Embed Size (px)
Citation preview
1817 West Braker Lane, Building F, Suite 200, Austin, TX 78758 Phone 512.583.2000 • Fax 512.583.2011 • www.revenuecycleinc.com
1817 West Braker Lane, Building F, Suite 200, Austin, TX 78758 • Phone 512.583.2000 • Fax 512.583.2002 • www.revenuecycleinc.com
Work product, information and guidance provided by Revenue Cycle Inc. are subject to the terms and limitations provided at http://www.revenuecycleinc.com/disclaimer. By using this information or guidance, you agree to such terms and limitations.
CY 2016 Final Rule Summary
Hospital Outpatient Prospective Payment System
(HOPPS)
Provided To:
Revenue Cycle Inc. Client
Prepared On:
November 3, 2015
Work product, information and guidance provided by Revenue Cycle Inc. are subject to the terms and limitations provided at http://www.revenuecycleinc.com/disclaimer. By using this information or guidance, you agree to such terms and limitations.
1817 West Braker Lane, Building F, Suite 200, Austin, TX 78758 • Phone 512.583.2000 • Fax 512.583.2002 • www.revenuecycleinc.com
Page 2 of 14
Introductory Summary
On October 30, 2015 the Centers for Medicare and Medicaid Services (CMS) issued the final rule for the Hospital
Outpatient Prospective Payment System (HOPPS) for CY 2016.
HOPPS Final Rule Highlights
The CY 2016 may be located in its entirety by following the link below:
https://s3.amazonaws.com/public-inspection.federalregister.gov/2015-27943.pdf
This document in PDF form is 1221 pages in length. The format of the information on the following pages
is intended to summarize information contained within the final rules pertaining to radiation oncology
services.
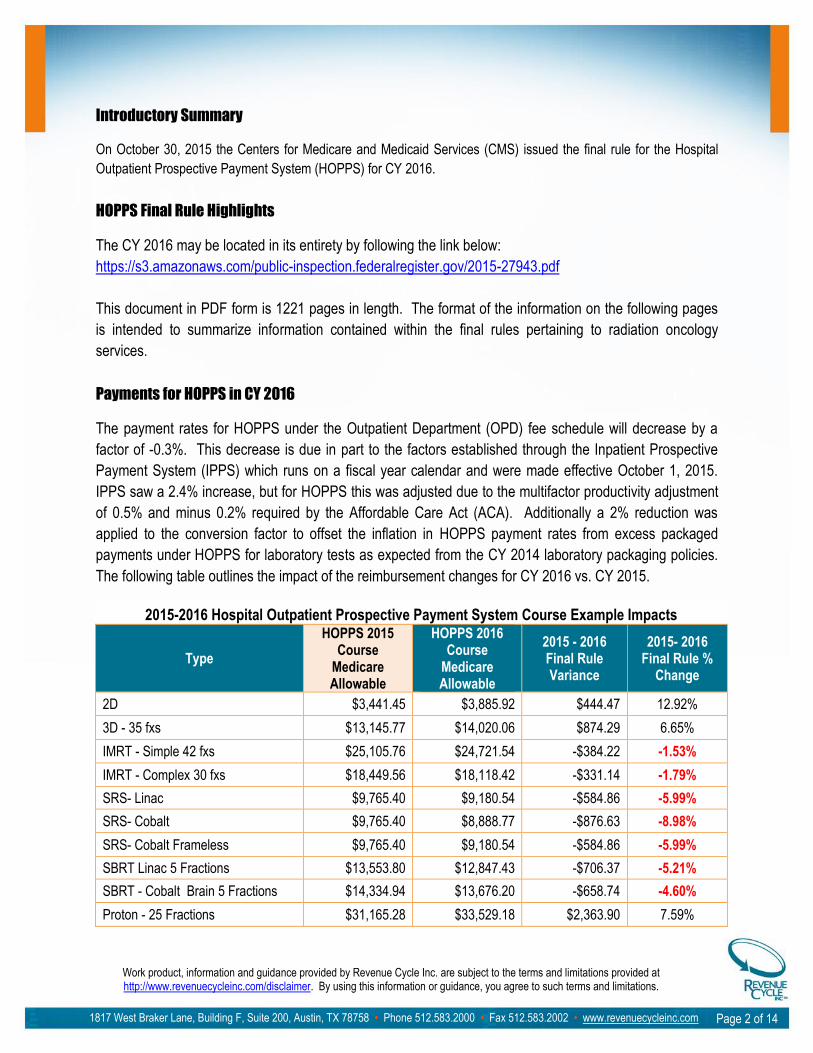
Payments for HOPPS in CY 2016
The payment rates for HOPPS under the Outpatient Department (OPD) fee schedule will decrease by a
factor of -0.3%. This decrease is due in part to the factors established through the Inpatient Prospective
Payment System (IPPS) which runs on a fiscal year calendar and were made effective October 1, 2015.
IPPS saw a 2.4% increase, but for HOPPS this was adjusted due to the multifactor productivity adjustment
of 0.5% and minus 0.2% required by the Affordable Care Act (ACA). Additionally a 2% reduction was
applied to the conversion factor to offset the inflation in HOPPS payment rates from excess packaged
payments under HOPPS for laboratory tests as expected from the CY 2014 laboratory packaging policies.
The following table outlines the impact of the reimbursement changes for CY 2016 vs. CY 2015.
2015-2016 Hospital Outpatient Prospective Payment System Course Example Impacts
Type
HOPPS 2015 Course
Medicare Allowable
HOPPS 2016 Course
Medicare Allowable
2015 - 2016 Final Rule Variance
2015- 2016 Final Rule %
Change
2D $3,441.45 $3,885.92 $444.47 12.92%
3D - 35 fxs $13,145.77 $14,020.06 $874.29 6.65%
IMRT - Simple 42 fxs $25,105.76 $24,721.54 -$384.22 -1.53%
IMRT - Complex 30 fxs $18,449.56 $18,118.42 -$331.14 -1.79%
SRS- Linac $9,765.40 $9,180.54 -$584.86 -5.99%
SRS- Cobalt $9,765.40 $8,888.77 -$876.63 -8.98%
SRS- Cobalt Frameless $9,765.40 $9,180.54 -$584.86 -5.99%
SBRT Linac 5 Fractions $13,553.80 $12,847.43 -$706.37 -5.21%
SBRT - Cobalt Brain 5 Fractions $14,334.94 $13,676.20 -$658.74 -4.60%
Proton - 25 Fractions $31,165.28 $33,529.18 $2,363.90 7.59%
Work product, information and guidance provided by Revenue Cycle Inc. are subject to the terms and limitations provided at http://www.revenuecycleinc.com/disclaimer. By using this information or guidance, you agree to such terms and limitations.
1817 West Braker Lane, Building F, Suite 200, Austin, TX 78758 • Phone 512.583.2000 • Fax 512.583.2002 • www.revenuecycleinc.com
Page 3 of 14
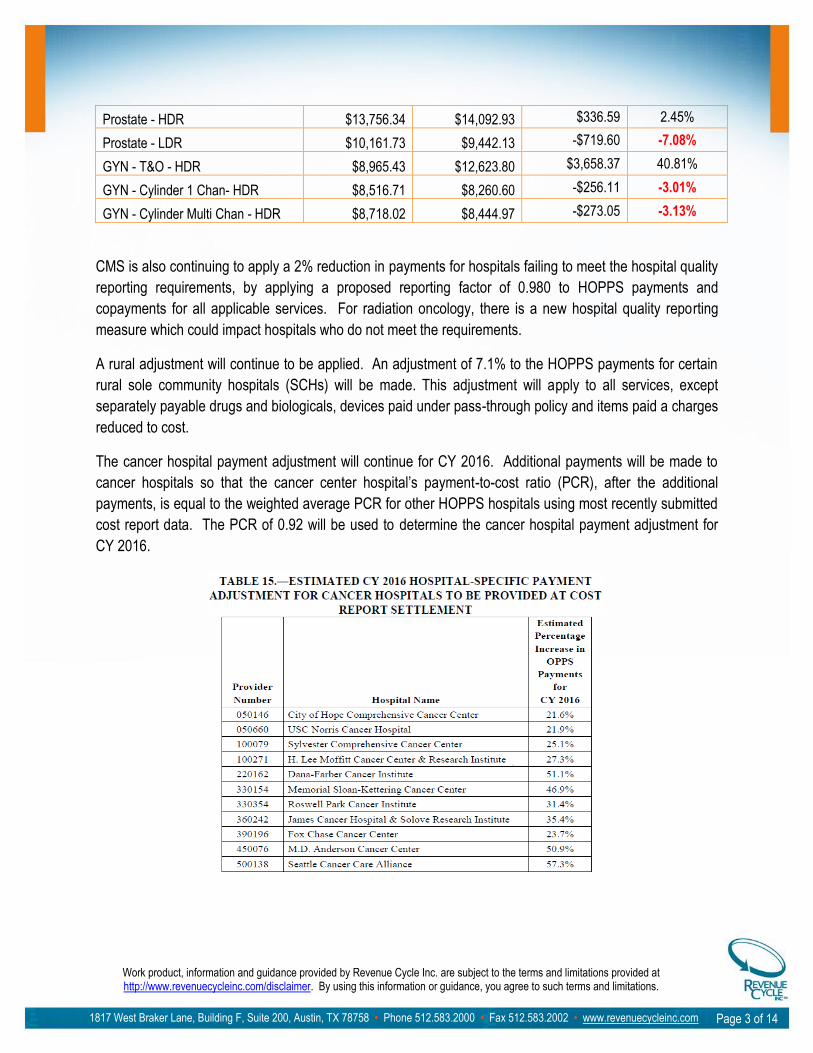
Prostate - HDR $13,756.34 $14,092.93 $336.59 2.45%
Prostate - LDR $10,161.73 $9,442.13 -$719.60 -7.08%
GYN - T&O - HDR $8,965.43 $12,623.80 $3,658.37 40.81%
GYN - Cylinder 1 Chan- HDR $8,516.71 $8,260.60 -$256.11 -3.01%
GYN - Cylinder Multi Chan - HDR $8,718.02 $8,444.97 -$273.05 -3.13%
CMS is also continuing to apply a 2% reduction in payments for hospitals failing to meet the hospital quality
reporting requirements, by applying a proposed reporting factor of 0.980 to HOPPS payments and
copayments for all applicable services. For radiation oncology, there is a new hospital quality reporting
measure which could impact hospitals who do not meet the requirements.
A rural adjustment will continue to be applied. An adjustment of 7.1% to the HOPPS payments for certain
rural sole community hospitals (SCHs) will be made. This adjustment will apply to all services, except
separately payable drugs and biologicals, devices paid under pass-through policy and items paid a charges
reduced to cost.
The cancer hospital payment adjustment will continue for CY 2016. Additional payments will be made to
cancer hospitals so that the cancer center hospital’s payment-to-cost ratio (PCR), after the additional
payments, is equal to the weighted average PCR for other HOPPS hospitals using most recently submitted
cost report data. The PCR of 0.92 will be used to determine the cancer hospital payment adjustment for
CY 2016.
Work product, information and guidance provided by Revenue Cycle Inc. are subject to the terms and limitations provided at http://www.revenuecycleinc.com/disclaimer. By using this information or guidance, you agree to such terms and limitations.
1817 West Braker Lane, Building F, Suite 200, Austin, TX 78758 • Phone 512.583.2000 • Fax 512.583.2002 • www.revenuecycleinc.com
Page 4 of 14
Outlier payments are provided by CMS to assist in mitigating high-cost complex procedures where the APC payment may create a scenario in which the hospital is presented with a significant financial loss when performed. CMS will continue providing outlier payments to those who meet the specific criteria in CY 2016. In order to qualify in CY 2016, the hospital’s cost of furnishing the service must exceed the 1.75 times multiplier threshold to the APC payment, and that amount must be more than $3,250. When this criterion is met 50% of the amount by which the service exceeds the 1.75 times APC payment amount will be paid to the hospital.
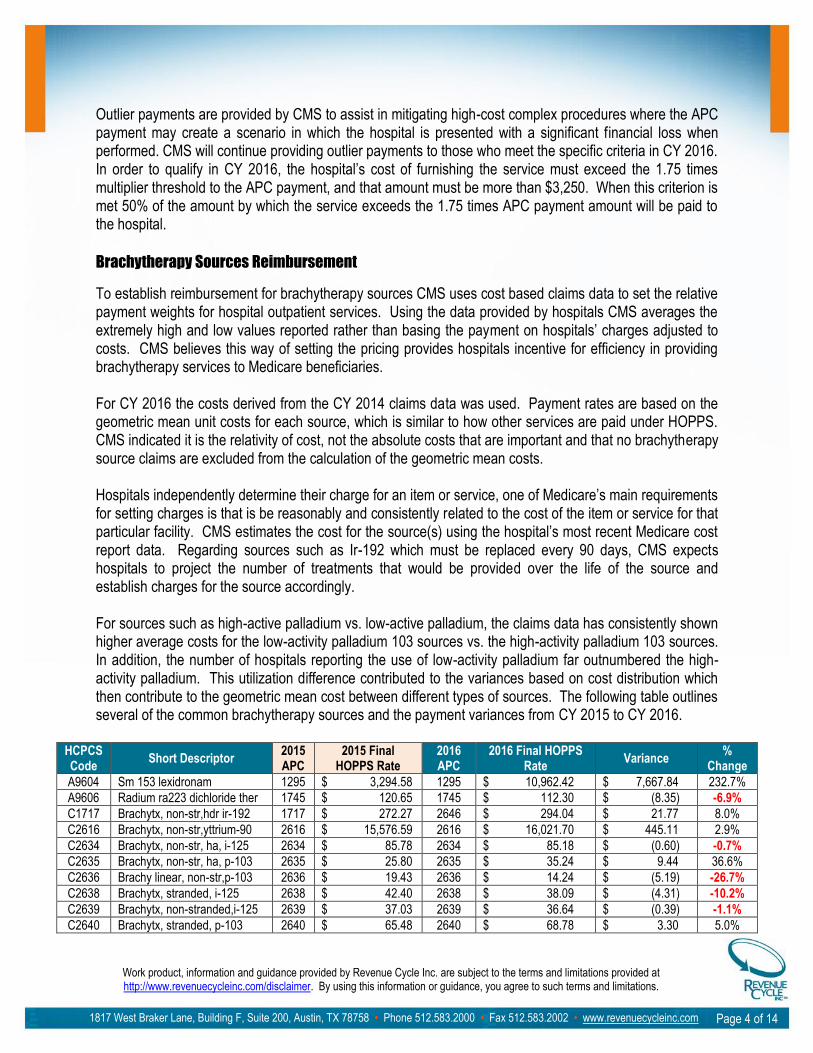
Brachytherapy Sources Reimbursement
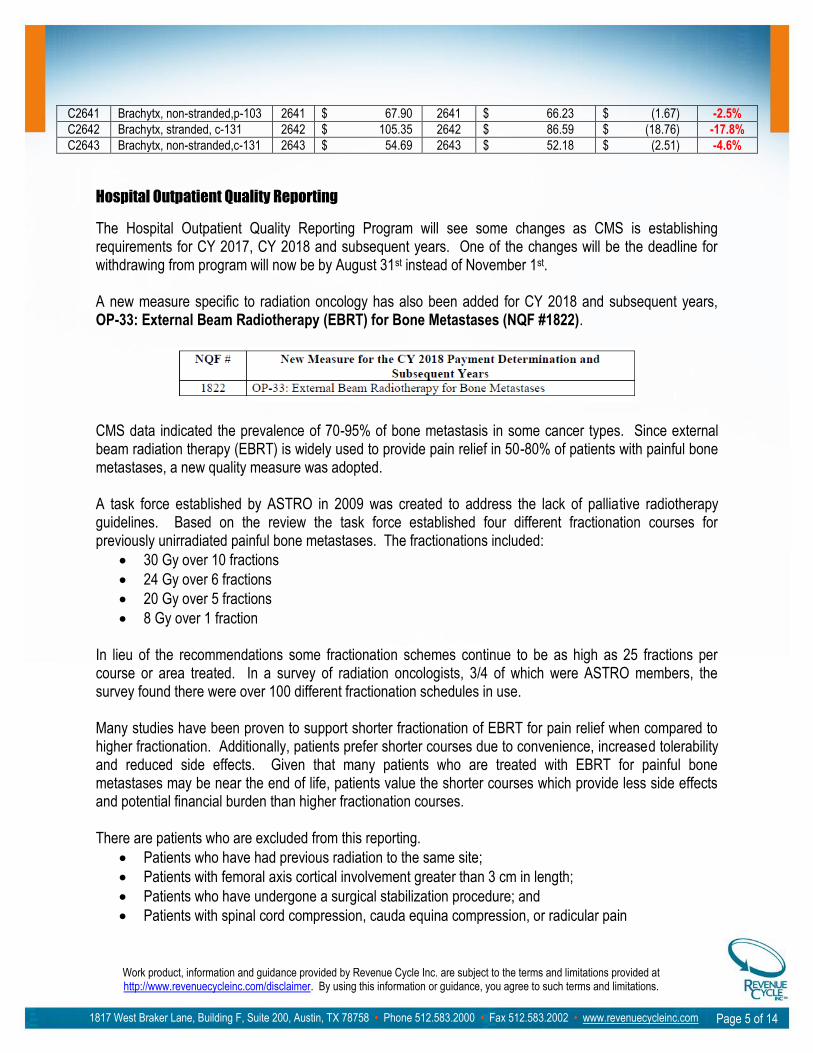
To establish reimbursement for brachytherapy sources CMS uses cost based claims data to set the relative payment weights for hospital outpatient services. Using the data provided by hospitals CMS averages the extremely high and low values reported rather than basing the payment on hospitals’ charges adjusted to costs. CMS believes this way of setting the pricing provides hospitals incentive for efficiency in providing brachytherapy services to Medicare beneficiaries. For CY 2016 the costs derived from the CY 2014 claims data was used. Payment rates are based on the geometric mean unit costs for each source, which is similar to how other services are paid under HOPPS. CMS indicated it is the relativity of cost, not the absolute costs that are important and that no brachytherapy source claims are excluded from the calculation of the geometric mean costs. Hospitals independently determine their charge for an item or service, one of Medicare’s main requirements for setting charges is that is be reasonably and consistently related to the cost of the item or service for that particular facility. CMS estimates the cost for the source(s) using the hospital’s most recent Medicare cost report data. Regarding sources such as Ir-192 which must be replaced every 90 days, CMS expects hospitals to project the number of treatments that would be provided over the life of the source and establish charges for the source accordingly. For sources such as high-active palladium vs. low-active palladium, the claims data has consistently shown higher average costs for the low-activity palladium 103 sources vs. the high-activity palladium 103 sources. In addition, the number of hospitals reporting the use of low-activity palladium far outnumbered the high-activity palladium. This utilization difference contributed to the variances based on cost distribution which then contribute to the geometric mean cost between different types of sources. The following table outlines several of the common brachytherapy sources and the payment variances from CY 2015 to CY 2016.
HCPCS Code
Short Descriptor 2015 APC
2015 Final HOPPS Rate
2016 APC
2016 Final HOPPS Rate
Variance %
Change
A9604 Sm 153 lexidronam 1295 $ 3,294.58 1295 $ 10,962.42 $ 7,667.84 232.7%
A9606 Radium ra223 dichloride ther 1745 $ 120.65 1745 $ 112.30 $ (8.35) -6.9%
C1717 Brachytx, non-str,hdr ir-192 1717 $ 272.27 2646 $ 294.04 $ 21.77 8.0%
C2616 Brachytx, non-str,yttrium-90 2616 $ 15,576.59 2616 $ 16,021.70 $ 445.11 2.9%
C2634 Brachytx, non-str, ha, i-125 2634 $ 85.78 2634 $ 85.18 $ (0.60) -0.7%
C2635 Brachytx, non-str, ha, p-103 2635 $ 25.80 2635 $ 35.24 $ 9.44 36.6%
C2636 Brachy linear, non-str,p-103 2636 $ 19.43 2636 $ 14.24 $ (5.19) -26.7%
C2638 Brachytx, stranded, i-125 2638 $ 42.40 2638 $ 38.09 $ (4.31) -10.2%
C2639 Brachytx, non-stranded,i-125 2639 $ 37.03 2639 $ 36.64 $ (0.39) -1.1%
C2640 Brachytx, stranded, p-103 2640 $ 65.48 2640 $ 68.78 $ 3.30 5.0%
Work product, information and guidance provided by Revenue Cycle Inc. are subject to the terms and limitations provided at http://www.revenuecycleinc.com/disclaimer. By using this information or guidance, you agree to such terms and limitations.
1817 West Braker Lane, Building F, Suite 200, Austin, TX 78758 • Phone 512.583.2000 • Fax 512.583.2002 • www.revenuecycleinc.com
Page 5 of 14
C2641 Brachytx, non-stranded,p-103 2641 $ 67.90 2641 $ 66.23 $ (1.67) -2.5%
C2642 Brachytx, stranded, c-131 2642 $ 105.35 2642 $ 86.59 $ (18.76) -17.8%
C2643 Brachytx, non-stranded,c-131 2643 $ 54.69 2643 $ 52.18 $ (2.51) -4.6%
Hospital Outpatient Quality Reporting
The Hospital Outpatient Quality Reporting Program will see some changes as CMS is establishing requirements for CY 2017, CY 2018 and subsequent years. One of the changes will be the deadline for withdrawing from program will now be by August 31st instead of November 1st. A new measure specific to radiation oncology has also been added for CY 2018 and subsequent years, OP-33: External Beam Radiotherapy (EBRT) for Bone Metastases (NQF #1822).
CMS data indicated the prevalence of 70-95% of bone metastasis in some cancer types. Since external beam radiation therapy (EBRT) is widely used to provide pain relief in 50-80% of patients with painful bone metastases, a new quality measure was adopted. A task force established by ASTRO in 2009 was created to address the lack of palliative radiotherapy guidelines. Based on the review the task force established four different fractionation courses for previously unirradiated painful bone metastases. The fractionations included:
30 Gy over 10 fractions
24 Gy over 6 fractions
20 Gy over 5 fractions
8 Gy over 1 fraction In lieu of the recommendations some fractionation schemes continue to be as high as 25 fractions per course or area treated. In a survey of radiation oncologists, 3/4 of which were ASTRO members, the survey found there were over 100 different fractionation schedules in use. Many studies have been proven to support shorter fractionation of EBRT for pain relief when compared to higher fractionation. Additionally, patients prefer shorter courses due to convenience, increased tolerability and reduced side effects. Given that many patients who are treated with EBRT for painful bone metastases may be near the end of life, patients value the shorter courses which provide less side effects and potential financial burden than higher fractionation courses. There are patients who are excluded from this reporting.
Patients who have had previous radiation to the same site;
Patients with femoral axis cortical involvement greater than 3 cm in length;
Patients who have undergone a surgical stabilization procedure; and
Patients with spinal cord compression, cauda equina compression, or radicular pain
Work product, information and guidance provided by Revenue Cycle Inc. are subject to the terms and limitations provided at http://www.revenuecycleinc.com/disclaimer. By using this information or guidance, you agree to such terms and limitations.
1817 West Braker Lane, Building F, Suite 200, Austin, TX 78758 • Phone 512.583.2000 • Fax 512.583.2002 • www.revenuecycleinc.com
Page 6 of 14
By adopting this measure CMS believes it will reduce the rate of EBRT overuse and continues to support their commitment to promoting patient safety and the National Quality Strategy (NQS) priority of Making Care Safer. Specifically this measure will address the gap in care, ensure appropriate use and prevent overuse of radiation therapy.
Coding Changes for CY 2016
There are several coding changes for CY 2016. The following are some of the changes impacting radiation oncology.
Codes removed from Comprehensive Ambulatory Payment Classification (C-APC) for SRS services (Cobalt-60 and linac based)
Acceptance of AMA coding changes
Restructuring of APCs o Teletherapy Planning APCs o IMRT Planning, including information on initial simulation billing for IMRT courses o Radiation Therapy (Including Brachytherapy)
Coding Changes to C-APC for SRS services For CY 2015, CMS created a new C-APC (0067); this new comprehensive APC established a single reimbursement for a one day surgical event, stereotactic radiosurgery (Cobalt-60 and linac based). Any services which are performed in conjunction with and ancillary to the treatment delivery are considered packaged into the treatment delivery and not separately reimbursed. The codes for the services are billed on the claim form for cost reporting purposes, but not separately reimbursed. When CMS reviewed claims data to establish payment rates for CY 2016 they identified an issue related to the newly established C-APC that could impact the calculated reimbursement. SRS services using the Cobalt-60 course are typically performed on a single date of service and reflected on the claim in this manner. Courses using linac based SRS treatment delivery typically do not include the use of the head frame which allows for the services to span over a number of days and potentially be reported on additional claim forms. It was identified that many of the linac based reporting SRS services included the imaging, simulation and/or planning on dates of service preceding the actual treatment delivery. When this occurred the hospital could potentially receive reimbursement for the imaging, simulation and planning services since they were on a different claim in addition to the C-APC payment for the treatment, which was designed to include those separately reimbursed services. Therefore, the linac based procedures were potentially receiving considerably more reimbursement than the same Cobalt-60 treatment course which was not the intent. Section 634 of the American Taxpayer Relief Act of 2012 requires that HOPPS payments for Cobalt-60 SRS (CPT code 77371) must be equal to the payments for robotic linear accelerator based (linac) SRS (CPT code 77372) furnished after April 1, 2013. Since the intent of the C-APC is to bundle payment for all services related and adjunctive to the primary procedure, in this case the SRS treatment, billing for services on separate claims per the process of care would appear as an unbundling of services with increased reimbursement.
Work product, information and guidance provided by Revenue Cycle Inc. are subject to the terms and limitations provided at http://www.revenuecycleinc.com/disclaimer. By using this information or guidance, you agree to such terms and limitations.
1817 West Braker Lane, Building F, Suite 200, Austin, TX 78758 • Phone 512.583.2000 • Fax 512.583.2002 • www.revenuecycleinc.com
Page 7 of 14
To correct for this and collect better data for which to establish a reimbursement reflective of all ancillary and adjunctive services, CMS is removing the following codes from the C-APC payment for CYs 2016 and 2017. The following codes will be reimbursed separately when reported within 30 days prior and/or on the same date of service as the treatment delivery codes, 77371 or 77372.
CT localization (HCPCS codes 77011 and 77014);
MRI imaging (HCPCS codes 70551, 70552, and 70553);
Clinical treatment planning (HCPCS codes 77280, 77285, 77290, and 77295); and
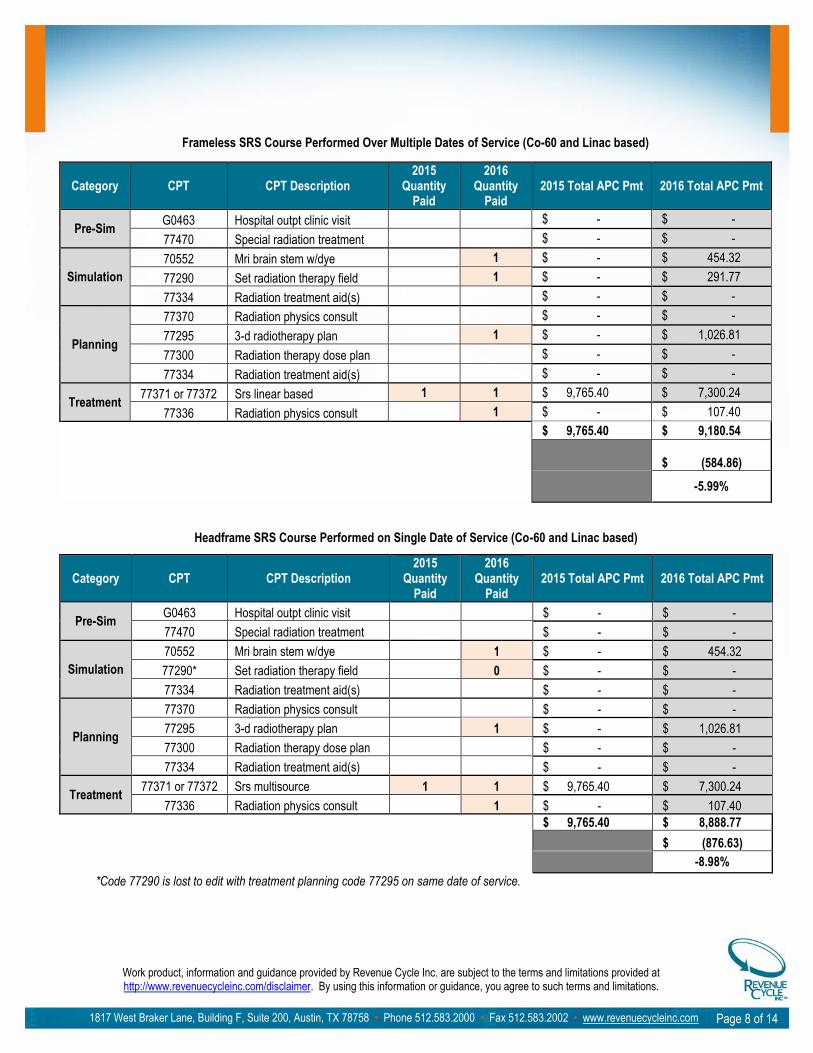
Physics consultation (HCPCS code 77336) When any of the above mentioned services are performed ancillary to the SRS treatment, but on a date at least 30 days prior to the treatment, the HCPCS modifier “CP” (Adjunctive service related to a procedure assigned to a comprehensive ambulatory payment classification (C-APC) procedure, but reported on a different claim) must be applied to those services on the different date and/or claim. Providers are expected to identify the appropriate services and apply the HCPCS modifier; CMS will not be reviewing the claims to determine which services are considered ancillary to the treatment code. CMS also indicated that they intend to issue further sub regulatory guidance on the use of the modifier with respect to SRS services prior to January 1, 2016. CMS will pay for the HCPCS codes 70551, 70552, 70553, 77011, 77014, 77280, 77285, 77290, 77295, and 77336 separately even when they are performed on the same date as the treatment and billed on the same claim form in CYs 2016 and 2017, with the expectation that in CY 2018 the full C-APC will be once again implemented. Only when the above services are performed on and billed on a separate date of service than the SRS treatment delivery code must the –CP modifier be applied to each of the separately approved codes. C-APC 0067 will also be changed to C-APC 5627 (Level 7 Radiation Therapy) and in the Clinical Family, RADTX. The Medicare national average payment rate for codes 77371 and 77372 will be $7,300.24; this is a reduction from the current CY 2015 rate of $9,765.40. The new payment has removed the above codes which when factored in and based on possible variances in the imaging codes used for diagnostic or treatment planning purposes, and the fact that due to NCCI edits some codes may not be reimbursed when performed on the same date as the treatment plan or delivery; there are a few different scenarios of possible reimbursement. The following tables reflect possible reimbursement scenarios for Cobalt-60 and linac based SRS. The first table reflects the possible work flow for a Cobalt-60 frameless process of care carried out over multiple dates. This would also match a process of care for the linac based frameless system. The second table reflects the reimbursement for a head frame process of care carried out on the same date of service for both Cobalt-60 and linac based.
Work product, information and guidance provided by Revenue Cycle Inc. are subject to the terms and limitations provided at http://www.revenuecycleinc.com/disclaimer. By using this information or guidance, you agree to such terms and limitations.
1817 West Braker Lane, Building F, Suite 200, Austin, TX 78758 • Phone 512.583.2000 • Fax 512.583.2002 • www.revenuecycleinc.com
Page 8 of 14
Frameless SRS Course Performed Over Multiple Dates of Service (Co-60 and Linac based)
Category CPT CPT Description 2015
Quantity Paid
2016 Quantity
Paid 2015 Total APC Pmt 2016 Total APC Pmt
Pre-Sim G0463 Hospital outpt clinic visit $ - $ -
77470 Special radiation treatment $ - $ -
Simulation
70552 Mri brain stem w/dye 1 $ - $ 454.32
77290 Set radiation therapy field 1 $ - $ 291.77
77334 Radiation treatment aid(s) $ - $ -
Planning
77370 Radiation physics consult $ - $ -
77295 3-d radiotherapy plan 1 $ - $ 1,026.81
77300 Radiation therapy dose plan $ - $ -
77334 Radiation treatment aid(s) $ - $ -
Treatment 77371 or 77372 Srs linear based 1 1 $ 9,765.40 $ 7,300.24
77336 Radiation physics consult
1 $ - $ 107.40
$ 9,765.40 $ 9,180.54
$ (584.86)
-5.99%
Headframe SRS Course Performed on Single Date of Service (Co-60 and Linac based)
Category CPT CPT Description 2015
Quantity Paid
2016 Quantity
Paid 2015 Total APC Pmt 2016 Total APC Pmt
Pre-Sim G0463 Hospital outpt clinic visit $ - $ -
77470 Special radiation treatment $ - $ -
Simulation
70552 Mri brain stem w/dye 1 $ - $ 454.32
77290* Set radiation therapy field 0 $ - $ -
77334 Radiation treatment aid(s) $ - $ -
Planning
77370 Radiation physics consult $ - $ -
77295 3-d radiotherapy plan 1 $ - $ 1,026.81
77300 Radiation therapy dose plan $ - $ -
77334 Radiation treatment aid(s) $ - $ -
Treatment 77371 or 77372 Srs multisource 1 1 $ 9,765.40 $ 7,300.24
77336 Radiation physics consult
1 $ - $ 107.40
$ 9,765.40 $ 8,888.77
$ (876.63)
-8.98%
*Code 77290 is lost to edit with treatment planning code 77295 on same date of service.
Work product, information and guidance provided by Revenue Cycle Inc. are subject to the terms and limitations provided at http://www.revenuecycleinc.com/disclaimer. By using this information or guidance, you agree to such terms and limitations.
1817 West Braker Lane, Building F, Suite 200, Austin, TX 78758 • Phone 512.583.2000 • Fax 512.583.2002 • www.revenuecycleinc.com
Page 9 of 14
Composite APC for LDR Prostate Seed Implant
The Low Dose Rate Composite APC 8001 which includes CPT codes 55875 and 77778 when performed on the same date of service for prostate seed implantation is continuing without change. The recognized C-APC 8001 will not be changed to match or fall in line with the other APC restructuring. CMS felt this C-APC clearly represented the codes included. CMS is also finalizing without any change to continue their current process for rate setting for this C-APC. Acceptance of AMA coding changes
CPT codes are created by the American Medical Association (AMA) and the Level II HCPCS codes are created by the CMS HCPCS Workgroup. CMS then uses and recognizes these codes when reimbursing providers for services rendered. When coding updates are received by CMS from the AMA prior to the February 10th deadline, CMS will submit the codes to the Panel for valuation and APC assignment. Those codes not received by the deadline, CMS will continue to create G-codes that mirror the predecessor CPT codes and retain the current APC assignments and status indicators for a year until CMS can propose APC and status indicator assignments for the following year.
The CY 2016 coding changes by the AMA were received by the deadline. This includes the changes to the brachytherapy treatment codes for HDR, LDR and electronic brachytherapy.
Codes that will be deleted in 2016 include
HDR codes 77785, 77786 and 77787
LDR codes 77776 and 77777
Electronic Brachytherapy code 0182T New codes or code changes in 2016 include
HDR skin codes 77767 and 77768
HDR intracavitary and interstitial codes 77770, 77771 and 77772
LDR code 77778 definition updated
Electronic brachytherapy skin code 0394T
Electronic brachytherapy intracavitary and interstitial code 0395T Restructuring of APCs
The hospital outpatient clinic visit code, G0463, in APC 0632 will be in APC 5012 staring January 1, 2016. APC 5012 will continue to be the base setting APC for all other APCs as the clinic visit (G0463) is the most frequently furnished service in the hospital outpatient setting. The reimbursement for G0463 will increase from $96.22 in CY 2015 to $102.12 in CY 2016.
Teletherapy Planning APCs
CMS proposed and finalized new APC classifications related to planning for radiation oncology.
APC 5611 (Level 1 Therapeutic Radiation Treatment Preparation);
APC 5612 (Level 2 Therapeutic Radiation Treatment Preparation);
APC 5613 (Level 3 Therapeutic Radiation Treatment Preparation); and
Work product, information and guidance provided by Revenue Cycle Inc. are subject to the terms and limitations provided at http://www.revenuecycleinc.com/disclaimer. By using this information or guidance, you agree to such terms and limitations.
1817 West Braker Lane, Building F, Suite 200, Austin, TX 78758 • Phone 512.583.2000 • Fax 512.583.2002 • www.revenuecycleinc.com
Page 10 of 14
APC 5614 (Level 4 Therapeutic Radiation Treatment Preparation).
The standard isodose planning codes, 77306 and 77307 are in the same APC for CY 2015, this means there is no distinction between the resources for the simple vs. the complex level. One commenter stated there should be a distinction between the two as the resources for the complex level are very different and more involved than the simple level. CMS agreed with this and has moved the two isodose planning codes into two different APCs.
The reimbursement for code 77306 and 77307 in 2015 is $113.12, in CY 2016 code 77306 will be reimbursed $166.65 (this accounts for the loss of the MU calculations (77300)) and code 77307 will be reimbursed $291.77 (also accounting for the loss of billing code 77300).
The new code, C9743 (injection/implantation of bulking or spacer material (any type) with or without image guidance (not to be used if a more specific code applies) used for the gel spacer in prostate cancer patients was effective October 1, 2015. When initially created it was added to the same APC as the fiducial marker placement codes for the prostate, lung and abdomen. Effective for CY 2016 CMS has moved code C9743 out of this APC and it will now be in APC 5374 with reimbursement of $2,243.39, this is an increase of 116.1% from the CY 2015 pricing.
IMRT Planning
CMS addressed whether or not the initial simulation is billable for an IMRT course after several comments and the ASTRO Coding Guidance Articles, Process of Care: Treatment Preparation, were provided for clarification by stakeholders.
CMS was very clear in the CY 2016 Final Rule publication that the initial simulation is not billable when the course of treatment is IMRT. They cited two different CMS transmittals which they indicate support this stance.
CMS cited the Medicare Claims Processing Manual, Chapter 4, Section 200.3.2, in effect since 2008 which state the simulation services are part of the IMRT planning process and not separately billable. The following is the statement from the Medicare Claims Processing Manual;
“Payment for the services identified by CPT codes 77014, 77280-77295, 77305-77321, 77331, 77336, and 77370 is included in the APC payment for IMRT planning when these services are performed as part of developing an IMRT plan that is reported using CPT code 77301. Under those circumstances, these codes should not be billed in addition to CPT code 77301 for IMRT planning.”
They also cited the National Correct Coding Initiative (NCCI) guidance in the NCCI Policy Manual for Medicare Services, Chapter 9, page IX-17 which also states IMRT includes simulation codes 77280 – 77295. The following is from the NCCI Policy Manual;
“12. Intensity modulated radiotherapy (IMRT) plan (CPT code 77301) includes therapeutic radiology simulation-aided field settings. Simulation field settings for IMRT should not be reported separately with CPT codes 77280 through 77295. Although procedure-to-procedure edits based on this principle exist in NCCI for procedures performed on the same date of service, these edits
Work product, information and guidance provided by Revenue Cycle Inc. are subject to the terms and limitations provided at http://www.revenuecycleinc.com/disclaimer. By using this information or guidance, you agree to such terms and limitations.
1817 West Braker Lane, Building F, Suite 200, Austin, TX 78758 • Phone 512.583.2000 • Fax 512.583.2002 • www.revenuecycleinc.com
Page 11 of 14
should not be circumvented by performing the two procedures described by a code pair edit on different dates of service.”
CMS went on to further explain this in the following excerpt from the final rule publication their rationale for stating the initial simulation is part of the IMRT planning process.
“…We believe that the types of services included in IMRT treatment planning include simulation…we believe CMS’ longstanding Manual and coding guidance issued in CY 2008 has been precise in conveying its policy and instructions regarding coding for IMRT services and that, generally, IMRT services have been properly reported by hospitals.
It is our policy that payments for the services identified by CPT codes 77280 through 77295 are included in the APC payment for IMRT planning services, and that the services described by these CPT codes should not be reported separately from services described by CPT code 77301, regardless of when the various services that comprise CPT code 77301 are performed. If a hospital submits a claim that separately reports services described by one of these simulation CPT codes in addition to separately reporting IMRT planning services that are performed, we would consider this reporting to constitute unbundling of the APC payment, which is prohibited. We will revise and update the Medicare Claims Processing Manual and coding guidance in the near future to ensure that this policy is more directly stated. The clarified coding guidance will state the following:
“Payment for the services identified by CPT codes 77014, 77280 through 77295, 77305 through 77321, 77331, and 77370 is included in the APC payment for CPT code 77301 (IMRT planning). These codes should not be reported in addition to CPT code 77301 (on either the same or a different date of service) unless these services are being performed in support of a separate and distinct non-IMRT radiation therapy for a different tumor.”
CPT code 77301 will be moved to APC 5614 (Level 4 Therapeutic Radiation Treatment Preparation), this will also include CPT code 77295. This means these two treatment planning codes will once again be reimbursed the same amount in a hospital setting, but only the initial simulation is bundled into the IMRT treatment planning code. Current reimbursement for codes 77295 and 77301 is $1,038.12 and will be $1,026.81 in 2016. The final geometric mean cost of the services described by CPT code 77301 is approximately $1,125. CMS stated “if the clarification of our coding guidance for IMRT planning services results in a significant change in the geometric mean cost of services described by CPT code 77301 in future years, we will consider an alternative APC assignment for the code other than APC 5614.” Radiation Therapy (Including Brachytherapy)
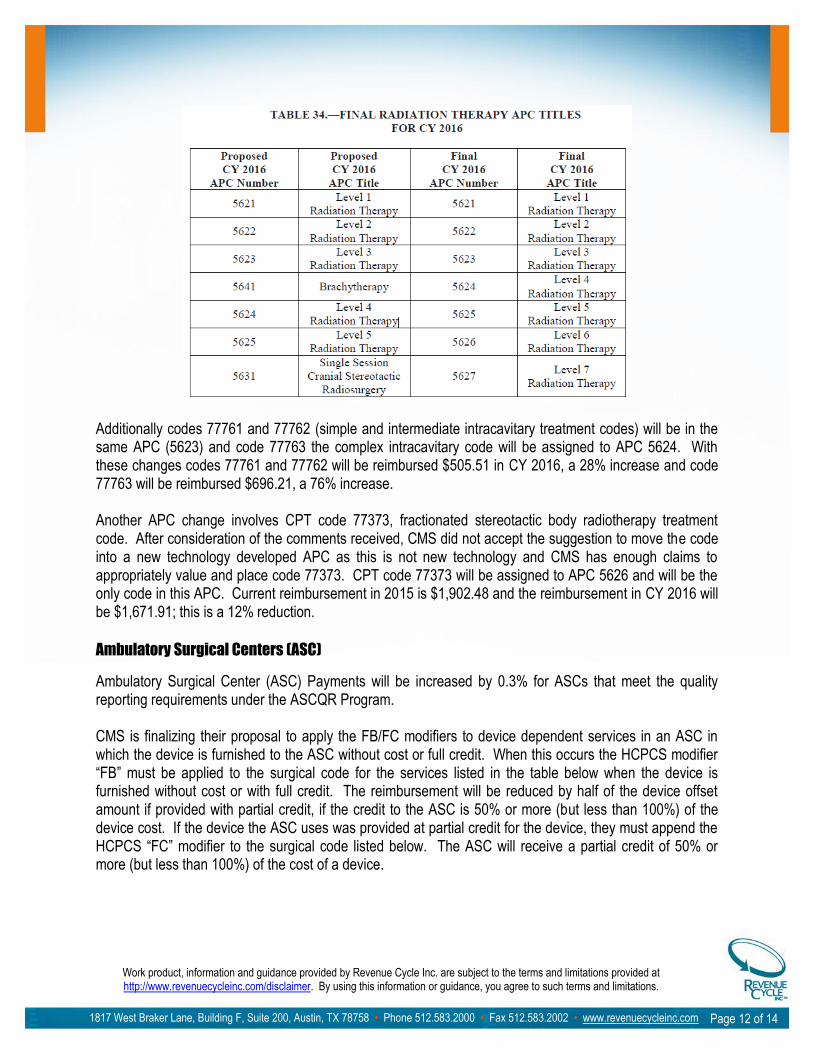
CMS finalized the following table of APC numbers and titles for 2016. Some of these are different than what was originally proposed.
Work product, information and guidance provided by Revenue Cycle Inc. are subject to the terms and limitations provided at http://www.revenuecycleinc.com/disclaimer. By using this information or guidance, you agree to such terms and limitations.
1817 West Braker Lane, Building F, Suite 200, Austin, TX 78758 • Phone 512.583.2000 • Fax 512.583.2002 • www.revenuecycleinc.com
Page 12 of 14
Additionally codes 77761 and 77762 (simple and intermediate intracavitary treatment codes) will be in the same APC (5623) and code 77763 the complex intracavitary code will be assigned to APC 5624. With these changes codes 77761 and 77762 will be reimbursed $505.51 in CY 2016, a 28% increase and code 77763 will be reimbursed $696.21, a 76% increase. Another APC change involves CPT code 77373, fractionated stereotactic body radiotherapy treatment code. After consideration of the comments received, CMS did not accept the suggestion to move the code into a new technology developed APC as this is not new technology and CMS has enough claims to appropriately value and place code 77373. CPT code 77373 will be assigned to APC 5626 and will be the only code in this APC. Current reimbursement in 2015 is $1,902.48 and the reimbursement in CY 2016 will be $1,671.91; this is a 12% reduction.
Ambulatory Surgical Centers (ASC)
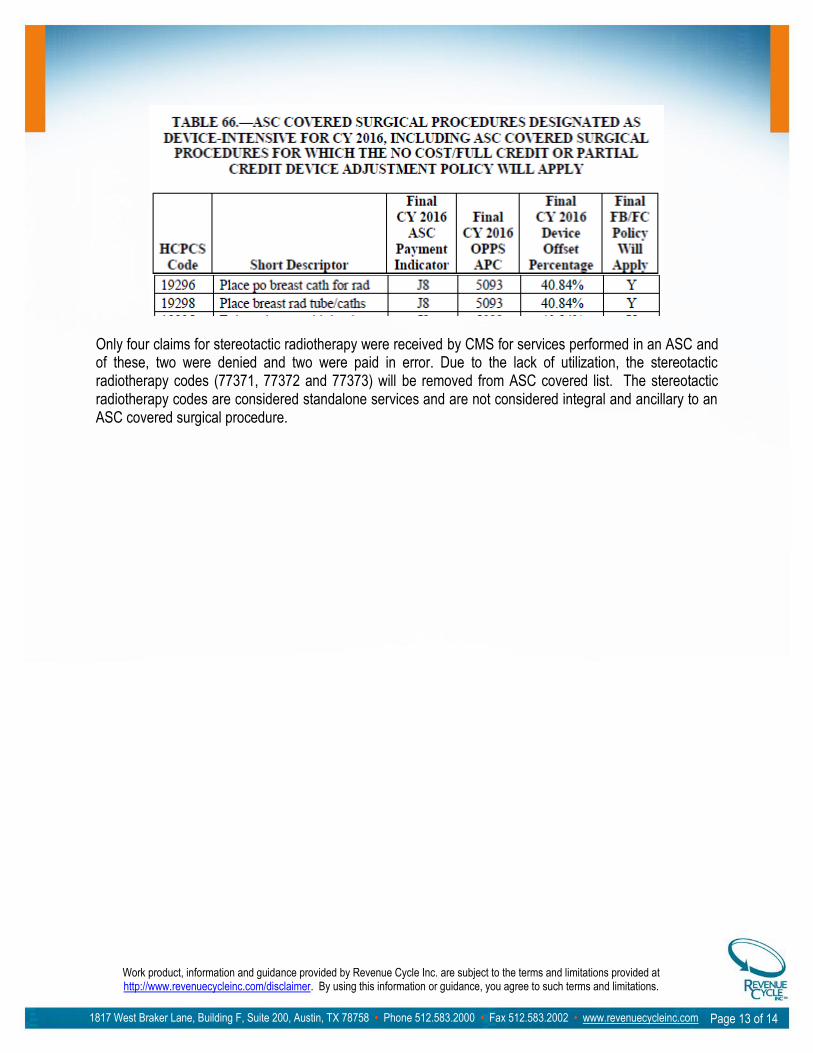
Ambulatory Surgical Center (ASC) Payments will be increased by 0.3% for ASCs that meet the quality reporting requirements under the ASCQR Program. CMS is finalizing their proposal to apply the FB/FC modifiers to device dependent services in an ASC in which the device is furnished to the ASC without cost or full credit. When this occurs the HCPCS modifier “FB” must be applied to the surgical code for the services listed in the table below when the device is furnished without cost or with full credit. The reimbursement will be reduced by half of the device offset amount if provided with partial credit, if the credit to the ASC is 50% or more (but less than 100%) of the device cost. If the device the ASC uses was provided at partial credit for the device, they must append the HCPCS “FC” modifier to the surgical code listed below. The ASC will receive a partial credit of 50% or more (but less than 100%) of the cost of a device.
Work product, information and guidance provided by Revenue Cycle Inc. are subject to the terms and limitations provided at http://www.revenuecycleinc.com/disclaimer. By using this information or guidance, you agree to such terms and limitations.
1817 West Braker Lane, Building F, Suite 200, Austin, TX 78758 • Phone 512.583.2000 • Fax 512.583.2002 • www.revenuecycleinc.com
Page 13 of 14
Only four claims for stereotactic radiotherapy were received by CMS for services performed in an ASC and of these, two were denied and two were paid in error. Due to the lack of utilization, the stereotactic radiotherapy codes (77371, 77372 and 77373) will be removed from ASC covered list. The stereotactic radiotherapy codes are considered standalone services and are not considered integral and ancillary to an ASC covered surgical procedure.
Work product, information and guidance provided by Revenue Cycle Inc. are subject to the terms and limitations provided at http://www.revenuecycleinc.com/disclaimer. By using this information or guidance, you agree to such terms and limitations.
1817 West Braker Lane, Building F, Suite 200, Austin, TX 78758 • Phone 512.583.2000 • Fax 512.583.2002 • www.revenuecycleinc.com
Page 14 of 14
Disclaimer
The information and guidance provided by Revenue Cycle Inc. on the preceding pages and the following
course comparison data materials is subject to the following terms and limitations and by using this
information or guidance, you agree to such terms and limitations. Terms and limitations may be viewed in
their entirety by visiting http://www.revenuecycleinc.com/disclaimer .
I. Analysis of federal / state regulations and health plan billing or payment policies
A. The opinions expressed by RCI regarding the applicability, interpretation or impact of any federal or state
law or regulation or health plan billing, coding or payment policy are only the opinions of RCI. Such
opinions are not intended to address specific facts and circumstances. RCI summaries of federal or state
laws or regulations or health plan billing, coding or payment policies may omit information that is applicable
to you. You should not rely on the opinions of RCI without consulting with a qualified attorney as to the
applicability, interpretation or impact of any federal or state law or regulation or health plan billing, coding or
payment policy relative to your specific facts and circumstances. RCI is not legal counsel, is not a substitute
for legal counsel, and does not purport to provide legal advice.
B. Federal and state laws and regulations and health plan billing, coding or payment policies, and the
interpretations thereof, are subject to change; unless specifically undertaken in writing by RCI, RCI has no
obligation to update or revise any opinions or information regarding any federal or state law or regulation or
health plan billing, coding or payment policy and it is your sole responsibility to verify that any such opinion
or information is valid at the time you view, access, use or rely on such opinion or information.
II. Use of RCI Information
A. You may only use or rely on RCI work product for those purposes for which it is specifically intended.
Disclosure of RCI work product to third parties is not authorized if such work product is modified in any way,
including the removal of or changes to any RCI statement regarding the context or limitations of any such
work product. If you disclose RCI work product to a third party for any purpose without disclosing all RCI
statements regarding the context or limitations of the RCI work product, you are solely responsible to the
third party for any damages that are related to such third party’s reliance on the RCI work product and you
agree to indemnify RCI for any costs, claims or damages incurred by RCI related to such third party’s
reliance on the RCI work product.












![Medicare Program; CY 2018 Updates to the Quality …...Medicare Program; CY 2018 Updates to the Quality Payment Program [CMS-5522-P] Summary of Proposed Rule Subject Page I. Introduction](https://img.pdfslide.us/doc/110x75/5f086c667e708231d421f073/medicare-program-cy-2018-updates-to-the-quality-medicare-program-cy-2018-updates.jpg)
















