for 2 weeks (Figs. 7, 8, 9). No significant changes were
Effect of Dietary Oleic Acid and Palmitic Acid on Cerebellum Histological Changes and Sensorimotor Coordination in Rat
12
observed in other groups with comparison to control group.
02468
1012141618
1
palmitic acid
diag
ram
of m
olcu
lar l
ayer
palmitic1weekpalmitic2weekpalmitic3weekpalmitic4weekcontrol
*
Fig. 8: Mean ± SD diameter of molecular layer of cerebellum in groups which fed with palmitic acid for 1 to 4 weeks and control group. * shows significant difference (p < 0.05).
Fig. 9: Showing three layers of cerebllum; granular (G) and molecular (M) and Purkeinje (P) layers in group which fed with palmitic acid (H&E×240).
4. Discussion
This study showed that palmitic acid in diet for 1, 2 weeks and oleic acid diet for 4 weeks were positive significant on sensorimotor coordination and balance (Figs. 1, 2,). Indeed, diameter of granular and molecular layers in cerebellum tissue was increased in some groups. The mean of sensorimotor coordination and balance was significantly increased in groups which were fed with oleic acid for 4 weeks.
Unsaturated fatty acids such as linoleic acid can be effective in the treatment of mood disorders; their food supply may decrease the prevalence of behavioral and motor activity such as dyslexia, dyspraxia and autism [12]. In a study, locomotors activity in open field test was significantly increased with purified diet
containing 9% flow oil which was given to mice for 6 weeks [13]. In other study, the rats had significantly hyperactivity and more locomotors activity when they received olive oil daily at dose 15 mg/kg for 32 days [14]. Heller and et al. (2005) observed the oleic acid ability to increasing MN9D dopamine activity is shared by a number of other long-chain fatty acids including arachidonic, linoleic, linolenic, palmitoleic and cis-13-octadecenoic acid [15].
Oleic acid promotes axonal growth, neuronal clustering, and the expression of the axonal growth-associated protein (GAP-43). All these observations point to oleic acid as a key factor in neuronal differentiation. GAP-43 is a marker of neuronal differentiation. This protein is located in growing axons, where it is bound to the membrane [16]. Moreover, oleic acid was shown to activate the alpha, beta subtypes of protein kinase C with a subsequent phosphorylation of the regeneration-associated protein GAP-43 ([17]. The presence of oleic acid up regulated microtubule associated protein-2 (MAP-2) a marker of dendrite growth [18]. So, that is probably that growth diameter of granular and molecular layers during administration omega 9 may be due this change.
Protein palmitoylation represents a common lipid modification of neuronal proteins [19, 20]. The mechanism that regulate dopamine uptake are of medicinal importance as potential sites of action for Parkinson and other neurological diseases, and for psychiatric and other complex diseases involving dopamine [21]. Also many G-protein receptors have been shown to be palmitoylated at cycteine residues in the cytoplasm tail such as metabotropic glutamate (mGlu4), D1 and D2 dopaminergic receptor. Palmitoylation the function such as receptor internalization and down-regulation may be affected by elimination of palmitoylation [22]. Thus, palmitic acid probably affects on sensorimotor coordination via dopamine receptors. Our study showed that sensorimotor coordination was increased with administration of palmitic acid for 1 and 2 weeks but
Effect of Dietary Oleic Acid and Palmitic Acid on Cerebellum Histological Changes and Sensorimotor Coordination in Rat
13
histology examination showed that diameter of granular layer and molecular layer was increased after 2 weeks palmitic acid consumption (Figs. 7, 8, 9). However, we don’t know why histological and behavioral results did not match.
In summery, the present study shows adding palmitic and oleic acid to diet of rats probably can change lipid contain of brain and improves behavior of rats and tissue of cerebellum; but this effect is related to duration of fatty acid administration.
Acknowledgment
The authors express their gratitude to the research council of shahid Chamran University for their financial supports.
References [1] D. I. Mostosky, S. Rabinovitz and S. Yehuda, The use of
fatty acid supplementation for seizer management, Neurobiology of Lipids 2004 (4) 17-25.
[2] S. Yehuda, S. Rabinovitz and D. I. Mostofsky, Nutritional deficiencies in learning and cognition, Journal of Pediatric Gastroenterology and Nutrient 2006 (suppl 3) S22-25.
[3] S. Rabinovitz, D. I. Mostosk and S. Yehuda, Anticonvulsant efficiency, behavioral performance and cortisol levels: a comparison of carbamazepine (CBZ) and fatty acid compound (SR-3), Phychoneuroendocrinology 2004 (2) 113-124.
[4] S. Yehuda, Omega-6/omega-3 ratio and brain-related function, World Review of Nutrition and Dietetics 2003 (92) 37-56.
[5] J. C. McCann and B. N. Ames, Is docosahexaenoic acid, an n_3 long-chain polyunsaturated fatty acid, required for development of normal brain function? An overview of evidence from cognitive and behavioral tests in humans and animals, The American Journal of Clinical Nutrition, 2007 (82) 281–295.
[6] M. Oksman, H. Iivonen, E. Hogyes, Z. Amtul, B. Penke, I. Leenders, L. Broersen, D. Lütjohann, T. Hartmann and H. Tanila, Impact of different saturated fatty acid and cholesterol containing diets on beta-amyloid accumulation in APP/PSI transgenic mice, Neurobiology of Disease 2006 (3) 563-572.
[7] B. N. Marbois, H.O. Ajie, R. A. Korsak, D. K. Sensharma and J. Edmond, The origin of palmitic acid in brain of the developing rat, Lipid 1992 (8) 587-592.
[8] Z. Hosseinzadeh, A. A. Moazedi and R. Chinipardaz, The effect of palmitic acid on spatial learning and extinction in adult male rat, Pakistan Journal of Biological Sciences, 2007 (16) 2653-58.
[9] Z. Hosseinzadeh, A. A. Moazedi and R. Chinipardaz, The
effect of oleic acid (omega 9) on spatial learning in adult male rat, Korean Journal, 2006 (10) 7-67.
[10] T. Hirvonen, J. Virtamo, P. Korhonen, D. Albanes and P. Pietinen, Intake of flavenoids, carotenoid, vitamin C and risk of stroke in male smokers, Stroke 2000 (31) 2301-2306.
[11] J. D. Bancroft and M. Gamble, Theory and Practice of Historical Techniques (5th ed.), Churchill Livingstone, 2002, pp. 125-138.
[12] Richardson, Long-chain polyunsaturated fatty acids in childhood developmental and psychiatric disorders, Lipids 2004 (12) 1215-1222.
[13] M. Umezawa, K. Kogishi, H. Tojo, S. Yoshimura, N. Seriu, A. Ohta, T. Takeda and M. Hosokawa, High-linoleate and high-alpha- linolenate diets affect learning ability and natural behavior in SAMR1 mice, The Journal of Nutrition1999 (2) 431-437.
[14] C. V. Borlongan, T. B. Freeman, T. A. Scorcia, K. A. Sherman, W. C. Olanow, D. W. Cahill and P. R. Sanberg, Cyclosporine-A increases spontaneous and dopamine agonist-induced locomotors behavior in normal rats, Cell Transplantation 1995 (1) 65-73.
[15] A. Heller, L. Won, N. Bubula, S. Hessefort, J. W. Kurutz, G. A. Reddy and M. Gross, Long-chain fatty acids increase cellular dopamine in an immortalized cell line (MN9D) derived from mouse mesencephalon, Neuroscience Letters 2005 (376) 35-39.
[16] B. Granda , A. Tabernero , V. Tello and J. M. Medina, Oleic acid induces GAP-43 expression through a protein kinase C-mediated mechanism that is independent of NGF but synergistic with NT-3 and NT-4/5, Brain Research 2003 (998) 1-8.
[17] S. Breuer, K. Pech, A. Buss, C. Spitzer, J. Ozols, E. M. Hol, N. Heussen, J. Noth, F. W. Schwaiger and A. B. Schmitt, Regulation of stearoyl-COA desaturase-1 after central and peripheral nerve lesions, BMC Neuroscience 2004 (5) 15.
[18] R. A. Rodriguez-Rodriguez, A. Tabernero, A. Velasco, E. M. Lavado and J. M. Medina, The neurotrophic effect of oleic acid includes dentritic differentiation and the expression of the neuronal basic helix-loop- helix transcription factor NeuroD2, Journal of Neurochemistry, 2004 (88) 1041-1051.
[19] Ael-Del-Husseini and D. S. Bredt, Protein palmitoylation: a regulator of neuronal development and function, nature reviews, Neuroscience, 2002 (3) 791-802.
[20] M. E. Linder and R. J. Deschenes, Palmitoylation: policing protein stability and traffic. Nature reviews, Molecular cell biology 2007 (1) 74-84.
[21] M. K. Hahn and R. D. Blakely, Monoamine transporter gene structure and polymorphisms in relation to psychiatric and other complex disorders, The Pharmacogenomics Journal 2002 (4) 217-35.
[22] H. Jin, Z. Xie, S. R. George and B. F. O'Dowd, Palmitoylation occurs at cysteine 347 and cysteine 351 of the dopamine D1 receptor, European Journal of Pharmacology 1999 (386) 305-12.

Apr.2010, Volume7, No.4 (Serial No.65) Journal of US-China Medical Science, ISSN 1548-6648, USA
Apr.2010, Volume7, No.4 (Serial No.65) Journal of US-China Medical Science, ISSN 1548-6648, USA
Pro-apoptotic Effect of Recombinant Anti-HER2 Fusion Protein Scfv/Tbid on Osteosarcoma E10 Cells
Xiuchun Qiu1*, Lequn Shan1*, Sai Ma2, Zhengang JI1, Tongtao Yang 1, Hua Long1, Yanming Xu3, Yong Zhou1, Baoan Ma1, Angang Yang4 and Qingyu Fan1 1. Department of Orthopaedics Surgery, Tangdu hospital, Xi’an 710038, China
2. Department of Prosthodontics, School of Stomatology, Fourth Military Medical University, Xi'an 710038, China
3. Department of Biochemistry and Molecular Biology, Fourth Military Medical University, Xi'an 710038, China
4. Department of Immunology, Faculty of Preclinical Medicine; Fourth Military Medical University, Xi'an 710038, China Abstract: Objective: To construct the gene of a recombinant anti-HER2 fusion protein, ScFv/tBid, and investigate its pro-apopotic effect on osteosarcoma E10 cell line. Methods: First, the expression of HER-2 in E10 cells was examined. Then the gene of recombinant tBid fusion protein was constructed by sequentially fusing the coding sequences of a signal peptide, a single-chain HER2 antibody, a PE translocation domain and tBid. The effect of the recombinant fusion protein on the morphology and growth status of E10 cells was studied by immunofluorescent staining. Meanwhile, pro-apoptotic effect was observed by Annexin V-FITC staining and TUNEL staining. Results: The expression of HER-2 in E10 was higher than control group. The recombinant ScFv/tBid protein was expressed and cell shrinkage and nuclear condensation can be detected in E10 cells transfected with pCMV-ScFv/tBid. The apoptosis rate in E10 cells transfected with pCMV-ScFv/tBid or pCMV was 16.1% and 4.5%, respectively. The pro-apoptotic effect of recombinant ScFv/tBid protein was further verified by TUNEL staining. Conclusion: The recombinant ScFv/tBid protein can induce apoptosis in HER2/neu - positive osteosarcoma. Key words: TBid, HER2, fusion protein, osteosarcoma cell, apoptosis.
1. Introduction
BH3-interacting domain death agonist (BID) is a pro-apoptotic BH3 domain– only member of the Bcl-2 family. Normally, full-length BID presents in the cytosol, and does not exert any active pro-apoptotic effect. However, when it is stimulated by apoptotic signals, BID can be cleaved and activated by a number of protease, including caspase-8, granzyme B, calpains and cathepsins, into a 15.5-kDa COOH-terminal fragment (tBID), which can subsequently translocate to the mitochondria, cause the release of Cytochrome C and other pro-apoptotic molecules, and finally lead to apoptosis of the cell. [1-5]
* The first two authors contributed equally to this study
Cocorresponding author: Qingyu Fan, MD., professor, research fields: malignant bone tumor, pelvic tumor, sacral tumor and so on. E-mail address: [email protected].
HER2 is identified as a member of the epidermal growth factor receptor family and its intra-cellular domain act as tyrosine kinase. The amplification and over-expression of HER2 gene can be observed in a variety of malignant tumors, including 20% to 25% ovarian cancer and breast cancer, 35% to 45% pancreatic cancer, 90% colorectal cancer, 16%~57% nonsmall-cell lung cancer [3] and 58% pulmonary metastasis of osteosarcoma. [6, 7] Now, HER2 is accepted as a marker for malignant tumors and is deemed as an ideal target molecular for cancer gene therapy. [8] The single-chain HER2 antibody e23sFv is derived from a mouse monoclonal antibody e23 with high-affinity binding to the extracellular domain of HER2 protein. [9] HER2 antibody can act as a targeting system that help to send the therapeutic molecular HER2 positive tumor tissues specifically and induce targeted killing of the tumor tissues. Up to now, several

Pro-apoptotic Effect of Recombinant Anti-HER2 Fusion Protein Scfv/Tbid on Osteosarcoma E10 Cells
15
therapeutic immunotoxins that employ HER2 antibody as a targeting molecule have been in the stage of clinical trial. To make normal cells, such as lymphocytes and myocytes, capable of secreting certain therapeutic molecules that could targetedly recognize and kill tumor cells is accepted as a new strategy in tumor treatment and has been adopted by several researchers.
Osteosarcoma is the most common primary malignant bone tumor in children and adolescents. Overexpression of HER2 has been observed in 40%-50% osteosarcoma cases and 58% samples of pulmonary metastasis of osteosarcoma. [6-7] Moreover, it has been suggested that the higher the expression of HER2 is, the worse the outcome of the patients would be. [10] In this study, we constructed the gene of a recombinant anti-HER2 fusion protein, ScFv/tBid, investigated the pro-apoptotic effect of the recombinant protean on osteosarcoma cell line E10, and explored the possible application of this recombinant protein in future osteosarcoma treatment.
2.Materials and Methods
2.1 Materials
Recombinant immuno-AIF gene was constructed by Dr. Yu by sequential fusion of the gene of a signal peptide, a single-chain Her2 antibody e23sFv, a PEA translocation PEII and an active AIF gene. [11] pCMV vector, pcDNA3-tBid61 plasmid and pCDNA3-PE/ tBid61 plasmid were constructed and reserved by our institusion. Competent bacteria DH5α and human osteosarcoma cell line E10 were reserved by our institusion. PRIM 1640, liposome Lipofecta- mine2000TM and fetal calf serum were purchased from Invitrogen Inc. Goat anti-human tBid multiclonal antibody, rabbit anti-human Cyt C multiclonal antibody, mouse anti-human HER2 multiclonal antibody and isotype were purchased from Santa Cruz Biotechnology Inc (Santa Cruz, CA). Biotin labeled rabbit anti-goat IgG, FITC labeled goat anti-rabbit IgG, DAPI, Avidin-Cy3 were products of Molecular Probes
(Oregon, USA). TUNEL kit was purchased from Calbiochem (Darmstadt, Germany). Restriction enzyme XbaⅠ, EcoRⅠ, NotⅠ and T4 DNA ligase were all purchased from TaKaRa Biotechnology Inc (Shiga, Japan).
2.2 Evaluation of HER2 Expression on Osteosarcoma Cell Line E10 by Indirect Immunofluorescence Staining and Flow Cytometry.
Cell suspension was prepared using RPMI 1640 containing 10% fetal bovine serum to reach a density of 5×106~1×107/mL. 40 μl of this cell suspension and 50μl inactivated rabbit serum (1:20 diluted with DPBS) were added into a plastic centrifuge tube containing 5~50μl mouse anti-human HER2 antibody. The mixture was incubated at 4℃ for 30 min before it was washed with eluant for three times (2 mL eluant each time, centrifuged at 1000 rpm for 5min). The supernatant was discarded and 100 μl FITC labeled goat anti-mouse IgG (1: 60) was added. This mixture was well shaken and incubated at 4℃ for 30 min before it was washed for three times (4℃, 1000 rpm × 5 min). Finally 1 mL fixation fluid was added and flow cytometry analysis was performed.
2.3 Construction of Recombinant pCMV-ScFv/tBid Vector
Recombinant ScFv/tBid gene was generated by sequential fusion of the following gene constructs: a signal peptide (MKHLWFFLLLVAAPRWVLS), a single-chain HER2 antibody (sFv23e, human origin), a PE translocation domain (aa 253-358) and a truncated Bid (tBid). The recombinant gene was cloned into a pCMV plasmid and was verified by DNA sequencing.
2.4 Cell Transfection
E10 cells at ogarithmic growth phase were harvested and plated into a 6-well plate at a density of 1×106 per well. After 24h’s incubation, the cells were washed twice with RPMI 1640. pCMV-ScFv/tBid and pCMV were mixed with Lipofectamine2000TM, respectively,
Pro-apoptotic Effect of Recombinant Anti-HER2 Fusion Protein Scfv/Tbid on Osteosarcoma E10 Cells
16
and the mixtures were incubated for 20 min at room temperature to form DNA-liposome mixtures. The DNA-liposome mixtures were administered to cells and the whole mixtures were incubated at 37℃ with 5% CO2 for 6 h. Finally, the DNA-liposome mixture was removed and the cells were further incubated with 1 mL PRMI 1640 containing 200 ml/L fetal calf serum and no antibiotic.
2.5 Immunocytochemistry Study of Cell Morphology and Bid Expression
The cells were cultured on coverslips in RPMI 1640 containing 10% fetal bovine serum, fixed with a freshly prepared paraformaldehyde solution [40g/L in PBS (pH 7.4)] for 30 min at room temperature, and permeated with 0.1% Triton X- 100 for 15 min. Endogenous peroxidase was deactivated with 30ml/L H2O2, and the samples were blocked with goat serum. The cells were stained with antibodies recognizing tBid and cytochrome c as the primary antibodies, with biotin-linked anti-goat IgG and FITC-linked anti-rabbit IgG as the secondary antibodies and Avidin-Cy3- linked anti-biotin antibodies (1: 100) as the tertiary antibody. DAPI was also used for nucleus staining. Finally, the samples were observed with with fluorescence microscope.
2.6 Flow Cytometry Study of Cell Apoptosis after Pcmv-Scfv/Tbid Infection
E10 cells were plated into a 6-well plate at the density of 1×106 per well. Cells were collecte 72 hours after they were infected with either pCMV-ScFv/tBid vector (experimental group) or pCMV vector (control group), and Annexin V-FITC/PI staining was done according to the manufacturer’s instructions. Cells were then analyzed by flow cytometry.
2.7 Apoptosis Detection by TUNEL Staining
TUNEL staining was performed using TdT-FragELTM DNA Fragmentation Detection kit according to the manufacture’s instructions. In the
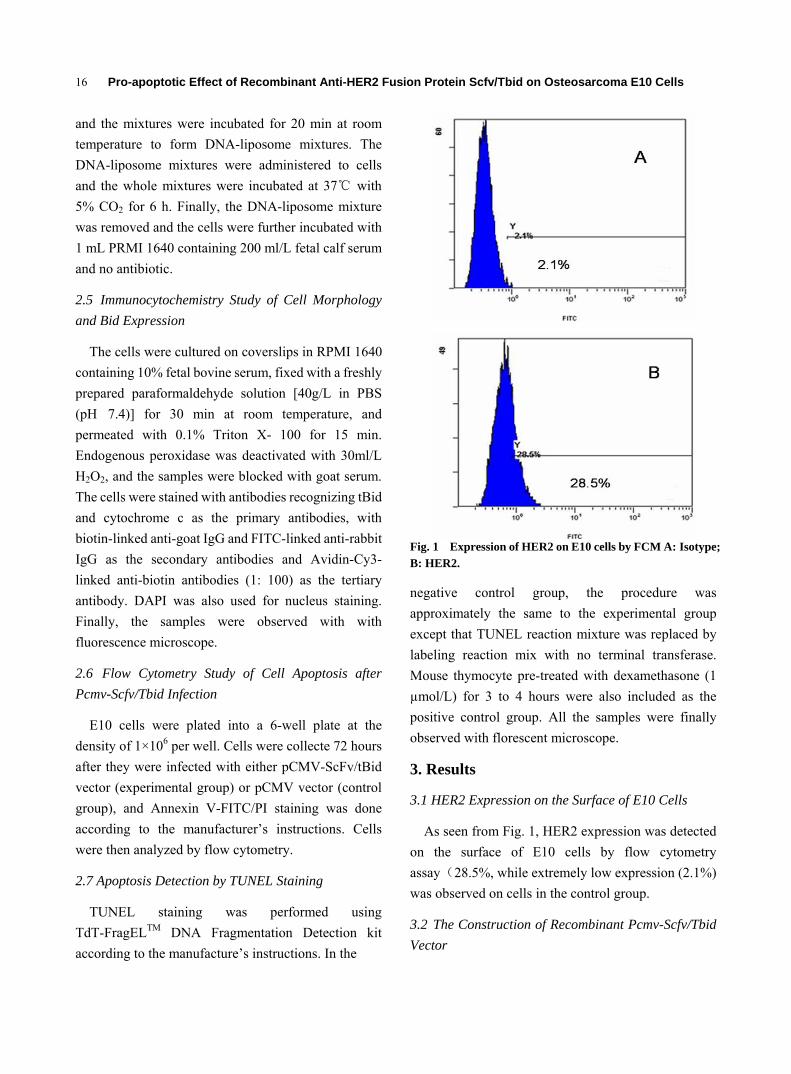
Fig. 1 Expression of HER2 on E10 cells by FCM A: Isotype; B: HER2.
negative control group, the procedure was approximately the same to the experimental group except that TUNEL reaction mixture was replaced by labeling reaction mix with no terminal transferase. Mouse thymocyte pre-treated with dexamethasone (1 µmol/L) for 3 to 4 hours were also included as the positive control group. All the samples were finally observed with florescent microscope.
3. Results
3.1 HER2 Expression on the Surface of E10 Cells
As seen from Fig. 1, HER2 expression was detected on the surface of E10 cells by flow cytometry a (ssay 28.5%, while extremely low expression (2.1%) was observed on cells in the control group.
3.2 The Construction of Recombinant Pcmv-Scfv/Tbid Vector
Pro-apoptotic Effect of Recombinant Anti-HER2 Fusion Protein Scfv/Tbid on Osteosarcoma E10 Cells
17
The constructed pCMV-e23sFv-PE II(253-364)- tBid61 vector was verified through double digestion (EcoRⅠ and XbaⅠ, NotⅠ, XbaⅠ, respectively). As seen from the result of electrophoresis, the two fragments, 400 bp and 750bp respectively, were of the same size as anticipated. The construct was also verified by DNA sequencing, and named pCMV-ScFv/tBid (Fig. 2).
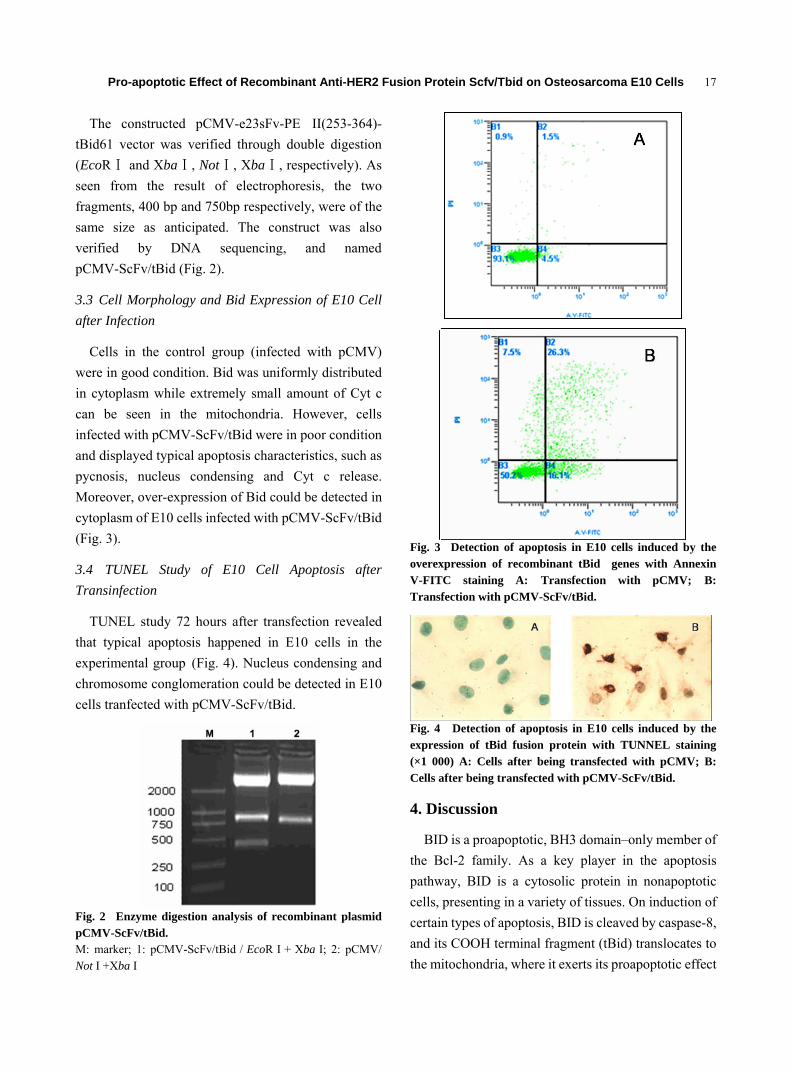
3.3 Cell Morphology and Bid Expression of E10 Cell after Infection
Cells in the control group (infected with pCMV) were in good condition. Bid was uniformly distributed in cytoplasm while extremely small amount of Cyt c can be seen in the mitochondria. However, cells infected with pCMV-ScFv/tBid were in poor condition and displayed typical apoptosis characteristics, such as pycnosis, nucleus condensing and Cyt c release. Moreover, over-expression of Bid could be detected in cytoplasm of E10 cells infected with pCMV-ScFv/tBid (Fig. 3).
3.4 TUNEL Study of E10 Cell Apoptosis after Transinfection
TUNEL study 72 hours after transfection revealed that typical apoptosis happened in E10 cells in the experimental group (Fig. 4). Nucleus condensing and chromosome conglomeration could be detected in E10 cells tranfected with pCMV-ScFv/tBid.
Fig. 2 Enzyme digestion analysis of recombinant plasmid pCMV-ScFv/tBid. M: marker; 1: pCMV-ScFv/tBid / EcoR I + Xba I; 2: pCMV/ Not I +Xba I
Fig. 3 Detection of apoptosis in E10 cells induced by the overexpression of recombinant tBid genes with Annexin V-FITC staining A: Transfection with pCMV; B: Transfection with pCMV-ScFv/tBid.
Fig. 4 Detection of apoptosis in E10 cells induced by the expression of tBid fusion protein with TUNNEL staining (×1 000) A: Cells after being transfected with pCMV; B: Cells after being transfected with pCMV-ScFv/tBid.
4. Discussion
BID is a proapoptotic, BH3 domain–only member of the Bcl-2 family. As a key player in the apoptosis pathway, BID is a cytosolic protein in nonapoptotic cells, presenting in a variety of tissues. On induction of certain types of apoptosis, BID is cleaved by caspase-8, and its COOH terminal fragment (tBid) translocates to the mitochondria, where it exerts its proapoptotic effect

Pro-apoptotic Effect of Recombinant Anti-HER2 Fusion Protein Scfv/Tbid on Osteosarcoma E10 Cells
18
by inducing the release of proapoptotic factors, such as cytochrome C and Apoptosis Inducing Factor (AIF). Cytochrome c can activate Apaf-1-Caspase 9 apoptotic complex and thereafter induce apoptosis by activating the Caspase passway, while AIF, which could translocate from cytoplasm to nucleus after releasing from the mitochondia, could induce cutting of large pieces of DNA and mediate a specific apoptosis procedure that is independent of Caspase passway. [1-2, 12-13] Since tBid could induce apoptosis through two independent passways, it is deemed as a potent proapoptotic factor that could be widely used in tumor researches.
The HER2 protein is a transmembrane glycoprotein (p185), classified as a member of the epidermal growth factor receptor (EGFR) family. It is reported to be overexpressed in several adenocarcinomas, including breast, lung, and stomach tumors, [14-16] but is not detected in normal cells. Thus HER2 may be an ideal molecular target for cancer gene therapy. Up to now, several therapeutic immunotoxins that employ HER2 antibody as a targeting molecule have been in the stage of clinical trial [11, 17-19]. In this study, HER2 expression was detected on the surface of E10 cells by flow cytometry assay(28.5%, suggesting that HER2 might be an effective target for osteosarcoma therapy.
In the study reported here, we employed tBid as an effector molecule on consideration that tBid is a small molecule with strong and prompt pro-apoptotic effect. We transfected osteosarcoma cell line E10 with the gene encoding this recombinant protein ScFv/tBid and studied the pro-apoptotic effect of this recombinant protein gainst HER2 positive E10 cells. The result of indirect immunofluorescent assay showed that after pCMV-ScFv/tBid transfection, E10 cells displayed several morphoplgy characteristics of apoptosis including cell pycnosis and nucleus condensing. Further verification by Annexin V and flow cytometry study revealed that the apoptosis rate in cells transfected with pCMV-ScFv/tBid was significantly higer than those transfected with pCMV. Moreover, the
pro-apoptotic effect of the constructed pCMV-ScFv/tBid was again verified by TUNEL staining since E10 cells in the experimental group displayed typical characteristics of apoptosis.
In summary, this study proved that the expression of the recombinant protein ScFv/tBid could effectively induce apoptosis in HER2 positive osteosarcoma cells and this study may hopefully provoke some new thoughts in the treatment of HER2 positive tumors and might lead to a novel practical therapeutic strategy of osteosarcoma patients.
Acknowledgements
This work was supported by grants from the National Natural Science Foundation of China (No. 30471988, 30873027, 30901784 and No.30330610) and Postdoctoral Science Foundation of China (No.2005038259).
References [1] X. M. Yin, Bid, a BH3-only multi-functional molecule, is
at the cross road of life and death, Gene 2006 (369) 7–19. [2] M. D. Esposti, The roles of Bid, Apoptosis 2002 (7)
433-440. [3] C. N. Baxevanis, P. A. Sotiropoulou and N. N. Sotiriadou
et al., Immunobiology of HER-2/neu oncoprotein and its potential application in cancer immunotherapy, Cancer lmmunol lmmunother 2004 (53) 166-175.
[4] N. J. Waterhouse, K. A. Sedelies and J. A. Trapani et al, Role of Bid-induced mitochondrial outer membrane permeabilization in granzyme B-induced apoptosis, Immunol Cell Biol 2006 (84)72-78.
[5] S. N. Willis and J. M. Adams, Life in the balance: how BH3-only proteins induce apoptosis, Curr Opin Cell Biol 2005 (17) 617-625.
[6] H. Zhou and R. L. Randall, Brothman: Her-2/neu expression in osteosarcoma increases risk of lung metastasis and can be associated with gene amplification, J Pediatr Hematol Oncol 2003 (25) 27-32.
[7] C. D. Morris, R. Gorlick and G. Huvos et al., Human epidermal growth factor receptor 2 as a prognostic indicator in Osteogenic Sarcoma, Clin Orthop Relat Res 2001 (382)59-65.
[8] F. Penault-Llorca, Targeted therapies: the question of target detection and evaluation, Bull Cancer 2007 (94) 245-248.

Pro-apoptotic Effect of Recombinant Anti-HER2 Fusion Protein Scfv/Tbid on Osteosarcoma E10 Cells
19
[9] J. K. Batra, P. G. Kasprzyk and R. E. Bird et al., Recombinant anti-erbB2 immunotoxins containing Pseudomonas exotoxin, Proc Natl Acad Sci USA 1992 (89) 5867–5871.
[10] R. Gorlick, A. G. Huvos and G. Heller et al., Expression of HER2/erbB-2 correlates with survival in osteosarcoma, J Clin Oncol1 1999 (7) 2781–2788.
[11] C. J. Yu, L. T. Jia and Y. L. Meng et al., Selective proapoptotic activity of a secreted recombinant antibody/AIF fusion protein in carcinomas overexpressing HER2, Gene Therapy 2005 (13) 313-320.
[12] C. Penaloza, S. Orlanski and Y. Ye et al., Cell death in mammalian development, Curr Pharm Des1 2008 (4) 184-96.
[13] S. Zinkel, A. Gross and E. Yang et al., BCL2 family in DNA damage and cell cycle control, Cell Death Differ 2006 (13)1351-1359.
[14] T. Cooke, J. Reeves, A. Lannigan and P. Stanton et al., The value of the human epidermal growth factor receptor-2 (HER2) as a prognostic marker, European Journal of Cancer 2001 (Supplement 1) 3-10.
[15] K. Junker, U. Stachetzki and D. Rademacher et al., HER2/neu expression and amplification in non-small cell lung cancer prior to and after neoadjuvant therapy, Lung Cancer 2005 (48) 59-67.
[16] M. Tanner, M. Hollmen and T. T. Junttila et al., Amplification of HER-2 in gastric carcinoma: association with Topoisomerase IIalpha gene amplification, intestinal type, poor prognosis and sensitivity to trastuzumab, Ann Oncol 2005 (16) 273–278.
[17] L. T. Jia, L. H. Zhang and C. J. Yu et al., Specific tumoricidal activity of a secreted proapoptotic protein consisting of HER2 antibody and constitutively active caspase-3, Cancer Res 2003 (63) 3257-3262.
[18] T. Wang, J. Zhao and J. L. Ren et al., Recombinant immunoproapoptotic proteins with furin site can translocate and kill HER2-positive cancer cells, Cancer Research 2007 (67)11830-11839.
[19] Y. M. Xu, L. F. Wang and L. T. Jia et al., A caspase-6 and anti-human epidermal growth factor receptor-2 (HER2) antibody chimeric molecule suppresses the growth of HER2-overexpressing tumors, J Immunol 2004 (173) 61-67.
Apr.2010, Volume7, No.4 (Serial No.65) Journal of US-China Medical Science, ISSN 1548-6648, USA
The Aged Organism as a Model of Successful Copping with Tumor Progression–Implications for Therapy
Judith Leibovici, Tatiana Kaptzan, Orit Itzhaki, Ehud Skutelsky, Judith Sinai, Moshe Michowitz, Ginnette Schiby, Annette Siegal and Monica Huszar Department of Pathology, Sackler Faculty of Medicine, Tel-Aviv University, Tel-Aviv, 69978 Israel Abstract: The proportion of aged individuals in the population is constantly rising. Few studies have been dedicated to the effect of aging on tumor biology and even fewer on age-adjusted cancer therapy. Cancer incidence is known to augment with age. However, tumor growth and metastasis often proceed at a slower rate in aged organisms. Mechanisms underlying this reduced tumor aggressiveness in the aged have been demonstrated by our and other groups: (1) Increased apoptosis of tumor cells in old mice; (2) Reduced angiogenesis; (3) Modifications in immune responses. Aged tissues presumably create a microenvironment which favors decreased tumor aggressiveness. We postulated that it may be possible to design age-adjusted treatment modalities based on the mechanism(s) responsible for the reduced tumor progression rate in the aged. Based on these mechanisms, we have shown that three treatment modalities (drugs inducing apoptotic cell death, anti-angiogenic agent and immunomodulators) display an age-related differential effect on two experimental tumors. Very remarkably, the inhibition was generally more pronounced in old than in young mice. The microenvironment of the aged organism appears to cope more successfully with metastatic spread and mice survival than that of young organisms. This might have implications for a novel approach to advanced cancer therapy. Key words: Cancer therapy, aging, tumor microenvironment.
1. Introduction
Cancer is a disease that occurs predominantly in elderly individuals who represent an ever growing fraction of the population. The absolute number of cancer patients in the USA is expected to double by year 2030 [1]. In Europe, over 45% of all cancers occur in patients over 70 years of age [2]. Seventy percent of all neoplasms are expected to occur in persons 65 years and over by the year 2020, which will lead to an increased cancer-related morbidity among the elderly [3].
Treatment of cancer has improved in persons under 50 but mortality has not been reduced for older cancer patients [4], probably due to the reluctance that physicians display to undertake aggressive therapy in elderly cancer patients [5]. Aged cancer patients have actually often been offered suboptimal treatment [6],
Corresponding author: Judith Leibovici, PhD, professor, research fields: cancer therapy, tumor microenvironment, aging, immunotherapy. Email: [email protected].
due to the numerous pathologies of aged individuals and to their higher susceptibility to the aggressive anti-tumoral treatments in use.
Evidently, the ageing host is very different from the young one. What is less known, or in any case, not at all considered, is that tumor behavior in the aged is also different. Specifically, while cancer incidence is known to augment with age [7], paradoxically, tumor growth and metastasis were often found to proceed at a slower rate in aged organisms, in both humans [8] and in experimental models [9]. Bronchogenic cancer [10] and cancers of breast [11] and colon [12] were reported to grow and metastasize at a lower rate in old patients. A reduced aggressiveness in aged as compared to young animals was found as well in experimental tumors [9, 13, 14]. We have also reported this phenomenon in the B16 melanoma 15 and in the AKR lymphoma [16].
The mechanisms responsible for the interesting phenomenon of the reduced tumor aggressiveness in

The Aged Organism as a Model of Successful Copping with Tumor Progression – Implications for Therapy
21
aged compared to young organisms have not yet been established. Decreased proliferative capacity in the old has been suggested [17]. The rate of DNA synthesis in tumors from old animals in organ culture was found to be lower than in tumors from young animals [18] and decreases in growth factor and hormone availability with age have also been documented [19, 20].
We have demonstrated an increased apoptotic cell death in tumors from old as compared to those from young mice bearing the B16 melanoma and the AKR lymphoma [21]. Reduced angiogenesis with age has also been suggested to constitute a possible mechanism of the decreased tumor progression rate in old as compared to young organisms [22, 23]. Modifications in anti-tumoral immune reactions with age have been demonstrated by the group of Ershler (18, 24) and by our group [25, 26]. Klement et al. [27] found that atherosclerosis in old Apo E -/- mice can also reduce neovascularization in tumors. We have recently found incidentally another possible mechanism, namely passage from tetraploidy in B16 melanoma of young mice to diploidy in tumors of old animals [28].
We suggest that the diminished aggressiveness of tumors often observed in the aged, and the elucidation of the mechanisms underlying this interesting phenomenon, might suggest new therapeutic modalities more appropriate for the old organism. We postulated that it may be possible to design age-adjusted treatment modalities based on the mechanism(s) responsible for the reduced tumor progression rate in the aged.
2. Materials and Methods
2.1 Mice and Tumors
Studies on animal models were performed according to the guidelines of the Tel- Aviv University. C57BL/6J and AKR/J mice were purchased from the Tel-Aviv University Breeding Center. Two age groups were used: young mice: 6–8 weeks for both C57BL/6J and AKR/J mice; old mice: 16–24 months for C57BL/6J mice and 7–9 months for AKR/J mice. We
chose this age as ‘‘old’’ for the AKR mice, because the lifespan of this strain of mice is short, and in order to avoid the use of mice with spontaneous tumors which begin to appear at around 6 months [29]. Mice were examined (by palpation of inguinal lymph nodes) for presence of spontaneous tumors and those which developed such tumors were not included in the experiments. Tumor cell suspensions of both AKR lymphoma and B16 melanoma were prepared as previously described [30]. Tumor cells suspended in 0.2ml RPMI-1640 medium (Sigma–Aldrich, Rehovot, Israel) were inoculated subcutaneously (s.c.) in the back of mice. For AKR lymphoma, the inoculum of 1x104 cells was chosen in order to obtain the maximum differential biological behavior of the tumor between young and old mice. In the case of B16 melanoma the inoculum of 2.2 × 105 cells was chosen so that there were (usually) no survivors in the non-treated groups but there were survivors in the treated mice groups. Tumor growth was evaluated by recording the incidence and by measuring 2–3 times a week the diameter of the tumors formed at the s.c. site of inoculation. Mice mortality was recorded daily. Long-term survival was followed for 100 days at least.
2.2 Histological Examination
2.2.1 H&E Staining The resected primary tumors were fixed in formalin,
embedded in paraffin and 4 mm-thick sections were stained by ordinary H&E.
2.2.2 Giemsa Staining Tumors were excised and tumor cell suspensions
were prepared, spread on slides, fixed with methanol and stained with May–Grunwald–Giemsa.
2.2.3 ApopTag Staining Apoptosis was identified by labeling the DNA
30-OH nick-ends using a variant of TUNEL staining. ApopTag staining was carried out according to the manufacturer’s instructions using the materials provided in the kit (ApopTag, Intergen Company, New York). After deparaffinization in xylene and
The Aged Organism as a Model of Successful Copping with Tumor Progression – Implications for Therapy
22
rehydration in a series of decreasing concentrations of alcohol, the 5 mm thick tissue sections were incubated at 37℃ for 1 h in the presence of terminal deoxynucleotidyl transferase (TdT) and digoxigenin- labelled nucleotides. After washing, anti-digoxigenin- peroxidase was added to the slides which were incubated in a humidified chamber for 30 min at room temperature. After washing in PBS, the slides were stained with diaminobenzidine (Sigma–Aldrich, Rehovot, Israel) and then counterstained with 1% methylgreen (Vector, Burlingame, CA). The percentage of apoptotic bodies was determined at high power fields. A total of 300 cells were counted.
2.2.4 Factor VIII Immunostaining Slides with sections (4 mm thick) of the
paraffin-embedded tumours were prepared, deparaffinized by three washes in xylene, and rehydrated through a graded ethanol series (100%, 90% and 70%). Endogenous peroxide was blocked with 3% H2O2 for 20 min. Factor VIII was detected by a rabbit polyclonal antibody, prediluted read-to-use solution (ImmuStain, CA, USA) after predigestion with trypsin (Zymed Laboratories Inc., CA, USA) and by a standard streptavidin–biotin horseradish peroxidase complex detection method (Histostain-Plus Bulk Kit) with 3,3-diaminobenzidine (DAB) as a chromogen (Zymed Laboratories Inc., CA, USA). Faint nuclear counter- staining was achieved with Meyer’s hematoxylin solution and coverslipped with permanent mounting media.
2.2.5 Assessment of Host Response: Macrophage Content in Tumors
Host response to tumors was assessed in situ following H&E staining in sections of B16 melanoma and AKR lymphoma local primary tumors and their environment.
2.3 Ladder Type DNA Degradation
The purification of genomic DNA was done with Puregene DNA Isolation Kit (Gentra, Minneapolis, Minnesota). DNA from AKR lymphoma, grown in
young or old mice, was analyzed by horizontal electrophoresis during 2 h on 2% agarose gel (Talron, Rehovot, Israel) and visualized by UV fluorescence after staining with ethidium bromide (0.5 μg/ml) (GibcoBRL, Rockville, MA). As DNA marker, pUC18 DNA marker HaeIII digest, 102–587 b.p. (Sigma-Aldrich), was used in this study.
2.4 Anti-tumoral Treatments
2.4.1 Treatment of Young and Old Tumor-Bearing Mice by Apoptosis-Inducing Agents
Treatment was performed with single doses of 500 mg of HC. Single doses were administered 24 h following tumor inoculation.
Each experimental group consisted of 5 mice and each experiment was repeated with Hydrocortisone, 5 times for B16 melanoma and 4 times with AKR lymphoma.
2.4.2 Treatment of Young and Old Tumor-Bearing Mice with the Anti-angiogenic Agent TNP-470
Treatment with TNP-470 was performed by injecting 400 mg per mouse intratumorally 3 times a week, beginning 24 h after tumor inoculation and continued for the duration of the experiment. Each experimental group consisted in 5 mice and each experiment was repeated 4 and 3 times with the B16 melanoma and AKR lymphoma, respectively. The authors wish to thank Takeda Pharmaceutical Company, Ltd. (Osaka, Japan) for the generous gift of TNP-470.
2.4.3 Treatment of Young and Old Tumor-Bearing Mice by Immunomodulating Agents
Treatment with BCG was performed with single doses of 25 mg per mouse 24 h following tumor inoculation. Each experimental group consisted of 5 mice and each experiment was repeated 3 times for B16 melanoma and AKR lymphoma.
2.4.4 Statistical Evaluation Statistical evaluation was performed by Student’s
t-test.
3. Results
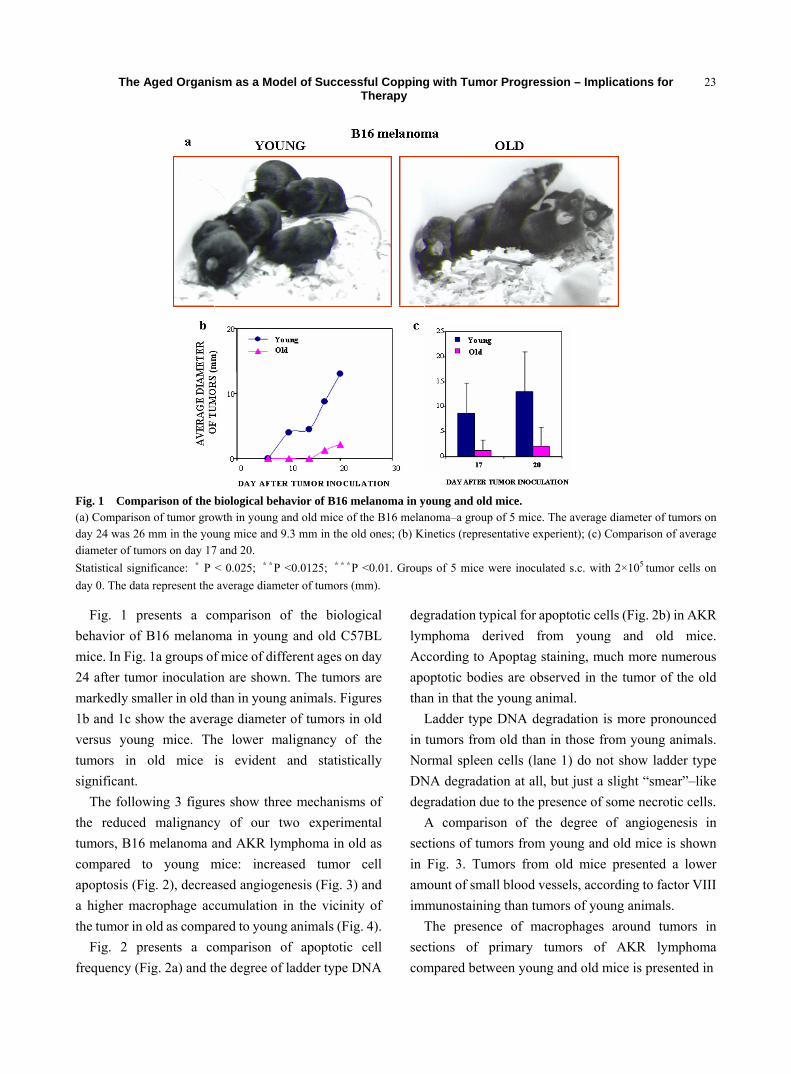
The Aged Organism as a Model of Successful Copping with Tumor Progression – Implications for Therapy
23
Fig. 1 Comparison of the biological behavior of B16 melanoma in young and old mice. (a) Comparison of tumor growth in young and old mice of the B16 melanoma–a group of 5 mice. The average diameter of tumors on day 24 was 26 mm in the young mice and 9.3 mm in the old ones; (b) Kinetics (representative experient); (c) Comparison of average diameter of tumors on day 17 and 20. Statistical significance: * P < 0.025; **P <0.0125; ***P <0.01. Groups of 5 mice were inoculated s.c. with 2×105 tumor cells on day 0. The data represent the average diameter of tumors (mm).
Fig. 1 presents a comparison of the biological behavior of B16 melanoma in young and old C57BL mice. In Fig. 1a groups of mice of different ages on day 24 after tumor inoculation are shown. The tumors are markedly smaller in old than in young animals. Figures 1b and 1c show the average diameter of tumors in old versus young mice. The lower malignancy of the tumors in old mice is evident and statistically significant.
The following 3 figures show three mechanisms of the reduced malignancy of our two experimental tumors, B16 melanoma and AKR lymphoma in old as compared to young mice: increased tumor cell apoptosis (Fig. 2), decreased angiogenesis (Fig. 3) and a higher macrophage accumulation in the vicinity of the tumor in old as compared to young animals (Fig. 4).
Fig. 2 presents a comparison of apoptotic cell frequency (Fig. 2a) and the degree of ladder type DNA
degradation typical for apoptotic cells (Fig. 2b) in AKR lymphoma derived from young and old mice. According to Apoptag staining, much more numerous apoptotic bodies are observed in the tumor of the old than in that the young animal.
Ladder type DNA degradation is more pronounced in tumors from old than in those from young animals. Normal spleen cells (lane 1) do not show ladder type DNA degradation at all, but just a slight “smear”–like degradation due to the presence of some necrotic cells.
A comparison of the degree of angiogenesis in sections of tumors from young and old mice is shown in Fig. 3. Tumors from old mice presented a lower amount of small blood vessels, according to factor VIII immunostaining than tumors of young animals.
The presence of macrophages around tumors in sections of primary tumors of AKR lymphoma compared between young and old mice is presented in
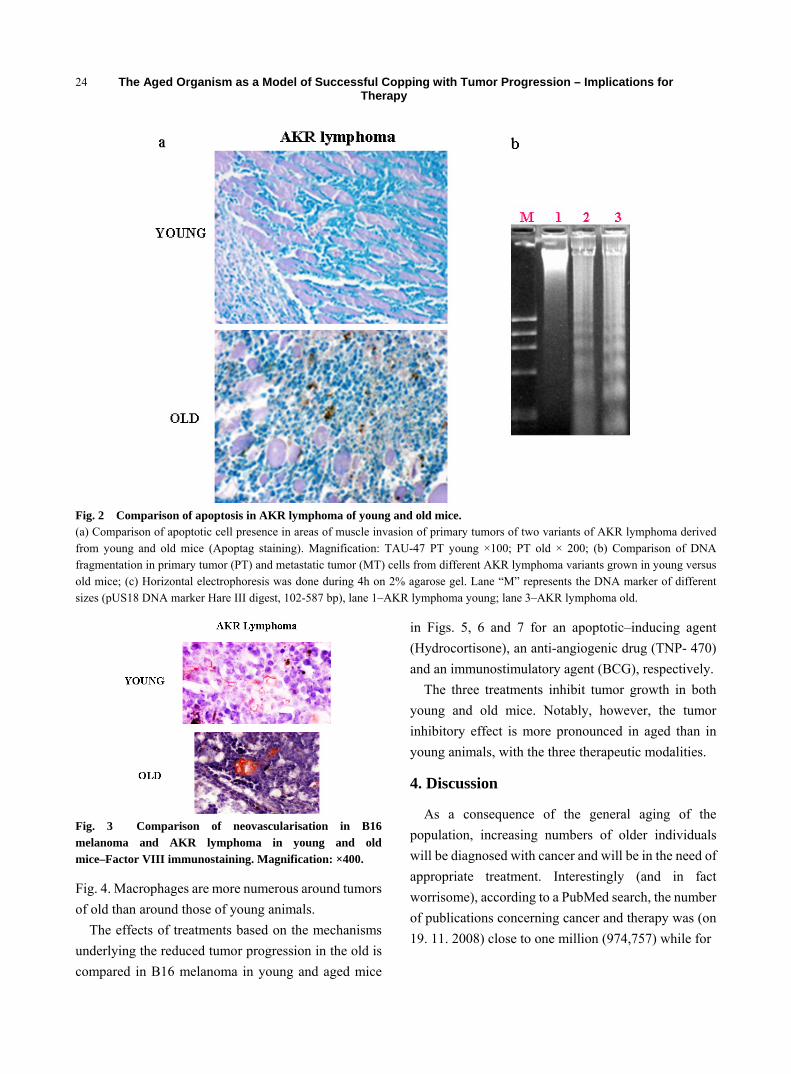
The Aged Organism as a Model of Successful Copping with Tumor Progression – Implications for Therapy
24
Fig. 2 Comparison of apoptosis in AKR lymphoma of young and old mice. (a) Comparison of apoptotic cell presence in areas of muscle invasion of primary tumors of two variants of AKR lymphoma derived from young and old mice (Apoptag staining). Magnification: TAU-47 PT young ×100; PT old × 200; (b) Comparison of DNA fragmentation in primary tumor (PT) and metastatic tumor (MT) cells from different AKR lymphoma variants grown in young versus old mice; (c) Horizontal electrophoresis was done during 4h on 2% agarose gel. Lane “M” represents the DNA marker of different sizes (pUS18 DNA marker Hare III digest, 102-587 bp), lane 1–AKR lymphoma young; lane 3–AKR lymphoma old.
Fig. 3 Comparison of neovascularisation in B16 melanoma and AKR lymphoma in young and old mice–Factor VIII immunostaining. Magnification: ×400.
Fig. 4. Macrophages are more numerous around tumors of old than around those of young animals.
The effects of treatments based on the mechanisms underlying the reduced tumor progression in the old is compared in B16 melanoma in young and aged mice
in Figs. 5, 6 and 7 for an apoptotic–inducing agent (Hydrocortisone), an anti-angiogenic drug (TNP- 470) and an immunostimulatory agent (BCG), respectively.
The three treatments inhibit tumor growth in both young and old mice. Notably, however, the tumor inhibitory effect is more pronounced in aged than in young animals, with the three therapeutic modalities.
4. Discussion
As a consequence of the general aging of the population, increasing numbers of older individuals will be diagnosed with cancer and will be in the need of appropriate treatment. Interestingly (and in fact worrisome), according to a PubMed search, the number of publications concerning cancer and therapy was (on 19. 11. 2008) close to one million (974,757) while for
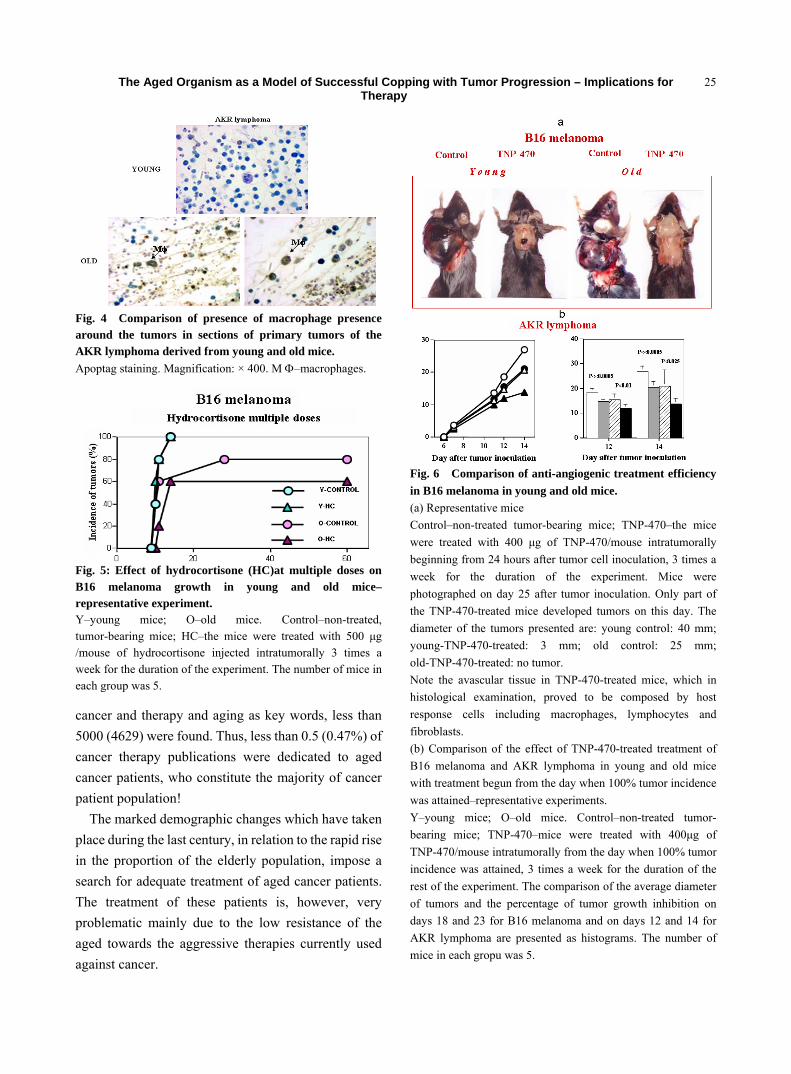
The Aged Organism as a Model of Successful Copping with Tumor Progression – Implications for Therapy
25
Fig. 4 Comparison of presence of macrophage presence around the tumors in sections of primary tumors of the AKR lymphoma derived from young and old mice. Apoptag staining. Magnification: × 400. M Φ–macrophages.
Fig. 5: Effect of hydrocortisone (HC)at multiple doses on B16 melanoma growth in young and old mice– representative experiment. Y–young mice; O–old mice. Control–non-treated, tumor-bearing mice; HC–the mice were treated with 500 μg /mouse of hydrocortisone injected intratumorally 3 times a week for the duration of the experiment. The number of mice in each group was 5.
cancer and therapy and aging as key words, less than 5000 (4629) were found. Thus, less than 0.5 (0.47%) of cancer therapy publications were dedicated to aged cancer patients, who constitute the majority of cancer patient population!
The marked demographic changes which have taken place during the last century, in relation to the rapid rise in the proportion of the elderly population, impose a search for adequate treatment of aged cancer patients. The treatment of these patients is, however, very problematic mainly due to the low resistance of the aged towards the aggressive therapies currently used against cancer.
Fig. 6 Comparison of anti-angiogenic treatment efficiency in B16 melanoma in young and old mice. (a) Representative mice Control–non-treated tumor-bearing mice; TNP-470–the mice were treated with 400 μg of TNP-470/mouse intratumorally beginning from 24 hours after tumor cell inoculation, 3 times a week for the duration of the experiment. Mice were photographed on day 25 after tumor inoculation. Only part of the TNP-470-treated mice developed tumors on this day. The diameter of the tumors presented are: young control: 40 mm; young-TNP-470-treated: 3 mm; old control: 25 mm; old-TNP-470-treated: no tumor. Note the avascular tissue in TNP-470-treated mice, which in histological examination, proved to be composed by host response cells including macrophages, lymphocytes and fibroblasts. (b) Comparison of the effect of TNP-470-treated treatment of B16 melanoma and AKR lymphoma in young and old mice with treatment begun from the day when 100% tumor incidence was attained–representative experiments. Y–young mice; O–old mice. Control–non-treated tumor- bearing mice; TNP-470–mice were treated with 400μg of TNP-470/mouse intratumorally from the day when 100% tumor incidence was attained, 3 times a week for the duration of the rest of the experiment. The comparison of the average diameter of tumors and the percentage of tumor growth inhibition on days 18 and 23 for B16 melanoma and on days 12 and 14 for AKR lymphoma are presented as histograms. The number of mice in each gropu was 5.
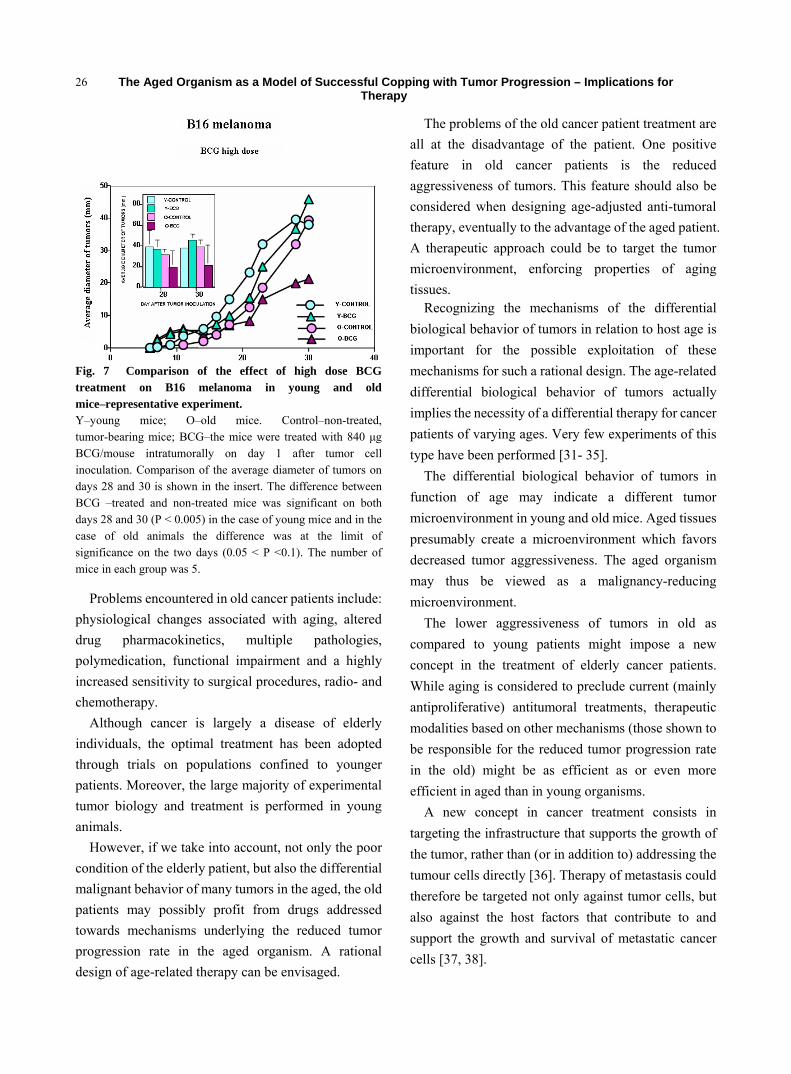
The Aged Organism as a Model of Successful Copping with Tumor Progression – Implications for Therapy
26
Fig. 7 Comparison of the effect of high dose BCG treatment on B16 melanoma in young and old mice–representative experiment. Y–young mice; O–old mice. Control–non-treated, tumor-bearing mice; BCG–the mice were treated with 840 μg BCG/mouse intratumorally on day 1 after tumor cell inoculation. Comparison of the average diameter of tumors on days 28 and 30 is shown in the insert. The difference between BCG –treated and non-treated mice was significant on both days 28 and 30 (P < 0.005) in the case of young mice and in the case of old animals the difference was at the limit of significance on the two days (0.05 < P <0.1). The number of mice in each group was 5.
Problems encountered in old cancer patients include: physiological changes associated with aging, altered drug pharmacokinetics, multiple pathologies, polymedication, functional impairment and a highly increased sensitivity to surgical procedures, radio- and chemotherapy.
Although cancer is largely a disease of elderly individuals, the optimal treatment has been adopted through trials on populations confined to younger patients. Moreover, the large majority of experimental tumor biology and treatment is performed in young animals.
However, if we take into account, not only the poor condition of the elderly patient, but also the differential malignant behavior of many tumors in the aged, the old patients may possibly profit from drugs addressed towards mechanisms underlying the reduced tumor progression rate in the aged organism. A rational design of age-related therapy can be envisaged.
The problems of the old cancer patient treatment are all at the disadvantage of the patient. One positive feature in old cancer patients is the reduced aggressiveness of tumors. This feature should also be considered when designing age-adjusted anti-tumoral therapy, eventually to the advantage of the aged patient. A therapeutic approach could be to target the tumor microenvironment, enforcing properties of aging tissues.
Recognizing the mechanisms of the differential biological behavior of tumors in relation to host age is important for the possible exploitation of these mechanisms for such a rational design. The age-related differential biological behavior of tumors actually implies the necessity of a differential therapy for cancer patients of varying ages. Very few experiments of this type have been performed [31- 35].
The differential biological behavior of tumors in function of age may indicate a different tumor microenvironment in young and old mice. Aged tissues presumably create a microenvironment which favors decreased tumor aggressiveness. The aged organism may thus be viewed as a malignancy-reducing microenvironment.
The lower aggressiveness of tumors in old as compared to young patients might impose a new concept in the treatment of elderly cancer patients. While aging is considered to preclude current (mainly antiproliferative) antitumoral treatments, therapeutic modalities based on other mechanisms (those shown to be responsible for the reduced tumor progression rate in the old) might be as efficient as or even more efficient in aged than in young organisms.
A new concept in cancer treatment consists in targeting the infrastructure that supports the growth of the tumor, rather than (or in addition to) addressing the tumour cells directly [36]. Therapy of metastasis could therefore be targeted not only against tumor cells, but also against the host factors that contribute to and support the growth and survival of metastatic cancer cells [37, 38].
The Aged Organism as a Model of Successful Copping with Tumor Progression – Implications for Therapy
27
The mechanisms of the age-dependent differential behavior of tumors point to elements in the microenvironment which favor the reduced aggressiveness of tumors in the old. An age-adjusted therapeutic approach could consist in designing modifications of microenvironmental elements with the aim of inducing a lower malignancy of tumors. It may be possible to enforce properties of aging tissues (such as, for instance, tendency to apoptosis) in the microenvironment of tumors.
We have shown that three treatment modalities, based on mechanisms underlying the reduced tumor progression in aged organisms (drugs inducing apoptotic cell death, anti-angiogenic agents and immunomodulators) display an age-related differential effect on two experimental tumors. We have demonstrated that these three treatment modalities which induce elements of an “aging microen- vironment” exert an inhibitory effect on tumors of young and old mice. Notably, the inhibition is generally more pronounced in old than in young mice.
Considering the problems encountered in the treatment of elderly cancer patients, finding treatment modalities which might be as efficient or even more efficient against tumors of aged patients may be of importance. Moreover, designing aging microen- vironmental conditions in tumors of young patients might possibly alleviate neoplastic aggressiveness in these patients as well.
In addition to our published results in two tumor models, B16 melanoma and AKR lymphoma, with 5 different treatments [21, 26, 39] and summarized here, very few studies which compared the effectiveness of anticancer treatment in relation to age were performed.
Because most cancer patients are old, it is important to try to find suitable treatment modalities particularly for this population. These studies lead us, moreover, to the possibility of envisaging treatment of young cancer patients with those agents which induce an ageing microenvironment which favoring a reduced aggressive behavior.
References [1] J. Mandelblatt, Treating breast cancer: the age old
dilemma of old age, J Clin Oncol 2006 (24) 4369-2370. [2] S. Lonardi, A. Bortolami, M. Stefani and S. Monfardini,
Oral anticancer drugs in the elderly: an overview, Drugs Ageing 2007 (24) 395-410.
[3] L. Balducci and M. Extermann, Cancer and aging: an evolving panorama, Hematol Oncol Clin North Am 2000 (14) 1-16.
[4] L. Balducci and G. H. Lyman, Cancer in the elderly: epidemiological and clinical implications, Clin Geriatr Med 1997 (13) 1-14.
[5] L. L. Siu, Clinical trials in the elderly–a concept comes of age, N. Engl J Med 2007 (356) 1575-1576.
[6] L. Balducci, Aging, frailty, and chemotherapy, Cancer Control 2007 (14) 7-12.
[7] R. A. DePinho, The age of cancer, Nature 2000 (408) 248-254.
[8] W. B. Ershler, Why tumors grow more slowly in old people, J Natl Cancer Inst 1986 (77) 837-839.
[9] W. B. Ershler, J. A. Steward, M. P. Hacker, A. L. Moore, and B. H. Tindle, B16 murine melanoma and aging: slower growth and longer survival of mice, J Natl Cancer Inst 1984 (72) 161-164.
[10] W. B. Ershler, M. A. Socinski and C. J. Green, Bronchogenic cancer, metastasis, and aging, J Am Geriatr Soc 1983 (31) 673-676.
[11] C. J. Fisher, M. K. Egan, P. Smith, K. Wicks, R. R. Millis and I. S. Fentinan, Histopathology of breast cancer in relation to age, Br J Cancer 1997 (75) 593-596.
[12] C. T. Calabrese, Y. G. Adam and H. Volk, Geriatric colon cancer, Am J Surgery 1973 (1250 181-184.
[13] T. Tsuda, Y. T. Kim, G. W. Siskind, A. De Blasio, R. Schwab, W. B. Ershler and M. E. Weksler, Role of the thymus and T cells in slow growth of B16 melanoma in old mice, Cancer Res 1987 (47) 3097-3100.
[14] R. Peto, F. J. Roe, P. N. Lee, N. Levy and J. Clack, Cancer and aging in mice and men, Br J Cancer 1975 (32) 411-426.
[15] N. Donin, J. Sinai, E. Staroselski, T. Mahlin, I. Nordenberg and J. Leibovici, Comparison of growth rate of two B16 melanomas differing in metastatic potential in young versus middle- aged mice, Cancer Invest 1997 (15) 416-421.
[16] O. Itzhaki, E. Skutelski, T. Kaptzan, A. Siegal, M. Michowitz, J. Sinai, M. Huszar, S. Nafar and J. Leibovici, Macrophage–recognized molecules of apoptotic cells are expressed at higher levels in AKR lymphoma of aged as compared to young mice, Adv Exp Med Biol 2000 (479) 251-262.
The Aged Organism as a Model of Successful Copping with Tumor Progression – Implications for Therapy
28
[17] I. L. Cameron, Cell proliferation and renewal in aging mice, J Gerontol 1972 (27) 162-172.
[18] N. J. Holbrook and Ikeyama, Age-related decline in cellular response to oxidative stress: links to growth factor signaling pathways with common defects, Biochem Pharmacol 2002 (64) 999-1005.
[19] G. S. Roth, Hormone action during aging: alterations and mechanisms, Mech Ageing Dev 1979 (9) 497-514.
[20] H. S. Chahal and W. M. Drake, The endocrine system and aging, J Pathol 2007 (211) 173-180.
[21] O. Itzhaki, T. Kaptzan, E. Skutelsky, J. Sinai, M. Michowitz, A. Siegal, G. Schibi, M. Huszar, L. Ben-Dor and J. Leibovici, Age-adjusted antitumoral therapy based on the demonstration of increased apoptosis as a mechanism underlying the reduced malignancy of tumors in the aged, Biochim Biophys Acta 2004 (1688) 145-159.
[22] R. A. Kreisle, B. A. Stebler and W. B. Ershler, Effect of host age on tumor associated angiogenesis in mice, J Natl Cancer Inst 1999 (82) 44-47.
[23] R. Pili, Y. Guo, J. Chang, H. Nakanishi, G. R. Martin and A. Passaniti, Altered angiogenesis underlying age- dependent changes in tumor growth, J Natl Cancer Inst 1994 (86) 1303-1314.
[24] P. R. Kaesberg and W. B. Ershler, The importance of immunesenescence in the incidence and malignant properties of cancer in hosts of advanced age, J Gerontol 1989 (44) 63-66.
[25] N. Donin, J. Sinai, M. Michowitz, J. Hiss, J. Nordenberg and J. Leibovici, Role of immune response as determinant of tumour progression in function of host age in the B16 melanoma, Mech Ageing Dev 1995 (80) 121-137.
[26] T. Kaptzan, E. Skutelsky, O. Itzhaki, J. Sinai, M. Michowitz , Y. Yossipov, G. Schiby and J. Leibovici, Age-dependent differences in the efficacy of cancer immunotherapy in C57BL and AKR mouse strains, Exp Gerontol 2004 (39) 1035-1048.
[27] H. Klement, B. St Croix, C. Milsom, L. May, Q. Guo, J. L. Yu, P. Klement and J. Rak, Atherosclerosis and vascular aging as modifiers of tumor progression, angiogenesis, and responsiveness to therapy, Am J Pathol 2007 (171) 1342-1351.
[28] O. Itzhaki, E. Skutelsky, T. Kaptzan, A. Siegal, J. Sinai, G. Schiby, M. Michowitz, M. Huszar and J. Leibovici, Decreased DNA ploidy may constitute a mechanism of the reduced malignant behavior of B16 melanoma in aged mice, Exp Gerontol 2008 (43) 164-175.
[29] E. Wainfan, M. Dizik, M. Kilkenny and J. P. O’Callaghan, Prolonged survival of female AKR mice fed diets supplemented with methionine and choline, Carcinogenesis 1990 (11) 361-363.
[30] J. Leibovici, G. Susskind-Brudner and M. Wolman, Direct antitumor effect of high-molecular-weight levan on Lewis lung carcinoma cells in mice, J Natl Cancer Inst 1980 (65) 391-396.
[31] J. M. Yuhas and R. L. Ullrich, Responsiveness of senescent mice to the antitumor properties of Corynebacterium parvum, Cancer Res 1976 (36) 161-166.
[32] T. Watanabe, Suppressive effects of Lactobacillus casei cells, a bacterial immunostimulant, on the incidence of spontaneous thymic lymphoma in AKR mice, Cancer Immunol Immunother 1996 (42) 285-290.
[33] C. Gravekamp, Cancer vaccines in old age, Exp Gerontol 2007 (42) 441-450.
[34] N. Takeichi, X. B. Li, J. Hamada and H. Kobayashi, Age-related decrease of pulmonary metastasis of rat mammary carcinoma by activated natural resistance, Cancer Immunol Immunother 1990 (31) 81-85.
[35] E. B. Katz and E. S. Boylan, Stimulatory effect of high polyunsaturated fat diet on lung metastasis from the 13762 mammary adenocarcinoma in female retired breeder rats, J Natl Cancer Inst 1987 (79) 351-358.
[36] J. B. Bartlett, K. Dredge and A. G. Dalgleish, The evolution of thalidomide and its IMiD derivatives as anticancer agents, Nat Rev Cancer 2004 (4) 314-322.
[37] I. J. Fidler, The organ microenvironment and cancer metastasis, Differentiation 2002 (700 498-505.
[38] R. R. Langley and I. J. Fidler, Tumor cell-organ microenvironment interactions in the pathogenesis of cancer metastasis, Endocr Rev 2007 (28) 297-321.
[39] T. Kaptzan, E. Skutelski, O. Itzhaki, J. Sinai, M. Huszar, A. Siegal, R. Ben-Zvi, Y. Yossipov, M. Michowitz, G. Schiby and J. Leibovici, Efficacy of anti-angiogenic treatment of tumours in old versus young mice, Mech Ageing Dev 2006 (127) 398-409.
Apr.2010, Volume7, No.4 (Serial No.65) Journal of US-China Medical Science, ISSN 1548-6648, USA
Diagnosis and Management of Intractable Hemoptysis
by Bronchoscopic Intervention
Faguang Jin, Deguang Mu, Dongling Chu, Enqing Fu, Yonghong Xie and Tonggang Liu Department of Respiratory Disease, Tangdu Hospital, Fourth Military Medical University, Xi’an City, China
Abstract: Objective: To investigate the efficacy of bronchoscopic intervention therapy in the diagnosis and management of intractable hemoptysis. Methods: 106 patients with intractable hemoptysis and in whom clinical medicine, bronchial artery embolization failed to stop the bleeding were analyzed. Results: Therapy was very effective in 58 cases (54.7%); somewhat effective in 41 cases (38.7%); and ineffective in 7 cases (6.6%). Conclusion: Bronchoscopic intervention therapy is safe, convenient and an efficacious method for hemoptysis. Key words: Diagnosis, management, intractable hemoptysis, bronchoscopic interventional therapy.
1. Introduction
Hemoptysis is a life-threatening condition. The main threat in the acute phase remains asphyxiation resulting from flooding of the airways and alveoli with blood. The underlying diagnosis of hemoptysis includes inflammation, tuberculosis, tumor, bronchiectasia, et al. The therapeutic thechniques in the management of hemoptysis are drug, bronchial artery embolization (BAE), and/or surgery. However, these methods may be ineffective for some patients. We reffered to this kind of hemoptysis as intractable hemoptysis. During December 2000 to December 2006, we treated 106 patients with intractable hemoptysis. The results of these studies are reported here.
2. Subjects and Methods
2.1 Subjects
From December 2000 to December 2006, 106 patients including 76 males and 30 females underwent bronchoscopy for intractable hemoptysis in our hospital. All of these patients underwent medical treatment, 31 patients underwent bronchial artery
Correspondence author: Faguang Jin, professor, research
fields: lung cancer, cor pulmonale and asthma. Email: [email protected]
embolization therapy. But the hemoptysis still continued. The quantity of hemoptysis ranged from 50 ml to 400 ml per day and the duration of hemoptysis was from 21 to 80 days.
2.2 Methods
All the patient confidentiality was maintained. We inserted a bronchoscope in the usual manner and confirmed hemorrhaging sites by aspiration and forceps were used to facilitate blood clot debridement if present. Once the exact bleeding location was determined, the bronchoscope was placed into the hemorrhaging bronchus. We started a cold saline solution lavage, followed by the instillation of a 1:20,000 epinephrine solution or infusion 5 to 10 ml of a 1000 U/ml thrombin solution. The bronchoscope, which was retained in place for about 5 min following infusion, was removed after confirming, by aspiration, that hemostasis occurred. All endoscopically visible abnormalities were sampled for diagnostic examination, brushed, or lavaged for adequate speciments. Bronchoscopically nonvisible but radiologically suspected abnormalities were sampled or brushed only when the subseqmental bronchus leading to the pathology was an actively bleeding subsegment.
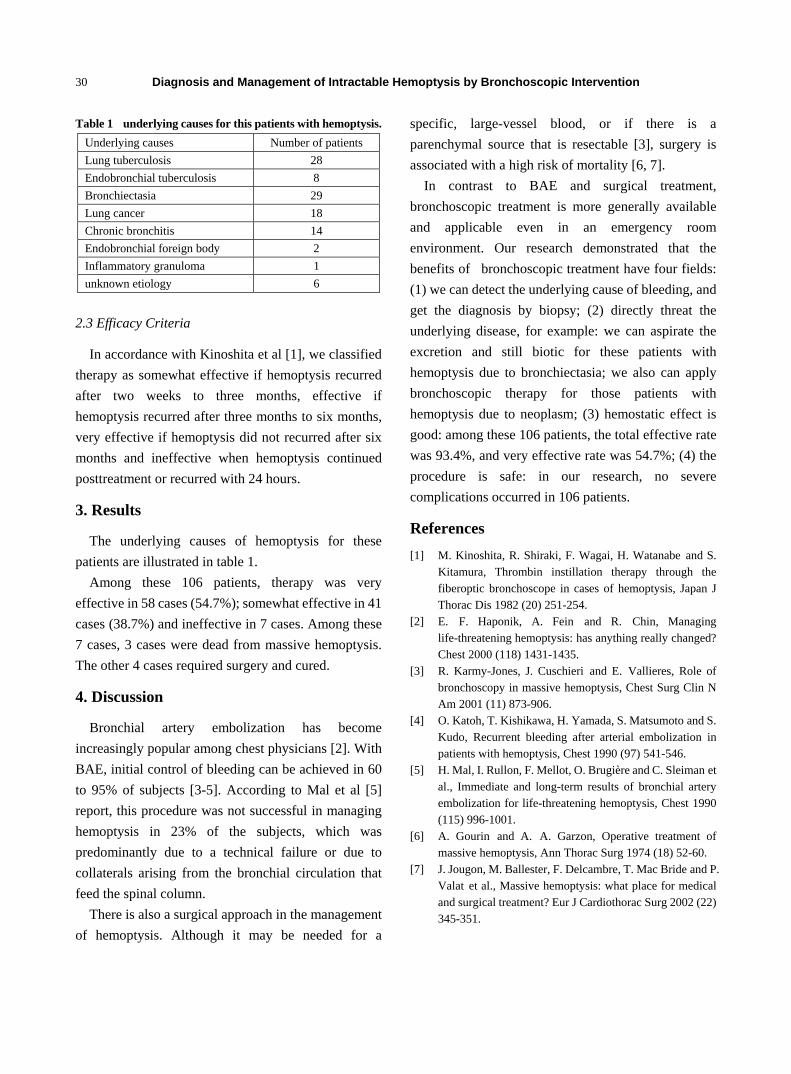
Diagnosis and Management of Intractable Hemoptysis by Bronchoscopic Intervention
30
Table 1 underlying causes for this patients with hemoptysis. Underlying causes Number of patients Lung tuberculosis 28 Endobronchial tuberculosis 8 Bronchiectasia 29 Lung cancer 18 Chronic bronchitis 14 Endobronchial foreign body 2 Inflammatory granuloma 1 unknown etiology 6
2.3 Efficacy Criteria
In accordance with Kinoshita et al [1], we classified therapy as somewhat effective if hemoptysis recurred after two weeks to three months, effective if hemoptysis recurred after three months to six months, very effective if hemoptysis did not recurred after six months and ineffective when hemoptysis continued posttreatment or recurred with 24 hours.
3. Results
The underlying causes of hemoptysis for these patients are illustrated in table 1.
Among these 106 patients, therapy was very effective in 58 cases (54.7%); somewhat effective in 41 cases (38.7%) and ineffective in 7 cases. Among these 7 cases, 3 cases were dead from massive hemoptysis. The other 4 cases required surgery and cured.
4. Discussion
Bronchial artery embolization has become increasingly popular among chest physicians [2]. With BAE, initial control of bleeding can be achieved in 60 to 95% of subjects [3-5]. According to Mal et al [5] report, this procedure was not successful in managing hemoptysis in 23% of the subjects, which was predominantly due to a technical failure or due to collaterals arising from the bronchial circulation that feed the spinal column.
There is also a surgical approach in the management of hemoptysis. Although it may be needed for a
specific, large-vessel blood, or if there is a parenchymal source that is resectable [3], surgery is associated with a high risk of mortality [6, 7].
In contrast to BAE and surgical treatment, bronchoscopic treatment is more generally available and applicable even in an emergency room environment. Our research demonstrated that the benefits of bronchoscopic treatment have four fields: (1) we can detect the underlying cause of bleeding, and get the diagnosis by biopsy; (2) directly threat the underlying disease, for example: we can aspirate the excretion and still biotic for these patients with hemoptysis due to bronchiectasia; we also can apply bronchoscopic therapy for those patients with hemoptysis due to neoplasm; (3) hemostatic effect is good: among these 106 patients, the total effective rate was 93.4%, and very effective rate was 54.7%; (4) the procedure is safe: in our research, no severe complications occurred in 106 patients.
References [1] M. Kinoshita, R. Shiraki, F. Wagai, H. Watanabe and S.
Kitamura, Thrombin instillation therapy through the fiberoptic bronchoscope in cases of hemoptysis, Japan J Thorac Dis 1982 (20) 251-254.
[2] E. F. Haponik, A. Fein and R. Chin, Managing life-threatening hemoptysis: has anything really changed? Chest 2000 (118) 1431-1435.
[3] R. Karmy-Jones, J. Cuschieri and E. Vallieres, Role of bronchoscopy in massive hemoptysis, Chest Surg Clin N Am 2001 (11) 873-906.
[4] O. Katoh, T. Kishikawa, H. Yamada, S. Matsumoto and S. Kudo, Recurrent bleeding after arterial embolization in patients with hemoptysis, Chest 1990 (97) 541-546.
[5] H. Mal, I. Rullon, F. Mellot, O. Brugière and C. Sleiman et al., Immediate and long-term results of bronchial artery embolization for life-threatening hemoptysis, Chest 1990 (115) 996-1001.
[6] A. Gourin and A. A. Garzon, Operative treatment of massive hemoptysis, Ann Thorac Surg 1974 (18) 52-60.
[7] J. Jougon, M. Ballester, F. Delcambre, T. Mac Bride and P. Valat et al., Massive hemoptysis: what place for medical and surgical treatment? Eur J Cardiothorac Surg 2002 (22) 345-351.
Apr.2010, Volume7, No.4 (Serial No.65) Journal of US-China Medical Science, ISSN 1548-6648, USA
VEGF and Angiogenesis in Renal Cell Carcinoma: A
Minireview
Ketao Jin1, Ling Zheng2, Kaiyan Fu3, Yefei Zhang2, Tieming Zhu1 and Zhigang Jin1 1. Department of General Surgery, the People’s Hospital of Zhuji, Zhuji, 311800, China;
2. Department of Pharmacy, the People’s Hospital of Zhuji, Zhuji, 311800, China;
3. Department of Emergency, the People’s Hospital of Zhuji, Zhuji, 311800, China Abstract: Across a wide range of human tumors and/or cell lines, expression of VEGF has been shown to lead to the development and maintenance of a vascular network that promotes tumor growth and metastasis. Moreover, a large and growing body of evidence indicates that both VEGF gene expression and VEGF production are associated closely with poor prognosis. This review explores the implications of VEGF activity in renal cell carcinoma (RCC). Key words: Angiogenesis, VEGF, renal cell carcinoma.
1. Introduction
Recent advances in the understanding of the pathogenesis and molecular biology of RCC have identified angiogenesis as a key factor in the development of the disease. A major component of the angiogenic process in RCC is VEGF [1]. In this review, we reviewed information on the implications of VEGF in RCC, including the unique role of VEGF and angiogenesis in RCC biology, evidence and prevalence of VEGF-expressing tumors and the potential role of VEGF as a prognostic factor.
2. Biology of Rcc
Approximately 80% of RCCs have clear-cell histology i.e. cells appear clear under a microscope [2]. In the majority of clear-cell RCCs, the VHL gene is inactivated through means such as deletion or other genetic mutation [1].
Under normoxic conditions, the pVHL closely regulates HIF-1α by causing its rapid degradation, so that HIF-1α is not normally found in the cell. As a result, HIF-1α is unavailable to bind to the
Corresponding author: Tieming Zhu, MD, research fields:
general surgery and oncology, basic and clinical.
corresponding subunit, HIF-1β, and the subsequent cascade of cellular signals does not occur [3]. In contrast, under hypoxic conditions, pVHL regulation of HIF-1α is impaired. As a result, HIF-1α is not degraded. The resulting accumulation of HIF-1α within the cell is responsible for the high degree of vascularity commonly seen in VHL-deficient tumours [4]. A critical consequence of VHL inactivation is upregulation of VEGF via a pathway involving accumulation of HIF-1α [3, 5, 6].
Recent research also indicates that VHL silencing results in defects in a process called ubiquitination, in which cellular proteins (in this case, HIF-1α) are tagged for degradation with molecules known as ubiquitins [5]. Impairments in the ubiquitination pathway lead to the accumulation of HIF-1α within the cell, even without hypoxic conditions [3]. HIF-1α is a key transcriptional factor in the molecular pathway of hypoxia and regulates the expression of a number of genes whose products are critical to tumor angiogenesis, proliferation, survival and metabolism. With respect to angiogenesis in RCC, one of the most important gene products downstream of HIF-1α is VEGF [1-3, 5, 6].
Ubiquitination is a cellular regulatory process in wh-

VEGF and Angiogenesis in Renal Cell Carcinoma: A Minireview
32
ich proteins called ubiquitins were added to another, larger protein-the target protein. This process acts as a signal for the target protein to undergo degradation. Under normoxic conditions and with normal VHL function, the pVHL plays a role in the ubiquitination and subsequent degradation of HIF-1α [3, 5, 7].
3. Effects of Vegf in Rcc
VEGF is a potent inducer of tumor angiogenesis [1, 8]. VEGF is expressed in many human cancers, but RCC in particular produces remarkably high levels, with tumors having a highly vascular histological appearance. The overexpression of VEGF in RCC is the direct result of inactivation of VHL gene. Data suggest that VHL inactivation occurs in the majority of clear-cell RCCs [1, 3].
Loss of pVHL expression results in constitutive expression of HIF-1α and induction of hypoxia -regulated genes, including those encoding for VEGF, PDGF-β and TGF-α [5]. These gene products have been implicated in the malignant phenotype of RCC, which is characterised by hypervascular tumors, local and distant metastases via haematogenous spread, uncontrolled growth and resistance to apoptosis [1, 3, 8, 9].
The role of VEGF in particular has been explored as a key factor in the pathogenesis of RCC. VEGF functions to increase vascular permeability, induce endothelial cell proliferation and migration and promote endothelial cell survival. Thus, VEGF serves as a potent promoter of angiogenesis [1]. Furthermore, VEGFR expression has been observed in RCC cells, suggesting that VEGF may also serve as an autocrine stimulus in RCC [10].
4. Evidence of Vegf Expression in Rcc
Angiogenesis is a major driving factor in the pathogenesis of RCC. The angiogenic phenotype occurs as a result of the high incidence of VHL loss, which leads to HIF dysregulation and a subsequent increase in pro-angiogenic factors [1, 3]. Thus, it
would be expected that VEGF expression would be evident in RCC. Indeed, several investigators have confirmed this hypothesis by measuring VEGF expression either through mRNA or protein levels. VEGF expression was observed in the vast majority of RCCs and several reports noted increased VEGF expression in tumor tissue compared with normal renal tissue. A number of investigators have examined RCCs to see whether VEGF is overexpressed. Their methods include the measurement of VEGF mRNA expression, as well as the measurement of VEGF protein levels. The results of six clinical studies show that the vast majority of RCCs express VEGF, underscoring the critical role of VEGF and angiogenesis in RCC [11-16]. Together, these data demonstrate that VEGF is a key mediator of angiogenesis in RCC.
5. Prognostic Implications of Vegf in Rcc
VEGF has been significantly correlated with poor OS in RCC [8]. Jacobsen et al. examined VEGF expression in 229 tumor samples from patients who underwent nephrectomy for RCC at various disease stages. The investigators reported correlation between VEGF expression and tumor size and tumor stage. More notably, they reported significantly decreased survival for patients whose tumors expressed VEGF, as measured by tissue microarray (p=0.011) [8]. This study supports the use of VEGF as a prognostic factor in RCC.
In 74 RCC samples, Paradis et al. demonstrated that VEGF expression was significantly correlated with decreased survival [17]. Furthermore, Yildiz et al. investigated the relationship between clinical outcomes and both microvessel invasion and VEGF expression in 48 RCC tumor samples. This group demonstrated a statistically significant correlation between microves- sel invasion and death due to RCC (p<0.001). The investigators also observed that VEGF expression levels were significant negative predictors of survival in RCC (p<0.001) [9].
6. Conclusion

VEGF and Angiogenesis in Renal Cell Carcinoma: A Minireview
33
Both translational and clinical researches continue to offer a better understanding of the significance of angiogenesis and VEGF in RCC. The loss of function of VHL leads to VEGF expression and angiogenesis, a critical step in the pathobiology of RCC. Several reports have demonstrated the prevalence of VEGF expression in the vast majority of RCCs and still other reports have implicated VEGF as an important prognostic factor. Further research is necessary to better define the relationship between prognosis and VEGF and angiogenesis in RCC.
References [1] B. I. Rini and E. J. Small, Biology and clinical
development of vascular endothelial growth factor- targeted therapy in renal cell carcinoma, J Clin Oncol 2005 (5) 1028-1043.
[2] American Cancer Society, What is Kidney Cancer? Available online at: http://www.cancer.org/docroot/CRI/ content/CRI_2_2_1X_What_is_kidney_cancer_22.asp?
[3] V. H. Haase, The VHL/HIF oxygen-sensing pathway and its relevance to kidney disease, Kidney Int 2006 (8) 1302-1307.
[4] H. T. Cohen and F. J. McGovern, Renal-cell carcinoma, N Engl J Med 2005 (23) 2477-2490.
[5] D. J. George and W. G. Jr. Kaelin, The von Hippel-Lindau protein, vascula r endothelial growth factor, and kidney cancer, N Engl J Med 2003(5) 419-421.
[6] O. Iliopoulos, A. P. Levy and C. Jiang et al., Negative regulation of hypoxia-inducible genes by the von Hippel-Lindau protein, Proc Natl Acad Sci USA 1996 (20) 10595-10599.
[7] L. E. Huang, J. Gu and M. Schau et al., Regulation of hypoxia-inducible factor 1alpha is mediated by an O2-dependent degradation domain via the ubiquitin- proteasome pathway, Proc Natl Acad Sci USA 1998 (14) 7987-7992.
[8] J. Jacobson, K. Grankvist and T. Rasmuson et al., Expression of vascular endothelial growth factor protein in human renal cell carcinoma, BJU Int 2004 (3) 297-302.
[9] E.Yildiz, G. Gokce and H. Kilicarslan et al. Prognostic value of the expression of Ki-67, CD44 and vascular endothelial growth factor, and microvessel invasion, in renal cell carcinoma, BJU Int 2004 (7) 1087-1093.
[10] N. Tsuchiya, K. Sato and T. Akao et al., Quantitative analysis of gene expressions of vascular endothelial growth factor-related factors and their receptors in renal cell carcinoma, Tohoku J Exp Med 2001 (2) 101-113.
[11] B. Hemmerlein, A. Kugler and R. Ozisik et al., Vascular endothelial growth factor expression, angiogenesis, and necrosis in renal cell carcinomas, Virchows Arch 2001 (5) 645-652.
[12] J. S. Lee, H. S. Kim and J. J. Jung et al., Expression of vascular endothelial growth factor in renal cell carcinoma and the relation to angiogenesis and p53 protein expression, J Surg Oncol 2001 (1) 55-60.
[13] X. Na, G. Wu and C. K. Ryan et al., Overproduction of vascular endothelial growth factor related to von Hippel-Lindau tumor suppressor gene mutations and hypoxia-inducible factor-1 alpha expression in renal cell carcinomas, J Urol 2003 (2 Pt 1) 588-592.
[14] D. Nicol, S. I. Hii and M. Walsh et al., Vascular endothelial growth factor expression is increased in renal cell carcinoma, J Urol 1997 (4) 1482-1486.
[15] A. Takahashi, H. Sasaki and S. J. Kim et al., Markedly increased amounts of messenger RNAs for vascular endothelial growth factor and placenta growth factor in renal cell carcinoma associated with angiogenesis, Cancer Res 1994 (15) 4233-4237.
[16] M. Tomisawa, T. Tokunaga and Y. Oshika et al., Expression pattern of vascular endothelial growth factor isoform is closely correlated with tumour stage and vascularisation in renal cell carcinoma, Eur J Cancer 1999 (1) 133-137.
[17] V. Paradis, N. B. Lagha and L. Zeimoura et al., Expression of vascular endothelial growth factor in renal cell carcinomas, Virchows Arch 2000 (4) 351-356.
Apr.2010, Volume7, No.4 (Serial No.65) Journal of US-China Medical Science, ISSN 1548-6648, USA
The Influence of Hyperoxygenated Solution for High Altitude Hemorrhagic Shock Rabbits' Resuscitational
Effects and Plasma Endothelin and Nitric Oxide Release
Qiquan Zhou1, 2, Dongxue Zhi3, Liju Gao3 and Bo Zhou4
1. Department of High Altitude Disease, College of High Altitude Medicine, Third Military Medical University, Chongqing 400038,
China
2. Key laboratory of High Altitude Medicine, Third Military Medical University, Ministry of Education and Key Llaboratory of High
Altitude Physiology and Mountain Sickness Research of PLA, Chongqing 400038, China
3. Department of Clinical Laboratory, First Hospital of Chinese PLA, Lanzhou 730000, China
4. Department of Clinical Laboratory, 25th Hospital of Chinese PLA, Jiuquan 735000, Gansu, China
Abstract: Objective: In order to seek further simple, convenient and effective prevantive and treated measure as well as first-aid method on hemorrhagic shock in high altitude; Methods: The oxygenated hypertonic hypercolloid solution for high altitude hemorrhagic shock rabbits' resuscitation at kunlun mountain pass transport oil pump station of altitude 4700 m in high altitude field was observed; Results: This oxygenated hypertonic hypercolloid solution can rise the blood pressure and intraventricular pressure, picked up going up speed of intraventricular pressure in isovolumetric contraction phase and going down speed of intraventricular pressure in isovolumetric relaxation phase on rabbits with hemorrhagic shock in high altitude, raise survival time and survival rate of shock animal, improve obvious pulmonary and kidney function of shock animal, no any adverse reaction,its effect superiorer obvious than the effect of isomotic solution plus vitamin C and naloxone, the experiment was still further demonstrated that the oxygenated hypertonic hypercolloid solution infused can reduce obvious the plasma the level of endothelin (ET), raise the plasma the level of nitric oxide(NO), maintenance the equilibrium of ET and NO ratio of intrakidney, the results showed that oxygenated solution infusion can influence the vascular endotheliocytes and other cells on resease of ET and No; Conclusion: The resuscitation effect of oxygenated hypertonic hypercolloid solution on rabbits with hemorrhagic shock in high altitude field was better than other antishock solution. Key Words: Endothelin, nitric oxide, high altitude, hemorrhagic shock, oxygenated hypertonic hypercolloid solution, resuscitation.
1. Introduction
A high altitude hemorrhagic shock is serious symptoms in high altitude area, not only critical but also high mortolity, because of be influenced by high altitude areas natural enviroment that shock status in this human critical the blood volume inadequate with hipoxemia when it not promptly correct at once be bound to make further aggravate the hipoxemia, make shock guickly worsevery difficult treat and cure. So
Corresponding author: Qiquan Zhou, MD., professor,
research field: highland acute. E-mail: [email protected].
that to search for simple acute administration successfully cure way, whereas to be come high altitude hemorrhagic shock prevention and treatment to study on key. The results of experiments showed that hypertonic hypercolloid solution for hypoxia on condition that rabbits hemorrhagic shock get have more good resuscitation effect ableto grosly blood pressure to increase survival time and survivalrate of animals, in subsidence histic damage degree of pulmonary and renal with reactivity of endocrine [1-3]. Buthypertonic hypercolloid solution to resuscitation not able tocorrect put right hypoxemia of shock animals, so that hypertonic hypercollid solution there is

The Influence of Hyperoxygenated Solution for High Altitude Hemorrhagic Shock Rabbits' Resuscitational Effects and Plasma Endothelin and Nitric Oxide Release
35
localized. If take oxygen carrying solution to acute mountain sickness prevention most probably for heart muscle to protect act as [4-5], there upon oxygenated hypertonic hypercollid solution to resuscitation rabbits' hypoxemic shock have carried out high altitude on the spot experimental abservation to get saticfactory result has approached on anticipated purpose.
2. Material and Method
2.1. Address
Kulun mountain outlet pump station, elevention 4700m; atmospheric pressure 58. 41kPa;atmospheric oxygen partial pressure 11.32 kPa;outdoor temper- ature(T) -2℃; laboratory room T12~20℃.
2.2 Animals
Standard grey rabbits 70, male, weight 1.5~2.0 kg, from Lanzhou organism’s products research institute experimental animals center, transported to labratory spot by car in three days.
2.3 Instrument
NSA-Ⅱphysiologic signal processing system, multichannel physiologic recorder, light quantum hemotherapier, blood gas analyser, freezer, routine operatiing-appliances, tablewith fixed rabbit, cardiac catheter, medical oxygen, centrifuge, ultrasonic cells grinder, two-passage gamma counter.
2.4 Oxygenate Soultion Preparation
Take 7.5% hyperosmotic natriumchloride solution and 6% molecule dextran40 aa 125ml mixturein bottle, befor experimental 30min perfuse blood cure instrumentin quarts glass, thereafter put in ultraviolet rays 10min, thenoxygenate, oxygen outflow 5 L/min, oxygenate 5 min, in quarts glassjar post-mixing pour into normal salines' bottle spare, hermetic work in all.The solution of postoxygenate than solution of unoxygenate for oxygen content raising 3.7~7.4 double, averageraising 5.36 double.
2.5. Experimental Way and Procedure
Take healthy grey rabbits 40, was divided into five groups (normal saline treatment group, NS group; no-treated group, NT group; oxygenated solution treatment group ,OS group; vitamine C treatment group,VC group; naloxane treatment group,NX group) in under general anesthesia (3% sodium pentobarbital 30 mg/kg i.v) according to weiger's methodsmade artificial reproduced bleeding shock made artificial postbleeding 60 min, the first group animals give oxygenated hypertonic hypercolloid solution (oxygenated solution) treatment, blood pressure stabilize observating 4 hours; the second group: give animals with vitamine C 1000 mg mixture proper dosage normal saline solution drop i.v; the third group:give animals with naloxane 0.8 mg mixture NS solution drop i.v; the fourth group: giving animals with NS solution treatment, four groups' solution dosage equal8 ml/kg drop i.v. the fifth group: control animals not givemedical solution cure to animals natural die(no-treated group);the five groups' animals in proshock or postshock and postcure 30, 60, 120, 240 min from femoral atery to drew blood assayplasma endothelin (ET) and nitric oxide(NO) and thromboxaneb2 (TXB2) and 6-ketone-prostaglandin F1a (6-keto-PGF1a) content.Observatingto four hours later would all animals put to death imenediatly dissected on the ice board took down heart, lungs, kidneystissues to homogenize lymph later assay above-mentioned eachindex. And fetch of heart, lungs, liver, kidneys to do tissue-chemistry with ultrastructural be observed.
A laboratory data by Mean ± SEM. to indication, F examine prominent of with do between groups variation.
3. Results
2.1 The Influence of Animals Survival Times and Survivals Rate

The Influence of Hyperoxygenated Solution for High Altitude Hemorrhagic Shock Rabbits' Resuscitational Effects and Plasma Endothelin and Nitric Oxide Release
36
The five groups shock animals compare of survival times and survival rate by oxygenated hypertonic hyper colloid solution management groups animals survival times longest post management four hours survival times 100 percent; vitamine C management group and naloxone management group next, post management four hours survival rate separately 63 percent and 67 percent; after fourhours NS management group only survival rate 50 percent; nottransfusion control group of shock animal to pass two hours alldeath.
2.2 The Influence for Mean Artery Pressure (MAP) and Ventricle Pressure (See Table 1)
The five groups animals' blood pressure of changes that have nothing in common with each other, each groups animals have been treated the blood pressure rise again, but oxygenated hypertonic hypercolloid solution management group of blood pressure riseagain notablest, passed since transfusion their blood pressure continued rise and the animals' life continued four hours. Next vitamine C group, naloxone group of animals' blood pressure lowest but not continuced assume wave; NS group be situated between in vitamine C group and naloxone; not transfusion control group of blood pressure have not rise.
For five groups of animals' peak ventricle pressure(PVP) inshock of before or after compare notable rise, in ventricle pressure of maximun rise speed (±dp/dt-max) increase, cardiaccontract time(T-dp-min) shorten, in diastole ventricle pressure most fallen speed(-dp/dt-max) retard. After give solution different by heart function difference degree take a turn for the better, but oxygenated hypertonic hypercolloid solution management group in ventricle pressure of largest speed raising and again continuous in higher level, yet ventricle diastole it pressure drop increase fast, vitamine C group and naloxone group twohours there after ventricle pressure suddenly drop, in ventricle pressure drop speed patency slow down.
2.3 The Influence of Lungs and Kidneys Function
The five groups shock animals' compare to see oxygenated hypertonic hypercolloid solution group of lungs assume pink, not bleeding and edema, the section not froth state fluid also notrespiratory distress symptoms, by infusion oxygenated solution that urine capacity to notable increase, each animal of urineaverage 100 ml/h; vitamine C group animal's lungs lobe enlargement assume light red color, the lungs section to see a few froth fluid, there are respirotory stress, thereafter management by urine capacity to increase, but effected as not oxygenated solution treated group for average urine capacity 15ml/h;Analoxone group animal's the lungs lobe notable enlargement surface of the lungs present blood stasis of scattered, in the present lungs' section that frothy fluid more than, there spiratory distress symptoms’ patency for urine measure average 5ml/h; A not management control group and control group of lung slobes average pantent enlargement and the lungs surface hemorrhagic at large piece and the lungs' section there is fluidexudated after cure firstend not have urine, their kidneys function not pantent improvement.
2.4 The Influence for Endothelin and Nitric Oxide to Release (See Table 2, Table 3)
2.5 The Influence for Thromboxaneb2 (TXB2) and 6-Keto-PGF1a (See Table 4)
3. Discussion
The high altitude hemorrhagic shock is different in the plain hemorrhagic shock, the patients' condition serious as well as highmortality but cure difficulty, their have all serious inhypovolemia and hypoxemia. In the past research [5-6] all only proceed from replacement blood volume, therefore resuscitated effect not very ideal. Thises research not only attented replacement blood volume at the same times attented improveorganism anoximia. We experimented on observated state clearly, this method have true special effect, not only rises bloodpressure quickly but also
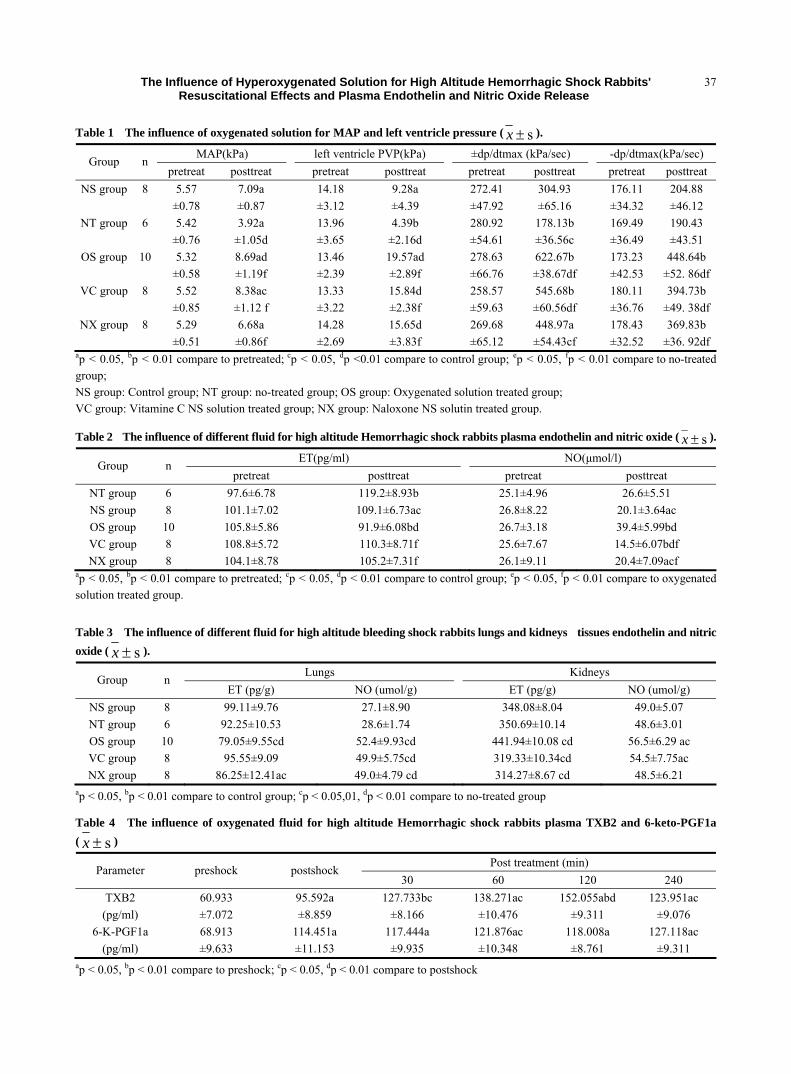
The Influence of Hyperoxygenated Solution for High Altitude Hemorrhagic Shock Rabbits' Resuscitational Effects and Plasma Endothelin and Nitric Oxide Release
37
Table 1 The influence of oxygenated solution for MAP and left ventricle pressure ( s±x ).
MAP(kPa) left ventricle PVP(kPa) ±dp/dtmax (kPa/sec) -dp/dtmax(kPa/sec) Group n pretreat posttreat pretreat posttreat pretreat posttreat pretreat posttreat
NS group 8 5.57 7.09a 14.18 9.28a 272.41 304.93 176.11 204.88 ±0.78 ±0.87 ±3.12 ±4.39 ±47.92 ±65.16 ±34.32 ±46.12
NT group 6 5.42 3.92a 13.96 4.39b 280.92 178.13b 169.49 190.43 ±0.76 ±1.05d ±3.65 ±2.16d ±54.61 ±36.56c ±36.49 ±43.51
OS group 10 5.32 8.69ad 13.46 19.57ad 278.63 622.67b 173.23 448.64b ±0.58 ±1.19f ±2.39 ±2.89f ±66.76 ±38.67df ±42.53 ±52. 86df
VC group 8 5.52 8.38ac 13.33 15.84d 258.57 545.68b 180.11 394.73b ±0.85 ±1.12 f ±3.22 ±2.38f ±59.63 ±60.56df ±36.76 ±49. 38df
NX group 8 5.29 6.68a 14.28 15.65d 269.68 448.97a 178.43 369.83b ±0.51 ±0.86f ±2.69 ±3.83f ±65.12 ±54.43cf ±32.52 ±36. 92df
ap < 0.05, bp < 0.01 compare to pretreated; cp < 0.05, dp <0.01 compare to control group; ep < 0.05, fp < 0.01 compare to no-treated group; NS group: Control group; NT group: no-treated group; OS group: Oxygenated solution treated group; VC group: Vitamine C NS solution treated group; NX group: Naloxone NS solutin treated group.
Table 2 The influence of different fluid for high altitude Hemorrhagic shock rabbits plasma endothelin and nitric oxide ( s±x ).
ET(pg/ml) NO(μmol/l) Group n pretreat posttreat pretreat posttreat
NT group 6 97.6±6.78 119.2±8.93b 25.1±4.96 26.6±5.51 NS group 8 101.1±7.02 109.1±6.73ac 26.8±8.22 20.1±3.64ac OS group 10 105.8±5.86 91.9±6.08bd 26.7±3.18 39.4±5.99bd VC group 8 108.8±5.72 110.3±8.71f 25.6±7.67 14.5±6.07bdf NX group 8 104.1±8.78 105.2±7.31f 26.1±9.11 20.4±7.09acf
ap < 0.05, bp < 0.01 compare to pretreated; cp < 0.05, dp < 0.01 compare to control group; ep < 0.05, fp < 0.01 compare to oxygenated solution treated group.
Table 3 The influence of different fluid for high altitude bleeding shock rabbits lungs and kidneys tissues endothelin and nitric oxide ( s±x ).
Lungs Kidneys Group n ET (pg/g) NO (umol/g) ET (pg/g) NO (umol/g)
NS group 8 99.11±9.76 27.1±8.90 348.08±8.04 49.0±5.07 NT group 6 92.25±10.53 28.6±1.74 350.69±10.14 48.6±3.01 OS group 10 79.05±9.55cd 52.4±9.93cd 441.94±10.08 cd 56.5±6.29 ac VC group 8 95.55±9.09 49.9±5.75cd 319.33±10.34cd 54.5±7.75ac NX group 8 86.25±12.41ac 49.0±4.79 cd 314.27±8.67 cd 48.5±6.21
ap < 0.05, bp < 0.01 compare to control group; cp < 0.05,01, dp < 0.01 compare to no-treated group
Table 4 The influence of oxygenated fluid for high altitude Hemorrhagic shock rabbits plasma TXB2 and 6-keto-PGF1a ( s±x )
Post treatment (min) Parameter preshock postshock 30 60 120 240
TXB2 60.933 95.592a 127.733bc 138.271ac 152.055abd 123.951ac (pg/ml) ±7.072 ±8.859 ±8.166 ±10.476 ±9.311 ±9.076
6-K-PGF1a 68.913 114.451a 117.444a 121.876ac 118.008a 127.118ac (pg/ml) ±9.633 ±11.153 ±9.935 ±10.348 ±8.761 ±9.311
ap < 0.05, bp < 0.01 compare to preshock; cp < 0.05, dp < 0.01 compare to postshock
The Influence of Hyperoxygenated Solution for High Altitude Hemorrhagic Shock Rabbits' Resuscitational Effects and Plasma Endothelin and Nitric Oxide Release
38
continued, the organ function improvepatency but not others bad reaction.Although vitamine C and naloxone for high altitude bleeding shock but also all resuscitated effect the better [7].but from effect to see thefurther not oxygenated solution evidence, that the naloxone ofcure asit make to lungs and intestin bleeding nacrosis, thereforeshould cause arise respiratory distress syndrom..
The resuscitation efffect of the oxygenated and hypertonichypercolloid solution get drop not only could quickly replacementblood volume but also improve tissues bring forth oxygen basicfrecdom and clearly to else tissues putrefactive that therebyabete tissues damage. Once upon a time proved high altitudebleeding shock for lungs and kidneys of putrefactive and prostatemetabolism correlation when taken hypertonic and hypercolloidsolution could timely cure balance disorder of thromboxane and6-keto-PGF1a [8-9], thises research result the further make knownoxygenated and hypertonic and hypercolloid solution also couldcure thromboxone and 6-keto-PGF1a of balance disorder. The endothelin is blood vessels endothelial cell to release of a tissues factor that it have action of fervent systolic vessels;it in shock now and again to release by maintence blood pressure for main organ of blood perfusion in termldiate have studied by researchers [10]. The under normal circumstance, the blood vesselsendothelial cells and endocardium of endothelial cellls by influence of bloodflow with blood vessels wall of sensible stressbut also release little volume nitric oxide by regulate tensionof blood vessels. In the endotoxemia, macraphage and other cellsto synthesis with release nitric oxide of large volume for induceblood vessels dilatation and blood pressure drop. Therefore nitric oxide of effect in the endotoxin shock induce for extensive attention [11-12], but nitric oxide of studies not so much in the bleeding shock, Yang Guiyuan et al. experiment proved after bleeding shock of blood vessels reaction drop but also nitricoxide product have much correlation [13]. This is experiment
study result, the early of high altitude bleeding shock of plasmanitric oxide not changes conspicuous but plasma endothelin haveincrease by give oxygenated hypertonic hypercolloid solution, the plasma endothelin conspicuous drop but the plasma nitric oxidecon spicuous rises but animals organs of shock cases between byheart and lungs and liver changes best conspicuous, in oxygenated and hypertonic and hypercolloid solution cure group animals' heartand lungs in tissues by nitric oxide conspicuous high controlgroup, thereby all endothelin and nitric oxide cause high altitude bleeding shock by give oxygenated solution cure thereafter couldinfluence of diffference degree nitric oxide and endothelin gethigh altitude bleeding shock animals quickly resuscitation.
References
[1] Q. Q. Zhou and D. X. Zhi, Effects of hypertonic saline infusion on endocrine function in rabbits with hemorrhagic shock under acute hypoxia, Chinese Med Sci J 1996 (1) 7-8.
[2] Q. Q. Zhou and D. X. Zhi, Protection of hypertonic saline for lungs injure with hemorrhagic shock under hypoxia, Chin Experimental Surgery J 1994 (5) 299-300.
[3] Q. Q. Zhou, D. X. Zhi and L. J. Gao, Effect of hypertonic saline on pulmonary diffusion function in hemorrhagic shock under acute hypoxia, Chinese Med Sci J 1995 (2) 123.
[4] J. Y. Yang, J. G. Li and X. P. Wang et al., Prelimonary observation on hypodermal injection of oxygen for the prevention of acute mountain sickness of people moving to altitude, Qinghai Med J 1986 (6) 10-14.
[5] Y. Y. Zhang, Protection of carring oxygen solution for myocardium, Chin Cardiovascular Disease J 1987 (1) 78-80.
[6] V. Kreimier and K. Messmer, Use of hypertonic nacl solutions in primary volume therapy, Zentralbl Chir 1992 (10) 532-539.
[7] J. Hamar, F. Scheiflinger, H. Redl, S. Bahrami, K. Zimmermann and Z. Szelényi et al., Small-volume fluid resuscitation with hypertonic saline prevents inflammation but not mortality in a rat model of hemorrhagic shock, Shock 2006 (3) 283-289.
[8] Z. Z. Xie, X. B. Gao and F. Y. Liu et al., Therapeutic effect of vitamin C on experimental high altitude hemorrhagic shock., Chinese Pathophysiology J 1998 (6) 699-702.
The Influence of Hyperoxygenated Solution for High Altitude Hemorrhagic Shock Rabbits' Resuscitational Effects and Plasma Endothelin and Nitric Oxide Release
39
[9] X. B. Mou, Y. Q. Gao and F. Y. Liu et al., Study on the relation between the change of endothelial cell endothelium derived factors in patients with high altitude pulmonary edema (HAPE) and the hypoxic pulmonary artery hypertention (HPAH), J Qinghai Med College 2004 (4) 295-297.
[10] C. H. Wang and H. Sun, A comparison of regularity of changes in endothelin and nitric oxide in the early stage of septic shock and hemorrhagic shock, Chinese Crit Care Med 2008 (8) 495-496.
[11] Y. Benhamou, J. Favre and P. Musette et al., Toll-like receptors 4 contribute to endothelial injury and
inflammation in hemorrhagic shock in mice, Crit Care Med 2009 (5) 1724-1728.
[12] C. E. Wright, D. D. Rees and S. Moneada, Protective and pathological roles of nitric oxide in endotoxin shock, Cardiovasc Res 1992 (1) 48-57.
[13] R. G. Alvarez, Z. B. Zamora and A. Borrego et al., Ozone oxidative preconditioning reduces nitrite levels in blood serum in LPS: induced endotoxic shock in mice, Inflamm Res 2009 (8) 441-443.
[14] G. Y. Yang and K. X. Zhao et al., Mechanism of vascular hyporeactivity induced by NO in hemorrhagic shock. Chinese Pathophysiology J 2000 (11) 1163-1166.
Apr.2010, Volume7, No.4 (Serial No.65) Journal of US-China Medical Science, ISSN 1548-6648, USA
Discussion about the Prognoses of Wilson's Disease
with Severe Cortex Structure Impairment—A Case
Report of Wilson’s Disease (WD) Treated by the
Traditional Chinese Medicine and Western Medicine
Songlin Chen, Yingyin Liang, Xiangxue Zhou and Xunhua Li Department of Neurology, The First Affiliated Hospital of Zhongshan University, Guangzhou, China Abstract: Introduction: As we know, Wilson's disease( WD) patient with severe structure and function impairment will have a poor prognosis. We met an exceptional case and madea report, then discussed some viewpoints about prognosis of WD patients. Case report: A WD patient presenting with severe cortex structure and cerebral function impairment was followed up for 5 years , including his therapeutic regiment–the combined treatment of traditional Chinese medicine and western medicine, clinical manifestation, the 24-hr urine copper output and brain MRI. By effective copper-excluding therapy, his clinical manifestation went on worse 1st year after diagnosis, and then was improved in the following years. The patient's symptoms almost complete recover 3 years afterward. During 5 years, the 24-hr urine copper excreted is tapered, but it was still higher than normal. The cerebral MR image of the patient was getting worse at 1st year, then began to recover, and improved markedly 5 years after. Conclusion: For WD patients, treated with the traditional Chinese medicine and western medicine, even therapy start in serious conditions and in late adolescent, clinical manifestation may get striking improvement. Key words: Wilson’s Disease (WD), treating effect, cranial MRI.
1. Introduction
WD is a rare familial inherited disorder as an autosomal recessive trait, being characterised by excessive accumulation of copper in the body, particularly the liver, brain, cornea and kidney. WD was one of those minority inherited diseases which might have good therapeutic prognoses. Early diagnosis and therapy with copper chelating agents are important to the prognoses [1]. However, the relationship between the prognoses and the condition of initial treatment, such as age, pathogenesis condition, and the course of disease, are not known thoroughly. It is regarded that if the age of initial treatment is more than 15 years old (for adolescent type WD), with or without serious cerebral structure impairment, serious
Corresponding author: Xunhua Li, professor, research
fields: neurological genetic diseases and neuromuscular diseases. E-mail: [email protected].
pathogenesis condition, the pharmacotherapy is hard to ameliorate the symptoms [2]. There is also a report that the necrosis or cystic change in the brain are irreversible [3]. Here we report a WD subject with serious intelligence impairment and cerebral cystic change, and also has dramatic prognoses.
2. Material and Methods
Following a 15 years old WD patient, who was the preliminary diagnosed in 2002. His pathogenetic condition, therapy method and clinical outcome were recorded and followed since then.
2.1 Clinical Material
A 15 years old high school student was admitted with a main complaint of difficulty on lettering and four limbs joints pain. And his learning ability descended and he change from excellent to inferior
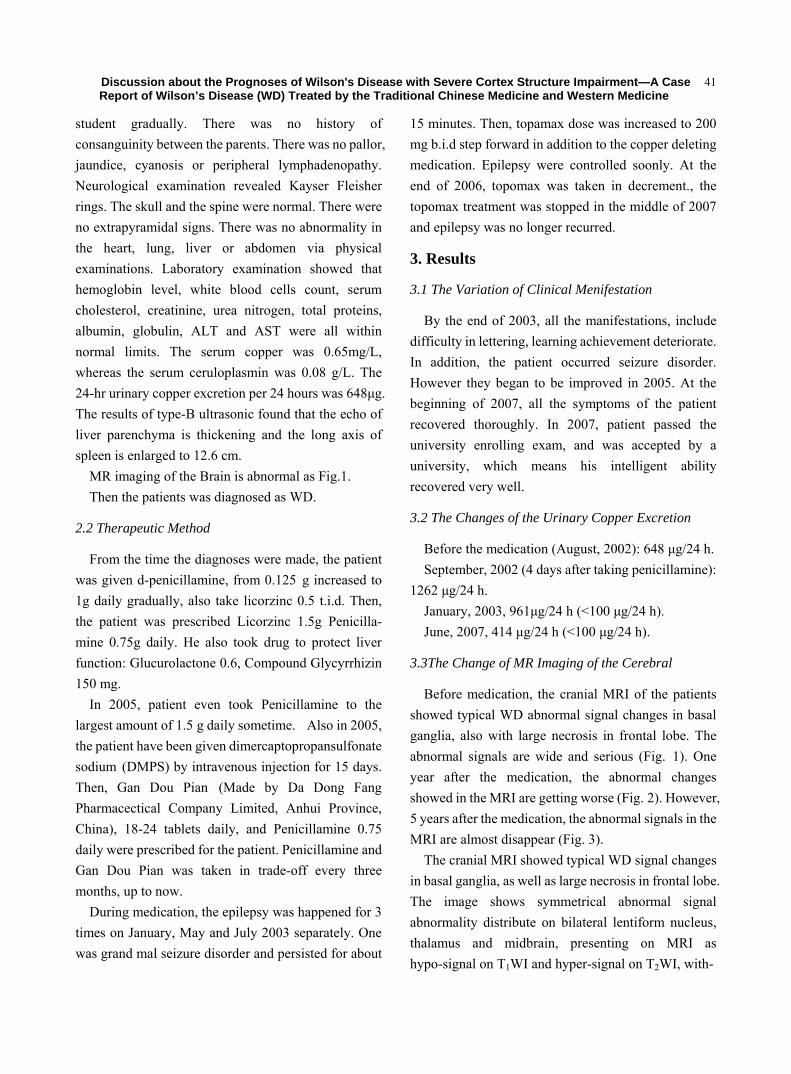
Discussion about the Prognoses of Wilson's Disease with Severe Cortex Structure Impairment—A Case Report of Wilson’s Disease (WD) Treated by the Traditional Chinese Medicine and Western Medicine
41
student gradually. There was no history of consanguinity between the parents. There was no pallor, jaundice, cyanosis or peripheral lymphadenopathy. Neurological examination revealed Kayser Fleisher rings. The skull and the spine were normal. There were no extrapyramidal signs. There was no abnormality in the heart, lung, liver or abdomen via physical examinations. Laboratory examination showed that hemoglobin level, white blood cells count, serum cholesterol, creatinine, urea nitrogen, total proteins, albumin, globulin, ALT and AST were all within normal limits. The serum copper was 0.65mg/L, whereas the serum ceruloplasmin was 0.08 g/L. The 24-hr urinary copper excretion per 24 hours was 648μg. The results of type-B ultrasonic found that the echo of liver parenchyma is thickening and the long axis of spleen is enlarged to 12.6 cm.
MR imaging of the Brain is abnormal as Fig.1. Then the patients was diagnosed as WD.
2.2 Therapeutic Method
From the time the diagnoses were made, the patient was given d-penicillamine, from 0.125 g increased to 1g daily gradually, also take licorzinc 0.5 t.i.d. Then, the patient was prescribed Licorzinc 1.5g Penicilla- mine 0.75g daily. He also took drug to protect liver function: Glucurolactone 0.6, Compound Glycyrrhizin 150 mg.
In 2005, patient even took Penicillamine to the largest amount of 1.5 g daily sometime. Also in 2005, the patient have been given dimercaptopropansulfonate sodium (DMPS) by intravenous injection for 15 days. Then, Gan Dou Pian (Made by Da Dong Fang Pharmacectical Company Limited, Anhui Province, China), 18-24 tablets daily, and Penicillamine 0.75 daily were prescribed for the patient. Penicillamine and Gan Dou Pian was taken in trade-off every three months, up to now.
During medication, the epilepsy was happened for 3 times on January, May and July 2003 separately. One was grand mal seizure disorder and persisted for about
15 minutes. Then, topamax dose was increased to 200 mg b.i.d step forward in addition to the copper deleting medication. Epilepsy were controlled soonly. At the end of 2006, topomax was taken in decrement., the topomax treatment was stopped in the middle of 2007 and epilepsy was no longer recurred.
3. Results
3.1 The Variation of Clinical Menifestation
By the end of 2003, all the manifestations, include difficulty in lettering, learning achievement deteriorate. In addition, the patient occurred seizure disorder. However they began to be improved in 2005. At the beginning of 2007, all the symptoms of the patient recovered thoroughly. In 2007, patient passed the university enrolling exam, and was accepted by a university, which means his intelligent ability recovered very well.
3.2 The Changes of the Urinary Copper Excretion
Before the medication (August, 2002): 648 μg/24 h. September, 2002 (4 days after taking penicillamine):
1262 μg/24 h. January, 2003, 961μg/24 h (<100 μg/24 h). June, 2007, 414 μg/24 h (<100 μg/24 h).
3.3The Change of MR Imaging of the Cerebral
Before medication, the cranial MRI of the patients showed typical WD abnormal signal changes in basal ganglia, also with large necrosis in frontal lobe. The abnormal signals are wide and serious (Fig. 1). One year after the medication, the abnormal changes showed in the MRI are getting worse (Fig. 2). However, 5 years after the medication, the abnormal signals in the MRI are almost disappear (Fig. 3).
The cranial MRI showed typical WD signal changes in basal ganglia, as well as large necrosis in frontal lobe. The image shows symmetrical abnormal signal abnormality distribute on bilateral lentiform nucleus, thalamus and midbrain, presenting on MRI as hypo-signal on T1WI and hyper-signal on T2WI, with-
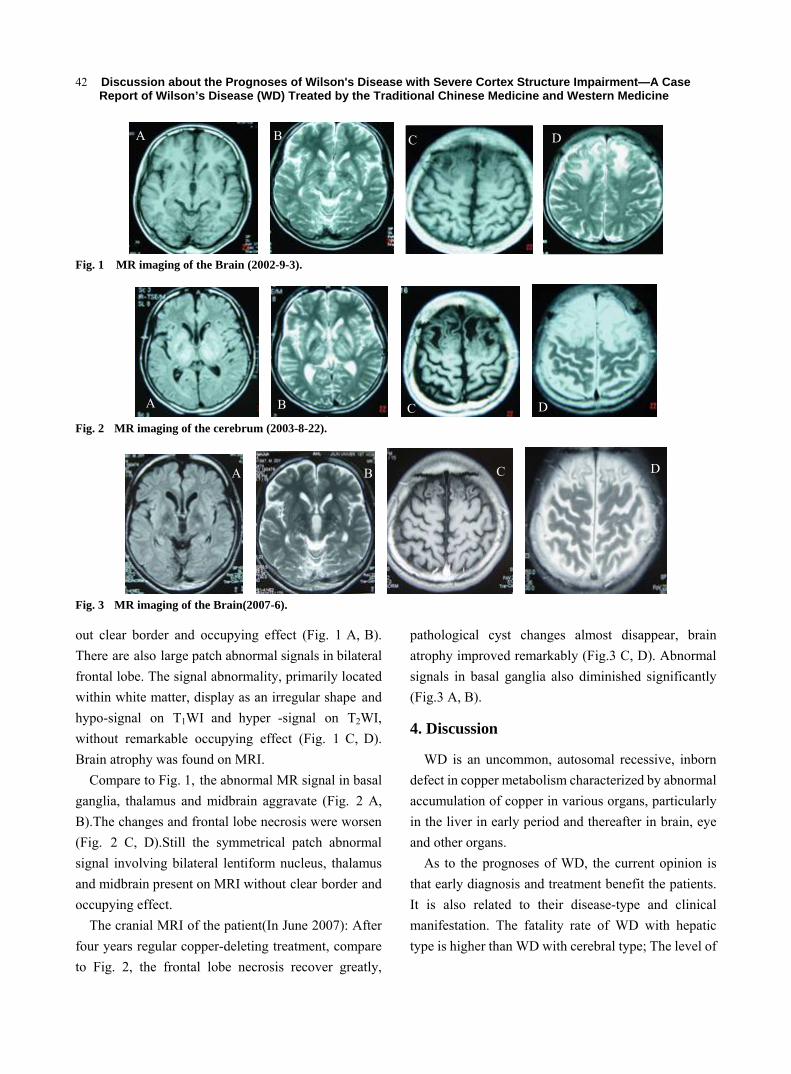
Discussion about the Prognoses of Wilson's Disease with Severe Cortex Structure Impairment—A Case Report of Wilson’s Disease (WD) Treated by the Traditional Chinese Medicine and Western Medicine
42
Fig. 1 MR imaging of the Brain (2002-9-3).
Fig. 2 MR imaging of the cerebrum (2003-8-22).
Fig. 3 MR imaging of the Brain(2007-6).
out clear border and occupying effect (Fig. 1 A, B). There are also large patch abnormal signals in bilateral frontal lobe. The signal abnormality, primarily located within white matter, display as an irregular shape and hypo-signal on T1WI and hyper -signal on T2WI, without remarkable occupying effect (Fig. 1 C, D). Brain atrophy was found on MRI.
Compare to Fig. 1, the abnormal MR signal in basal ganglia, thalamus and midbrain aggravate (Fig. 2 A, B).The changes and frontal lobe necrosis were worsen (Fig. 2 C, D).Still the symmetrical patch abnormal signal involving bilateral lentiform nucleus, thalamus and midbrain present on MRI without clear border and occupying effect.
The cranial MRI of the patient(In June 2007): After four years regular copper-deleting treatment, compare to Fig. 2, the frontal lobe necrosis recover greatly,
pathological cyst changes almost disappear, brain atrophy improved remarkably (Fig.3 C, D). Abnormal signals in basal ganglia also diminished significantly (Fig.3 A, B).
4. Discussion
WD is an uncommon, autosomal recessive, inborn defect in copper metabolism characterized by abnormal accumulation of copper in various organs, particularly in the liver in early period and thereafter in brain, eye and other organs.
As to the prognoses of WD, the current opinion is that early diagnosis and treatment benefit the patients. It is also related to their disease-type and clinical manifestation. The fatality rate of WD with hepatic type is higher than WD with cerebral type; The level of
A B C D
A B C D
A B C D
Discussion about the Prognoses of Wilson's Disease with Severe Cortex Structure Impairment—A Case Report of Wilson’s Disease (WD) Treated by the Traditional Chinese Medicine and Western Medicine
43
serum bilirubin and ascites are close related to its prognoses [4].
WD patients of cerebral type have deglutition, language dysfunction and torsion dystonia usually. Motor dysfunction leads to low quality of life and disabled life. Our patient mainly showed disturbance of intelligence, so he is WD of cerebral type. The overall cognitive function of WD is lower than healthy individuals [5]. The mentality of WD with cerebral type is lower than healthy person. By regular copper-deleting treatment, their mentality may restore to some extent [6]. However, if the patients have long pathogenesis and serious impairment on memory, their prognoses are worse. And early diagnoses and regular treatment are very helpful to the recovery of their memory [7]. However, in this case, subject began treatment with the seriously impairment on intelligence, cerebral structure, almost recover thoroughly after 4 years. The recovery reason might be the patient is adolescent and his cerebral function is elastic. By regular and consisting treatment, the deposition of copper in the brain tissue disappear, neural stem cells regenerate and restore the function. This phenomenon indicated the patients with hypophrenia might have better prognoses than those with myodystonia.
In terms of the copper excretion, when treated by penicillamine for about 6 month regular and effective medication, the urine excretion amount in most patients will reduce obviously. Our patients also have similar phenomenon. There are two reasons for the phenomenon: firstly, large amount of the body copper has been discarded. Secondly, the patient is insensitive to penicillamine. To the former, although the amount of the copper excretion of twenty-four-hour urine reduced, the symptoms are improved continuously. So we considered the reduction in the copper excretion of our patient may be the first reason.
Penicillamine has been used abroad in treating WD patients by improving the excretion of urinary copper. It has excellent therapeutic effect, although it has a few side effects and its decreasing tendency of efficacy on
excretion of urinary copper. Gan dou pian is a medicine which’s prescription is made by the theory of Chinese traditional medicine. According to the theory of Chinese traditional medicine of basing treatment on syndrome differentiation, copper toxic substance is accumulated in the body, Damp and Heat are gathered in hepato-biliary system, which is the main pathogenesis of WD, therefore the treatment of bitter herbal medicine’s purgation, antipyresis and detoxication, unobst ruct bowels, diuresis, and removing Dampness are ways suitable to treat this disease. The ingredients such as rhubarb, coptis and turmeric in Gandou pian have the functions of antipyresis, detoxication, and could relieve Fire and Heat, regulate Qi and menstruation and dry the Dampness, houttuynia and water plantain could allay the fever, remove the Dampness, and promote the metabolism of water; edoary could remove stasis and improve blood circulation, and therefore it is beneficial for treating WD-patients [8]. It has the function of continuous excretion of urinary copper without requirement on dose adjustment. Moreover it has few side-effects [9], so patients have good compliance.
Pathologic changes to the central nervous system in WD are always associated with a significant increase of tissue copper content. Despite the MR image often show the pathologic findings limited to the basal ganglia, thalamus, and brainstem. Histopathologic studies have shown abnormalities throughout central system in patients with WD. These abnormalities include atrophy, spongy softening, cavitation, ageneral reduction of neurons, increased cellularity, and the presence of Opalski cells [10].
According to literature, the neuropathologic findings of WD, the high-signal-intensity lesions on T2-weighted images can becaused by edema, gliosis, demyelinization, neuronal necrosis, or cystic degeneration [11]. It has been reported that the phagocytes containing iron pigment were commonly seen in the globus pallidus and substantia nigra in WD [12]. On the basis of the aforementioned data, the
Discussion about the Prognoses of Wilson's Disease with Severe Cortex Structure Impairment—A Case Report of Wilson’s Disease (WD) Treated by the Traditional Chinese Medicine and Western Medicine
44
central low-signal-intensity is as on T2-weighted images were explained as the result of increased iron deposition in the areas with accumulation of copper. However, our results suggest that the reversible process of copper metabolism can be a possible explanation for the reversibility of hypointensity after copper chelating therapy, as evidenced by the patients who experienced clinical improvement.
The cause of hyperintensity in T1- weighted images may result from the toxic effect of copper overload in the brain and indirectly from liver failure as a result of copper intoxication [13]. Kozicetal suggested that hyper-intensity might be reversible during the course of chronic chelating therapy [14]. Our case also showed that the three kind signal changes on MR, hyper-intensity in T1-weighted and high-intensity on T2-weighted, may be improved by effective copper chelating therapy.
5. Conclusions
WD may be a kind of disease with good prognosis. But there are multiple factors, such as the age of onset when treated, pathogenetic condition, the course of disease, act on the prognosis. Here we reported a WD case, with seriously cerebral impairment, also can get improve dramatically by therapy. We believe the prognosis of WD maybe better than the current opinions.
References [1] J. Aaseth, T. P. Flaten and O. Andersen, Hereditary iron
and copper deposition: diagnostics, pathogenesis and therapeutics. Scand J Gastroenterol 2007 (6) 673-681.
[2] Z. Jianming, X.Q. Li and G. Yu et al., Values of magnetic resonance imaging in evaluating prognoses of childhood hepatolenticular degeneration, J Clin Pediatri 2007 (25) 95-98.
[3] A. C. A. Magalhaes, P. C. Caramelli and J. R. Menezes et al., Wilson’s disease, MRI with clinical correlation, Neuroradiol, 1994 (36) 97-102.
[4] H. Li, X. H. Li and X. L. Li et al, Prognostic and the effects of therapeutic factors on Wilson’s disease, Chin Nerv Ment Dis 2006 (32) 11-15.
[5] K. Wang., R. M. Yang and R. Hoosain et al., Impairment of recognition of disgust in Chinese with Huntington’s or Wilson’s disease, Chin J Neurol 2003 (5) 527-537.
[6] C. H. Liang, R. M. Yang and S. H. Xu et al., Perspective study on intelligence quotient of 28 Hepatic Lenticular degeneration patients with treatment combining traditional Chinese and Western medicine, CJITWM, 1996 (16) 8-12.
[7] Y. Cai, Y. L. Cai and L. Xu et al., The clinical observation on the influence of combined therapy of TCM and WM on memory of patients with cerebral hepatiolenticular degeneration, JETCM 2007 (16) 527-530.
[8] Y. Z. Han, G. Y. He and X. Wang et al., Comparative study on therapeutic effects of Gandou Tablet I and Dimercaptosuccinate Acid in treating on Wilson's Disease, Chinese Journal of Integrative Medicine 1992 (2) 69-70.
[9] W. B. Hu, R. M. Yang and M. S. Ren et al., Observation of the clinical therapeutic effect of Gandou Tablet I on Hepatolenticular Degeneration, CJIM 2002 (8) 7-10.
[10] C. Harper and R. Butterworth, Nutritional deficiencies and metabolic disorders, in J. G. Greenfield, J. Hume Adams, L.W. Duchen (Eds.): Greenfield’s Neuropathology (5th ed.), London, UK: Edward Arnold, 1992, pp.838-840.
[11] C. C. Huang and N. S. Chu, Wilson disease: resolution of MRI lesions following long-term oral zinc therapy, Acta Neurol Scand 1996 (93) 215-218.
[12] A. D. King, J. M. Walshe and B. E. Kendall et al., Cranial MR imaging in Wilson disease, Am J Roentgenol 1996 (167)1579-1584.
[13] H. Mochizuki, K. Kamakura and T. Masaki et al., Typical MRI features of Wilson disease: high signal in globus pallidus on T1-weighted images, Neuroradiol 1997 (39) 171-174.
[14] D. Kozic, M. Svetel and B. Petrovic et al., MR imaging of the brain in patients with hepatic form of Wilson disease, Eur J Neurol 2003 (10) 587-592.
Apr.2010, Volume7, No.4 (Serial No.65) Journal of US-China Medical Science, ISSN 1548-6648, USA
Case Report: Treatment of Canary Pox with Orally
Administration of Acyclovir
Mansour Mayahi and Forogh Talazade
Faculty of Veterinary Medicine, Shahid Chamran University of Ahvaz, Iran Abstract: Objective: In this study, the effects of acyclovir on treatment of canary pox were examined. Two Canaries (one live & one dead) were referred to Avian Medicine Clinic. At post mortem examination, pox like lesions were observed in mouth, pharynx, larynx and upper part of trachea. In examination of the live bird, clinical signs such as depression, dyspnea, gasping were seen. Acyclovir is phosphorylated by viral thymidine kinase and inhibits viral DNA polymerase. The live bird was treated with acyclovir and was inspected every day. Methods: The live canary was treated with acyclovir at 80 mg/kg each 6hr/day orally for 10 days and was inspected every day. Results: The apetite of bird was improved gradually. After 10 days, all of clinical signs and gross lesion were disappear. Conclusions: Canary pox will be treated by acyclovir at 80 mg/kg each 6hr/day orally for 10 days. Key words: Canary, acyclovir, diphtheritic pox.
1. Introduction
Avian pox is a common viral disease of domestic and wild birds [1, 2]. Avian pox has been reported in various birds, including ostrich [3], quail [4], grackles [5], racing pigeon [6], red-tailed hawk [7], prey [8], and cherrug falcon [9], for example. Two hundred and thirty-two bird species in 23 orders from approximately 9000 bird species have been reported to have acquired a natural poxvirus infection. Avian poxviruses infect birds of both sexes and all ages. The course of the disease in the individual bird takes three to five weeks. Affected young birds are retarded in growth, laying birds experience a drop in egg production. Birds of all ages that have oral or respiratory system involvement have difficulty eating and breathing. Among companion birds, avian poxvirus infections most often occur in Amazon parrots and in large aviaries of canaries. Canaries are highly susceptible to canary poxvirus but show resistance to turkey, fowl, and pigeon poxviruses [10]. Avian pox occurs frequently in domestic poultry,
Corresponding author: Mansour Mayahi, professor,
research fields: avian diseases. Email: [email protected].
pigeons, and canaries. Avian pox is a large DNA virus. Four closely related strains have been identified: fowl pox virus (chickens), turkey pox virus, pigeon pox virus, and canary pox virus. Birds that survive avian pox infection usually have durable immunity against reinfection with the same virus [11]. It is a slow-spreading disease. Clinical signs in naturally infected birds depend on various factors including virus virulence, host susceptibility, distribution and type of lesions as well as other factors. Two forms of manifestations can be distinguished. The cutaneous form, characterised by nodular proliferative skin lesions on the nonfeathered parts of the body, and the diphteritic form, which leads to fibrino-necrotic and proliferative lesions in the mucous membrane of the pharynx, esophagus and the upper respiratory tract. A systemic form with high mortality rates is frequently seen in canaries. Cutaneous lesions may occur as papules, pustules, or crusty scabs, depending on the stage of the infection. Diphtheritic lesions are yellow, caseous plaques that are usually found in the mouth or pharynx but may be present in the esophagus, trachea, sinuses, conjunctiva, or larynx. Large cytoplasmic viral inclusions (Bollinger's bodies) are frequently
Case Report: Treatment of Canary Pox with Orally Administration of Acyclovir
46
present in infected epithelial cells [12]. Asyclovir is synthetic nucleoside analogs of deoxyguanosine, whose antiviral activities are restricted to herpes viruses. Acyclovir is monophosphorylated by viral thymidine kinase 200 times easier than by the similar mammalian enzyme, which contributes to its good selective toxicity and high therapeutic index.. Pharmacokinetic data are available for human patients. Acyclovir is available as a topical, oral, and intravenous preparation .Orally administered asyclovir at 80 mg/kg 24 hours after herpes virus infection in Quaker parakeets was shown to be more effective in preventing death than either low or high dose(40 or 250 mg/kg) intramascular injections. At the highest dose tested, asyclovir toxicity, as seen by local muscular necrosis, was thought to contribute to bird mortality. Acyclovir has been shown to decrease mortality in psittacine birds with herpesviral infections if the drug is administered prior to onset of clinical signs. [13] The purpose of this study was to evaluate the effects of acyclovir on treatment of canary pox.
2. Case Report
During June 2008, two 4-6 months old canaries (one live & one dead) were referred to Avian Medicine Clinic. The live canary had severe respiratory distress with open-mouthed gasping and rales. Excessive lacrimation and conjunctivitis were noted. In dead specimen, upon necropsy, proliferative lesions were observed at the opening to the trachea, and a thick, yellow caseous exudate adhered to the lesions. These lesions extended down the trachea for various distances but were limited to the upper quarter and the exudate had occluded the lumen to the trachea. No external proliferative lesions commonly seen with canary pox were observed in any of these specimens. The live canary was treated with acyclovir at 80
mg/kg each 6hr/day orally for 10 days and was inspected every day. The apetite of bird was improved gradually. After 10 days, all of clinical signs and gross lesion were disappear. It seems canary pox will be treated by acyclovir at 80 mg/kg each 6hr/day orally for 10 days.
References [1] P. Kirmse, Pox in wild birds: an annotated bibliography, J
Wildl Dis. 1967 (49) 1–10. [2] MGT Yoshikkawa and J. Alam, Histopathological
studiesof fowl pox in Bantams, Int J Poult Sci. 2002 (1) 197–199.
[3] D. M. Allwright, W. P. Burger, A. Geyer and J. Wessles, Avian pox in ostriches, J. S. Afr. Vet. Assoc. 1994 (65) 23–25.
[4] J. A. Crawford, Differential prevalence of avian pox in adult and immature California quail, J. Wildl. Dis. 1986 (22) 564–566.
[5] D. E. Docherty, R. I. Long, E. L. Flickinger and L. N. Locke, Isolation of poxvirus from debilitating cutaneous lesions on four immature grackles (Quiscalus sp.), Avian Dis. 1991 (35) 244–247.
[6] K. Dodd, Pox in racing pigeons, Vet. Rec. 1974 (95) 41–43.
[7] G. L. Griffiths and D. A. Purcell, Fowl pox in the trachea of point of lay hens, Aust. Vet. J., 1986 (63)91–92.
[8] J. H. Samour and J. E. Cooper, Avian pox in birds of prey (order Falconiformes) in Bahrain, Vet. Rec. 1993 (132) 343–345.
[9] J. H. Thiele and H. D. Adolphs, Avian pox virus: an ultrastructural study on a cherrug falcon, Brief report. Arch. Virol. 1979 (62) 77–82.
[10] D. N. Tripathy and W. M. Reed, Pox, in: Y. M. Saif (Eds), Diseases of Poultry (11th ed.), Iowa State University Press, Ames, IA, 2007, pp. 253–269.
[11] C. H. Cunningham, Avian pox, in: M. S. Hofstad, B. W. Calnek, C. F. Helmboldt, W. M. Reid and H. W. Jr. Yoder (Eds), Diseases of Poultry (7th ed.), Iowa State University Press, Ames, Iowa., 1978, pp. 597-609.
[12] C. E. Whiteman and A. A. Bickford, Avian Disease Manual, Colorado State University, 1979, pp. 17-19.
[13] H. Richard Adams, Veterinary Pharmacology and Therapeutics (8th ed.), 2001, p. 936.
Apr.2010, Volume7, No.4 (Serial No.65) Journal of US-China Medical Science, ISSN 1548-6648, USA
A Deformity Fetus Delivered by a Hepatitis B Woman
Treated with Lamivudine during Pregnancy
Qing He, Liansan Zhao, Qiyuan Tang and Zhou Zhou Third Hospital of Shenzhen, Buxin Road 2019, Shenzhen 518020, China
Abstract: A female HBV patient who had been treated with lamivudine for 71 weeks was stopped taking lamivudine after she was found 10 weeks pregnant. At the 23th week of gestation ultrasonic examination showed facial malformation of the fetus and induced labor was performed. Other factors that might have caused the deformity have been ruled out. Therefore, it is assumed that the fetal deformity may result from the patient’ s prior long-term treatment with lamivudine. Key words: Lamivudine, deformity, pregnancy.
1. Introduction
Mrs. Sun, female, 26 years-old, suffered from HBV (hepatitis B virus) infection for 10 years, with liver function abnormal for 5 years. Further consultation on July 25th, 2005 clewed her serological profile of positive hepatitis B surface antigen (HBsAg), e antigen (HBeAg), c antigen (HBcAg) and the presence of HBV-DNA 3.55 × 105 copies/ml (PCR), ALT 80U/L (ELISA) in serum. Therefore she was prescribed lamivudine 0.1g/day for anti-HBV therapy. After the doze of 11 months, her liver function returned to normal and HBeAg turned negative, HBV-DNA < 5.0 × 102 copies/ml. She was prescribed lamivudine continuously until Jan 1st, 2007, while she was found to be 10 weeks pregnant, as her first gestation. By then, the patient had already used lamivudine for more than 71 weeks. At once, her lamivudine therapy was terminated and further observation was requested.
At the 23rd week of gestation, the patient came back for Ultrasonic examination. It showed intrauterine pregnancy in the form of single living fetus with severe facial malformation consisting of right eye abnormal
* The publication of the information relevant to the privacy of the patient has been approved by the patient concerned.
Corresponding author: Liansan Zhao, M.D., research field: viral Hepatitis and infectious diseases. Email:[email protected].
smallness, nose abnormality, and widened side ventricle.
Fetus cell chromosome test of amniocentesis was performed. The result showed: G-banding Pattern, 46, XY, not obviously abnormal for the fetus cell chromosome. Meanwhile, TORCH tests for the pregnant woman showed the results were negative. She denied the use of any other drugs during pregnancy and one month before the pregnancy. Moreover, exposure to other toxic materials or radiation in the living environment of the patient and her husband during the last 3 years and their family histories of heredity diseases were denied by both of them. Lastly the couple were not married in proximity of blood.
With complete awareness of all the situation and consent by the pregnant patient and her husband, the patient was given rivanol injection inside amniotic cavity for induction of labor on the day of Mar 23rd, 2007 (at the 24th week of gestation). Then delivered was a dead male fetus with severe face abnormality (see fig. 1, 2). Before and 3 weeks after the operation, the liver function tests of the patient showed normal results, and HBV-DNA detections were below 5.0 × 102copies/ml.
2. Discussion
This case is a young woman with chronic hepatitis

A Deformity Fetus Delivered by a Hepatitis B Woman Treated with Lamivudine During Pregnancy
48
Fig. 1 frontal view of the deformed fetus.
Fig. 2 lateral view of the deformed fetus.
B, who had used lamivudine for 71 weeks until her 10th week of gestation was confirmed. At her 23rd week of gestation, an living fetus with severe face deformity was delivered. There is neither other suspicious teratogenesis drug, nor TORCH tests positive evidence for the patient. Also, there is neither recent exposure to other toxic materials or radiation in her living environment, nor histories of family heredity diseases for this woman and her husband. Even marriage in proximity of blood was ruled out. Furthermore, the amniocentesis indicated that XY chromosome test with the fetus showing no abnormal result.
Since there are various factors leading to abnormality, the cause for birth defect is difficult to recognize sometimes. After comprehensive analysis of the disease course of this patient, the relation between severe face deformity of the fetus and the use of lamivudine can not be eliminated.
Since the alarming report of the world-wide fetal abnormality in the 1960s when thalidomide was found to be the cause of deformed limbs, extensive research on the teratogenesis effect of drugs was carried on [1]
Thalidomide as a sedative drug used for prevention of nausea during early pregnancy. It was not realized that Thalidomide molecules could cross the placental wall affecting the foetus until it was too late. Analysis indicates that the fetus injury or abnormality induced by causer drugs usually occurs during the first trimester of gestation, especially in the first 8 weeks, which is the most active differentiation period for germ cell, when the rudiment of different tissues and organs is growing up. During this most important period if the pregnant woman used some drugs with teratogenesis effect, cells of some tissues and organs of the embryo would cease to grow or lead to body deformity and abnormality.
According to the definition used for pregnancy risk categories as defined by the US Food and Drug Administration, the fatalness to fetus was divided into 5 levels (A, B, C, D, X). Category A: Controlled studies in women fail to demonstrate a risk to the fetus in the first trimester. Category B: Either animal reproduction studies have not demonstrated a fetal risk. Category C: Either studies in animals have revealed adverse effects on the fetus (teratogenic or embryocidal or other) and there are no controlled studies in women or studies in women and animals are not available [2]. As the reproduction studies in pregnant rats and rabbits showed that lamivudine was transferred to the fetus through the placenta, and evidence of early embryo lethality was seen in the rabbit at exposure levels similar to those observed in humans [3], so lamivudine belongs to Level C which is not safe for pregnant women. Actually, Long-term in utero adverse effects of infants exposed perinatally to lamivudine are still unknown [4].
So far, there has been no agreement on the need of the termination of pregnancy for female patients treated with lamivudine therapy. Anyway, our case report is intended to remind clinic staff that the consideration of lamivudine safety for fetal development and growth should be placed on the first-line issue.
A Deformity Fetus Delivered by a Hepatitis B Woman Treated with Lamivudine During Pregnancy
49
In case of a pregnancy in a patient infected with hepatitis B virus there is a risk of intrauterine fetus infection, which rises significantly with the presence of HBV DNA in serum [5]. There are a few case reports concerning the prescription of lamivudine for intervention of HBV vertical transmission from the mother to her fetus [6]. These scholars argued that lamivudine could be used to reduce the load of HBV in blood, which might be helpful to lower the risk of HBV maternal-fetal vertical transmission. The evidence of this point is that lamivudine has already become the routine treatment for interrupting the HIV maternal-fetal vertical transmission [7]. However, there are great differences in both situations between HIV and HBV infection. The infection of HIV will almost affect the infant forever and need lifetime dose of drugs to control the viral level of HIV. Once the nightmare of AIDS comes true for anyone infected with HIV, nearly all of them will end up in death soon. Whether for the individuals concerned or public health safety, the risk of HIV infection caused by vertical transmission is more serious than the risk of teratogenesis effect with lamivudine. Balancing the advantages and disadvantages of using lamivudine for prevention from HIV maternal-fetal vertical transmission, the risk of fetus abnormality caused by lamivudine seems to be subordinate. In other words, Lamivudine should be used during pregnancy only if the potential benefits outweigh the risks.
However, HBV infection is a quite different story. Hepatitis B is remediable with much better curative effect than AIDS. The possible risk of fetus abnormality with the use of lamivudine is obviously unendurable for preventing HBV maternal-fetal vertical transmission only.
References [1] C. Brooks and et al., Linear growth of children with limb
deformities following exposure to thalidomide in utero, Acta Paediatr Scan 1977(66) 673-675.
[2] Available online at: http://www.fda.gov/fdac/features/ 2001/ 301_ preg.html#categories.
[3] Available online at: http://www.fda.gov/cder/foi/nda/ 98/21003_Epivir-HBV_prntlbl.pdf.
[4] A. Poblano, L. Figueroa, D. R. Figueroa and L. Schnaas, Effects of prenatal exposure to Zidovudine and Lamivudine on brainstem auditory evoked potentials in infants from HIV-infected women, Proc West Pharmacol Soc. 2004 (47) 46-49.
[5] L. S. Zhao, To elininated hepatitis B virus verical transmission: the resolved and unresolved, World Chinese Journal of Digestology 2007 (15) 1677-1681.
[6] H. Fota-Markowska, Modrzewska R., Borowicz I., Kiciak S., Pregnancy during lamivudine therapy in chronic hepatitis B–case report, Ann Univ Mariae Curie Sklodowska [Med] 2004 (2) 1-3.PMID: 16146039 [PubMed - indexed for MEDLINE].
[7] F. Dabis, L. Bequet, D. K. Ekouevi, I. Viho, F. Rouet, A. Horo, C. Sakarovitch, R. Becquet, P. Fassinou, L. Dequae-Merchadou, C. Welffens-Ekra, C. Rouzioux and V. Leroy, Field efficacy of zidovudine, lamivudine and single-dose nevirapine to prevent peripartum HIV transmission, AIDS. 2005 (3) 309-318.
Apr.2010, Volume7, No.4 (Serial No.65) Journal of US-China Medical Science, ISSN 1548-6648, USA
Hyperglycemia and Lactic Acidosis after Ingestion of a Lethal Dose of Slow-Release Nidedipine––Case Report
Cristina Bologa1, Adorata Coman2, Catalina Lionte1, Ovidiu Petris3 and Laurentiu Sorodoc1 1. “Sf Ioan” Emergency Hospital, Departament of Internal Medicine, “Gr. T Popa” University of Medicine and Pharmacy, Iasi,
Romania
2. “Sf. Spiridon” Ambulatory Unit, Departament of Preventive Medicine, “Gr. T Popa” University of Medicine and Pharmacy, Iasi,
Romania
3.“Sf Ioan” Emergency Hospital, Departament of Nursing, “Gr. T Popa” University of Medicine and Pharmacy, Iasi, Romania
Abstract: We present the case of a 23-year-old woman patient hospitalized 8 hours after ingesting of 300 tablets of 10 mg slow-release nifedipine (3000 mg) in a suicide attempt, showing–collapse, hyperglycemia, lactic acidosis. In evolution, anuria and acute pulmonary edema emerged. Under supported treatment of the vital functions, fluid resuscitation associated with amine pressors, administration of large doses of calcium gluconate and euglycemic insulin therapy, the evolution is in the end favorable. Key words: Calcium-channel blocker, nifedipine overdose, hyperglycemia, lactic acidosis.
1. Introduction
The acute intoxications with high doses of calcium-channel blockers are often lethal, especially if slow-release preparations are involved. The toxic effects of the calcium-channel blockers are represented by cardio-vascular effects–arterial hypotension, brady- arrhythmias and by metabolic effects–hyperglycemia, lactic acidosis.
Calcium-channel blockers agents are medicines that were first used in the 1970s for treating arterial hypertension, cardiac arrhythmias, angina pectoris, migraines etc. [1] If in the period 1980 –1990, the acute intoxications with calcium-channel blockers were rarely used in practice, after 2000 it was noticed both an increase of their occurrence and in the mortality rate generated by them, especially if slow-release preparations are involved. [1, 2]
The acute intoxications with cardiovascular drugs are among the first five causes of mortality in toxicology. The first position is held by analgesics, followed by
Corresponding author: Cristina Bologa, professor. Email: [email protected].
sedatives and antipsychotics then follows antide- pressants, next are drugs and on the fifth position are cardiovascular agents. [1]
Three main categories of calcium-channel blockers are described depending on their chemical composition: phenylalkylamines (the most representative is the verapamil), dihydropyridine (nifedipine and others), benzathiazepines (the most representative being diltiazem). [1] As toxic effects, the calcium-channel blockers of the phenylalkylamine group cause arterial hypotension associated with intracardiac conduction disorders, the dihydropyridine group causes severe arterial hypotension accompanied by reflex tachycardia and only rarely conduction disorders, and those belonging to benzathiazepine group mainly determine intracardiac conduction disorders and rarely arterial hypotension. [1-3]
2. Case Presentation
A 23-year-old woman patient without a previously known pathological history was brought by ambulance to the emergency admission unit of our hospital at about 8 hours after she had ingested 300 tablets of 10

Hyperglycemia and Lactic Acidosis after Ingestion of a Lethal Dose of Slow-Release Nidedipine––Case Report
51
mg slow-release nifedipine (3000 mg) in a suicide attempt after an argument in the family.
At admission, she presented: pallor of the skin, cold and cyanotic extremities, low perceptive peripheral pulse, systolic arterial pressure–60 mm Hg, tachycardia 128 /minute, drowsiness. The readings of other examinations devices were within normal limits. The electrocardiogram showed a sinus tachycardia of 128 /minutes. A blood sample was taken for laboratory analysis and first measures were taken to sustain the vital functions–fluid resuscitation as well as administration of the first antidote dose (40 ml of 10% calcium gluconate).
The patient was admitted in the intensive care unit where the fluid resuscitation went on, as well as the administration of 6000 ml crystalloid solution associated with amine pressors (dopamine 15-18 μg/kg/min and then noradrenaline 30 μg/min) during the first 24 hours. Antidote administration was continued untill a total dose of 12 g of calcium gluconate during the first 24 hours.
The biological tests carried out at her admission showed: hyperglycemia (445 mg/dl), metabolic acidosis (pH-7.16, paCO2-56, paO2-96), hyperlactaci- demia (9.5 mg/dl), hyperleucocytosis (18 800 /mmc), the remaining analyses were within normal limits.
During the first 24 hours of her admission, the systolic arterial pressure did not exceed 70 mmHg, resulting in anuria setting. In this instance, it was started the administration of 20U actrapid insulin in bolus followed by continuous infusion at a rate of 0.7 UI/kg/h. We checked the serum capillary glucose level every one hour. After 48 hours of starting the euglycemic insulin therapy, the patient became normoglycemic, hemodynamically stable and starts the diuresis.
We mention the emergence in the second hospitalization day of the phenomena of acute respiratory distress that imposed orotracheal intubation and mechanical ventilation, maintained for the next 4 days. The clinical evolution was favorable and the
patient was discharged in the 6th day after addmision.
3. Discussion
The acute intoxications with calcium-channel blockers administrated in large doses are lethal in most of the cases, as the literature in the field also indicates, especially if calcium-channel blockers of phenylchilamine group or slow-release preparations are involved. The toxic effects of calcium channel blockers are represented, on one hand, by the cardiovascular effects–arterial hypotension, brady- arrhiyhmias, and on the other hand by the metabolic effects–hyperglycemia, lactic acidosis. [1-4].
The toxicity of calcium-channel blockers is determined by blocking the L-type calcium channels at the level of myocardium, vascular smooth muscle cells and of pancreatic beta cells. Our patient had arterial hypotension associated with hyperglycemia, lactic acidosis and acute respiratory distress by non-cardiogenic acute pulmonary edema that emerged after ingestion of a large dose of slow-release dihydropyridine (nifedipine) in a suicide attempt. [1-4]
The emergence of hyperglycemia in the acute intoxication with calcium-channel blockers is considered severe prognosis factor and is present in the severe forms of calcium-channel blockers. Hyperglycemia is considered to be produced by the decrease in insulin secretion at the beta pancreatic cellular level and induction of systemic insulin- resistance. [2-4]
The lactic acidosis is mainly a consequence of tissular hypoperfusion induced by extended arterial hypotension associated with a decrease of the insulin secretion and an increase of the calcium-channel blockers induced insulin resistance. [2-4]
The literature in the field describes a series of rare complications that can occur in acute intoxication with calcium-channel blockers: convulsions, non-cardiogen acute pulmonary edema, cerebral vascular injuries, acute myocardic infarct or intestinal infracts. Our

Hyperglycemia and Lactic Acidosis after Ingestion of a Lethal Dose of Slow-Release Nidedipine––Case Report
52
patient manifested one of these complications, namely, non-cardiogen acute pulmonary edema. In acute intoxication with calcium-channel blockers, the mechanism of producing the non-cardiogen acute pulmonary edema is not yet elucidated and it is considered to have two major causes: the selective precapillary vasodilatation and excessive fluid resuscitation in order to fight arterial hypotension. [1, 3, 4]
The treatment of the acute intoxication with calcium-channel blockers is not yet well stated giving rise to a multitude of questions over the past few years. Over time, various therapeutic schemes were suggested, but no standardized treatment algorithm was found.
The first therapeutic movement recommended by experts, as with any other intoxication, in case the patient reaches the hospital in the first two hours of ingestion is the gastric lavage and administrating activated charcoal in this way trying to limit the toxic substance absorption. [2] On our patient the gastric lavage was not carried out because of the delayed arrival at the hospital (8 hours after the ingestion) and the emergence of the cardio-vascular effects (arterial hypotension and reflex tachycardia).
As for the pharmacological treatment, the first recommended pharmacologic line is represented by intravenous calcium administration, as an antidote along with monitoring the calcemia that should be kept at a value of 2 mmol/l. [1-4] Our patient benefited from an antidote treatment from the moment she was admitted in the hospital, by intravenous administration of calcium gluconate at the same time with the fluid resuscitation. A total amount of 12 g of calcium gluconate was administrated on the first 24 hours after her admission.
The next recommended pharmacological line for patients with no improvement of their hemodynamic status by fluid resuscitation in association with calcium is represented by glucagon administration. [1, 2, 4-6] Initially, it is administrated intravenously a
dose of 3 mg glucagon, followed by repeating of dose of 7 mg and, if needed, an intravenous perfusion of 3-5 mg/hour. Precaution is recommended on patients presenting hyperglycemia, the administration of glucagon could increase even more the values of glycemia. On our patient, only 3 mg of glucagon were administrated because of the increased values of glycemia (over 400 mg/dl) that augmented even more after glucagon injection, reaching 500 mg/dl, reason why the glucagon treatment was stopped.
Another therapeutic method used by some authors for patients intoxicated with calcium-channel blockers where collapse is not recovered by fluid resuscitation and antidote administration, is the so called “hyperinsulinic englycemia” consisting of actrapid insulin in continuous perfusion in doses varying within 0.2UI-1UI/kgc/hour aiming to improve the cardiac inotropism, to improve the peripheral vascular resistance most likely by improving the taking over and use of carbohydrates by the myocytes. [1-6] We administrated on our patient 20 U actrapid insulin boluse, followed by a continuous infusion at a rate of 0.7 U/kg/h obtaining a normalization of the glycemic values as well as the improvement of hemodynamic status in about 48 hours since admission.
The case we presented has a range of clinical features. Firstly, the very large dose of ingested slow-release dihydropidine (3000 mg of 10-mg slow-release nifedipine), then the delayed admission in hospital, at about 8 hours since ingestion. Another feature is represented by the association between hyperglycemia and the lactic acidosis in collapse, being aware of the fact that the metabolic effects are rarely encountered in the acute intoxication with calcium-channel blockers compared to the cardiovascular effects. In addition to all we mentioned above, we also render the emergence of non- cardiogenic acute pulmonary edema, a complication not so often encountered in acute intoxication with dehydropiridine. The evolution of our patient was favorable by intravenous gluconic calcium admini-

Hyperglycemia and Lactic Acidosis after Ingestion of a Lethal Dose of Slow-Release Nidedipine––Case Report
53
stration and euglycemic insulinotherapy along the fluid resuscitation, pharmacologic treatment methods recommended in all calcium-channel blockers intoxications.
References [1] N. S. Harris, A 40-year old woman with hypotension after
an overdose of amlodipine: presentation of case, N Engl J Med 2006 (355) 602-611.
[2] C. R. DeWitt and J. C. Waksman, Pharmacology, pathophysiology and management of calcium channel blocker and B-blocker toxicity, Toxicol Rev 2004 (4) 223-238.
[3] S. Ghosh and M. Sircar, Calcium channel blocker overdose: experience with amlodipine, Indian J Crit Care Med 2008 (12) 190-193.
[4] V. Ojetti, A. Migneco, F. Bononi, A. De Lorenzo and N. Gentiloni Silveri, Calcium channel blockers, beta-blockers and digitalis poisoning: management in the emergency room, European Review for Medical and Pharmacological Sciences 2005 (9) 241-246.
[5] E. W. Boyer and M. Shannon, Treatment of calcium-channel-blocker intoxication with insulin infusion, N Engl J Med. 2001 (344) 1721–1722.
[6] M. D. Levine and E. W. Boyer, Hyperinsulinemia- euglycemia therapy: a useful tool in treating calcium channel blocker poisoning, Crit Care 2006 (4) 149.
Apr.2010, Volume7, No.4 (Serial No.65) Journal of US-China Medical Science, ISSN 1548-6648, USA
The Effect of Official Automation on Performance Improvement Based on Balanced Scorecard Model
(BSC)
Nour Mohammad Yaghoubi and Sadegh Khazaee Asl Management Department, University of Sistan and Baluchestan, Zahedan 9816745685, Iran
Abstract: The aim of this research is to evaluate the effect of official automation on performance improvement in the medical Sciences university of Zahedan based on the Balanced Scorecard model (BSC). The research method is descriptive and is of the survey type. The statistical population is all of the 212 managers and the staff of the medical Sciences university of Zahedan among which 130 people were selected as the sample initially through the Purposive sampling method and then by the random selection. The main goal of the research is determining the effect of official automation in the medical university of Zahedan on the performance based on the BSC model; and the subsidiary aims are stating the effect of using official automation on the improvement of internal processes, learning and growth increment, increasing the customer satisfaction and financial improvement. The research tool is the questionnaire based on the Likert scale. The reliability of the questionnaire was 0.876; and data analysis showed that the most effect of official automation has been on financial improvement and the least has been on the learning and growth increment. The final results of the study present that official automation has lead to the performance improvement of the medical Sciences university of Zahedan. Key words: Information Technology (IT), official automation, performance evaluation, balanced scorecard.
1. Introduction
Technology will have a critical role in 21st century [1], as most of the organizations will require using any kind of technology as a way of rebuilding the production competency and increasing their flexibility. Therefore, nowadays using IT is essential for every organization [2]. Rivalry increment, miniaturization maintenance, reaching the better performance level, globalization and enfranchisement are examples of the wide changes which many organizations deal with and has made them to reform and reorganize. They also must be converted from functional hierarchy to flexible, network-based and with high performance organizations. The organizations require IT as a determinant factor to overcome these challenges. They
Corresponding author: Nour Mohammad Yaghoubi, PhD,
assistant professor, research fields: public management, e-government, e-commerce, rural development and so on. Email: [email protected].
use it not only to improve the effectiveness and efficiency, but also for fast and continuous responding to the customer requirements and competitive pressures and optimal supply through the distribution channels and empowering the staff to communicate with the customers, suppliers and other stakeholders [3]. During the last semi-century, modern organi- zations have increased investing on IT, because they believe that IT has a positive effect on the organizational performance [4]. While has been a propellant for distinction the strategic and organizational plans in the …period [5] and has been converted from a supporter of the business operations to a key factor of substructure and sometimes to the business itself. In the organizations, data network has become as important as the social network and they are actually has been merged together [6]. Finally it must be noted that nowadays IT application is a common

The Effect of Official Automation on Performance Improvement Based on Balanced Scorecard model (BSC)
55
characteristic of organizations and has been proved as a vital factor in the success of many organizations [7].
2. Literature Review of the Research
Organizational performance has always affected significantly on the firms’ activities. Considering the importance of the subject, the approaches of valid evaluation of the performance is an important branch of the organizations and also scientific institutes [8]. Performance evaluation can be defined as evaluating the method of optimum organizational management and the created value for the customers and other stakeholders [9]. In this uncertain world which changes quickly, IT is a “necessity” for the survival of the organizations; and functions of the IT departments are getting more important. Hence, evaluating the performance of IT department is essential to understand its partake in the organization’s goals. Many methods and techniques have been suggested over the years to evaluate the investments made in IT and information systems. Traditional methods focus on Well-Known financial Measures, Such as the Return of Investment (ROI), net Present Value (NPV), the internal rate of return (IRR), and the Payback period [10]. But these financial scales present an imperfect and limited view of the business performance; and relying on such data will prevent creating the valuable business in the future. Therefore, we must complete the financial scales with the other factors [11]. The balanced scorecard can obviate the weakness of the traditional evaluation approach. Robert Kplan and David Norton, in 90 decade created a set of indicators and named it the Balanced Scorecard [12]. The Balanced Scorecard is a performance measurement system [13-14], a strategic management system [15] and a communicational tool [13-14]. The Balanced Scorecard presents a compound view of the total performance of the organization and the strategic goals. It merges the financial scales with other performance key factors to create a viewpoint consisted of both financial and non-financial aspects (The aspects of
customer, internal processes and learning and growth) [15-16].
The balanced scorecard describes that the staff require which systems, skills and knowledge (learning and growth Perspective) for innovation, efficiency and strategic competencies (internal processes Perspective) which offers a special value to the market (customer Perspective) and consequently will lead to higher value for the stakeholder (financial Perspective) [17]. Among the people who have suggested utilizing the balanced scorecard for IT performance evaluation, Martinsons et al. (1998) and Stewart (2007) can be mentioned. Martinsons et al. believe that financial scales like the rate of ROI, NPV and turnover period are not proper for evaluating the performance of information systems. Because these systems bring a wide range of resources for the organization, as much of them are not sensible and it will not be easy to quantize all of the value and advantage of the information system and make them ponder able with the financial scales. Therefore, they suggest the balanced scorecard as a proper approach for evaluation of performance and managing the information systems and IT [10]. Stewart in his studies searches for a structured frame for managing the life cycle of IT projects. This frame contains three phases of the life cycle of IT projects which are selecting the IT project, strategic implication of the project and evaluating the IT performance. Stewarts suggest that generally, IT investment appraisal is more difficult than other investment decisions Because IT-induced benefit are hard to identify and quantify. In an attempt to provide a balanced approach to IT performance evaluation, the aَuthor recently development and empirically validated an IT performance evalution framework. This frame is called balanced scorecard which is a polyhedral model and contains five perspectives, which are:(1-operational perspective, 2- benefits perspective, 3-user orientation perspective, 4- strategic competitiveness perspective, and 5- technology/system perspective) [18].
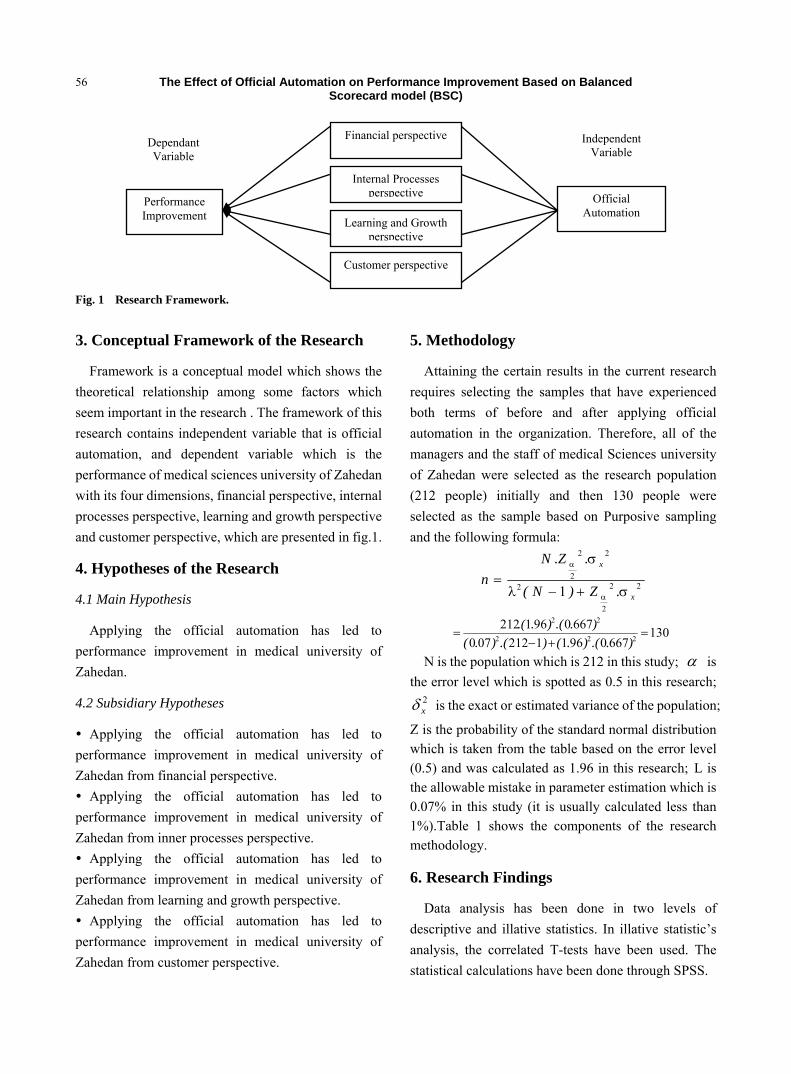
The Effect of Official Automation on Performance Improvement Based on Balanced Scorecard model (BSC)
56
Fig. 1 Research Framework.
3. Conceptual Framework of the Research
Framework is a conceptual model which shows the theoretical relationship among some factors which seem important in the research . The framework of this research contains independent variable that is official automation, and dependent variable which is the performance of medical sciences university of Zahedan with its four dimensions, financial perspective, internal processes perspective, learning and growth perspective and customer perspective, which are presented in fig.1.
4. Hypotheses of the Research
4.1 Main Hypothesis
Applying the official automation has led to performance improvement in medical university of Zahedan.
4.2 Subsidiary Hypotheses
Applying the official automation has led to performance improvement in medical university of Zahedan from financial perspective. Applying the official automation has led to
performance improvement in medical university of Zahedan from inner processes perspective. Applying the official automation has led to
performance improvement in medical university of Zahedan from learning and growth perspective. Applying the official automation has led to
performance improvement in medical university of Zahedan from customer perspective.
5. Methodology
Attaining the certain results in the current research requires selecting the samples that have experienced both terms of before and after applying official automation in the organization. Therefore, all of the managers and the staff of medical Sciences university of Zahedan were selected as the research population (212 people) initially and then 130 people were selected as the sample based on Purposive sampling and the following formula:
22
2
2
22
2
1 x
x
.Z)N(
.Z.Nn
σ+−
σ=
α
α
λ
13066709611212070
6670961212222
22
=+−
=)..().().().(
)..()..(
N is the population which is 212 in this study; α is the error level which is spotted as 0.5 in this research;
2xδ is the exact or estimated variance of the population;
Z is the probability of the standard normal distribution which is taken from the table based on the error level (0.5) and was calculated as 1.96 in this research; L is the allowable mistake in parameter estimation which is 0.07% in this study (it is usually calculated less than 1%).Table 1 shows the components of the research methodology.
6. Research Findings
Data analysis has been done in two levels of descriptive and illative statistics. In illative statistic’s analysis, the correlated T-tests have been used. The statistical calculations have been done through SPSS.
Learning and Growth perspective
Internal Processes perspective
Financial perspective
Customer perspective
Official Automation
Performance Improvement
Independent Variable
Dependant Variable
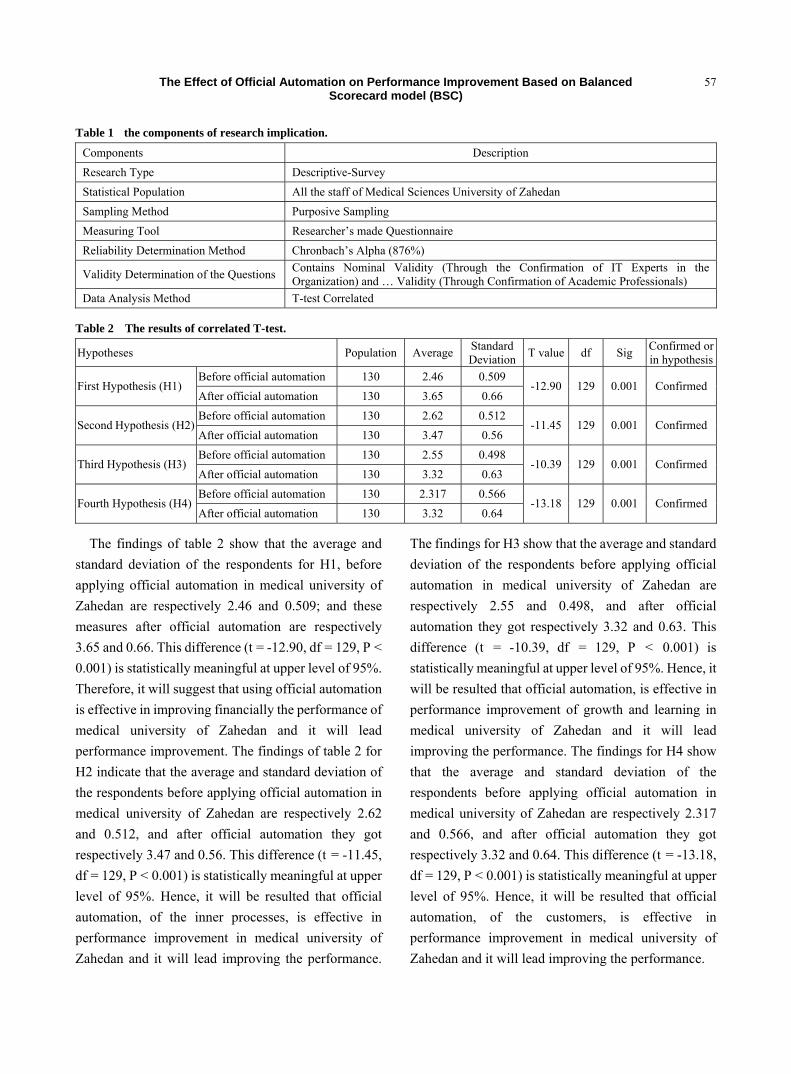
The Effect of Official Automation on Performance Improvement Based on Balanced Scorecard model (BSC)
57
Table 1 the components of research implication.
Components Description Research Type Descriptive-Survey Statistical Population All the staff of Medical Sciences University of Zahedan Sampling Method Purposive Sampling Measuring Tool Researcher’s made Questionnaire Reliability Determination Method Chronbach’s Alpha (876%)
Validity Determination of the Questions Contains Nominal Validity (Through the Confirmation of IT Experts in the Organization) and … Validity (Through Confirmation of Academic Professionals)
Data Analysis Method T-test Correlated
Table 2 The results of correlated T-test. Confirmed or in hypothesisSig df T value Standard
DeviationAveragePopulationHypotheses
0.509 2.46 130 Before official automation Confirmed0.001 129 -12.90
0.66 3.65 130 After official automation First Hypothesis (H1)
0.512 2.62 130 Before official automation Confirmed0.001 129 -11.45
0.56 3.47 130 After official automation Second Hypothesis (H2)
0.498 2.55 130 Before official automation Confirmed0.001 129 -10.39
0.63 3.32 130 After official automation Third Hypothesis (H3)
0.566 2.317 130 Before official automation Confirmed0.001 129 -13.18
0.64 3.32 130 After official automation Fourth Hypothesis (H4)
The findings of table 2 show that the average and standard deviation of the respondents for H1, before applying official automation in medical university of Zahedan are respectively 2.46 and 0.509; and these measures after official automation are respectively 3.65 and 0.66. This difference (t = -12.90, df = 129, P < 0.001) is statistically meaningful at upper level of 95%. Therefore, it will suggest that using official automation is effective in improving financially the performance of medical university of Zahedan and it will lead performance improvement. The findings of table 2 for H2 indicate that the average and standard deviation of the respondents before applying official automation in medical university of Zahedan are respectively 2.62 and 0.512, and after official automation they got respectively 3.47 and 0.56. This difference (t = -11.45, df = 129, P < 0.001) is statistically meaningful at upper level of 95%. Hence, it will be resulted that official automation, of the inner processes, is effective in performance improvement in medical university of Zahedan and it will lead improving the performance.
The findings for H3 show that the average and standard deviation of the respondents before applying official automation in medical university of Zahedan are respectively 2.55 and 0.498, and after official automation they got respectively 3.32 and 0.63. This difference (t = -10.39, df = 129, P < 0.001) is statistically meaningful at upper level of 95%. Hence, it will be resulted that official automation, is effective in performance improvement of growth and learning in medical university of Zahedan and it will lead improving the performance. The findings for H4 show that the average and standard deviation of the respondents before applying official automation in medical university of Zahedan are respectively 2.317 and 0.566, and after official automation they got respectively 3.32 and 0.64. This difference (t = -13.18, df = 129, P < 0.001) is statistically meaningful at upper level of 95%. Hence, it will be resulted that official automation, of the customers, is effective in performance improvement in medical university of Zahedan and it will lead improving the performance.
The Effect of Official Automation on Performance Improvement Based on Balanced Scorecard model (BSC)
58
7. Results and Discussion
In this research for determining the effect of official automation on the performance improvement in the organization based on the BSC model, using the scientific method, researcher’s made questionnaire and SPSS, the following results were obtained:
Based on the analysis of the findings of H1, the hypothesis was confirmed. Therefore, official automation is effective in improving financially the performance of medical university of Zahedan and it will lead performance improvement. Among the financial indexes, applying official automation in the medical university of Zahedan has had the least effect on the cost of the documents’ maintenance.
Based on the analysis of the findings of H2, this hypothesis was also confirmed. Hence, it will be resulted that official automation, of the inner processes, is effective in performance improvement in medical university of Zahedan and it will lead improving the performance. Among the indexes of inner processes, official automation has had the least effect on the index of wasting the ownership, monopoly of the organizational information and public access to the information, proportionate to the organizational level.
Based on the analysis of the findings of H3, this hypothesis was also confirmed. So, it will be resulted that official automation, is effective in performance improvement of growth and learning in medical university of Zahedan and it will lead improving the performance. Among the indicators of growth and learning, official automation has had the least effect on the index of empathy creation in the organization (teamwork culture …).
Based on the analysis of the findings of H4, this hypothesis was also confirmed. Therefore, it will be resulted that official automation, of the customers, is effective in performance improvement in medical university of Zahedan and it will lead improving the performance. Among the indicators of the customers, official automation has had the least effect on the indexes of better perception of the requirements
(offering proper services) and exposing full time attendances.
Consequently, according to the confirmation of the hypotheses of this study, the main hypothesis was confirmed. So, applying official automation in the medical university of Zahedan has caused better performance. But, its effect has not been the same on 4 points of view. The findings displayed that the most and the least effects have been respectively on the financial improvement and the growth and learning increment.
References [1] H. Alinston, Corporate planning, forecasting and the long
mave, Futures 2002 (34) 317. [2] K. Palithe, R. Smith and P. Mondar, IT project
implementation strategies for effective change? Review Lojestic Information Management 2002 (2) 126.
[3] E. J. Mutsaers, Z. Hanvander and G. Henrik, The evolution of information technology, Information Management & Computer Security 1998 (3) 113.
[4] K. Muata, O. Bryson and K. Myung, Exploring the Relationship between Information Technology Investment and Firm Performance Using Regression Splints Analysis, Department of Information Systems, available online at: http://www.Elsevier.com / locate /dsw, 2003.
[5] G. Masion, Information Technology and Dilemmas in Organizational Learning, Journal of Organizational Change Management 1999 (5) 360-376, available online at: http://www.emerald-library.com.
[6] A. Baines, Using Information Technology to Facilitate Organizational Change, Work Study 1998 (2) 49.
[7] M. McClea and D. C. Yen, A Frame Work for the Utilization of Information Technology in higher Education Admission Department, International Journal of Educational Management 2005 (2) 8, available online at: http://www.emeraldinsight.com/research register.
[8] R. Kaplan and D. Norton, The Balanced Scorecard: Translating Stratgy Into Action, Harvard Bussiness School Press, Boston, MA, 1996.
[9] M. Moullin, Eight essentials of performance measurment, International Journal of Health Care Quality Assurance 2004 (13) 110.
[10] M. Martinsons, R. Davison and D. Tse, The balanced scorecard: a foundation for the strategic management of information system, Decision Support System 1999 (1) 71-78.
[11] R. Kaplan and D. Norton, The Balanced Scorecard: Translating Stratgy into Action, Harvard Bussiness School Press, Boston, MA, 1996, p.8.
The Effect of Official Automation on Performance Improvement Based on Balanced Scorecard model (BSC)
59
[12] D. Otely, Performance management: a framework for management control systems research, Management Accounting Research, 1999 (10) 374.
[13] R. Kaplan and D. Norton, The Strategy-focused Organization: How Balanced Scorecard Companies, Thrive in the New Business Environmental, Harvard Bussiness School Press, Boston, MA, 2001.
[14] P. R. Niven, Balanced Scorecard Step by Step, Johan Wiley & Sons, Newyork, NY, 2002.
[15] H. S. Chen and Y. Y. Shiau, The application of balanced scorecard in the performance evaluation of higher education, The TQM Magazine 2006 (2) 190-205.
[16] C. H. Huang, Designing a knowledge-based system for strategic planing: a balanced scorecard perspective, Expert Systems with Applications 2009 (1) 209-218.
[17] U. Cebeci, Fuzzy AHP-based decision support system for selecting erp systems in textile industry by balanced scorecard, Expert Systems with Applications 2009 (5) 8900-8909.
[18] A. R. Stewart, A framework for the life cycle management of information technology projects: project IT, Information Journal of Project Management 2008 (2) 203-212.

Call for Paper
Discription Journal of US-China Medical Science is an international, scholarly and peer-reviewed journal (print and
online) published monthly by David Publishing Company, USA which was founded in 2001. The Journal seeks to bridge and integrate the intellectual, methodological, and substantive diversity of medical science scholarship, and to encourage a vigorous dialogue between medical science scholars and practitioners.
The journal is publishing good quality of research work in all areas of medical sciences. The Journal serves wide ranges of international audiences of medical researchers, pharmaceutical employees, specialized and general clinicians. Submissions of papers in areas of basic medical sciences are welcomed as well as papers in clinical and experimental research related to the studies of human diseases.
The journal invites papers in all areas of medicine and medical sciences such as: ◆ Clinical Medicine ◆ Basic Medical Sciences ◆ Experimental Medicine ◆ Preventive Medicine ◆ Social Medicine
Information for Authors
1. The manuscript should be original, and has not been published previously nor be currently under consideration for publication elsewhere. Manuscripts submitted under multiple authorship are reviewed on the assumption that all listed authors concur with the submission and that a copy of the final manuscript has been approved by all authors and tacitly or explicitly by the responsible authorities in the laboratories where the work was carried out. 2. Manuscripts may be 3000-8000 words or longer if approved by the editor, including an abstract, texts, tables, footnotes, appendixes, and references. The title should be on page 1 and not exceed 15 words, and should be followed by an abstract of 100 – 200 words.3-5 keywords or key phrases are required. 3. The manuscript should be in MS Word format, submitted as an email attachment to our email address. 4. Authors of the articles being accepted are required to sign the Transfer of Copyright Agreement form. 5. Author will receive 2 copies of the issue of the journal containing their article. 6. It is not our policy to pay authors.
Peer Review Policy
Journal of US-China Medical Science is a refereed journal. All research articles in this journal undergo rigorous peer review, based on initial editor screening and anonymised refereeing by at least two anonymous referees.
Editorial Procedures
All papers considered appropriate for this journal are reviewed anonymously by at least two outside reviewers. The review process usually takes two to three weeks. Papers are accepted for publication subject to no substantive, stylistic editing. The Editor reserves the right to make any necessary changes in the papers, or request the author to do so, or reject the paper submitted. A copy of the edited paper along with the first proofs will be sent to the author for proofreading. They should be corrected and returned to the Editor within seven days. Once the final version of the paper has been accepted, authors are requested not to make further changes to the text.
Submission of Manuscript
All manuscripts submitted will be considered for publication. Manuscripts should be sent online or as an email attachment to: [email protected], [email protected], [email protected].






























