Embed Size (px)
Citation preview

DATA HANDOVER FOR HEALTHCARE FACILITIES MANAGEMENT
Dr. Allan D. Chasey, Program Chair, [email protected]
Arundhati Ghosh, Graduate Research Assistant, [email protected]
Del E Webb School of Construction,
Arizona State University, Tempe, AZ, USA
Outline
• The Problem
• The FM-Technology-Data-BIM Vision
• BIM+FM: Combining the data
• Why Healthcare?
• Research Method
• Objectives and Methods
• Information Model
• Communication Model
• Conclusions
Background
Business Function
o Lower operating costs & manage life-cycle costs
o Optimize performance, maintain environment quality
o Enhance productivity by generating cost savings
while adding strategic value to the organization
Success of a FM team
o Making informed decisions
o Availability of accurate and up to date information
o Knowledge of the current operations
Inefficiencies caused by
o Numerous channels, networks, levels, and formats of communication
o Absence of a well-integrated information management system
o Late involvement of the FM at the front end
o Lack of documentation of FM needs based on daily processes
$4.8 billion for information verification and validation
$613 million to transfer the data to a single usable
communication format
$6.9 billion on interoperability
$1.5 billion on information delays and 'idle-time' of employees
due to the unavailability of 'as-is' information
Gallaher, M. P., Connor, A. C., Dettbarn, J. L., & Gilday, L. T. (2004), Cost Analysis of Inadequate
Interoperability in the U . S . Capital Facilities Industry, National Institute of Standards and
Technology Gaithersburg, Maryland.
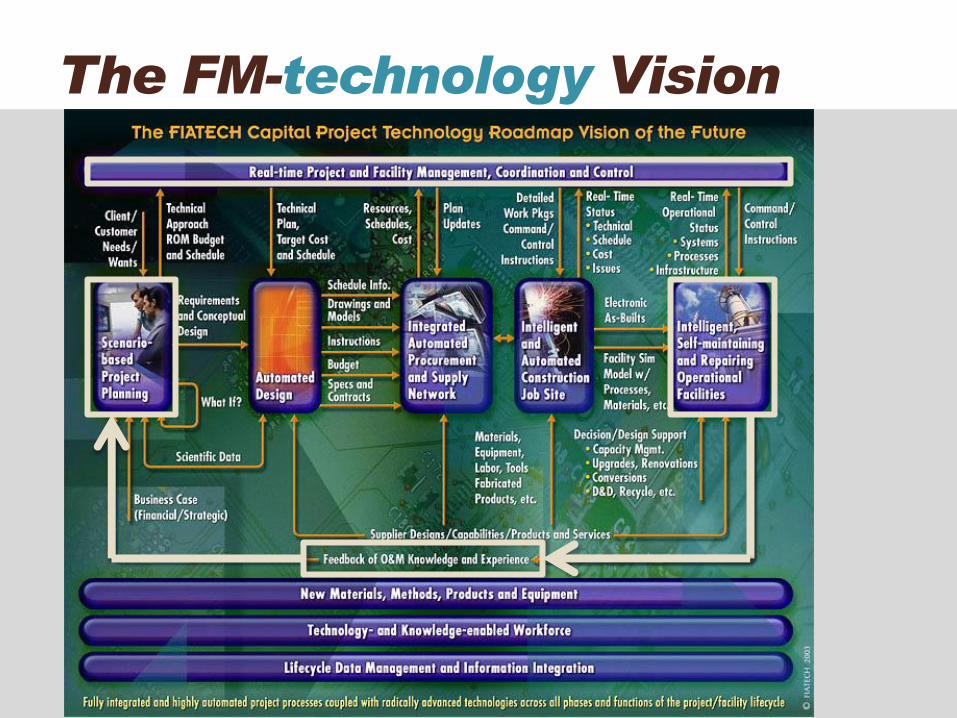
The FM-technology Vision
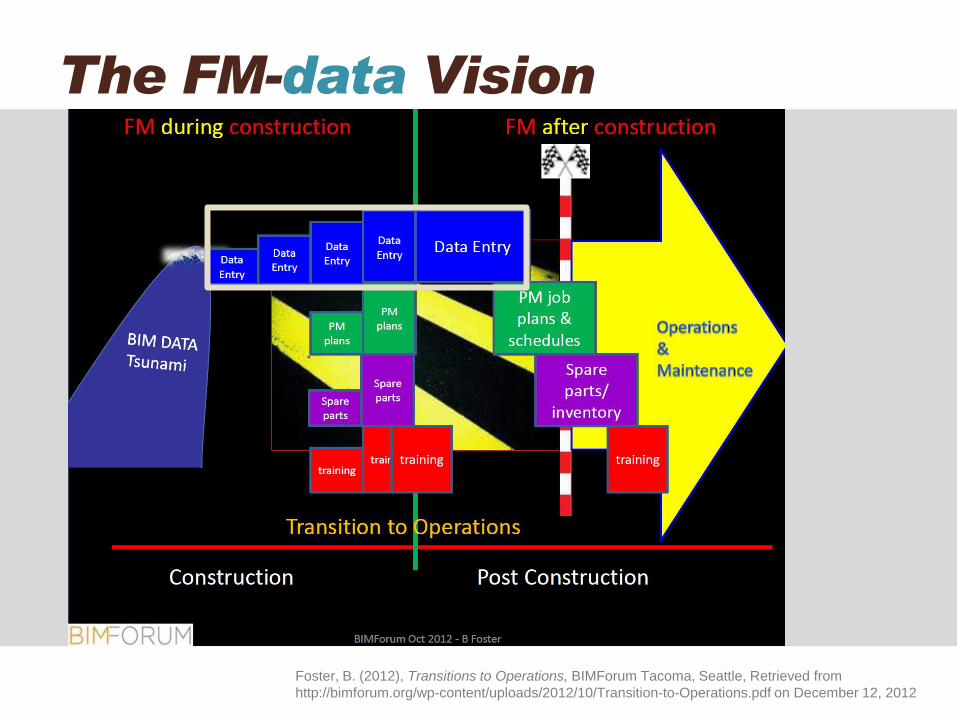
The FM-data Vision
Foster, B. (2012), Transitions to Operations, BIMForum Tacoma, Seattle, Retrieved from
http://bimforum.org/wp-content/uploads/2012/10/Transition-to-Operations.pdf on December 12, 2012
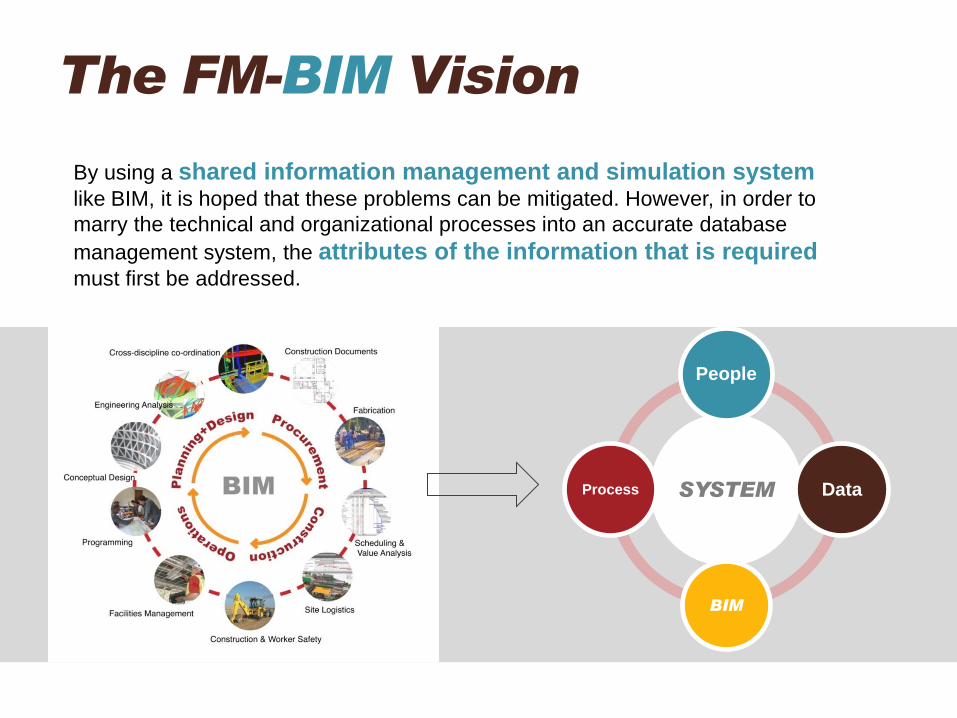
By using a shared information management and simulation system like BIM, it is hoped that these problems can be mitigated. However, in order to
marry the technical and organizational processes into an accurate database
management system, the attributes of the information that is required must first be addressed.
SYSTEM
People
Data
BIM
Process
The FM-BIM Vision
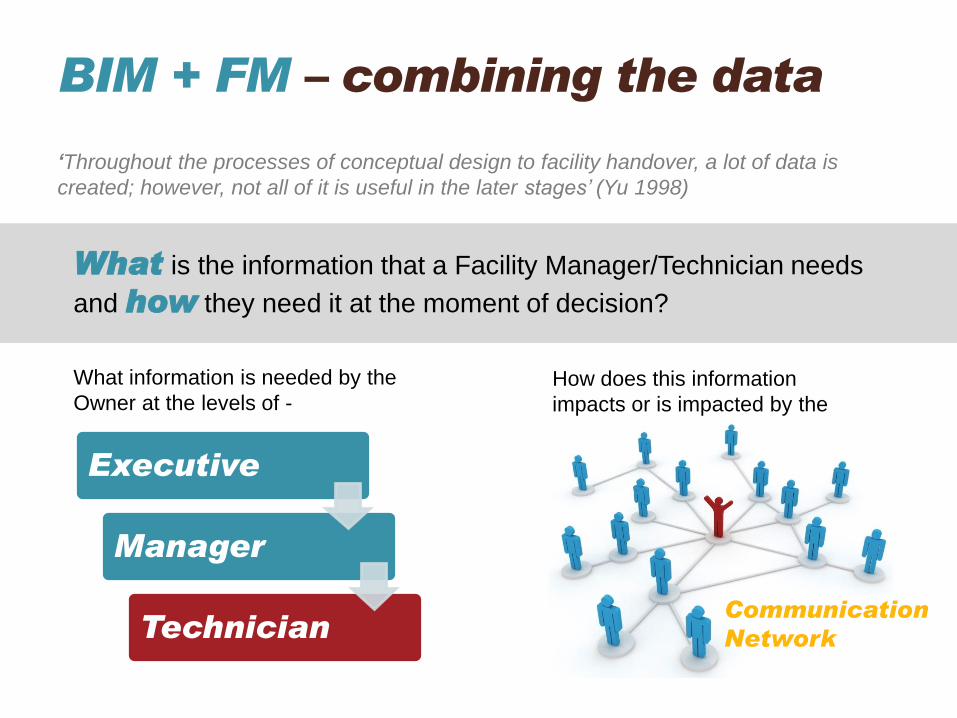
‘Throughout the processes of conceptual design to facility handover, a lot of data is
created; however, not all of it is useful in the later stages’ (Yu 1998)
BIM + FM – combining the data
Executive
Manager
Technician
What information is needed by the
Owner at the levels of - How does this information
impacts or is impacted by the
Communication
Network
What is the information that a Facility Manager/Technician needs
and how they need it at the moment of decision?
Similar to other advanced technology facilities, healthcare architecture is a myriad of critical
systems (including medical gases, chemicals, radioactive elements), structures, hazardous wastes,
environmental conditions, risk and safety factors.
Owners of healthcare facilities typically tend to own, operate and maintain their facilities and are
usually fast to get on board with the use of advanced project delivery
techniques for the design, construction and maintenance of their complex projects (Lavy 2010).
The dependency of human lives on the skilled staff (doctors, nurses and specialists) and
the infrastructure systems that support daily operations makes the services critical in nature
mandating dedicated research.
Additionally, a healthcare facility supports large numbers of people (patients, doctors,
staff, and visitors), numerous medical equipments, and a fast developing technology.
The decisions made up front affect the medical outcomes, capital
expenditures and operational expenditures.
Why Healthcare?
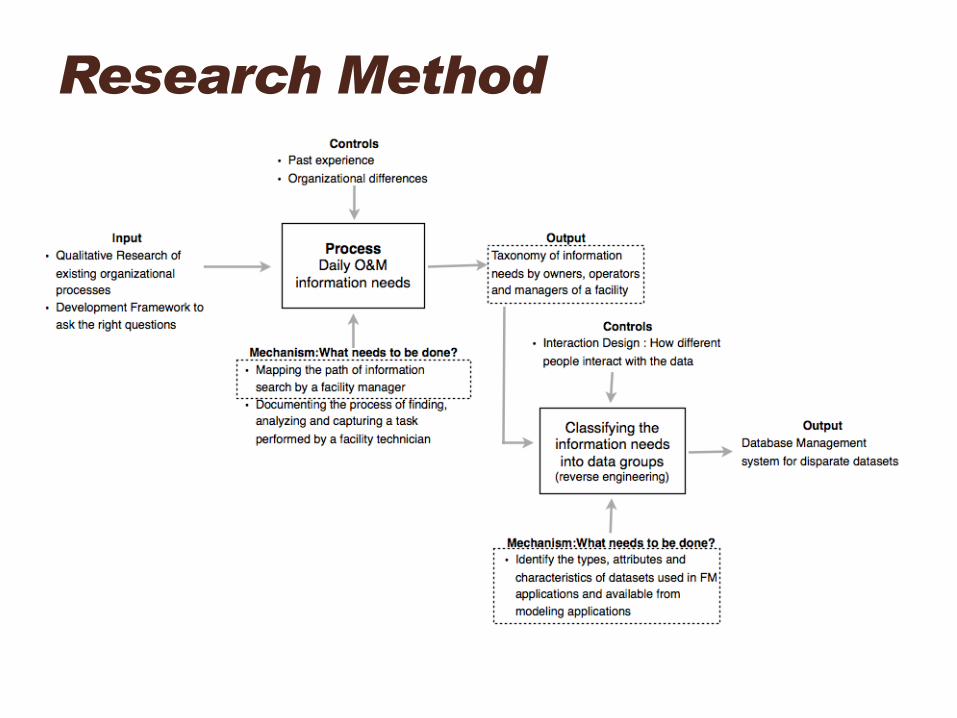
Research Method
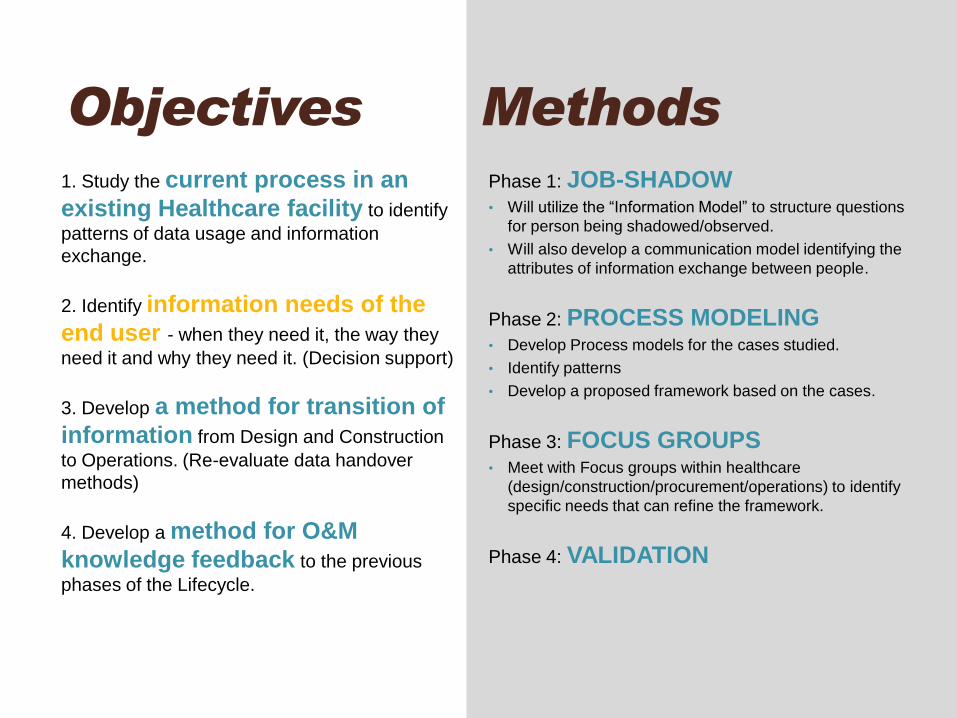
Phase 1: JOB-SHADOW • Will utilize the “Information Model” to structure questions
for person being shadowed/observed.
• Will also develop a communication model identifying the
attributes of information exchange between people.
Phase 2: PROCESS MODELING • Develop Process models for the cases studied.
• Identify patterns
• Develop a proposed framework based on the cases.
Phase 3: FOCUS GROUPS • Meet with Focus groups within healthcare
(design/construction/procurement/operations) to identify
specific needs that can refine the framework.
Phase 4: VALIDATION
1. Study the current process in an
existing Healthcare facility to identify
patterns of data usage and information
exchange.
2. Identify information needs of the
end user - when they need it, the way they
need it and why they need it. (Decision support)
3. Develop a method for transition of
information from Design and Construction
to Operations. (Re-evaluate data handover
methods)
4. Develop a method for O&M
knowledge feedback to the previous
phases of the Lifecycle.
Objectives Methods
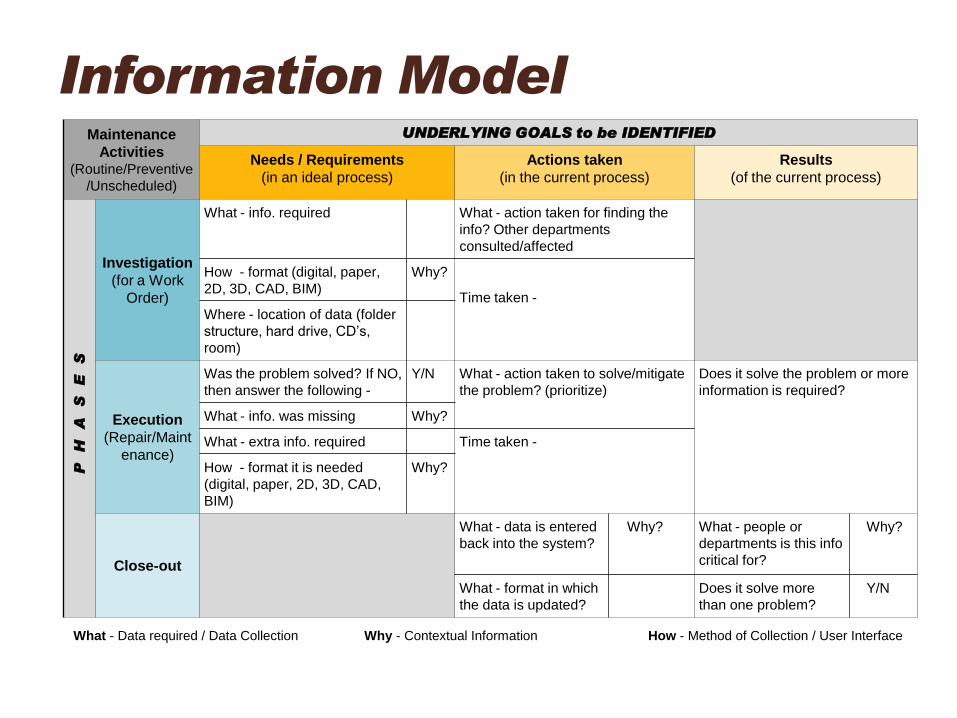
Information Model Maintenance
Activities (Routine/Preventive
/Unscheduled)
UNDERLYING GOALS to be IDENTIFIED
Needs / Requirements
(in an ideal process)
Actions taken
(in the current process)
Results
(of the current process)
PH
AS
ES
Investigation
(for a Work
Order)
What - info. required What - action taken for finding the
info? Other departments
consulted/affected
How - format (digital, paper,
2D, 3D, CAD, BIM)
Why?
Time taken -
Where - location of data (folder
structure, hard drive, CD’s,
room)
Execution
(Repair/Maint
enance)
Was the problem solved? If NO,
then answer the following -
Y/N What - action taken to solve/mitigate
the problem? (prioritize)
Does it solve the problem or more
information is required?
What - info. was missing Why?
What - extra info. required Time taken -
How - format it is needed
(digital, paper, 2D, 3D, CAD,
BIM)
Why?
Close-out
What - data is entered
back into the system?
Why? What - people or
departments is this info
critical for?
Why?
What - format in which
the data is updated?
Does it solve more
than one problem?
Y/N
What - Data required / Data Collection Why - Contextual Information How - Method of Collection / User Interface
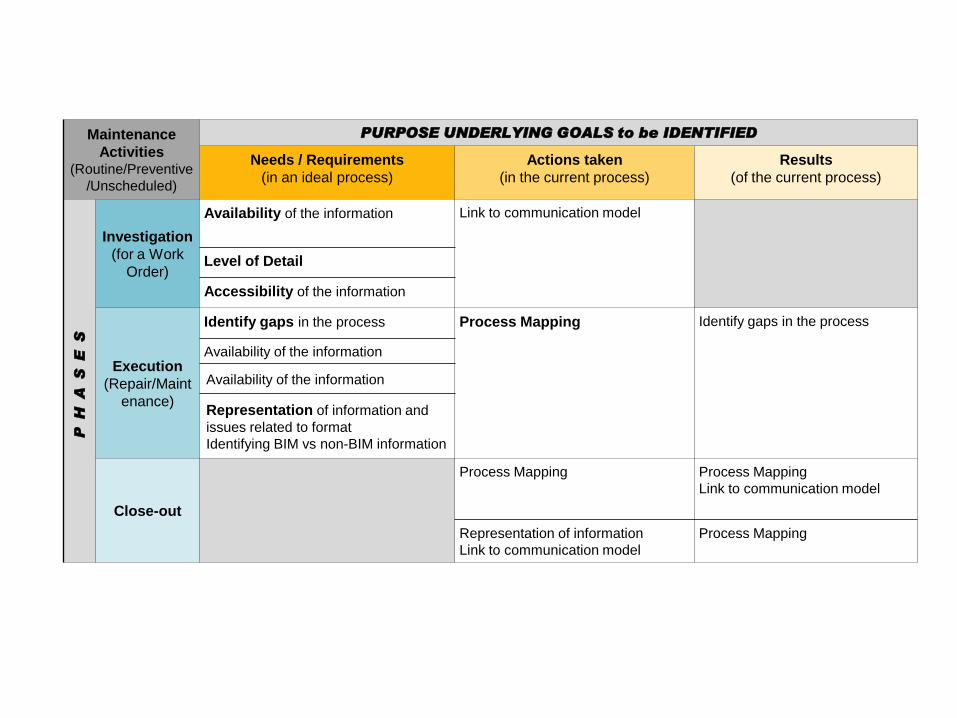
Maintenance
Activities (Routine/Preventive
/Unscheduled)
PURPOSE UNDERLYING GOALS to be IDENTIFIED
Needs / Requirements
(in an ideal process)
Actions taken
(in the current process)
Results
(of the current process)
PH
AS
ES
Investigation
(for a Work
Order)
Availability of the information Link to communication model
Level of Detail
Accessibility of the information
Execution
(Repair/Maint
enance)
Identify gaps in the process Process Mapping
Identify gaps in the process
Availability of the information
Availability of the information
Representation of information and
issues related to format
Identifying BIM vs non-BIM information
Close-out
Process Mapping
Process Mapping
Link to communication model
Representation of information
Link to communication model
Process Mapping
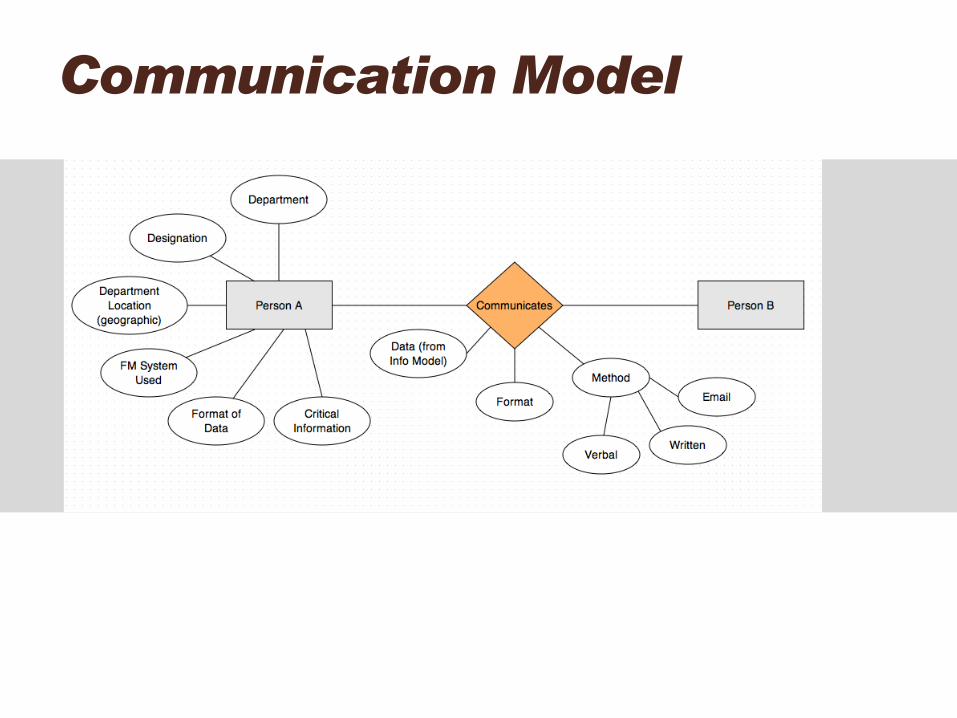
Communication Model
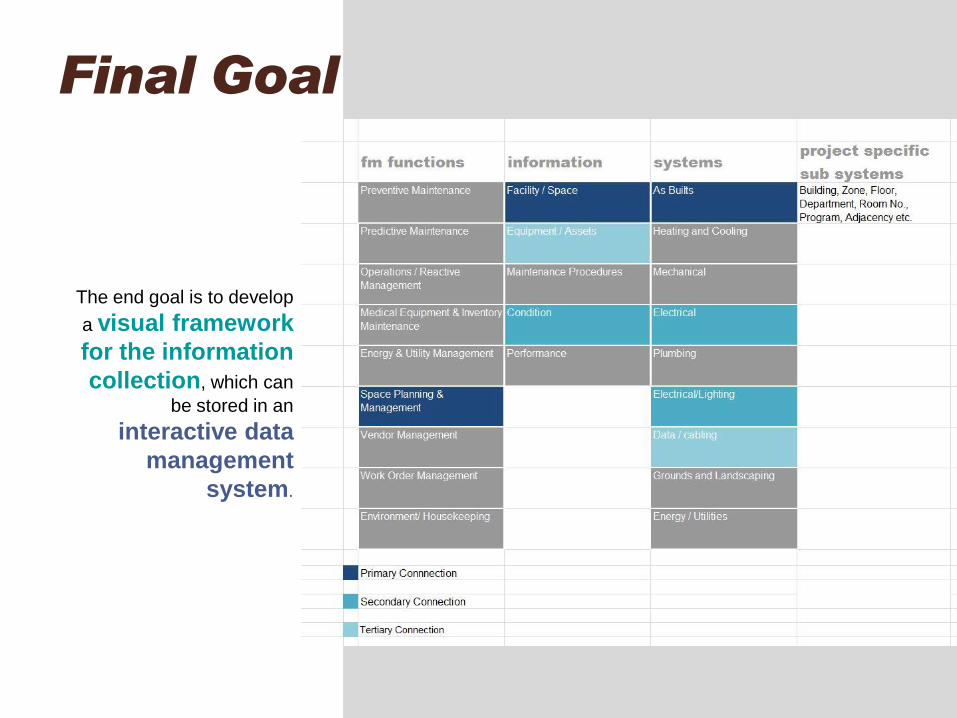
Final Goal
The end goal is to develop
a visual framework
for the information
collection, which can
be stored in an
interactive data
management
system.
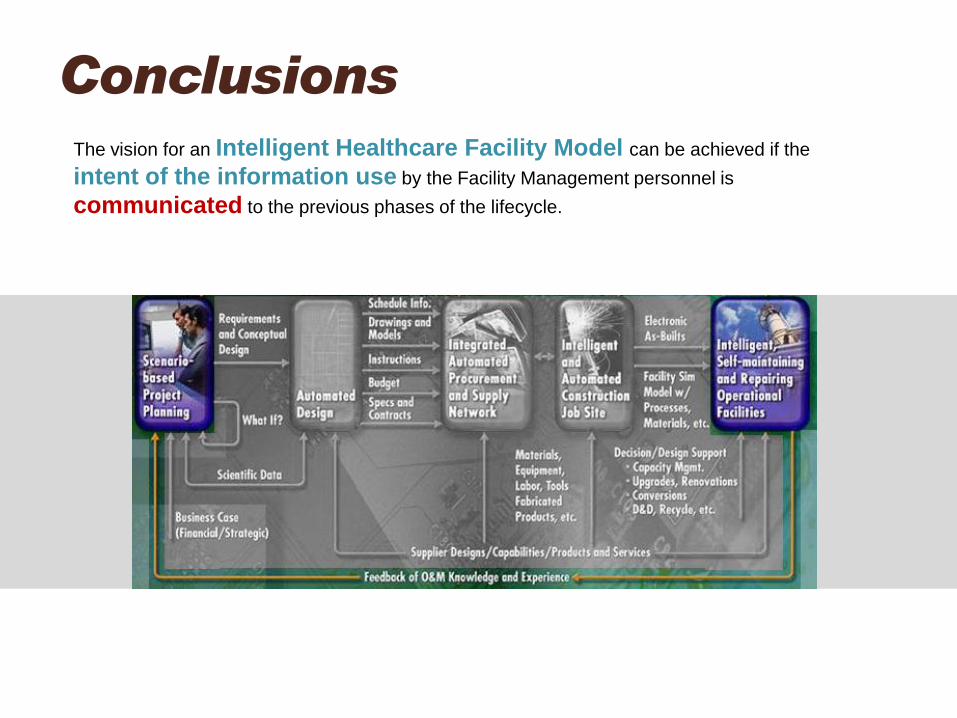
Conclusions The vision for an Intelligent Healthcare Facility Model can be achieved if the
intent of the information use by the Facility Management personnel is
communicated to the previous phases of the lifecycle.
• Cotts, D.G., Roper, K.O., Payant, R., (August 2009), The Facility Management Handbook, (Third edition) New York: AMACOM Publishing.
• Shohet, I.M. & Lavy, S. (2004), “Healthcare facilities management: state of the art review”, Facilities, Vol. 22 No. 7/8, pp. 210-220.
• Lucas, J., Bulbul, T., & Thabet, W. (2011), “A lifecycle framework for using BIM in Healthcare Facility Management”, CIB W78-W102 2011:
International Conference, Sophia Antipolis, France. Retrieved from http://itc.scix.net/data/works/att/w78-2011-Paper-73.pdf
• Gallaher, M. P., Connor, A. C., Dettbarn, J. L., & Gilday, L. T. (2004), Cost Analysis of Inadequate Interoperability in the U . S . Capital
Facilities Industry, National Institute of Standards and Technology Gaithersburg, Maryland.
• Yu, K., Froese, F., Grobler, F., (October 1998), “Development of Industry Foundation Classes by International Alliance for Interoperability”,
Computing Congress 98, American Society for Civil Engineers (ASVE), Boston.
• Akcamete, A., Akinci, B., & Garrett, Jr., J. H. (2009), “Motivation for Computational Support for Updating Building Information Models
(BIMs)”, Computing in Civil Engineering (2009) (pp. 523–532). Reston, VA: American Society of Civil Engineers.
• Shen, W., Hao, Q., & Xue, Y. (2012), “A loosely coupled system integration approach for decision support in facility management and
maintenance”, Automation in Construction, 25, 41–48.
• Foster, B. (2010), BIM for Facility Management : “Design for maintenance.” Retrieved from www.sandia.gov
• FM:Systems (2012). Products. Retrieved from http://www.fmsystems.com/products/index.html
• Starkov, I., Yee, P., Aspurez, V., & Alpert, D. (2012). Emerging Applications of BIM to Facilities Management: What Architects Need to Know
about Connecting Design and Operations. Washington DC.
• Whyte, J., Lindkvist, C., & Ibrahim, N. H. (2010). Value to Clients through Data Hand-Over : A Pilot Study Value to Clients through Data
Hand-Over : A Pilot Study. Retrieved from http://www.reading.ac.uk/web/FILES/designinnovation/DIRC_Working_Paper_1.pdf
• Gelnay, B. (2002), “Facility management and the design of Victoria Public Hospitals”, Proceedings of the CIB Working Commission 70:
Facilities Management and Maintenance Global Symposium 2002, Glasgow, pp. 525-45 as cited in Shohet, I.M. & Lavy, S. (2004),
“Healthcare facilities management: state of the art review”, Facilities, Vol. 22 No. 7/8, pp. 210-220.
• Lavy, S. & Solis, J.F. (2010), “Complex Healthcare Facility Management and Lean Construction”, Health Environments Research & Design
Journal, Vol. 3 No. 2, pp. 3-6.
• Goedert, J. D., & Meadati, P. (2008). Integrating Construction Process Documentation into Building Information Modeling. Journal of
Construction Engineering and Management, 134(7), 509–516.
• Autodesk. (2004). BIM and Facilities Management.
• Yau, N. (2010). Global agenda councils who should work together. Retrieved from http://www.visualizing.org/visualizations/global-agenda-
councils-who-should-work-together
References
Questions?
Thank You!





























