Embed Size (px)
Citation preview
ORIGINAL ARTICLE
Cutaneous Sebaceous Neoplasms With a Focal GlandularPattern (Seboapocrine Lesions): A Clinicopathological
Study of Three Cases
Dmitry V. Kazakov, MD, PhD,* Eduardo Calonje, MD,† Dip RCPath, Arno Rutten, MD,‡
Kathrin Glatz, MD,§ and Michal Michal, MD*
Abstract: Presented here are three cutaneous sebaceous tumors
(one carcinoma and two sebaceomas), each demonstrating a focal
glandular pattern representing apocrine differentiation. The patients,
two males and one female, each clinically presented with a small
solitary nodule or tumor on the scalp. None of the patients had
features of Muir–Torre syndrome. Surgical removal of the lesions was
performed in all cases. None of the patients developed recurrence or
metastasis after surgery (follow-up ranged from 18 to 24 months).
The glandular areas represented a minor but significant component of
the lesions and appeared as glands of various complexity, mostly as
simple round or elongated tubular structures lined by a row of
cuboidal to columnar cells with eosinophilic cytoplasm and round
nuclei, with or without a distinct nucleolus. Decapitation secretion
was evident but not prominent. In both sebaceomas, at least a portion
of the glands had a peripheral small-cell layer that appeared similar to
the basal/myoepithelial cells of normal eccrine and apocrine ducts. In
some glands, the basal/myoepithelial cells seemed to have undergone
hyperplasia, resulting in two or more rows of cells that even formed
small islands, with an overall appearance reminiscent of basal cell
hyperplasia in the prostate, arising in the basal layer of the prostatic
glands. The descriptive terms seboapocrine carcinoma or seboapo-
crine sebaceoma are proposed for such lesions. These tumors may be
viewed as rare histopathological variants of sebaceous carcinoma and
sebaceoma, with a second type of differentiation along the lines of the
folliculosebaceous–apocrine unit.
Key Words: adnexal tumors, sebaceous neoplasms, apocrine
differentiation, multidirectional differentiation, myoepithelial cells
(Am J Dermatopathol 2007;29:359–364)
Sebaceous tumors of the skin are most commonly classifiedinto carcinoma (ocular and extraocular), sebaceoma, and
sebaceous adenoma.1 These show different degrees of
sebaceous differentiation and different architectural andcytological features, usually allowing clear histopathologicalseparation, although some histopathological overlap exists.The tumor cells in these sebaceous neoplasms grow mainly ina cohesive fashion, although rare tumors manifest distinctivegrowth patterns such as the rippled, labyrinthine/sinusoidal,and carcinoid-like ones that are apparently specific for lesionswith sebaceous differentiation and are encountered either sin-gly or in combination in cutaneous tumors with sebaceousdifferentiation.2–6 So-called adenoid and acinar patterns havebeen recorded in some examples of ocular sebaceus carcinoma,7
and rare sebaceous neoplasms have been reported to focallyexhibit apocrine differentiation.8,9 Presented here are threefurther cutaneous sebaceous tumors with a focal glandularpattern representing apocrine differentiation.
MATERIALS AND METHODSHistological slides from approximately 200 malignant
and benign cutaneous sebaceous tumors (ocular and extra-ocular carcinomas, sebaceomas, sebaceous adenomas, basalcell carcinoma with sebaceous differentiation, cystic seba-ceous tumor10), including those associated with the Muir–Torre syndrome,11 were evaluated. Cases of organoid nevus(nevus sebaceus of Jadassohn) and secondary tumors arisingin it were not studied and, when recognized histologically assuch, were excluded. Eight sebaceous tumors manifestinga glandular pattern were found. The term glandular is used todescribe structures containing lumina surrounded by epithelialcells, with or without evidence of decapitation secretion.Multiple sections were reviewed to exclude the possibility thatthese glandular areas might represent preexisting ducts orrepresent a pseudoglandular pattern attributable to variouscauses (holocrine secretion, cell discohesive arrangementattributable to necrosis, acantholysis, or myxoid degeneration),as was the case in five tumors that were subsequently excludedfrom the study. Clinical information and follow-up on the threeincluded cases were obtained from pathology reports, sub-mitting pathologists, patients, and their clinicians.
Paraffin blocks or reserved unstained slides wereavailable in two cases for immunohistochemical study.Immunohistochemical stains were performed on 5-mM-thick,formalin-fixed, paraffin-embedded tissue sections, and appro-priate controls were applied using the monoclonal and poly-clonal antisera listed in Table 1. The avidin–biotin complex or
From the *Sikl’s Department of Pathology, Charles University, MedicalFaculty Hospital, Pilsen, Czech Republic (D.V.K., M.M.); †Department ofDermatopathology, St John’s Institute of Dermatology, St Thomas’sHospital, London, England, UK (E.C.); ‡DermatohistopathologischeGemeinschaftspraxis, Friedrichshafen, Germany (A.R.); and §Institute ofPathology, University of Basel, Basel, Switzerland (K.G.).
Reprints: Dmitry V. Kazakov, MD, PhD, Sikl’s Department of Pathology,Charles University Medical Faculty Hospital, Alej Svobody 80, 304 60PILSEN, Czech Republic (e-mail: [email protected]).
Copyright � 2007 by Lippincott Williams & Wilkins
Am J Dermatopathol � Volume 29, Number 4, August 2007 359

streptavidin–biotin complex, labeled with peroxidase oralkaline phosphatase, were employed as the detection systems.Automated immunostaining employing the Lab Visionautomatic stainer was used.
RESULTS
Clinical DataThe patients, two males and one female, each clinically
presented with a small solitary nodule or tumor on the scalp(Table 2). Ulceration was seen in case 1, which representedsebaceous carcinoma. None of the patients had features ofMuir–Torre syndrome. Surgical removal of the lesions wasperformed in all cases. None of the patients developedrecurrence or metastasis after surgery (follow-up ranged from18 to 24 months).
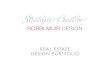
Histopathological FindingsOne case was classified as sebaceous carcinoma because
of the presence of architectural (asymmetry, infiltrativegrowth) and cytological atypia (cellular and nuclear pleomor-phism, cell necrosis, atypical mitoses; Fig. 1A–D). Twolesions were classified as sebaceomas (Fig. 2A–C). All threeneoplasms manifested a multinodular architecture and werepredominantly composed of basaloid cells and cells withvacuolated cytoplasm and scalloped nuclei. The neoplasmcells grew mainly in a cohesive fashion, but in both seba-ceomas, labyrinthine/sinusoidal, poorly developed carcinoid-like, and rippled patterns, as previously reported,2–4 wereidentified (Fig. 2B).
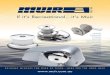
The glandular areas represented a minor but significantcomponent of the lesions; they appeared as glands of various
complexity, mostly as simple round or elongated tubularstructures lined by rows of cuboidal to columnar cells witheosinophilic cytoplasm and round nuclei, with or without adistinct nucleolus (Fig. 1E and F and Fig. 2D–F). Decapitationsecretion was evident but not prominent (Fig. 2E). In onesebaceoma (case 3), the cytoplasm of the luminal cells inglandular structures contained zymogen granules (Fig. 2F).In both sebaceomas, at least a portion of the glands had aperipheral small-cell layer that seemed similar to the basal/myoepithelial cells of normal eccrine and apocrine ducts. Thegland structures were numerous and were distributed some-what haphazardly. In some glands, the basal/myoepithelialcells seemed to have undergone hyperplasia, resulting in twoor more rows of cells that even formed small islands, with anoverall appearance reminiscent of basal cell hyperplasia inthe prostate, arising in the basal layer of the prostatic glands.(Fig. 2G). Glands with basal/myoepithelilal cells and thoselacking them were intermingled.
In one sebaceoma (case 2), there were foci of immaturesquamous metaplasia and areas composed of basaloid cells,devoid of sebaceous differentiation, that housed scatteredlymphocytes, with the resulting picture vaguely resemblinga spiradenoma. In both sebaceomas, differentiation towardsebaceous ducts was seen. No other metaplastic phenomena oradnexal-type differentiations were observed, nor were thereany recognizable microscopic features of nevus sebaceus ofJadassohn.
Immunohistochemical FindingsImmunohistochemical studies were performed on the
sebaceomas. The glandular areas were positive for CAM5.2and CK7 (Fig. 2H). Stains for CK7 also highlighted sebocyteswith multivacuolated cytoplasm, as did the stains for EMA(Fig. 2I). CK14 stained the entire tumors, including theglandular parts and basaloid cells; GCDFP-15 was tested incase 3 and proved positive in the glandular luminal cells. Theperipheral basal/myoepithelial-like cells in the glandular areaswere positive for p63 in both cases; they tested negative foractins in case 3.
DISCUSSIONWe have presented three sebaceous cutaneous neo-
plasms with a focal glandular pattern. The detection of thisfeature in an otherwise typical sebaceous tumor seems to haveno clinical or prognostic implication, but this microscopicfinding may be confusing. Two of the presented cases wereconsultations, and the submitting pathologists specifically
TABLE 1. Antibodies Used for Immunohistochemical Study
Antibody Specificity Clone Dilution Source
CK7 OV-TL 12/30 1:200 DakoCytomation
CK 14 Ll002 1:1000 NeoMarkers
EMA E29 1:700 DakoCytomation
CK 8 &18 CAM5.2 1:200 Becton Dickinson
ASMA 1A4 1:200 DakoCytomation
MSA HHF-35 1:5000 DakoCytomation
GCDFP-15 BRST-2 1:1000 Signet Laboratories
p63 4A4 1:500 Biotex
CK, cytokeratin; EMA, epithelial membrane antigen; ASMA, a-smooth muscleactin; MSA, muscle-specific actin; GCDFP-15, gross cystic disease fluid protein-15.
TABLE 2. The Main Clinical Features of Patients With Seboapocrine Carcinoma (Case 1) and Seboapocrine Sebaceomas(Cases 2 and 3)
Case Sex Age Location Clinical Presentation Size (cm) Treatment Follow-Up MTS
Case 1 Female 76 Scalp Solitary tumor 3 3 1.7 Excision NED at 29 months No
Case 2 Male 36 Scalp Solitary grey nodule.Atheroma? Fibroma?
1.2 3 0.8 Excision NED at 18 months No
Case 3 Male 84 Scalp Solitary tumor. BCC? 1 3 0.8 Excision NED at 24 months No
NED, no evidence of disease; MTS, Muir–Torre syndrome; BCC, basal cell carcinoma.
360 q 2007 Lippincott Williams & Wilkins
Kazakov et al Am J Dermatopathol � Volume 29, Number 4, August 2007

asked for the meaning of this feature and the preciseclassification of the lesions. We suggest that the descriptiveterms seboapocrine carcinoma, seboapocrine sebaceoma, orsebaceous carcinoma (or sebaceoma) with focal apocrinedifferentiation can be used in such situations. The termseboapocrine sebaceoma should not be mistaken for the termsebocrine adenoma, which has been used by Zaim8 to describetwo lesions that were regarded later as apocrine poroma.Conjoint apocrine, sebaceous and follicular differentiation ina cutaneous appendageal tumor, is not an unexpected findinggiven the embryological derivation of the apocrine gland,sebaceous gland, and hair follicle from the commonfolliculosebaceous–apocrine unit.12–14 The simultaneous occur-rence of two or three types of differentiation along the lines ofthe folliculosebaceous–apocrine unit in cutaneous adnexaltumors15–23 is not rare; it may, in fact, be underrecognized.
Combined folliculosebaceous–apocrine differentiation is quiteoften seen in apocrine mixed tumors12,24–26 and nevus sebaceusof Jadassohn.27–31 In the classification of cutaneous adnexalneoplasms proposed by McCalmont,32 the lesions that arereported herein can be added to the apocrine–sebaceouscategory to join apocrine poroma33–37 and may be viewed asexamples of adnexal tumors with divergent (multidirectional)differentiation.32,38–40 Parenthetically, a sebaceoma in one ofour patients manifested small areas resembling those seenin a spiradenoma, the entity that some authorities now con-sider an apocrine neoplasm.12,41 Evidence supporting thisissue is provided by the reported cases of spiradenomaassociated with areas of sebaceous and/or follicular differen-tiation in adnexal lesions or simultaneous occurrence ofspiradenoma and other follicular, sebaceous, or apocrineneoplasms in patients with Brooke–Spiegler syndrome, or
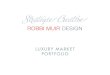
FIGURE 1. Sebaceous carcinoma. A and B, Asymmetric multinodular neoplasm with an infiltrative growth pattern. C and D,Cytological details: cohesive growth of cells with pleomorphic round nuclei and prominent nucleolus. The cytoplasm of some cellscontained tiny vacuoles and a mature sebocyte can be seen in the center. Note atypical mitotic figures. E and F, A glandularstructure with decapitation secretion.
q 2007 Lippincott Williams & Wilkins 361
Am J Dermatopathol � Volume 29, Number 4, August 2007 Seboapocrine Skin Tumors
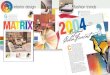
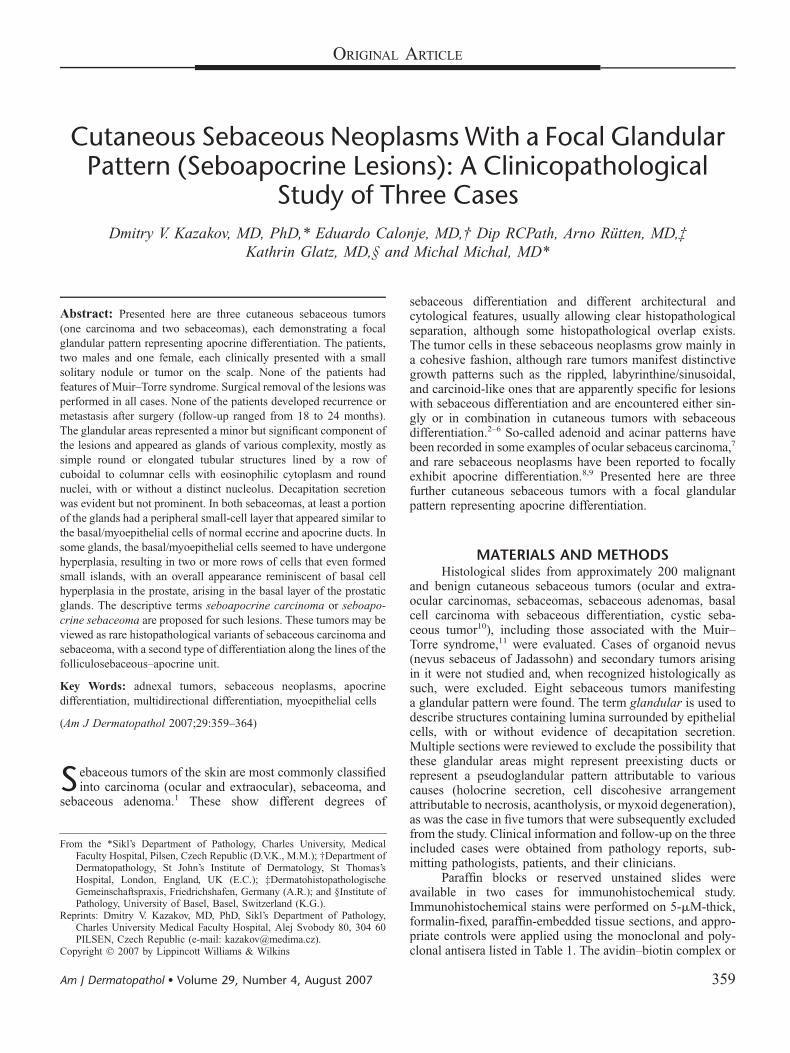
FIGURE 2. Sebaceoma. A, Whole-mount view of the vertically oriented multinodular lesion. B, Labyrinth-like /sinusoidal pattern.C, Cytological detail: monomorphous basaloid cells admixed with mature sebocytes. D–G, Glandular areas. Numerous elongatedtubules and small round lumens can be seen (D). Note rare vacuolated sebocytes in the adjacent areas (D, lower left). Glands ofmore complex architecture surrounded by a distinct peripheral basal/myoepithelial cell layer and decapitation secretion in theluminal cells (E). Zymogen granules in the luminal cells of the glands (F). In some glands, the basal/myoepithelial cell layer appearshyperplastic resulting in two or more rows of cells that even form small islands (G, arrows). This appearance can be linked to basalcell hyperplasia in the prostate. H and I, Immunohistochemical staining. The glandular structures are positive for CAM5.2, whereasthe rest of the tumor reacted negatively (H). Both scattered sebocytes with vacuolated cytoplasm and glandular structures arepositive for CK7 (I).
Kazakov et al Am J Dermatopathol � Volume 29, Number 4, August 2007
362 q 2007 Lippincott Williams & Wilkins

folliculosebaceous–apocrine tumors manifesting spiradenom-atous areas.12,40,42–51
The glandular patterns described above should be dis-tinguished from a pseudoglandular pattern, in which theformation of structures resembling glands is caused by the lossof integrity of solid epithelial structures attributable to cellnecrosis, acantholysis, or myxoid degeneration. Holocrinesecretion may sometimes impart a pseudoglandular appear-ance to a sebaceous tumor. Further, small aggregations ofneoplastic sebaceous cells with vacuolated cytoplasm mayproduce cleftlike spaces resembling tubules. Glandularpatterns, especially simple, small, round, tubular ones, shouldalso be distinguished from preexisting adnexal structures thatbecame entrapped by the tumor. Clues to the latter situationinclude a small number of tubular elements in the lesion, thelocation of tubular/ductal structures near the preexisting hairfollicle, or a traceable vertical arrangement suggesting involv-ed excretory ducts. The glands in both sebaceomas in ourseries were numerous—exceeding the number that one wouldexpect to see with the preexisting ducts—and were haphaz-ardly distributed. Still, we had the impression that theneoplastic tubules may have indeed originated from thepreexisting ducts, because some glands were surrounded inpart by a preserved basal/myoepithelial layer. On the otherhand, one cannot fully discard the fact that the ducts withbasal/myoepithelial cells may represent newly formed neo-plastic ducts. Three lines of evidence may indirectly supportthis preposition. First, the glands containing a peripheralbasal/myoepithelial cell layer and those lacking it wereintermingled, as if they belonged to the same origin. Second,they showed decapitation secretion, which is normally seenonly in the secretory part, and never in the ducts (hence,apocrine and eccrine ducts cannot be distinguished morpho-logically). Third, some glands showed focal hyperplasia ofcells comprising the peripheral layer, resulting in an appear-ance reminiscent of basal cell hyperplasia of the prostate. Toour knowledge, this feature has not been described in normaleccrine or apocrine ducts, but we have seen a similar phe-nomenon in rare examples of cutaneous tubular adenoma andsyringocystadenoma papilliferum (Kazakov et al, unpublishedobservations, 2006).
In summary, we have described three sebaceouscutaneous neoplasms with a focal glandular pattern, for whichthe descriptive terms seboapocrine carcinoma or seboapo-crine sebaceoma are proposed. These cases most probably donot represent separate entities; instead, they may be viewed asrare, histopathological variants of sebaceous carcinoma andsebaceoma, with a second type of differentiation along thelines of the folliculosebaceous–apocrine unit.
REFERENCES1. LeBoit PE, Burg G, Weedon D, et al. World Health Organization
Classification of Tumours. Pathology and Genetics of Skin Tumours.Lyon; France: IARC Press; 2006.
2. Ackerman AB, Ball E, Guo Y. Labyrinthine/sinusoidal pattern insebaceoma. Dermatopathol Pract Conc. [serial online]. 2002;8. Availableat: http://www.derm101.com/dynaweb/resources/dpc/136403/@Generic_BookTextView/136403;cs¼pr. Accessed October 2006.
3. Ohata C, Ackerman AB. ‘‘Ripple pattern’’ in a neoplasm signifies seba-ceous differentiation [sebaceoma (not trichoblastoma or trichomatricoma)
if benign and sebaceous carcinoma if malignant]. Dermatopathol PractConc. [serial online]. 2001;7:355–362. Available at: http://www.derm101.com/dynaweb/resources/dpc/130926/@Generic_BookTextView/130926;cs¼pr. Accessed October 2006.
4. Kazakov DV, Kutzner H, Rutten A, et al. Carcinoid-like pattern insebaceous neoplasms: another distinctive, previously unrecognizedpattern in extraocular sebaceous carcinoma and sebaceoma. Am JDermatopathol. 2005;27:195–203.
5. Requena L, Barat A. Giant trichoblastoma on the scalp. Am JDermatopathol. 1993;15:497–502.
6. Graham BS, Barr RJ. Rippled-pattern sebaceous trichoblastoma. J CutanPathol. 2000;27:455–459.
7. Ni C, Searl SS, Kuo PK, et al. Sebaceous cell carcinomas of the ocularadnexa. Int Ophthalmol Clin. 1982;22:23–61.
8. Zaim MT. Sebocrine adenoma. An adnexal adenoma with sebaceous andapocrine poroma-like differentiation. Am J Dermatopathol. 1988;10:311–318.
9. Okuda C, Ito M, Fujiwara H, et al. Sebaceous epithelioma with sweatgland differentiation. Am J Dermatopathol. 1995;17:523–528.
10. Rutten A, Burgdorf W, Hugel H, et al. Cystic sebaceous tumors as markerlesions for the Muir-Torre syndrome: a histopathologic and moleculargenetic study. Am J Dermatopathol. 1999;21:405–413.
11. Mathiak M, Rutten A, Mangold E, et al. Loss of DNA mismatch repairproteins in skin tumors from patients with Muir-Torre syndrome andMSH2 or MLH1 germline mutations: establishment of immunohisto-chemical analysis as a screening test. Am J Surg Pathol. 2002;26:338–343.
12. Requena L, Kiryu H, Ackerman AB. Neoplasms with ApocrineDifferentiation. Philadelphia, Pa: Lippincott-Raven; 1998.
13. Ackerman AB, Reddy VB, Soyer HP. Neoplasms with FollicularDifferentiation. 2nd ed. New York, NY: Ardor Scribendi Publishers; 2001.
14. Requena L. Neoplasias Anexiales Cutaneas. Madrid, Spain: Aulo MedicoEdiciones; 2004.
15. Hanau D, Grosshans E, Laplanche G. A complex poroma-like adnexaladenoma. Am J Dermatopathol. 1984;6:567–572.
16. Sanchez Yus E, Requena L, Simon P, et al. Complex adnexal tumor of theprimary epithelial germ with distinct patterns of superficial epitheliomawith sebaceous differentiation, immature trichoepithelioma, and apocrineadenocarcinoma. Am J Dermatopathol. 1992;14:245–252.
17. Boyd AS, Rapini RP. Cutaneous collision tumors. An analysis of 69 casesand review of the literature. Am J Dermatopathol. 1994;16:253–257.
18. Pujol RM, LeBoit PE, Su WP. Microcystic adnexal carcinoma with exten-sive sebaceous differentiation. Am J Dermatopathol. 1997;19:358–362.
19. Gianotti R, Alessi E. Clear cell hidradenoma associated with the folliculo-sebaceous-apocrine unit. Histologic study of five cases. Am JDermatopathol. 1997;19:351–357.
20. Gianotti R, Coggi A, Alessi E. Cutaneous apocrine mixed tumor: derivedfrom the apocrine duct of the folliculo-sebaceous-apocrine unit? Am JDermatopathol. 1998;20:323–325.
21. Heenan PJ. Sebaceous differentiation in microcystic adnexal carcinoma.Am J Dermatopathol. 1998;20:537–538.
22. Usmani AS, Rofagha R, Hessel AB. Trichoblastic neoplasm with apocrinedifferentiation. Am J Dermatopathol. 2002;24:358–360.
23. Kazakov DV, Mukensnabl P, Michal M. Tubular adenoma of the skin withfollicular and sebaceous differentiation: a report of two cases. Am JDermatopathol. 2006;28:142–146.
24. Hassab-el-Naby HM, Tam S, White WL, et al. Mixed tumors of the skin.A histological and immunohistochemical study. Am J Dermatopathol.1989;11:413–428.
25. Requena L, Sanchez Yus E, Santa Cruz DJ. Apocrine type of cutaneousmixed tumor with follicular and sebaceous differentiation. Am JDermatopathol. 1992;14:186–194.
26. Salama ME, Azam M, Ma CK, et al. Chondroid syringoma. Cytokeratin 20immunolocalization of Merkel cells and reappraisal of apocrine folliculo-sebaceous differentiation. Arch Pathol Lab Med. 2004;128:986–990.
27. van der Putte SC. Apoeccrine glands in nevus sebaceus. Am JDermatopathol. 1994;16:23–30.
28. Ng WK. Nevus sebaceus with apocrine and sebaceous differentiation.Am J Dermatopathol. 1996;18:420–423.
29. Shapiro M, Johnson B Jr, Witmer W, et al. Spiradenoma arising ina nevus sebaceus of Jadassohn: case report and literature review.Am J Dermatopathol. 1999;21:462–467.
30. Jaqueti G, Requena L, Sanchez Yus E. Trichoblastoma is the mostcommon neoplasm developed in nevus sebaceus of Jadassohn:
q 2007 Lippincott Williams & Wilkins 363
Am J Dermatopathol � Volume 29, Number 4, August 2007 Seboapocrine Skin Tumors

a clinicopathologic study of a series of 155 cases. Am J Dermatopathol.2000;22:108–118.
31. Cribier B, Scrivener Y, Grosshans E. Tumors arising in nevus sebaceus:a study of 596 cases. J Am Acad Dermatol. 2000;42:263–268.
32. McCalmont TH. A call for logic in the classification of adnexalneoplasms. Am J Dermatopathol. 1996;18:103–109.
33. Harvell JD, Kerschmann RL, LeBoit PE. Eccrine or apocrine poroma? Sixporomas with divergent adnexal differentiation. Am J Dermatopathol.1996;18:1–9.
34. Groben PA, Hitchcock MG, Leshin B, et al. Apocrine poroma: a distinctivecase in a patient with nevoid basal cell carcinoma syndrome. Am JDermatopathol. 1999;21:31–33.
35. Lee NH, Lee SH, Ahn SK. Apocrine poroma with sebaceousdifferentiation. Am J Dermatopathol. 2000;22:261–263.
36. Misago N, Narisawa Y. Sebaceous carcinoma with apocrine differenti-ation. Am J Dermatopathol. 2001;23:50–57.
37. Santos-Briz A, Rodriguez-Peralto JL, Miguelez A, et al. Trichoblastomaarising within an apocrine poroma. Am J Dermatopathol. 2002;24:59–62.
38. Nakhleh RE, Swanson PE, Wick MR. Cutaneous adnexal carcinomas withdivergent differentiation. Am J Dermatopathol. 1990;12:325–334.
39. Wong TY, Suster S, Cheek RF, et al. Benign cutaneous adnexal tumorswith combined folliculosebaceous, apocrine, and eccrine differentiation.Clinicopathologic and immunohistochemical study of eight cases. Am JDermatopathol. 1996;18:124–136.
40. Kazakov DV, Kutzner H, Mukensnabl P, et al. Low-grade adnexalcarcinoma of the skin with multidirectional (glandular, trichoblastoma-tous, spiradenocylindromatous) differentiation. Am J Dermatopathol.2006;28:341–345.
41. Michal M. Spiradenoma associated with apocrine adenoma component.Pathol Res Pract. 1996;192:1135–1139.
42. Gubareva AV. [Mixed tumors of the skin]. Arkh Patol. 1963;25:17–24.43. Apatenko AK. [Eccrine spiradenoma of the skin]. Arkh Patol. 1965;27:
25–32.44. Weyers W, Nilles M, Eckert F, et al. Spiradenomas in Brooke-Spiegler
syndrome. Am J Dermatopathol. 1993;15:156–161.45. Puig L, Nadal C, Fernandez-Figueras MT, et al. Brooke-Spiegler
syndrome variant: segregation of tumor types with mixed differentiationin two generations. Am J Dermatopathol. 1998;20:56–60.
46. Biernat W, Biernat S. Cutaneous adnexal carcinoma arising withina solitary cylindroma-spiradenoma. Am J Dermatopathol. 1996;18:77–82.
47. Michal M, Lamovec J, Mukensnabl P, et al. Spiradenocylindromas of theskin: tumors with morphological features of spiradenoma and cylindromain the same lesion: report of 12 cases. Pathol Int. 1999;49:419–425.
48. Clarke J, Ioffreda M, Helm KF. Multiple familial trichoepitheliomas:a folliculosebaceous-apocrine genodermatosis. Am J Dermatopathol.2002;24:402–405.
49. Uede K, Yamamoto Y, Furukawa F. Brooke-Spiegler syndrome associatedwith cylindroma, trichoepithelioma, spiradenoma, and syringoma.J Dermatol. 2004;31:32–38.
50. De Francesco V, Frattasio A, Pillon B, et al. Carcinosarcoma arising ina patient with multiple cylindromas. Am J Dermatopathol. 2005;27:21–26.
51. Kazakov DV, Soukup R, Mukensnabl P, et al. Brooke-Spiegler syndrome:report of a case with combined lesions containing cylindromatous,spiradenomatous, trichoblastomatous, and sebaceous differentiation. Am JDermatopathol. 2005;27:27–33.
364 q 2007 Lippincott Williams & Wilkins
Kazakov et al Am J Dermatopathol � Volume 29, Number 4, August 2007