Embed Size (px)
Citation preview

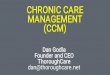
TABLE 11: Summary of CY 2017 Chronic Care Management (CCM) Service Elements and Billing Requirements
Initiating Visit- Initiation during an AWV, IPPE, or face-to-face E/M visit (Level 4 or 5 visit not required), for new patients or patients not seen within 1 year prior to the commencement of chronic care management (CCM) services.
Structured Recording of Patient Information Using Certified EHR Technology – Structured recording of demographics, problems, medications and medication allergies using certified EHR technology. A full list of problems, medications and medication allergies in the EHR must inform the care plan, care coordination and ongoing clinical care.
24/7 Access & Continuity of Care
Provide 24/7 access to physicians or other qualified health care professionals or clinical staff including providing patients/caregivers with a means to make contact with health care professionals in the practice to address urgent needs regardless of the time of day or day of week.
Continuity of care with a designated member of the care team with whom the beneficiary is able to schedule successive routine appointments.
Comprehensive Care Management- Care management for chronic conditions including systematic assessment of the beneficiary’s medical, functional, and psychosocial needs; system-based approaches to ensure timely receipt of all recommended preventive care services; medication reconciliation with review of adherence and potential interactions; and oversight of beneficiary self-management of medications.
Comprehensive Care Plan
Creation, revision and/or monitoring (as per code descriptors) of an electronic patient-centered care plan based on a physical, mental, cognitive, psychosocial, functional and environmental (re)assessment and an inventory of resources and supports; a comprehensive care plan for all health issues.
Must at least electronically capture care plan information, and make this information available timely within and outside the billing practice as appropriate. Share care plan information electronically (can include fax) and timely within and outside the billing practice to individuals involved in the beneficiary’s care.
A copy of the plan of care must be given to the patient and/or caregiver
Management of Care Transitions
Management of care transitions between and among health care providers and settings, including referrals to other clinicians; follow-up after an emergency department visit; and follow-up after discharges from hospitals, skilled nursing facilities or other health care facilities.
Create and exchange/transmit continuity of care document(s) timely with other practitioners and providers.

Source: Pages 331, Federal Register/November 15, 2016
(Link provided, but will be moved as of November 16 upon final publication)
https://s3.amazonaws.com/public-inspection.federalregister.gov/2016-26668.pdf
Provided by Elizabeth Woodcock @ www.elizabethwoodcock.com
Home- and Community-Based Care Coordination
Coordination with home and community based clinical service providers.
Communication to and from home- and community-based providers regarding the patient’s psychosocial needs and functional deficits must be documented in the patient’s medical record.
Enhanced Communication Opportunities- Enhanced opportunities for the beneficiary and any caregiver to communicate with the practitioner regarding the beneficiary’s care through not only telephone access, but also through the use of secure messaging, Internet, or other asynchronous non-face-to-face consultation methods.
Beneficiary Consent
Inform the beneficiary of the availability of CCM services; that only one practitioner can furnish and be paid for these services during a calendar month; and of their right to stop the CCM services at any time (effective at the end of the calendar month).
Document in the beneficiary’s medical record that the required information was explained and whether the beneficiary accepted or declined the services.
Medical Decision-Making- Complex CCM services require and include medical decision-making of moderate to high complexity (by the physician or other billing practitioner).

By Elizabeth W. Woodcock, MBA, FACMPE, CPC
2016©
2
Elizabeth W. Woodcock, MBA, FACMPE, CPCSpeaker, Author, Trainerwww.elizabethwoodcock.com MBA, Wharton School of Business, University of Pennsylvania BA, Duke University Fellow, American College of Medical Practice Executives Certified Professional Coder Author, 16 textbooks and more than 500 Articles Founder and Principal, Woodcock & Associates Former Consultant, Medical Group Management Association; Group Practice Services Administrator, University of Virginia Health Services Foundation; Former Senior Associate, Health Care Advisory Board
©2

2016©
3
Medicare 2017 ICD10 Meaningful Use Penalties Quality Payment Program
Merit-based Incentive Payment System
Conclusion
2016©
4
CMS Final Rule
November 2, 2016
Publication Date: November 15, 2016
http://bit.ly/2fFJ6Hf

2016©
5
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
Law
Actual
Exception - 2014Q1 had a 0.5% rate increase
0.50%
(0.26%)
0.24%
2016©
6
Average cuts based on claims processed under the taxonomy code associated with the specialty; represents RVU changes only. Includes physician specialties only. All other specialties 0% impact.
Review Your Appendix
Allergy/Immunology 1% Ophthalmology -2%Family Medicine 1% Urology -2%General Practice 1% Gastroenterology -1%Geriatrics 1% Interventional Radiology -1% Internal Medicine 1% Neurosurgery -1%
Oral/Maxillofacial Surgery -1%Otolaryngology -1%Pathology -1%Radiology -1%

2016©
7
Effective for services furnished beginning
January 1, 2017… [Medicare] reduces by
20 percent the payment amounts…for the
technical component (TC) (including the
TC portion of a global service) of imaging
services that are X-rays taken using film.
The modifier FX is required on claims for the technical component of the X-ray service, including when the service is billed globally,
Modifier FX
2016©
8
G0502: Initial psychiatric collaborative care management, first 70 minutes in the first calendar
month of behavioral health care manager activities…
G0503: Subsequent psychiatric collaborative care management, first 60 minutes in a
subsequent month of behavioral health care manager activities…
G0504: Initial or subsequent psychiatric collaborative care management, each additional 30
minutes in a calendar month of behavioral health care manager activities…
Behavioral Health
Note: CPT codes are a registered trademark of the
American Medical Association (AMA). Please
review the complete definition in your CPT®
Manual, and any applicable guidance from the
Centers for Medicare & Medicaid Services if billing
a Medicare-only “G” code.

2016©
9
99490 Chronic Care Management Services
“Services are provided when medical and/or psychosocial
needs of the patient require establishing, implementing,
revising, or monitoring the care plan. Patients who receive
chronic care management services have two or more
chronic conditions or episodic health conditions that are
expected to last at least 12 months, or until the death of
the patient, and place the patient at significant risk of
death, acute exacerbation/decompensation, or functional
decline.”
$40.82Starting with January 1, 2015 Dates of Service
Reimbursement based on current “Georgia - 1020201” reimbursement for Medicare 2016. Locality 1020299 (“Rest of Georgia”) is $38.91. Non-
facility.
2016©
10
G0506: Comprehensive assessment of and care planning by the
physician or other qualified health care professional for patients requiring
chronic care management services, including assessment during the
provision of a face-to-face service (billed separately from monthly care
management services) (Add-on code, list separately in addition to primary
service).
99490
99487 Complex chronic care w/o pt vsit99489 Complex chronic care addl 30 min

2016©
11
Review Your Appendix
99490 – Highlight of Changes
• Creation of structured clinical summary record not
required.
• Separate written patient consent not required; sufficient
to document acceptance of services in medical record.
• 24/7 access equates to contact with health care
professional; access to electronic care plan not required.
• Care plan can be shared with other practitioners via fax.
2016©
12
CPT code 99358 (Prolonged evaluation and
management service before and/or after direct patient care,
first hour); and
CPT code 99359 (Prolonged evaluation and
management service before and/or after direct patient care,
each additional 30 minutes (List separately in addition to
code for prolonged service).
Non-Face-to-
Face Services

2016©
13
TelehealthESRD-Related Services
Advanced Care PlanningCritical Care Telehealth Consults
New Place of Service Code 02
Under ScrutinyZero-Day Global Services billed
with Modifier -25
Global Period@270 CPT Codes
Surgeons in Groups of 10+9 States; Not MS
Informal ReviewPQRS/VBPM informal review streamlined for participating
physicians
2016©
14
TelehealthESRD-Related ServicesAdvanced Care PlanningCritical Care Telehealth Consults
New Place of Service Code 02
Under ScrutinyZero-Day Global Services billed
with Modifier -25
Global Period@270 CPT Codes
Surgeons in Groups of 10+9 States; Not GA
Informal ReviewPQRS/VBPM informal review streamlined for participating
physicians

2016©
15
TelehealthESRD-Related Services
Advanced Care PlanningCritical Care Telehealth Consults
New Place of Service Code
Under ScrutinyZero-Day Global Services billed
with Modifier -25
Global Period@270 CPT Codes
Surgeons in Groups of 10+9 States; Not GA
Informal ReviewPQRS/VBPM informal review streamlined for participating
physicians
2016©
16
TelehealthESRD-Related Services
Advanced Care PlanningCritical Care Telehealth Consults
New Place of Service Code
Under ScrutinyZero-Day Global Services billed
with Modifier -25
Global Period@270 CPT CodesSurgeons in Groups of 10+9 States; Not GA
Informal ReviewPQRS/VBPM informal review streamlined for participating
physicians

2016©
17
TelehealthESRD-Related Services
Advanced Care PlanningCritical Care Telehealth Consults
New Place of Service Code
Under ScrutinyZero-Day Global Services billed
with Modifier -25
Global Period@270 CPT Codes
Surgeons in Groups of 10+9 States; Not GA
Informal ReviewPQRS/VBPM informal review streamlined for participating
physicians
2016©
18
Was Over
October 1,
2016
ICD-10
2017 Updates (Oct 1, 2016-Sept 30, 2017) Posted
http://go.cms.gov/28ZiPxA

2016©
19
…any continuous 90-
day period between
January 1, 2016 and
December 31, 2016.
http://bit.ly/2fcXuUl
2016©
20
Year eRx PQRS EHR (MU) VBPM+ Total
2012 -1.0% - - - -1.0%
2013 -1.5% - - - -3.5%
2014 -2.0% - - - -4.0%
2015 - -1.5% -1.0% -1.0% -5.5%
2016 - -2.0% -2.0% -2.0% -8.0%
2017 - -2.0% -3.0% -4.0% -9.0%
2018 - -2.0% -3.0% -4.0% -9.0%+Value-Based Payment Modifier phases in the payment adjustments based on the size of the practice, so the penalty may be higher.
Remember… 2018 is being determined by your participation in 2016!!
Penalties for Not Participating (in the
Government’s Programs) are Piling Up

2016©
21
CO237 = Legislative Penalty
N699 = PQRS
N700 = EHR Incentive Program
N701 = Value-Based Payment Modifier
http://go.cms.gov/2e1Zv5Z
Medicare Remittance
2016©
22
1. Advanced
Alternative Payment
Model (APM)
Participant
2. Everyone Else
Merit-based Incentive
Payment System

2016©
23
2016©
24
$30,000 in Total Allowed Part B Charges
1. Allowed charges = Allowable for that particular service
99213 $200.00 $73.40CPT® Your Charge Allowed Charge*
*Reflects the current (2016) National Payment Amount for 99213; non-facility price.
This is only an estimate, but this translates into $60,000 to $90,000 in gross
charges for most medical practices.
Payment
$??

2016©
25
“…Beneficiaries enrolled in Medicare Advantage plans that receive their Part B
services through their Medicare Advantage plan will not be included in allowed
charges billed under Medicare Part B for determining the low-volume threshold.”
- CMS
2. Part B = Traditional Medicare. It does not include
Medicare Advantage.
$30,000 in Total Allowed Part B Charges
• First Year Medicare Participant^…
• Perform Services for <100 Medicare patients
• Not enrolled in Medicare
^Per CMS, “a professional who first becomes a Medicare-enrolled eligible clinician within the PECOS.”
CMS will perform a quarterly check.
32.5%
2016©
26
“[We] intend to provide a NPI level lookup feature prior to or shortly after
the start of the performance period that will allow clinicians to determine if they do not exceed the low-volume threshold and are therefore excluded
from MIPS.”-CMS

2016©
27
October 14, 2016
List of Advanced APMs
Source: CMS. https://qpp.cms.gov/docs/QPP_Advanced_APMs_in_2017.pdf
“These APMs are
scheduled to be
implemented in 2017 or
2018 but have design
parameters that have not
yet been finalized. We
will update this list … to
reflect changes as they
are finalized.” 5 to 8%New ACO Track One Model 2018
2016©
28
2-Year
2019
Deadline

2016©
29
Option Result
Report all required elements for 90 consecutive days
Bonus
Report >1 quality measure, >1 improvement activity and all ACI measures
“Small” bonus
1 quality measure; 1 improvement activity OR all ACI measures
No payment increase; no penalty
Advanced APM Automatic 5% increase
“Pick Your Pace” 2017
If you do nothing, you will be penalized 4% on all of your Medicare reimbursement.
2016©
30
Potential for 3x adjustment for
“exceptional performance”
+4%
-4%
+5%
-5%
+7%
-7%
+9%
-9%
Adjusted Medicare Part B Payment to Clinician
[ based on a MIPS Composite Performance Score ]
2019 2020 2021 2022 onward

2016©
31
1
Quality
2
Cost
3
Advancing Care Information
4
Improvement Activities
Eliminated in 2017
Composite Performance
Score
Advancing Care Information = New Name for “Meaningful Use”
All measures can be viewed at https://qpp.cms.gov/
2016©
32
Basically Replicates the Current
Programs from a Reporting Perspective
“MACRA requires us to measure performance, not
reporting.” - CMSSource: CMS, Final Rule (10/14/16)

2016©
33
Performance = Comparison to
measure-specific benchmarks
2016©
34
QualityMeasure
100 Patients
80 Patients
80% 90%Measure-Specific
https://qpp.cms.gov/

2016©
35
• Medicare 2017
• ICD10
• Meaningful Use
• Penalties
• Quality Payment Program
• Merit-based Incentive Payment System
2016©
36
Question & Answer Session

2016©
37
Exempt from MIPS? Low-Volume Threshold Determination Period
“…Define the low-volume threshold determination period to mean a 24 month assessment period, which includes a two-segment
analysis of claims data during an initial 12-month period prior to the performance period followed by another 12-month period
during the performance period. The initial 12-month segment of the low-volume threshold determination period would span from the
last 4 months of a calendar year 2 years prior to the performance period followed by the first 8 months of the next calendar year
and include a 60-day claims run out, which will allow us to inform eligible clinicians and groups of their low-volume status during the
month (December) prior to the start of the performance period. To conduct an analysis of the claims data regarding Medicare Part B
allowed charges billed prior to the performance period, we are establishing an initial segment of the low-volume threshold
determination period consisting of 12 months.
12 months of data starting from September 1, 2015 to August 31, 2016, with a 60 day claims run out.
Material in this Appendix from the Centers for Medicare &
Medicaid Services (CMS) extracted from October 14, 2016 Final
Rule, noting that it will be published in an upcoming Federal
Register that will have a future date, unless otherwise specified.
https://qpp.cms.gov/docs/CMS-5517-FC.pdf
2016©
38
• Physician
• Physician assistant
• Nurse practitioner
• Clinical nurse specialist
• Certified registered nurse anesthetist
Eligible Clinicians
• Can instead report as a group• There will be an “election process.” “…If a group is submitting information
collectively, then it must be measured collectively for all four MIPS performance
categories: quality, cost, improvement activities, and advancing care information.” - CMS
• “Virtual groups” can be formed, but not until 2018

2016©
39
Eligible Clinicians
“While we have multiple identifiers for participation and performance, we are finalizing
the use of a single identifier, TIN/NPI, for applying the MIPS payment adjustment,
regardless of how the MIPS eligible clinician is assessed…Each unique TIN/NPI
combination will be considered a different MIPS eligible clinician, and MIPS
performance will be assessed separately for each TIN under which an individual bills.”
“[Others]… may voluntarily report on measures and activities under MIPS, but will not be
subject to the MIPS payment adjustment.”
Payment Adjustments will not be Applied to FQHC or RHC All-Inclusive Rates, so
Participation is not Expected, but it is Voluntary
Source: CMS, Final Rule (10/14/16)TIN = Tax Identification Number
NPI = National Provider Identifier
MIPS = Merit-based Incentive Payment System
FQHC = Federally Qualified Health Center
RHC = Rural Health Clinic
2016©
40
Basically Replicates PQRS from a Reporting Perspective
Per CMS, “The CPT codes that have historically been available under the PQRS program will be made available for the MIPS as part of the detailed measure
specifications which will be posted prior to the performance period at QualityPaymentProgram.cms.gov.”
Almost Exactly the Same Measures (271), as well as Reporting Options
CMS Web Interface for Groups
Qualified Clinical Data Registry (QCDR)*
Qualified Registry
Electronic Health Record
Claims
Accountable Care Organization~
*More information: https://www.cms.gov/medicare/quality-initiatives-patient-assessment-instruments/pqrs/qualified-clinical-data-registry-reporting.html
At least 50% of patients that meet
the measure’s denominator criteria,
regardless of the payer
Same, but only Medicare Part B
Sample provided by CMS; 248
Medicare beneficiaries
No separate reporting; via ACO
~“Official” ACO, recognized as able to successfully submit data to CMS (e.g., Medicare Shared Savings)
PQRS = Physician Quality Reporting System

2016©
41
Base Score
50 Points
[ Required Measures* ]
*Failure to report any of these five elements successfully results in a “zero” base score, which automatically translates into a “zero” performance
score for this category.
^MIPS-eligible clinicians who write fewer than 100 permissible prescriptions in a performance period may elect to report a null value.
Perform Security Risk Assessment
(Y/N)
ePrescribe^
Send Summary of Care
Request/Accept Summary of Care
Provide Patient Access
In 2017, can
use 2014 or
2015 Edition
CEHRT; must
be 2015
Edition
certified in
2018.
This table reflects the 2015 Edition of CEHRT (Certified EHR Technology). If using 2014 Edition, see the “Transition” objectives
applicable for 2014 Edition users on the next page; these are slightly different.
*Required for Base Score, noting that your performance also contributes to your supplemental performance score.
Per CMS, “The performance score…is based on a MIPS eligible clinician’s performance rate for each measure reported for the
performance score (calculated using the numerator/denominator).” If your ratio is 90 out of 100 patients, for example, you’ll get 90% of
10 points, which is 9 points.
^Recommended, as “Yes” achieves the full 10 points.
Category Maximum # of Points
Provide Patient Access* 10
Patient-Specific Education 10
View, Download or Transmit 10
Secure Messaging 10
Patient-Generated Health Data 10
Send a Summary of Care* 10
Require/Accept Summary of Care* 10
Clinical Information Reconciliation 10
Immunization Registry^ 10
Bonus: (Any) Public Health/Clinical Data Registry^ 5
Bonus: Report your improvement activities using CEHRT^
10
Need 50
Points Here
to Maximize
Your
Performance
Score
(100)
155 Total
2015 Edition of CEHRT

This table reflects the 2014 Edition of CEHRT.
*Required for Base Score, noting that your performance also contributes to your supplemental performance score.
Per CMS, “The performance score…is based on a MIPS eligible clinician’s performance rate for each measure reported for the
performance score (calculated using the numerator/denominator).” If your ratio is 90 out of 100 patients, for example, you’ll get 90% of
10 points, which is 9 points.
^Recommended, as “Yes” achieves the full 10 points.
Category Maximum # of Points
Provide Patient Access* 20
Patient-Specific Education 10
View, Download or Transmit 10
Secure Messaging 10
Health Information Exchange* 20
Medication Reconciliation 10
Immunization Registry^ 10
Bonus: (Any) Public Health/Clinical Data Registry^ 5
Bonus: Report your improvement activities using CEHRT^
10
Need 50
Points to
Maximize
Your
Performance
Score
MIPS Category
Advancing Care Information
2014 Edition of CEHRT
2016©
44
Regularly assess the patient experience of care through
surveys, advisory councils and/or other mechanisms.
Seeing new and follow-up Medicaid patients in a
timely manner, including individuals dually eligible for
Medicaid and Medicare (HIGH).
Timely communication of test results defined as timely
identification of abnormal test results with timely
follow-up.
Performance of regular practices that include providing
specialist reports back to the referring…clinician or
group to close the referral loop or where the referring
…clinician or group initiates regular inquiries to
specialist for specialist reports which could be
documented or noted in the certified EHR technology.
Implementation of regular care coordination training.
Improvement Activity

2016©
45
Elizabeth W. Woodcock, MBA, FACMPE, CPC
Woodcock & Associates
Speaker, Trainer, Author
Atlanta, Georgia
404.373.6195
www.elizabethwoodcock.com
These handouts may not be reproduced without the written consent of the speaker.

TOTAL 0% ORTHOPEDIC SURGERY 0%
ALLERGY/IMMUNOLOGY 1% OTOLARNGOLOGY -1%
ANESTHESIOLOGY 0% PATHOLOGY -1%
CARDIAC SURGERY 0% PEDIATRICS 0%
CARDIOLOGY 0% PHYSICAL MEDICINE 0%
COLON AND RECTAL SURGERY 0% PLASTIC SURGERY 0%
CRITICAL CARE 0% PSYCHIATRY 0%
DERMATOLOGY 0% PULMONARY DISEASE 0%
EMERGENCY MEDICINE 0% RADIATION ONCOLOGY 0%
ENDOCRINOLOGY 0% RADIOLOGY -1%
FAMILY PRACTICE 1% RHEUMATOLOGY 0%
GASTROENTEROLOGY -1% THORACIC SURGERY 0%
GENERAL PRACTICE 0% UROLOGY -2%
GENERAL SURGERY 0% VASCULAR SURGERY -1%
GERIATRICS 1% AUDIOLOGIST 0%
HAND SURGERY 0% CHIROPRACTOR 0%
HEMATOLOGY/ONCOLOGY 0% CLINICAL PSYCHOLOGIST 0%
INFECTIOUS DISEASE 0% CLINICAL SOCIAL WORKER 0%
INTERNAL MEDICINE 1% DIAGNOSTIC TESTING FACILITY -1%
INTERVENTIONAL PAIN MGMT 0% INDEPENDENT LABORATORY -5%
INTERVENTIONAL RADIOLOGY -1% NURSE ANES / ANES ASST 0%
MULTISPECIALTY CLINIC/OTHER 1% NURSE PRACTITIONER 0%
NEPHROLOGY 0% OPTOMETRY -1%
NEUROLOGY 0% PHYSICAL/OCCUPATIONAL THERAPY 1%
NEUROSURGERY -1% PHYSICIAN ASSISTANT 0%
NUCLEAR MEDICINE 0% PODIATRY 0%
OBSTETRICS/GYNECOLOGY 0% PORTABLE X-RAY SUPPLIER 0%
OPHTHALMOLOGY -2% RADIATION THERAPY CENTERS 0%
ORAL/MAXILLOFACIAL SURGERY -1% OTHER 0%
Source: Pages 1329-1330, Federal Register/November 15, 2016
(Link provided, but will be moved as of November 16 upon final publication)
https://s3.amazonaws.com/public-inspection.federalregister.gov/2016-26668.pdf
Provided by Elizabeth Woodcock @ www.elizabethwoodcock.com
TABLE 62: CY 2017 PFS FINAL ESTIMATED IMPACT ON TOTAL ALLOWED CHARGES BY SPECIALTY
Specialty
Combined
Impact (%) Specialty
Combined
Impact (%)

MEASURE NAME MEASURE DESCRIPTIONRequired
for Base
Performance
Score Weight
e-Prescribing
At least one permissible prescription written by the MIPS eligible
clinician is queried for a drug formulary and transmitted electronically Yes 0
Health Information Exchange
The MIPS eligible clinician that transitions or refers their patient to
another setting of care or health care clinician (1) uses CEHRT to create
a summary of care record; and (2) electronically transmits such
summary to a receiving health care clinician for at least one transition Yes Up to 20%
Immunization Registry
Reporting
The MIPS eligible clinician is in active engagement with a public health
agency to submit immunization data. No 0 or 10%
Medication Reconciliation
The MIPS eligible clinician performs medication reconciliation for at
least one transition of care in which the patient is transitioned into the
care of the MIPS eligible clinician. No Up to 10%
Patient-Specific Education
The MIPS eligible clinician must use clinically relevant information from
CEHRT to identify patient-specific educational resources and provide
electronic access to those materials to at least one unique patient seen
by the MIPS eligible clinician. No Up to 10%
Provide Patient Access
At least one patient seen by the MIPS eligible clinician during the
performance period is provided timely access to view online, download,
and transmit to a third party their health information subject to the
MIPS eligible clinician's discretion to withhold certain information. Yes Up to 20%
Secure Messaging
For at least one unique patient seen by the MIPS eligible clinician during
the performance period, a secure message was sent using the
electronic messaging function of CEHRT to the patient (or the patient-
authorized representative), or in response to a secure message sent by
the patient (or the patient-authorized representative) during the No Up to 10%
Security Risk Analysis
Conduct or review a security risk analysis... including addressing the
security (to include encryption) of ePHI data created or maintained by
certified EHR technology...and implement security updates as necessary
and correct identified security deficiencies as part of the MIPS eligible
clinician's risk management process. (See 45 CFR 164.) Yes 0
Specialized Registry Reporting
The MIPS eligible clinician is in active engagement to submit data to
specialized registry. Earn a 5% bonus in the advancing care information
performance category score for submitting to one or more public
health or clinical data registries. No 0
Syndromic Surveillance
Reporting
The MIPS eligible clinician is in active engagement with a public health
agency to submit syndromic surveillance data. Earn a 5% bonus in the
advancing care information performance category score for submitting
to one or more public health or clinical data registries. No 0
View, Download, or
Transmit (VDT)
At least one patient seen by the MIPS eligible clinician during the
performance period (or patient-authorized representative) views,
downloads or transmits their health information to a third party during
the performance period. No Up to 10%
Merit-based Incentive Payment SystemAdvancing Care Information - 2017 Requirements
Provided by Elizabeth W. Woodcock, MBA, FACMPE, CPC | Source: https://qpp.cms.gov/measures/aci

ACTIVITY NAME ACTIVITY DESCRIPTIONACTIVITY
WEIGHTING
Additional improvements in access as a
result of QIN/QIO TA
As a result of Quality Innovation Network-Quality
Improvement Organization technical assistance, performance
of additional activities that improve access to services (e.g.,
investment of on-site diabetes educator). Medium
Administration of the AHRQ Survey of
Patient Safety Culture
Administration of the AHRQ Survey of Patient Safety Culture
and submission of data to the comparative database (refer to
AHRQ Survey of Patient Safety Culture website
http://www.ahrq.gov/professionals/quality-patient-
safety/patientsafetyculture/index.html) Medium
Annual registration in the Prescription
Drug Monitoring Program
Annual registration by eligible clinician or group in the
prescription drug monitoring program of the state where they
practice. Activities that simply involve registration are not
sufficient. MIPS eligible clinicians and groups must participate
for a minimum of 6 months. Medium
Merit-Based Incentive Payment SystemImprovement Activities - 2017 Requirements
Provided by Elizabeth W. Woodcock, MBA, FACMPE, CPC | Source: https://qpp.cms.gov

Anticoagulant management
improvements
MIPS eligible clinicians and groups who prescribe oral Vitamin K
antagonist therapy (warfarin) must attest that, in the first
performance year, 60 percent or more of their ambulatory care
patients receiving warfarin are being managed by one or more of
these clinical practice improvement activities: Patients are being
managed by an anticoagulant management service, that involves
systematic and coordinated care*, incorporating comprehensive
patient education, systematic INR testing, tracking, follow-up, and
patient communication of results and dosing decisions; Patients are
being managed according to validated electronic decision support
and clinical management tools that involve systematic and
coordinated care, incorporating comprehensive patient education,
systematic INR testing, tracking, follow-up, and patient
communication of results and dosing decisions; For rural or remote
patients, patients are managed using remote monitoring or
telehealth options that involve systematic and coordinated care,
incorporating comprehensive patient education, systematic INR
testing, tracking, follow-up, and patient communication of results
and dosing decisions; and/or For patients who demonstrate
motivation, competency, and adherence, patients are managed using
either a patient self-testing (PST) or patient-self-management (PSM)
program. The performance threshold will increase to 75 percent for
the second performance year and onward. Clinicians would attest
that, 60 percent for first year, or 75 percent for the second year, of
their ambulatory care patients receiving warfarin participated in an
anticoagulation management program for at least 90 days during the
performance period. High
Care coordination agreements that
promote improvements in patient tracking
across settings
Establish effective care coordination and active referral
management that could include one or more of the following:
Establish care coordination agreements with frequently used
consultants that set expectations for documented flow of
information and MIPS eligible clinician or MIPS eligible
clinician group expectations between settings. Provide
patients with information that sets their expectations
consistently with the care coordination agreements; Track
patients referred to specialist through the entire process;
and/or Systematically integrate information from referrals into
the plan of care. Medium
Care transition documentation practice
improvements
Implementation of practices/processes for care transition that
include documentation of how a MIPS eligible clinician or
group carried out a patient-centered action plan for first 30
days following a discharge (e.g., staff involved, phone calls
conducted in support of transition, accompaniments,
navigation actions, home visits, patient information access,
etc.). Medium
Provided by Elizabeth W. Woodcock, MBA, FACMPE, CPC | Source: https://qpp.cms.gov

Care transition standard operational
improvements
Establish standard operations to manage transitions of care
that could include one or more of the following: Establish
formalized lines of communication with local settings in which
empaneled patients receive care to ensure documented flow
of information and seamless transitions in care; and/or
Partner with community or hospital-based transitional care
services. Medium
Chronic care and preventative care
management for empanelled patients
Proactively manage chronic and preventive care for
empaneled patients that could include one or more of the
following: Provide patients annually with an opportunity for
development and/or adjustment of an individualized plan of
care as appropriate to age and health status, including health
risk appraisal; gender, age and condition-specific preventive
care services; plan of care for chronic conditions; and advance
care planning; Use condition-specific pathways for care of
chronic conditions (e.g., hypertension, diabetes, depression,
asthma and heart failure) with evidence-based protocols to
guide treatment to target; Use pre-visit planning to optimize
preventive care and team management of patients with
chronic conditions; Use panel support tools (registry
functionality) to identify services due; Use reminders and
outreach (e.g., phone calls, emails, postcards, patient portals
and community health workers where available) to alert and
educate patients about services due; and/or Routine
medication reconciliation. Medium
CMS partner in Patients Hospital
Engagement Network
Membership and participation in a CMS Partnership for
Patients Hospital Engagement Network. Medium
Collection and follow-up on patient
experience and satisfaction data on
beneficiary engagement
Collection and follow-up on patient experience and
satisfaction data on beneficiary engagement, including
development of improvement plan. High
Collection and use of patient experience
and satisfaction data on access
Collection of patient experience and satisfaction data on
access to care and development of an improvement plan, such
as outlining steps for improving communications with patients
to help understanding of urgent access needs. Medium
Completion of the AMA STEPS Forward
program
Completion of the American Medical Association's STEPS
Forward program. Medium
Completion of training and receipt of
approved waiver for provision opioid
medication-assisted treatments
Completion of training and obtaining an approved waiver for
provision of medication-assisted treatment of opioid use
disorders using buprenorphine. Medium
Consultation of the Prescription Drug
Monitoring program
Clinicians would attest that, 60 percent for first year, or 75
percent for the second year, of consultation of prescription
drug monitoring program prior to the issuance of a Controlled
Substance Schedule II (CSII) opioid prescription that lasts for
longer than 3 days. High
Provided by Elizabeth W. Woodcock, MBA, FACMPE, CPC | Source: https://qpp.cms.gov

Depression screening
Depression screening and follow-up plan: Regular
engagement of MIPS eligible clinicians or groups in integrated
prevention and treatment interventions, including depression
screening and follow-up plan (refer to NQF #0418) for patients
with co-occurring conditions of behavioral or mental health
conditions. Medium
Diabetes screening
Diabetes screening for people with schizophrenia or bipolar
disease who are using antipsychotic medication. Medium
Electronic Health Record Enhancements
for BH data capture
Enhancements to an electronic health record to capture
additional data on behavioral health (BH) populations and use
that data for additional decision-making purposes (e.g.,
capture of additional BH data results in additional depression
screening for at-risk patient not previously identified). Medium
Engagement of community for health
status improvement
Take steps to improve health status of communities, such as
collaborating with key partners and stakeholders to
implement evidenced-based practices to improve a specific
chronic condition. Refer to the local Quality Improvement
Organization (QIO) for additional steps to take for improving
health status of communities as there are many steps to select
from for satisfying this activity. QIOs work under the direction
of CMS to assist MIPS eligible clinicians and groups with
quality improvement, and review quality concerns for the
protection of beneficiaries and the Medicare Trust Fund. Medium
Engagement of new Medicaid patients and
follow-up
Seeing new and follow-up Medicaid patients in a timely
manner, including individuals dually eligible for Medicaid and
Medicare. High
Engagement of patients, family and
caregivers in developing a plan of care
Engage patients, family and caregivers in developing a plan of
care and prioritizing their goals for action, documented in the
certified EHR technology. Medium
Engagement of patients through
implementation of improvements in
patient portal
Access to an enhanced patient portal that provides up to date
information related to relevant chronic disease health or
blood pressure control, and includes interactive features
allowing patients to enter health information and/or enables
bidirectional communication about medication changes and
adherence. Medium
Engagement with QIN-QIO to implement
self-management training programs
Engagement with a Quality Innovation Network-Quality
Improvement Organization, which may include participation in
self-management training programs such as diabetes. Medium
Engage patients and families to guide
improvement in the system of care.
Engage patients and families to guide improvement in the
system of care. Medium
Provided by Elizabeth W. Woodcock, MBA, FACMPE, CPC | Source: https://qpp.cms.gov

Enhancements/regular updates to practice
websites/tools that also include
considerations for patients with cognitive
disabilities
Enhancements and ongoing regular updates and use of
websites/tools that include consideration for compliance with
section 508 of the Rehabilitation Act of 1973 or for improved
design for patients with cognitive disabilities. Refer to the CMS
website on Section 508 of the Rehabilitation Act
https://www.cms.gov/Research-Statistics-Data-and-
Systems/CMS-Information-
Technology/Section508/index.html?redirect=/InfoTechGenInf
o/07_Section508.asp that requires that institutions receiving
federal funds solicit, procure, maintain and use all electronic
and information technology (EIT) so that equal or
alternate/comparable access is given to members of the public
with and without disabilities. For example, this includes
designing a patient portal or website that is compliant with
section 508 of the Rehabilitation Act of 1973 Medium
Evidenced-based techniques to promote
self-management into usual care
Incorporate evidence-based techniques to promote self-
management into usual care, using techniques such as goal
setting with structured follow-up, Teach Back, action planning
or motivational interviewing. Medium
Glycemic management services
For outpatient Medicare beneficiaries with diabetes and who
are prescribed antidiabetic agents (e.g., insulin, sulfonylureas),
MIPS eligible clinicians and groups must attest to having: For
the first performance year, at least 60 percent of medical
records with documentation of an individualized glycemic
treatment goal that: a) Takes into account patient-specific
factors, including, at least 1) age, 2) comorbidities, and 3) risk
for hypoglycemia, and b) Is reassessed at least annually. The
performance threshold will increase to 75 percent for the
second performance year and onward. Clinician would attest
that, 60 percent for first year, or 75 percent for the second
year, of their medical records that document individualized
glycemic treatment represent patients who are being treated
for at least 90 days during the performance period. High
Implementation of additional activity as a
result of TA for improving care
coordination
Implementation of at least one additional recommended
activity from the Quality Innovation Network-Quality
Improvement Organization after technical assistance has been
provided related to improving care coordination. Medium
Provided by Elizabeth W. Woodcock, MBA, FACMPE, CPC | Source: https://qpp.cms.gov

Implementation of analytic capabilities to
manage total cost of care for practice
population
Build the analytic capability required to manage total cost of
care for the practice population that could include one or
more of the following: Train appropriate staff on
interpretation of cost and utilization information; and/or Use
available data regularly to analyze opportunities to reduce
cost through improved care. Medium
Implementation of antibiotic stewardship
program
Implementation of an antibiotic stewardship program that
measures the appropriate use of antibiotics for several
different conditions (URI Rx in children, diagnosis of
pharyngitis, Bronchitis Rx in adults) according to clinical
guidelines for diagnostics and therapeutics Medium
Implementation of co-location PCP and
MH services
Integration facilitation, and promotion of the colocation of
mental health services in primary and/or non-primary clinical
care settings. High
Implementation of condition-specific
chronic disease self-management support
programs
Provide condition-specific chronic disease self-management
support programs or coaching or link patients to those
programs in the community. Medium
Implementation of documentation
improvements for practice/process
improvements
Implementation of practices/processes that document care
coordination activities (e.g., a documented care coordination
encounter that tracks all clinical staff involved and
communications from date patient is scheduled for outpatient
procedure through day of procedure). Medium
Implementation of episodic care
management practice improvements
Provide episodic care management, including management
across transitions and referrals that could include one or more
of the following: Routine and timely follow-up to
hospitalizations, ED visits and stays in other institutional
settings, including symptom and disease management, and
medication reconciliation and management; and/or Managing
care intensively through new diagnoses, injuries and
exacerbations of illness. Medium
Implementation of fall screening and
assessment programs
Implementation of fall screening and assessment programs to
identify patients at risk for falls and address modifiable risk
factors (e.g., Clinical decision support/prompts in the
electronic health record that help manage the use of
medications, such as benzodiazepines, that increase fall risk). Medium
Provided by Elizabeth W. Woodcock, MBA, FACMPE, CPC | Source: https://qpp.cms.gov

Implementation of formal quality
improvement methods, practice changes
or other practice improvement processes
Adopt a formal model for quality improvement and create a
culture in which all staff actively participates in improvement
activities that could include one or more of the following:
Train all staff in quality improvement methods; Integrate
practice change/quality improvement into staff duties; Engage
all staff in identifying and testing practices changes; Designate
regular team meetings to review data and plan improvement
cycles; Promote transparency and accelerate improvement by
sharing practice level and panel level quality of care, patient
experience and utilization data with staff; and/or Promote
transparency and engage patients and families by sharing
practice level quality of care, patient experience and utilization
data with patients and families. Medium
Implementation of improvements that
contribute to more timely communication
of test results
Timely communication of test results defined as timely
identification of abnormal test results with timely follow-up. Medium
Implementation of integrated PCBH model
Offer integrated behavioral health services to support patients
with behavioral health needs, dementia, and poorly controlled
chronic conditions that could include one or more of the
following: Use evidence-based treatment protocols and
treatment to goal where appropriate; Use evidence-based
screening and case finding strategies to identify individuals at
risk and in need of services; Ensure regular communication
and coordinated workflows between eligible clinicians in
primary care and behavioral health; Conduct regular case
reviews for at-risk or unstable patients and those who are not
responding to treatment; Use of a registry or certified health
information technology functionality to support active care
management and outreach to patients in treatment; and/or
Integrate behavioral health and medical care plans and
facilitate integration through co-location of services when
feasible. High
Implementation of medication
management practice improvements
Manage medications to maximize efficiency, effectiveness and
safety that could include one or more of the following:
Reconcile and coordinate medications and provide medication
management across transitions of care settings and eligible
clinicians or groups; Integrate a pharmacist into the care
team; and/or Conduct periodic, structured medication
reviews. Medium
Provided by Elizabeth W. Woodcock, MBA, FACMPE, CPC | Source: https://qpp.cms.gov

Implementation of methodologies for
improvements in longitudinal care
management for high risk patients
Provide longitudinal care management to patients at high risk
for adverse health outcome or harm that could include one or
more of the following: Use a consistent method to assign and
adjust global risk status for all empaneled patients to allow
risk stratification into actionable risk cohorts. Monitor the risk-
stratification method and refine as necessary to improve
accuracy of risk status identification; Use a personalized plan
of care for patients at high risk for adverse health outcome or
harm, integrating patient goals, values and priorities; and/or
Use on-site practice-based or shared care managers to
proactively monitor and coordinate care for the highest risk
cohort of patients. Medium
Implementation of practices/processes for
developing regular individual care plans
Implementation of practices/processes to develop regularly
updated individual care plans for at-risk patients that are
shared with the beneficiary or caregiver(s). Medium
Implementation of use of specialist
reports back to referring clinician or group
to close referral loop
Performance of regular practices that include providing
specialist reports back to the referring MIPS eligible clinician or
group to close the referral loop or where the referring MIPS
eligible clinician or group initiates regular inquiries to
specialist for specialist reports which could be documented or
noted in the certified EHR technology. Medium
Improved practices that disseminate
appropriate self-management materials
Provide self-management materials at an appropriate literacy
level and in an appropriate language. Medium
Improved practices that engage patients
pre-visit
Provide a pre-visit development of a shared visit agenda with
the patient. Medium
Integration of patient coaching practices
between visits
Provide coaching between visits with follow-up on care plan
and goals. Medium
Leadership engagement in regular
guidance and demonstrated commitment
for implementing practice improvement
changes
Ensure full engagement of clinical and administrative
leadership in practice improvement that could include one or
more of the following: Make responsibility for guidance of
practice change a component of clinical and administrative
leadership roles; Allocate time for clinical and administrative
leadership for practice improvement efforts, including
participation in regular team meetings; and/or Incorporate
population health, quality and patient experience metrics in
regular reviews of practice performance. Medium
Provided by Elizabeth W. Woodcock, MBA, FACMPE, CPC | Source: https://qpp.cms.gov

Leveraging a QCDR for use of standard
questionnaires
Participation in a QCDR, demonstrating performance of
activities for use of standard questionnaires for assessing
improvements in health disparities related to functional health
status (e.g., use of Seattle Angina Questionnaire, MD
Anderson Symptom Inventory, and/or SF-12/VR-12 functional
health status assessment). Medium
Leveraging a QCDR to promote use of
patient-reported outcome tools
Participation in a QCDR, demonstrating performance of
activities for promoting use of patient-reported outcome
(PRO) tools and corresponding collection of PRO data (e.g., use
of PQH-2 or PHQ-9 and PROMIS instruments). Medium
Leveraging a QCDR to standardize
processes for screening
Participation in a QCDR, demonstrating performance of
activities for use of standardized processes for screening for
social determinants of health such as food security,
employment and housing. Use of supporting tools that can be
incorporated into the certified EHR technology is also
suggested. Medium
MDD prevention and treatment
interventions
Major depressive disorder: Regular engagement of MIPS
eligible clinicians or groups in integrated prevention and
treatment interventions, including suicide risk assessment
(refer to NQF #0104) for mental health patients with co-
occurring conditions of behavioral or mental health
conditions. Medium
Measurement and improvement at the
practice and panel level
Measure and improve quality at the practice and panel level
that could include one or more of the following: Regularly
review measures of quality, utilization, patient satisfaction and
other measures that may be useful at the practice level and at
the level of the care team or MIPS eligible clinician or
group(panel); and/or Use relevant data sources to create
benchmarks and goals for performance at the practice level
and panel level. Medium
Participate in IHI Training/Forum Event;
National Academy of Medicine, AHRQ
Team STEPPS(R) or other similar activity.
For eligible professionals not participating in Maintenance of
Certification (MOC) Part IV, new engagement for MOC Part IV,
such as IHI Training/Forum Event; National Academy of
Medicine, AHRQ Team STEPPS(R) Medium
Participation in a 60-day or greater effort
to support domestic or international
humanitarian needs.
Participation in domestic or international humanitarian
volunteer work. Activities that simply involve registration are
not sufficient. MIPS eligible clinicians attest to domestic or
international humanitarian volunteer work for a period of a
continuous 60 days or greater. High
Participation in an AHRQ-listed patient
safety organization. Participation in an AHRQ-listed patient safety organization. Medium
Provided by Elizabeth W. Woodcock, MBA, FACMPE, CPC | Source: https://qpp.cms.gov

Participation in a QCDR, that promotes
collaborative learning network
opportunities that are interactive.
Participation in a QCDR, that promotes collaborative learning
network opportunities that are interactive. Medium
Participation in a QCDR, that promotes
implementation of patient self-action
plans.
Participation in a QCDR, that promotes implementation of
patient self-action plans. Medium
Participation in a QCDR, that promotes
use of patient engagement tools.
Participation in a QCDR, that promotes use of patient
engagement tools. Medium
Participation in a QCDR, that promotes
use of processes and tools that engage
patients for adherence to treatment plan.
Participation in a QCDR, that promotes use of processes and
tools that engage patients for adherence to treatment plan. Medium
Participation in Bridges to Excellence or
other similar program
Participation in other quality improvement programs such as
Bridges to Excellence Medium
Participation in CAHPS or other
supplemental questionnaire
Participation in the Consumer Assessment of Healthcare
Providers and Systems Survey or other supplemental
questionnaire items (e.g., Cultural Competence or Health
Information Technology supplemental item sets). High
Participation in CMMI models such as
Million Hearts Campaign
Participation in CMMI models such as the Million Hearts
Cardiovascular Risk Reduction Model Medium
Participation in Joint Commission
Evaluation Initiative
Participation in Joint Commission Ongoing Professional
Practice Evaluation initiative Medium
Participation in MOC Part IV
Participation in Maintenance of Certification (MOC) Part IV for
improving professional practice including participation in a
local, regional or national outcomes registry or quality
assessment program. Performance of monthly activities across
practice to regularly assess performance in practice, by
reviewing outcomes addressing identified areas for
improvement and evaluating the results. Medium
Participation in population health research
Participation in research that identifies interventions, tools or
processes that can improve a targeted patient population. Medium
Participation in private payer CPIA
Participation in designated private payer clinical practice
improvement activities. Medium
Participation in systematic anticoagulation
program
Participation in a systematic anticoagulation program
(coagulation clinic, patient self-reporting program, patient self-
management program)for 60 percent of practice patients in
year 1 and 75 percent of practice patients in year 2 who
receive anti-coagulation medications (warfarin or other
coagulation cascade inhibitors). High
Provided by Elizabeth W. Woodcock, MBA, FACMPE, CPC | Source: https://qpp.cms.gov

Participation on Disaster Medical
Assistance Team, registered for 6 months.
Participation in Disaster Medical Assistance Teams, or
Community Emergency Responder Teams. Activities that
simply involve registration are not sufficient. MIPS eligible
clinicians and MIPS eligible clinician groups must be registered
for a minimum of 6 months as a volunteer for disaster or
emergency response. Medium
Population empanelment
Empanel (assign responsibility for) the total population, linking
each patient to a MIPS eligible clinician or group or care team.
Empanelment is a series of processes that assign each active
patient to a MIPS eligible clinician or group and/or care team,
confirm assignment with patients and clinicians, and use the
resultant patient panels as a foundation for individual patient
and population health management. Empanelment identifies
the patients and population for whom the MIPS eligible
clinician or group and/or care team is responsible and is the
foundation for the relationship continuity between patient
and MIPS eligible clinician or group /care team that is at the
heart of comprehensive primary care. Effective empanelment
requires identification of the active population" of the
practice: those patients who identify and use your practice as
a source for primary care. There are many ways to define
"active patients" operationally allowing inclusion of younger
patients who have minimal acute or preventive health care." Medium
Practice improvements for bilateral
exchange of patient information
Ensure that there is bilateral exchange of necessary patient
information to guide patient care that could include one or
more of the following: Participate in a Health Information
Exchange if available; and/or Use structured referral notes. Medium
Practice improvements that engage
community resources to support patient
health goals
Develop pathways to neighborhood/community-based
resources to support patient health goals that could include
one or more of the following: Maintain formal (referral) links
to community-based chronic disease self-management
support programs, exercise programs and other wellness
resources with the potential for bidirectional flow of
information; and/or Provide a guide to available community
resources. Medium
Provided by Elizabeth W. Woodcock, MBA, FACMPE, CPC | Source: https://qpp.cms.gov

Provide 24/7 access to eligible clinicians or
groups who have real-time access to
patient's medical record
Provide 24/7 access to MIPS eligible clinicians, groups, or care
teams for advice about urgent and emergent care (e.g.,
eligible clinician and care team access to medical record, cross-
coverage with access to medical record, or protocol-driven
nurse line with access to medical record) that could include
one or more of the following: Expanded hours in evenings and
weekends with access to the patient medical record (e.g.,
coordinate with small practices to provide alternate hour
office visits and urgent care); Use of alternatives to increase
access to care team by MIPS eligible clinicians and groups,
such as e-visits, phone visits, group visits, home visits and
alternate locations (e.g., senior centers and assisted living
centers); and/or Provision of same-day or next-day access to
a consistent MIPS eligible clinician, group or care team when
needed for urgent care or transition management High
Provide peer-led support for self-
management. Provide peer-led support for self-management. Medium
Regularly assess the patient experience of
care through surveys, advisory councils
and/or other mechanisms.
Regularly assess the patient experience of care through
surveys, advisory councils and/or other mechanisms. Medium
Regular review practices in place on
targeted patient population needs
Implementation of regular reviews of targeted patient
population needs which includes access to reports that show
unique characteristics of eligible professional's patient
population, identification of vulnerable patients, and how
clinical treatment needs are being tailored, if necessary, to
address unique needs and what resources in the community
have been identified as additional resources. Medium
Regular training in care coordination Implementation of regular care coordination training. Medium
RHC, IHS or FQHC quality improvement
activities
Participating in a Rural Health Clinic (RHC), Indian Health
Service Medium Management (IHS), or Federally Qualified
Health Center in ongoing engagement activities that
contribute to more formal quality reporting in line with
Section 1848(q)(2)(B)(iii) of the Act that requires the Secretary
to give consideration to the circumstances of practices located
in rural areas and geographic HPSAs. Rural Health Clinics
would be included in that definition for consideration of
practices in rural areas. High
TCPI participation
Participation in the CMS Transforming Clinical Practice
Initiative. High
Provided by Elizabeth W. Woodcock, MBA, FACMPE, CPC | Source: https://qpp.cms.gov

Tobacco use
Tobacco use: Regular engagement of MIPS eligible clinicians or
groups in integrated prevention and treatment interventions,
including tobacco use screening and cessation interventions
(refer to NQF #0028) for patients with co-occurring conditions
of behavioral or mental health and at risk factors for tobacco
dependence. Medium
Unhealthy alcohol use
Unhealthy alcohol use: Regular engagement of MIPS eligible
clinicians or groups in integrated prevention and treatment
interventions, including screening and brief counseling (refer
to NQF #2152) for patients with co-occurring conditions of
behavioral or mental health conditions. Medium
Use evidence-based decision aids to
support shared decision-making.
Use evidence-based decision aids to support shared decision-
making. Medium
Use group visits for common chronic
conditions (e.g., diabetes).
Use group visits for common chronic conditions (e.g.,
diabetes). Medium
Use of certified EHR to capture patient
reported outcomes
In support of improving patient access, performing additional
activities that enable capture of patient reported outcomes
(e.g., home blood pressure, blood glucose logs, food diaries, at-
risk health factors such as tobacco or alcohol use, etc.) or
patient activation measures through use of certified EHR
technology, containing this data in a separate queue for
clinician recognition and review. Medium
Use of decision support and standardized
treatment protocols
Use decision support and standardized treatment protocols to
manage workflow in the team to meet patient needs. Medium
Use of patient safety tools
Use of tools that assist specialty practices in tracking specific
measures that are meaningful to their practice, such as use of
the Surgical Risk Calculator. Medium
Use of QCDR data for ongoing practice
assessment and improvements
Use of QCDR data, for ongoing practice assessment and
improvements in patient safety. Medium
Use of QCDR data for quality
improvement such as comparative
analysis reports across patient populations
Participation in a QCDR, clinical data registries, or other
registries run by other government agencies such as FDA, or
private entities such as a hospital or medical or surgical
society. Activity must include use of QCDR data for quality
improvement (e.g., comparative analysis across specific
patient populations for adverse outcomes after an outpatient
surgical procedure and corrective steps to address adverse
outcome). Medium
Use of QCDR for feedback reports that
incorporate population health
Use of a QCDR to generate regular feedback reports that
summarize local practice patterns and treatment outcomes,
including for vulnerable populations. High
Provided by Elizabeth W. Woodcock, MBA, FACMPE, CPC | Source: https://qpp.cms.gov

Use of QCDR patient experience data to
inform and advance improvements in
beneficiary engagement.
Use of QCDR patient experience data to inform and advance
improvements in beneficiary engagement. Medium
Use of QCDR to promote standard
practices, tools and processes in practice
for improvement in care coordination
Participation in a Qualified Clinical Data Registry,
demonstrating performance of activities that promote use of
standard practices, tools and processes for quality
improvement (e.g., documented preventative screening and
vaccinations that can be shared across MIPS eligible clinician
or groups). Medium
Use of QCDR to support clinical decision
making
Participation in a QCDR, demonstrating performance of
activities that promote implementation of shared clinical
decision making capabilities. Medium
Use of telehealth services that expand
practice access
Use of telehealth services and analysis of data for quality
improvement, such as participation in remote specialty care
consults or teleaudiology pilots that assess ability to still
deliver quality care to patients. Medium
Use of toolsets or other resources to close
healthcare disparities across communities
Take steps to improve healthcare disparities, such as
Population Health Toolkit or other resources identified by
CMS, the Learning and Action Network, Quality Innovation
Network, or National Coordinating Center. Refer to the local
Quality Improvement Organization (QIO) for additional steps
to take for improving health status of communities as there
are many steps to select from for satisfying this activity. QIOs
work under the direction of CMS to assist eligible clinicians
and groups with quality improvement, and review quality
concerns for the protection of beneficiaries and the Medicare
Trust Fund. Medium
Use of tools to assist patient self-
management
Use tools to assist patients in assessing their need for support
for self-management (e.g., the Patient Activation Measure or
How's My Health). Medium
Provided by Elizabeth W. Woodcock, MBA, FACMPE, CPC | Source: https://qpp.cms.gov

Provided by Elizabeth W. Woodcock, MBA, FACMPE, CPC | Source: https://qpp.cms.gov

Provided by Elizabeth W. Woodcock, MBA, FACMPE, CPC | Source: https://qpp.cms.gov

Provided by Elizabeth W. Woodcock, MBA, FACMPE, CPC | Source: https://qpp.cms.gov

Provided by Elizabeth W. Woodcock, MBA, FACMPE, CPC | Source: https://qpp.cms.gov

Provided by Elizabeth W. Woodcock, MBA, FACMPE, CPC | Source: https://qpp.cms.gov

Provided by Elizabeth W. Woodcock, MBA, FACMPE, CPC | Source: https://qpp.cms.gov

Provided by Elizabeth W. Woodcock, MBA, FACMPE, CPC | Source: https://qpp.cms.gov

Provided by Elizabeth W. Woodcock, MBA, FACMPE, CPC | Source: https://qpp.cms.gov

Provided by Elizabeth W. Woodcock, MBA, FACMPE, CPC | Source: https://qpp.cms.gov

Provided by Elizabeth W. Woodcock, MBA, FACMPE, CPC | Source: https://qpp.cms.gov

Provided by Elizabeth W. Woodcock, MBA, FACMPE, CPC | Source: https://qpp.cms.gov

Performance Period Measure TypeSubmission
Mechanism
Submission Criteria Data Completeness
A minimum of one
continous 90-day
period during CY2017
Individual
MIPS eligible
clinicans
Part B Claims Report at least six measures
including one outcome measure,
or if an outcome measure is not
available report another high
priority measure, if less than six
measures apply then report on
each measure that is applicale.
MIPS eligible clinicans and
groups will have to select their
measures from either the list of all
MIPS Measures in Table A or a
set of specialty-specific measures
in Table E.
50 percent of MIPS
eligible clinician’s
Medicare Part B patients
for the performance
period
A minimum of one
continuous 90-day
period during CY2017
Individual
MIPS eligible
clinicians or
Groups
QCDR
Qualified
Registry EHR
Report at least six measures
including one outcome measure,
or if an outcome measure is not
available report another high
priority measure; if less than six
measures apply then report on
each measure that is applicable.
MIPS eligible clinicians and
groups will have to select their
measures from either the list of all
MIPS Measures in Table A or a
set of specialty-specific measures
in Table E.
50 percent of MIPS
eligible clinician’s or
groups patients across
all payers for the
performance period
Jan 1- Dec 31 Groups CMS Web
Interface
Report on all measures included
in the CMS Web Interface; AND
populate data fields for the first
248 consecutively ranked and
assigned Medicare beneficiaries
in the order in which they appear
in the group’s sample for each
module/measure. If the pool of
eligible assigned beneficiaries is
less than 248, then the group
would report on 100 percent of
assigned beneficiaries.
Sampling requirements
for their Medicare Part B
patients
Table 5: Summary of Final Quality Data Submission Criteria for MIPS Payment Year 2019 via Part B Claims,
QCDR, Qualified Registry, EHR, CMS Web Interface, and CAHPS for MIPS Survey

Jan 1- Dec 31 Groups CAHPS for
MIPS Survey
CMS-approved survey vendor
would have to be paired with
another reporting mechanism to
ensure the minimum number of
measures are reported. CAHPS
for MIPS Survey would fulfill the
requirement for one patient
experience measure towards the
MIPS quality data submission
criteria. CAHPS for MIPS Survey
will only count for one measure.
Sampling requirements
for their Medicare Part B
patients
Source: https://qpp.cms.gov/docs/CMS-5517-FC.pdf. Pages 434-435.