Embed Size (px)
Citation preview
Maryam Khaja, Rihab Kaissi, BSc(pharm)
Doctor of Pharmacy Students
College of Pharmacy
19 th of January 2012
CUSHING’S SYNDROME
1
� Introduction
� Epidemiology
� Causes
� Pathophysiology
� Clinical presentation
� Diagnosis
� Complications
� Goals of therapy
� Treatment
� Prognosis
Outline
2
� In 1932, Cushing first described a syndrome of pituitary basophilism
� Until this time patients with:
� Unexplained central obesity
� Cutaneous striae
� Osteoporosis, weakness
� Hypertension
� Diabetes mellitus
� No definite diagnosis
� Cushing emphasized that the disease was of pituitary origin
Introduction
3
DiPiro JT. Pharmacotherapy: A pathophysiologic approach. New York: McGraw Hill; 2008.
� Ten years later, after the development of the method for measuring urinary steroids
� Daughaday discovered ↑↑ steroids in the urine of patients
with cushing’s disease
� Finally, the end product was identified
� Cushing’s syndrome was correctly explained
� An excess of cortisol in the plasma (hypercortisolism)
Introduction
4
DiPiro JT. Pharmacotherapy: A pathophysiologic approach. New York: McGraw Hill; 2008.
� Most cases of Cushing syndrome are due to
� Exogenous glucocorticoids
� Incidence of endogenous Cushing syndrome has been estimated at 13 cases per million individuals
� 70% � a pituitary ACTH-producing tumor
� 15% � ectopic ACTH
� 15% � a primary adrenal tumor
� Female-to-male incidence ratio is approximately 5:1
� Adrenal or pituitary tumor
Epidemiology
5DiPiro JT. Pharmacotherapy: A pathophysiologic approach. New York: McGraw Hill; 2008.Brown RJ, Kelly MH, Collins MT. Cushing Syndrome in the McCune-Albright Syndrome. J ClinEndocrinol Metab. Feb 15 2010
� Ectopic Adrenocorticotropic hormone (ACTH) production men >women
� The increased incidence of lung tumors
� The peak incidence of Cushing syndrome due to
� An adrenal or pituitary adenoma is in persons aged 25-40 years
� Ectopic ACTH production due to lung cancer occurs later in life
Epidemiology
6
DiPiro JT. Pharmacotherapy: A pathophysiologic approach. New York: McGraw Hill; 2008.
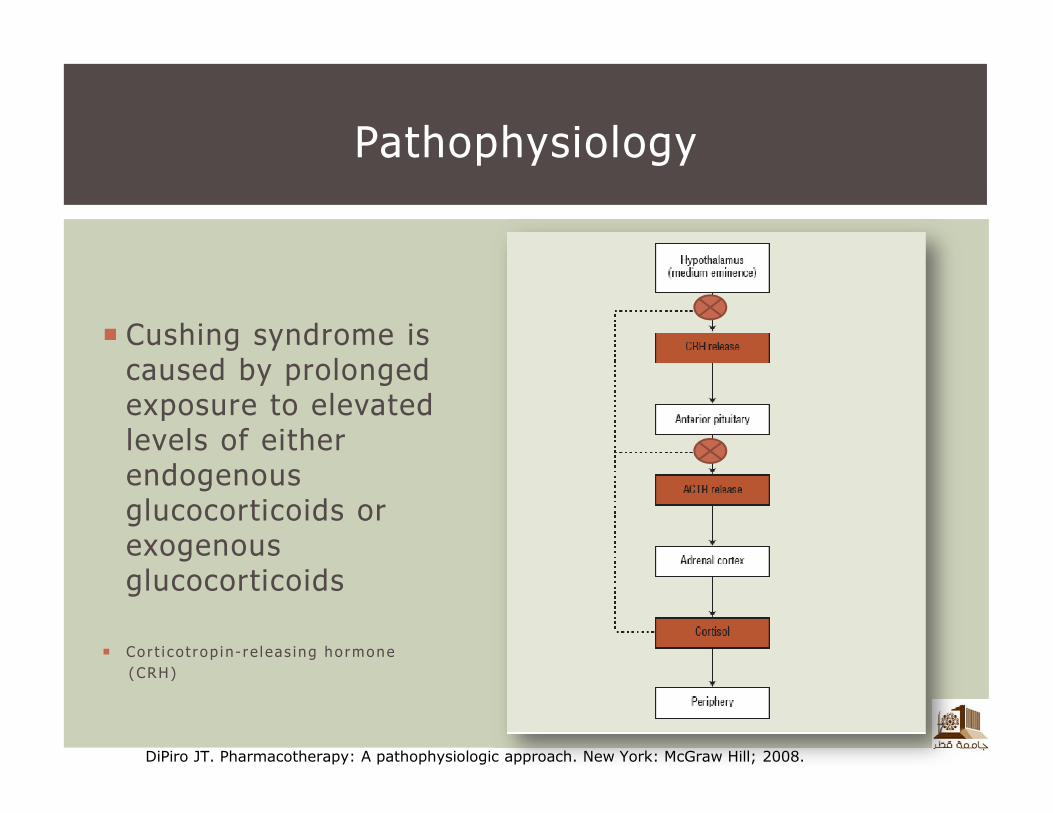
� Cushing syndrome is caused by prolonged exposure to elevated levels of either endogenous glucocorticoids or exogenous glucocorticoids
� Co r t i co t r op i n - r e l eas ing ho rmone
(CRH)
Pathophysiology
7
DiPiro JT. Pharmacotherapy: A pathophysiologic approach. New York: McGraw Hill; 2008.
� Exogenous steroid administration
� Injections of steroids into joints and the use of steroid inhalers
� Patients with diseases that respond to steroid therapy are especially likely to receive steroids and thus develop Cushing syndrome
� Rheumatologic, pulmonary, neurological, and nephrologicdiseases
Causes
8
DiPiro JT. Pharmacotherapy: A pathophysiologic approach. New York: McGraw Hill; 2008.
� Endogenous glucocorticoid overproduction (ACTH-dependent)� causing adrenal hyperplasia
� (≈70% of Cushing’s cases)
� OR abnormal adrenocortical tissues (ACTH-independent)� Adenoma
� Ectopic ACTH syndrome refers to excessive ACTH production resulting from an endocrine or nonendocrine tumor
� Usually of the pancreas, thyroid, or lung
� Small-cell carcinoma of the lung will lead to ectopic ACTH secretion in 0.5% to 2% of cases,
� Whereas bronchial carcinoid tumors are usually the most common
Causes
9
DiPiro JT. Pharmacotherapy: A pathophysiologic approach. New York: McGraw Hill; 2008.
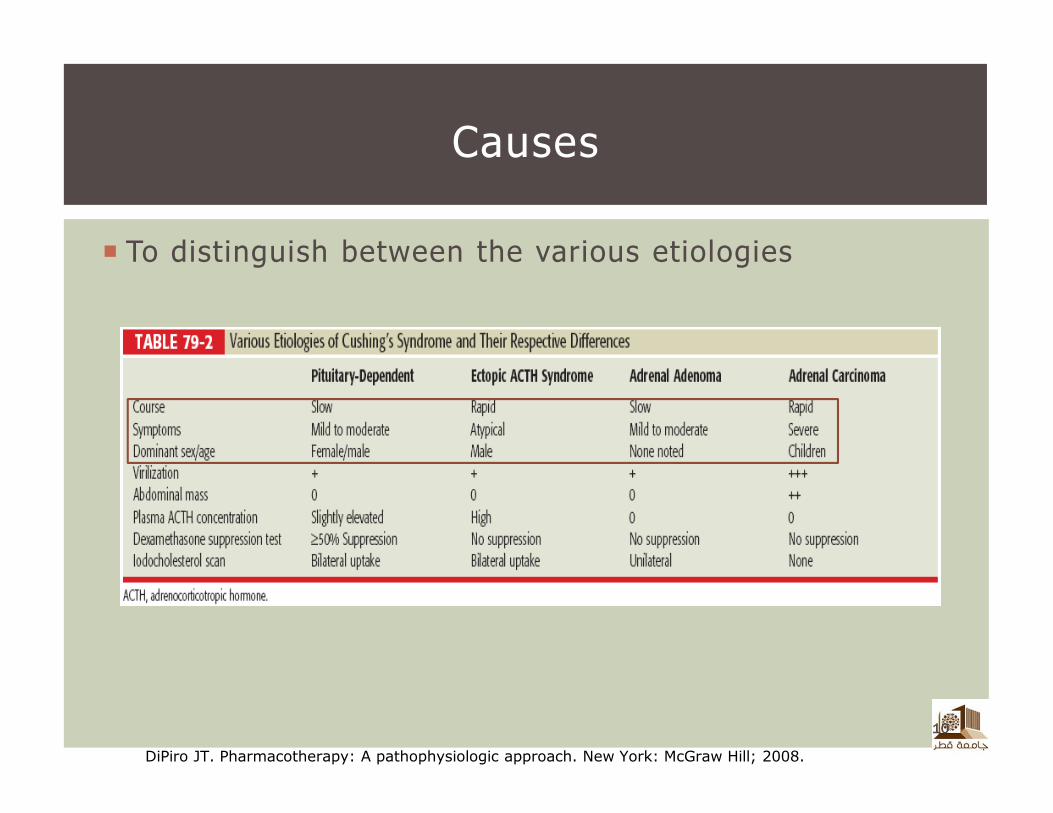
� To distinguish between the various etiologies
Causes
10
DiPiro JT. Pharmacotherapy: A pathophysiologic approach. New York: McGraw Hill; 2008.
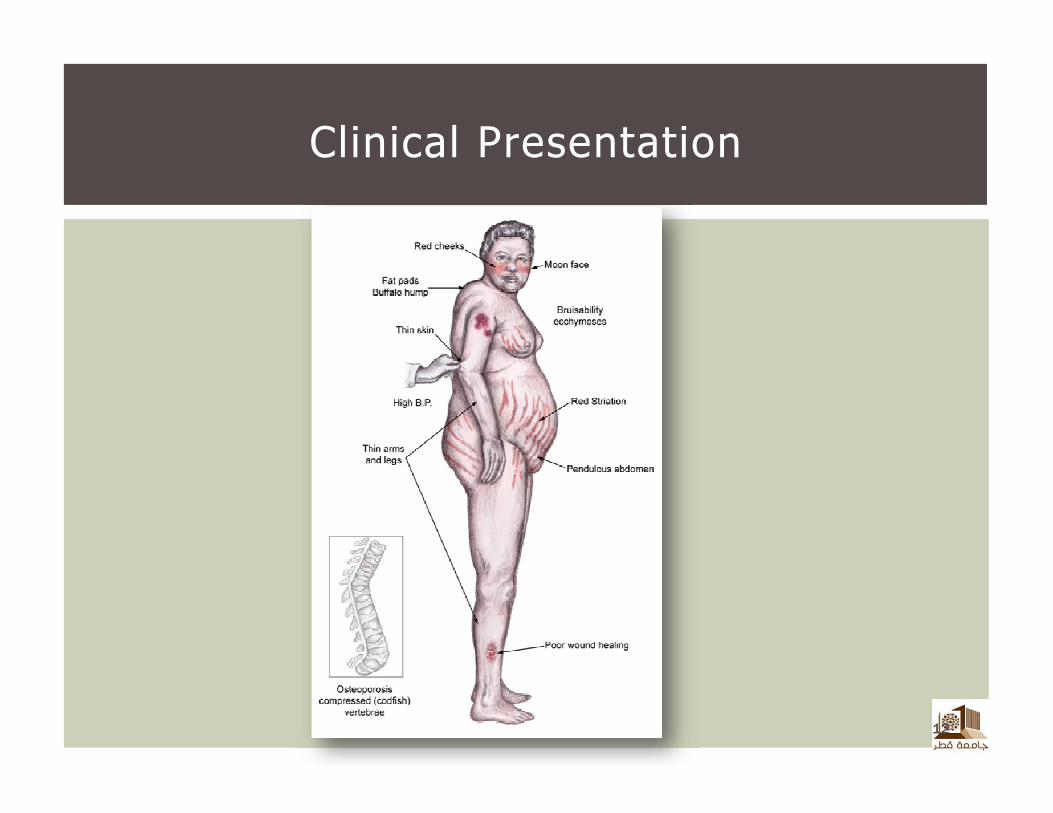
� 90% of patients:
� Central obesity and facial rounding (moon face)
� 50% of patients will exhibit:
� Peripheral obesity and fat accumulation (buffalo hump)
� Striae are usually present along the lower abdomen and take on a red to purple color
� Hypertensive (morbidity and mortality of Cushing’s syndrome 75% to 85% of patients)
� Glucose intolerance is present in 60% of patients
Clinical Presentation
11
DiPiro JT. Pharmacotherapy: A pathophysiologic approach. New York: McGraw Hill; 2008.
12
Clinical Presentation
� Central obesity, hypertension, and glucose intolerance are components of metabolic syndrome and can increase the risk of coronary heart disease (CHD) and stroke threefold
Clinical Presentation
13
DiPiro JT. Pharmacotherapy: A pathophysiologic approach. New York: McGraw Hill; 2008.
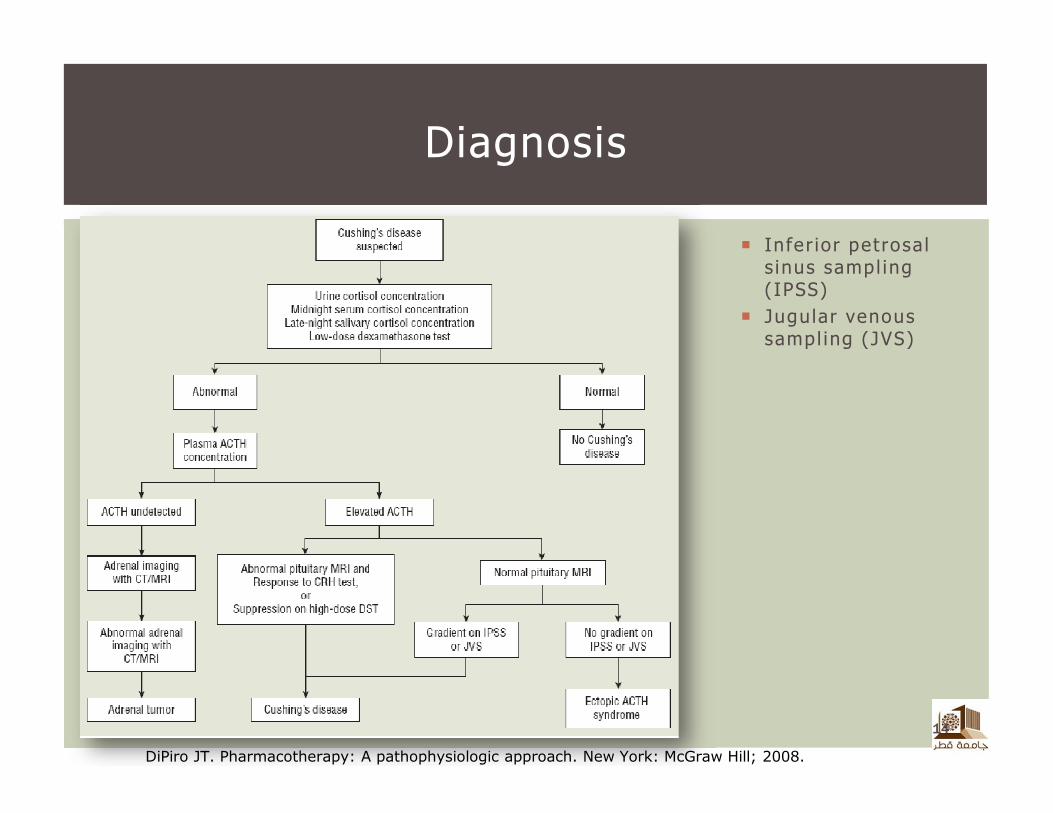
� Infer ior petrosals inus sampl ing (IPSS)
� Jugular venous sampl ing (JVS)
Diagnosis
14
DiPiro JT. Pharmacotherapy: A pathophysiologic approach. New York: McGraw Hill; 2008.
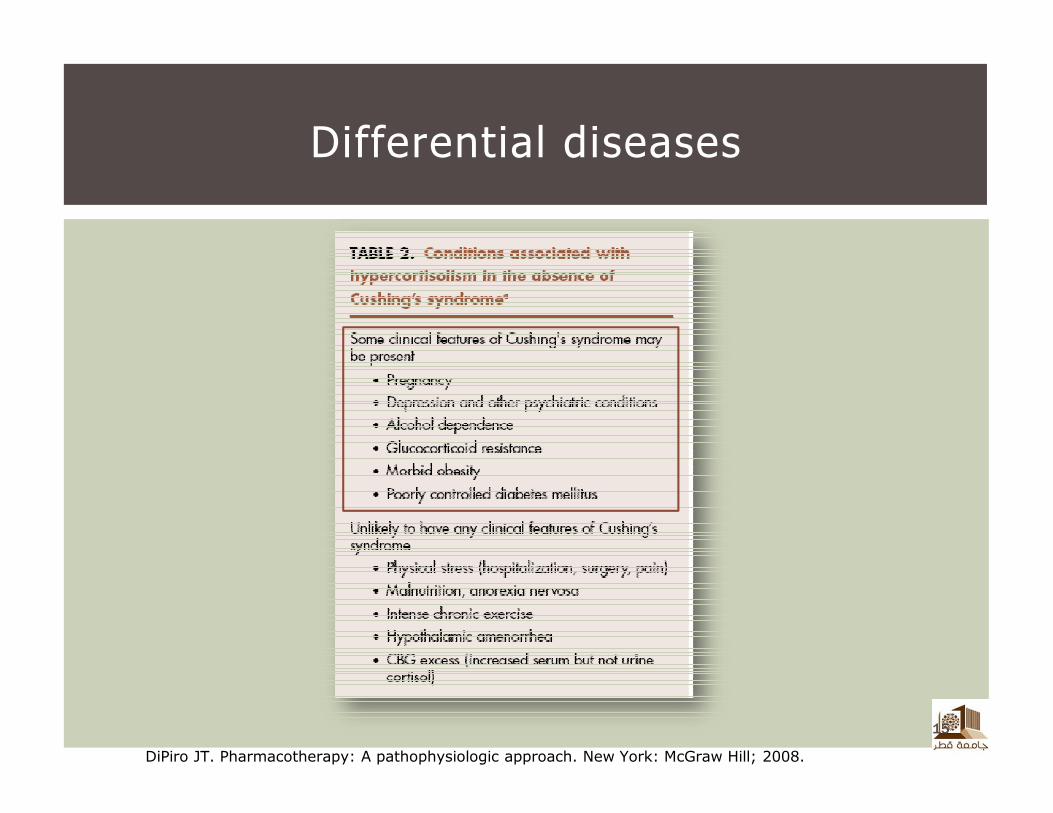
Differential diseases
15
DiPiro JT. Pharmacotherapy: A pathophysiologic approach. New York: McGraw Hill; 2008.
� Bone loss (osteoporosis), which can result in unusual bone fractures, such as rib fractures and fractures of the bones in the feet
� High blood pressure (hypertension)
� Diabetes
� Frequent or unusual infections
� Loss of muscle mass and strength
Complications
www.mayoclinic.com
� Reverse the clinical manifestations by reducing cortisol secretion to normal
� Eradicate any tumor threatening the health of the patient
� Avoid permanent dependence upon medications
� Avoid permanent hormone deficiency
Goals of Therapy
www.uptodate.om
� Surgery
� Transsphenoidal resection of the pituitary microadenoma
� Preservation of pituitary function
� Low complication rate
� High clinical improvement rate
Non-pharmacological Therapy
Dipiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM. Pharmacotherapy: A pathophysiologic approach. 7th edc
� Surgery
� Irradiation of the pituitary has provided clinical improvement
in approximately 50% of patients
� Improvement is usually not seen until 6 to 12 months
� Can create pituitary-dependent hormone deficiencies
� Reserved for patients with persistent hypercortisolemia after transsphenoidal surgery
Non-pharmacological Therapy
Dipiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM. Pharmacotherapy: A pathophysiologic approach. 7th edc
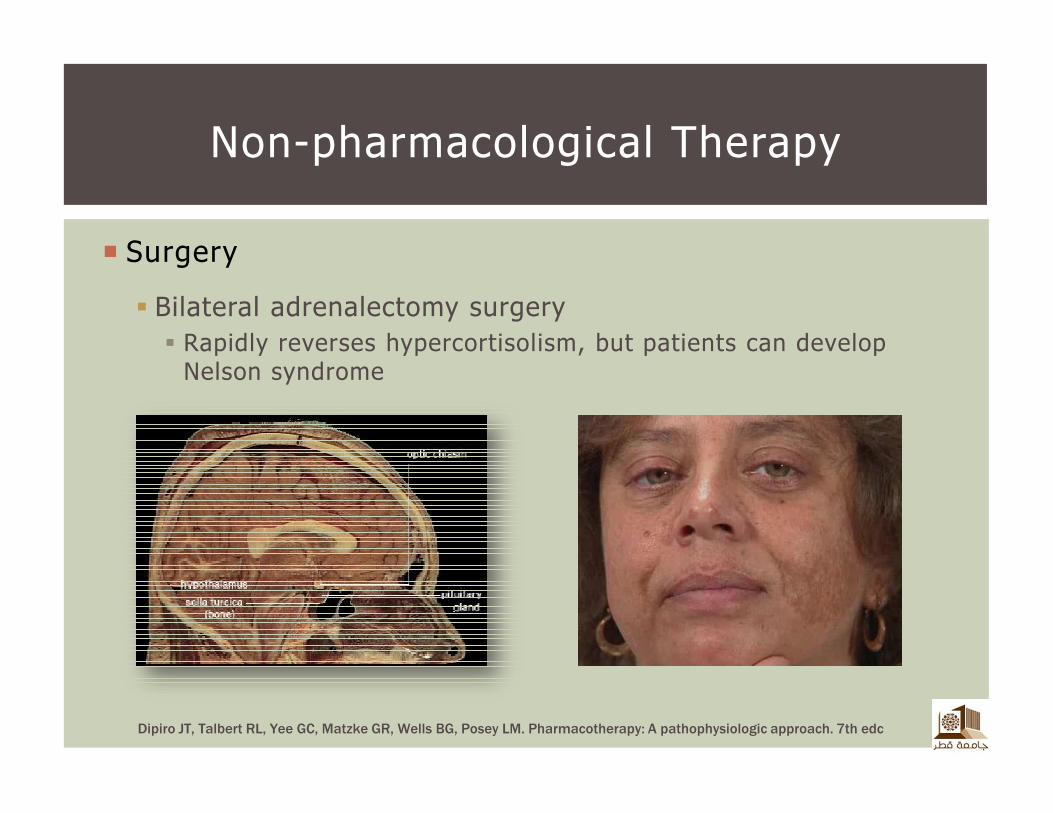
� Surgery
� Bilateral adrenalectomy surgery
� Rapidly reverses hypercortisolism, but patients can develop Nelson syndrome
Non-pharmacological Therapy
Dipiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM. Pharmacotherapy: A pathophysiologic approach. 7th edc

� Surgery
� Adrenal Adenoma
� Surgical resection is associated with relatively few side effects and a high cure rate
� Steroid replacement is needed both perioperatively and postoperatively
� Therapy should be continued for 6 to 12 months following surgery
� Ectopic ACTH syndrome
� Multiple sites of tumors exist
� Locating the ectopic sites are essential but often difficult
� Surgical excision remains optimal in these patients
Non-pharmacological Therapy
Dipiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM. Pharmacotherapy: A pathophysiologic approach. 7th edc
� Surgery
� Adrenal Carcinoma
� Patients have an unpredictable and unfavorable outcome with surgical resection
� Complete tumor cannot be excised, leaving the patient with some degree of symptomatology and extra-adrenal involvement
� Radiotherapy can be used if metastases are discovered
� Palliative pharmacologic intervention(e.g.mitotane) for patients not candidate for a surgery
Non-pharmacological Therapy
Dipiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM. Pharmacotherapy: A pathophysiologic approach. 7th edc
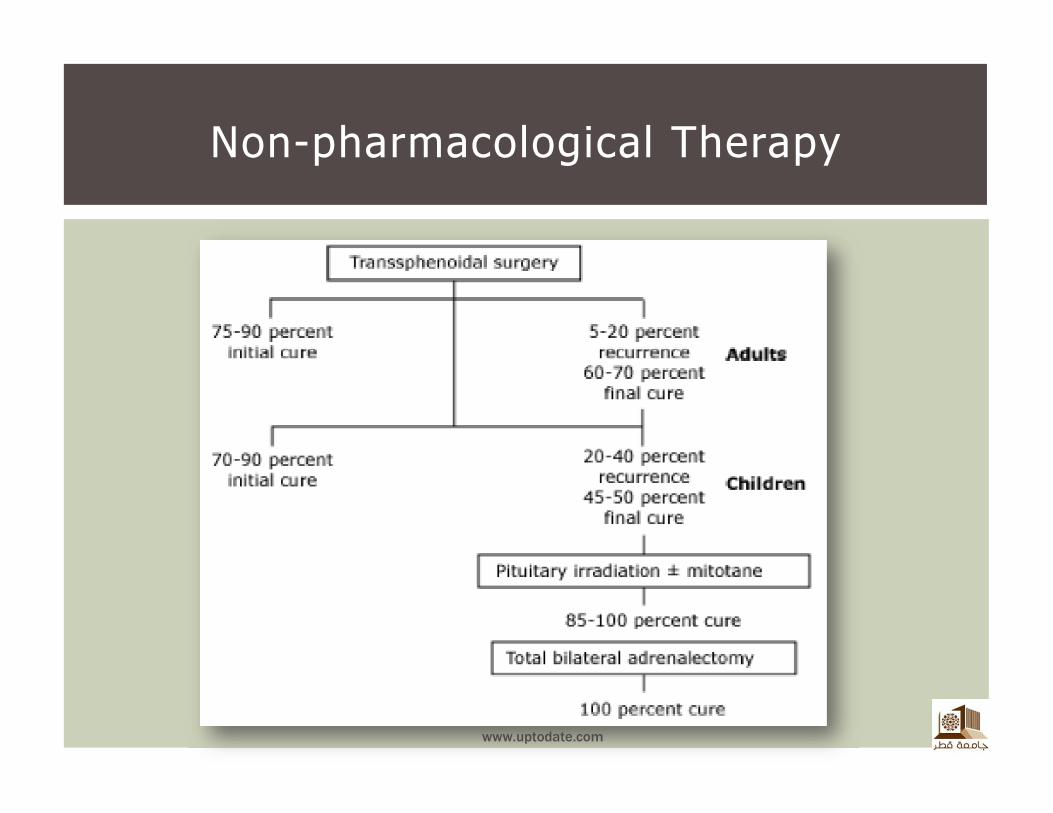
Non-pharmacological Therapy
www.uptodate.com
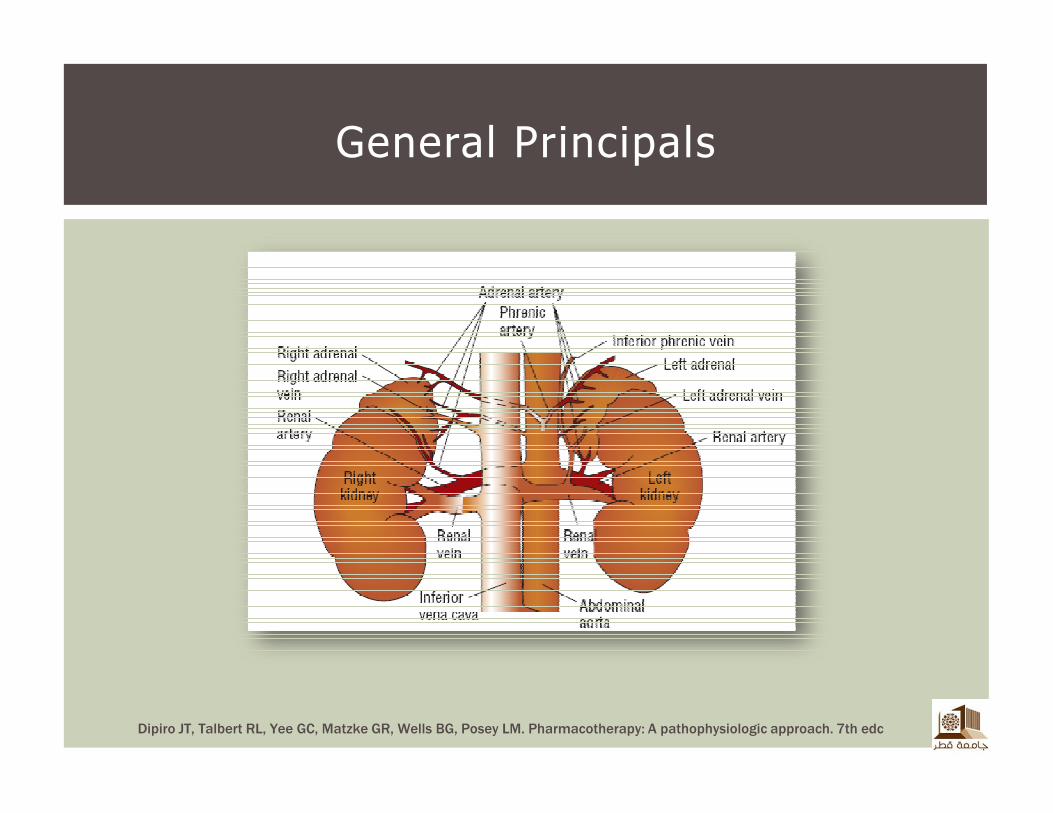
General Principals
Dipiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM. Pharmacotherapy: A pathophysiologic approach. 7th edc
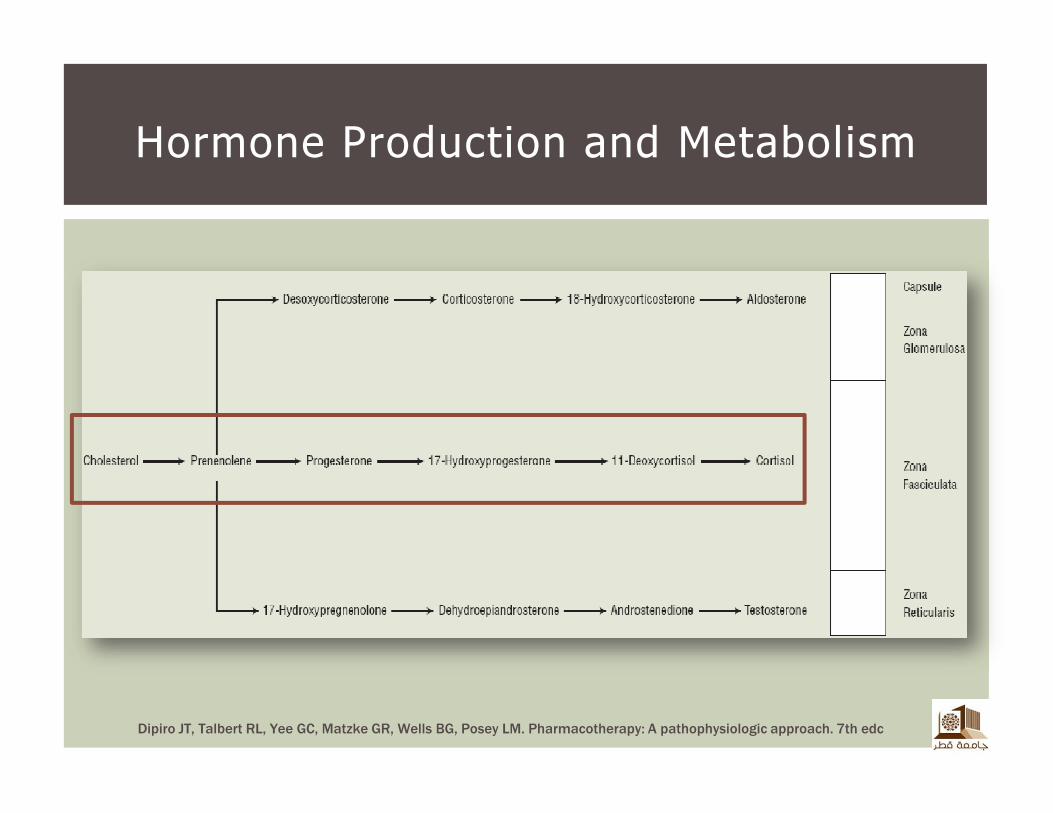
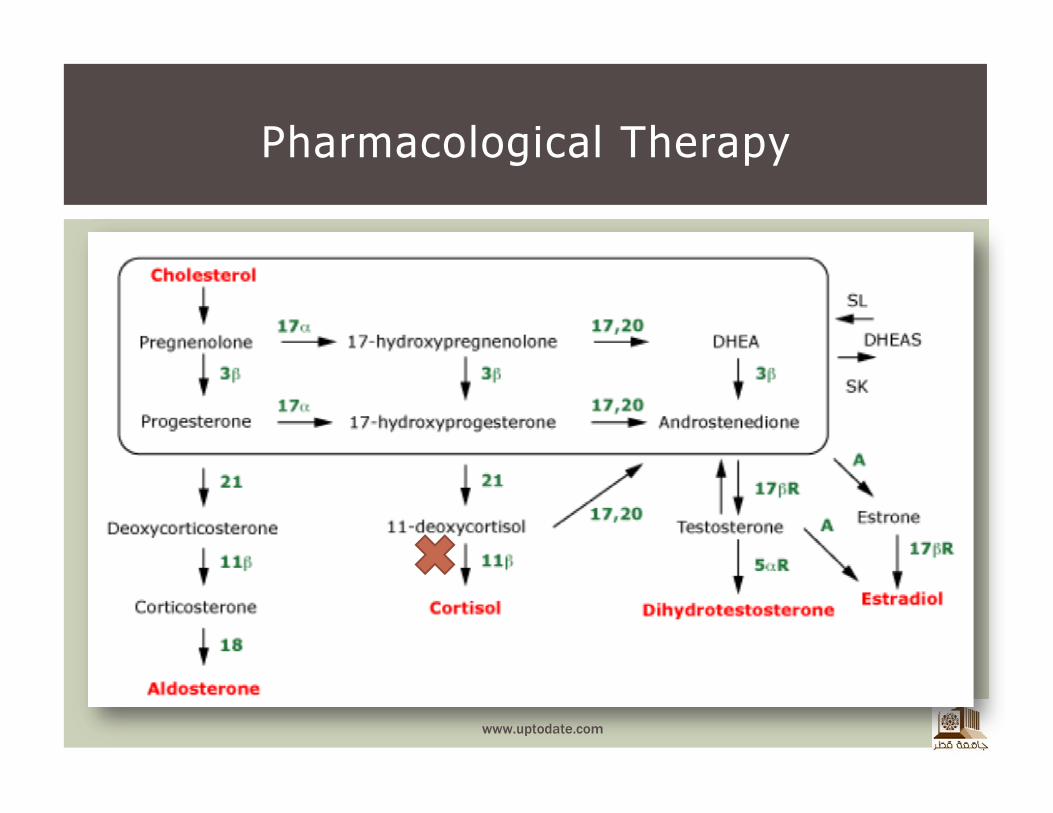
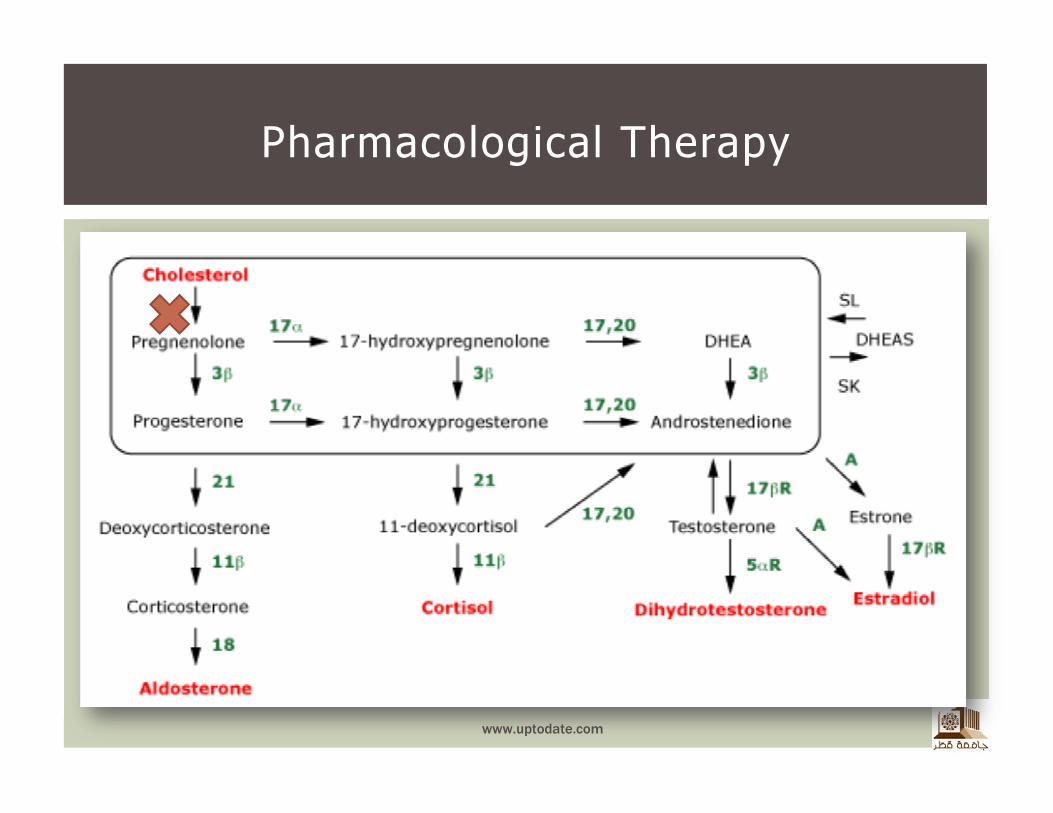
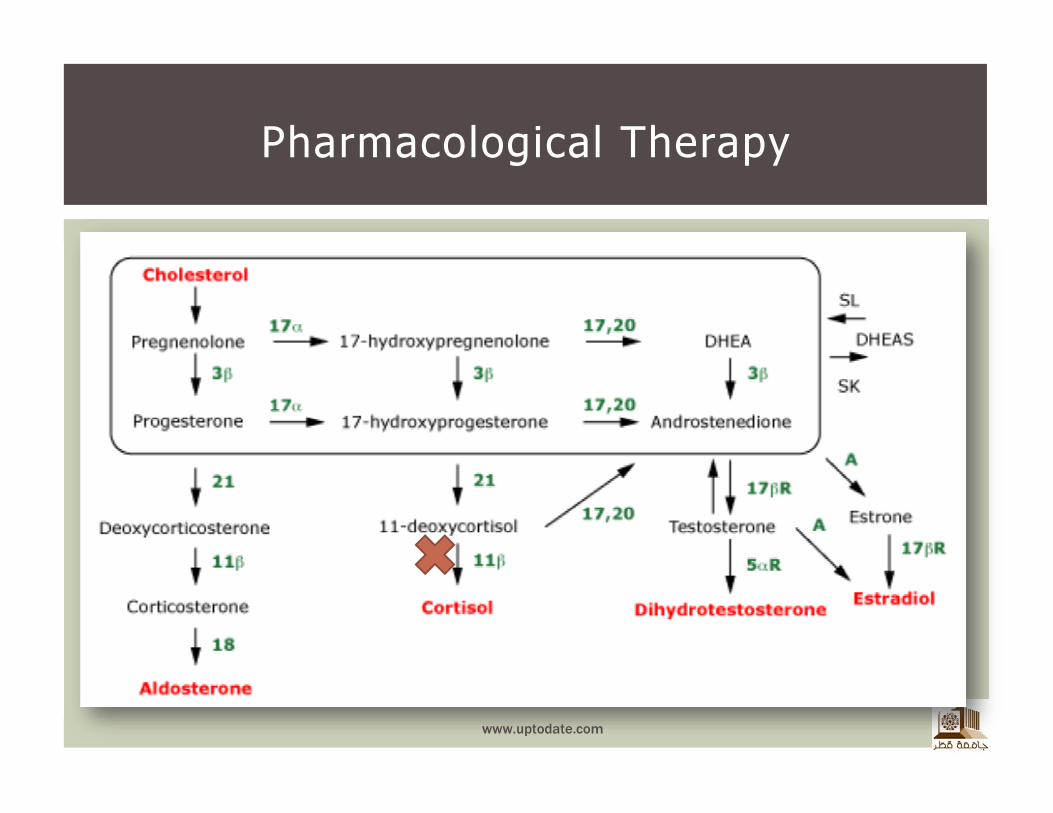
Hormone Production and Metabolism
Dipiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM. Pharmacotherapy: A pathophysiologic approach. 7th edc
� The main indications for medical therapy
� Management of hypercortisolism when surgery is contraindicated
� Control of hypercortisolism in preparation for surgery
� Persistence or recurrence of hypercortisolism after surgery
� Control of hypercortisolism while waiting for the effect of pituitary radiation in patients with ACTH-secreting pituitary tumors
� Treatment of occult ectopic ACTH syndrome
Pharmacological Therapy
www.uptodate.com
� Pharmacotherapy of Cushing’s syndrome can be divided into 4 categories
� Steroidogenic inhibitors
� Adrenolytic agents
� Neuromodulators of ACTH release
� Glucocorticoid receptor blocking agents
Pharmacological Therapy
Dipiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM. Pharmacotherapy: A pathophysiologic approach. 7th edc
� Steroidogenic inhibitors
� Metyrapone
� Aminoglutethimide
� Ketoconazole
� Etomidate
� Fluconazole
� Trilostane
� Should not be used after successful surgery!
� Combinations have additive or synergistic therapeutic effects
Pharmacological Therapy
ACTH dependent
Cushing's syndrome
www.uptodate.com
� Metyrapone
� Inhibits 11-hydroxylase activity
� Initial ACTH concentrations can cause an in androgenic and mineralocorticoid hormones
� Side effects include nausea, vomiting, vertigo, headache, dizziness, abdominal discomfort, and allergic rash
Pharmacological Therapy
Dipiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM. Pharmacotherapy: A pathophysiologic approach. 7th edc
Pharmacological Therapy
www.uptodate.com
� Aminoglutethimide
� Blocks the conversion of cholesterol to pregnenolone
� Alone is indicated for short-term use in inoperable Cushing’s disease with ectopic ACTH syndrome
� Has limited efficacy as a single agent, with relapse occurring after discontinuation of therapy
� Side effects include severe sedation, nausea, ataxia, and skin rashes
Pharmacological Therapy
Dipiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM. Pharmacotherapy: A pathophysiologic approach. 7th edc
Pharmacological Therapy
www.uptodate.com
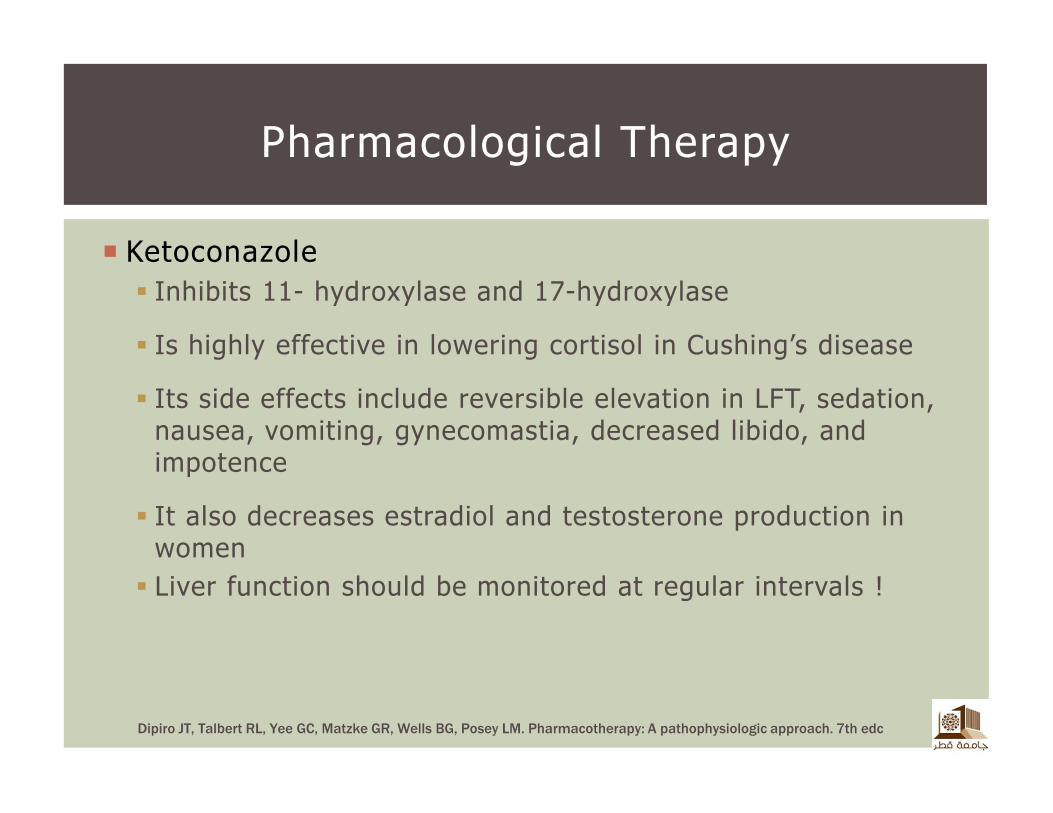
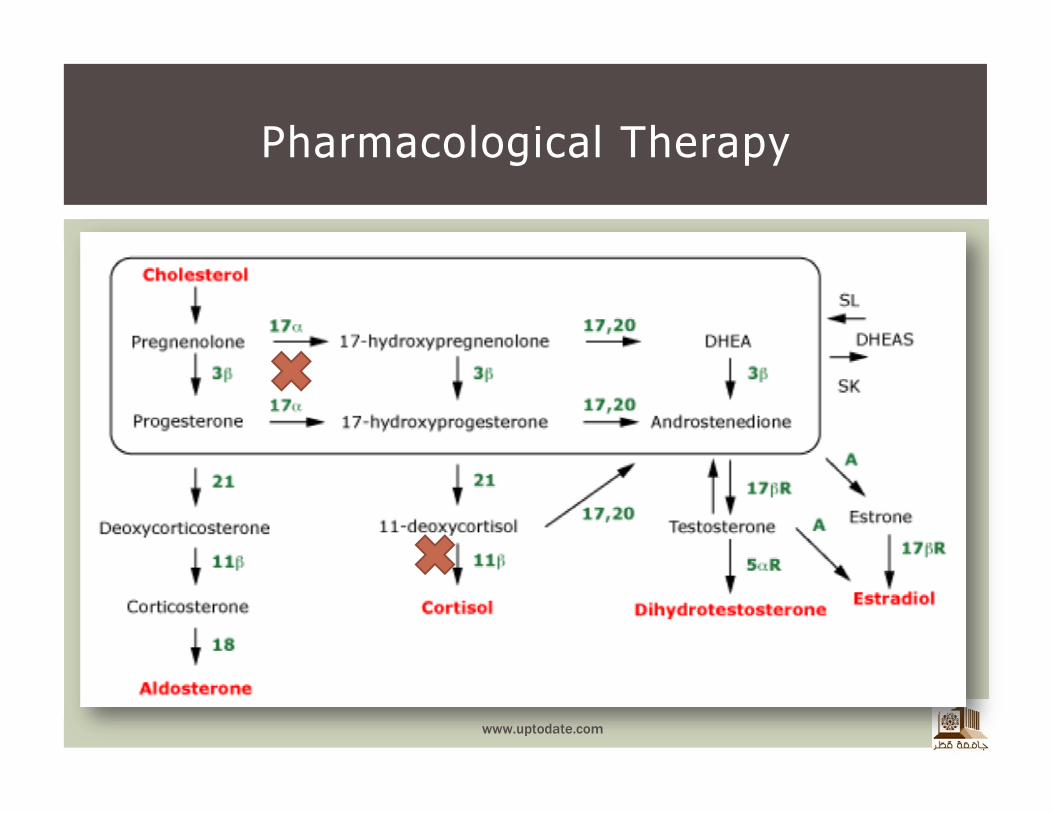
� Ketoconazole
� Inhibits 11- hydroxylase and 17-hydroxylase
� Is highly effective in lowering cortisol in Cushing’s disease
� Its side effects include reversible elevation in LFT, sedation, nausea, vomiting, gynecomastia, decreased libido, and impotence
� It also decreases estradiol and testosterone production in women
� Liver function should be monitored at regular intervals !
Pharmacological Therapy
Dipiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM. Pharmacotherapy: A pathophysiologic approach. 7th edc
Pharmacological Therapy
www.uptodate.com
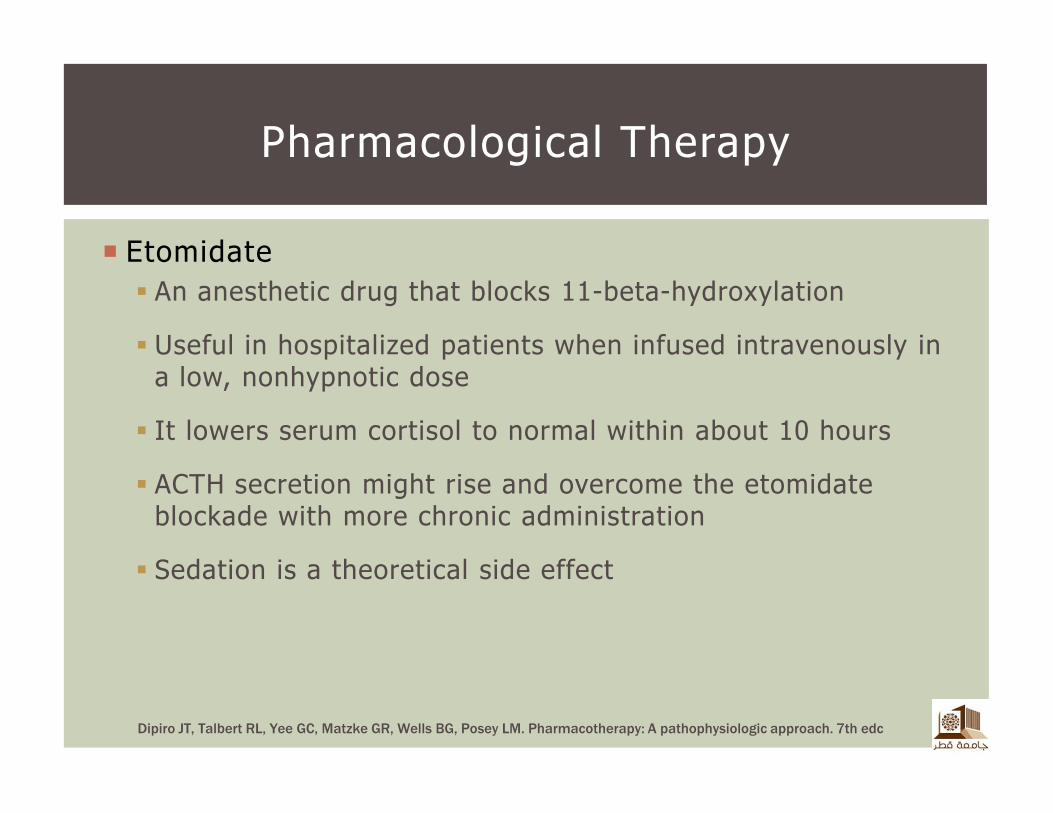
� Etomidate
� An anesthetic drug that blocks 11-beta-hydroxylation
� Useful in hospitalized patients when infused intravenously in a low, nonhypnotic dose
� It lowers serum cortisol to normal within about 10 hours
� ACTH secretion might rise and overcome the etomidateblockade with more chronic administration
� Sedation is a theoretical side effect
Pharmacological Therapy
Dipiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM. Pharmacotherapy: A pathophysiologic approach. 7th edc
Pharmacological Therapy
www.uptodate.com
� Adrenolytic agents
�Mitotane
Pharmacological Therapy
Dipiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM. Pharmacotherapy: A pathophysiologic approach. 7th edc
�Mitotane
� Used primarily for the treatment of adrenal carcinoma
� It can also be used to achieve medical adrenalectomy or as an adjunctive medication in patients with ectopic ACTH secretion
� The usual duration of adjunctive mitotane is 6 to 9months
� It is taken up by fatty tissues and persists in plasma long after the drug is discontinued
� The major side effects are nausea, vomiting, and anorexia
Pharmacological Therapy
Dipiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM. Pharmacotherapy: A pathophysiologic approach. 7th edc
� Neuromodulators of ACTH release
� Cyproheptadine
� Ritanserin
� Bromocriptine
� Cabergoline
� Valproic acid
� Octreotide
� Lanreotide
� Rosiglitazone
� Tretinoin
Pharmacological Therapy
No Consistent clinical
efficacy !
Dipiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM. Pharmacotherapy: A pathophysiologic approach. 7th edc
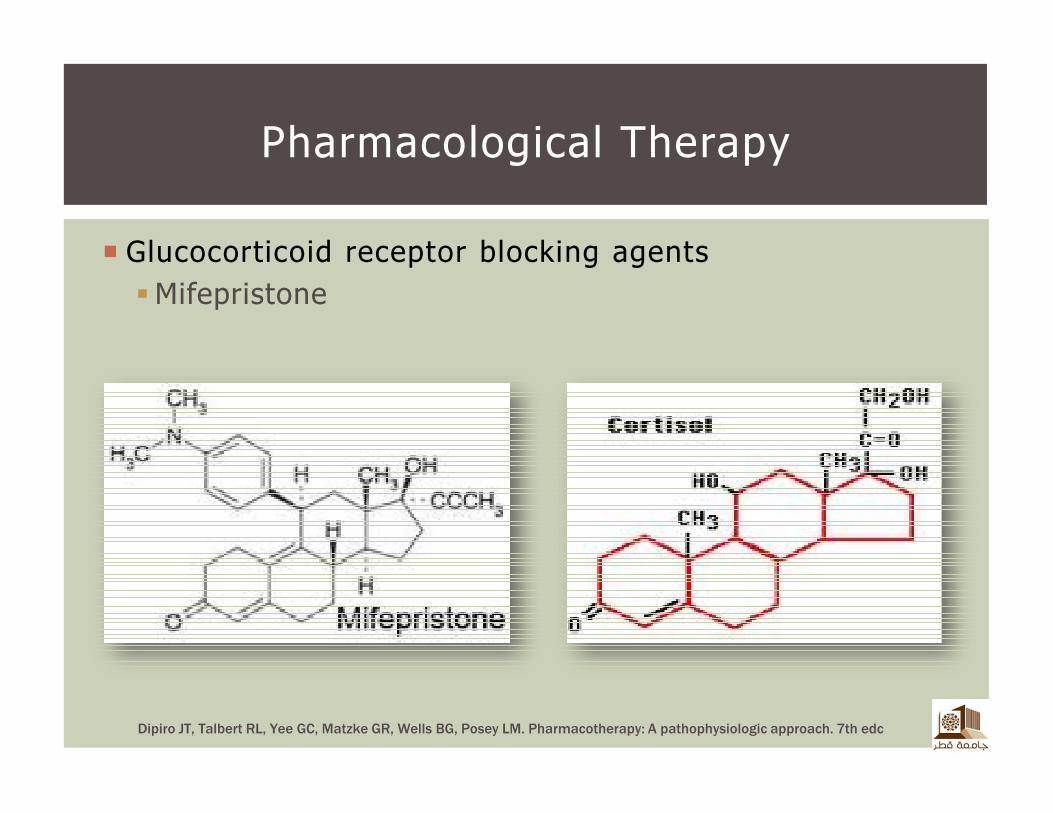
� Glucocorticoid receptor blocking agents
�Mifepristone
Pharmacological Therapy
Dipiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM. Pharmacotherapy: A pathophysiologic approach. 7th edc
� Mifepristone
� Is an anti-progestational drug
� Competes with glucocorticoids for binding to their receptor, thereby blocking their action
� It appears to be effective, although cortisol secretion increased in some
� It blocks the action of exogenous glucocorticoid
Pharmacological Therapy
Dipiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM. Pharmacotherapy: A pathophysiologic approach. 7th edc
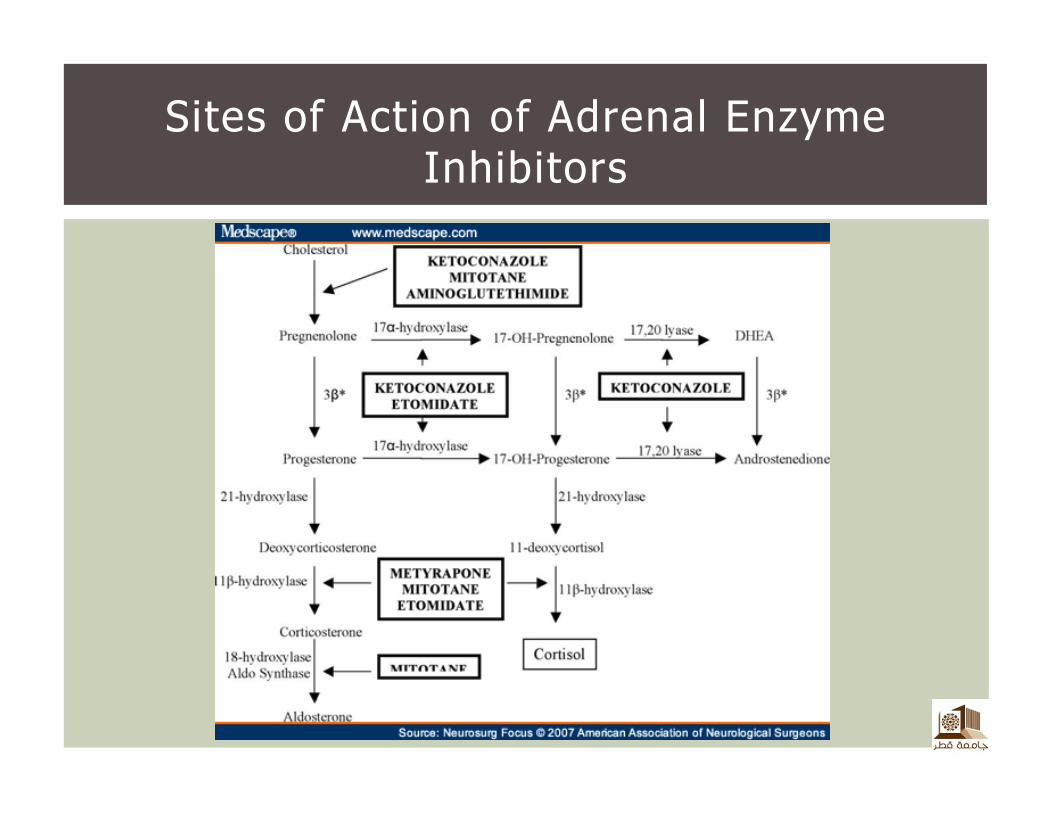
Sites of Action of Adrenal Enzyme Inhibitors
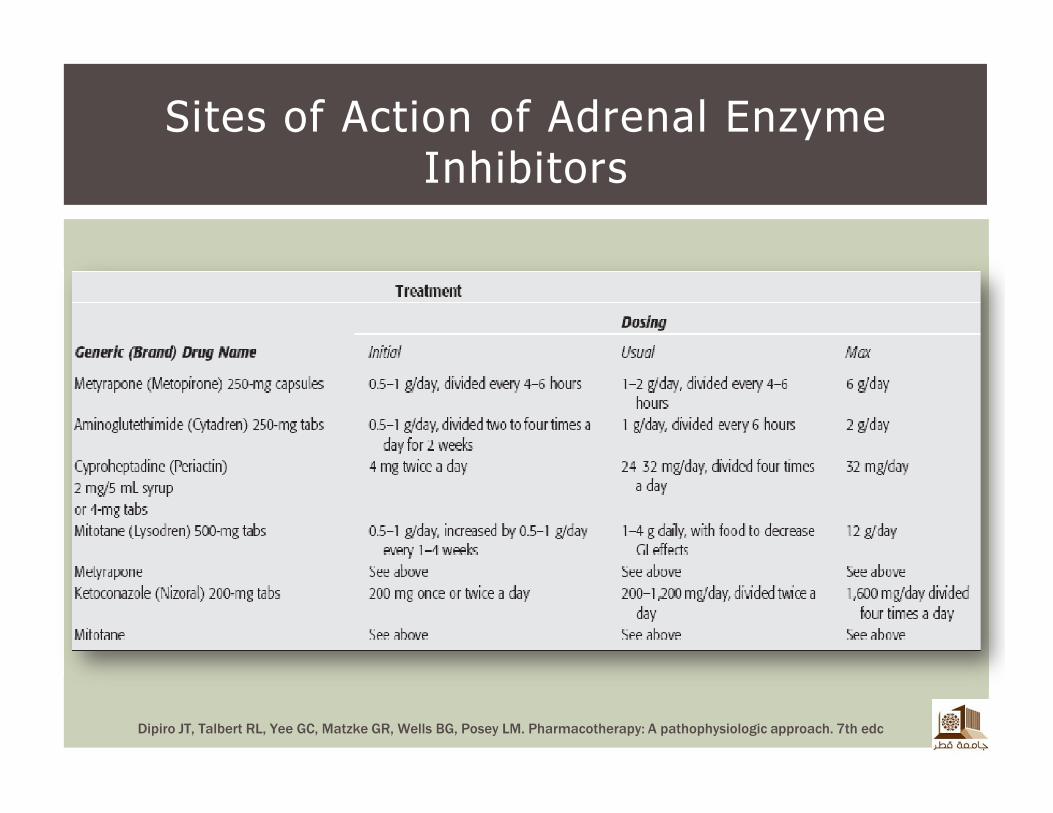
Sites of Action of Adrenal Enzyme Inhibitors
Dipiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM. Pharmacotherapy: A pathophysiologic approach. 7th edc
� Suggested approach
� Block and replace
� Normalization strategy
� Hydrocortisone
� Prednisone
� Dexamethasone
Pharmacological Therapy
www.uptodate.com
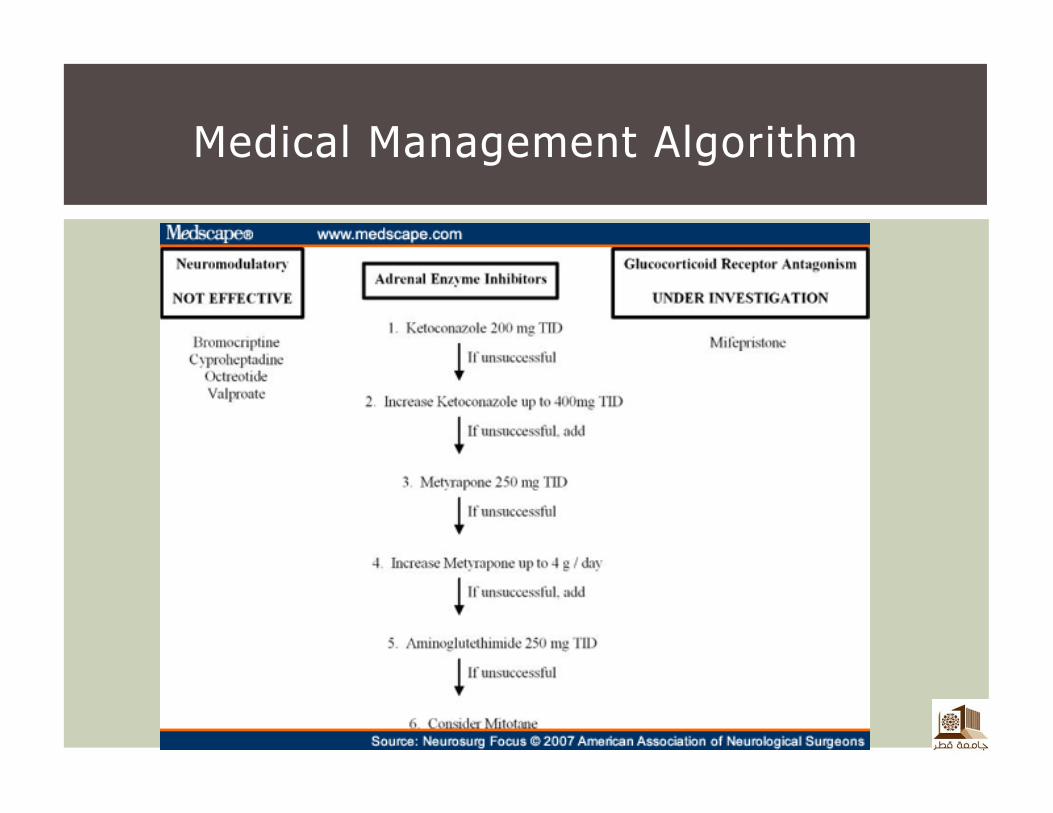
Medical Management Algorithm
� Untreated Cushing's syndrome is often fatal
� Most deaths being due to
� Cardiovascular, thromboembolic, or hypertensive complications or bacterial or fungal infections
� Cushing's disease is virtually always curable
� No patient with Cushing's syndrome of any cause should die from persistent hypercortisolism
Prognosis
www.uptodate.com
47