Embed Size (px)
Citation preview

Depressed Mood and Other PsychiatricManifestations of Cushing's Syndrome:Relationship to Hormone Levels
MONICA N. STARKMAN, MD, DAVID E. SCHTEINGART, MD, ANDM. ANTHONY SCHORK, PHD
Thirty-five consecutive patients with Cushing's syndrome were studied prospectively prior totreatment. A consistent constellation of psychiatric disturbances was found, including impair-ments in affect (depressed mood and crying), cognitive functions (decreased concentration andmemory), and vegetative functions (decreased libido and insomnia). A statistically significantrelationship was found between the overall psychiatric disability rating and cortisol and ACTHlevel. The relationship of depressed mood and hormone levels was examined. Low ACTH levelswere significantly associated with milder rather than pronounced depressed mood. Theimplications of the similarities in psychiatric manifestations between Cushing's syndrome andthe primary affective disorders are discussed.
INTRODUCTION
The relationship of endocrine andmetabolic factors to mental symptomatol-ogy has long been of interest to behavioralscientists and clinicians. Psychiatricdisturbances of psychotic dimensionsassociated with the exogenous admini-tration of steroid hormones have beenparticularly well recognized (1, 2). Hyper-cortisolism also occurs spontaneously; in-dividual case reports as well as reviewsconfirm that emotional disturbances are
From the Department of Psychiatry and the De-partment of Internal Medicine (Division of Endocri-nology and Metabolism and the Metabolism Re-search Unit), School of Medicine and the Depart-ment of Biostatistics, School of Public Health, Uni-versity of Michigan, Ann Arbor, Michigan.
Address requests for reprints to: Dr. Monica N.Starkman. Director, Consultation-Liaison Program,Department of Psychiatry, University of MichiganMedical Center, Ann Arbor, MI 48109.
Received for publication March 17, 1980; finalrevision received September 24, 1980.
frequent features of its clinical presenta-tion (3). However, prospective studies de-scribing the specific neuropsychiatric ab-normalities in patients with Cushing'ssyndrome, their frequency, and their rela-tionship to the abnormal hormone levelspresent in this disease are lacking.
Patients with spontaneous Cushing'ssyndrome provide a unique opportunityto study the relationship between cortisoland adrenocorticotrophin (ACTH) andpsychiatric symptomatology. Since thedisease may originate in several ways,patients present with differing profilesof cortisol and ACTH. In the majority ofcases, there is excessive secretion ofACTH, usually by the pituitary gland,occasionally by a paraendocrine tumor,which causes excessive cortisol secretionby the adrenal glands. In other cases, anadrenal tumor secretes excessive cortisol,which then suppresses ACTH secretion.
This report describes the relationship ofcortisol and ACTH levels with psychiatricsymptomatology in 35 consecutive pa-
Psychosomatic Medicine Vol. 43, No. 1 (February 1981)
Copyright © 1981 by the American PsychoPublished by Elsevier North Holland, Inc.52 Vanderbill Ave , New York, NY 10017
003 3-3174/81101000316$02.50

MONICA N. STARKMAN et al.
tients with spontaneous Cushing's syn-drome studied prospectively prior totreatment. Psychiatric features are de-scribed, with particular attention to theclinical characteristics of depressedmood, which occurs with high frequencyin this disorder. The data to be presentedindicate that there is an association be-tween overall psychiatric disability andthe level of cortisol and ACTH present inthese patients. Furthermore, the datasuggest that there may be an association ofdepressed mood and ACTH levels.
MATERIALS AND METHODS
Subjects
As the beginning phase of a longitudinal study.35 patients with active Cushing's syndrome werestudied prior to initiation of treatment. Twenty-eightwere white and seven were black. Seven were maleand 28 were female, approximating the expected 1:3ratio of males to females seen in this syndrome. Themean age was 35, with a range of 19 to 59 years. Thediagnosis of Cushing's syndrome was established inthese patients by the demonstration of excessivecortisol secretion, as measured by cortisol secretionrates, urinary free cortisol, and plasma cortisol. Inaddition, cortisol levels lacked the normal circadianrhythm and failed to suppress normally with 2 mg ofdexamethasone.
The etiologic type of Cushing's syndrome wasdetermined for each patient on the basis of baselinecortisol and ACTH levels and ACTH response todexamethasone suppression and metyrapone stimu-lation. Twenty-eight patients had ACTH-dependentCushing's syndrome, with high cortisol and highACTH levels. Of these, 22 had pituitary hyperfunc-tion without a detectable pituitary tumor. Four otherpatients had pituitary macroadenomas. One patienthad an ectopic ACTH-producing thymoma. Anotherpatient had ACTH-dependent Cushing's syndromewith unusual hormone patterns that still refuse toyield to classification. Seven patients had ACTH-independent Cushing's syndrome, with high cortisoland low ACTH levels. Of these, five patients had an
adrenal adenoma and two patients had an adrenalcarcinoma.
Psychiatric Evaluation
Patients were evaluated psychiatrically duringtheir initial diagnostic hospitalization at the timethat baseline hormone levels were being obtained.Because of the characteristic physical stigmata ofCushing's syndrome, it was not possible for theevaluator (MNS) to be unaware of the patient'sdiagnosis. However, at the time of the assessment,the evaluator had no knowledge of the etiologic typeof Cushing's syndrome or the hormone levels of thepatient.
A semistructured interview technique was de-signed in order to obtain as comprehensive aphenomenologic description of the psychiatricsymptoms as possible. Attention was given to defin-ing the quality and characteristics of these symptomsin addition to simply scoring their absence, pres-ence, and quantitative degree. After a spontaneousrecounting of symptoms was elicited, a standardizedset of questions was asked. Particular attention wasgiven to affective, vegetative, and cognitive distur-bances. Items selected for study were derived frompreviously reported observations of psychiatricsymptoms in Cushing's syndrome, as well as theauthors' pilot study of patients with this disease. Asemiquantitative rating scale was established inorder to allow both for comparisons among patientsand for comparison of individual patients withthemselves at future stages of treatment. For thisnewly constructed assessment technique, a disad-vantage is that neither reliability nor validity has yetbeen established. Otherwise useful standard ratingscales were not suitable for use with these patients.The Hamilton Psychiatric Rating Scale for depres-sion includes items that are characteristic of thephysiologic manifestations of Cushing's syndrome(e.g., muscle weakness, urinary frequency) or the notunrealistic preoccupation with body functioning (4).The Research Diagnostic Criteria are prohibited foruse with such patients because of the existence of aspecific organic disease causing both physical andmental symptoms (5). Many items from these scales,however, were incorporated into the structured por-tion of the interview. A mental status examinationwas also performed.
Forty-five items (see Tables 1 and 2) were studiedby symptom report and/or observation during men-tal status examination. Each item was scored on afour-point scale (absent, mild, moderate, severe)based on quality, intensity, and frequency. Further,
Psychosomatic Medicine Vol. 43, No. 1 (February 1981)

PSYCHIATRIC MANIFESTATIONS OF CUSHING'S SYNDROME
TABLE 1. Frequency of Psychiatric Symptoms in35 Patients With Cushing's Syndrome
Symptom %
Increased fatigue 100Decreased energy 97Irritability 86Impaired memory 83Depressed mood 74Decreased libido 69Middle insomnia 69Anxiety 66Impaired concentration 66Crying 63Restlessness 60Late insomnia 57Social withdrawal 46Hopelessness 43Guilt 37Increased appetite 34Dreams 31Early insomnia 29Decreased appetite 20Thought blocking 17Speeding thoughts 14Elation-hyperactivity 11Slowing thoughts 11Perceptual distortions 11Rapid, loud speech 9Paranoid thoughts 9Hyperactivity 9Depersonalization 3Persistent anhedonia 3Derealization 3Decreased fatigue 3Increased energy 3
an overall score of psychiatric disability was gener-ated based on two factors: the summation of the rawscores for each of the 45 items in the symptomreview and the mental status examination and theclinical global judgment of the seriousness of thepsychiatric symptoms and degrees of psychiatricimpairment. This overall score ranged from 1 to 4(mild, moderate, severe, very severe). Individualsrated as having severe psychiatric impairment man-ifested more marked and disabling affective andvegetative symptoms than those rated as having mildor moderate psychiatric impairment. Those patientsrated as having a very severe psychiatric impairmentmanifested in addition a thought disorder withparanoid ideation and /or confusional states.
Hormone Analysis
Cortisol secretion rate—the amount of cortisolsecreted over a 24-hour period—was measured byisotope dilution (6). Total plasma cortisol (whichincludes both protein-bound and biologically activefree cortisol), 24-hour urinary free cortisol, andplasma ACTH were measured by radioimmunoassay(7, 8). Serum dehydroepiandrosterone sulfate(DHEA-S), a mild androgen frequently abnormal inCushing's syndrome but not anticipated to havemajor psychiatric effects, was also examined forcomparison. DHEA-S was also measured byradioimmunoassay (9). Plasma or serum samples forcortisol, DHEA-S, and ACTH were obtained severaltimes during the day for assessment of circadianrhythm. Where multiple plasma or serum sampleswere obtained, values were found to vary littleduring the day, a characteristic of Cushing's syn-drome. Since the 8 AM samples were obtained mostconsistently, these values were used for statisticalanalysis.
Although efforts were made to obtain the entirebattery of baseline hormone levels for each patient,in several instances one particular hormone level isnot available because of technical difficulties.
RESULTS
Frequency of PsychiatricSymptoms
Table 1 lists the frequency of psychiat-ric symptoms reported by the 35 patients.A consistent constellation of symptomswas found at a high frequency (above50%). These symptoms include impair-ments in affect (depressed mood, crying],cognitive functions (decreased concentra-tion and memory), and vegetative func-tions (decreased libido and insomnia).
Description
IrritabiJity-Anger. Increased irritabil-ity, a very frequent symptom, was theearliest psychiatric symptom to appear inthe majority of cases. It began concomi-
Psychosomatic Medicine Vol. 43, No. 1 (February 1981)

MONICA N. STARKMAN et al.
TABLE 2. Frequency of Abnormal Findings in theMental Status Examination in 35 Patients withCushing's Syndrome
Abnormal Findings
AnxietySerial 7 subtractionProverb interpretationRecall of presidentsRecall of 3 cities after 15 minutesSadnessAffective labilityPerseverationFlight of ideasThought blockingParanoid trendsConfusionExpansive, euphoric affect
%
63514646312617
966633
tant with the onset of weight gain andprior to the appearance of other physicalmanifestations of Cushing's syndrome.Patients described themselves as havingbecome overly sensitive, unable to ignoreminor irritations, feeling impatient withor pressured by others. Since some pa-tients reported that external noisesbothered them excessively, this may be areflection of a generalized hypersensitiv-ity to stimuli. In addition, an overreactiv-ity and easy development of anger wasreported. Patients described feeling thatthey were often on the verge of an emo-tional explosion and that the intensity ofanger experienced was also increased.
Verbal dyscontrol was frequent; pa-tients noted that they were overly ar-gumentative and unable to "hold theirtongue." They also felt like expressingtheir irritation and frustration rhotori-cally, such as by smashing objects. Al-though most could restrain themselves, afew patients reported actual motor out-bursts. Patients were frightened by theirirritability and potential for verbal or phy-
sical dyscontrol. They described being onguard for a flare-up of anger and fleeingfrom a confrontation to avoid a feared lossof control.
Mood Disturbances: Depressed Mood.Depressed mood was reported by three-quarters of the patients. Many describedthat they would wake up depressed andremain depressed throughout the day orthe next day as well. Alternatively, theonset of depressed mood and/or cryingmight occur during the day. Patientsstressed that the onset of depression wassudden, at times with a rapid shift at somepoint during the day.
Some patients described hypersensitiv-ity and oversentimentality as determi-nants leading to crying spells. For somepatients, crying was experienced as theironly available behavioral response toanger, frustration, and feelings of inabilityto respond effectively. Patients also de-scribed the spontaneous onset of de-pressed mood or crying in the absence ofany preceding upsetting thought or event.There was a range in the intensity ofdepressed mood. Some patients describedshort spells of sadness; others experi-enced feelings of hopelessness and givingup. Six patients had had suicidalthoughts. Two of these patients had madesuicide attempts since the onset of theCushing's syndrome.
Social withdrawal, when present, wasrelated to feelings of discomfort in largegroups. Patients experienced shame be-cause of their physical appearance anddid not wish to be seen in public. More-over, the unstructured setting of a largegroup elicited a decreased sense of focus,alertness, and clarity that led to a general-ized sense of uneasiness. Most patients
Psychosomatic Medicine Vol. 43, No. 1 (February 1981)

PSYCHIATRIC MANIFESTATIONS OF CUSHINC'S SYNDROME
reported an increased desire to have con-tact with significant family members.However, as noted previously, sporadicwithdrawal might occur because of thepatient's need to remove him/herself froma situation of overstimulation that elicitedthe fear of impending emotional dyscon-trol. Guilt, when present, was not exces-sive, self-accusatory, or irrational. It wasrelated primarily to remorse about thefrequent and uncontrollable angry out-bursts and inability to function as well aspreviously at work and in the family.Hopelessness, when present, was attrib-uted to the existence of a chronic illnesswith increasing physical and emotionaldisability that so far had proved undiag-nosable and untreatable.
The time course of the mood distur-bances, was noteworthy. Patients reportedthat their mood disturbances were inter-mittent rather than sustained. Althoughthere were intervals when they felt un-pleasure, these patients did not describepersistent anhedonia. They did not ex-perience the unrelenting, unremitting in-ability to experience pleasure that ischaracteristic of patients with endogen-ous major depressive illness. There wereintervals when they retained the capacityfor pleasure and found enjoyment in hob-bies, activities, and interpersonal rela-tionships. At times, some patients found itdifficult to initiate such activities; onceothers mobilized them, they would enjoythem.
The duration of each depressiveepisode was usually 1 to 2 days and rarelylonger than 3 days at a time. A frequentweekly total of dysphoria was reported asbeing 3 days per week. There was noregular cyclicity, however, so that pa-tients could not predict when a depressiveday would occur.
Mood Disturbances: Blation-Hyper-activity. A minority of patients had ex-perienced episodes of elation-hyperactivi-ty early in the course of the disease. As thedisease progressed and new physicalsigns of Cushing's syndrome began toappear, this type of episode became rareor disappeared entirely. The quality ofthese episodes of elation was describedmost frequently as a "high." Patients weremore ambitious than usual and might at-tempt to do more than their ability andtraining made reasonable. Increasedmotor activity was present, with restless-ness and rapidly performed activities.Three patients reported finding, to theirembarrassment, that their speech wasboth loud and rapid. In one of the mostseverely disturbed patients, who had anectopic ACTH-secreting thymoma, a typi-cal full-blown manic syndrome with in-creased pressure of speech, rhyming ofwords, and paranoid ideation was pre-sent.
Cognitive Disturbances. Difficultywith concentration was frequently noted.Patients complained of mind-wanderingwhen reading, watching television, andduring the course of conversations. Theyreported a decreased ability to focus theirminds, inattention, distractibility, andshortened attention span.
Difficulty with reasoning ability, com-prehension, and processing of new infor-mation was reported. There were distur-bances in the rate of thinking: some pa-tients reported episodes of rapid and scat-tered thinking; others complained of slowand ponderous thinking. Blocking oc-curred, so that patients would experiencetheir thoughts suddenly gone and theirminds becoming blank while thinking orspeaking.
Psychosomatic Medicine Vol. 43, No. 1 (February 1981)

MONICA N. STARKMAN et al.
Patients complained of not being ableto think of or articulate the proper word,using incorrect words while speaking, or-dering words incorrectly in a spokenphrase, and misspelling simple words.
Impairment of memory was one of themost frequent symptoms. Patients re-ported problems with registration of newinformation, which could be related inpart to impaired concentration. Theycommonly repeated themselves in ongo-ing conversations. They easily forgotitems such as appointments made, namesof people, and location of objects. Diffi-culty occurred with recall of importantdates in their personal or medical his-tories.
Disorientation and Confusion. Twopatients mentioned having difficulty re-calling the day of the week. Three of thefour most severely disturbed patients ex-perienced at least one confusional episodeof severe degree.
Basic Biological "Vegetative" Drives.Data on three areas of basic biological"vegetative" drives were reported:
1) -Appetite and Eating Behav-ior: Fifty-two percent of the patientshad an alteration in their appetite: in34%, appetite had increased, in 20%, ithad decreased.2] Libido: A decrease in libido was alsofrequent. Several patients remarked thatthis symptom appeared very early in thecourse of their disease.3) Sleep and Dreams: Difficulty withsleep, particularly middle night insom-nia and late insomnia (early morningawakening), was found in more than50% of the patients. Difficulty withearly insomnia (not falling asleep atbedtime) was not as frequent. One-thirdof the patients reported an alteration in
the frequency or quality of their dreams.Some noted an absence of dreams;others reported a marked increase intheir frequency and intensity. Theirdreams had become bizarre, oftenfrightening, and very vivid. These pa-tients also reported that they had lostthe ability to wake themselves out of anightmare.
Perceptual Disorders. Perceptual dis-tortions were rare. Three nondelirious pa-tients did report instances when doorframes or pictures on the wall appeared tobe slanted, yet when measured or ob-served by others this was not the case.One patient reported an episode of a vis-ual illusion during which a metal showerbar seemed to be bending out of shape asshe was watching it.
Mental Status Examination
The frequency of abnormal findings inthe mental status examination is shown inTable 2. Notable are the difficulties withserial 7 subtractions, interpretation ofproverbs, and recall of presidents seen inclose to 50% of the patients. Difficultywith recall of 3 cities after 15 minutes wasseen in more than 30% of the patients.
Overall Psychiatric Disability
The overall psychiatric disability scoresof the 35 patients were as follows: Thirty-four percent were rated as having a mildpsychiatric disability, 26% moderate,29% severe, and 11% very severepsychiatric disability.
There was variability in the clinicalpresentation of the four patients rated ashaving a very severe psychiatric disabil-ity. One of the two patients with pituitaryACTH-dependent Cushing's syndromewas depressed with paranoid ideation.
Psychosomatic Medicine Vol. 43, No. 1 (February 1981)

PSYCHIATRIC MANIFESTATIONS OF CUSHING'S SYNDROME
The other was troubled predominantly byepisodic confusional states. One patientwith an ectopic ACTH-secreting thymomawas manic with paranoid ideation. Onepatient with still unclassified ACTH-dependent syndrome was depressed andconfused with paranoid ideation.
Association of Hormone Levelswith Overall Psychiatric Disability
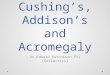
The association of cortisol and ACTHlevels with overall psychiatric disabilityrating is shown in Figure 1.
An analysis of variance revealed astatistically significant relationship be-tween the overall psychiatric disabilityscore and the degree of cortisol elevationas measured by the cortisol secretion rate(p = 0.00), urinary free cortisol (p = 0.00),and plasma cortisol at 8 AM (p = 0.02). Foreach of these three measures of cortisol,the most severely disturbed group of pa-tients (those manifesting a thought disor-der with paranoid ideation and/or confu-sional states) had the highest hormonelevels and were clearly differentiated fromthe rest of the sample.
« TJ
2 3
SCORES
EJ
2 3
SCORES
Fig. 1 Relationship between severity of overall psychiatric disability and hormone levels in Cushing'ssyndrome, (mean ± SEM) Of all 35 patients, 34% had an overall disability rating of 1 (mild), 26% of2 (moderate), 29% of 3 (severe), and 11% of 4 (very severe).
Psychosomatic Medicine Vol. 43, No. 1 (February 1981)

MONICA N. STARKMAN et al.
There was also a statistically significantrelationship found between the overallpsychiatric disability rating and ACTH (p= 0.01). In contrast, such a relationshipwas not found between the overall disabil-ity rating and serum DHEA (p = 0.66).
Association of Hormone Levelswith Depressed Mood
The association of cortisol and ACTHlevels with the specific symptom, de-pressed mood, is of particular interest.Analysis of these data will be presented inseveral forms.
In the first group of analyses, each hor-mone is considered separately. As shownin Table 3 , 2 X 2 tables were constructed.Depressed mood scores were collapsedinto two categories: milder (0, 1) andpronounced (2, 3). Cortisol secretion rate,urinary free cortisol, and ACTH levelswere also collapsed into two categories.Although the data suggest that highercortisol levels are more likely to be as-sociated with milder rather than pro-nounced depressed mood, this relation-ship did not reach statistical significance.
TABLE 3. The Relationship of Depressed Mood toCortisol and ACTH Levels
CortisolSecretionRates
UrinaryFreeCortisol
PlasmaACTH
Depressed Mood Score
moderate
high
moderate
high
low, normalmoderate, high
0, 1
9
13
7
14
10
10
2, 3
3
8
7
4
0
10
P
0.70
0.14
0.01
The association of ACTH and depressedmood did reach statistical significance(Fisher exact probability = 0.01). Of 10patients with low or normal ACTH levels,all reported milder rather than pro-nounced depressed mood. No patientwith a pronounced depressed mood had alow or normal ACTH level. It should benoted that patients with moderate to highACTH levels were not necessarily se-verely depressed and were equally likelyto show milder or pronounced depressedmood.
The data in their original non-categorized form were also analzyedusing an analysis of variance. With thismethod of analysis, the association be-tween depressed mood and ACTH, thethree measures of cortisol and DHEA,each examined separately, did not reachstatistical significance.
In the next group of analyses, the datawere examined in order to study the rela-tionship of depressed mood and the levelsof cortisol and ACTH considered together.The results of these analyses suggest thatdepressed mood may be associated withthe balance between ACTH and cortisol.
Figure 2 depicts the relationship be-tween depressed mood scores and thelevels of urinary free cortisol and plasmaACTH. (Urinary free cortisol is used be-cause it is directly correlated with thelevel of biologically active free cortisol inplasma.) In the upper half of the figure,this relationship is shown for the entiresample of 35 patients; in the lower half,for the patients with pituitary ACTH-dependent Cushing's syndrome without adetectable pituitary tumor. Depressedmood scores on a 4-point scale (none,mild, moderate, severe) are shown on thehorizontal axis. For each mood score, themean urinary free cortisol level is shownin crosshatched bars on the left and the
10 Psychosomatic Medicine Vol. 43, No. 1 (February 1981)

PSYCHIATRIC MANIFESTATIONS OF CUSHING'S SYNDROME
18001- A. ALL PATIENTS
a.8 - .
!i a
8. PITUITARY ACTH-DEPENDENT
< 200
11
DEPRESSED MOOD SCORE
Fig. 2. Relationship between depressed mood scores and mean (± SEM) levels of cortisoland ACTH in Cushing's syndrome. Of all patients (upper half of figure), 26% had adepressed mood score of 0 (none), 42% of 1 (mild), 23% of 2 (moderate), and 9% of3 (severe).
mean ACTH level is shown in open barson the right. It can be seen that at each ofthe four depressed mood scores, there aredifferences in the relative proportion ofcortisol to ACTH: as the depressed moodscore increases, the relative proportion ofcortisol to ACTH decreases.
The "corelationship" of ACTH and cor-tisol with depressed mood was exploredfurther. The ratio of free cortisol to ACTHwas generated for each patient, and ananalysis of variance was performed. Theresults of this analysis are depicted in
Figure 3. The top panel of the figureshows this relationship for the total sam-ple; the middle panel only for patientswith pituitary ACTH-dependent Cush-ing's syndrome without a demonstrablepituitary tumor. Although statistical sig-nificance is not reached, a tendency issuggested: as the degree of depressionincreases, the ratio of cortisol to ACTHdecreases. For the patients with adrenaladenomas, shown in the bottom panel,this relationship is readily apparent andreaches statistical significance.
Psychosomatic Medicine Vol. 43, No. 1 (February 1981) 11

MONICA N. STARKMAN et al.
A.-ALL PATIENTS
P = 1 1
B.-PITUITARY ACTH-OEPENDENT
C.-ADRENAL ADENOMA
0 1 2 3DEPRESSED MOOD SCORE
Fig. 3. Relationship between depressed moodscore and the ratios of urinary freecortisol to ACTH (UFF/ACTH 8) (mean± SEM).
Relationship of Depressed Moodand Etiologic Type of Cushing'sSyndromeAs noted previously, it is of interest to
compare the association of depressed
mood and etiologic type of Cushing'ssyndrome since these types have differingprofiles of ACTH and cortisol and dif-ferent pathways of origin of the illness.Table 4 shows the 2 times 2 table con-structed to compare depressed moodscores in patients with pituitary ACTH-dependent Cushing's syndrome without ademonstrable pituitary tumor (high cor-tisol, high ACTH levels] and in patientswith adrenal adenomas (high cortisol, lowACTH levels). Although statistical sig-nificance is not reached, all the patientswith adrenal adenomas reported milderrather than marked depressed mood.Using Student's t-test, the mean cortisollevels of these two etiologic subgroupswere not significantly different; the meanACTH levels were significantly different(p < 0.05).
DISCUSSION
A constellation of symptoms includingirritability, mood disturbance, impairedmemory, poor concentration, decreasedlibido, and insomnia occurred with highfrequency in Cushing's syndrome. Addi-tional psychiatric symptomatology ofgreater severity, such as paranoid andconfusional states, were much less fre-quent and were associated with particu-
TABLE 4. Comparison of Depressed Mood in Sub-types of Cushing's Syndrome
PituitaryACTH-dependent
Adrenaladenoma
Depressed Mood Score
0,1 2,3 p
15
5
7
0
0.28
12 Psychosomatic Medicine Vol. 43, No. 1 (February 1981)

PSYCHIATRIC MANIFESTATIONS OF CUSHINC'S SYNDROME
larly high cortisol and ACTH levels. Thefour patients in the present study with themost severe overall psychiatric disabilityhad a mean cortisol secretion rate of 157mg per day, which is the equivalent ofapproximately 40 mg of prednisone perday. This parallels the observation thatduring steroid therapy the probability ofdeveloping an acute psychotic reaction ishighest when daily doses greater than 40mg of prednisone or its equivalent areadministered (1, 2).
Although an age-matched controlgroup of hospitalized patients withnonendocrine illness was not studied, theconstellation of psychiatric symptomsthat develop in Cushing's syndrome andthe quality of the symptoms argue for apathogenesis over and above a non-specific response to severe physical ill-ness. Irritability and decreased libido oc-cur early, often before patients are awarethat they have any physical problem otherthan a steady increase in weight. De-pressed mood is experienced not simplyas the demoralization common to patientswith medical illness, but also as episodicsadness and crying often occurring in theabsence of depressing thought content.The characteristic disorders of memoryand concentration occur in patients whohave no disorientation or overt cloudingof consciousness. Of the 35 patients in thestudy, the electroencephalographs (EEGs)of only two were characteristic of de-lirium. (Both had been classified as hav-ing very severe psychiatric disability priorto knowledge of EEG findings.)
A consistent pattern of premorbid func-tioning or personality type was not foundas a possible predisposing factor. Al-though some patients had stormy premor-bid psychosocial functioning, others hadstable family lives and work histories. Nosingle personality trait such as obsessive-
compulsive or hysteric predominatedamong these patients.
The relationship of depressed mood tocortisol and ACTH levels is of particularinterest. When the data were examined incategorized form with each hormone con-sidered separately, higher cortisol levelswere more likely to be associated withmilder rather than pronounced depressedmood, although statistical significancewas not reached. In contrast, lower ACTHlevels were significantly associated withmilder rather than pronounced depressedmood. Further, the work reported heresuggests that the relative proportion ofcortisol to ACTH, rather than the level ofeither hormone by itself, may be related tothe severity of depressed mood. Althoughhigher ACTH levels in themselves werenot uniformly associated with more se-vere depressed mood, there was a ten-dency for the degree of depressed mood toincrease as the ratio of cortisol to ACTHdecreased. Even though the relationshipwas not statistically significant, this pat-tern showed some specificity. That is,when items related to depressed mood,such as crying, guilt, and hopelessness,were examined, this pattern of increasingseverity with decreasing cortisol/ACTHratios was also noted. In contrast, greaterdifficulties with concentration tended tooccur with increasing cortisol/ACTHratios.
Patients with adrenal adenomas, be-cause of their suppressed ACTH produc-tion, have a high cortisol /ACTH ratio. Inour study, less severe depressivesymptoms were seen in such patients ascompared with those with pituitary-ACTH disorders. Unfortunately, since ad-renal adenomas occur infrequently, thenumber of patients with adenomas in ourseries is small and this observation didnot reach statistical significance. The
Psychosomatic Medicine Vol. 43, No. 1 (February 1981) 13

MONICA N. STARKMAN et al.
finding is supported, however, by twoprevious reports. In a review of 78 cases ofCushing's syndrome reported in the litera-ture, Carroll (10) found that although % ofpatients with pituitary-ACTH distur-bances had "a problem with depression,"only V* of patients with predominantlyadrenal tumor disease had depression.This difference was highly statisticallysignificant. Second, in a recent clinicalstudy, Cohen (11) found that 3 of 8 pa-tients with adrenal tumors were free ofpsychiatric disorder, whereas only 1 of 21patients with bilateral adrenalhyperplasia (pituitary ACTH-dependentdisease) were free of psychiatric disorder,a difference that was also statistically sig-nificant. The high ratio of cortisol toACTH in patients with adrenal adenomasreflects the different pathway of origin ofCushing's syndrome, which may be thecritical factor for the presence and degreeof depressed mood and other psychiatricsymptoms. For example, although there isinsufficient data to support the hypo-thesis, it has been suggested that somecases of pituitary ACTH-dependent Cush-ing's syndrome result from a primary dis-order in the limbic system leading to anoverproduction of corticotrophin releas-ing factor (CRF) and thence to increasedsecretion of ACTH and cortisol (12).
In Addison's disease, a low cortisol/ACTH ratio is a consistent metabolic fea-ture: primary failure of the adrenal cortexleads to subnormal levels of cortisol, andhypersecretion of ACTH occurs due to thelack of feedback inhibition by cortisol.Clinically, depression has been reportedas a frequent finding in Addison's disease(13). Thus, in this disease, depressedmood is associated with a low cortisol/ACTH ratio.
These observations support the specu-lation by Sachar (14) and others that
excess ACTH itself exerts primarily a de-pressing effect on mood, whereas excesscorticosteroids may tend to producemostly elation. However, it seems likelythat the phenomenon is more complexthan a simple arithmetic effect based onthe relative proportion of the two hor-mones. We have observed a small numberof patients with normal cortisol levels andhighly elevated ACTH levels who are notseverely depressed despite a low cor-tisol/ACTH ratio. (These patients, whodid not have active Cushing's syndromeand thus did not meet the criteria forinclusion in this study, had developedACTH-secreting pituitary macroad-enomas postadrenalectomy.) It may bethat normal levels of cortisol stabilizeimportant psychoneurophysiologic sys-tems and protect against the effects ofelevated ACTH levels. Conversely, ab-normally elevated or deficient levels ofcortisol, as in active Cushing's syndromeor Addison's disease, respectively, maydestabilize these important systems, mak-ing the nervous system more vulnerable tothe effects of elevated ACTH. A similarmechanism has been proposed by Prange(15) with regard to the role of neuro-transmitters in affective disorders. He hassuggested a "permissive hypothesis" inwhich a central indoleaminergic deficitmay permit the development of affectivedisorder but is insufficient in itself so thatan associated decrease in catecholamineactivity is required for the onset of depres-sion.
Patients with Cushing's syndrome meetcriteria for organic brain syndromes andindeed are so classified in DSM-III asexamples of Organic Affective Syndrome.Their affective lability, irritability, im-paired concentration, and distractibilityare characteristic of organic etiology. Ab-normalities during mental status testing
14 Psychosomatic Medicine Vol. 43, No. 1 (February 1981)

PSYCHIATRIC MANIFESTATIONS OF CUSHING'S SYNDROME
are present despite most patients' effortsto perform well. However, these patientsdemonstrate some unique features. Al-though they complain of feeling "foggy,"which may represent some clouding ofconsciousness, they are not disoriented.Although a small minority report visualillusions, most have neither visual norauditory hallucinations. Most retain somecapacity for abstract thinking and many,though not all, continue to retain em-ployment because their cognitive im-pairment is not at the level of severedeterioration.
At the same time, patients with Cush-ing's syndrome demonstrate many of theclinical features of a primary depressivedisorder, particularly the vegetative onessuch as disturbances of sleep, libido, andappetite. Indeed, the majority of patientswith Cushing's syndrome could meet theDSM-III diagnostic criteria for a MajorDepressive Disorder (except for the exclu-sion of an Organic Mental Disorder). Al-though similar in many respects to themajor depressive disorders, the depres-sion seen in Cushing's syndrome has cer-tain unique characteristics. Irritability is aprominent and consistent feature. De-pressed affect is intermittent, withepisodes of 1-3 days duration, recurringvery frequently at irregular intervals. Be-cause of this, patients do not experiencethe relentless depressed mood and unre-mitting persistent anhedonia so charac-teristic of most patients with primary en-dogenous depression. Psychomotor retar-dation, although present in many pa-tients, is usually not so pronounced as tobe clinically obvious and is usually ap-parent only in retrospect after improve-ment with treatment. The majority ofthese patients are not withdrawn, apathe-tic, monosyllabic, unspontaneous, orhopeless. Significant cognitive impair-
ment including disorder of memory is aconsistent and prominent clinical featureof patients with Cushing's syndrome.
It is of interest that a syndrome soclearly organic in etiology has many fea-tures associated with primary depressivedisorder. This may suggest the presenceof similarities in the pathophysiology ofCushing's syndrome and depressive dis-orders.
One line of evidence supporting thisview concerns the endocrine abnor-malities that have been found in bothdisorders. In Cushing's syndrome, ele-vated cortisol levels and resistance topituitary-adrenal suppression by the syn-thetic steroid dexamethasone are diagnos-tic features of the disease. As for depres-sive disorder, a substantial proportion ofdepressed patients also show elevatedcortisol levels and escape from pituitary-adrenal suppression by dexamethasone(16).
Biogenic amines have been implicatedin the hypothalamic regulation of the re-lease of anterior pituitary hormones, in-cluding ACTH (17). There is a vast body ofliterature regarding the relationship ofdepression and biogenic amines. Al-though the confirmatory evidence is in-complete, it is possible that at least somedepressions are associated with an abso-lute or relative deficiency of catechol-amines, particularly norepinephrine, atimportant adrenergic receptor sites in thebrain (18).
Corticosteroids have significant effectson intracellular electrolytes. Experimentsin animals have indicated that glucocor-ticoids mediate shifts of electrolytes .andwater at the cellular level and that cortisolcan exert effects on brain intracellularsodium (19, 20). Clinical depression hasbeen found to be associated with sodiumretention, and an increase in erythrocyte
Psychosomatic Medicine Vol. 43, No. 1 (February 1981) 15

MONICA N. STARKMAN et al.
sodium concentration has been describedin association with the successful treat-ment of depressed patients with lithiumcarbonate. It has been hypothesized thatthere may be a subgroup of depressedpatients with a genetically determinedabnormality affecting movement of elec-trolytes across the cell membrane (21).
Neuroactive peptides are probably ofmajor importance. One such peptide,/3-endorphin, arises from the same pitu-itary precursor molecule as does ACTH(22). /8-endorphin and ACTH are secretedconcomitantly in increased amounts inresponse to an ACTH-releasing stimulus(23). It seems reasonable to expect thatwhen abnormalities in the production ofACTH exist, such as in pituitary ACTH-dependent Cushing's syndrome, abnor-mal levels of /3-endorphin might occuras well. Although plasma levels of/3-endorphin in control subjects are low,/3-endorphin has been found to beelevated in the plasma of patients withCushing's disease (24). The role of/3-en-dorphins in psychiatric disease is as yetunclear. Although preliminary studiesreport changes in psychiatric symptom-atology with administration of /3-endorphinor the opiate antagonist, naloxone, theseearly studies are often contradictory andincomplete (25). Since depressed patientshave been shown to have increased painthresholds and pain tolerance when com-pared with normal subjects, Davis (26) hassuggested that a relative excess of endor-phins may play a role in both the relativeanalgesia and psychiatric symptoms seenin patients with depressive disorders.
The clinical similarity between patientswith Cushing's syndrome and patientswith depressive disorders may haveanother explanation. It may reflect thelimited number of behavioral responsesavailable to diverse physiologic or
biochemical disturbances. For example, itis usually impossible to determine theetiology of an acute delirium by any dis-tinguishing features of the clinical presen-tation. While the search for specificity inthe biochemistry of mental disorders pro-ceeds, it is useful to keep in mind that thebrain may have a limited number of "finalcommon pathways" and that similar re-sponses to a wide variety of etiologicfactors may occur.
This hypothesis would suggest thatother neuropsychiatric similarities be-tween Cushing's syndrome and depres-sive disorder might also exist. One suchsimilarity may be the presence of signifi-cant cognitive deficits in both disorders.Cognitive deficits in primary depressivedisorders are generally viewed as second-ary to disturbances in affect and due todecreased motivation. Individuals withdepression are considered to have intactcognitive function provided that they aresufficiently motivated to perform. How-ever, cognitive deficits in depressive dis-orders may be largely unrecognized sincemost current research on depression usesinstruments that focus on the affectiveand vegetative characteristics of depres-sion and not on cognitive disorders. Theevidence for the existence of significantcognitive deficits in affective disordershas been reviewed recently (27). Furthersupport comes from a study in whichpatients with affective disorders madesignificantly more errors on an aphasiascreening test measuring language andmotor-perceptual dysfunction than didcontrol subjects (28).
SUMMARY
In 35 consecutive patients with Cush-ing's syndrome studied prior to treatment,
16 Psychosomatic Medicine Vol. 43, No. 1 (February 1981)

PSYCHIATRIC MANIFESTATIONS OF CUSHING'S SYNDROME
a consistent constellation of psychiatricdisturbances was found. Irritability, de-pressed mood, decreased libido, insom-nia, poor concentration, and impairedmemory occurred with high frequency inCushing's syndrome. Psychotic and/orconfusional states were much less fre-quent and were associated with particu-larly high cortisol and ACTH levels. Theconstellation of symptoms and theircharacteristics argue for a pathogenesisover and above a nonspecific response tosevere physical illness.
The relationship of depressed mood tocortisol and ACTH levels was examined.Higher cortisol levels were more likely tobe associated with milder rather than pro-nounced depressed mood. In contrast,lower ACTH levels were significantly as-sociated with milder rather than pro-nounced depressed mood. Furthermore,
the data suggest that the relative propor-tion of cortisol to ACTH may be related tothe severity of depressed mood.
The observation that patients withCushing's syndrome have many featuresassociated with primary depressive dis-ease suggests the presence of similaritiesin the pathophysiology of both types ofdisorder. Evidence is reviewed that altera-tions in biogenic amines, electrolyteshifts, and/or neuroactive peptides maybe of significance in both types of disor-ders. Alternatively, the similar clinicalfeatures may reflect the limited number ofbehavioral responses available to diversephysiologic or biochemical disturbances.
This research was supported in part byU.S. PubJic Health Service Grant 5 MolRR-4216.
REFERENCES
1. Boston Collaborative Drug Surveillance Program: Acute adverse reactions to prednisone in relation todosage. Clin Pharmacol Ther 13:694-698, 1972
2. Hall RCW, Popkin MK, Stickney SK, et al: Presentation of the steroid psychoses. J Nerv Ment Dis167:229-236, 1979
3. Trethowan WH, Cobb S: Neuropsychiatric aspects of Cushing's syndrome. AMA Arch NeurolPsychiatry 67:283-309, 1952
4. Hamilton M: A rating scale for depression. J Neurol Neurosurg Psychiatry 23:55-62, 19605. Spitzer RL, Endicott J, Robins, E: Research diagnostic criteria. Rationale and reliability. Arch Gen
Psychiatry 35:773-782, 19786. Schteingart DE, Gregerman RI, Conn JW: A comparison of the characteristics of increased adrenal
corticol function in obesity and Cushing's syndrome. Metabolism 12:484-497, 19637. Dash AJ, England BG, Midgley AR, et al: Specific non-chromatographic radioimmunoassay for human
plasma cortisol. Steroids 26:647-661, 19758. Vague PH, Oliver C, Jaquet P, et al: Le dosage radio-immunologique de l'ACTH plasmatique. Eur J Clin
Biol Res 16:485-493, 19719. Buster JE, Abraham GE: Radioimmunoassay of plasma DHEA sulfate. Ann Letters 5:203-215, 1972
10. Carroll BJ: Psychiatric disorders and steroids, in Neuroregulators and Psychiatric Disorders. Edited by EUsdin, DA Hamburg, JD Barchas. New York, Oxford University Press, 1977, pp. 276-282
11. Cohen SI: Cushing's syndrome: A psychiatric study of 29 patients with observations on the aetiology ofthe depressive symptoms. Br J Psychiatry 133:371, 1978
12. Krieger DT: The central nervous system and Cushing's syndrome. Mt. Sinai J Med NY 39:416-428,1972
Psychosomatic Medicine Vol. 43, No. 1 (February 1981) 17

MONICA N. STARKMAN et al.
13. Cleghorn RA: Adrenal cortical insufficiency: Psychological and neurological observations. Can MedAssoc J 65:449-454, 1951
14. Sachar EJ: Psychiatric disturbances associated with endocrine disorders, in American Handbook ofPsychiatry, vol. 4. Edited by MF Reiser. New York, Basic Books, 1975, pp. 299-313
15. Prange AJ, Wilson I, Lynn CW, et al: L-Tryptophan in mania. Contribution to a permissive hypothesis ofaffective disorders. Arch Gen Psychiatry 30:56-62, 1974
16. Brown WA, Johnston R, Mayfield D: The 24-hour dexamethasone suppression test in a clinical setting:Relationship to diagnosis, symptoms, and response to treatment. Am J Psychiatry 136:543-547, 1979
17. Ettigi PG, Brown GM: Psychoneuroendocrinology of affective disorder: An overview. Am J Psychiatry134:493-501, 1977
18. Schildkraut JJ: The catecholamine hypothesis of affective disorders: A review of supporting evidence.Am J Psychiatry 122:509-522, 1965
19. Swingle WW, DaVanzo JP, Glenister D, et al: Effect of mineralo- and glucocorticoids on fastedadrenalectomized dogs subjected to electroshock. Proc Soc Exp Biol Med 104:184-188, 1960
20. Woodbury DM: Relation between the adrenal cortex and the central nervous system. Pharmacol Rev10:275-357, 1958
21. Mendels J, Frazer A: Lithium distribution in depressed patients: implications for an alteration in cellmembrane function in depression, in The Psychobiology of Depression. Edited by J Mendels. New York,Spectrum Publications, 1975
22. Mains RE. Eipper BA, Ling N: Common precursor to corticotropins and endorphins. Proc Natl Acad SciUSA, 74:3014-3018, 1977
23. Nakao K, Nakai Y, Oki S, et al: Presence of immunoreactive /3-endorphin in normal human plasma. JClin Invest 68:1395-1398, 1978
24. Suda T, Liotta A, Krieger DT: /3-endorphin is not detectable in plasma from normal human subjects.Science 202:221-223, 1978
25. Verebey K, Volavka J, Clouet D: Endorphins in psychiatry. An overview and a hypothesis. Arch GenPsychiatry 35:877-888, 1978
26. Davis GC, Buchsbaum MS, Bunney WE: Analgesia to painful stimuli in affective illness. Am JPsychiatry 136:1148-1151, 1979
27. Kirstein L, Bukberg J: Temporal disorganization and primary affective disorder. Am J Psychiatry136:1313-1316, 1979
28. Taylor MA, Greenspan B, Abrams R: Lateralized neuropsychological dysfunction in affective disorderand schizophrenia. Am J Psychiatry 136:1031-1034, 1979
18 Psychosomatic Medicine Vol. 43, No. 1 (February 1981)