Embed Size (px)
Citation preview
DANGERS LURKING WITHIN YOUR CUPBOARDS: OUTCOMES AND MANAGEMENT OF INTENTIONAL OR ACCIDENTAL INGESTIONS
Session Goals
Content of annual report of the National Poison Data Summary (NPDS)
Review cases that highlight the ease of household ingestions whether or not intentional
Management of a common life threatening ingestion
Poison Control Services within California
Hypercalcemia
Symptoms at 12 Normal 9-10.5 Emergent if >15 >2500mg per day is considered toxic Cleared renally TUMs have 200-400mg per pill treatment with IVF fluids and salt then
diuretics and if needed biphosphinates and calcitonin
National Poison Data System (NPDS) There are 57 Poison Control Centers across
the country >2 million human poison exposures per year Maintain a data base of >350,000 drugs,
chemicals, and agents and their exposure behaviors
There are 4 poison control centers in California (SF, SD, Sacramento, Central Valley) originated in 1997. CPCS keeps 78% at home.
NPDS Summary 2011
1158 fatalities - 6% children <20 yo and 94% in adults
1077 intentional and 147 unintentional deaths 94.5% were either ingestion or
inhalation/nasal With children, death is unintentional and
adults is intentional Nearly 50% of exposures were in children <6
with the greatest number in 1-2 yo
NPDS Summary 2011
Nearly 50% of exposures are single substance Analgesics are the #1 exposure followed by
cosmetics and personal care products Kids <5 years old are exposed most often to
cosmetics/PC products Adults exposures are
analgesics/sedatives/hypnotics/antipsychotic 52 pediatric deaths (street, analgesics,
stimulants
Up and Away Campaign
1. Pick a place for medications where children cannot reach. 2. Put medications away after use… Every time! 3. Make sure the safety cap is locked. 4. Teach your children about medicine safety. 5. Tell guests about medication safety. 6. Be prepared in case of an emergency, have the number located for all to see. 1-800-222-1222
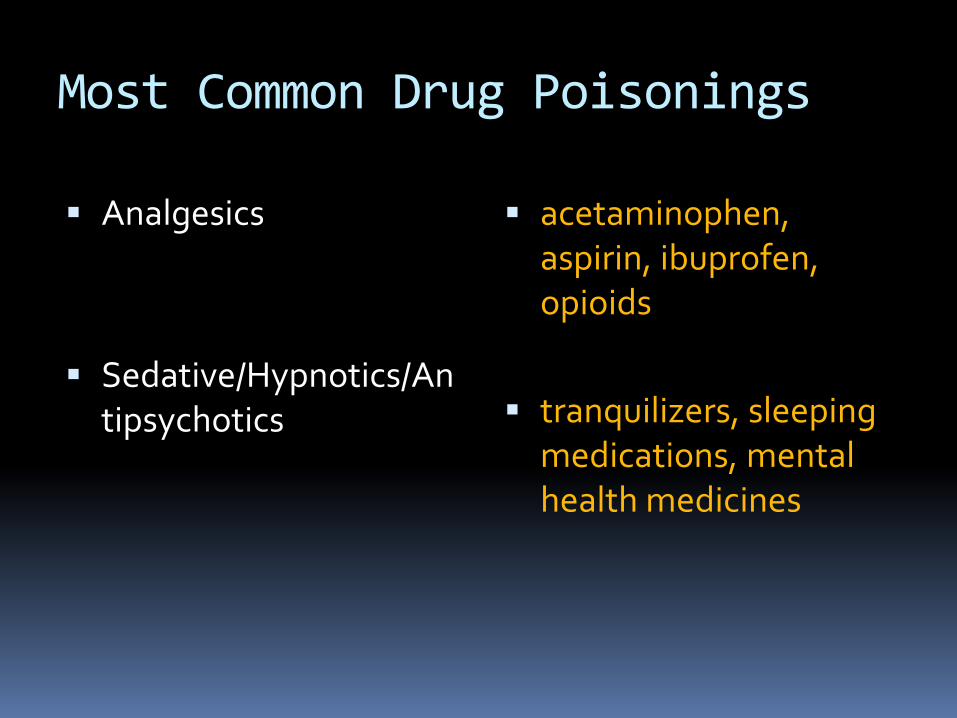
Most Common Drug Poisonings
Analgesics
Sedative/Hypnotics/Antipsychotics
acetaminophen, aspirin, ibuprofen, opioids
tranquilizers, sleeping
medications, mental health medicines
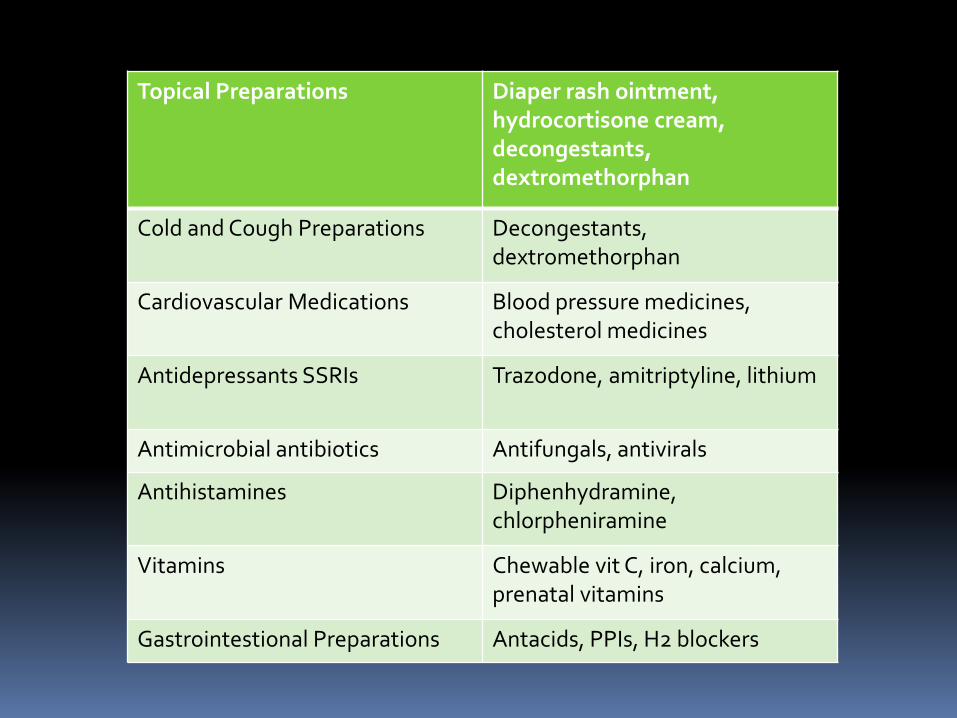
Topical Preparations Diaper rash ointment, hydrocortisone cream, decongestants, dextromethorphan
Cold and Cough Preparations Decongestants, dextromethorphan
Cardiovascular Medications Blood pressure medicines, cholesterol medicines
Antidepressants SSRIs Trazodone, amitriptyline, lithium
Antimicrobial antibiotics Antifungals, antivirals
Antihistamines Diphenhydramine, chlorpheniramine
Vitamins Chewable vit C, iron, calcium, prenatal vitamins
Gastrointestional Preparations Antacids, PPIs, H2 blockers
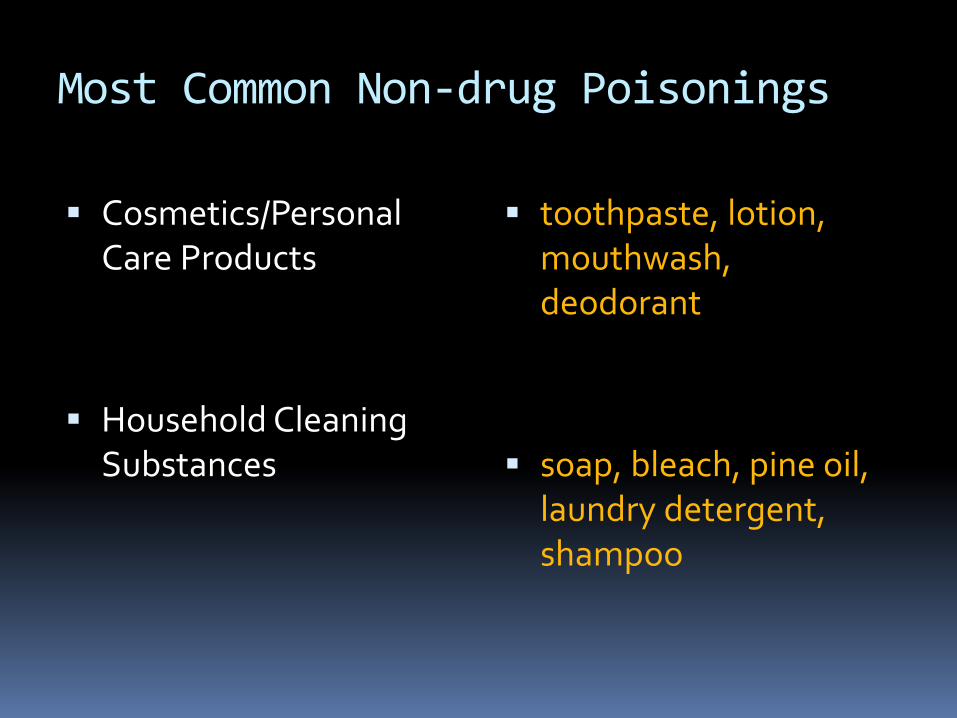
Most Common Non-drug Poisonings
Cosmetics/Personal Care Products
Household Cleaning Substances
toothpaste, lotion, mouthwash, deodorant
soap, bleach, pine oil, laundry detergent, shampoo
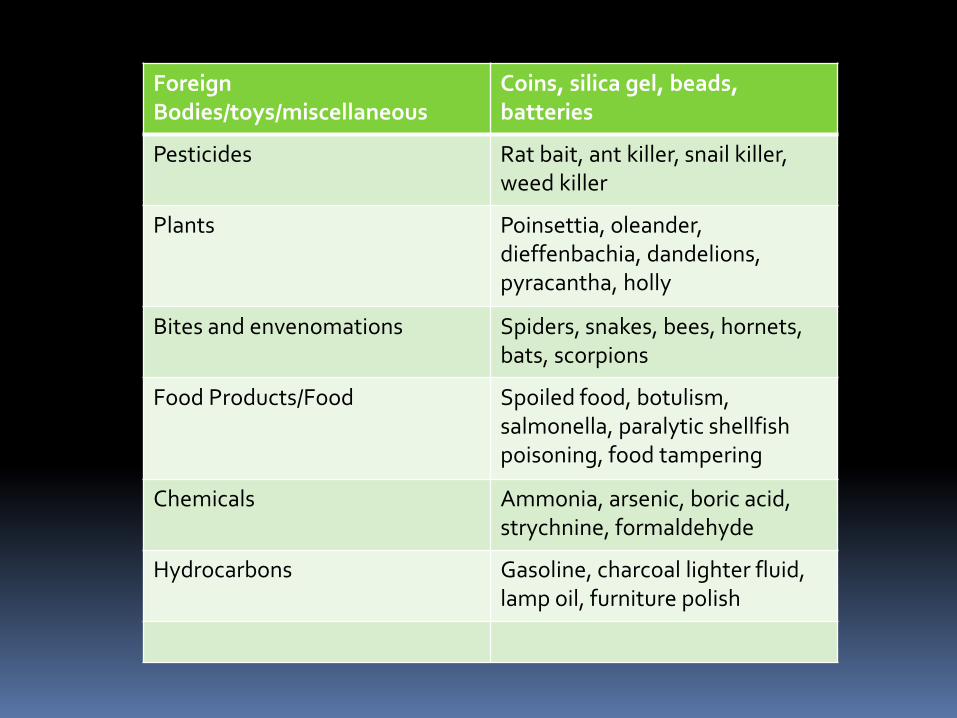
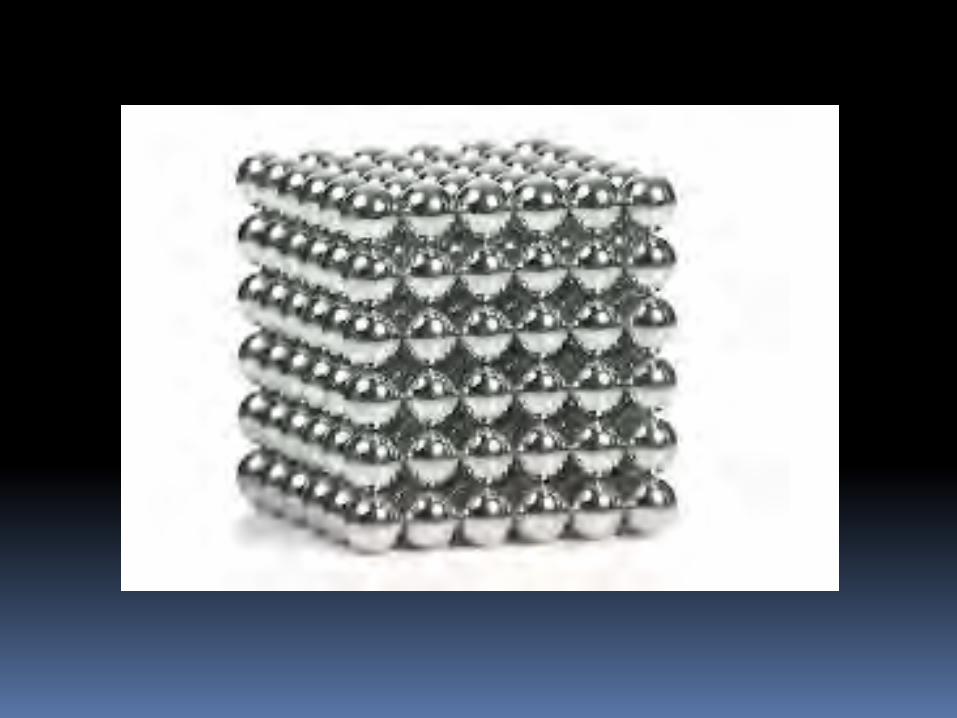
Foreign Bodies/toys/miscellaneous
Coins, silica gel, beads, batteries
Pesticides Rat bait, ant killer, snail killer, weed killer
Plants Poinsettia, oleander, dieffenbachia, dandelions, pyracantha, holly
Bites and envenomations Spiders, snakes, bees, hornets, bats, scorpions
Food Products/Food Spoiled food, botulism, salmonella, paralytic shellfish poisoning, food tampering
Chemicals Ammonia, arsenic, boric acid, strychnine, formaldehyde
Hydrocarbons Gasoline, charcoal lighter fluid, lamp oil, furniture polish
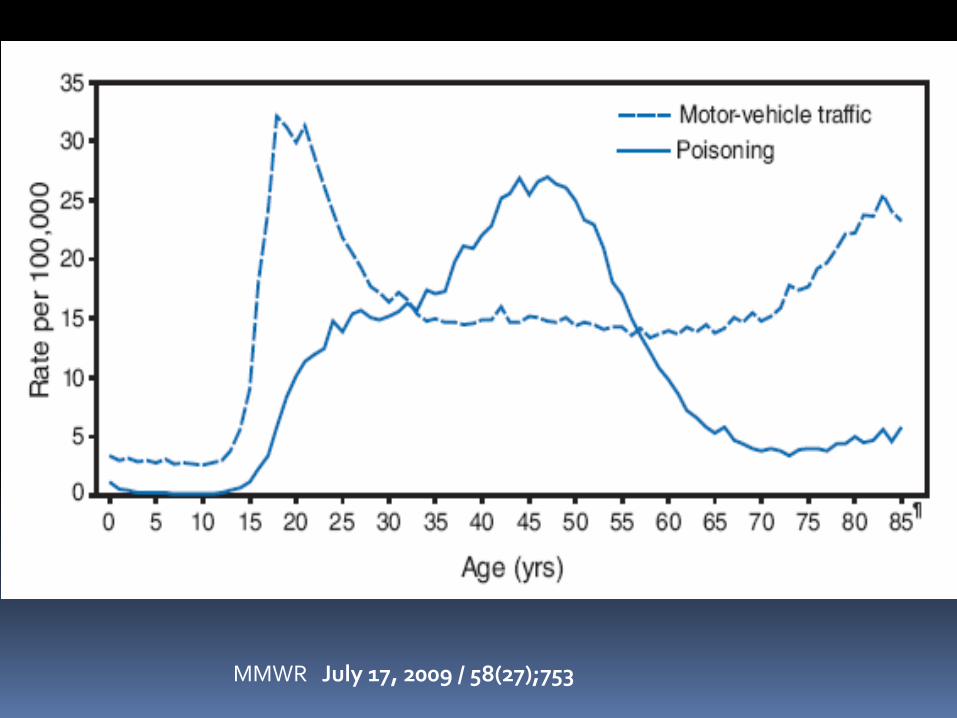
MMWR July 17, 2009 / 58(27);753
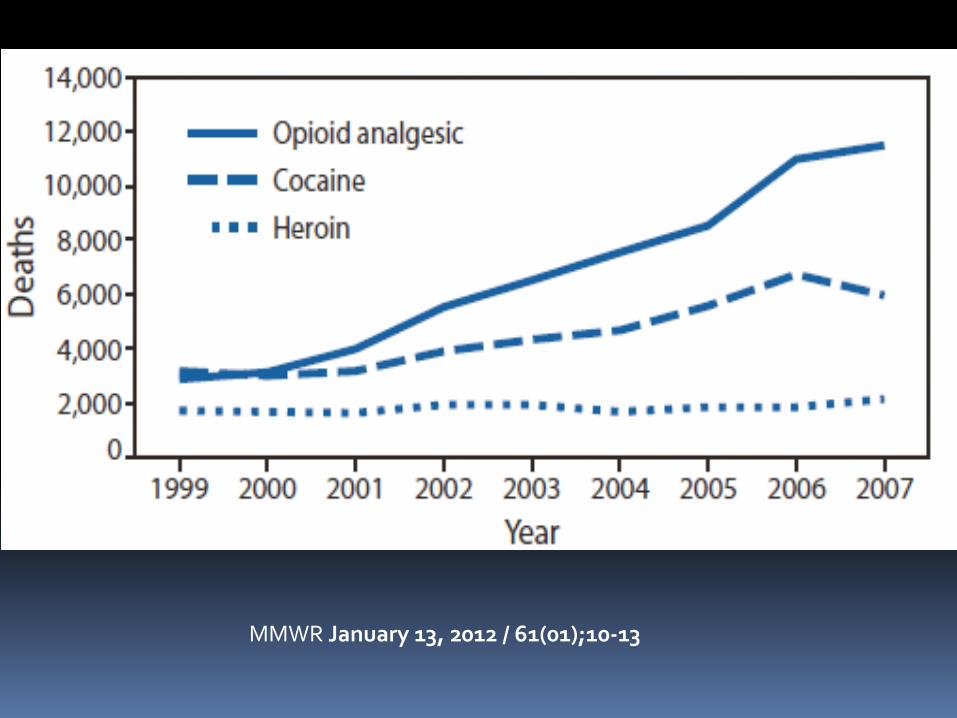
MMWR January 13, 2012 / 61(01);10-13
Why Expertise of CPCS matters:
NONTOXIC Nail polish Oil of Olay Barium sulfate Hair conditioner
TOXIC Nail glue remover Oil of wintergreen Barium chloride Hair straightener
Child ingestion
A 30-month-old, previously healthy and active toddler had two vomiting episodes that the parents believed to be due to an intestinal virus.
Later that day , the child was pale, weak and continued to vomit, resulting in a presentation to the emergency department.
At the hospital, the child was diagnosed with dehydration, and an X -ray revealed.....

Child Ingestion
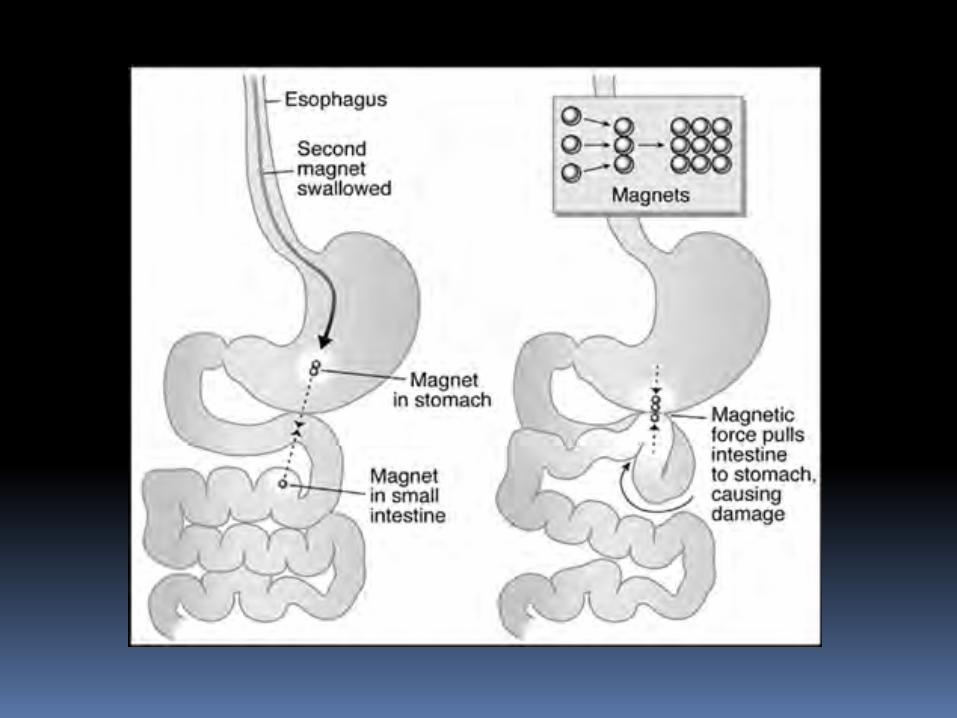
The child developed a fever and abdominal swelling and was taken to surgery, where bowel perforation was found.
The injured bowel was surgically removed. Five days after the operation, the child
suffered a clot in the blood supply resulting in small intestine ischemia. In the operating room, the child was found to have a large area of dead bowel
Emergency Department Presentation 32 yo black female PMH of depression, remote suicide attempt,
obesity, chronic pain Meds: two antidepressants and two narcotics
and klonopin Arrived via 911 call unable to speak but
communicating via writing on paper stating that she had been unable to speak or take her pain meds for 3d and wanted a feeding tube
Had no other complaints
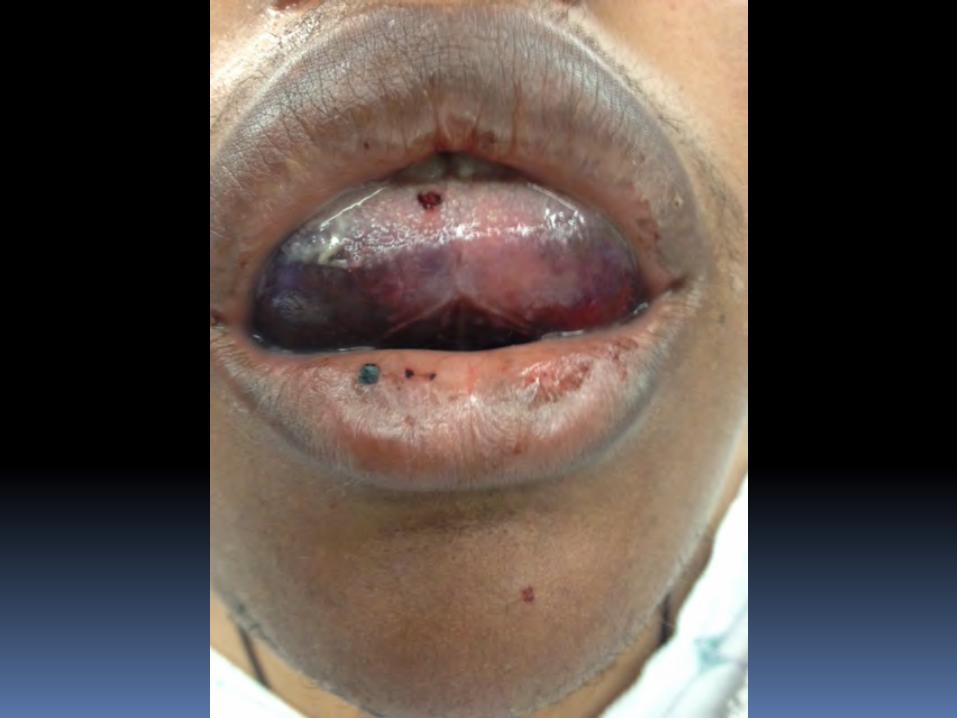
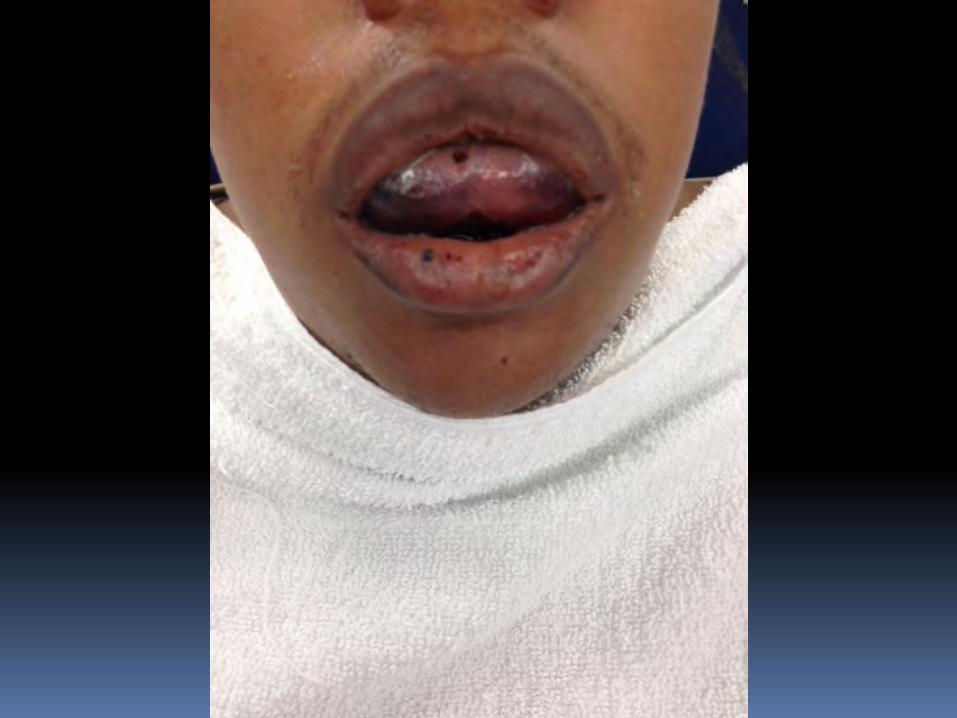
Physical examination
temp 37.0, BP 142/86, HR 98, RR 16, O2 96% RA
Appeared well, no distress Protruding tongue and muffled voice Enlarged chin and anterior neck Lungs clear and unable to examine the oral
cavity, full ROM of the neck Labs – abnl was INR at >13.7, all others
normal
Treatment Course
Immediate – clindamycin, dexamethasone, benadryl, famotadine, considered epinephrine
ENT consultation OR Nasal awake intubation for airway protection FFP, Vitamin K – LOTS In ICU for 2 weeks and transitioned to floor
and discharged on daily vitamin K
Sore Throat Presentation in ED
26 yo female with no PMH presented to the ED with unilateral sore throat for 3d
Progressive fullness on the right side of throat and fever to 101.7
No difficulty with secretions or respirations but odynaphagia
Did have difficulty speaking with muffled voice
Sore Throat Presentation to ED
Patient underwent a PTA aspiration after local use of Hurricaine Spray
Tolerated well and 10cc aspirated At discharge RN comes to NP and states the
discharge vital signs are abnormal with O2 sat at 91% which within 15 minutes becomes 88% and patient is symptomatic and rapidly moved to the resuscitation room.
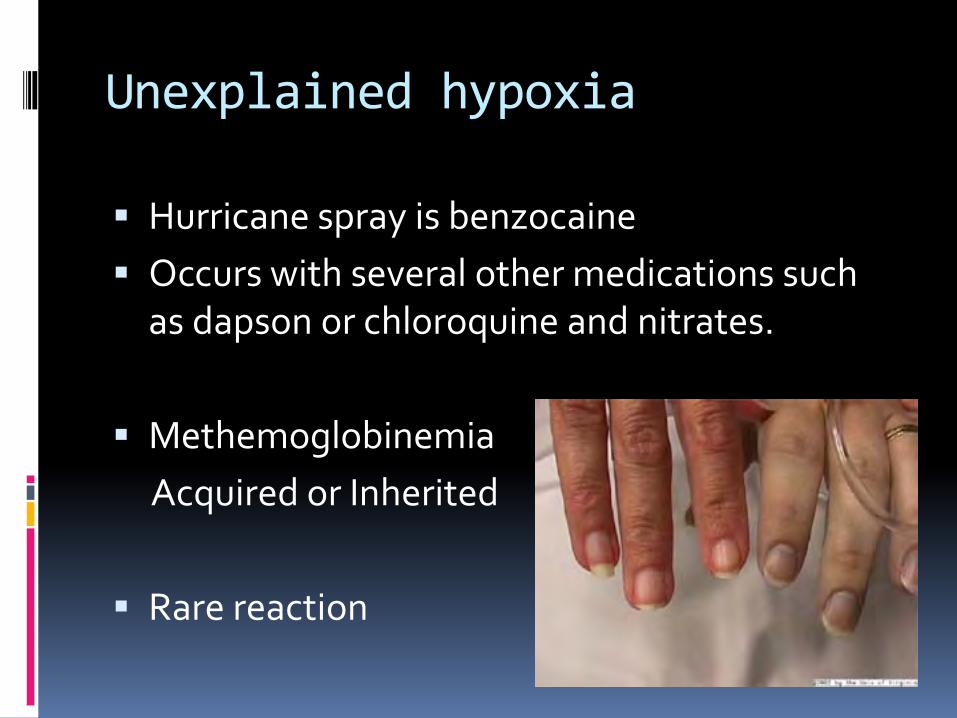
Unexplained hypoxia
Hurricane spray is benzocaine Occurs with several other medications such
as dapson or chloroquine and nitrates.
Methemoglobinemia Acquired or Inherited
Rare reaction


Treatment
Methylene blue – 1-2 mg/kg over 3-5 minutes in 1% NS solution. Repeat every 30 minutes as needed up to 7mg/kg to goal of methemaglobin below 20%. Must have functional G6PD
Ascorbic acid – 500mg/day with Riboflavin 20mg/d. Not a good choice with renal stone Hx
Hyperbaric oxygen therapy or exchange infusions
Lithium Ingestion
Homeless male 34 with PMH of ETOH abuse and depression
Presented intoxicated and unable to walk, well known to ED, similar presentation
Usual observation and resident did no labs or ETOH level
Returned within 8 hours via ambulance ataxic with slurred speech
Renal clearance imperative and competes with other medications
Lithium level has a very narrow therapeutic window 0.6 to 1.5meq/l. Patient’s was 2.8
Lithium Overdose
Overdose symptoms are generally GI related but include weakness and dizziness
These are followed by neurological symptoms such coma, dysarthria and dysmetria, and uncontrolled eye movements
If only GI symptoms then usually reversible but if neurological symptoms develop, they can be irreversible.
Lithium Overdose
TREATMENT Time to treatment may warrant activated
charcoal IVF and dialysis Gastric lavage is used less often and only if exact
time and amount of ingestion is known Symptom management of nausea
Tylenol Overdose 3 phases of tylenol toxicity over a 3-5 day
period Despite the serious liver damage and hepatic
failure, full recovery of hepatic function is possible with prompt treatment
Children are more likely to have early symptoms and vomit after ingestion making toxicity less likely but mimics other GI illnesses
Tylenol overdose
Important to understand how drugs are metabolized
Normal metabolism involves 95% conjugation and then 5% cytochrome 450 enzyme system oxidation in the liver.
Normally involves the conversion to toxic N-acetyl-p-benzoquinoneimine via cytochrome P450 system but overdose overwhelms glutathione stores.
Tylenol overdose
Toxicity in adults vs children >10grams (20 extra strength tylenol tabs) >200mg/kg in children
Time from ingestion to treatment is important as influences effectiveness of therapy and hepatic recovery
If ingestion is considered and many hours after ingestion, treatment is indicated as laboratory studies are pending
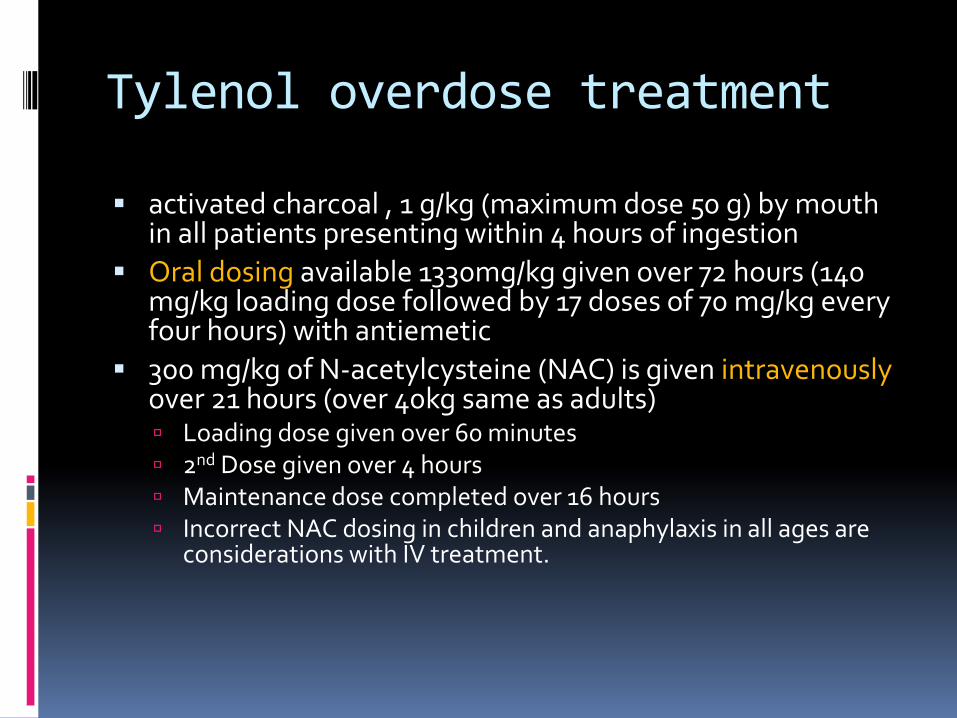
Tylenol overdose treatment
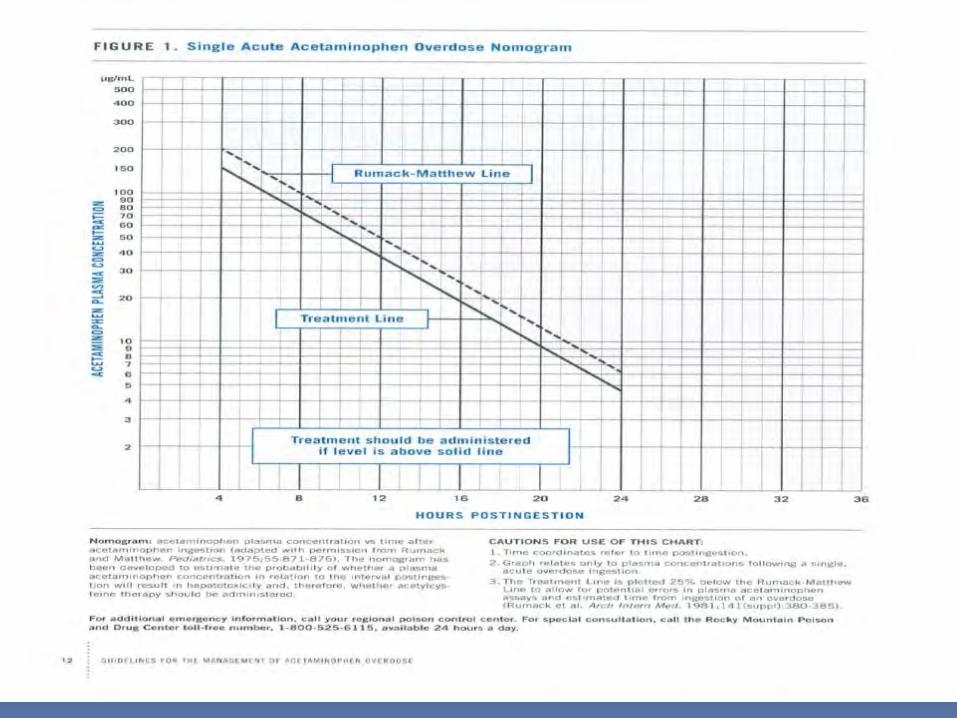
activated charcoal , 1 g/kg (maximum dose 50 g) by mouth in all patients presenting within 4 hours of ingestion
Oral dosing available 1330mg/kg given over 72 hours (140 mg/kg loading dose followed by 17 doses of 70 mg/kg every four hours) with antiemetic
300 mg/kg of N-acetylcysteine (NAC) is given intravenously over 21 hours (over 40kg same as adults) Loading dose given over 60 minutes 2nd Dose given over 4 hours Maintenance dose completed over 16 hours Incorrect NAC dosing in children and anaphylaxis in all ages are
considerations with IV treatment.
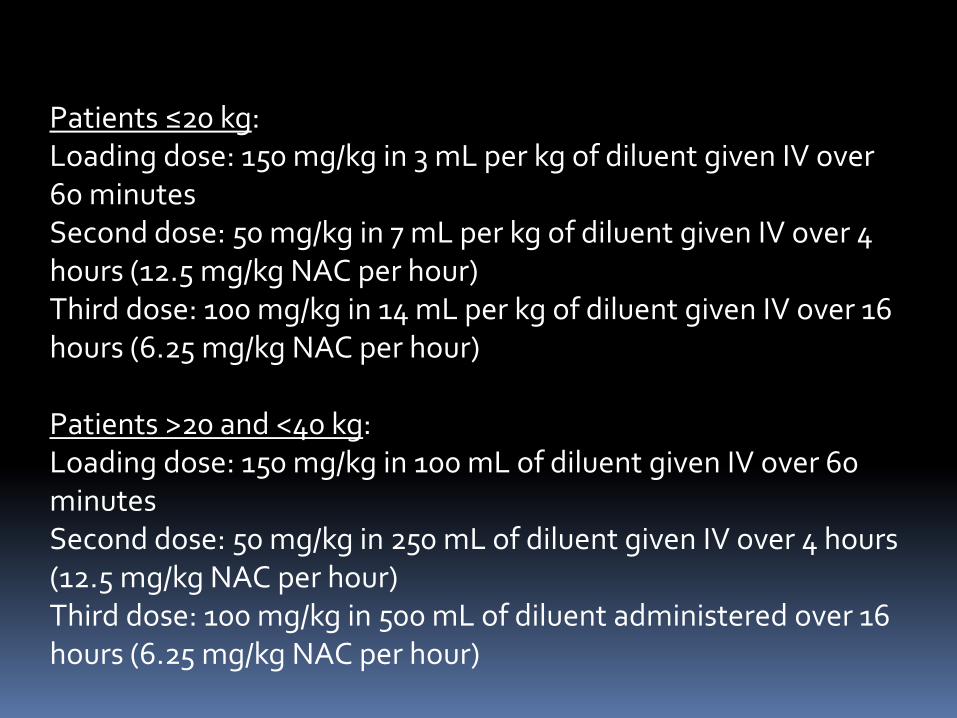
Patients ≤20 kg: Loading dose: 150 mg/kg in 3 mL per kg of diluent given IV over 60 minutes Second dose: 50 mg/kg in 7 mL per kg of diluent given IV over 4 hours (12.5 mg/kg NAC per hour) Third dose: 100 mg/kg in 14 mL per kg of diluent given IV over 16 hours (6.25 mg/kg NAC per hour) Patients >20 and <40 kg: Loading dose: 150 mg/kg in 100 mL of diluent given IV over 60 minutes Second dose: 50 mg/kg in 250 mL of diluent given IV over 4 hours (12.5 mg/kg NAC per hour) Third dose: 100 mg/kg in 500 mL of diluent administered over 16 hours (6.25 mg/kg NAC per hour)
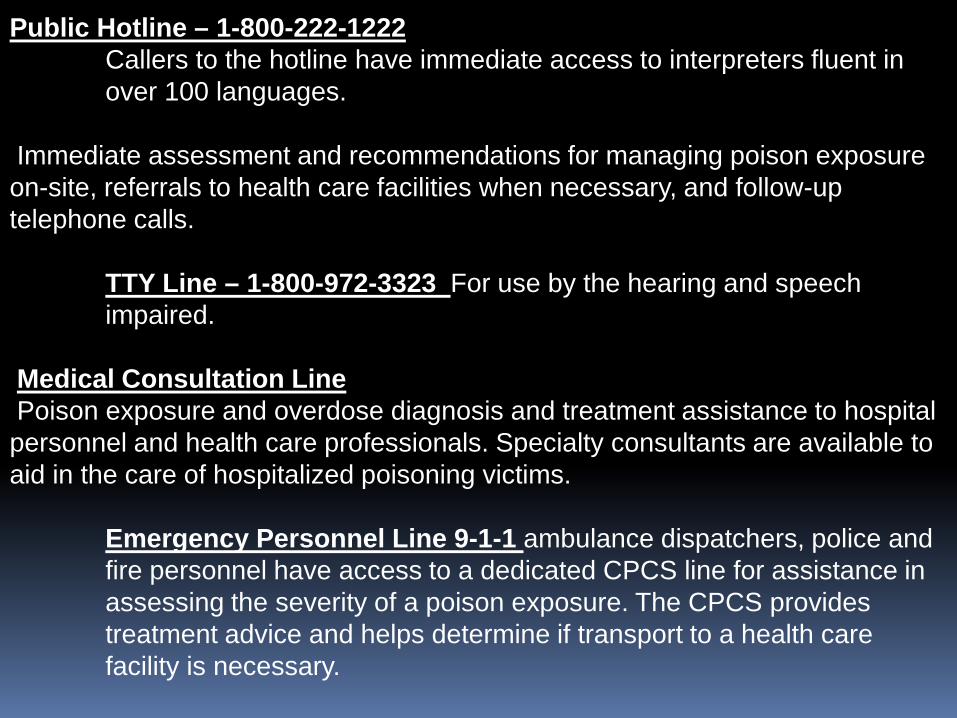
Public Hotline – 1-800-222-1222 Callers to the hotline have immediate access to interpreters fluent in over 100 languages. Immediate assessment and recommendations for managing poison exposure on-site, referrals to health care facilities when necessary, and follow-up telephone calls. TTY Line – 1-800-972-3323 For use by the hearing and speech impaired. Medical Consultation Line Poison exposure and overdose diagnosis and treatment assistance to hospital personnel and health care professionals. Specialty consultants are available to aid in the care of hospitalized poisoning victims. Emergency Personnel Line 9-1-1 ambulance dispatchers, police and fire personnel have access to a dedicated CPCS line for assistance in assessing the severity of a poison exposure. The CPCS provides treatment advice and helps determine if transport to a health care facility is necessary.

Newer Drugs
Pradaxa No known antidote Treat with FFP, Vit K, Bebulin and hope for the
best