Embed Size (px)
Citation preview

CZ3253: Computer Aided Drug designCZ3253: Computer Aided Drug design
Lecture 1: Drugs and Drug Development Lecture 1: Drugs and Drug Development Part I Part I
Prof. Chen Yu ZongProf. Chen Yu Zong
Tel: 6874-6877Tel: 6874-6877Email: Email: [email protected]@nus.edu.sghttp://xin.cz3.nus.edu.sghttp://xin.cz3.nus.edu.sg
Room 07-24, level 7, SOC1, Room 07-24, level 7, SOC1, National University of SingaporeNational University of Singapore

22
History
33
History
Ancient knowledge of the materials that could relieve
pain, alter moods and perceptions, aid against infection,
poison etc.
The first written treatises were generated by the Chinese
e.g. Pen Tsao was written ~2700 B.C., describing uses
and classifications of medicinal plants.
44
History
The ancient Egyptians by 1550 B.C. had written
prescriptions using a range of pharmaceutically
active ingredients and vehicles for their delivery. At
about the same time, similar medical advances were
being made in Babylonia and India.
Between about 400-300 B.C. the Greeks made
enormous advances in the knowledge of anatomy
and physiology.
55
History
Philippus Theophrastus Bombastus von Hohenheim (1493-1541), also known as Aureolus Paracelcus, took up the pharmacological baton.
He is often referred to as the ‘grandfather of pharmacology’ and also the ‘grandfather of toxicology’ because of his impact on the understanding between dose and response
“All things are poisons, for there is nothing without poisonous qualities. It is only the dose which makes a thing a poison”.

66
History
No real further advances until the sciences of chemistry and physiology had developed:
• To provide pure compounds.
• Allow careful monitoring of their physiological effects.
This combination of circumstances arose in the early 19th Century.

77
History
Modern Drug Development
Random screening against disease assays
Natural products, synthetic chemicals
Rational drug design and testing
• Speed-up screening process
• Efficient screening (focused, target directed)
• Computer aided drug design (target directed)
• Integration of testing into design process
• Fail drugs fast (remove hopeless ones as early as possible)
88
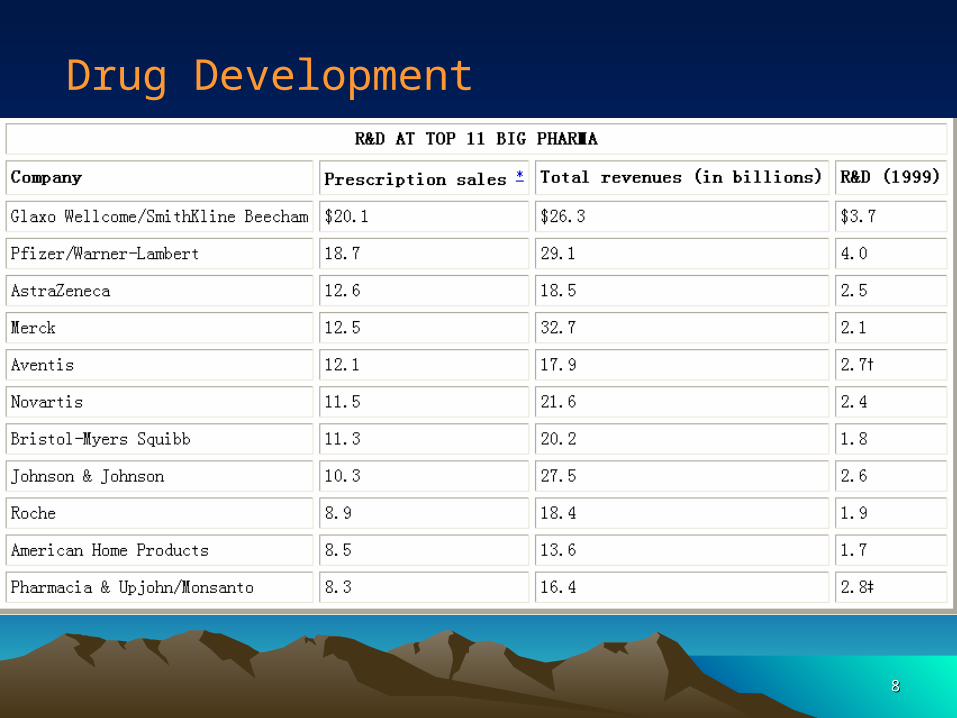
Drug Development
99
Traditional Drug Design Traditional Drug Design Methods: Methods: Random screeningRandom screening
• Long design cycle: 7-12 years.
• High cost: $350 million USD per marketed drug.
Drug Discovery Today 2, 72-78 (1997)
Too slow and costly to meet demand.
1010
Strategies for improving Strategies for improving design cycle:design cycle:
• Smart screening: – High-throughput robotic screening.
• Diversity of chemical compounds:– Combinatorial chemistry.
Nature 384 Suppl., 2-7 (1996)
High expectation.
1111
Any Other Alternative Approach?Any Other Alternative Approach?
• Current situation:– Molecular mechanism of disease processes,
structural biology.– Rising cost of experimental equipment and
resources.– Computer revolution (low cost, high power).– Software development.
Natural Conclusion: Computer approach?
1212
Strategies for improving design cycle:Strategies for improving design cycle:
• Computer-aided drug design:
– Receptor 3D structure unknown: • QSAR.
– Receptor 3D structure known: • Ligand-protein docking.
Science 257, 1078-1082 (1992)
Definition of receptor given later
1313
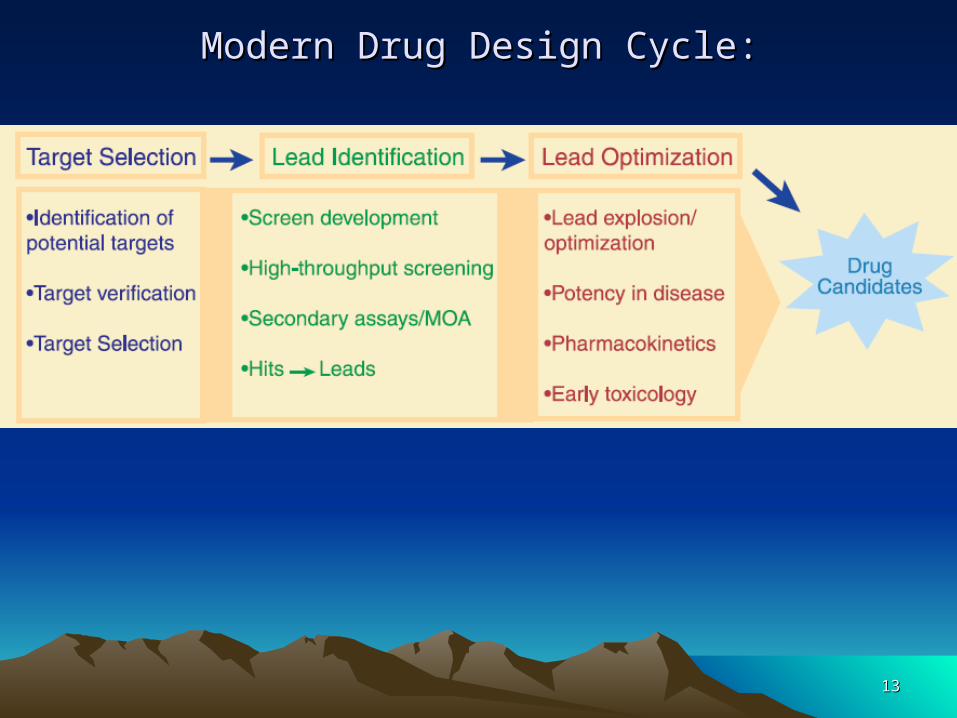
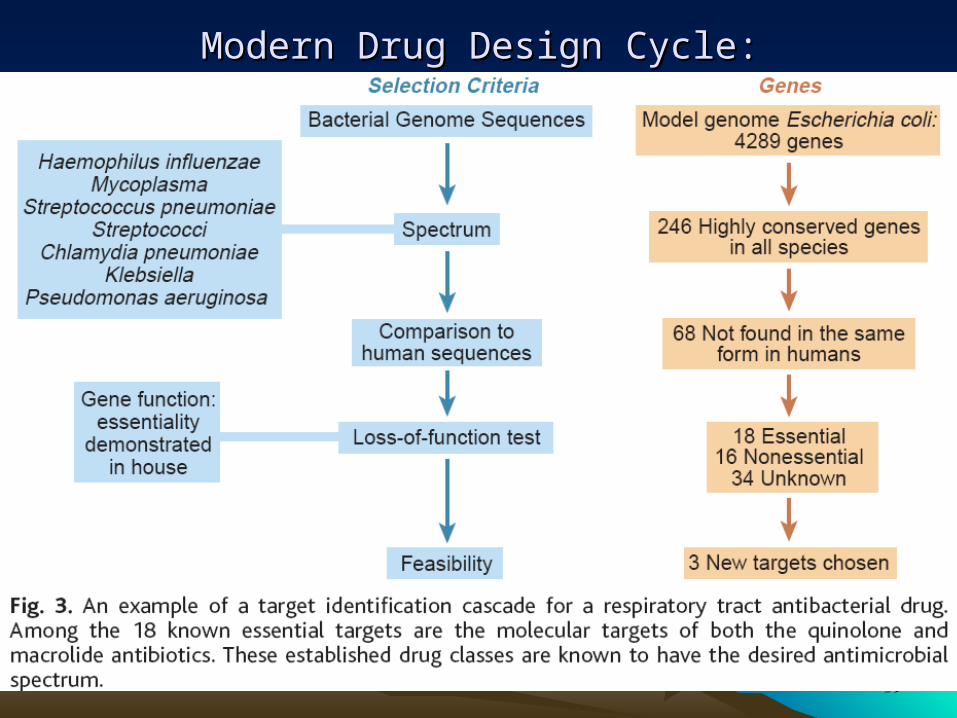
Modern Drug Design Cycle:Modern Drug Design Cycle:

1414
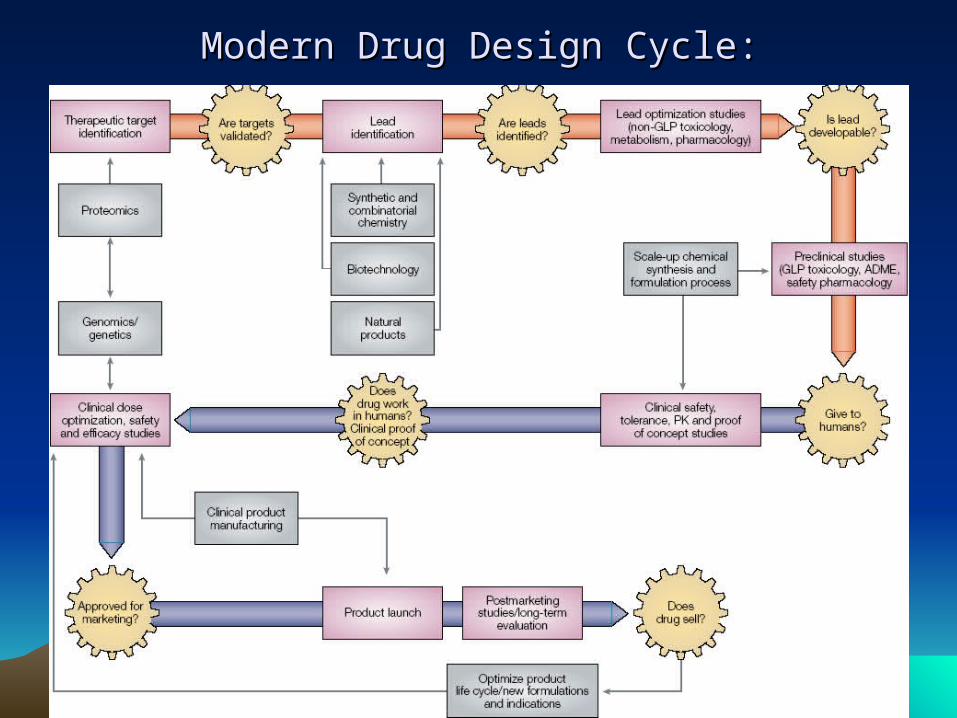
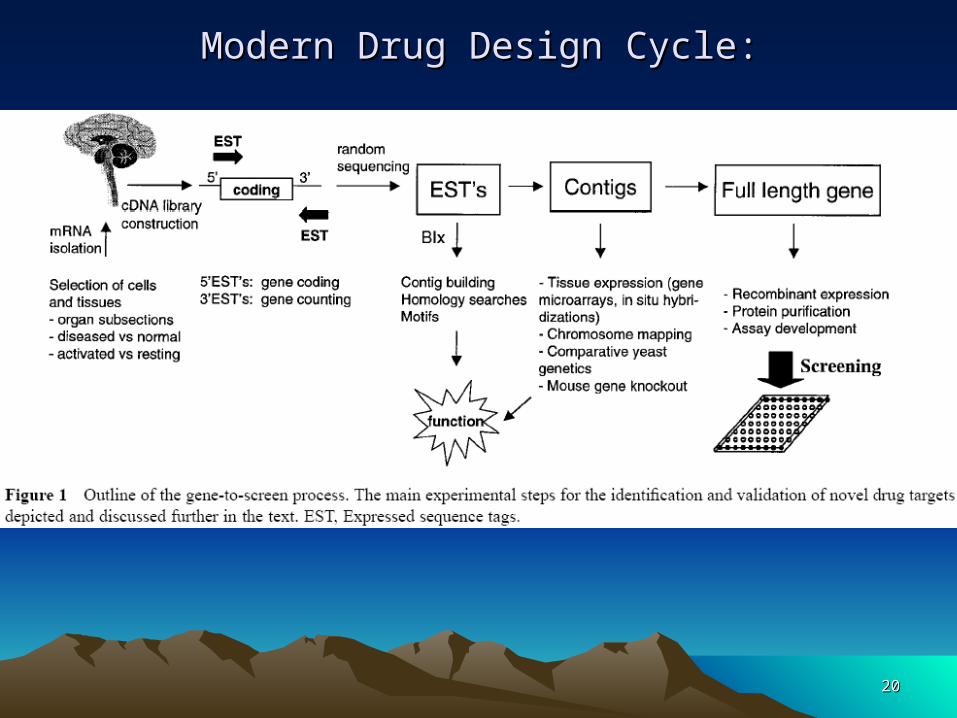
Modern Drug Design Cycle:Modern Drug Design Cycle:

1515
Modern Drug Design CycleModern Drug Design Cycle
1616
Modern Drug Design Cycle:Modern Drug Design Cycle:

1717
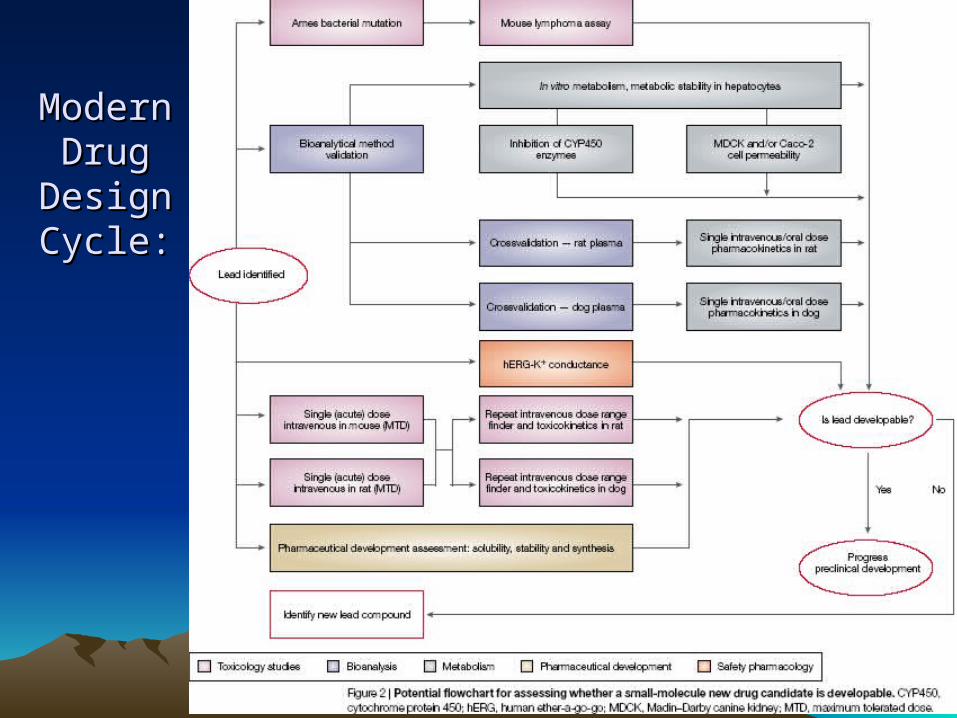
Modern Drug Modern Drug Design Cycle:Design Cycle:
1818
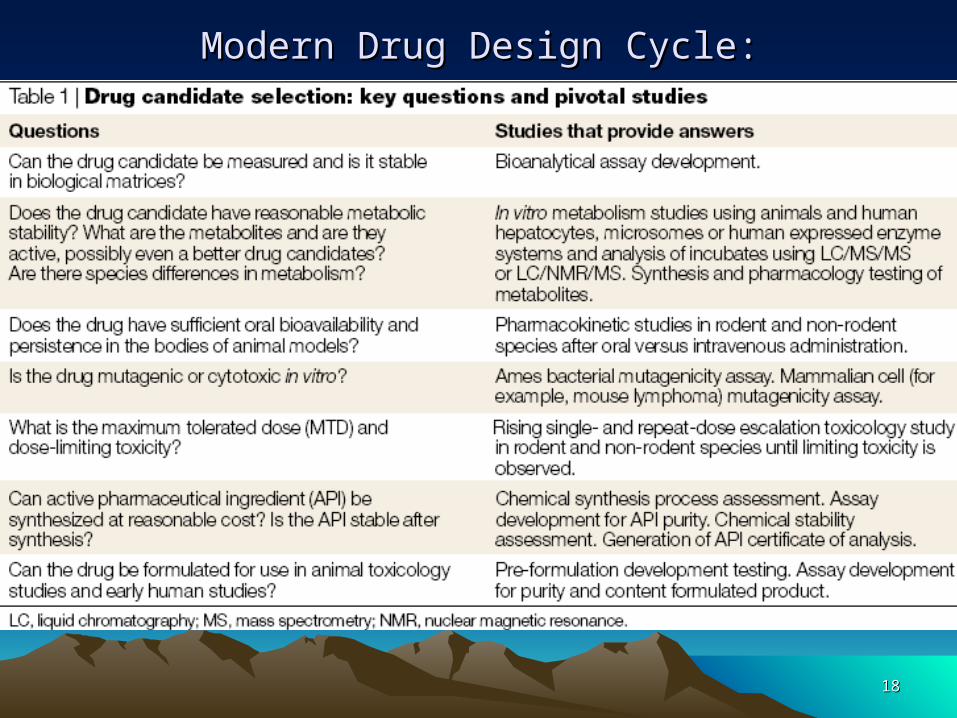
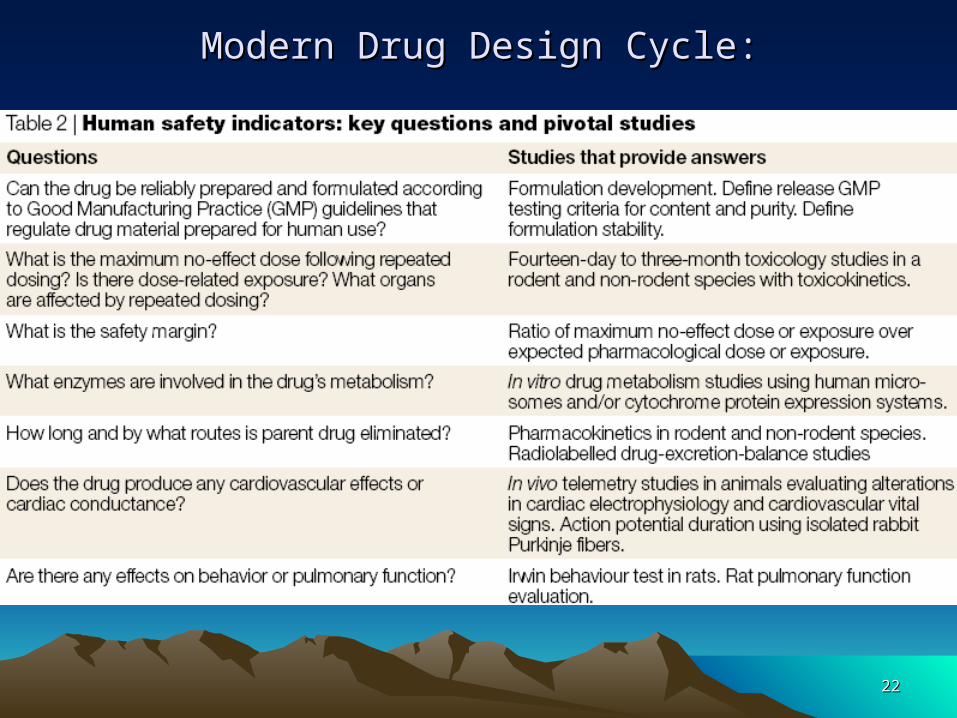
Modern Drug Design Cycle:Modern Drug Design Cycle:
1919
Modern Drug Design Cycle:Modern Drug Design Cycle:
2020
Modern Drug Design Cycle:Modern Drug Design Cycle:
2121
Modern Modern Drug Drug
Design Design Cycle:Cycle:
2222
Modern Drug Design Cycle:Modern Drug Design Cycle:
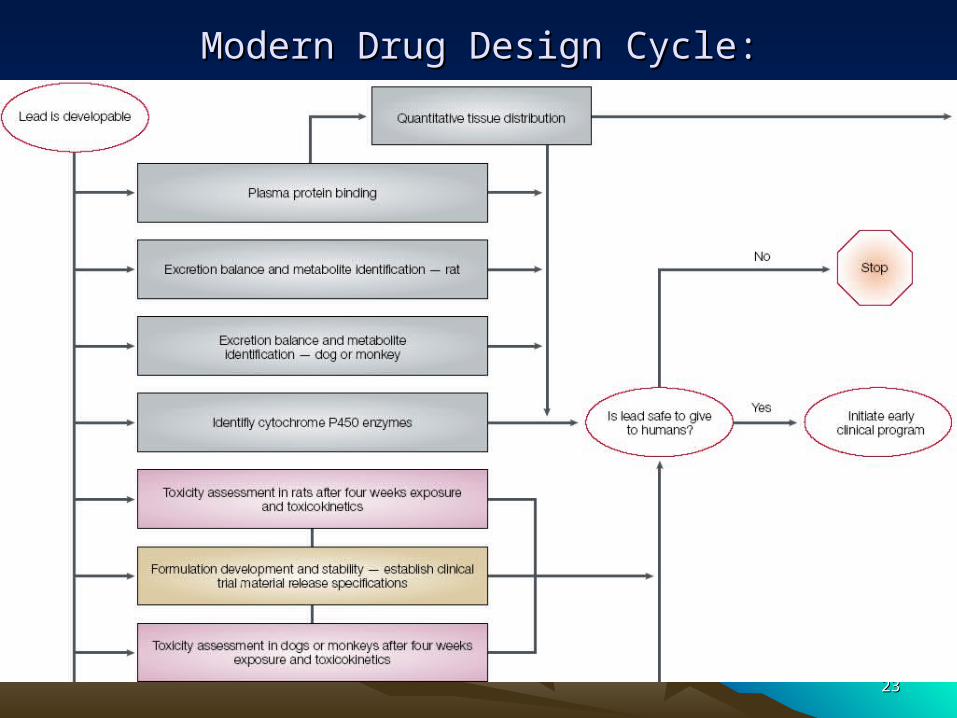
2323
Modern Drug Design Cycle:Modern Drug Design Cycle:
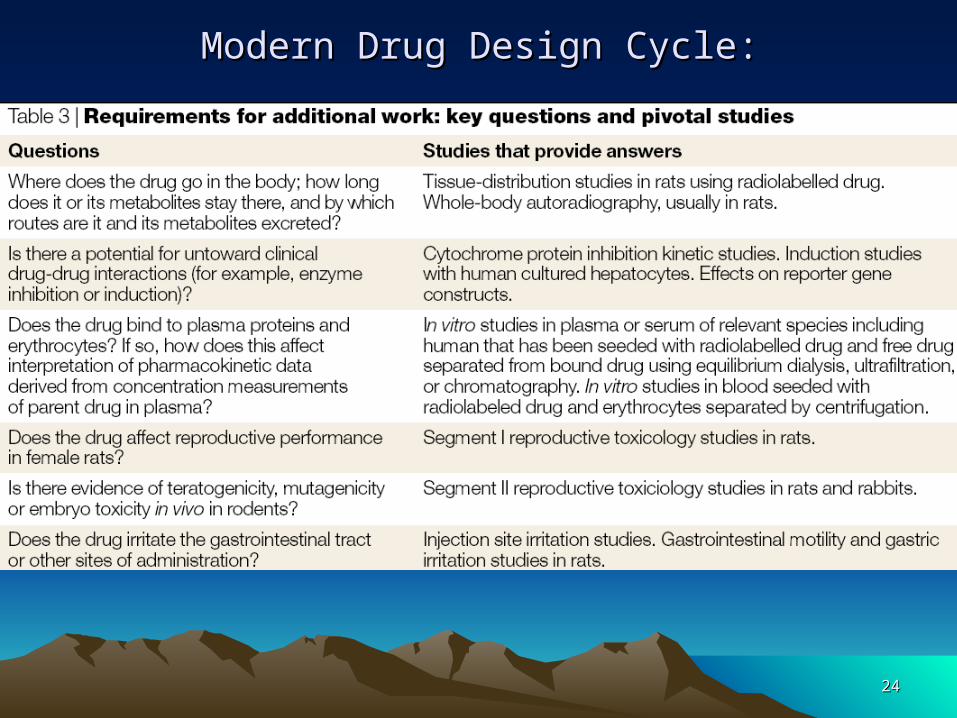
2424
Modern Drug Design Cycle:Modern Drug Design Cycle:
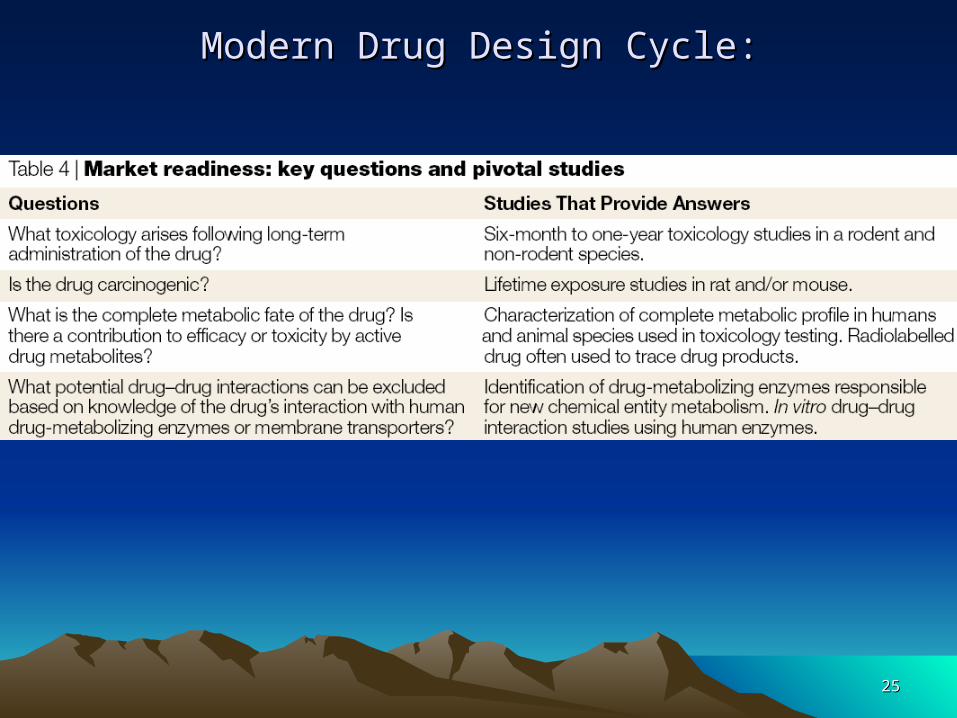
2525
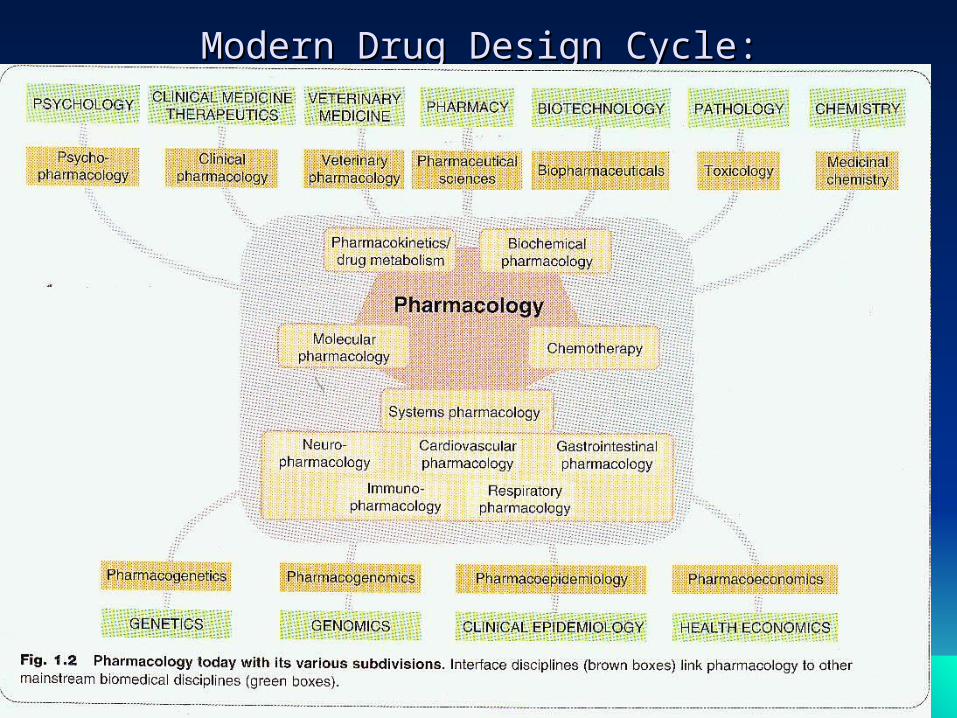
Modern Drug Design Cycle:Modern Drug Design Cycle:

2626
Modern Drug Design Cycle:Modern Drug Design Cycle:
2727
Modern Drug Design Cycle:Modern Drug Design Cycle:
2828
Definitions
Xenobiotic: A chemical that is not endogenous to an organism.
Endogenous: Made within.
Drug: A chemical taken that is intended to modulate the current physiological status quo.
Ligand: A chemical that binds to another molecule, such as a receptor protein.
Bioavailability: The amount or proportion of drug that becomes available to the body following its administration.
Pharmacokinetics: What the body does to a drug.
Pharmacodynamics: What a drug does to the body .

2929
Drug action
A drug is a compound that can modify the response of a tissue
to its environment.
A drug will exert its activity through interactions at one or more
molecular targets.
• The macromolecular species that control the functions of
cells.
• May be surface-bound proteins like receptors and ion
channels or
• Species internal to cells, such as enzymes or nucleic
acids.
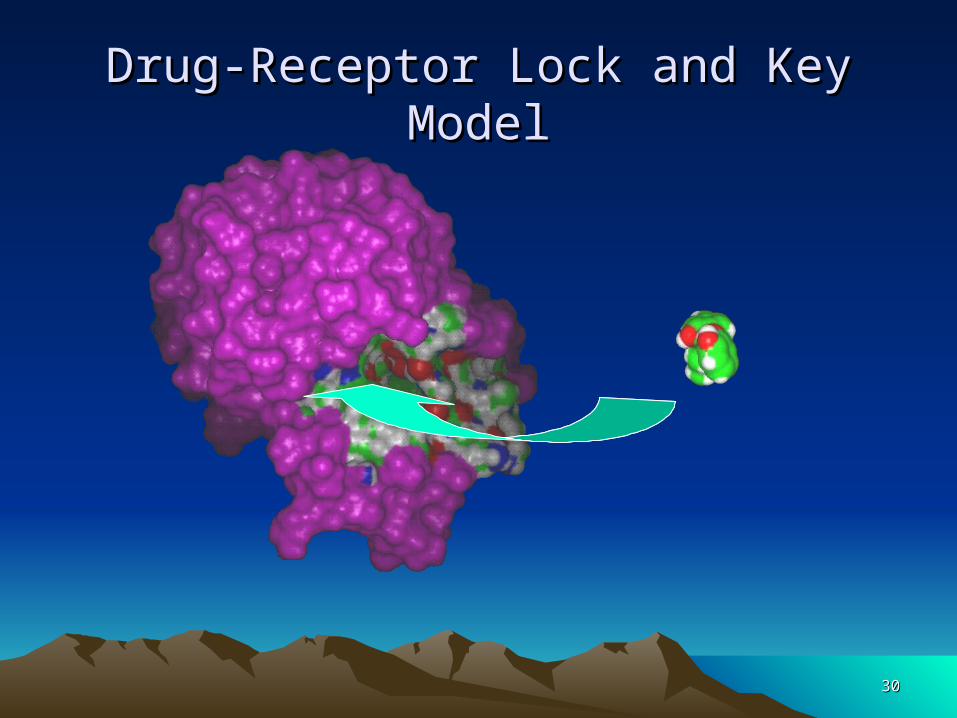
3030
Drug-Receptor Lock and Key ModelDrug-Receptor Lock and Key Model
3131
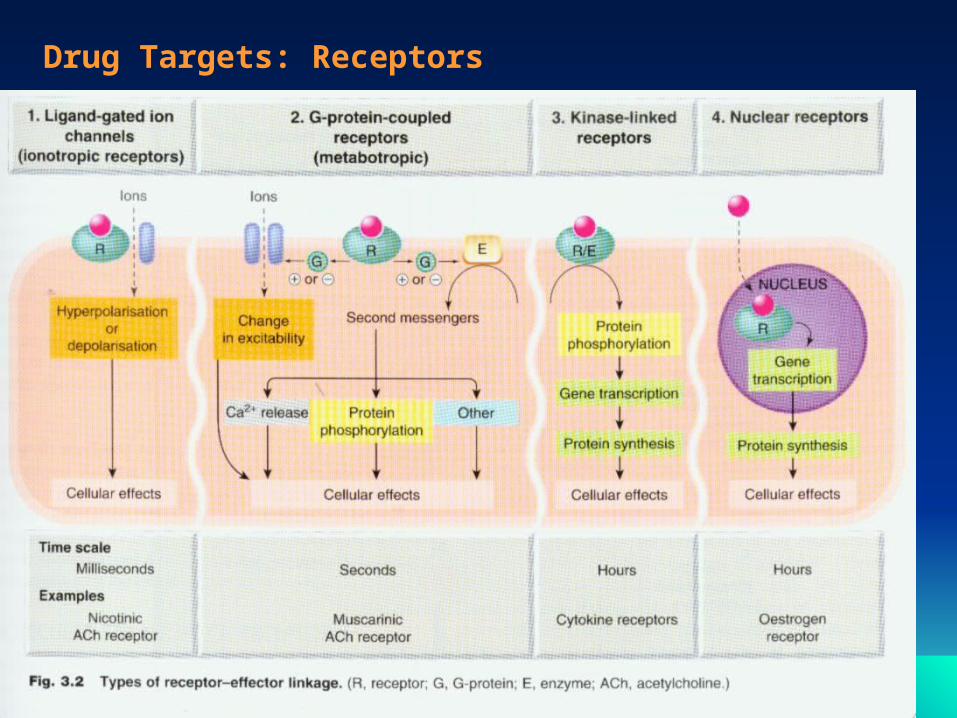
Drug Targets: Receptors
Receptors are the sites at which biomolecules such as
hormones, neurotransmitters and the molecules responsible
for taste and odour are recognised.
A drug that binds to a receptor can either:
• Trigger the same events as the native ligand - an agonist.
Or
• Stop the binding of the native agent without eliciting a
response - an antagonist.
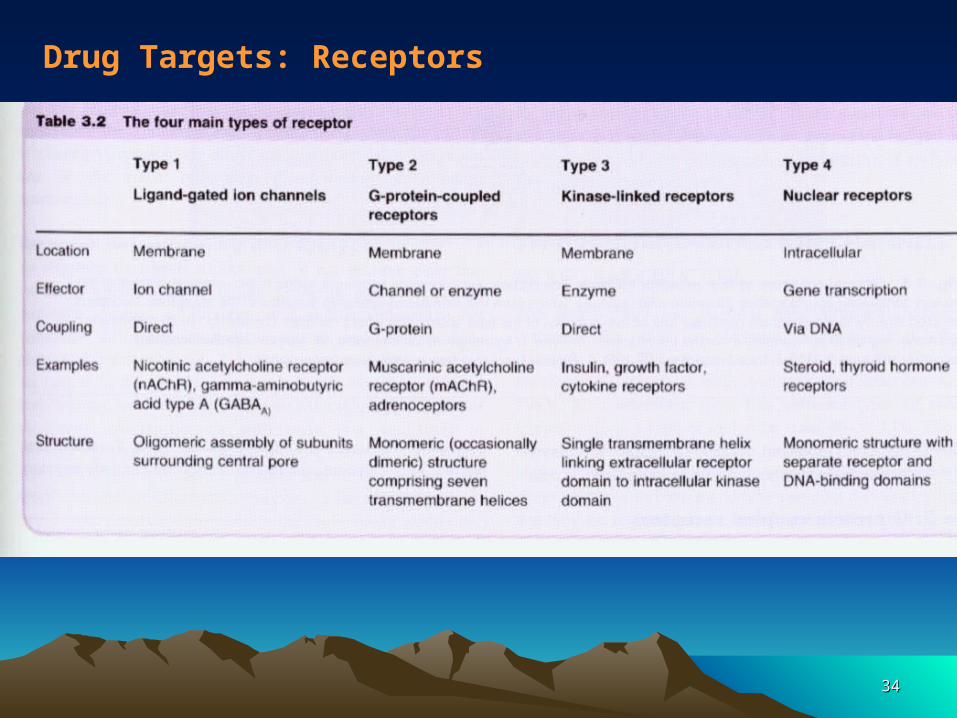
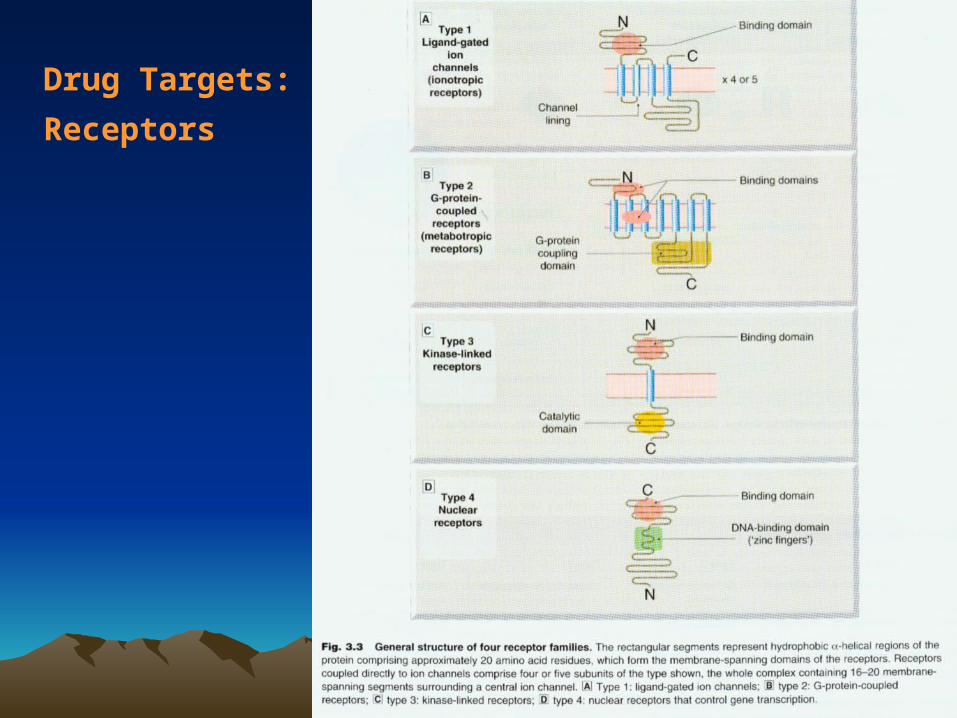
There are four ‘superfamilies’ of receptors.
3232
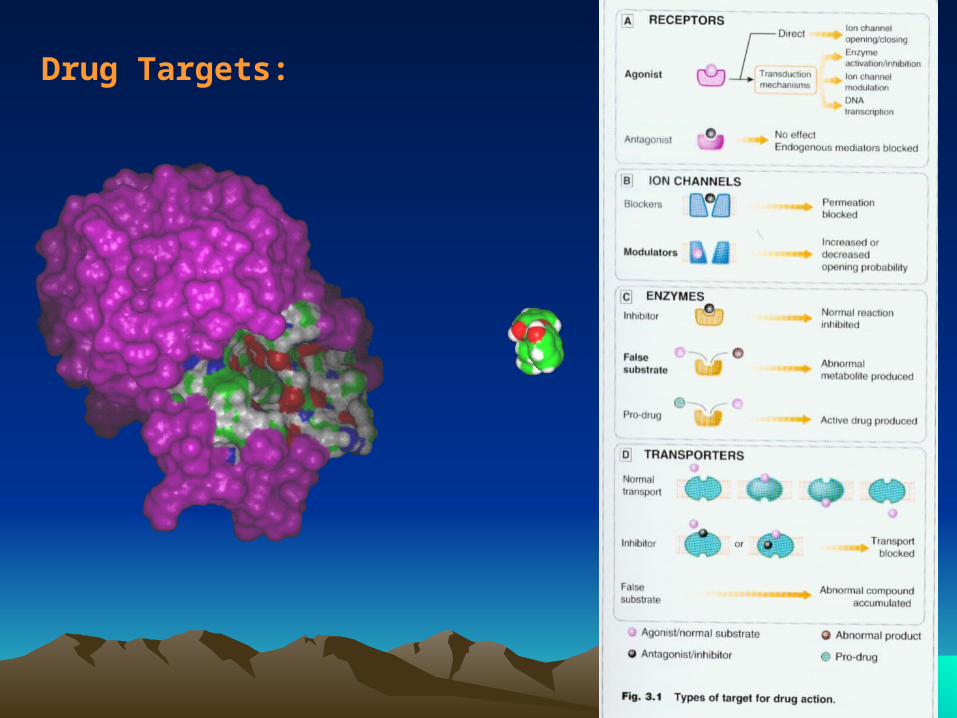
Drug Targets:
3333
Drug Targets: Receptors
3434
Drug Targets: Receptors
3535
Drug Targets:
Receptors
3636
Drug Targets: Enzymes
They are proteins that catalyse the reactions required for cellular function.
Generally specific for a particular substrate, or closely related family of substrates.
Molecules that restrict the action of the enzyme on its substrate are called inhibitors.
Inhibitors may be irreversible or reversible.
Reversible inhibitors may be:
• Competitive.
• Non-competitive.
Enzyme inhibitors might be seen to allow very ‘fine control’ of cellular processes.
3737
Drug targets: Nucleic acids
Potentially the most exciting and valuable of the available drug targets.
BUT designing compounds that can distinguish target nucleic acid sequences is not yet achievable.
There are compounds with planar aromatic regions that bind in-between the base pairs of DNA or to the DNA grooves.
These generally inhibit the processes of DNA manipulation required for protein synthesis and cell division.
• Suitable as drugs for applications where cell death is the goal of therapy - such as in the case of the treatment of cancer.
• Name another use where cell death is desirable.
3838
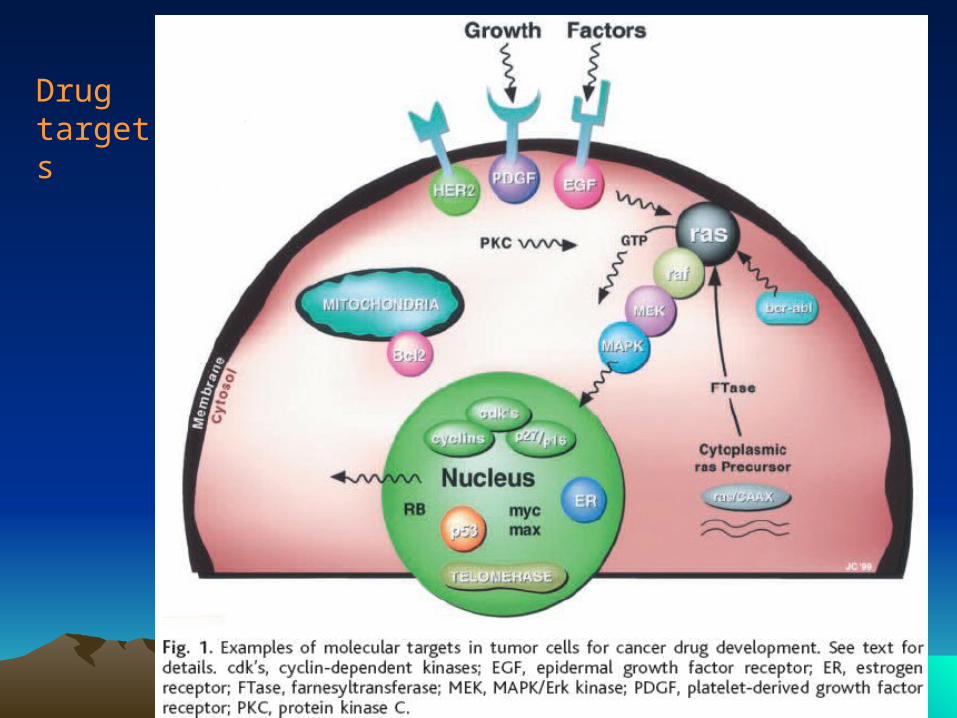
Drug targets

3939
Drug targets