Embed Size (px)
Citation preview

D-R12? 823 DEPRECIATION ACCOUNTING IN THE UN4IFORM CHART OF 1/2ACCOUNTS(U) NAVAL POSTGRADUATE SCHOOL MONTEREY CAC L GEORGE DEC 82
UNCLASSIFIED F/G 6/ N
smhohhhhhhhiEsmhhhhhhhhhhhsmhhhhhhhhhhh

-. , . 0
'.8
NATIONAL BUREAU OF STANDARDS- 963-A
EL 3,6
o. oH - I ' ,20"'i:- ' :-..2-.2. '21 .i',: .- , ' " " . .I . ... -i m .

NAVAL POSTGRADUATE SCHOOLMonterey, California
I-
THESIS
DEPRECIATION ACCOUNTING IN THEUNIFORM CHART OF ACCOUNTS
by -%1
Charles Lee George
Lj~j
December 1982
Thesis Advisor: Shu S. Liao
Approved for public release; distribution unlimited
.* -

ISCUSIY CLASSIFICATION OF THIS PA4E9 (91i 0490 too~) _________________
REPORT DOCMENTATION PAGE REA ISTcrTONS
I EON UME 1 Govi ACCEMN 00. S. 011CIPIENTYS CATALOG NuMBE -O
4. TTLE Awd ubtlft)S. TYPE or RE PORT a PE*IoO CovIERWO
Master's Thesis;Depreciation Accounting in the Uniform Dembr18Chart of Accounts .PSOiwON.EORlumm
- . AUTHOR.*) 6. CONTRACT 001 GRANT 61,.,MgER(s)
Charles Lee George
9. PERFORMING OR1GANIZATION MNZM ANO ACRS 10SPOGAM EONE UNT.VE TAUISK
Naval Postgraduate SchoolMonterey, CA 93940
II. CONTROL.LING OFFICE NAME NAWOg$ 15352. REPORT OAT9
Nava Potgrduat ScoolDecember 1982Nava PosgrauateScholIS. HNGER OF PAGES
Monterey, CA 9394010-U- MONITORING AGENCY NAME A ADOOUESIIf aIlem.00 Itai Cottallf~E 0#1190 IS. SECURITY CLASS. (011110 fte l)
UNCLASSIFIED
III& OICL ASSI PICATI ON/ 00111IGRAOIGuSCHEDOULE
I14. CISYSSeUUION STATEMENT (feDho lAeatt)
Approved for public release; dii--ribution unlimited.
17. OISTRI@UTI@M STATEMENT (ofIA the ac 09 ,001d 1a91 16111 20. 1#iteue . ~~u
19. SUPPLEMENTARY NOTES
1S. KEY 30505 (CIa"1140 an po.,r.. sideo ics ear me fgemett aSP &I** RVRW3
Health Care Hospital Cost AccountingHospital Financial ManagementDepreciation AccountingUniform Chart of Accounts
20. ASITACT (CORehe ON POWrne ede It .eeS mi600 M~.d D A? 55.* '"Mawe)
This paper examines depreciation's contribution to the totalcost of providing health care. In particular it analyzes thedepreciation method used to measure the consumption of health
4care resources, the validity of the depreciation process and6 .4 the subsequent allocation procedures. As defined by the Uniform
Chart of Accounts, the usefulness of depreciation in determiningthe total cost of providing health care is attenuated by the
fact that a major portion of a facility's capital assets are
DD I A11 1473 'NOV 63o oIevsois ODIOL 113T
1 gCUQJTV CLASSIFICATION OF T"08S PAOErm maSnm

20. (continued)
excluded from the depreciation process, the rate of depreciationunderstates the estimated useful service life of the assets,double counts certain expenses, and makes no provisions toperiodically evaluate and adjust the composite rate ofdepreciation.
Comparisons are made between depreciation accounting in themilitary health service system and the civilian health caresector. Issues raised with the implementation of depreciationaccounting within the Uniform Chart of Accounts are addressedand recommendations are made that may enhance the usefulness ofthe depreciation methodology.
Accession ForNTIS GRA&IDTIC TABUnannouncedJustification
" - ByDistribution/
Availability Codes
Avail ard/orDi Special
o .j
Ai
O"SPECTWO2M
*DD Foria 1473MS.an gI.i01%2-nl4-66n1 SIU81TV €&LuoPoCAIPoU or vil$ PaGuAM&A owe 614,o.*e

Approved for public release; distribution unlimited
Depreciation Accounting in theUniform Chart of Accounts
by
Charles Lee GeorgeLieutenant, Medical Service Corps, United States Navy
B.S., College of Charleston, 1978
Submitted in partial fulfillment of therequirements for the degree of
MASTER OF SCIENCE IN MANAGEMENT
from theNAVAL POSTGRADUATE SCHOOL
December 1982
Author: / - --,
Approved by: _ _ _ _ ___ _
Thesis Advisor
Chairman, Department of istrative Sciences
Dean of Information and Policy Sciences
3

ABSTRACT
--- This paper examines depreciation's contribution to the
total cost of providing health care. In particular it analyzes
the depreciation method used to measure the consumption of
health care resources, the validity of the depreciation pro-
cess and the subsequent allocation procedures. As defined by
the Uniform Chart of Accounts, the usefulness of depreciation
in determining the total cost of providing health care is at-
tenuated by the fact that a major portion of a facility's
capital assets are excluded from the depreciation process,
the rate of depreciation understates the estimated useful
service life of the assets, double counts certain expenses,
and makes no provisions to periodically evaluate and adjust
the composite rate of depreciation.
Comparisons are made between depreciation accounting in
the military health service system and the civilian health
care sector. Issues raised with the implementation of
depreciation accounting within the Uniform Chart of Accounts
are addressed and recommendations are made that may enhance
the usefulness of the depreciation methodology.
.....

TABLE OF CONTENTS
I. INTRODUCTION------------------------------------------ 7
A. BACKGROUND---------------------------------------- 7
B. PURPOSE OF THESIS-------------------------------- 9
C. RESEARCH METHODOLOGY----------------------------- 10
D. THESIS ORGANIZATION------------------------------ 10
II. DEPRECIATION METHODOLOGY----------------------------- 12
A. FACTORS AFFECTING DEPRECIATION------------------ 1
B. METHODS OF DEPRECIATION------------------------- 1
C. GENERAL PRICE LEVEL EFFECT ONDEPRECIATION EXPENSES---------------------------- 24
III. DEPRECIATION METHODOLOGY USED BY CIVILIANHOSPITALS AND BY THE MILITARY MEDICALDEPARTMENT-------------------------------------------- 27
A. INTRODUCTION------------------------------------- 27
B. DEPRECIATION METHODOLOGIES USED BYCIVILIAN HOSPITALS------------------------------- 28
C. DEPRECIATION EXPENSE UNDER THE UCA-------------- 31
D. PROPERTY SUBJECT TO DEPRECIATION---------------- 31
E. DEPRECIATION EXPENSE ALLOCATION----------------- 34
F. CONCLUSION--------------------------------------- 34
IV. A CRITICAL ANALYSIS OF UCA DEPRECIATIONMETHODOLOGY AND RECOMMENDATIONS---------------------- 36
A. INTRODUCTION------------------------------------- 36
B. ASSUMPTIONS UNDERLYING THE UCA
DEPRECIATION METHODOLOGY------------------------- 37
C. UNIFORM CHART OF ACCOUNT'S DEPRECIATION:IS IT SYSTEMATIC AND REASONABLE?---------------- 41
5

D. DOES THE CURRENT UCA METHOD OF DEPRECIATIONALLOW MEANINGFUL COST COMPARABILITY AMONGMILITARY MEDICAL TREATMENT FACILITIES ANDWITH THE CIVILIAN HEALTH SECTOR?------------------ 47
E. IS THE UCA. DEPRECIATION REQUIREMENT SORESTRICTIVE AS TO MINIMIZE THE EFFECT OFDEPRECIATION ON THE TOTAL COST OFPATIENT CARE--------------------------------------- 51
F. CAN DEPRECIATION'S CONTRIBUTION TO TOTALCOST OF PATIENT CARE BE ISOLATED IN ORDERTHAT MANAGEMENT DECISIONS WILL NOT BEINFLUENCED BY SUNK COSTS?-------------------------- 53
G. CONCLUSION------------------------------------------ 54
V. RECOMMENDATIONS FOR CHANGES TO UCA
DEPRECIATION-------------------------------------------- 57
A. INTRODUCTION--------------------------------------- 57
B. RECOMMENDATIONS------------------------------------ 58
VI. SUMMARY AND CONCLUSION--------------------------------- 68
A. SUMMARY--------------------------------------------- 68
B. CONCLUSION------------------------------------------ 71
APPENDIX A: UNIFORM CHART OF ACCOUNTS FOR FIXEDMILITARY MEDICAL AND DENTAL TREATMENTFACILITI'FS-------------------------------------- 74
APPENDIX B: STATISTICAL ANALYSIS OF THE UNIFORMCHART OF ACCOUNTS COMPOSITE RATE OFDEPRECIATION------------------------------------ 89
LIST OF REFERENCES-------------------------------------------- 99
INITIAL DISTRIBUTION LIST------------------------------------ 102
*66

I. INTRODUCTION
A. BACKGROUND
outlays for health care in the nation reached approximately
$192.4 billion for the calendar year 1978 (Ref. 1]. This
represented approximately 9.1% of the Gross National Product
and amounted to approximately $863 per capita expenditure
[Ref. 11. Since 1965 health care costs have grown at an
average of 12.2% per year while prices in the economy as a
whole have grown at a 9.0% annual rate. This imbalance has
given rise to several attempts to control hospital costs either
by fiat (Economic Stabilization Act) or through the enactment
of federal laws such as the Health Maintenance Organization
Act of 1973, P.L. 93-222 or the Nstional Health Planning Act
of 1974, P.L. 93-641. By the end of 1980 the cost of health
care is estimated to be approximately 10% of the Gross Na-
tional Product.
The Department of Defense has not escaped the effect that
rising costs have had on the delivery of health care. Donald
Rice (Ref. 2] has estimated that during the period of 1967
through 1978 health care costs were rising at a rate of 30%
per year. The effect of these escalating health care costs
became more acute as the post-Vietnam military budget was
reduced in size and the purchasing power of the dollar was
eroded by inflation and the significant increases in weapons
system and personnel cost.
7
UA

Anticipating the squeeze that would be placed on the
military health care dollar the Department of Defense, Office
of Management and Budget, and Department of Health, Education
and Welfare, acting on a presidential mandate, initiated a
joint study of the military health care system in 1973.
The study was concluded in 1975 and was generally compli-
mentary toward the military health service system (MHSS). Not
only did the study show that the MHSS provided a broad spec-
trum of medical services to more than nine million beneficiaries,
but it demonstrated that the MHSS was capable of responding to
a variety of military and civil emergencies. However, it did
conclude that a number of opportunities existed to improve the
effectiveness and efficiency of the MHSS while maintaining the
delivery of quality health care to eligible beneficiaries
[Ref. 3].
Of the nine major recommendations outlined, one poisted
the need for a uniform medical data system within the three
military services. This recommendation led to the develop-
ment of a Department of Defense Uniform Chart of Accounts (UCA)
[Ref. 4]. The UCA was designed to record accumulate and re-
port information regarding the expense and workload within
military treatment facilities as a means of determining the
total cost of treating a patient. Among the benefits that
are expected to accrue to the MHSS by using the UCA are:
(1) enhanced cost awareness, (2) cost effectiveness evalua-
4 tion, (3) more effective decision-making when cost or
8d..

performance is a factor, and (4) better comparison among
military medical facilities and with the civilian health
sector (Ref. 41.
Appendix A contains an expanded explanation of the Uni-
form Chart of Accounts. The UCA is composed of six operating
expense accounts, two intermediate and four final. It is the
intermediate Support Service account that is of particular
relevance to this thesis. It is within this account that the
depreciation expense associated with military medical facili-
ties capital assets are accumulated and eventually allocated
to other support and mission centers.
B. PURPOSE OF THE THESIS
The purpose of this thesis is to analyze the issues con-
-fronting asset depreciation in the Naval Health Service System
(NHSS).
1. Issues
a. Does the current UCA method recognize deprecia-
tion expenses in a systematic and rational manner?
b. Does the current UCA method of depreciation allow
meaningful cost comparability among military medical treat-
ment facilities and with the civilian health sector?
c. Is the UCA depreciation requirement so restric-
tive as to minimize the affect that depreciation has on the
total cost of patient cazq?
9
*" - .'i , . 2 2 :; '". -. .. i , •. ..

d. Can depreciation's contribution to the total cost
of patient care be isolated in order that management decisions
will not be unduly influenced by a sunk cost?
C. RESEARCH METHODOLOGY
Thesis research methodology included a literature search
to identify the types of depreciation commonly used in the
health care industry, and interviews with civilian and mili-
tary health care administrators to identify their views on
depreciation accounting and each associated facility's used
depreciation accounting. Military directives were reviewed to
determine the basis for depreciation accounting. Statistical
analysis of plant account records from selected Naval Regional
Medical Centers was done to determine whether the assets shared
common features such as service lives and similar populations.
D. THESIS ORGANIZATION
The remainder of the thesis will be arranged as follows:
Chapter Two will discuss two types of depreciation
employed by business and industry in the private sector:
Straight-line (to include unit and composite rates) and ac-
celerated depreciation. Examples of each depreciation pro-
cedure will be given along with a synopsis of depreciation
methods used by four civilian medical organizations.
Chapter Three will be a comparison and analysis of
depreciation methods used by civilian hospitals and in the
Uniform Chart of Accounts.
10
i1 m m ~''i l kt -i lnml h i . . ' '

*Chapter Four will be a critical analysis of UCA
* depreciation.
Chapter Five will contain recommendations for changes
to the UCA depreciation methodology.
Chapter Six will summarize and conclude the thesis.
a
11
I

II. DEPRECIATION METHODOLOGY
The comparability of depreciation expenses among military
medical treatment facilities and between military medical
treatment facilities and the civilian health care sector can
be greatly influenced by the method of depreciation chosen,
depreciable base used and the estimated useful life of the
assets involved. In order to adequately evaluate the issues
surrounding depreciation and the subsequent use of the computed
expense, an understanding of the effect different depreciation
methods have on cost allocation would be helpful.
Therefore, this chapter will be concerned with describing
the various methods of depreciation and the effect these
methods have on the allocation of an asset's cost. It will
cover factors affecting depreciation, as well as discuss the
accelerated and straight-line method of depreciation. An il-
lustration of the effect various depreciation methods have on
cost allocation will be given, as well as briefly discussing
the effect that changes in the general price level have on
depreciation expense. It will also discuss the depreciation
method used by the Civilian Health Sector.
A. FACTORS AFFECTING DEPRECIATION
Accounting for the consumption of long-lived assets under
the accrual basis of accounting is done through a process of
6 depreciation. Depreciation is an accounting procedure by
12

which the cost (less salvage value -if any) of fixed assets
are allocated to expenses over the estimated useful lives of
such assets in a systematic and rational manner; it is a
process of cost allocation, not valuation. [Ref. 51
The estimation of depreciation is dependent on three
variables: Service life, depreciation base, and method of
cost apportionment. The service life of an asset is the total
units of service expected to be derived from that asset
(Ref. 5]. Arriving at the total units of service involves
* choosing the appropriate unit in which service life is to be
measured and then estimating how many units of service are
embodied in each asset. This usually involves estimating the
causes of the decreases in asset service and can generally be
divided into two classes: physical causes and function/
economic causes. Decreased asset service brought about by
physical deterioration results largely from wear and deteriora-
tion over time. These physical forces terminate the useful-
ness of plant items by rendering them incapable of performing
the service for which they were intended and thus set maximum
limit on service life (Ref. 5]. Functional depreciation on
the other hand arises from obsolescence or inadequacy of the
asset to perform effectively. Obsolescence may arise when
there is no further demand for the product that the depre-
ciable asset produces, or the same function for substantially
less cost. Inadequacy on the other hand refers to the effect
that growth and changes in the scale of a facility's operations
13

have on the termination of the asset's service life [Ref. 6].
For example, an x-ray processor may be in sound condition, but
if greater processing capacity is required which cannot
economically be provided by modifying the current machine,
the old machine has become inadequate and its economic service
life to the hospital is ended. Generally, any asset is
inadequate whose capacity is such that it cannot be operated
with optimum results, or whose capacity does not or cannot
fit the requirements of the organization [Ref. 6].
The second variable that must be considered is that por-
tions of the depreciations base that should be charged against
revenue during its service life. The depreciable base should
include all normal expenditures of readying an asset for use
and should consider the salvage value that may be realized at
* the end of the asset's useful life. Frequently, depreciable
assets have little or no salvage value at the end of their
estimated useful life and, if immaterial, the amount(s) may
be ignored [Ref. 61.
B. METHODS OF DEPRECIATION
The goal of depreciation should be to provide a reason-
* able, consistent matching of revenue and expenses by systemat-
ically allocating the cost of the asset over its estimated
useful life [Ref. 71. The most commonly encountered methods
in hospital accounting that attempt to accomplish this alloca-
tion are: straight-line depreciation methods (unit and group)
and accelerated depreciation. These methods differ in that
14

depreciation under the unit straight-line and accelerated
methods is a function of time, whereas depreciation under
the group method is based on a weighted-average of the
service lives of the assets involved [Ref. 7].
1. Straight-line Depreciation
a. Unit straight-line: The distinguishing character-
istic of the unit straight-line method is that an equal por-
tion of an individual asset's acquisition cost is allocated
to each year of service life. The annual portion of the
depreciation expense is computed in the following manner:
Depreciation Expense Acquisition Cost - Salvage Value
Number of years in the service life
Another distinguishing feature of calculating depreciation
expense for a unit depreciation schedule is that the decrease
in assets useful life is constant over time. A principal
advantage of the unit method is that it is simple to apply
and it may result in a reasonably accurate measure of an
asset's use. On the other hand, the objections to the
straight-line method center around economic productivity and
income measurement. Part of the controversy is that a con-
stant depreciation charge for each operating period does not
reflect variations in the rate of asset use and may accentuate
fluctuations in net income. Another objection to this method
is that for a given asset producing relatively constant earn-
ings each period, the use of the straight-line method will
show an increasing rate of return on the unrecovered
15Io

investment during each period of service life. Furthermore,
a constant depreciation charge overstates an asset's economic
productivity by not considering the fact that productivity
declines sharply as the asset ages [Ref. 8].
b. Composite and group depreciation are forms of
straight-line depreciation that are used when an organization
finds it expedient to account for depreciation on a group
basis rather than as individual assets. The term composite
usually refers to a collection of dissimilar assets; while
group depreciation refers to depreciating a collection of
similar assets. In either case, they are processes of averag-
ing the service life of a number of property units and then
taking depreciation on the entire lot as if it were an operat-
ing unit. A distinguishing feature of a composite or group
depreciation rate is that once the rate is computed, it is
continued in use until there is a material change in either
the composition of the assets or in the assets service lives
[Ref. 9].
Basic assumptions underlying the use of a com-
posite or group depreciation method are:
(1) Assets are regularly retired near the endof their service lives.
(2) Assets are replaced with similar assets.
(3) Proceeds on retirement are approximatelyequal to the estimated salvage value [Ref. 91.
16o.

"" 2. Accelerated Methods of Depreciation
The assumption that plant assets yield either a greater
quantity of service or more valuable services in early years
of service life has led accountants to devise methods of de-
preciation that will result in large amounts of depreciation
being recognized in the early years of the asset's service
life, and smaller amounts in later years (See Figure 1)
[Ref. 91. There are a number of different approaches that
can be used to compute an accelerated depreciation rate.
Only three will be dealt with in this thesis. These methods
are: fixed percentage of declining balance, double-declining
balance, and the sum-of-the-years-digits.
a. Fixed-percentage-of-declining balance method
computes a percentage depreciation rate which when applied
to the book value of the asset at the beginning of each
period, will result in writing the asset down to its estimated
net salvage value. The computed depreciation rate is applied
on a consistently declining asset value. The amount of de-
preciation expense decreases each year. The formula for
computing the required rate is:
n~et Salvage Value
Depreciation Rate =1- bAcquisition Cost
n = years of service life
17
-

A net salvage value greater than
zero must be estimated.
Example: Asset acquisition cost is $15,000
Net salvage value is $1,500
Service life is 5 years
5 $1,500
Depreciation Rate =1- $15,000
= 1 - .63
= .37
b. Double-declining-balance method uses a rate that
is twice the straight-line method (Ref. 9]. For example, an
asset with a five year service life would have a double-
declining rate of 40%, computed as follows: 2/n where n
equals the asset's service life in years. The one limiting
factor is that the asset can not be depreciated below its
estimated net salvage value. Taking for example an asset
with an acquisition cost of $15,000, a salvage value of
$1,500 and a service life of 5 years, the double declining
rate would be 40%. The depreciation expense in Year 4 would
be $1,269 and the book value of the asset would be $1,944.
Therefore, in Year 5 the maximum depreciation that could be
taken would be $544, reducing the asset's book value to the
estimated net salvage value floor of $1,500.
c. Sum-of-the-years-digits method computes a decreas-
ing depreciation expense by a simple mathematical procedure
relating to arithmetic progression [Ref. 61. The sum of a
18

series of numbers representing the years of service life
becomes the denominator of the depreciation fraction for any
one year. The formula for determining the denominator of the
depreciation fraction for an asset with a 5 year service life
is: n(n + 1)/2, where n equals the service life in years-
5(5 + 1)/2 = 15. The number of years of the asset's esti-
mated service life is the numerator for the depreciation
fraction in the first year. In each succeeding year the
numerator is reduced by one, until in the last year the de-
preciation fraction becomes a reciprocal.
The depreciation expense for an asset with an
estimated service life of 5 years in the first year would be
5/15 of the depreciable base and in Year 5, 1/15 of the base
would be credited to the accumulated depreciation account.
Since the denominator is constant and the numerator declines
each year, the result is a decreasing depreciation charge.
Because the total of the numerators of the depreciation frac-
tion equals 1, 100% of the depreciable base will ultimately
be charged to expense [Ref. 7].
3. Comparison of Different Methods
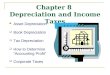
Figure 1 and Tables 1, 2 and 3 illustrate the effect
that the foregoing depreciation methods have on the magni-
tude and timing of depreciation expense. Table 1 shows that
by using the straight-line method, each year of service life
absorbs an equal portion of the acquisition cost. The book
value at the end of the fifth year equals the estimated
salvage value.
19

- .!~ •....- . . . ... ... . .. , .
Figure 1K Graphic Uisplay
of the timing ofDepreciation ExpensesShown in Fiure 1
100 Straight-Line 100 Fixed Percentage
of a
Declining Balance
50 50
1 2 3 4 5 1 2 3 4 5
(A) (B)
100 100
Sum-Of-The Double-Declining
. Years Digits Balance
50 50
1 2 3 4 5 1 2 3 4 5
(C) (D)
20

Table 1
Asset: Blood Chemistry Auto Analyzer
Acquisition Cost: $200,000
Salvage Value: $ 10,000
Service Life: 4 years
Sum of Double Fixed %
Service Straight the Years Declining of Declining
Year Line Digits Balance Balance
1 Dpr Exp $ 38,000 $ 63,333 $ 80,000 $ 90,144
Book Vl $162,000 $136,667 $120,000 $109,856
2 Dpr Exp $ 38,000 $ 50,667 $ 48,000 $ 49,514
Book Vl $124,000 $ 86,000 $ 72,000 $ 60,342
3 Dpr Exp $ 38,000 $ 38,000 $ 28,800 $ 27,197
Book Vl $ 86,000 $ 48,000 $ 43,200 $ 33,145
4 Dpr Exp $ 38,000 $ 25,333 $ 17,280 $ 14,939
Book V1 $ 48,000 $ 22,667 $ 25,920 $ 18,206
5 Dpr Exp $ 38,000 $ 12,667 $ 10,368 $ 8,206
Book Vl $ 10,000 $ 10,000 $ 15,552 $ 10,000
a
21
..

Table 2
Composite Depreciation Methods
Acquisition Service = Depreciation
Asset Cost Life(Yrs) Expense
Surgical Instrument
Cabinet $ 1,331 20 $ 66
Electrosurgical
Apparatus $ 13,032 8 $ 1,629
Surgical Table
(Remote Control) $ 8,910 15 $ 594
Carniotomy Table $ 1,390 15 $ 93
Telemetry Monitor $ 5,100 7 $ 728
Physiological Sys
Monitor (ICU) $ 85,000 7 $ 12,143
Coloson - 53 Pediatric
Stretcher $ 4,242 15 283
Double Pedestal
Desk $ 1,003 20 50
Total $120,008 $ 15,586
Composite rate equals: $15,586/$120,008 = 12.9%
22
,4

Table 3
Group Depreciation, Methods
Asset Qtv Unit Cost Total Cost Serv Life
* . Wheeled Hospital
Stretcher 27 $2,500 $67,500 15
Under the group method this group of assets would contri-
bute $67,500/15 =$4,500 annually as a unit to depreciation
expense.
The composite depreciation rate is 12.9%, with a composite
life of 6.8 years. Therefore 12.9% of the total acquisition
cost of this dissimilar group of assets, or $15,586, will be
expensed each year so that in 6.8 years the accumulated de-
preciation amount will equal the composite book value amount.
23

The sum-of-the-years-digit method allocates a larger
portion of the assets acquisition cost to the early years of
service life. By the end of the fifth year the book value,
like the book value obtained by the straight-line method,
equals the estimated net salvage value.
Using the double-declining method (Table 1), a uniform
* rate is applied to the asset's current book value. Since
book value is always reduced by the preceding year's deprecia-
tion expense, the rate is applied to a constantly declining
book value. As previously mentioned, an asset can not be
depreciated below its estimated salvage value when using the
double-declining-balance method of depreciation.
Depreciation expense computed using the fixed-percent-
age-of-declining-balance method declines sharply after the
first year and decreases at a decreasing rate until at Year
Five the book value approximates the estimated net salvage
value. The sharp decline in the depreciation expense occurs
because the depreciation for each year after Year 1 is only
55% of the preceding year's expense.
C. GENERAL PRICE LEVEL EFFECT ON DEPRECIATION EXPENSES
In 1976 the American Hospital Association (AHA) recom-
mended formally adjusting the plant asset accounts to ieflect
7- the effects of inflation as measured by changes in the general
purchasing power of the dollar. As a means of adjusting the
plant assets account, the AHA suggested using the index of
I
" 2 4

general prices known as the Gross National Product Implicit
* Price Deflator that is published quarterly by the Bureau of
Labor Statistics (Ref. 8].
- - As an example of7 the procedure to adjust for inflation,
assuame that an asset purchased on 1 Jan 1980 at a cost of
$70,000 has estimated life of 5 years and a salvage value of
- . $10,000. The GNP Deflator on 1 January 1980 was 200 and on
31 December 1980 it was 212. The entries to record the price
level change:
General Journal
* .Major Moveable Equipment
Price Level Increment $4,500
Unrestricted Fund Balance
Price Level Reevaluation $4,500
To record general price level increase.
($75,000 x 212/200) = $79,500
Historical Cost = 75,000
Price Level Increase $ 4,500
Depreciation Expense - Price
Level Adjustment
Accumulated Depreciation
Major Moveable Equipment
II Price Level Adjustment $720
25

To record price level adjustment on major moveable
equipment depreciation.
($12,000 x 212/200) $12,720
Historical Dpr Expense = 12,000
Price Level Increase $ 720
Except for those companies that meet the requirements of
the Financial Accounting Standards Board (FASB) Statement 33,
entitled "Financial Reporting and Changing Prices," account-
ing for inflation has not gained the status of a generally
accepted accounting principle [Ref. 6]. The AHA's recommenda-
tion is only a partial approach to the problem of accounting
for the effects of inflation on hospital operations [Ref. 7].
-. However, its use, while not meeting all of the requirements
for a generally accepted accounting principle is suggested
as supplementary information to financial statements [Ref. 7].
2r26
e"

* III. DEPRECIATION METHODOLOGY USED BY CIVILIAN HOSPITALSAND THE MILITARY MEDICAL DEPARTMENTS
* A. INTRODUCTION
Depreciation accounting is a recent occurrence within
the military medical departments. It became an official part
of the accounting and reporting systems in 1979 with the
advent of the Uniform Chart of Accounts (UCA). The accumula-
tion of depreciation expenses is an attempt to account for
the cost of consumption of long-lived fixed assets as an
operating expense over the property's estimated useful life. 1
It is a part of a larger expense collecting system that is
designed to determine the total cost of patient care. The
intent being among other things, to foster an atmosphere of
cost awareness, enhance cost-effective decision making, make
coherent work counts and serve as a gauge by which to make
meaningful comparisons among military medical facilities and
the civilian health sector (Ref. 41.
Depreciation can have a substantial effect on the deter-
.4 mination of the total cost of patient care depending on such
factors as the method of allocation selected, depreciable
base used, and the useful life of the fixed asset. These
* factors can in turn influence the degree of comparability of
1 Fixed assets are defined as those long-lived propertyitems not intended for resale in the regular business of theenterprise. Building and equipment constitute a subclassof the fixed assets category (Ref. 151.
27

the UCA cost figures among the military medical facilities
and between the military and civilian health sectors.
In order to better understand the effect of depreciation
on the cost of patient care and its subsequent effect on
cost comparability, a description of the UCA depreciation
methodology would be helpful. Accordingly, this chapter will
be devoted to describing and analyzing the depreciation
methodology used by civilian hospitals and the methodology
used in the Uniform Chart of Accounts for Military Medical
Treatment Facilities. Depreciation as a cost center within
the Uniform Chart of Accounts will be described along with
the threshold dollar value and type of equipment that con-
tributes to depreciation expense. The basic assumptions
underlying the UCA methodology will be analyzed and an example
will be used to illustrate the procedures used to calculate
the annual UCA depreciation expense.
B. DEPRECIATION MFTHODOLOGIES USED BY CIVILIAN HOSPITALS
The choice of depreciation used by a civilian hospital
depends upon how the depreciation expense is to be used.
Interviews with four civilian hospital finance directors
revealed that depreciation was used to determine income,
rate setting, Third Party reimbursements, cash flow genera-
tion, and for funding of asset replacements. Finance
directors interviewed were from: Kaiser Foundation Health
Plan, Inc., Oakland, CA., Community Hospital of the Monterey
Peninsula, Monterey, CA., Grace Hospital Inc., Morgantown,
28
4l

N.C., and California Hospital Association, Sacramento, CA.
Kaiser Foundation Health Plan is a prepaid group medical
plan, the Community Hospital of the Monterey Peninsula and
Grace Hospital Inc., are not-for-profit community hospitals
while the California Hospital Association administers the
MediCare and MediCal programs in the State of California.
* Kaiser Foundation Health Plan uses either an accelerated
or straight-line depreciation method for any class of
* depreciable assets and either a composite or unit rate method
for moveable equipment (Ref. 10, 11]. Depreciation is used
for two purposes: (1) calculate reimbursement rates and (2)
generate cash flow to meet future capital requirements.
Reimbursement rates receive a portion of the depreciation
expenses based on guidelines set forth by the California
Hospital Association and other Third-Party Payees [Ref. 10].
Funds provided by depreciation help meet future construction
needs. According to Mr. Philip Beretta, Regional Controller
for the Northern Region of the Kaiser Foundation Health Plan,
Kaiser Foundation can borrow approximately 50% of the construc-
tion cost of a new facility. The other 50% must come from
earnings (Ref. 10]. The amount of earning to be generated
by prepaid dues is determined by estimating the total capital
* requirements for a ten year period, subtract funds provided
by depreciation and borrowings during the same period to
arrive at a dollar figure for prepaid dues.
296'

The Director of Finance at the Community Hospital of the
Monterey Peninsula [Ref. 12] uses straight-line depreciation
in accordance with the accounting policies of the California
Hospital Association. The resulting depreciation expense is
used to compute a reimbursement rate.
Grace Hospital Inc., of Morgantown, N.C. [Ref. 13] uses
straight-line depreciation for rate setting, third-party
reimbursement and for funding for the replacement of capital
assets. Grace Hospital Inc. sets aside funds in an amount
equal to the annual depreciation expense to be used to provide
for the replacement of capital assets.
The California Hospital Association stipulates that the
method of depreciation used by hospitals for reporting to the
Association's Health Facilities Commission must be straight-
line depreciation method for all assets purchased after June
30, 1974 [Ref. 14]. If hospitals in California use a dif-
ferent method for accounting purposes, all timing differences
created by the difference between accounting and reporting
must be reflected in reports to the Health Facilities
Commission. The corresponding depreciation figure(s) is/are
used in determining reimbursement rates [Ref. 14].
Grace Hospital Inc. [Ref. 13] uses straight-line deprecia-
* tion for rate setting, third-party reimbursement and for
funding of capital assets replacement.
In selecting a method of depreciation, each hospital first
decides the purpose for which depreciation will be used, then
30

the hospital selects the appropriate depreciation method.
Straight-line depreciation was generally selected for rate
setting and reimbursement. Accelerated depreciation was
generally selected for cash flow and tax purposes.
C. DEPRECIATION EXPENSE UNDER THE UCA
Depreciation expenses under the UCA are computed using a
form of depreciation similar to the composite rate methodology.
Essentially the UCA method considers all equipment to have a
useful service life of eight years and that all equipment
subject to depreciation is fully depreciated after eight
years [Ref. 4].
Basically, under the eight-year moving average the assign-
ment procedure consists of adding the current fiscal years'
purchases to the present totals. Then subtracting the oldest
years totals as well as the dollar value of equipment surveyed,
lost, or destroyed during the preceding year. The new total
in each category (Dental Care, All Other) is divided by eight.
The resulting figure is the current fiscal year's depreciation
expense that will be allocated to the operating expense ac-
counts on a quarterly basis [Ref. 4].
Table 4 is an example of the method used to determine
the annual depreciation expense under the UCA procedures.
D. PROPERTY SUBJECT TO DEPRECIATION
Under the Uniform Chart of Accounts (UCA), depreciable
properties will include only those cost associated with
31

Table 4
Value of Investment Equipment
compromising the depreciable
base - Fiscal Years 1972
through 1979: l,584,000
Investment Equipment
Purchased Fiscal Year 1980 750,000
t2,334,000
Less:
Investment Equipment
Transferred FY 1980 $50,000
Investment Equipment
Surveyed FY 1980 25,000
Modernization and or
Replacement Investment
Equipment Purchased
FY 1972 400,000 ( 475,000 )
Value of Investment Equipment
comprising the depreciable
base: FY1973 - 1980 l,859,000
Annual depreciation expense = $1,859,000 x .125 depreciation factor fl/8)
$ 232,375
Quarterly depreciation expense 58,094
32
Ug

modernization and replacement equipment. Any equipment less
than the investment equipment threshold value of $1,000 will
2not be depreciated. Equipment less than $1,000 will be
3* charged to the receiving cost center as an operating expense
[Ref. 4].
The only investment depreciation expense allocated to the
operating expense accounts are those expenses associated
with replacement and modernization equipment funded from the
Other Procurement Appropriation [Ref. 41. Specifically ex-
cluded from the depreciation process are expenses associated
with: (1) new and expanded facilities, (2) those items
classified as real property (elevators, environmental control
units, etc.), (3) War Readiness Reserves, (4) support of any
Program Element other than PEC 877110, "Care in Defense
Facilities," and (5) support of Special Programs, such as
vehicles, clinical investigations, drug abuse programs, and
alcohol abuse rehabilitation.
2lInvestment equipment is equipment that is long-lived(greater than one-year), repairable and has a dollar valuegreater than $1,000. After October 1980 the dollar valuefor Investment Equipment will increase to $3000.
3As defined by DODINST 6010.10M a cost center is adiscrete functional or organization subdivision of amilitary medical facility for which provisions are madeto accumulate and measure its expenses and determineits workload performance.
33

E. DEPRECIATION EXPENSE ALLOCATION
Distribution of the depreciation expenses between the
Inpatient and Ambulatory care accounts is to be based on the
average occupied bed days:
Average Daily Occupied Distribution PercentageBed Days Inpatient Ambulatory
Greater than 250 60% 40%
Between 50 and 250 50% 50%
Less than 50 40% 60%
Clinics -0- 100%
Once the distribution percentage between Inpatient and
Ambulatory accounts has been determined, a ratio of occupied
bed days for the inpatient account to the total number of
occupied bed days will determine how much of the depreciation
expense is to be allocated to the particular inpatient account.
Allocation of the depreciation expense to the Ambulatory Care
work centers is based on a ratio of ambulatory clinic visits
to the total number of visits to the medical treatment
facility [Ref. 4].
F. CONCLUSION
The depreciation methodologies used by civilian hospitals
vary according to the use for which a hospital accumulates
4 depreciation. Military hospitals choice of depreciation is
set by fiat.
Civilian hospitals initially decide the purpose for
accumulating depreciation and then selects the most appropriate
34

depreciation method. Straight-line depreciation is generally
selected for :ate setting and third-party reimbursements.
While "==zlerated depreciation is usually chosen for cash
flow purposes and tax avoidance.
The method used by military hospitals is established by
the Department of Defense and is essentially a composite rate
of depreciation with an useful life based on an eight-year
moving average. The UCA depreciation method is used primarily
in determining the full cost of patient care. Once computed,
depreciation expenses are allocated to the various Inpatient
Care and Ambulatory Care accounts based on the facility's
daily average occupied bed days. After determining the dis-
tribution percentage between the two categories of accounts,
distribution to individual accounts is done on a ratio of the
individual account's work units to the total work units for
the medical treatment facility.
35
4

IV. A CRITICAL ANALYSIS OF UCA DEPRECIATION METHODOLOGY ANDRECOMMENDATIONS
A. INTRODUCTION
As stated in Chanter One, the Uniform Chart of Accounts
was developed by the Department of Defense as a cost collec-
tion system designed to record, accumulate and report informa-
tion regarding the expense and workload within a military
treatment facility as a means of determining the total cost of
treating a patient [Ref. 4]. An integral part of the total
cost of providing health care is accounting for the consumption
of long-lived fixed assets used in the delivery of health care.
The accepted means of recognizing this consumption is through
depreciation. Depreciation is defined as a system of account-
ing whose purpose is to distribute the cost or other basic
value of tangible capital assets over the estimated useful
life of the unit in a systematic and reasonable manner
[Refs. 6, 211.
Accepting the foregoing definition, the UCA established
a system of depreciation that would account for the consump-
tion of long-lived assets and then allocate the consumption
based on a ratio of occupied bed days, in the case of Inpatient
Care, or a ratio of clinic visits for Ambulatory Care [Ref. 4].
Taking into consideration the UCA depreciation methodology
and its underlying assumptions, four issues are raised:
* (1) Does the current UCA method recognize depreciation expense
36
I1

in a systematic and reasonable manner? (2) Does the current
UCA method of depreciation allow meaningful cost comparability
among military medical treatment facilities and with the
*[ civilian health sector? (3) Is the UCA depreciation require-
ment so restrictive as to minimize the effect of depreciation
on the total cost of patient care? (4) Can depreciation's
contribution to the total cost of patient care be isolated so
that management decisions will not be influenced by sunk
costs? (5) Expense involving the purchase equipment in the
$1,000 to $2,999 range are double counted.
The purpose of this chapter is to analyze the underlying
assumptions regarding UCA depreciation and challenge the
foregoing issues as well as offer recommendations that may
enhance the value of depreciation accounting within the Uni-
form Chart of Accounts.
B. ASSUMPTIONS UNDERLYING THE UCA DEPRECIATION METHODOLOGY
The depreciation scheme used in the UCA is basically a
composite rate of depreciation whereby the rate has been set
by fiat at 12.5% [Ref. 4]. Assumptions that have to be made
for the eight-year (or 12.5%) moving average to give valid
depreciation information are: the useful life of the medical
equipment is normally distributed throughout the populationIiand has a mean life expectancy of eight years; retired assets
are replaced with assets having similar useful lives; there
will be no material change in the composition of assets; only
37

modernization and replacement equipment with a value above
the $1000 threshold contributes to the expense of providing
medical care in a military medical treatment facility [Ref. 4].
As a means of testing the validity of the assumption that
the average useful life of medical equipment is eight years
and is normally distributed throughout the equipment population,
a series of five random samples were drawn from equipment list
of seven Naval Regional Medical Centers (NRMC) and analyzed to
see if the eight-year mean useful service life was a reason-
able figure. Statistical tests were completed to see if the
individual samples were drawn at random, if they came from the
same population, and if the sample averages came from identical
populations. Appendix B outlines the methodology used to
determine the mean, standard deviation, confidence interval,
the results of the Runs Test for Randomness and the Kruskal-
Wallis One-Way Analysis of Variance. The results of the anal-
ysis supports the contention that while the equipment in use
* at the various NRMCs come from identical populations, the
* eight year useful life is too low. The range of sample
averages are:
Confidence Interval at 95%
Lower Limit Upper Limit
NRMC, Bethesda, Md 11.7 yrs 13.3 yrs
NRMC, Camp Lejuene, NC 11.5 yrs 13.5 yrs
NRMC, Charleston, SC 9.0 yrs 10.6 yrs
4 NRMC, San Diego, CA 10.6 yrs 12.4 yrs
38

NRMC, Camp Pendelton, CA 11.2 yrs 13.1 yrs
NRMC, Long Beach, CA 10.0 yrs 11.0 yrs
NRMC, Oakland, CA 11.0 yrs 12.6 yrs
Overall Confidence Interval 10.5 yrs 12.5 yrs
Intuitively, second and third assumptions are difficult
to accept. Saying that retired assets are replaced with assets
having similar useful lives and there will be no material
change in the composition of assets one would have to ignore
state-of-the-art changes in medical equipment. Plus, accept
the contention that military medicine is a static undertaking
that does not respond to innovation in health care.
The fourth assumption has the greatest impact on the amount
of depreciation expenses that will be allocated to the inpatient
and ambulatory care accounts. Considering only modernization
and replacement equipment as contributors to the expense of
providing medical care excludes a majority of a Naval Regional
Medical Center's capital assets. In order to evaluate the
impact of excluding real property and new and expanded
facilities on depreciation expenses, real property and equip-
K1O ment records from four Naval Regional Medical Centers,
Charleston, SC, Camp Lejeune, NC, Long Beach, CA, Bremerton,
WA were reviewed and compared with the depreciation expenses
reported under the UCA procedures for Fiscal Year 1980.
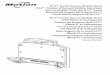
As can be seen from Table 5 the effect of excluding real
property and new equipment can have a substantial impact on
6 the amount of depreciation expenses that are allocated to the
39

LIi 0 C14
0n 0 -
0
N(
0 0 -c
%D4W 0 0a
uj LU CN4-U( -4
-4.-I C) ca
> U)o .- L Z0 '0
-4~~~- 41 *- -I-*.4.) a% >a)--1
a-0% 4-I U; *0(N 0 L~) -4
-H ' OW6 -o4 4)co -4
0r ao 0 L)> >40) -a-aW0. a'. L 1 r-40 C) -- cO% 0 CU -14 0
X WL p 00 ON0 r.4 m (1) -4 .4 4-I4-) LL (nf r- -4 nN 4r NLAC4PQC U) -Z C:) aa CU a) 4.aL) 'D aU (N LJODC I 0%' '4 0% .4-141 cSC c -" %OI .r -4 '% co 0 a 4.Ua.. a) -4-).~ Zuta) 41(N C4Lr 4 Ln 1C \O(N A-) inV) -4 cc W 0 b d4tp 44 ~ f4 4 oV O0.0 Ca) 3-4 k 14-a) o. -
4 o a) -IL U) UM 0) 0)~ C wa LL.. 14F4 S4 $4 40
- 0-a -i U) m nu)s4 (1) at) %.4 a )c
0 CL'-0 Iw *5 -4.i64 (n 0) 0 N 00 00 0-I %.t (n Cm aU
cc0. CL *#-i - T - 4 -Z-4 - 0.qa -Yco-4 Cb~ U) -4
0)) Cczn 0N4 n c a% 10% 03>%> Go 0-4 CD 0 C 0 D '0 11 " .7V Q.. 0)I-W a
OLc-)r- 00 r-n100 0 -fr4r44)-a) Q) "a Wa cu co..a V4
0 '- -O ; n u nN' -O 0(N (L) -. a" ) QI- IAs CL~' C L >OU )4-c- r- C1 04*L N tAJ43 ) :3 V.4 )
CL a a o ao a a0 co 0. &.4- W.
ancc() -4
OZ 0 U' co0 CN0 0 0-4 'a -4) a)Q)1- Z4 1-4 -4 Cm-4
0) C. 11C40 ) "m x (f)00 1)V ( ) C UWa 0) r= " ) c
0L ". y.) U)C
4- 41 4-- 42.)> -
0. a) Z04-)CD a)c a c) w. a4 a
te\ ~ w 0w c L L4 4"
> 1 0 4 - 2 4041 W 4 J 4 1.4 I 1 )"L
k...........'0-)clw D

various medical care accounts. Several strong assumptions
were made regarding the depreciable base: no equipment in
service exceeds the composite service life in Column Five;
all of the property and equipment are used in support of
Program Element "Care in Defense Facilities," PEC 877110.
The effect that the foregoing assumptions have on the
overall amount of depreciation expense of course varies within
each facility. However, the value of the comparison is not
to show an absolute dollar variance. Rather it is to show
the magnitude of the variance. Excluding real property and
new or expanded facilities from depreciation results in a
variance in reported depreciation that ranges from $307,000
for NRMC Charleston, SC to around $2,700,000 for the new
facility at Bremerton, Washington. In Table 5, Real Property
was depreciated using a 40 year useful service life. The
category Real Property includes not only buildings with 40 year
estimated useful lives, but sidewalks, parking lots, ele-
vators and other items with estimated useful lives that range
from 12 to 25 years. However, in the final analysis the dif-
ference in depreciation expense using a composite life of 40
years and depreciating each item at its estimated service
lives was immaterial.
C. UNIFORM CHART OF ACCOUNT'S DEPRECIATION: IS ITSYSTEMATIC AND REASONABLE?
According to L. Van Seawell [Ref. 21] depreciation of
plant assets should be recognized by hospitals. The periodic
41

charge should be based upon a systematic and reasonable
allocation of the previously recorded acquisition costs of
such assets. Accepting this premise at face value gives
rise to a two part question about the current UCA depreciation
method. Is the UCA recognition of depreciation systematic and
reasonable?
Under the UCA depreciation is computed in a systematic
* manner. Guidelines are established to determine service life
of the assets to be depreciated, the depreciable base is
defined, and the method of allocating depreciation to the
operating expense accounts is outlined.
The reasonableness of the Uniform Chart of Accounts'
* depreciation can be questioned on several points: (1) exclud-
ing certain assets from depreciation understates the cost of
providing patient care, (2) the eight year service life under-
states the useful service life of the assets that are
depreciated, and (3) allocating depreciation from a common
cost pool disregards the fact that some clinical services are
more equipment intensive than others.
Under the Uniform Chart of Accounts, only modernization
and replacement equipment with a dollar value equal to or
greater than $1,000 will be depreciated [Ref. 41. Excluded
4 from this category of equipment are all buildings, land
improvements, furniture, new equipment and equipment with an
acquisition cost of under $1,000. Referring to Table 5, one
can gauge the effect that excluding real property, furniture
r42

and new equipment from the depreciation process has on the
annual depreciation expense. In the case of a new facility
-* . like the Naval Regional Medical Center, Bremerton, WA, the
foregoing exclusions can result in understating the annual
depreciation expense by about $2,600,000. The same exclusions
will understate depreciation expenses for an established
facility like Naval Regional Medical Center, Charleston, SC by
approximately $300,000.
Any process that ignores expenses ranging from $300,000
to $2,600,000 because of the source of funding [Ref. 4] used
to acquire the assets, or because of the assets classifica-
tion, appears to be unreasonable. If the purpose of account-
ing for depreciation within the UCA is to get a better picture
of the cost of providing medical care, the process should not
overlook assets that form the bulk of the cost of the medical
facility. Irrespective of how the assets were acquired or
what class of asset is involved, all assets are a cost to the
government and they are expenses attributable to providing
medical care. As such, they should be considered in account-
ing for the cost of providing medical care.
Another aspect of UCA depreciation that is open to question
is the validity of the standard eight year service life. As
indicated by Appendix B there is sufficient variation between
estimated service lives from the seven NRMC's sampled as to
suggest that a uniform depreciation rate does not accurately
4 represent how long individual Medical Centers can expect to
43

utilize their investment equipment. The eight year figure
understates the average estimated service life by a percent-
age that ranges from 13% to 35% for the Naval Regional Medical
Center Charleston, SC and from 46% to 69% for the Naval Re-
gional Medical Center, Camp Lejeune, NC. Considering the
range of the variation between the standard depreciation rate
and the various rates indicated by Appendix B, the accuracy of
determining the composite service life for each facility could
be improved if each facility computed individual composite rates
of depreciation.
However, data processing equipment obviates the need to
compute a composite rate of depreciation. NRMCs currently
possess sufficient data processing equipment to be able to
depreciate individual pieces of equipment on a straight-line
basis and circumvent the tedious manual task of trying to
accurately figure straight-line depreciation for a large
number of dissimilar assets. The necessary information is
maintained by each NRMC. Plant property records list the
item, acquisition cost, date the asset was placed in service,
and estimated service life, and the department to which the
asset is assigned [Ref. 22]. Using these data and with the
help of a computer, it becomes a minor task to write a program
or a subroutine to an existing program, that will compute and
total the depreciation expense. The convenience of using a
computer to figure depreciation expenses obviates the need
for simplicity in a manual system and bypasses the assumption
44
.4

that retired assets are replaced with assets having similar
costs and useful lives, events that rarely, if ever, occur.
The reasonableness of the depreciation allocation process
can be challenged on the grounds that it inequitably assigns
expenses to the various cost centers. All depreciation ex-
penses are assigned to a cost pool, then allocated on the
basis of a ratio of clinic visits in the case of ambulatory
care, or a ratio of occupied bed days for inpatient care.
Allocating depreciation on the basis of such ratios does not
take into account that certain clinical services are more
capital intensive than others [Refs. 19, 201. For example, a
Coronary Care Unit (CCU) will have more money invested in
equipment than will a more labor-intensive inpatient service
such as a Neurology Service [Refs. 15,16]. Under the UCA
procedures all inpatient accounts receive a proportional share
of equipment depreciation expenses irrespective of the amount
of equipment that the account owns. In effect, the heavy
investment of any service in equipment is distributed to other
services. Consequently, the cost of operating an equipment-
intensive service is understated while the cost of operating
the labor-intensive service is overstated. The same effect
is seen in allocating depreciation to the Ambulatory Services.
Those Ambulatory Services, such as a Primary Care Clinic,
that are labor-intensive receive a disproportion share of the
depreciation expense.
45

It would be more equitable and no more difficult to
charge depreciation expense on equipment to the using cost
center. Then only in those cases where a piece of equipment
is not readily identified to a particular cost center should
the corresponding depreciation expense be accumulated in a
common cost center and allocated to all cost centers on the
basis of occupied bed days or number of clinic visits [Refs.
24, 25].
A companion to the reasonableness issue is one that deals
with the double counting of certain UCA expenses. In partic-
ular the double counting of expenses associated with the pur-
chase of equipment in the $1,000 to $2,999 range. In the
absence of either increasing the UCA depreciation threshold
value to $3,000 or making year-end adjusting entries, double
counting of expenses associated with the purchase of equip-
ment whose acquisition cost ranges from $1,000 to $2,999 will
be a problem that will appear during Fiscal Year 1981 and
beyond.
Double counting expenses will occur because of the variance
in the way investment equipment is defined by the Resource
Management System and the Uniform Chart of Accounts. In Fiscal
Year (FY) 1981 the Resource Management System increased the
4 threshold value for Investment Equipment from $1,000 to $3,000
(Ref. 26]. However, the Uniform Chart of Accounts still main-
tains the threshold value for Investment Equipment at $1,000
4d [Ref. 4]. Without adjusting the UCA threshold value it will
46

be possible to expense the cost of a piece of equipment in
-_ the year of acquisition and then turn around and depreciate
it over an eight year period beginning in the following fiscal
year.
Under the Resource Management System (RMS) equipment cost-
ing less than $3,000 will be purchased with Operations andMaintenance (O&M) funds [Ref. 26]. The purchase of equipment
with O&M funds is subsequently reported on the Functional
Category/Expense Element Report, NAVCOMP 2171, as an expense
[Ref. 26]. The Uniform Chart of Accounts in turn allocates
the expense reported on the NAVCOMP 2171 to the appropriate
UCA operating expense account. However, since the equipment
depreciation threshold value under the UCA is still $1,000
[Ref. 4], there is a potential for either overstating deprecia-
tion expenses by 12.5% for eight years, or overstating
operating expenses for the cost center by an amount equal to
the total cost of equipment purchased in the $1,000 to $2,999
range in the year of acquisition.
D. DOES THE CURRENT UCA METHOD OF DEPRECIATION ALLOW MEANINGFULCOST COMPARABILITY AMONG MILITARY MEDICAL TREATMENTFACILITIES AND WITH THE CIVILIAN HEALTH SECTOR?
Comparability among military medical treatment facilities
is assured by the fact that all of the military facilities are
governed by the same Department of Defense directives and are
required to account for depreciation in the same way, follow-
ing identical allocation procedures [Ref. 4].
47

Comparability between military medical treatment facili-
ties and civilian health care centers is another matter. Where
the uniformity within the Department of Defense assures that
all military medical treatment facilities follow the same
guidelines in computing and allocating depreciation the lack
of uniformity between the military and civilian health sectors
in the use of depreciation accounting impedes cost comparability
between these two sectors. Table 6 illustrates the dissimilar-
ities between the UCA depreciation methodology and the methods
commonly used in the civilian health care sector.
The driving force behind a civilian medical facility's
choice of a depreciation method is the purpose to which the
resulting expense will be used. For example, if the purpose
of depreciation is to generate cash flow, accelerated deprecia-
tion would be used [Ref. 10]. However, if the purpose for
accumulating depreciation is to determine a contractural
reimbursement rate, straight-line depreciation would be used
(Ref. 28].
Table 6 illustrates that there is no uniformity in the
types of depreciation used by the civilian health care sector,
with the choice of depreciation relying on the purpose to
which the calculated expenses will be used. Lacking uniformity,
cost comparison between military and civilian medical facil-
ities is meaningless when the final cost figures include
depreciation expenses. Depending on the method used, the
estimated useful life, class of asset depreciated, and the
48

Table 6
Dissimilarites between theUniform Chart of AccountsMethod of Depreciation andDepreciation Methods used inthe Civilian Health Sector
Item Uniform Chart of Accounts 1 Civilian Health Sector 2
Threshold Value for $1,000 Variable. Ranges fromAsset Capitalization $25 to $25,000
dependingon the class of assetbeing capitalized.
Class of Asset Modernization and replace- Generally any assetDepreciated ment equipment only. that exceeds the
Real property capitalizationnew and expanded threshold value and has anfacilities are not expected useful lifedepreciated. greater than one year.
Depreciation Method Modified Composite Rate. Generally straight-lineComposite rate of depre- depreciation is used forciation has been estab- reimbursement rate settinglished by fiat at 12.5% and accelerated depreci-(eight year useful life). ation is used for account-
ing purposes.
Method of Based on a ratio occupied Assigns direct costAllocation of bed days or a ratio of depreciation to specific
clinic visits. Does not cost centers. Allocatescharge depreciation indirect cost based on thedirectly to the using value of equipment or thecost center. square footage of building
occupied.
Reason(s) for Compute full cost of Rate setting, cashaccounting for patient care flow generation and fund-depreciation ing for depreciation 3
1 Reference 4.
2 References 10, 12, 13, 14, 28.
3 Funding of depreciation refers to the process by which cash resourcesare set aside periodically and accumulated for the purpose of financingthe renewal or replacement of plant assets. (Ref. 21)
4
49

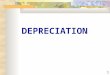
NAVAL REGIONAL MEDICAL CENTERCamp
Lejuene Charleston Long Beach BremertonINPATIENT CARE
Total Occupied Bed Days1 45,937 50,697 36,642 23,678
Fourth Quarter FY801
Cost Year-To-Date $8,035,100 $9,924,728 $9,955,199 $5,230,337
Figure 5, Page 38Variance multiplied by 0.5 363,824 150,000 527,201 1,317,354
Adjusted Fourth QuarterFY80 Cost Year-To-Date $8,398,934 $10,074,728 $10,462,400 $6,547,691
Approximate cost peroccupied bed day (Fourth QtrFY80 Cost YTD divided byOccupied Bed Days) $175 $196 $272 $221
Adjusted Cost Per Occupied(Adjusted Fourt Qtr FY80 Costdivided by Total Occupied BedDays) $183 $199 $286 $276Percent Increase Attributedto Depreciation 4.5% 1.5% 5.0% 25.0%
AMBULATORY CARE
Total Clinic Visits2 332,331 401,787 340,082 183,652
Total Ambulatory CareExpenses2 $7,444,632 $8,404,753 $10,108,776 $4,584,197
Figure 5, Page 38Variance multiplied by 0.5 363,834 150,000 527,201 1,217,354
Adjusted Total Expenses $7,808,466 $8,554,753 $10,635,977 $5,891,551
Average Cost Per Visit(Total Expenses/Total Visits) $21.89 $20.92 $30.41 $24.96
- Average Adjusted Cost PerVisit (Adjusted TotalExpenses/Total Visits $22.94 $21.29 $31.46 $32.12
Percent Increase Attributedto Depreciation 4.8% 1.8% 5.2% 28.7%
Table 7Adjusted Average Cost Per Occupied Bed Day
and Per Ambulatory Care Vist
1 Reference 292 Reference 30 50
I.

reason for accounting for depreciation, a medical facility can
adjust the total cost of health care delivery. Taking the
four NRMCs listed in Table 7 as representative of the degree
* . to which a Military Treatment Facility could influence the
recorded cost of health care delivery, it can be seen that by
carefully selecting the method of depreciation, estimated
useful life, and the depreciable base a Military Treatment
Facility can vary its reported cost by as much as 28%. Mean-
while civilian hospitals can alter their depreciation expenses
by choosing from among the various depreciation methods.
Their choice of which depreciation method to use would depend
upon the purpose for which the depreciation expenses are to be
used. Generally, civilian hospitals tend to select straight-
line depreciation for rate setting and reimbursements while
selecting accelerated depreciation for cash flow and tax
purposes (Refs. 7, 10, 11, 12, 13, 14].
E. IS THE UCA DEPRECIATION REQUIREMENT SO RESTRICTIVE AS TOMINIMIZE THE EFFECT OF DEPRECIATION ON THE TOTAL COST OFPATIENT CARE?
Iterating what has been said before, depreciation require-
* - ments minimize the effect of depreciation on the total cost of
patient care; ignoring depreciation expenses ranging from
$300,000 to $2,600,000 annually certainly decreases the value
of the depreciation process in the cost collection system.
Using the summary data in Table 5, and data from Reference 28
and 29, Table 8 illustrates the effect of excluding all but
51

Table 8
Depreciation's Contributionto the Total Cost of
Patient Care
Facility Adjusted TotalI Estimated UCA2 Depreciation'sExpenses FY1980 Depreciation Contribution to
FY 1980 Total Expenses
"RMC, Camp Lejeune, NC $16,215,400 $999,636 6.2%
NRMC, Charleston, SC $18,644,182 768,701 4.1%
NRMC, Long Beach, CA t2l,151,371 $1,095,802 5.2%
NRMC, Bremerton, WA $12,449,242 t2,794,4203 22.2%
1 Total Expenses for FY 1980 were taken from References 29 and 30, less UCA
depreciation reported for FY 1980, plus the estimated annual depreciationexpenses that included all Real Property in the depreciable base.
2 Total Depreciation for year, Table 5.
3 Depreciation expense includes the new facility plus all equipment with adollar value equal to or greater than tl,000.
52

modernization and replacement equipment from the depreciable
base of a Naval Treatment Facility. It should be noted that
the $2,600,000 variance shown in Table 5 for NRMC Bremerton
is attributed to Bremerton being a new facility with the
majority of its equipment being new.
F. CAN DEPRECIATION'S CONTRIBUTION TO THE TOTAL COST OFPATIENT CARE BE ISOLATED IN ORDER THAT MANAGEMENTDECISIONS WILL NOT BE INFLUENCED BY SUNK COSTS?
Once depreciation expenses are allocated to the Final
Operating Expense accounts, that portion of patient care cost
attributable to depreciation can not be isolated. After
expense allocation, a reader of UCA summary data would need a
copy of a NRMC's expense assignment worksheet similar to
Table 12, (Appendix A) in order to isolate depreciation's
effect on health care cost.
If one accepts the idea that all past costs are irrelevant
and should not be included in future decision [Ref. 31], or if,
in the future, UCA includes all capital assets in the depre-
ciable base, then it is important to be able to see what effect
depreciation has on patient care cost. If Real Property is
included in UCA depreciation procedures, the change in de-
preciation expenses would be material. Depreciation would
then have a mater4 I affect on the total cost of patient care.
Taking Figure 8 as being representative of all Naval Medical
Facilities, depreciation's contribution to the total cost
of patient care ranges from 4.1% to 22.2%.
53

G. CONCLUSION
As stated in the opening paragraph of this chapter,
depreciation accounting is a recent occurrence within the
* military medical services, tracing its origins to the imple-
mentation of the Uniform Chart of Accounts. The purpose of
UCA depreciation is to account for the consumption of certain
long-lived fixed assets as an expense of providing medical
care and it is a part of a larger expense accounting system
that is designed to account for the total cost of patient
care.
As it is currently used in the UCA, depreciation is essen-
tially a composite rate of depreciation. In cases where fully
depreciated assets remain in service no further depreciation
is taken. Nor, are any adjustments made to recognize an
obvious change in an accounting estimate that would affect
the amount of depreciation charged to the operating expense
accounts such as a change in a medical facility's mix of
depreciable equipment that would either increase or decrease
their composite service life.
7 Two factors are the driving force behind the amount of
depreciation expense that will be allocated to the various
medical care accounts. They are: (1) only modernization or
replacement equipment with an acquisition cost equal to, or
greater than, $1,000 will be depreciated, and (2) equipment
will be depreciated over an eight year period. Both factors
can be challenged on the grounds that they tend to misrepresent
54

the amount of depreciation expense allocated to the operating
expense accounts. As shown by Table 5, including only
modernization and replacement equipment seriously understates
the amount of expenses generated by depreciation. The second
factor, eight year service life, can be questioned based on
random samples of equipment from seven NRMCs. These random
samples (Appendix B) raise questions as to the validity of
the eight-year composite service life. By accepting the pre-
* mise that equipment used at the various medical treatment
facilities comes from identical populations and that the
mean useful service life is eight years, one would expect to
see a series of random samples where the eight year composite
life would fall within a confidence interval for the sample
means. Appendix B indicates that while the samples were
random and drawn from similar populations the confidence inter-
vals for the mean useful service life had a lower limit of 10.5
and an upper limit of 12.5 years. The eight year composite
life falls well outside of the sampling interval and supports
the contention that the composite rate of depreciation should
be higher than eight years. Considering the availability of
data processing equipment, there is really no need to compute
a composite service life. Equipment can be depreciated on a
4 straight-line basis.
The UCA depreciation expense allocation does not account
for the fact that some clinical services are more equipment-
intensive than others. Disregarding this fact and accumulating
55

all depreciation expenses in a common cost pool and then
allocating the accumulated expenses on the basis of either an
occupied bed ratio or on a ratio of clinic visits penalized
those services that are labor-intensive and have a small invest-
ment in depreciable equipment. Labor intensive services are
penalized by assigning thm a disproportionate share of de-
preciation expense. According to Ferrara [Ref. 24] and the
Cost Accounting Standards Board [Ref. 25] the foregoing in-
equity can be corrected by charging the using cost center with
the depreciation expenses directly identified with its
operation. Only when a piece of equipment can not be identi-
fied with a particular cost center should it be recorded in a
common account and allocated to all cost centers on the basis
of either the occupied bed ratio or the ratio of clinic
visits.
Finally, unless some changes are made in the UCA account-
ing procedures, depreciation expenses for FY 1982 and beyond
will be overstated by an amount equal to 12.5% of the acquisi-
* tion cost of equipment with a unit cost that ranges between
*$1,000 to $2,999 purchased with Operating and Maintenance
funds.
56

17.-
V. RECOMMENDATIONS FOR CHANGES TO UCA DEPRECIATION
A. INTRODUCTION
Accepting the premise that the purpose of the Uniform
Chart of Accounts is to determine the total cost of patient
care and that depreciation is a legitimate cost of patient
care, there are several changes to the current UCA methodology
that are recommended which may improve the accuracy of the cost
figures generated by depreciation.
As noted earlier, UCA excludes from the depreciation pro-
cess a large segment of fixed assets used in the health care
delivery process. Nor does the process recognize deprecia-
tion attributable to specific cost centers. Additionally, the
process underestimates the useful life of equipment and once
the depreciation expenses are allocated to the final operating
expense accounts, the effect of depreciation on the total cost
of patient care can not be isolated unless a copy of the
expense assignment worksheet is available. Furthermore, a
recent development within Fiscal Year 1981 establishes the
ground work for double counting expenses associated with the
purchase of equipment with a unit cost that ranges from $1,000
to $2,999. All of the foregoing oversights, underestimations
and exclusions tend to inhibit the accuracy and usefulness of
the expenses generated by depreciation. However, with minor
adjustments the accuracy and usefulness of the generated
depreciation expenses can be enhanced.
57

Accounting for depreciation as an element of the cost of
health care delivery can be improved in five ways: (1) include
all capital assets that exceed the depreciation threshold in
the depreciation process, (2) allocate depreciation expenses
on a direct basis as well as indirectly, (3) depreciate capital
assets using a unit straight-line depreciation method, (4)
display depreciation expenses for the final operating expense
accounts in a format that shows what portion of the total
expenses are attributable to depreciation, (5) utilize adjust-
ing entries at the end of each UCA reporting period to avoid
double counting expenses associated with the purchase of
equipment in the $1,000 to $2,999 range.
B. RECOMMENDATIONS
1. Include All Capital Assets in the Depreciation Process
a. The accuracy of determining the value of capital
assets consumed in the process of providing health care can be
improved if all assets that exceed the depreciation threshold
are included in the depreciation process, irrespective of the
source of funds used to purchase the assets.
b. Depreciation can be accumulated in two accounts:
Real Property Account (to include buildings, land improvements,
utilities, elevators and alarm systems) and Equipment Account.
In addition to equipment with a value greater than $1,000,
the Equipment Account would include patient and office fur-
niture that exceeds the depreciation threshold value.
58

c. Once depreciation expenses are collected they
can be allocated on the basis of square footage of building
occupied in the case of real property, or on the basis of
°* either a ratio of occupied bed days or a ratio of ambulatory
care visits.
2. Use Two Methods of Allocating Depreciation to Eitherthe Inpatient Care Accounts or to the Ambulatory Care Accounts
a. Treat depreciation as either a direct or indirect
cost depending on its traceability to a particular cost center.
If the total use of a piece of equipment is traceable to a
particular cost center then the resulting depreciation should
be allocated to the using cost center. If. however, the
piece of equipment can not be easily identified with a par-
ticular cost center, then the depreciation should be treated
as an indirect cost and allocated to the final expense ac-
counts on the basis of either a ratio of occupied bed days
or a ratio of ambulatory care visits.
b. Treating depreciation as either a direct or in-
direct cost will more closely show the full cost of operating
a cost center. Dealing with depreciation as an indirect cost,
assignable only on a prorated basis, understates the cost of
operating equipment-intensive cost centers while at the same
time overstating the cost of those cost centers that are
labor-intensive. Whereas depreciation as a direct cost will
reduce this inequity and assign the cost of asset consumption
to the producing department.
59
- 4

I
c. Assign real property depreciation as an indirect
expense to the corresponding Real Property depreciation
account. Accumulated expenses can then be allocated on the
basis of square footage of building(s) occupied by the various
cost centers.
d. Allocating depreciation expenses utilizing the
foregoing methods will help determine the total amount of
resources used by a cost center, with the full depreciation
cost being the sum of its direct depreciation expenses plus
-" an equitable share of the indirect depreciation expenses. The
general principle being that each cost center should be charged
with the full amount of the cost that they cause. In essence,
cost centers will receive those depreciation expenses that can
be traced directly to them as well as an equitable share of the
depreciation expenses incurred jointly for two or more cost
centers.
3. Depreciate All Capital Assets Using a Unit Straight-line Method
a. In place of a composite rate of depreciation, all
capital assets can be depreciated using the unit straight-line
method. Depreciating each capital asset based on the individ-
ual useful service life eliminates the need to make several
4 strong assumptions associated with the composite rate of
depreciation. Primarily, the need to assume that the useful
life of the equipment is normally distributed throughout the
Spopulation and has a mean life expectancy of eight years,
60
4!

retired assets are replaced with assets having similar useful
lives and there will be no material change in the composition
of assets will be eliminated.
b. Additionally, the unit straight-line depreciation
method will more closely match the expected consumption of the
assets over time than will the current composite rate of
depreciation. In the event a fully depreciated asset is still
in use, the unit straight-line method will permit a Naval
medical facility to adjust the useful service life to reflect
the revision in useful service life as well as revision of an
accounting estimate. Both adjustments would be an improve-
ment over the current method which assumes all assets are
considered to be fully consumed after eight years.
c. Depreciating assets on a unit basis and adjusting
the service life for fully depreciated assets still in use
parallels the depreciation policy set forth by the Assistant
Secretary of Defense (Comptroller) Memorandum dated 6 November
1979 outlining the Department of Defense's depreciation policy.
The memorandum states in part that, "... the straight line
method of depreciation is appropriate when the expected con-
sumption of the asset is reasonably level over the useful life
of the asset ... Assets that are still in use will not be
fully depreciated ... the estimated life of an asset will be
reviewed and adjusted periodically to conform to current
plans for (the) asset's usage
61

of4. Display Depreciation in a Format that Shows the EffectofDepreciation on tne Total Operating Expenses
a. After depreciation has been allocated to the
final operating expense accounts a reader of summary data can
not tell what effect depreciation has on the total cost of
providing health care. This inability to separate a sunk cost
from the total cost of providing health care could result in
management decisions being influenced by an irrelevant cost.
In such areas as deciding on the desireability of providing a
medical service or purchasing the samie service from a civilian
* health care facility, or in comparing relative efficiencies
between Naval medical facilities, incorporating an irrelevant
cost in the comparative cost analysis could persuade manage-
ment that it was cheaper to purchase health care rather than
provide the service in-house, or decide that one Naval medical
facility was more efficient than another when in fact the
margin of difference in each case was attributable to a sunk
cost like depreciation.
b. Reporting depreciation as a separate column on
either the Medical Expense Performance Report or on other
reports such as the UCA Analysis of Inpatient Care and
Ambulatory Care (Refs. 29,30] and will decrease the chance
that management decisions will be influenced by a sunk cost.
Modification of the tJCA collecting and reporting system could
Klead to the production of a report similar to Table 9. Ta-
ble 10 is the format typically used to report medical expenses.
62

0.r4 t . l a0oc-W U.% ̂ %a t- 0 O-W -.0 0% t- CJ %a %
41 1O; ~ 0:C 0a
E4 b woi 14M- W0 r
4a lot0 U% t-CI 40 fn
0.x 4- 10 f-01-00 .4 0 -V t- cu
0- 1- m - . o ^1
f-C'4U.00u
0 d0
C4 I x t- -T 4 3...Lr 04 4Q
Ql~ to N, aW0i- i cii 4 cic T c
00.00. * 4 z 9(a en.J( fn0 f-440'0' UM cm- % i 40 4li4-) 02.i .- . .a a uo a .0ATtf C 0c t-- 0 d- 0 1. 4Oa 0 0
04 9 0 10 0 0 0 MC n -% m C.4 0 7 cu . 2*
r C
L I1, 1 m Co.4 M."'~ fn0 r03. S43. aX E- A X CU enM n M L 0 0 4) v.
o 0 4 401 J 1- -. u~'0'.4 -40 "4P. - %M 0 W %L- u 1 $.,a a .,m
r -4 41k to 0.m .em.~I-C a0 V 14 C g ,
at 1..O ca kd.4 Cld3l'(a "U' W u (o 4 0 1 4m y l- 441d4 r4 -4) a -
z Cll'.. 1.0 u. ~ .3..Z0
Q1 *C'4P0 4A MCl6u cu m M 1140 0
P. *:oas6 00 v:03.Qa. U m 4S-'m ZW A.O 9: 1^ A.D 0~.pa - - 2 0 4
(6 o . T 0% 400'x 40 L-416 " 40%0( 4% 000-
W 120 c fnco n L. a 4 40 4 63
2 ct-c ." t 00 0- 44

000 MEDICAL TXPENSE AND PERFORMANCE REPORT' ItE eacln a,,(hpI;
NAME AND ADDRESS OF FACIL IT Y IS.,ed0E J Cod., 0FACILITY CODE #111VO REPORT PE RIOD
REPORTING AUT64ORITY 109)1 MEDICAL REGION
Navy - Bureau of Medicine Unrd Surgery 13 Cumulative YTD
PART 1. DIRECT PATIENT CARE itIj.I.l h.Na,.,I.d ... ,..A....I .IIVb,., 1
INPTINTCAE ISOSTINS TOTAL FOXPENSES INCLUDING CLINICIAN SALARY (OCCUPIEDINPTIET CRE ISPSITONS CLINICIAN SALARY (F NSE BED DAYS
MEDICAL CARE i,o8*r $1,879,)440 $77,665 6.o84
SURGICAL CARE 1,717 2,2,A9,651 224,991 7,43T
D.STETRICA LJGYN ECOLOGICAL CARE 2,416 2 027,957 62,235 7,889
PEDIATRIC CARE 2,183 1,113,761 30,010 6,730
ORTHOPEDIC CARE ~ 765 810,276 14,135 4,271
PSYCHIATRIC CARE 366 437,6o8 55,8141 2,982
TOTAL 8t534 $8 518,693 1$464,877 35,393AMEBULATORY CARE TOTAL OUTPATIENT EXPENSES] OUTPATIENT VISITS INPATIENT VISITS
2
MEDICAL CARE $ 873,11 22.368 973
SURGICAL CARE 582,350 24,677 1,331
OESTETRICAL/GYNFCOLOGICAL CARE (8o,111l 61 ,1o,3 0
PEDIATRIC CARE 574,'785 33,91*7 0
ORTHOPEDIC CARE 336 830 12,076 1,636
PSYCHIATRIC/MENTAIL HEALTH4 CARE 210,161 10 179 84
FAMILY PRACTICE CARE 9149 439 40 308 0
PRIMARY MEDICAL CARE 2 117,034 83,477 0
EMERGENCY MEDICAL CARE 920 557 25 408 0
PLIGHT MEDICINE CARE - --
UNDERSEAS MEDICINE CARE -
TOTAL _________ $7,344,378 31.6,513 4,o24____
DENTAL CARE TDTAL EXPENSES WEIGHTED DENTAL POEUE WEIGHYFO DENTAL PROSTH4ETICPROCDUREWORK UNIT
DENTAL SERVICES $133,083 NA
DENTAL LABORATORIES 13.220 NA
TOTAL $146,303
Do FOlm f' SEE ATTACHED CAVEATSI OCT,, 2202 E
7XP ENSES INCLUDED IN INPATIFNT CARE ACCOUNTS
Table 10
NAVCOMP 2171 Functional Category/Expense Element* Report Reconciliation with UCA Expenses
64

I
Table 10
(Continued)
(000)
Expense from the NAVCOMP 2171 Report
Year-To-Date $18,780.81
+ Free Receipts 15.2
+ Depreciation 345.8
+ Borrowed Labor 26.9
Unauthorized Absence Labor (10.0)
- Loaned Labor (52.3)
- Direct Reimbursable Expenses (16.0)
Total Expenses Reported on this MEPR $19,090.4
SYear-to-Date Expenses Total was taken from the FunctionalCategory/Expense Report (NAVCOMP 2171) prepared by the Auth-orized Accounting Activity.
'46
:"- 65

It summarizes the health care delivery expenses and reconciles
the UCA expense with the Resource Management System's Function
Category/Expense Element Report (NAVCOMP 2171). Table 9
refines the Medical Expense and Performance Report and dis-
plays depreciation expense along side the appropriate patient
care account. The formats proposed in Tables 9 and 10 will
allow an analyst the opportunity to decide whether or not
depreciation was a relevant cost to be used in any comparative
cost analysis. Isolating depreciation from the total expense
of providing health care takes on added significance in the
event all capital assets are included in the depreciation
process. The added significance is attributable to the increase
in depreciation's contribution to the total cost of health care
brought about by incorporating all capital assets in the de-
preciation base.
5. Use Adjusting Entries at the End of Each ReportingPeriod to Avoid Double Counting Expenses
a. The amount of expenses allocated to a cost center
that comes from purchasing equipment with a unit price that
ranges between $1,000 and $2,999 can be subtracted from the
operating expenses for that cost center before the UCA step-
down allocation process begins. Making the adjusting entries
" has advantages over raising the depreciation threshold value
to $3,000. The chief advantages are: (1) data reported will
be consistent with prior year reports; (2) adjusting entries
* will eliminate the need to maintain two property accounting
66
.....

systems, one system to account for property in the $1,000 to
$2,999 range previously expensed and another system to account
for equipment in the same range that is subject to depreciation.
b. Additional support for making adjusting entries
comes from the Comptroller General's accounting guidelines for
* - Federal Agencies [Ref. 25] Raising the depreciation threshold
value to $3,000 would exceed the Comptroller General's guide-
lines for capitalization of fixed assets by a factor of ten
[Ref. 221 According to the Comptroller General's accounting
guidelines for Federal Agencies, "Fixed assets owned or
acquired by each agency shall be capitalized in its accounts
... it is appropriate to establish reasonable dollar minimums
as a basis for excluding certain property units from
capitalization. No minimum in excess of $300 should be
established ... " [Ref. 22] Considering that capitalized
assets form the foundation for depreciation accounting, it
* * ~ would appear that raising the depreciation threshold value
in the UCA to $3,000 would exceed the foregoing guidelines
established by Comptroller General by a much wider margin
than can be justified.
67

VI. SUMMARY AND CONCLUSION
A. SUMMARY
Depreciation, as a cost of providing health care, became
an integral part of a cost collection system that was imple-
mented in the Department of Defense in 1979. Known as the
Uniform Chart of Accounts (TJCA), the system's purpose was to
record, accumulate and report information regarding expenses
and workloads within the various military treatment facilities
as a means of determining the full cost of treating a patient.
Among the benefits expected to be gained from knowing the full
cost of patient care are enhanced cost awareness, cost-effec-
tiveness evaluation, improved decision-making and improved
cost comparability among the military treatment facilities as
well as with the civilian health sector.
Under the UCA, depreciation is used to allocate the cost
of the fixed assets used in the health care delivery process
in a systematic and rational manner. The type of depreciation
used is a composite straight-line method that assumes all
assets are either modernization or replacement equipment.
Specifically excluded from the UCA depreciation accounting
are new and expanded facilities, real property, War Readiness
Reserves and expenses associated with the support of such
special programs as vehicles, clinical investigations, drug
and alcohol abuse programs.
68

Once accumulated, depreciation expenses are allocated to
the final UCA expense accounts on the basis of a ratio of
occupied bed days for a particular inpatient account to the
total number of occupied bed days for the facility. The final
ambulatory care expense accounts receive their portion of the
depreciation expenses based on a ratio of ambulatory clinic
visits to the total number of a facility's ambulatory clinic
visits.
Several factors are taken for granted in computing deprecia-
tion under the UCA. They are: (1) the useful life of de-
preciable equipment is distributed normally throughout the
equipment population and have a mean life expectancy of eight
years, (2) replacement equipment have useful lives similar to
the equipment being taken out of service, (3) only moderniza-
tion and replacement equipment with a value greater than
$1,000 contributes to the expense of providing medical care
in a military treatment facility.
Depreciation use varies markedly between the Military
Health Service System and the Civilian Health Care System.
Essentially there are two major differences. First, the Mili-
tary Health Service System used a uniform method of deprecia-
tion that ensures all of the military facilities accumulate
4 and distribute depreciation expenses in a uniform manner,
whereas civilian hosvitals use a variety of depreciation
methods depending on the purpose for accumulating depreciation
expenses. For example, if a civilian hospital accumulates
69

depreciation for the purpose of generating cash flow, it will
probably choose an accelerated method of depreciation [Ref. 101.
However, if the civilian hospital's purpose is accumulating
depreciation in order to determine a contractual reimbursement
rate, it will choose straight-line depreciation [Ref. 28].
The second major difference is that the Military Health Service
System ignores a substantial portion of its depreciation
expenses by excluding real property and new or expanded
facilities in the depreciation process. While, on the other
hand, the civilian hospitals will include any item that has a
useful life greater than one year and whose cost exceeds the
dollar threshold established by law or administrative
regulation. An example of an administrative regulation that
establishes a depreciation threshold value is the $100 mini-
mum established by the California Health Facilities Commission's
Hospital Accounting and Reporting Manual, [Ref. 28].
While the UCA depreciation methodology systematically
accumulated and allocates the consumption of long-lived assets
L used in the health care delivery process, it has several draw-
backs that detract from its usefulness. Firstly, not all
capital assets are included in the depreciation process. A
substantial portion of a military treatment facility's de-
preciable assets are ignored, consequently understating the
full cost of patient care. Secondly, a composite rate of
depreciation is used that overstates the rate at which assets
are consumed by as much as 50% (Figure 13, Appendix B).
70

Thirdly, depreciation is inequitably allocated to labor-
intensive cost centers. As a result of not being able to
charge depreciation directly to a using cost center, the UCA
overstates expenses for the labor-intensive cost centers
while at the same time understating expenses for equipment-
intensive cost centers. Fourthly, depreciation's effect on
total operating expenses can not be isolated once depreciation
has been allocated to the final expense accounts. The in-
ability to isolate depreciation's effect on total operating
expenses can lead to management decisions being unduly
influenced by sunk costs. Finally, expenses associated with
the purchase of equipment in the $1,000 to $2,999 range are
being double counted in the expense allocation process. The
amount of the double counting will be approximately 12.5%
per year of the total dollar value of the equipment in the
$1,000 to $2,999 range that was put in service during the
year.
B. CONCLUSION
In determining the full cost of providing patient care,
it is essential that the cost of the capital assets used in
I. the health care delivery process be taken into consideration.
The Uniform Chart of Accounts' approach is a good starting
point in allocating the cost of capital assets to the final
operating expense accounts. However, with some adjustments
it is felt that additional benefits can be gained from the
71
I!

accumulation and subsequent allocation of depreciation
expenses. If the UCA will include all capital assets that
exceed the dollar threshold in the depreciation process,
irrespective of asset classification or source of funding,
and depreciate all capital assets on a unit straight-line
basis the resulting expenses will more closely equal the
total cost of health care delivery. Additionally, the mili-
tary treatment facilities depreciation expenses will more
closely parallel those of the civilian health care sector.
* Another adjustment that would benefit the cost collection
system would be to allocate depreciation as a direct expense
when a piece of equipment or a building can be identified
with a particular cost center. For those pieces of equipment
or buildings whose use is ubiquitous to the treatment facil-
ity, depreciation can be allocated on the basis of square
footage of building occupied, or on a ratio of either occupied
bed days or a ratio of ambulatory clinic visits. Double count-
ing of equipment expenses can be avoided if adjusting entries
are made to the NAVCOMP 2171, Functional Category/Expense
Element Report, to remove the value of equipment in the $1,000
to $2,999 range that was purchased during the reporting period.
Redesigning the Department of Defense Form 2202, Medical
Expense and Performance Report, to show the effect that
depreciation has on the cost of providing health care would
also be beneficial. Displaying depreciation as a separate
4 column on the Medical Expense and Performance Report similar
72

to the way that clinician salary expenses are currently
shown will not only show the effect depreciation has on the
total cost of patient care, but it will also help management
avoid being unduly influenced by a sunk cost when making a
cost-benefit analysis.
The foregoing adjustment will make depreciation accounting
more beneficial to the Uniform Chart of Accounts and make cost
comparisons between the military treatment facilities and theU civilian health sector more meaningful. There is however,
another area of UCA depreciation accounting that would benefit
from additional study. Such an area would be in the area of
automated property accounting. A researcher using the U. S.
Army Medical Department Property Accounting System as a
model may be able to adapt that system to the Navy Medical
Department or devise a system that, from a single data base,
would perform property accounting, automatically schedule bio-
medical equipment maintenance, and forecast future asset
requirements at a prospective replacement costs. A subfunction
of such a system would be an improved method of accumulating
depreciation expenses.
73

APPENDIX AUNIFORM CHART OF ACCOUNTS
FOR
FIXED MILITARY MEDICAL AND DENTAL TREATMENT FACILITIES
Throughout this study frequent reference will be made to
the use of depreciation as a summary account within the Uni-
form Chart of Accounts for Fixed Military Medical and Dental
Treatment Facilities (UCA). As an aid to understanding the
- effect that the UCA has on a military medical treatment
facility's expense collection and reporting, a brief descrip-
tion of the system is in order. Out of necessity the descrip-
tion of the Uniform Chart of Accounts will be brief. It will
deal only with those features of the UCA that the author feels
are essential to understanding the workings of the system.
Those readers desiring a more detailed description of the
Uniform Chart of Accounts are invited to read the Department
of Defense Instruction 6010.10M where the subject of thisLi? appendix is dealt with at great length.
A. DESCRIPTION1
The Uniform Chart of Accounts is an expense collection
and reporting system that allocates patient care cost to six
Unless otherwise indicated, the bulk of the informationabout the Uniform Chart of Accounts was extracted from Depart-ment of Defense Instruction 6010.10M [Ref. 4].
74
I'

functional accounts: Inpatient care, Ambulatory Care, Dental
Care, Ancillary Services, Support Services, and Special Pro-
grams. Each functional account is further divided into sum-
mary and subaccounts (Figure 2).
r- L
Stib :cont Sbacat (2 E ESubaccount
Figure 2
Two functional accounts, Support Services and Ancillary
Services are intermediate operating accounts. The other four
functional accounts are final expense accounts. Expenses col-
lected in intermediate accounts are allocated to the final
accounts via a step-down process that is based on either per-
formance factors or units of service measurements. The UCA is
arranged in a hierarchy in which the functional accounts appear
at the top and subaccounts are at the bottom.
Regardless of their position in the hierarchy, there are
four elements that are common to all accounts:
1. Function Element
Contains a description of the type of activity
characteristic of the account. The functional description
tells what type and level of services were provided, administra-
tive duties performed and such other data as required to clearly
75

distinguish between accounts in order to facilitate the rational
accumulation of cost data and work performance measurements.
2. Cost Element
Identifies the operating expenses incurred in operat-
ing and maintaining a discrete functional or organizational
subdivision (workcenter) of a military medical facility.
3. Performance Element
A measure of work produced by a work center, i.e.,
patient visit, occupied bed day, square footage of building
occupied, weighted procedure, etc.
4. Assignment Procedure
A method of cost allocation that distributes the
operating expenses of the two intermediate operating expense
accounts to the final operating expense accounts.
As a means of assisting in the understanding of the
UCA classification a brief description will be given as to
how functional accounts, summary accounts, and subaccounts
are classified.
a. Functional Accounts
(1) Inpatient Care account provides for the
examination, diagnosis, treatment, and disposition of inpatients.
Inpatients are those individuals who are admitted to a bed in
a medical treatment facility which has authorized or designated
beds for inpatient medical or dental treatment. This is an
account into which all operating expenses of the seven major
ri inpatient care summary accounts, medical Care, Surgical Care,
76

Obstetrical and Gynecological Care, Pediatric Care, Ortho-
pedic Care, Psychiatric Care, and Ophthalmology and Otorhino-
laryngology Care are summarized. This summarization repre-
sents the total cost of inpatient care. The performance
factor used to measure the work produced is the occupied bed
day.
(2) Ambulatory Care accounts provide for accumula-
tion of expenses associated with patient care relative to
professional advice and consultation, examination, diagnosis,
treatment and disposition of all categories of inpatients and
outpatients 2presenting themselves to the various ambulatory
clinics. The Ambulatory Care account is an account into
* which all of the operating expenses associated with the major
Ambulatory Care summary accounts are summarized (refer to page
81 for a listing of major ambulatory care accounts).
(3) Dental Care account provides for the sum-
marization of expenses associated with delivering comprehensive
dental care to armed forces members, certain former members
(subject to availability of space and capabilities of the
staff) and providing dependent dental care in certain well
defined circumstances. This is a final operating expense
account which shall include all of the operating expenses
* incurred in operating and maintaining Dental Centers and
2An outpatient is an individual receiving health care foran actual or potential disease or injury that does not require
4 admission to a medical treatment facility for inpatient care.
77

Clinics. There are no specific performance measures for this
functional account.
(4) Ancillary Services account accumulates the
summarized expenses associated with those activities that
participate in the care of patients principally by assisting
and augmenting the talents of the attending physician and
dentist in diagnosing and treating human ills. Generally,
ancillary services do not have primary responsibility for the
management of patients. Rather, patient services are provided
'. on order of the attending physician or dentist. The Ancillary
Service account shall be a summary account which will include
all of the operating expenses summarized in the major ancil-
*lary summary accounts listed on page 82 paragraph (4). It
should be noted that the order of accounts listed in paragraph
(d) is identical to the order of the step-down process used
to allocate expenses to the final operating expense accounts.
The performance factor used to measure workload are weighted
procedures [Ref. 4].
(5) Support Services account is provided to accumu-
late the expenses necessary to direct and support the mission
assigned to the medical treatment facility. With the excep-
tion of the Depreciation account, Support Services perform the
management and administrative functions of Ref. 12:
Command and Administrative Support Service
Personnel Support Service
Public Works
78

Material Service
Housekeeping and Janitorial Services
Biomedical Equipment Repair
Linen and Laundry Service
Inpatient Food Service
N Ambulatory Care Administration
This account will summarize all of the operating expenses of
the major support services, including depreciation, outlined
U above. It will be noted that when Depreciation is placed at
the top of the list of accounts outlined above, the listing
is identical to the order of step-down used during the assign-
ment of expenses to the final operating expense accounts.
There are no performance factors associated with this account
since the Support Services account is used only as a summary
account in which to totalize and report cost of the major
inclusive accounts.
(6) Special Programs account summarizes the expen-
ses of a military treatment facility which are incurred as a
result of performing those portions of its mission other than
direct patient care. This account is essential in order to
preclude these expenses from being charged to the facilityvs
direct patient care accounts. Paragraph 3a, page 7 contains
a listing of the primary summary accounts associated with
this functional account. Since this account exists only as a
repository of summarized expenses from the primary summary
accounts associated with Special Programs, there is no
associated performance factor.
79

b. Sunnary Accounts and Subaccounts
(1) Summary accounts are the second level of the
UCA hierarchy and services as a collection point for cost data.
As indicated by their names, summary accounts generally co-
incide with the services that are performed by the treatment
facility. The number of summary accounts in each functional
account ranges from one in Dental Care to eleven in Ambulatory
Care. Generally the summary accounts are self-explanatory
and the discussion about them in this paper will be limited
to listing the summary accounts under their general functional
heading. If a more detailed explanation is desired, the
reader is invited to read the applicable portions of the De-
partment of Defense Instruction 6010.10 (series).
(2) Subaccounts are the lowest level of accounts
in the UCA hierarchy. They are generally accounts that are
identifiable performance units [Ref. 12]. Subaccounts can be
established in any manner deemed appropriate by the facility
commander. These accounts are used to accumulate the initial
operating expenses associated with a workcenter. They are
used to meet diverse internal needs of the various military
medical treatment facilities. The only constraints on sub-
accounts are that they be assigned to the proper summary ac-
4# count during the reassignment and summarization process
(Ref. 12]. Subaccounts make the UCA sufficiently flexible
to allow the identification of expenses with an individual
unit or as a means of aggregating operating expenses into a
common pool for allocation to the proper summary accounts.
80
L-

- .c. Account Listings According to Function
The following accounts are listed in hierarchial
order. That is, the major heading is the function account,
followed by the summary account, and finally the subaccount
is listed. As a means of illustration and in the interest of
brevity, subaccounts will only be listed for the Inpatient
Care and Ambulatory Care summary account "Medical Care". A
more detailed listing of subaccounts is contained in the
Department of Defense Instruction 6010.10M, "Uniform Chart
of Accounts for Fixed Military Medical and Dental Treatment
Facilities". For example, the Internal Medicine subaccount
would be listed under the functional account Inpatient Care
and the summary account Medical Care:
(1) Inpatient Care (functional account)
(a) Medical Care (summary account)
Internal Medicine (subaccount)
Cardiology
Coronary Care Unit
Dermatology
*Endocrinology
Gastroenterology
Hematology
Intensive Care (Medical)
Nephrology
Neurology
*4 Oncology
81
• I ' | i i ' m ' ,i -- o"

Pulmonary/Upper Respiratory Disease
K Rheumatology
Medical Care Not Elsewhere Classified!ii
(b) Surgical Care
(c) Obstetrical and Gynecological Care
(d) Pediatric Care
(e) Orthopedic Care
(f) Psychiatric Care
(2) Ambulatory Care
(a) Emergency Medical Care
(b) Flight Medicine Care
(c) Family Practice Care
(d) Medical Care
Internal Medicine Clinic
Allergy Clinic
Cardiology Clinic
Dermatology Clinic
Diabetic Clinic
Endocrinology (metabolic) Clinic
Gastroenterology Clinic
Hematology Clinic
Hypertension Clinic
Nephrology Clinic
Neurology Clinic
Nutrition Clinic
Oncology Clinic
82

Pulmonary Disease Clinic
Rheumatology Clinic
Medical Clinics Not Elsewhere Classified
(e) Obstetrical and Gynecological Care
(f) Orthopedic Care
(g) Pediatric Care
(h) Primary Medical Care
(i) Psychiatric/Mental Health Care
(j) Surgical Care
(3) Dental Care
(a) Dental Service
(b) Type 3 Dental Prosthetic Laboratory
(c) Type 2 Dental Prosthetic Laboratory
(4) Ancillary Services
(a) Pharmacy
(b) Pathology
(c) Radiology
(d) Special Procedures Service
(e) Central Sterile Supply/Material Services
(f) Surgical Service
(g) Same Day Service
(h) Rehabilitative Services
(i) Nuclear Medicine
83
4-

(5) Support Services
(a) Depreciation
(b) Command and Administrative Support Services
(c) Personnel Support Services
(d) Public Works
(e) Material Services
(f) Housekeeping and Janitorial Service
(g) Biomedical Equipment Repair
(h) Linen and Laundry Service
(i) Inpatient Food Service
(j) Inpatient Affairs
(k) Ambulatory Care Administration
(6) Special Programs
(a) Specified Health Related Programs
(b) Public Health Service
(c) Health Care Services Support
(d) Military Unique Medical Activities
(e) Patient Movement and Military PatientAdministration
B. EXPENSE REASSIGNMENT PROCEDURE
Expenses incurred for support and ancillary services are
allocated to the final operating expense accounts by a cost
assignment methodology that contains five steps. They are:
Step 1: Non-personnel direct expenses and performance
data are assigned to the appropriate intermediate and final
operating expense accounts.
84

Step 2: Full-time equivalent man-months and salary
expenses are distributed to the intermediate and final operat-
-ing expenses.
Step 3: A pre-step down purification of cost within and
to medical treatment facility accounts' is done within this
step. Many of the support and ancillary services accounts
require that the expense charged to an account be prorated
* based on a unit of service, performance factor or other
criteria. This step-down can be done during Step 3 as a
purification procedure before step-down or by the allocation
process of Step 4. If the expense in question does not
include overhead expenses then Step 3 is used. If the cost
to be allocated includes overhead expenses then the cost
allocation procedures of Step 4 should be uspd. Purification
is the process of reassigning expenses from one operating
expense account to one or more other operating expense ac-
counts with the sole objective of recognizing the benefitting
function or activity for which the work was performed. Pu-
rification during Step 3 will not include any expenses re-
assigned from other accounts. Any reassignment of stepped-
down expenses will be done in Step 5.
Step 4: Expenses of the intermediate operating expense
t j accounts and cost pools are assigned through a step-down
process to the final operating expense accounts during this
step.
85
14

Step 5: Post-step-down purification of the final operat-
ing expense accounts is done during this step. Based on a
performance factor or unit of service, stepped-down expenses
assigned to final operating expense accounts can be reassigned
to another expense account. For example, inpatient or am-
bulatory expenses may be charged to a special program account
such as the Alcohol and Drug Abuse/Rehabilitation program
account. If there is a purification (reassignment) of expenses
from Ambulatory Care to a Special Program account there must
be a corresponding reduction in the number of visits reported
by the Ambulatory Care account. The number of occupied bed
days reported by the Inpatient Care accounts will not be af-
fected by any reassignment of expenses to or from Inpatient
Care accounts.
Table 11 is an example of a truncated expense assignment
worksheet that illustrates the step-down procedures used to
allocate expenses from the intermediate expense accounts to
the final accounts.
After the allocation procedures have been completed and
the intermediate expense accounts are closed, a Medical
Expense and Performance Report is submitted to the Office ofL
the Surgeon General. This report is submitted on a quarterly
basis. It consists of five parts, Parts I through IV provide
statistical data and Part V provides for a narrative summary.
86d.

0800 8800 §s sss ss 0 Cr. = 4C .qt .o -m r.4. 4AM ft
C00 00 0000 0008
0 00o
%. AnCm r.at 4
00 00 0c0 000 0 00a 000 O 00 00 00 000 0 00. 0
m O 04- 00 %n C" 0 0 1A1 ml e'b
InN [CA) 000 00 000 00 00204r4 " 400 00 0
cc 00 0 0
0~~ r, 0' 0%O
I 000 00 000 00 000010QD 10 0 000 00 0 0c c0 0a
0% 018 0 0 w 0%00 in i n 1" 0
-i 4
000 00 000 0 00000C, " o00 0 =0 0c a
0 00 1000 00 00Nn -
I 4114MiOr ac! co cc 0c cIdC!ii so~& 04 0 co 0
8710 0

C. CONCLUSION
As stated at the beginning, this description of the Uni-
form Chart of Accounts is admittedly cursory in scope. How-
ever, it is hoped that the brief explanation was sufficient
to provide a basic understanding of the UCA to those familiar
with the Uniform Chart of Accounts for Military Medical Treat-
ment Facilities.
8
.°.-8
"a

APPENDIX B
STATISTICAL ANALYSIS OF THE UNIFORM CHART OF ACCOUNTS
COMPOSITE RATE OF DEPRECIATION
* A. INTRODUCTION
A basic assumption underlying the use of a composite life
of eight years is that the eight years is representative of
the average asset's useful life and that there have been no
material changes in either the composition of assets or in
the assets service lives [Ref. 91. As a test of the validity
of the eight-year assumption a series of 5 samples of size
30 were drawn from the equipment inventory lists from seven
*:- Naval Regional Medical Centers (NPMC). Samples from five of
the NRMCs were from the Equipment File List dated December
1979 on file at the Bureau of Medicine and Surgery, Navy
Department, Washington, DC. Samples for the NRMC, Long
Beach, CA were taken from that facility's Master Property
List as of 8 June 1980. NRMC, Camp Lejeune, NC samples were
drawn from the Item Category Report of equipment to be in-
cluded in the new facility under construction.
The tests that were done on the samples were computations
for means, standard deviations, confidence intervals, Runs
Test for Randomness, and a Kruskall-Walls One-Way Analysis of
Variance.
Except for NRMC Long Beach, CA each sample was drawn over
an interval where 30 items would be selected from the
89
4'°

facility's equipment list. NRMC Long Beach's samples were
drawn using a simple random sampling technique. Interval
sampling was selected as the primary means of obtaining
samples because of its simplicity and ease with which it could
be used with the format of the equipment list from which the
samples would be drawn. Interval sampling is the simplist
selection technique to use, and if used with care, it can
provide a reasonable degree of assurance that the sample had
been selected at random [Ref. 29].
B. MEAN, STANDARD DEVIATION, AND CONFIDENCE INTERVAL
Samples were drawn from the foregoing listings. A mean,
standard deviation and confidence interval was calculated for
each sample. Sample means were calculated as using the
formulas outlined in Wonnacott [Ref. 321.
1 nx z x.n- i=l 1
variance:
2 1 n (2S2 _ - E (X. - )n-i i=l J
Standard Deviation: S =J Variance
Confidence Interval: CI =X + t 025
4-i025
90
ff I- , -i-'- ' : ' , ... ... ... ... . . ;. ............ :. . .. ..... .. . . . .

where:
= estimated useful service life of each item
n =number of items in the sample (n =30)
0 2 5 =. Student's t variable for a confidenceinterval at 95%
Table 14 shows the results of the foregoing computations.
C. RUNS TEST FOR RANDOMNESS
As a means of verifying that the samples were selected at
* random a series of Runs Test for Randomness were performed.
Using the sample means a Runs Test for Randomness [Ref . 341
* were performed to determine if the samples were truly selected
at random. The null hypothesis H being that the samples were0
drawn at random. According to Wonnacott [Ref. 34], whenH0
is true the path of the observations crosses the sample median
frequently; pergo when His not true this happens much less
frequently. Accept H if and only if prob-value is greater0
than 5%.
In general there are 30 observations in each sample.
When His true, the distribution of the number of Runs (r)
is approximately normal with an expected mean value of:
n +1E(R) -7 Where n =the number of itemsin the sample
The expected Variance of the Runs Test is:
var~) =n(n-2) =(n-1)
.44
91

Using the normal approximation: Pr(r<UR)
can be determined [Ref. 34]. R
For example, take two samples one sample of 30 where the
equipment service lives crosses the median line a total of
6 times and a second sample where the observations crossed
the median line 15 times, the following prob-values would
be seen:
E(r) =30 + 1 =16
2
Var(r) = 30-1 = 7.25
4
Pr(6-16)
7.25
Pr(3.7)
Prob-Value = .0005 which indicates that the sample is not
random. On the other hand, in Sample Two with 15 runs:
Pr(15-16)
7.25
Pr(.37)
Prob-Value = .36 which strongly supports the assertio; that
the sample was selected at random. Table 12 is a tabulation
of the results of the Runs Test for Randomness. The results
of the Runs Test support the claim that the samples were
drawn at random.
92

TABLE 12
RUNS TEST FOR RANDOMNESS
NAVAL REGIONAL MEDICAL CENTER
Sample Bethesda Lejuene Charleston San Diego Pendleton Long Beach Oakland
1 .23 .36 .07 .13 .23 .36 .23
2 .14 .23 .23 .07 .03 .07 .03
3 .23 .36 .07 .36 .13 .24 .13
4 .23 .36 .36 .05 .23 .13 .23
5 .14 .36 .36 .36 .23 .07 .23
D. ONE-FACTOR ANALYSIS OF VARIANCE
A One-Factor Analysis of Variance was used to determine if
the samples for the individual NRMC's were drawn from the same
population. The answers sought were to the question, "Are the
sample means different because of differences in the underlying
population means? Or may the differences in sample means be
reasonably attributed to chance fluctuations?" Using the
methodology outlined by Wonnacott [Ref. 34] Table 13 shows
the calculations used to answer the foregoing questions.
E. KRUSKAL-WALLIS ONE-WAY ANALYSIS OF VARIANCE
The next step was to determine if the samples came from
identical populations with respect to the sample averages.
Accordingly, the Kruskall-Wallis One-Way Analysis of Variance
was selected as a useful device for testing the null hypothesis
that the samples came from identical populations [Ref. 33].
93

Table 13
Variance Analysis Results
Source of Variations Degrees of Variance F - RatioVariation Sum of Squares Freedom Mean Sum of Squares
(SS) (MSS)
Between Rows: P (\ --."explained" by TI ~ Xidifferene in , = ExplainedMeans Variance_Unexplained
VarianceWithin Rows:residual vari- 2 5-5ation resulting~ x~from chanceflucuations"unexplained"
*Total 0(i)X (71.%
Sample MeansBethesda Lejeune Charleston San Diego Pendleton Long Beach Oakland12.8 11.9 10.7 11.8 11.7 11.2 12.611.7 12.9 9.2 10.1 11.8 10.0 11.0
- 12.0 13.0 10.4 12.4 12.9 10.4 11.212.4 11.4 9.0 11.3 13.3 10.3 12.413.5 13.6 9.5 11.8 11.2 10.5 11.6
- 12.5 12.6 9.8 11.5 12.2 10.5 11.8 XiF-Ratio1.26 1.3 1.9 1.9 1.28 .43 1.35Prob-Value
.25 .25 .05PV< .1 .05CPVC.I0 .25 .25 .25Ho: UI = U2 = U3 = U4 = U5 Level of Significance is 5%
Decision: Reject H0 if and only if prob-value less than 5% or ifF-Ratio greater than 2.37
The F-Ratios in all cases were less than 2.37 and the prob-values were allgreater than 5%. Ho therefore cannot be rejected. The difference in samplemeans can be reasonably explained by chance fluctuations (Ref. 34).
94

. . . . -- -
Table 14Listing of Sample
Means, Standard Deviations and Confidence Intervals
NRMC, Bethesda, MdMean 12.8 11.7 12.0 12.4 13.5Standard Deviation: 3.6 2.4 3.4 4.8 3.8Confidence Interval:(11.5,14.1) (10.8,12.6) (10.7,13.3)(11.0,13.8)(11.1,14.9)Average CI: (11.7, 13.3)
NRMC, Camp Lejeune, NCMean 11.9 12.9 13.0 11.4 13.6Standard Deviation: 1.2 1.8 1.6 1.6 1.6Confidence Interval:(10.6,13.1) (11.1,14.6) (11.4,14.6)(9.8,13,0)(12.0,15.2)Average CI: (11.5, 13.5)
R MC, Charleston, SCMean 10.7 9.2 10.4 9.0 9.5Standard Deviation: 4.4 2.4 2.8 2.4 2.3Confidence Interval:(9.1,12.3) (8.3,10.1) 9.4,11.4) (9.8,13.0)(12.0,15.2)Average CI: (9.0, 10.6)
NRMC, San Diego, CAMean 11.8 10.1 12.4 11.3 11.8Standard Deviation: 1.4 0.9 1.4 1.2 1.3Confidence Interval:(10.4,13.2) (9.8,10.4) (11.9,12.9)(10.9,11.7)(11.3,12.3)Average CI: (10.6, 12.4)
NRMC, Camp Pendleton, CAMean 11.7 11.8 12.9 13.3 11.2Standard Deviation: 4.1 3.6 4.7 4.9 2.8Confidence Interval:(10.2,13.2) (10.5,13.1) (11.2,14.6)(11.5,15.1)(10.2,12.2)Average CI: (11.2, 13.1)
NRMC, Long Beach, CA* Mean 11.7 11.8 12.9 13.3 11.2
Standard Deviation: 1.3 1.3 1.1 1.4 1.5Confidence Interval:(9.9,12.5) (8.7,11.5) (9.3,11.5) 8.9,11.7)(9.0,12.0)Average CI: (10.0,11.0)
-RMC, Oakland, CAMean 12.6 11.0 11.2 12.4 11.6Standard Deviation: 3.3 3.0 3.9 3.5 3.0Confidence Interval:(11.4,13.8) (9.9,12.1) (9.8,12.6) (11.1,13.7)(10.5,12.7)Average CI: (11.0, 12.6)
95
i:
,,f ~ i 1 A ~ . .- . - -- - - - - - - -

AD-R127 823 DEPRECIATION ACCOUNTING IN THE UNIFORM CHRRT OF 2/2ACCOUNTS(U) NAVAL POSTGRADUATE SCHOOL MONTEREY CAC L GEORGE DEC 82
UNCLASSIFIED F/G 6/5 NL
IE E.'

1.0 Alto LIM,.
.M18
IjIJ -2 JIM8
MICRCOP REOUTO TESCAR
NAINA1 URA1f11NDRS-%-

In computing the Kruskal-Wallis Test, each sample average
was replaced by ranks. The smallest rank was replaced by 1,
the next smallest rank by 2, and the largest rank by N. Tied
averages were given the mean of the ranks for which tied.
The Kruskal-Wallis test determines whether the sums of ranks
are so disparate that they are not likely to have come from
samples drawn from identical populations [Ref. 33]. According
to Siegel (Ref. 331, it can be shown that if the null hypothesis
(Ho ) is true, and the samples are from identical populations,0
then the Kruskal-Wallis test statistic is distributed as a
Chi Square with degrees of freedom equal to (k-i) where k
equals the number of samples. Therefore, if the observed
value of the Kruskal-Wallis test statistic is less than the
value of Chi Square at the stated level of significance, the
H may be accepted at that level of significance.
Table 15 shows the results of the Kruskal-Wallis test.
Following Siegel's example, the null hypothesis that the
samples were drawn from identical populations can be accepted
at the 5% level of significance. The critical value for chi
square at 5% significance level with 34 degrees of freedom is
48.6 (Ref. 34]. The Kruskal-Wall.s test statistic is 23.34.
F. CONCLUSION
Based on the foregoing analysis of 35 random samples, it
is the author's contention that the samples came from identical
* populations. The analysis further supports the challenge
96

c c 00o v 0-4
0D 0o -4 -4 N -4 e-I Go4 0. 0 ~(L U ) -
o C wO w r- m 4I - ) C.)o a 0; Q P *0-4 Q)0) -4I 04 E a -E -4
X r-4 r-4 r-4 r--4 -) OE0 0l U
cr.n -- (n in "n00
04 0 N4 m LA (L0 0% -Y 'v-c - r-4 "I 0
a r-4 U) rq- .-
w 2 OrflO 4-)- -4 rIzin()
u) 0 in
0~m0 00
Inn MJ 0 C Cin .0) m W I6% 4 0r
0D C r- O ON M- N U)&DI) C C 4 -4 r-I c n
r- -9 -4-4 -4 1
o1 C it -4 ~0 -Y NYcIIcPy"n
tn ~0) c m U
f-eN C ICNh 0.C o 0 0 0% 0 M% Q)
C- c C M 04) G3C~4 (A-4 4
E-) X. r- > l -
0n 0 N r-4
(0 c - N -V 0 I
Q4 N~u 4~~ MI - M 4) a
4 4a. 0y 0Z 0 Tcc
u-I- > 4 i
97cn r .
............................

that the average useful life of the equipment used at the
Naval Regional Medical Centers is higher than the composite
eight year service life used in the Uniform Chart of Accounts
to determine the annual depreciation expense to charge to
patient care.
- 9
98

LIST OF REFERENCES
1. Gibson, Robert M., National Health Expenditure, 1978,Health Care Financing Review, Summer 1979.
2. Rice, Donald B., Defense Resource Management Study andSupporting Papers, Feb. 1979.
3. Department of Defense, Military. Health Care Study,Dec. 1975.
4. Department of Defense Instruction 6010.10M, UniformChart of Accounts for Fixed Military Medical and DentalTreatment Facilities.
5. Grant, Eugene L. and Norton, Paul T., Depreciation* Revised, Ronald Press Company, 1955.
6. Miller, Martin A., GAAP Guide, Harcourt, Brace Jovanovich,
1979.
7. Seawell, L. Vann, Introduction to Hospital Accounting,
Revised, Hospital Financial Management Association,1977.
8. Meigs, Walter B. and others, Intermediate AccountingSolution Manual, 3rd Edition, McGraw-Hill Book Company,1974.
9. Meigs, Walter B. and others, Intermediate Accounting,3rd Edition, McGraw-Hill Book Company, 1974.
10. Berretta, Philip L., Regional Controller, Kaiser Founda-tion Health Plan Inc., Oakland, California. InterviewJuly 1980.
11. Kaiser Foundation Health Plan Inc., Standard Proceduresfor Property Accounting, 1976.
12. Hasselbald, Gary, Director of Finance, Community Hospitalof the Monterey Peninsula, Monterey, California. Inter-view May 1980.
13. Skull, Gary, Controller, Grace Hospital Inc., Morganton,North Carolina, Interview July 1981.
14. Bishop, Wil, Financial Director, California HospitalAssociation, Sacramento, California. Interview August1980.
99
, . . ..

15. Navy Department, Bureau of Medicine and Surgery, Equip-ment File List, Naval Regional Medical Center, Charleston,S. C., January 1980.
16. Naval Regional Medical Center, Camp Lejeune, N. C.,Item Category Report February, 1979.
17. Daniels, Jeri, Fiscal Officer, Naval Regional MedicalCenter, Long Beach, California. Interview August 1981.
18. Naval Regional Medical Center, Long Beach, California,Master Property List, June 1980.
19. Naval Regional Medical Center, Bremerton, Washington,Item Category Report, January 1980.
20. Fiscal Officer, Naval Regional Medical Center, Bremerton,Washington. Interview July 1981.
21. Seawell, L. Vann, Hospital Financial Accounting:Theory and Practice, Hospital Financial ManagementAssociation, 1975.
22. Department of the Navy, Bureau of Medicine and Surgery,Investment Equipment Instruction 4235.5G, 1979.
23. Department of the Navy, Bureau of Medicine and SurgeryMessage R052240Z Mar 80, Unclas N07043 Threshold Change
* -to Investment Equipment Costs.
24. Ferrara, William L., Responsibility Accounting - A BasicControl Concept: Readings in Cost Accounting, Budgetingand Control, South-Western Publishing Co., Cincinnati,4th Ed., 1973.
25. Cost Accounting Standards Board, Rules and Regulations:Standard 409 - Depreciation of Tangible Capital Assets,40FR4264, 1975.
26. Department of the Navy, Office of the ComptrollerFinancial Management of Resources, Publication NumberNAVSO P3006-I, 1980.
27. Comptroller General of the United States, AccountingPrinciples and Standards for Federal Agencies, Title 2,1978.
28. California Health Facilities Commission, HospitalAccounting and Reporting Manual, Jul 1978.
100

," . . *.
29. Department of the Navy, Bureau of Medicine and Surgery,Uniform Chart of Accounts Analysis of Inpatient Care,Report Number 20381-M02 Jul 1980.
30. Department of the Navy, Bureau of Medicine and Surgery,Uniform Chart of Accounts Analysis of Ambulatory Care,Report Number 20381-M04 Jul 1980.
31. Horngren, Charles T., Cost Accounting; A ManagerialEmphasis, Prentice-Hall Inc., 1972.
32. Sawyer, Lawrence B., The Practice of Modern InternalAuditing, Institute of Internal Auditors, 1973.
33. Siegel, Sidney, Nonparamedic Statistics for the Behav-ioral Sciences, McGraw-Hill Book Company, 1956.
34. Wonnacott, Thomas H. and Wonnacott, Ronald J., Intro-ductory Statistics, 3rd Ed., John Wiley and Sons, 1977.
101

INITIAL DISTRIBUTION LIST
No. Copies
1. Defense Technical Information Center 2Cameron StationAlexandria, VA 22314
2. Defense Logistics Studies Information ExchangeU. S. Army Logistics Management CenterFort Lee, VA 23801
3. Library, Code 0142 2Naval Postgraduate SchoolMonterey, CA 93940
4. Assoc. Professor Shu S. Liao, Code 54LcDepartment of Administrative SciencesNaval Postgraduate SchoolMonterey, CA 93940
5. Assoc. Professor David R. Whipple, Code 54WpDepartment of Administrative SciencesNaval Postgraduate SchoolMonterey, CA 93940
6. Department Chairman, Code 54Js 1Department of Administrative SciencesNaval Postgraduate SchoolMonterey, CA 93940
7. LT Charles L. George, MSC, USN 3Box 95Naval Regional Medical CenterCharleston, SC 29408
102
. . . . . .

wr? :4
-ie1-
"A
f 2 z