Embed Size (px)
Citation preview
CVP measurement- III
ANATOMYFemoral vein is a direct continuation of the
popliteal vein. ↓ Ascends through the thigh, lying at first on the
lateral side of femoral artery, then posterior & then medial to it.
↓ Leaves the thigh, passes behind the inguinal
ligament to become the External iliac vein. ↓ Join its counterpart from the other leg → forms
the IVC (anterior & to the rt of L5 vertebrae).
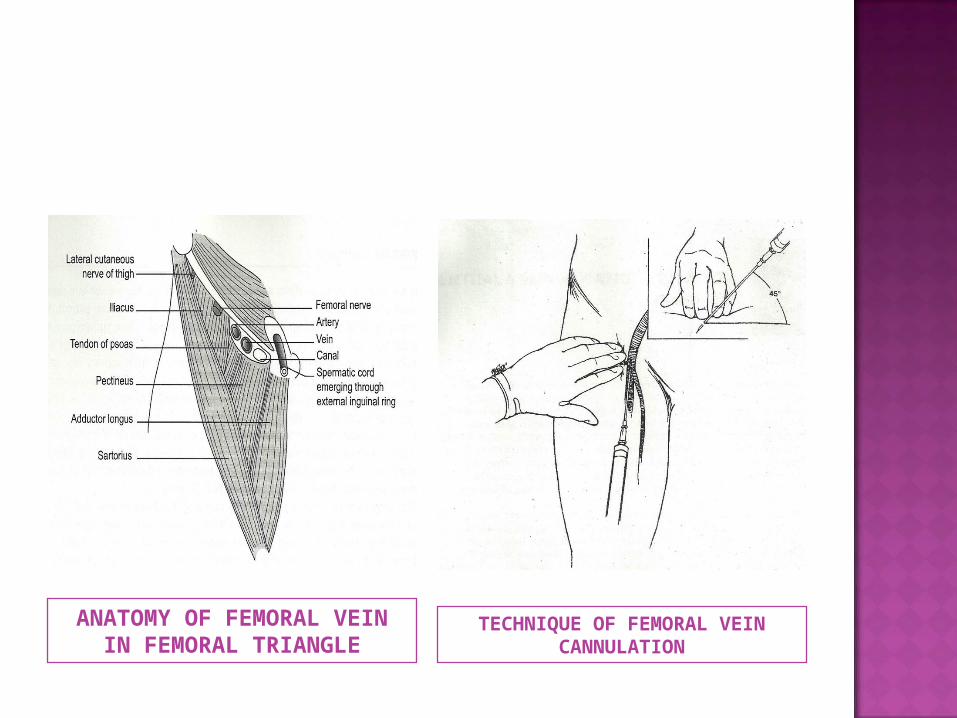
ANATOMY OF FEMORAL VEIN IN FEMORAL TRIANGLE
TECHNIQUE OF FEMORAL VEIN CANNULATION
1. Deep vein thrombosis & thrombophlebitis.
2. Pulmonary embolism.3. Sepsis.4. Femoral artery puncture .
1. Relatively simple.2. High success rate -
90-95%.3. Remote from the
airway & pleura.4. Directly
compressible.
1. Extremely high late complication rate.
2. Unsuitable for long term cannulation.
Peripherally inserted central catheters
• Alternative to centrally inserted catheters.• Venous access obtained through an
antecubital vein- basillic or cephalic vein.
ANATOMY Basilic vein- ulnar aspect of dorsal venous
network of hand. ↓Joins brachial vein to form axillary vein. ↓ Continues as Subclavian vein.
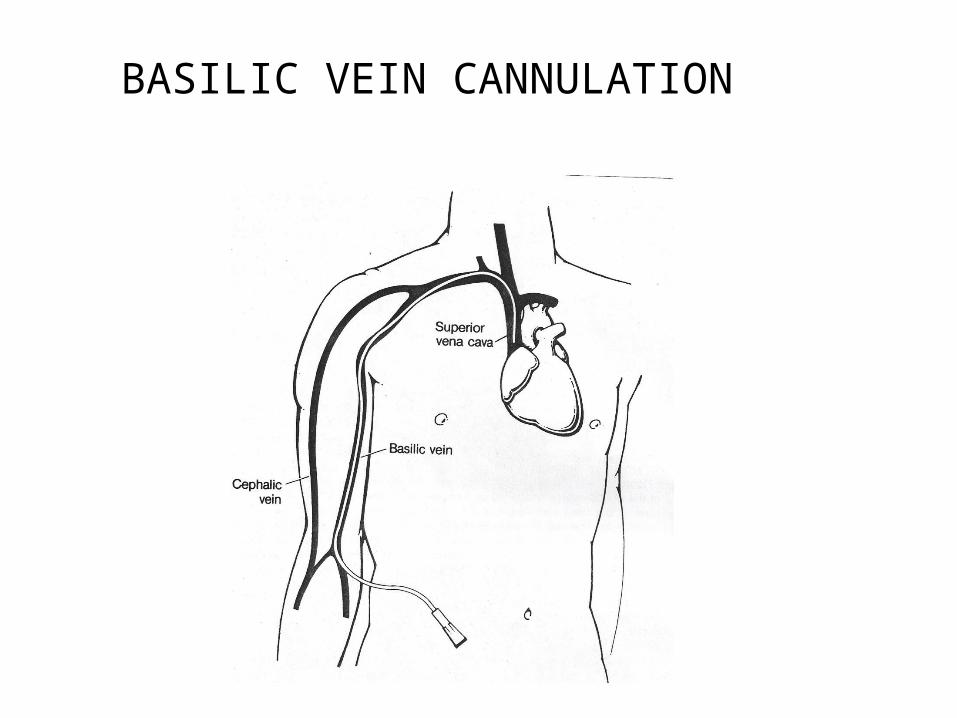
BASILIC VEIN CANNULATION
approach
– Patient’s arm at his/her side.– Antecubital fossa- prepared & draped. ↓– Tourniquet placed proximally.– Venepuncture- proximal to antecubital crease. ↓– Free back flow of venous blood– Tourniquet released & guidewire threaded (15-20 cms). ↓
↓
– Needle withdrawn & guidewire left in place.
– Thread sheath-introducer assembly over guidewire.
↓– Remove the guidewire.– Secure the catheter.– Rt basilic vein -52 cms.– Lt basilic vein – 56 cms.
complications
1. Thrombophlebitis.2. Limb edema.3. Hematoma at the puncture site.4. Infection.
Advantages disadvantages
1. Simplicity.2. Low complication rate3. Safe placement by non-
physicians.
1. Not suitable for long term placement.
2. Thrombophlebitis.3. Passageinto SVC
difficult.
complications
1. Vascular injury Arterial VenousHemothoraxCardiac tamponade
2. Respiratory compromise
Airway compression from hematoma.Tracheal, laryngeal injuryPneumothorax
3. Nerve injury
4. Arrhythmias
5. Thromboembolic Venous thrombosisPulmonary embolismArterial thrombosis & embolism (air, clot)Catheter or guidewire embolism
Complications contd….
6. Infectious Insertion site infectionCatheter infectionBloodstream infectionEndocarditis
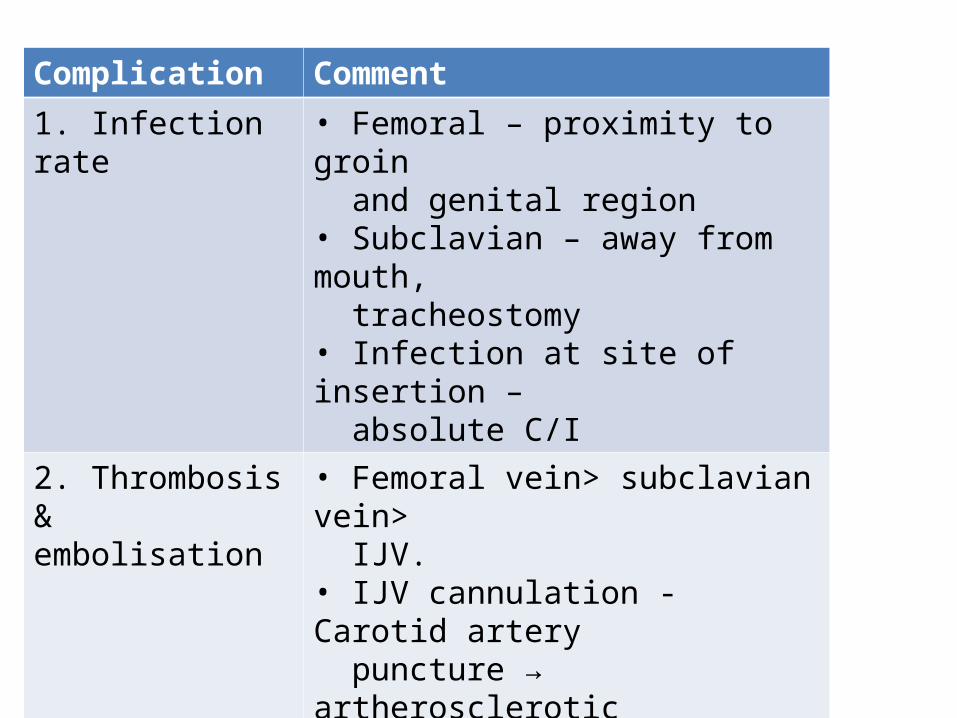
Complication Comment
1. Infection rate • Femoral – proximity to groin and genital region• Subclavian – away from mouth, tracheostomy• Infection at site of insertion – absolute C/I
2. Thrombosis & embolisation
• Femoral vein> subclavian vein> IJV.• IJV cannulation - Carotid artery puncture → artherosclerotic embolus to brain.( deadliest complication )
3. Vein stenosis • Catheter infection, mechanical stress
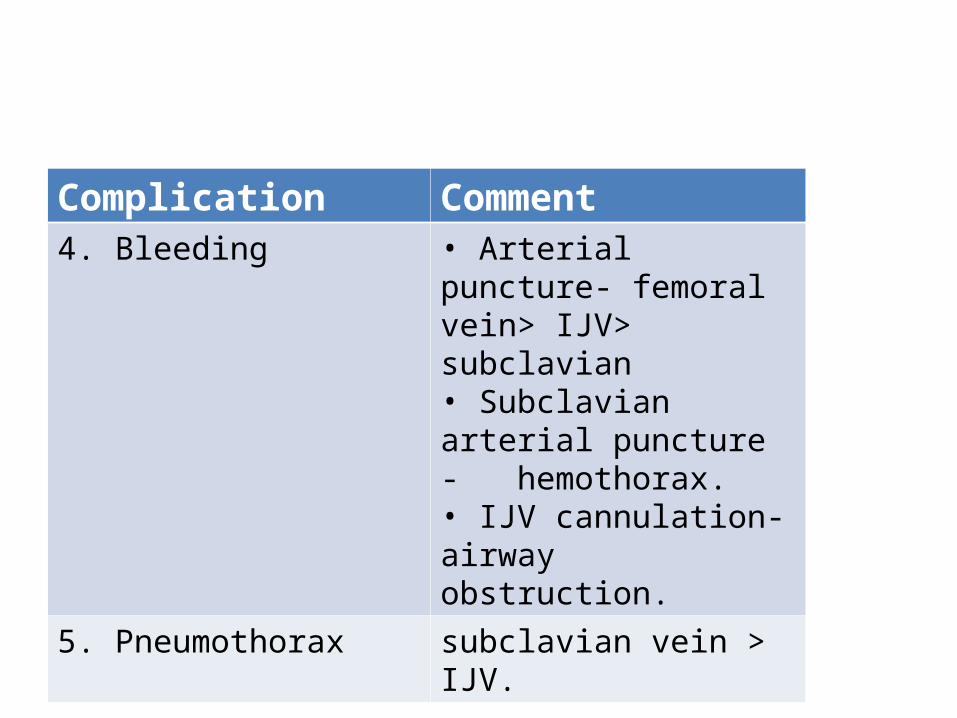
Complication Comment4. Bleeding • Arterial puncture-
femoral vein> IJV> subclavian• Subclavian arterial puncture - hemothorax.• IJV cannulation- airway obstruction.
5. Pneumothorax subclavian vein > IJV.
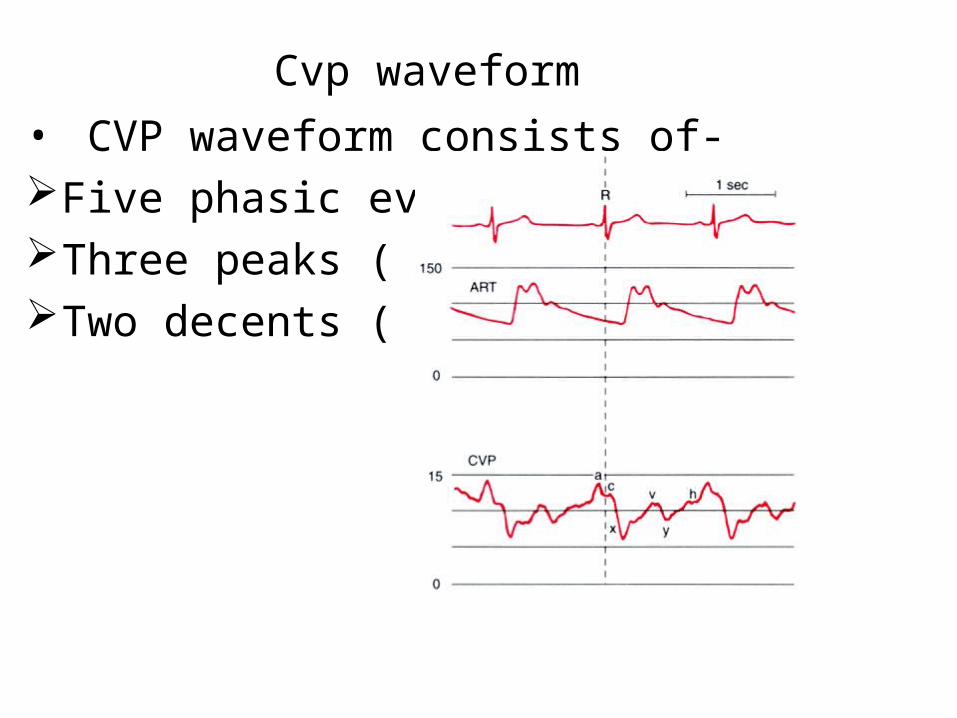
Cvp waveform• CVP waveform consists of-Five phasic eventsThree peaks ( a, c, v )Two decents ( x, y )
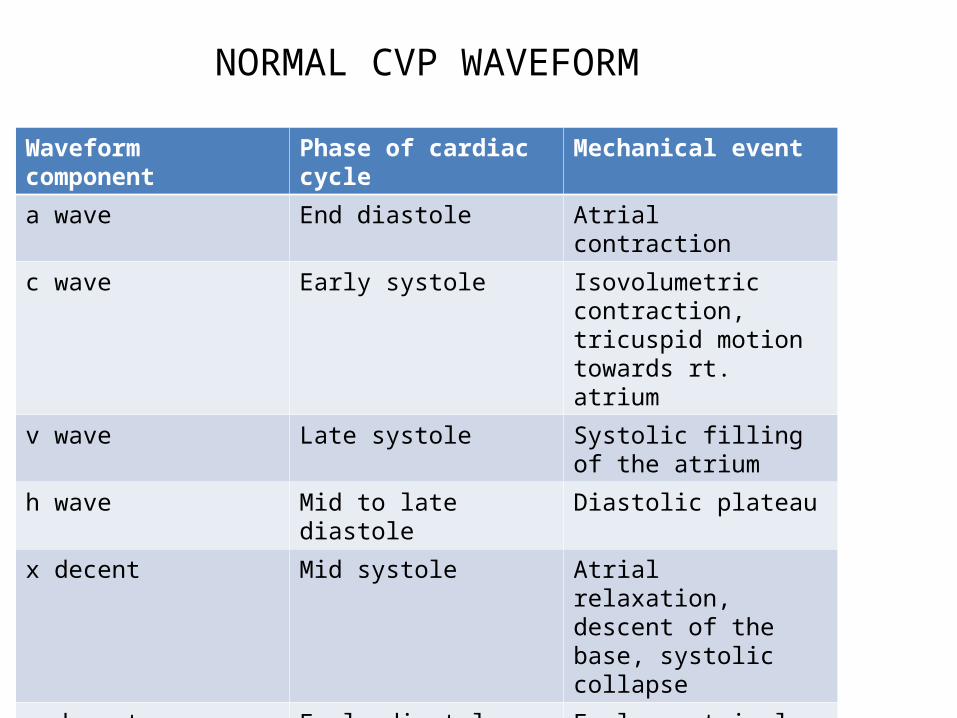
NORMAL CVP WAVEFORM
Waveform component Phase of cardiac cycle Mechanical event
a wave End diastole Atrial contraction
c wave Early systole Isovolumetric contraction, tricuspid motion towards rt. atrium
v wave Late systole Systolic filling of the atrium
h wave Mid to late diastole Diastolic plateau
x decent Mid systole Atrial relaxation, descent of the base, systolic collapse
y decent Early diastole Early ventricular filling, diastolic collapse
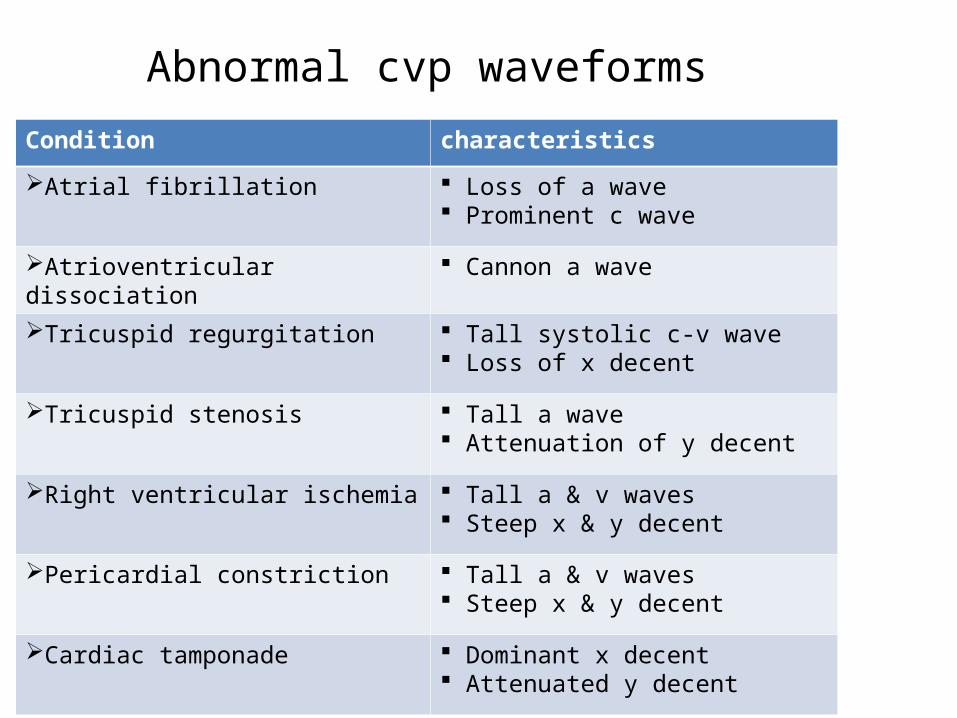
Abnormal cvp waveforms
Condition characteristics
Atrial fibrillation Loss of a wave Prominent c wave
Atrioventricular dissociation Cannon a wave
Tricuspid regurgitation Tall systolic c-v wave Loss of x decent
Tricuspid stenosis Tall a wave Attenuation of y decent
Right ventricular ischemia Tall a & v waves Steep x & y decent
Pericardial constriction Tall a & v waves Steep x & y decent
Cardiac tamponade Dominant x decent Attenuated y decent
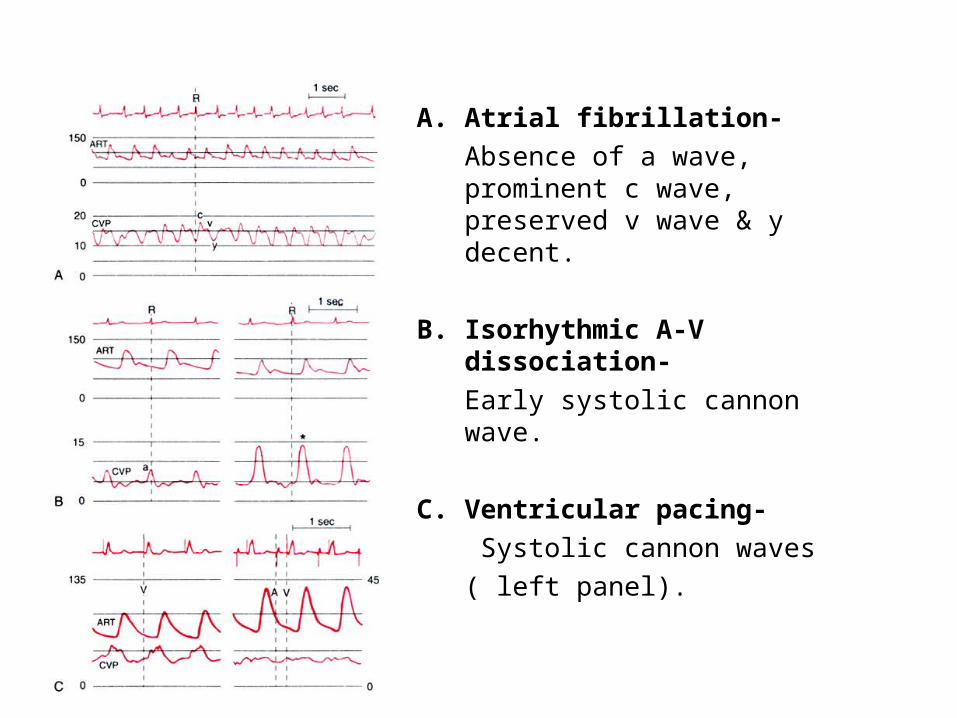
A. Atrial fibrillation- Absence of a wave, prominent c
wave, preserved v wave & y decent.
B. Isorhythmic A-V dissociation-Early systolic cannon wave.
C. Ventricular pacing- Systolic cannon waves ( left panel).
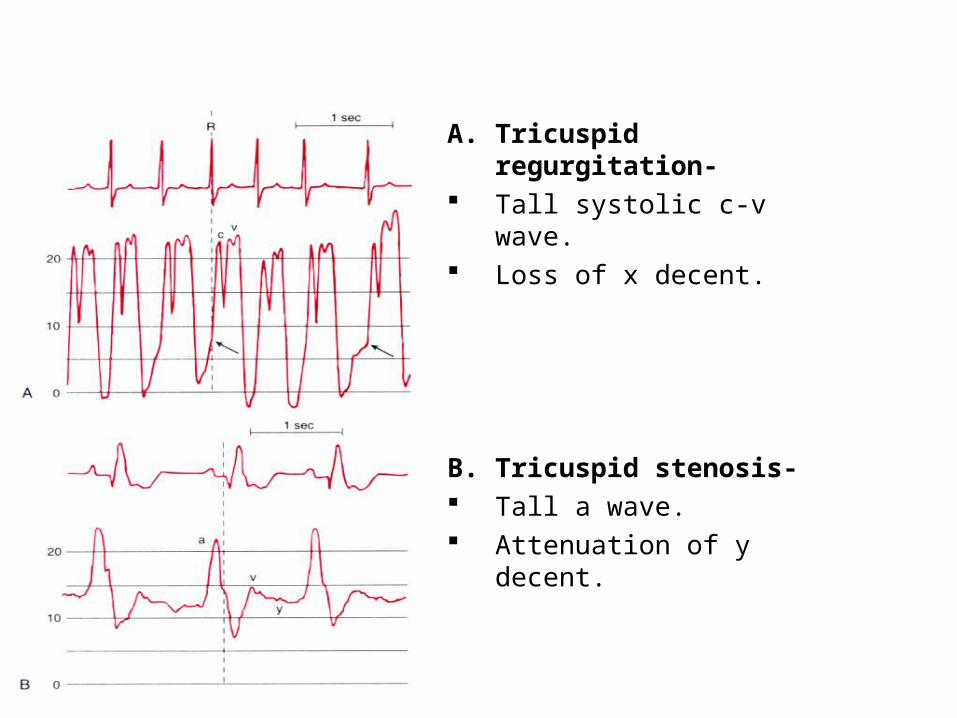
A. Tricuspid regurgitation- Tall systolic c-v wave. Loss of x decent.
B. Tricuspid stenosis- Tall a wave. Attenuation of y decent.
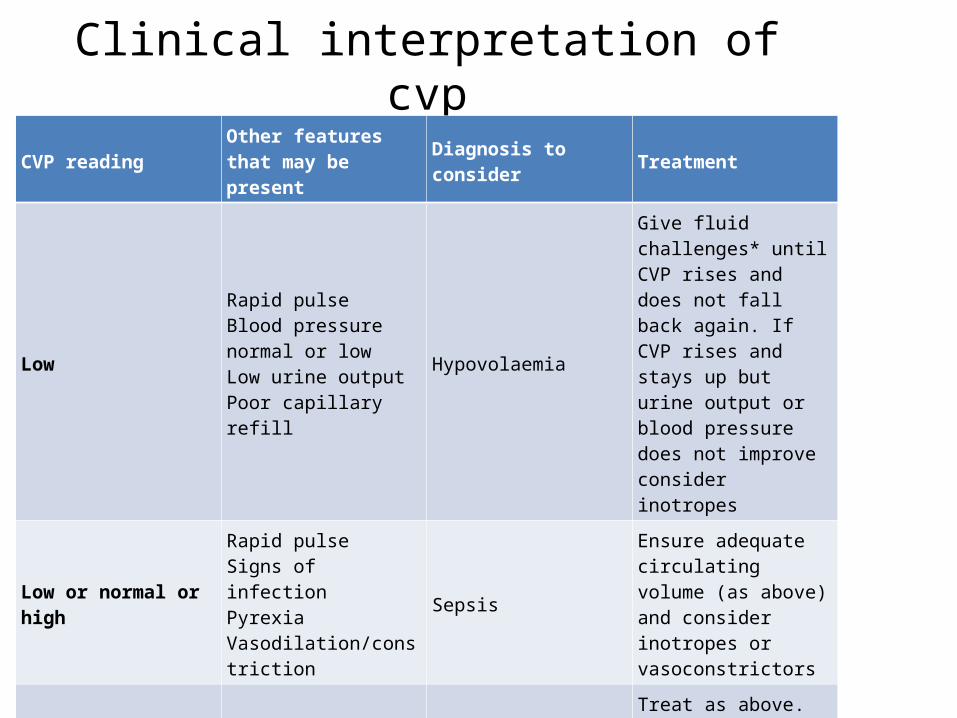
Clinical interpretation of cvp
CVP readingOther features that may be present
Diagnosis to consider Treatment
Low
Rapid pulseBlood pressure normal or lowLow urine outputPoor capillary refill
Hypovolaemia
Give fluid challenges* until CVP rises and does not fall back again. If CVP rises and stays up but urine output or blood pressure does not improve consider inotropes
Low or normal or high
Rapid pulseSigns of infectionPyrexiaVasodilation/constriction
Sepsis
Ensure adequate circulating volume (as above) and consider inotropes or vasoconstrictors
NormalRapid pulseLow urine outputPoor capillary refill
Hypovolaemia
Treat as above. Venoconstriction may cause CVP to be normal. Give fluid challenges* and observe effect as above.
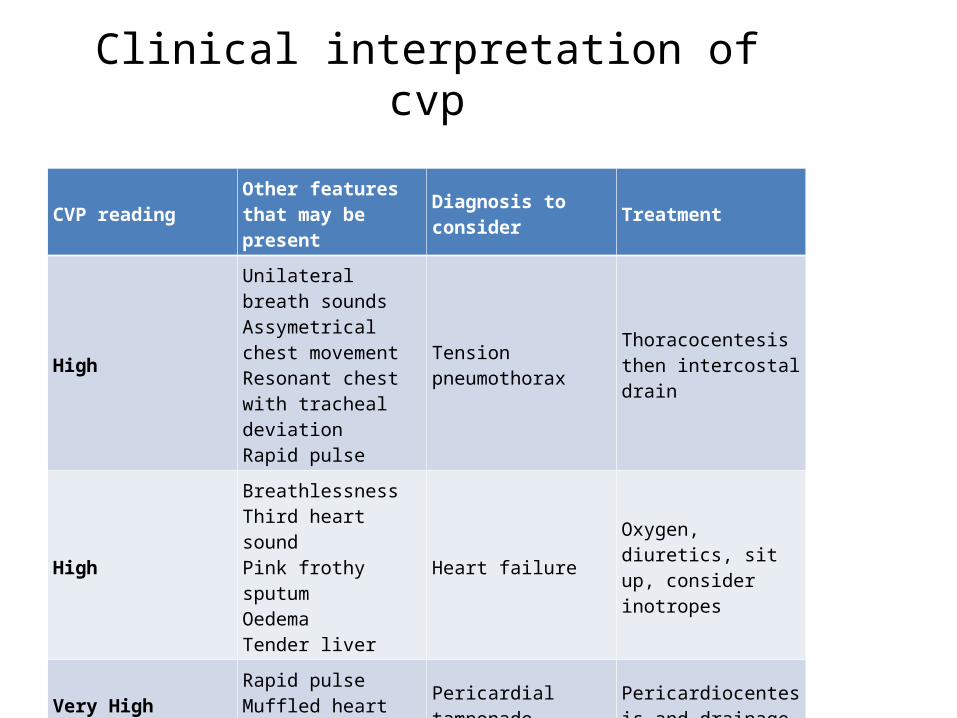
Clinical interpretation of cvp
CVP readingOther features that may be present
Diagnosis to consider Treatment
High
Unilateral breath soundsAssymetrical chest movementResonant chest with tracheal deviationRapid pulse
Tension pneumothoraxThoracocentesis then intercostal drain
High
BreathlessnessThird heart soundPink frothy sputumOedemaTender liver
Heart failureOxygen, diuretics, sit up, consider inotropes
Very HighRapid pulseMuffled heart sounds
Pericardial tamponadePericardiocentesis and drainage
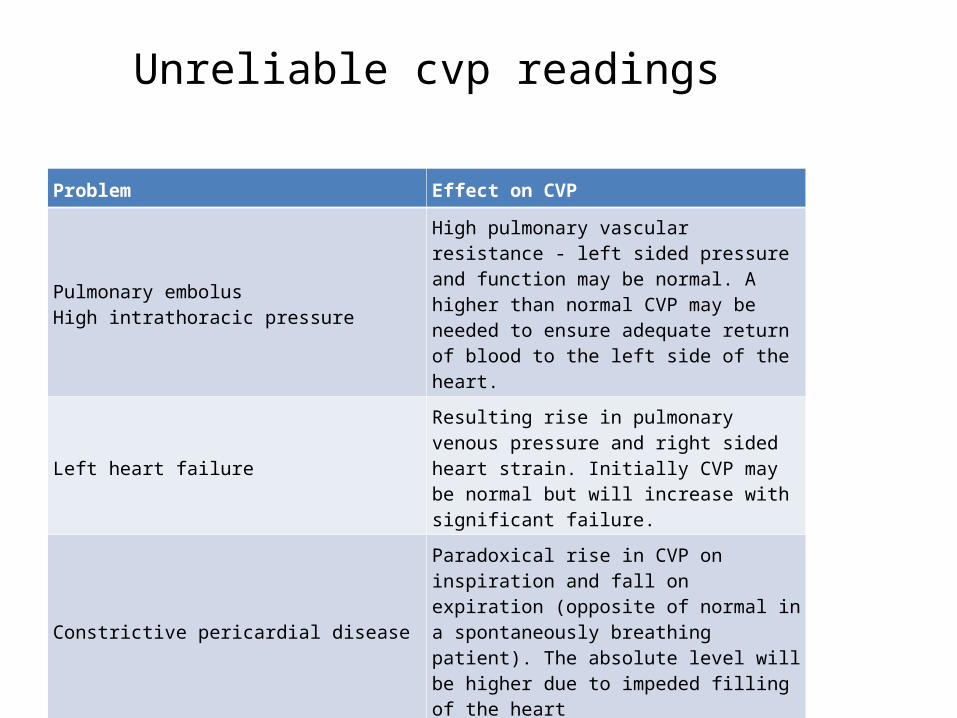
Unreliable cvp readings
Problem Effect on CVP
Pulmonary embolusHigh intrathoracic pressure
High pulmonary vascular resistance - left sided pressure and function may be normal. A higher than normal CVP may be needed to ensure adequate return of blood to the left side of the heart.
Left heart failureResulting rise in pulmonary venous pressure and right sided heart strain. Initially CVP may be normal but will increase with significant failure.
Constrictive pericardial disease
Paradoxical rise in CVP on inspiration and fall on expiration (opposite of normal in a spontaneously breathing patient). The absolute level will be higher due to impeded filling of the heart
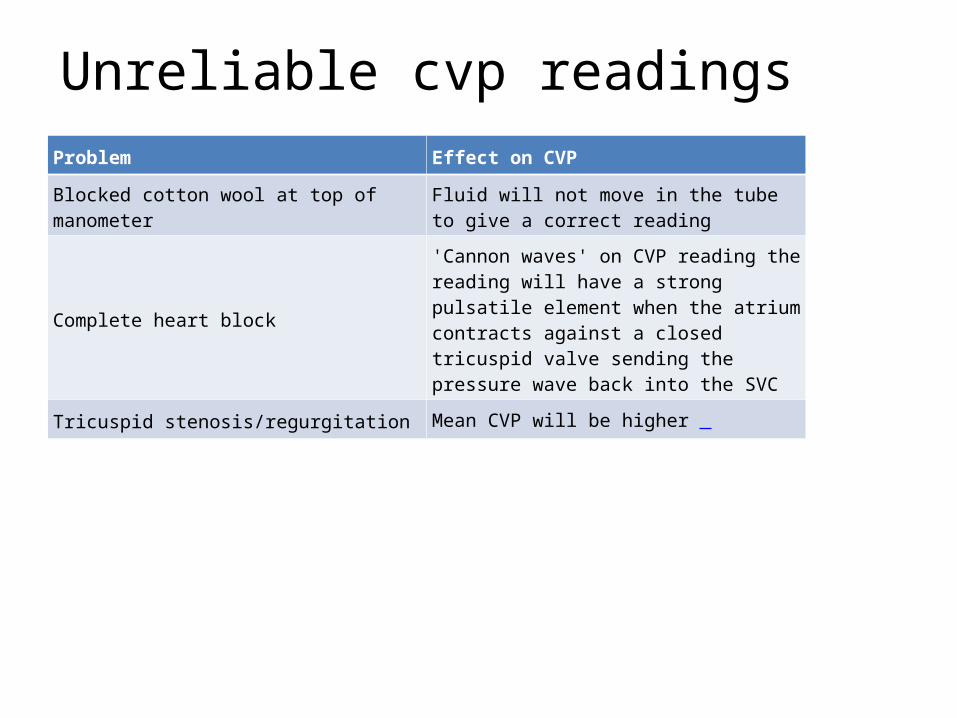
Unreliable cvp readingsProblem Effect on CVP
Blocked cotton wool at top of manometerFluid will not move in the tube to give a correct reading
Complete heart block
'Cannon waves' on CVP reading the reading will have a strong pulsatile element when the atrium contracts against a closed tricuspid valve sending the pressure wave back into the SVC
Tricuspid stenosis/regurgitation Mean CVP will be higher
summaryCVP is the pressure measured at the junction of
right atrium & SVC.Most sophisticated method of CVP measurement
is caliberated transducer.Most preferred route is IJV or subclavian vein.The possibility of pneumothorax remains upto 24
hrs, so patient should be watched for it.Strict aseptic precautions should be taken care of.CVP catheters are used for fluid administeration ,
especially in ICU’s.Femoral route , if possible should be avoided.
references
1. Miller’s Anesthesia. 7th edition. Cardiovascular monitoring.
2. Monitoring in Anaesthesia and Critical Care Medicine. 5th edition.
3. Mcleod’s Clinical Examination. 11th edition.4. Central Venous Catheters.2nd edition.5. Update in Anaesthesia. Central Venous Access
and Monitoring. Dr. Graham Hocking, Issue 12 (2000) Article 13.
6. Procedures, Techniques, And Minimally Invasive Monitoring in Intensive Care Medicine. 4th edition.
THANK YOU





























